國立台灣大學電機資訊學院電機工程學研究所 博士論文
Graduate Institute of Electrical Engineering
College of Electrical Engineering and Computer Science National Taiwan University
Doctoral Dissertation
穴蝕效應及輻射力在超音波血栓溶解及藥物傳輸所扮 演的角色
Roles of Cavitation and Radiation Force in Sono- thrombolysis and Drug Delivery
莊岳勳
Yueh-Hsun Chuang 指導教授: 李百祺 博士 Advisor: Pai-Chi Li, Ph.D.
中華民國 102 年 7 月 July 2013
1
Table of Contents:
Astract………..………4
中文摘要………....5
Chapter 1 Introduction……….………...6
Chapter 2 Effects of Ultrasound-Induced Inertial Cavitation on En- zymatic Thrombolysis……….………...…...…….15
2.1 Introduction………..………...……...…….15 2.2 Materials and Methods………...……….17
2.2.1 Blood Clot Preparation and Examination 2.2.2 Preparation of Microbubbles
2.2.3 Ultrasound Thrombolysis System 2.2.4 Experimental Design
2.2.5 Statistics
2.3 Results………..……...………21 2.4 Discussion………...………..26 2.5 Conclusions………..…...……....28
Chapter 3 Combining Radiation Forces with Cavitation for En- hanced Sonothrombolysis……….………..….……..30
3.1 Introduction………...………...……..…….30
2
3.2 Materials and Methods………...…..…..…….32 3.2.1 Blood Clot Preparation and Examination
3.2.2 Microbubble Preparation 3.2.3 Flow Cytometry Examination 3.2.4 Ultrasound System
3.2.5 Radiation Force Setting 3.2.6 Experimental Design 3.2.7 Statistics
3.3 Results……….………...…….36 3.4 Discussion………...…...…...……43 3.5 Conclusions………..…...…..…….45
Chapter 4 Albumin Acts Like TGF-β1 in Microbubble-Based Drug Delivery………...……46
4.1 Introduction…..………..…...…..……46 4.2 Materials and Methods…...………...………...50
4.2.1 Microbubble Preparation 4.2.2 Cell Preparation
4.2.3 Ultrasound System
4.2.4 Flow Cytometry Examination 4.2.5 Study Protocol
4.2.6 Statistics
4.3 Results………..……...………...…….54 4.4 Discussion………...………...……….59 4.5 Conclusions………...………...……….………….….62
3
Chapter 5 Discussion, Conclusions & Future Works………..64
5.1 Discussion………..….64
5.2 Conclusions………...…..66
5.3 Future Works………...…..66
References……….. Page 67
List of Figures………..………. Page 88
4
Abstract
Acoustic cavitation has been studied in application of thrombolysis. Radiation force induces gaps between endothelium and enhances the delivery of therapeutic substances. First, we evaluated the effects of cavitation, microbubbles (MBs), and streptokinase on thrombolysis. We found that temperature rise cannot fully explained enzymatic sonothrombolysis and the differential inertial cavitation dose is a good in- dicator. Second, we examined the efficacy of using radiation forces to localize and enhance the targeting of MBs in cavitation-induced sonothrombolysis. Our observa- tions confirm that radiation forces help MBs to distribute into a clot (as does cavita- tion). Combining radiation forces with cavitation would provide additional thrombo- lysis effects relative to cavitation alone. A local delivery method based on radiation forces has the potential to improve the safety and efficacy of sonothrombolysis. Third, we hypothesized that albumin MBs can be used for drug delivery to breast cancer cells without antibody conjugation for specific targeting. We also studied the possible roles of TGF-β1 and a radiation force in the behavior of cells and albumin MBs. The results show that albumin MBs can enter breast cancer cells and remain therein for at least 24 hours, even in the presence of paclitaxel loading. Applying radiation force further increased the percentage. This process could be blocked by TGF-β1, even with subsequent exposure to the radiation force. From these results we conclude that TGF-β1 receptors are involved in endocytosis of albumin MBs entering breast cancer cells. The albumin MBs without antibody conjugation can be a useful method of drug delivery. The entire study we presented here demonstrates that radiation force and cavitation play different roles and are important in thrombolysis and drug delivery.
