Title Page:
Type of manuscript:Brief communications
Manuscript title:Synergistic interaction between alcoholism and polypharmacy on the risk of falls in the elderly
Running head:alcoholism and polypharmacy
Authors' full names:
Hsien-Feng Lin, MD and MS 1,2; Shih-Wei Lai, MD,2,3; Kuan-Fu Liao, MD and MS 4,5,,6; Chih-Hsin Muo, MPH 7,,8; Dennis Paul Hsientang Hsieh, ScD 9
1 School of Chinese Medicine, ,3School of Medicine, 7Department of Public Health, and
9Department of Health Risk Management, China Medical University, Taichung, 404, Taiwan
2Department of Family Medicine, and 8Management Office for Health Data, China Medical University Hospital, Taichung, 404, Taiwan
4Department of Internal Medicine, Taichung Tzu Chi General Hospital, Taichung, 427, Taiwan
5School of Medicine, Tzu Chi University, Hualien, 970, Taiwan
6Department of health care administration, Central Taiwan University of Science and Technology, Taichung, 406, Taiwan
(The first three authors contributed equally to this study.)
Co-corresponding author:
Professor Dennis Paul Hsientang Hsieh, Sc.D.
Department of Health Risk Management, College of Public Health, China Medical University, 91 Hsueh-Shih Road, Taichung, 404, Taiwan
Tel: 886-4-2205-3366 ext 6510 Fax: 886-4-2207-0429 E-mail: dphsieh@mail.cmu.edu.tw
Word counts: 186 in abstract, 681 in the text, 2 tables, and 9 references Key words: alcoholism; polypharmacy; falls; elderly
ABSTRACT
The aim of this study was to explore the interaction between alcoholism and polypharmacy on the risk of falls in the elderly in Taiwan. A dataset of one million randomly sampled National Health Insurance claims in Taiwan was used in our analysis, from which 3482 new cases of falls in 2000-2008 and 13928 randomly selected controls without falls, both aged ≥ 65 years, were identified for a case-control study. Polypharmancy was defined as the average daily use of 5 or more prescribed drugs. Relative risks were estimated by adjusted odds ratio (OR) and 95% confidence interval (CI) using a multivariate logistic regression analysis. In comparison with subjects using 0-1 drug without alcoholism, the OR increased from 1.15 (95% CI 1.01-1.32) for those using 2-4 drugs without alcoholism, to 1.27 (95% CI 1.10-1.47) for those using ≥ 5 drugs without alcoholism, up to 5.32 (95% CI 1.58-18.0) for those using 2-4 drugs with alcoholism, and as high as to 6.29 (95% CI 2.22-17.8) for those using ≥ 5 drugs with alcoholism. We conclude that polypharmacy may interact with alcoholism and further increases the risk of falls in the elderly.
Key words: alcoholism; polypharmacy; falls; elderly
Brief communications
Little is known about the interaction between alcoholism and polypharmacy on the risk of falls in the elderly in Taiwan. We designed a case-control study using a dataset of one million randomly sampled National Health Insurance claims in Taiwan. The insurance program details can be found in previous studies 1-3. In this present study, 3482 subjects aged 65 or older presenting with the diagnosis of incident falls in ambulatory care from 2000 to 2008 were designated as “cases” (1627 men and 1855 women, mean age 78.5 years, standard deviation 7.4 years), based on diagnostic codes of the International Classification of Diseases (ICD) 9th Revision (ICD-9 codes E880- E888) 4. There were 13928 randomly selected individuals without falls as controls, also aged 65 years or older (8771 men and 5157 women, mean age 76.4 years,
standard deviation 5.9 years). Polypharmacy was defined as the average daily use of 5 or more prescribed drugs 5, 6. Relative risks were estimated by adjusted odds ratio (OR) and 95% confidence interval (CI) using a multivariate logistic regression
analysis.