5
中文摘要
超音波穴蝕效應已經有很多研究嘗試運用在血栓溶解上,超音波輻射力可以 使血管內皮細胞間隙變寬,及促進治療物質的傳送。首先,我們評估了結合穴蝕 效應、微氣泡及鏈激酶對於血栓溶解的效應。我們發現溫度上升不能完全解釋酵 素引發的血栓溶解效應,以及差異性惰性穴蝕效應劑量可以是一個有效的血栓溶 解指標。第二部分則是對於穴蝕效應引發的血栓溶解效應,我們檢視了利用施加 超音波輻射力對於聚集及標定微氣泡所產生的效果。我們的觀察也確定了輻射力 可以幫助微氣泡分布到血栓內部,穴蝕效應也同樣可以。結合輻射力及穴蝕效應 相對應於單純施加穴蝕效應,可以提供額外的血栓溶解效果。超音波輻射力所提 供的局部傳遞效果,有潛力可以用來提高超音波血栓溶解的安全性及效果。第三 部分我們假設了白蛋白微氣泡在不使用抗體作為專一性標定的情況下,可以針對 乳癌細胞進行藥物傳送。我們同時也研究了超音波輻射力以及轉化生長因子 TGF-β1,對於白蛋白微氣泡跟細胞之間互動的可能扮演角色。結果顯示白蛋白 微氣泡可以進入乳癌細胞而且存活超過 24 小時,即使氣泡帶有太平洋紫杉醇藥 物也可以。施加輻射力更可以增加這個現象的百分比。然而這個現象可以被轉化 生長因子 TGF-β1 阻斷,即使後續施加輻射力也是如此。由此我們得到的結論是 轉化生長因子 TGF-β1 的接受器應該有參與白蛋白微氣泡進入乳癌細胞的細胞吞 噬作用。另外,白蛋白微氣泡在沒有抗體接合來輔助標定的情況下,依然可以是 一個傳遞藥物的有效方法。整體來說,我們在此呈現的研究,主要展現了超音波 輻射力及穴蝕效應對於血栓溶解及藥物傳遞上,扮演了不同且重要的角色。
Chapter 1
6
Introduction
Ultrasound (US) imaging has been used clinically as an effective diagnostic tool since the 1960s [1-3]. It is a noninvasive medical examination that helps physicians diagnose and treat medical conditions. The advantages include real time imaging, non-invasive or minimally invasive, bedside availability, relatively cheaper than computed tomography and magnetic resonance imaging, and no radiation. However, there are some limitations in applications about medical ultrasound. First, the opera- tion of ultrasound depends on operator’s skill and experiences. Second, the display window and penetration depth are limited. Third, organs that contain air or bone are poorly visualized. Ultrasound can also be a way of treatment. Local heating by ultra- sound for physical therapy, extracorporeal shock wave lithotripsy, and high intensity focused ultrasound are wellknown examples. Extensive work has been done in the past showing harmful biological responses of cells and tissues to ultrasound exposure including growth suppression, retarded protein synthesis, cytoplasmic vacuolation and disruption of intracellular components such as mitochondria, microtubules and endo- plasmic reticulum [4]. Ultrasonic bioeffects can result from thermal and non-thermal mechanisms [3,5]. Both mechanisms are important and either may predominate, de- pending on the exposure conditions [6]. The thermal mechanism associated with the absorption of acoustic energy by the body and the generation of heat is reasonably well understood [7]. Non-thermal mechanisms are typically insignificant, unless a phenomenon known as cavitation occurs [8-12].
In recent years, lots of attention in research has been paid in acoustic cavitation.
This can be described briefly as the growth and oscillation of MBs in response to a driving acoustic field. If the acoustic and medium conditions are conducive, the MBs
7
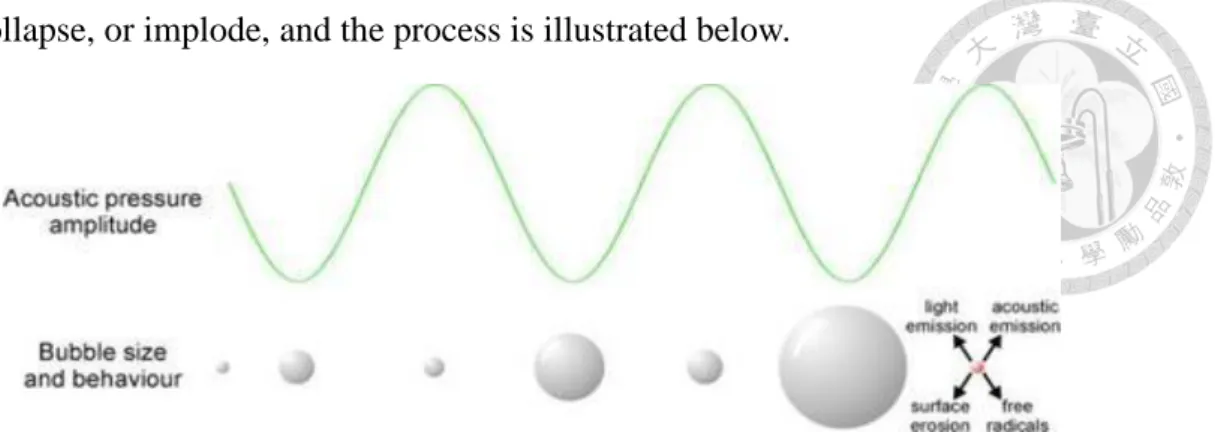
can collapse, or implode, and the process is illustrated below.
Figure 1. Bubble behavior under acoustic exposure.
A bubble initially at rest can grow during the rarefaction half-cycles of an ap- plied acoustic field. Through rectified diffusion, gas and vapor are transported into the bubble, until it reaches a critical size and collapses. The bubble contents are com- pressed rapidly, resulting in extreme local conditions. Extreme conditions occur at the collapse phase, perhaps with temperatures up to 5000 °K and pressures of 1000 at- mospheres. The cavitation process is more efficient with the presence in the liquid of small pockets of gas trapped in conical pits of solid impurities or covered with an or- ganic or surface-active molecule, the so called nuclei. The gas inside bubbles provides another way of contrast relative to that of tissues in ultrasonography. As the quantity of nuclei in the liquid increases, lower energy is needed for cavitation inception. Bub- bles can be either injected in some fluids or formed spontaneously due to the action of a pertinent source. For instance, there exist reports that sufficiently high amplitude ultrasound pulses cavitate the nucleation agents present in blood [13-15].
Until now, different kinds of MBs were developed and studied for their charac- teristics and applications. Contrast MBs are usually stabilized against dissolution and coalescence by the presence of additional materials at the gas-liquid interface [16-18].
In some cases, this material is an elastic solid shell that enhances stability by support-
8
ing a strain to counter the effect of surface tension. Shell materials like albumin and polymer are examples to meet this purpose. In other cases, this material is one or a combination of two or more surfactants, which promote stability by greatly reducing the surface tension at the interface. Lipid composition significantly impacted the acoustic dissolution rate, fragmentation propensity, and mechanism of excess lipid shedding [19]. Currently, some perfluorochemicals (PFCs) are being used as MB fill- ing gases due to their low solubility in blood and high saturation vapor pressure. The amount of PFCs is controlled to impart sufficient vapor pressure to counter the sum of the Laplace pressure (surface tension) and arterial blood pressure. Both the constrain- ing surface materials and insoluble filling gas of a contrast microbubble inhibit it to a certain degree from undergoing a swift expansion and, subsequently, a violent col- lapse that may occur to a free microbubble [17]. It is well-known that intense US causes the disappearance of contrast MBs [20-22], but the exact mechanism of de- struction is only partially understood and little is known regarding the relationship between cavitation bioeffects and microbubble destruction. MBs like Albunex and Optison (Molecular Biosystems, Inc., San Diego, CA) consist of gas (air and PFCs, respectively) MBs encapsulated within a shell of human serum albumin. However, each contrast agent exhibits different responses to ultrasound pulses because of the unique properties of the MB surface materials and filling gases. Acoustic pressures causing MB destruction for one agent are usually not necessarily the same for another agent. This implies that the conditions for the safe use of one agent may lead to poten- tially hazardous bioeffects if the same conditions are applied to another agent. There- fore, it is imperative to identify the conditions for the safe use of each new contrast agent.
Acoustic cavitation has been studied by many investigators interested in US bio-
9
effects. In its 1983 report [23], the National Council on Radiation Protection and Measurements identified both stable cavitation processes such as bubbled-associated microstreaming [24] and inertial cavitation processes, such as free radical generation and microjetting, as possible mechanisms of action. In stable cavitation, the radial pulsations of MBs driven by the US field are controlled by the stiffness of the gas in the bubbles. Microstreaming around the bubbles could cause damage to nearby cells or fibers, or act to stir fresh fibrinolytic enzyme into otherwise inaccessible regions in a clot. In inertial cavitation, the radial motion of a bubble is controlled by the inertia of the rapidly moving liquid surrounding it. For symmetrical collapse, hot spots can form that can produce hydroxyl free radicals [25] capable of attacking nearby fibers.
For asymmetrical collapse, microjets may form that can damage nearby fibers in the manner of pitting on ships’ propellers. In all cases, US-driven bubbles might exterior- ize new binding sites along fibers to allow fibrinolytic enzymes increased access.
MBs also had been applied to different kinds of application in recent years. Ex- amples are gene or drug delivery, contrast agent in blood stream, and molecular im- aging. MBs have been used in combination with ultrasound to improve the gene transfection and drug delivery efficiency. An in vitro study showed that, in inertial cavitation, the violent expansion, contraction and collapse of gas bubbles was related to hemolysis [26] and that the dose of inertial cavitation can be evaluated by measur- ing the power emitted during the cavitation process. Quantification methods for acoustic cavitation have been investigated by many researchers [26-29]. One method is to calculate the spectral broadband signal enhancement during MB destruction, since spectral spikes may appear at up to 30 to 40 MHz when MBs are destroyed [30].
Ultrasonic cavitation is thought to assist the delivery of molecules into a cell by tran- siently increasing the membrane permeability (also known as sonoporation) [31-36].