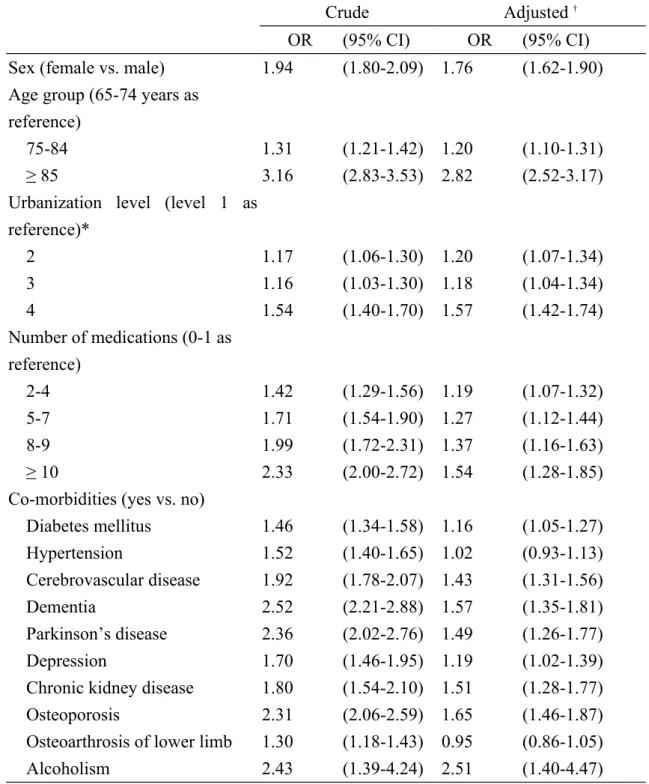
The subjects categorized as polypharmacy were more prevalent in falls cases than in controls (39.5% vs.29.1%, P < 0.001). After adjustment for covariates, in comparison with subjects using 0-1 drug, the adjusted ORs of falls were 1.19 (95% CI 1.07-1.32) in those using 2-4 drugs, 1.27 (95% CI 1.12-1.44) in those using 5-7 drugs, 1.37 (95%
CI 1.16-1.63) in those using 8-9 drugs, and 1.54 (95% CI 1.28-1.85) in those using ≥ 10 drugs. After adjusting for covariates, the results of multivariate unconditional logistic regression analysis indicated that female gender (OR 1.76, 95% CI 1.62-1.90) was strongly associated with falls. In addition, diabetes mellitus (OR 1.16, 95% CI 1.05-1.27), cerebrovascular disease (OR 1.43, 95% CI 1.31-1.56), dementia (OR 1.57, 95% CI 1.35-1.81), Parkinson’s disease (OR 1.49, 95% CI 1.26-1.77), depression (OR 1.19, 95% CI 1.02-1.39), chronic kidney disease (OR 1.51, 95% CI 1.28-1.77), osteoporosis (OR1.65, 95% CI 1.46-1.87), and alcoholism (OR 2.51, 95% CI 1.40- 4.47) were found as independent co-morbidities significantly associated with falls. In comparison with subjects aged 65-74, the ORs of falls were 1.20 (95% CI 1.10-1.31) in subjects aged 75-84, and 2.82 (95% CI 2.52-3.17) in subjects aged 85 and above. In comparison with subjects living in urbanization level 1, the ORs of falls were 1.20 (95% CI 1.07-1.34) in those living in urbanization level 2, 1.18 (95% CI 1.04-1.34) in those living in urbanization level 3, and 1.57 (95% CI 1.42-1.74) in those living in
urbanization level 4 (Table 1).
Table 2 shows the synergistic interactions between alcoholism and number of medications associated with falls. In comparison with subjects using 0-1 drug without alcoholism, the OR increased, from 1.15 (95% CI 1.01-1.32) for those using 2-4 drugs without alcoholism, to 1.27 (95% CI 1.10-1.47) for those using ≥ 5 drugs
without alcoholism, up to 5.32 (95% CI 1.58-18.0) for those using 2-4 drugs with alcoholism, and as high as to 6.29 (95% CI 2.22-17.8) for those using ≥ 5 drugs with
alcoholism.
In systematic reviews on drugs and falls, Leipzig and et al. found that the elderly using more than three medications were at increased risk of recurrent falls 7.
Similarly, Corsinovi and et al. reported that the elderly with polypharmacy were more likely to experience falls (relative risk 1.226; 95% CI 1.122-1.340) 8. In this present study, multivariate logistic regression analysis showed that the risk of falls indeed increased with number of medications used, in a dose-dependent fashion. In other words, the more the medications used, the higher the risk of falls. In further analysis, we found there were synergistic interactions between alcoholism and number of medications on the risk of falls. The odds ratio of falls increased to 6.29 for patients with alcoholism and using ≥ 5 drugs. These findings further alert the clinicians about the risk of falls in the elderly when simultaneously exposure to alcoholism and
polypharmacy.
We conclude that risk of falls in the elderly increases with number of medications used, in a dose-dependent fashion in Taiwan. Polypharmacy may interact with alcoholism and further increases the risk of falls.
Funding: This study was supported in part by grants from Taiwan Department of Health Clinical Trial and Research Center of Excellence (DOH101-TD-B-111-004), the Cancer Research Center of Excellence (DOH 100-TD-C-111-005), the National Science Council (NSC 100-2621-M-039-001), and China Medical University Hospital (1MS1). The funding agencies did not influence the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgements: The authors thank the National Health Research Institute in Taiwan for providing the insurance claims data.