10
Thrombolytic therapy using enzymes plays an important role in cardiovascular disease, stroke, peripheral vessel diseases, and dialysis graft occlusion. However, there remain significant limitations of thrombolytic therapy, including speed of clot dissolution, resistance of some thrombi to fibrinolysis, and the occurrence of bleeding complications. Therapeutic use of ultrasound contrast agents is an emerging technique with potential in the areas of thrombolysis (clot dissolution), drug delivery and gene therapy [37]. The use of ultrasound in all these applications is desirable because it al- lows the non-invasive treatment of deep lesions (such as tumors and thrombi) with little or no effect on overlying tissues or organs. In the area of sonothrombolysis, a considerable amount of research has been directed towards the detection and treat- ment of blood clot (thrombus) associated with nonhemorrhagic stroke, myocardial infarction, deep vein thrombosis, and peripheral artery thrombosis [37-39]. It has been 30 years since thrombus dissolution with ultrasound was first reported [40]. However, the dissolution mechanisms still are not well understood. There are many influential factors for sonothrombolysis, including (but not limited to) clot morphology and age, physical and chemical environment, microbubble technology (if a contrast agent is involved), and therapeutic ultrasound dosage. Everbach and Francis (2000) demon- strated an increase in thrombolysis due to cavitation effects, but also suggested the possibility of other unknown mechanisms [41]. Cavitation is generally classified into two types, stable cavitation, which results in emissions at subharmonics of the main excitation frequency and inertial cavitation, which is characterized by broadband noise emissions [42]. Stable cavitation can induce bubble-associated micro-streaming and shear stress, while inertial cavitation can even cause micro-jetting and pitting on solid surfaces [42]. Datta and colleagues (2006) investigated stable and inertial cavi- tation as possible mechanisms for enhancing thrombolysis with a lytic drug t-PA. In
11
most of their experiments conducted above the stable cavitation but below the inertial cavitation threshold, cavitation was present almost throughout the entire exposure du- ration. In the ultrasound exposure condition above the inertial cavitation threshold, the inertial cavitation activity was sporadic and was often preceded or followed by stable cavitation activity. Therefore, sustaining stable cavitation for a longer period of time appears to be more effective in the thrombolysis enhancement than inertial cavitation [42]. Prokop and co-workers (2007) also studied the role of both inertial and stable cavitation during ultrasound-accelerated enzymatic fibrinolysis (with t-PA) in vitro in the presence and absence of Optison contrast MBs [43]. The addition of MBs signifi- cantly increased lysis. Inertial cavitation was present only at the start of the ultrasound exposure, while stable cavitation with low-amplitude subharmonic emissions persist- ed throughout. Their study indicated a potentially important role of stable rather than inertial cavitation in microbubble-enhanced sonothrombolysis. Even without the presence of any thrombolytic drug, the use of ultrasound contrast agents has been shown to increase the effectiveness of sonothrombolysis. Xie and colleagues (2005) investigated microbubble-mediated sonothrombolysis using a canine thrombus model that consists of a dialysis graft connecting femoral artery and vein [44]. In the graft occluded by thrombus, therapeutic ultrasound was applied during an intravenous infu- sion of MRX-815 MBs (ImaRx). Restoration of rapid flow (as an indicator of suc- cessful treatment) within the graft was seen.
This is particularly important in the form of inertial cavitation, which is the vio- lent collapse of bubbles leading to very high localized increases in temperature and stress. Inertial cavitation generally requires a high ultrasound pressure (≥1.0 MPa) to activate the cavitation nuclei that are present in the medium. The nuclei may be sub- microscopic gas bodies or MBs that are usually much smaller than bubbles that would
12
be resonant at biomedical ultrasound frequencies [8]. The emerging diagnostic use of ultrasound contrast agents may change a relatively poorly gas nucleated environment in the human body to a richly nucleated medium. Thus, the risk of biological damage may increase due to cavitation effects associated with microbubble contrast agents [45,46]. The concern regarding ultrasonic bioeffects has been raised by the observa- tion of contrast-enhanced hemolysis and hemorrhage [28,47-52] both in vitro and in vivo. In vitro studies using human blood showed hemolysis at very high transmitted power levels [48]. Hemolysis in mice [49] and hemorrhage in the liver and kidney of anesthetized mice [50] were found using pulsed ultrasound at intensities utilized clin- ically, although at frequencies lower than those employed in medical imaging. Fortu- nately, no significant bioeffects have so far been found in animal models and humans (during clinical trials) from the use of US contrast agents such as Optison (Molecular Biosystems, Inc., San Diego, CA) at both intensities and frequencies of diagnostic US [51,53]. There is a paucity of studies on the mechanism of bioeffects associated with contrast MBs used in medical diagnostic US. This is partly owing to the complicated behavior of contrast MBs (when intensely insonified) resulting from their complex composition.
Applying low-intensity acoustic energy has been hypothesized as a way to move freely flowing contrast agents toward the endothelium [54,55]. Acoustic radiation forces (also known as Bjerknes forces) consist of two components: (1) a primary force directed away from the acoustic source in the direction of wave propagation and (2) a secondary attractive force that acts between individual bubbles. Dayton and col- leagues verified that the primary radiation forces were able to displace nontargeted contrast agent away from the vessel center in a flow chamber [55,56] and in the mouse microcirculation [22]. The use of acoustic radiation forces has also been sug-
13
gested for enhancing the delivery of therapeutic substances [57,58]. Radia- tion-force-induced displacements may cause shear forces between displaced and non-displaced tissue, and the resulting strain may induce gaps between endothelial cells [59,60] and widen intercellular spaces in epithelial tissue [61,62]. All of these effects of radiation forces provide promise in targeting MBs onto a clot for sono- thrombolysis. However, the characteristics of the shear forces induced by radiation forces are not yet fully understood in the thrombolysis model. Spengler et al. showed that radiation forces push the bubbles together in the fluid [63], while Sakharov et al.
showed that acoustic streaming enhanced thrombolysis by an amount equivalent to that induced by mild stirring of a thrombolytic solution around the thrombus [64].
Nevertheless, the behavior of MBs inside mediums such as blood clots or tissues ex- posed to radiation forces is not fully understood.
Chemotherapy is one of the most important approaches for treating breast cancer patients. However, chemotherapeutic drugs such as PTX and doxorubicin lack cyto- toxicity selectivity between cancer cells and normal cells, which frequently leads to serious side effects. Also, the poor water solubility of PTX makes it difficult to ad- minister in clinical applications. Drug resistance and limited access of the drug often results in the drug concentration not been sufficiently high to kill malignant cancer cells [65, 66]. Therefore, localized drug delivery looks promising in reducing system- ic toxicity and maximizing tumor exposure [67]. Drug-loaded-MBs destruction in combination with ultrasound has recently become one of the most promising thera- peutic applications in drug delivery [68], since drug-loaded MBs can be manipulated and destroyed by ultrasound applied at the tumor site, causing localized release of the drug [69-72]. In addition, combining MBs with ultrasound can increase the permea- bility of physiologic barriers such as the blood–brain barrier, capillary endothelium,
14
and the cell membrane for macromolecules or even colloidal particles [73, 74]. Sever- al investigations on the application of ultrasound contrast agents as tumor drug deliv- ery systems have recently been reported. Kang et al. showed an antitumor effect of docetaxel-loaded lipid-shelled MBs combined with ultrasound-targeted MB activation on VX2 rabbit liver tumors [75]. Xing et al. demonstrated the effective treatment of ovarian carcinoma using PTX-loaded ultrasound MBs [76]. Tinkov et al. developed doxorubicin-loaded MBs with ideal physical characteristics and showed that their cy- totoxic activity was enhanced relative to free doxorubicin and doxorubicin-loaded liposomes in in vitro experiments [77]. These studies have shown that shell-stabilized MBs can be used to load drugs or genes and improve the drug therapeutic index of a tumor when combined with ultrasound.
15
Chapter 2
Effects of Ultrasound-Induced Inertial Cavitation on Enzy- matic Thrombolysis
2.1 Introduction
Ultrasound enhances enzymatic fibrinolysis both in vitro and in vivo [78–86].
Two approaches for sonothrombolysis are generally taken. The first approach delivers low-frequency (20–30 kHz) and high-intensity (>10 W/cm2) ultrasound to the throm- bus site via an intravascular transducer. Such an acoustic wave is capable of destroy- ing thrombi and atherosclerotic plaques even without enzymatic thrombolysis. The most likely mechanisms of such destruction include vigorous cavitation (i.e., genera- tion of active bubbles and cavities in the liquid), accompanying microstreaming, and direct mechanical fragmentation of the thrombus by vibration of the ultrasonic trans- ducer tip [87,88]. Although several studies have demonstrated the efficacy of this ap- proach both in animal models and patients using pulsed wave ultrasound [89–91], several problems remain, including potential perforation of vessel wall and emboliza- tion due to the release of large fragments of a thrombus [92,93], and local overheating.
The other approach uses high-frequency (1–3 MHz) and low-intensity (0.5–5 W/cm2) ultrasound. Such excitation can also be used for imaging and for destroying thrombi directly, but it can also enhance enzymatic fibrinolysis [79, 81, 82, 84, 86, 87, 94].
This approach is of particular interest because it can be applied noninvasively and transcutaneously. Nonetheless, the main concern of using high-frequency ultrasound is potential heating of the surrounding tissue, since heat production is proportional to
16
the ultrasound frequency.
Mechanisms underlying the enhancement of enzymatic fibrinolysis by ultrasound remain to be delineated, particularly because such enhancement could occur in clini- cal applications of ultrasound. Several mechanisms have been proposed for ultrasound in the kilohertz frequency range. Some studies have hypothesized that non-thermal mechanisms enhance the transport of fibrinolytic enzymes into the clot [95–97].
Suchkova et al. proposed that mechanical processes unrelated to cavitation could also be involved [98]. Sakharov et al. attributed the increase in lysis rate induced by 1 MHz ultrasound to an increase in enzymatic action due to a temperature increase, but concluded that this temperature rise constitutes a minor part of the enhancement effect of ultrasound [99]. They also concluded that ultrasound can produce acoustic stream- ing, which is effectively equivalent to mild stirring. Pieters et al. attributed the in- crease in thrombolysis when using 40-kHz ultrasound to an increase in penetration of the thrombolytic agent into the clot [100]. Their results were based on a clot model, and suggested the presence of multiple mechanisms resulting in the increased transport of thrombolytic agent into the clot. Nevertheless, the mechanism underlying the transportation of the thrombolytic agent into the clot remains unclear.
Enzymatic thrombolysis might also be attributable to cavitation effects. Cavita- tion is generally classified into two types: stable and inertial. Stable cavitation results in the emission of subharmonics of the main excitation frequency and induces bub- ble-associated microstreaming [24], whereas inertial cavitation emits broadband noise and induces microjetting and pitting on solid surfaces [101, 102]. Everbach and Fran- cis demonstrated that cavitation increases thrombolysis, but they were unable to dis- tinguish between stable and inertial cavitation [41]. Some investigators have clearly shown that ultrasound accelerates enzymatic fibrinolysis by increasing the transport of
17
reactants via cavitation-related mechanisms [79,82,103]. Koch et al. provided evi- dence that ultrasound-assisted drug uptake is due to cavitation [103]. The results of these previous studies indicate that the respective roles of stable and inertial cavitation need to be further examined.