REFERENCES
1. Lai SW, Chen PC, Liao KF, et al. Risk of hepatocellular carcinoma in diabetic patients and risk reduction associated with anti-diabetic therapy: a population-based cohort study. Am J Gastroenterol 2012;107:46-52.
2. Lai SW, Liao KF, Chen PC, et al. Antidiabetes drugs correlate with decreased risk of lung cancer: a population-based observation in taiwan. Clin Lung Cancer 2012;13:143-148.
3. Liao KF, Lai SW, Li CI, et al. Diabetes mellitus correlates with increased risk of pancreatic cancer: A population-based cohort study in Taiwan. J Gastroenterol Hepatol 2012;27:709-713.
4. Huang ES, Karter AJ, Danielson KK, et al. The association between the number of prescription medications and incident falls in a multi-ethnic population of adult type-2 diabetes patients: the diabetes and aging study. J Gen Intern Med 2010;25:141-146.
5. Lai SW, Liao KF, Liao CC, et al. Polypharmacy correlates with increased risk for hip fracture in the elderly: a population-based study. Medicine (Baltimore) 2010;89:295-299.
6. Lai SW, Su LT, Lin CH, et al. Polypharmacy increases the risk of Parkinson's disease in older people in Taiwan: a population-based study.
Psychogeriatrics 2011;11:150-156.
7. Leipzig RM, Cumming RG, Tinetti ME. Drugs and falls in older people: a systematic review and meta-analysis: I. Psychotropic drugs. J Am Geriatr Soc 1999;47:30-39.
8. Corsinovi L, Bo M, Ricauda Aimonino N, et al. Predictors of falls and hospitalization outcomes in elderly patients admitted to an acute geriatric unit. Arch Gerontol Geriatr 2009;49:142-145.
9. Liu CY, Hung YT, Chuang YL, et al. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J Health Management 2006;49:1-22.
Table 1. Crude and adjusted odds ratios and 95% confidence intervals of falls associated with number of medications by multivariate logistic regression
Crude Adjusted †
OR (95% CI) OR (95% CI)
Sex (female vs. male) 1.94 (1.80-2.09) 1.76 (1.62-1.90) Age group (65-74 years as
reference)
75-84 1.31 (1.21-1.42) 1.20 (1.10-1.31)
≥ 85 3.16 (2.83-3.53) 2.82 (2.52-3.17)
Urbanization level (level 1 as reference)*
2 1.17 (1.06-1.30) 1.20 (1.07-1.34)
3 1.16 (1.03-1.30) 1.18 (1.04-1.34)
4 1.54 (1.40-1.70) 1.57 (1.42-1.74)
Number of medications (0-1 as reference)
2-4 1.42 (1.29-1.56) 1.19 (1.07-1.32)
5-7 1.71 (1.54-1.90) 1.27 (1.12-1.44)
8-9 1.99 (1.72-2.31) 1.37 (1.16-1.63)
≥ 10 2.33 (2.00-2.72) 1.54 (1.28-1.85)
Co-morbidities (yes vs. no)
Diabetes mellitus 1.46 (1.34-1.58) 1.16 (1.05-1.27)
Hypertension 1.52 (1.40-1.65) 1.02 (0.93-1.13)
Cerebrovascular disease 1.92 (1.78-2.07) 1.43 (1.31-1.56)
Dementia 2.52 (2.21-2.88) 1.57 (1.35-1.81)
Parkinson’s disease 2.36 (2.02-2.76) 1.49 (1.26-1.77)
Depression 1.70 (1.46-1.95) 1.19 (1.02-1.39)
Chronic kidney disease 1.80 (1.54-2.10) 1.51 (1.28-1.77)
Osteoporosis 2.31 (2.06-2.59) 1.65 (1.46-1.87)
Osteoarthrosis of lower limb 1.30 (1.18-1.43) 0.95 (0.86-1.05)
Alcoholism 2.43 (1.39-4.24) 2.51 (1.40-4.47)
†Adjusted for sex, age, urbanization level, diabetes mellitus, hypertension,
cerebrovascular disease, dementia, Parkinson's disease, depression, chronic kidney disease, osteoporosis, osteoarthrosis of lower limb and alcoholism
*1 indicated the highest level of urbanization and 4 the lowest (from reference 9)
Table 2. Interaction between alcoholism and number of medications associated with falls
No alcoholism Alcoholism
OR (95% CI) OR (95% CI)
Number of medications
0-1 1.00 (reference) 3.01 (0.57-15.9)
2-4 1.15 (1.01-1.32) 5.32 (1.58-18.0)
≥ 5 1.27 (1.10-1.47) 6.29 (2.22-17.8)
Adjusted for sex, age, urbanization level, diabetes mellitus, hypertension,
cerebrovascular disease, dementia, Parkinson’s disease, depression, chronic kidney disease, osteoporosis, and osteoarthrosis of lower limb