The optimal condition of ultrasound-assisted enzymatic thrombolysis still needs to be determined. High-frequency ultrasound is more promising for avoiding emboli- zation and perforation of vessel wall during sonothrombolysis due to the ability to focus at depth. Our previous study of the use of sonoporation to deliver DNA into cells suggested that inertial cavitation plays a role in thrombolysis [104]. Thus, the main purpose of the present study was to elucidate the effects of individual acoustic parameters (amplitude and duration) as well as the microbubble concentration on the reduction in the weight of a blood clot. The combined effects when also using throm- bolytic enzyme were also evaluated. This study was also motivated by the possibility of using the measured cavitation effects for sonothrombolysis to take the place of weight measurement in vivo.
2.2 Materials and Methods
2.2.1 Blood Clot Preparation and Examination
After obtaining our ethics committee’s approval and informed consent from vol- unteer, fresh human blood was drawn and divided into 0.2-ml Eppendorf tubes (Sci- entific Specialties, Lodi, CA, USA). Each tube contained 100 μl of blood and 10 μl of 0.5 M calcium chloride (Sigma-Aldrich, St. Louis, MO, USA). All samples were kept at 25C for 24 hours to ensure complete solidification and consistency of the blood clots. The blood clots were weighed before and after each ultrasound treatment to de-
18
termine the induced weight reduction. Before weighing, the clot was removed from the Eppendorf tube and placed on a paper towel to remove the superfluous liquid.
After experiments, the blood clots were fixed with formaldehyde, embedded with paraffin, sliced, and stained for microscopy examinations (CKX41, Olympus, Japan) and photography. The blood clots of the same group were placed on a single slide.
2.2.2 Preparation of MBs
We used two types of MBs in our experiments: (1) phospholipid-shelled MBs (SonoVue, Bracco, Amsterdam, Netherlands) and (2) albumin MBs made using our in-house protocols [106]. The concentration of the SonoVue MBs was about 1–5108 /ml (5 mg/ml).
After mixing human albumin (Octapharma, Lachen, Switzerland) with normal saline into a 3% solution, it was ventilated with perfluoropropane and sonicated for 2 min, then incubated on ice for 5 min. The concentration of the MBs was more than 8109 /ml, their diameters were 1.0–4.0 μm with a mean of 1.9 μm (Multisizer 3, Beckman Coulter, Fullerton, CA, USA), and their half-life was more than 3 hours.
The MBs were diluted to the desired concentration just before experiments.
2.2.3 Ultrasound Thrombolysis System
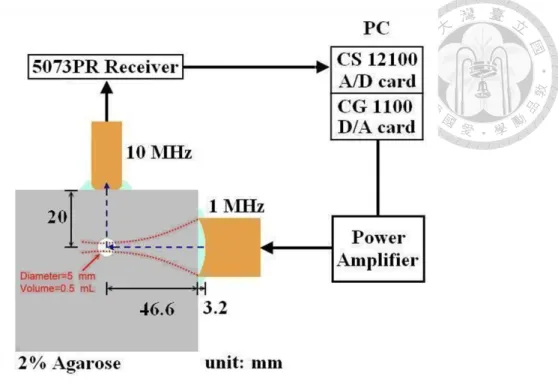
The setup for acoustic measurements (Fig. 2) allowed measurements of the iner- tial cavitation dose (ICD), which was proved as an effective tool for detecting and an- alyzing inertial cavitation [105].
19
Fig. 2. Setup for acoustic cavitation measurements.
A 10 MHz transducer was used to detect the broadband signal enhancement and to avoid harmonics of the 1 MHz transmitted signals. The incident amplitude of the harmonic at 10 MHz and the received subharmonic signal at 0.5 MHz were minimal.
The received signal was then quantified as the root-mean-square (RMS) value in the time domain between 9.5 and 10.5 MHz and integration over time. Finally, the back- ground time-amplitude curve (the measured RMS amplitude from water only) was subtracted and the resulting amplitude is referred to as the differential ICD that was used for subsequent signal analysis. In our model system, a 1.0 MHz focused trans- ducer (V302, Panametrics-NDT, Waltham, MA, USA) with a diameter of 25.4 mm and a focal length of 49.8 mm was used for transmission. The beam width and depth of field of the transducer were 6.0 mm and 55.0 mm, respectively. The transmitted waveforms were generated by a digital-to-analog converter (CompuGen 1100, GaGe Applied Technologies, Lachine, QC, Canada) and amplified by a power amplifier
20
(250A250A, Amplifier Research, Souderton, PA, USA). The pulsed waves used in this study had a repetition frequency of 100-Hz, which means several cycles of 1 MHz waves followed by a rest of 10 milliseconds. The acoustic signals were detected by an unfocused 10 MHz transducer (V312, Panametrics-NDT), sent to a receiver (5073PR, Panametrics-NDT), digitalized by an analog-to-digital converter (Com- puScope 12100, GaGe Applied Technologies), and analyzed using MATLAB (Math- Works, Natick, MA, USA). A 2% agarose phantom was made with a cylindrical cavity (5 mm in diameter and 25 mm deep) to contain the blood clot. The 1 MHz transducer was positioned with the -6-dB focal zone covered the entire cavity, as shown in fig- ure 2, while the unfocused 10 MHz transducer with a diameter of 6.4 mm was placed at 20 mm from the cavity. The overall ultrasound exposure duration was 1.5 second.
2.2.4 Experimental Design
We first evaluated the individual effects of the acoustic amplitude (by varying the driving voltage to the transducer), pulse duration (by varying the number of cycles of the transmit waveform), and microbubble concentration (by SonoVue) on throm- bolysis. Each measurement in different concentrations, cycle numbers and voltage settings were repeated five times to reduce human and system errors. The effects of MBs on thrombolysis were investigated at concentrations of 0 (as control), 0.25, and 0.5 mg/ml with a fixed driving voltage of 5 volts and a pulse duration of 10 cycles.
The effects of driving voltages of 0 (as control), 1, 2, and 5 volts were compared with a fixed microbubble concentration of 0.5 mg/ml and a pulse duration of 10 cycles.
The acoustic pressures produced with driving voltages of 1, 2, 5 volts were 0.52, 0.94, 1.30 MPa, respectively. Finally, pulse durations of 1 (as control), 2, 5, and 10 cycles were examined with a fixed driving voltage of 5 volts and a microbubble concentra-
21
tion of 0.5 mg/ml. The duty cycle for 10 cycle pulses, for example, equals to 0.1%.
We then compared the respective effects of ultrasound, MBs (albumin-shelled, in house), and streptokinase on thrombolysis relative to the results for the above experi- ments. The blood clot without being exposed to any of these effects was used as con- trol. On the other hand, the experimental groups include ultrasound, ultrasound with MBs, streptokinase, and ultrasound with MBs after streptokinase exposure. The measurements were repeated eight times in control and each experimental groups to reduce human and system errors. Streptokinase (Sigma-Aldrich, St. Louis, MO, USA) was introduced into the Eppendorf contained blood clot to produce a final concentra- tion of 1000 U/ml for 30 min at 25C. Then the blood clot was taken out and placed into phantom cavity for subsequent ultrasound and microbubble applications. The differential ICD (dICD) was calculated as the difference in ICD between the experi- mental and control groups. The ICD values of all control groups were checked and found equal to the ICD value of water.
2.2.5 Statistics
The obtained results are given here as mean and standard deviation values and compared using the Wilcoxon-Mann-Whitney test. A probability value of P < 0.05 was considered statistically significant.
2.3 Results
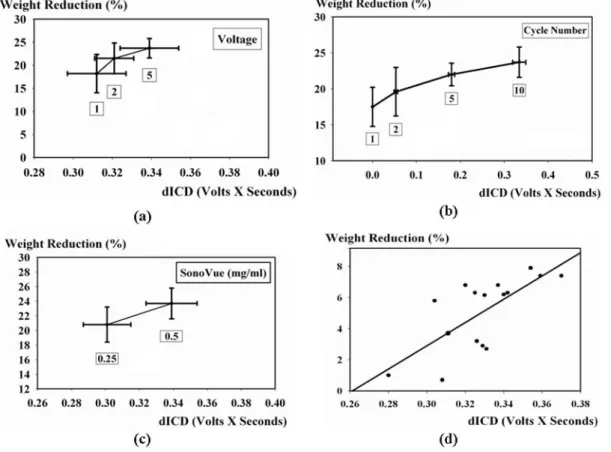
Figure 3 shows the relationships between clot weight reduction and dICD for different pulse durations, driving voltages, and microbubble concentrations. The weight reduction percentages and ICD values of all the control groups were set as ze-
22
ro in figure 3. Figure 3a shows that the weight reduction of a blood clot and the cavi- tation effect as evaluated by dICD increased approximately monotonically with the driving voltage. Lower voltages produced negligible effects since inertial cavitation did not occur. Figure 3b shows that the weight reduction of a blood clot and the dICD increased with the pulse duration. Figure 3c shows that the weight reduction of a blood clot and dICD increased monotonically with the microbubble concentration.
Higher concentrations were tested and found that the thrombolysis effects were re- duced. This can be explained by the increased shielding effect of MBs. A scatter plot with the linear regression of clot weight reduction versus dICD from the data in fig- ures 3a to 3c is shown in figure 3d, for which the correlation coefficient was 0.66.
Fig. 3. Relationships between dICD and clot weight reduction for different cavitation parameters: (a)
driving voltage, (b) pulse duration, and (c) microbubble concentration. (d) Linear regression of the ex-
perimental data.
23
Figure 4a shows the effects of ultrasound, MBs, and streptokinase on thrombo- lysis. The figure shows that the effects of sonothrombolysis can be greatly enhanced by combining ultrasound, MBs, and streptokinase. The weight of a blood clot was re- duced by about 50% in experiments. In contrast, the ICD values in sonothrombolysis, and shows that adding streptokinase to microbubble-induced inertial cavitation had no significant effect (P<0.01) on the ICD value (Fig. 4b). By comparing figures 3a, 3b, and 4a, we found that these two types of MBs exerted similar effects on sonothrom- bolysis (by weight reduction and ICD evaluation) for the experimental parameters we used.
Fig. 4. Individual effects of ultrasound, MBs, and streptokinase on thrombolysis as evaluated by clot
weight reduction (a) and ICD (b). Data are mean and standard deviation values.
Figures 5 and 6 are microscopy images of blood clots at two magnifications, and show that the blood clot of the control group (Fig. 5a) had an intact smooth surface, with higher magnification (Fig. 6a) revealing an intact red blood cell and clot struc- ture. Since whole blood was used in the experiment, the blood clot consisted of hya- line and red parts (mainly red blood cells). Blood clot exposed to ultrasound alone
24
(Figures 5b and 6b) show intact red blood cells that have separated from the surface or loosened within a certain depth of the blood clot on the exposure side. Exposure to ultrasound and MBs (Fig. 5c) produced a rough and porous surface (about 25 μm in depth) on the blood clot. Damaged red blood cells were evident around the surface (Fig. 6c, arrowhead). Blood clots exposed to streptokinase showed significant shrink- age in global size and disappearance of fibrin clots (the hyaline part) in observation.
Figures 5d and 6d showed the irregular surface of the clot created by Streptokinase, while remaining the red blood cells intact. Figure 5e shows a clot exposed to ultra- sound, MBs, and thrombolytic enzyme simultaneously. Several large cavities with av- erage depth of about 200 μm can be seen within the clot and distributed on the ex- posed side in every clot slice. Some cavities were close to the surface (indicated by arrowheads in the figure), while others were deep inside the clot. The side of the clot opposite to the side of ultrasound exposure looked the same as that in the streptoki- nase group (Fig. 5d), without the presence of cavities. Also, damaged red blood cells were readily identifiable in this experimental group (Fig. 6e, arrowheads). Comparing Figures 5e and d, it is possible that streptokinase not only induced lysis on the surface, but also penetrated into the blood clot and subsequently helped to enlarge the cavities.
25
Fig. 5. Microscopy images of blood clots for control (a), ultrasound (b), combined ultrasound and MBs
(c), streptokinase (d), and combined ultrasound, MBs, and streptokinase (e). Arrowheads indicate the
inlets of cavities. Rectangles indicate the area magnified in Fig. 6.
26
Fig. 6. Microscopy images of blood clots (at higher magnification) for control (a), ultrasound (b), com-
bined ultrasound and MBs (c), streptokinase (d), and combined ultrasound, MBs, and streptokinase (e).
Arrowheads indicate damaged red blood cells.
2.4 Discussion
Combining ultrasound, MBs, and thrombolytic agent appears to be a promising method for sonothrombolysis. Cavitation (especially inertial cavitation) probably un- derlies ultrasound-enhanced thrombolysis. The ICD we previously proposed was
27
proved to be a useful indicator of thrombolysis in this study [81]. In addition to the present investigation of inertial cavitation, future studies of stable cavitation would help further the understanding of the mechanisms underlying enzymatic sonothrom- bolysis.
Sakharov et al. attributed the increase in lysis rate induced by 1-MHz ultrasound to an increase in enzymatic action due to a 6C temperature rise, but concluded that this temperature rise constituted a minor part of the enhancing effect of ultrasound [64]. Our experimental results are consistent with this conclusion. Ultrasound was ap- plied in our experiments for 1.5 seconds after the blood clot had been soaked in streptokinase for 30 min. The temperature might increase, but the ultrasound duration is too short for this factor alone to produce the significant changes shown in figure 5e (relative to figure 5d). Sakharov et al. also concluded that the effect of ultrasound is equivalent to mild stirring, possibly caused by acoustic streaming. Our results indicate that inertial cavitation played a major role in producing cavities (Fig. 5e, arrowheads), with microjetting creating pitting on the surface, subsequent carving by MBs, and their size being increased by enzymes. Another notable feature was the damage to red blood cells. Since MBs and red blood cells are similar in size (1–2 versus 7 µm, on average), inertial cavitation can also happen on the surface of blood cells. The pres- ence of fragments of red blood cells in figure 6e supports this hypothesis. Applying acoustic cavitation alone without enzyme, as in figure 5c, also elicited microjetting on red blood cells. Further evidence of inertial cavitation was microbubble debris coming up to the solution surface within about 5 seconds after ultrasound exposure, with the solution becoming clear at the same time; without ultrasound irradiation, the solution remained cloudy. This indicates that MBs ruptured soon after being exposed to ultra- sound and produced inertial cavitation, as demonstrated by Prokop et al. The residual
28
microbubble concentration was believed to be too low for stable cavitation to play a major role in our experiments [43].
The microscopic differences between streptokinase alone (Fig. 5d) and combined ultrasound, MBs, and streptokinase (Fig. 5e) indicate that the enzyme already infil- trated into the clot during the 30 min of deposition. The thrombolytic enzyme strepto- kinase digested the fibrin clot macroscopically and possibly loosened connections among red blood cells within the clot by diffusion. The further application of ultra- sound and MBs readily enlarged the cavities (compared to figure 5c and 5e) by iner- tial cavitation. The role of enzyme is relatively limited during the 1.5 second exposure of cavitation. Francis et al.suggested the mechanical forces associated with ultrasonic radiation might push MBs and enzyme to penetrate the surface layer of red blood cells in their study [103]. The relatively short duration of ultrasonic radiation in our study makes the penetration of MBs and enzyme less significant. From these observations we can conclude that transport of fibrinolytic enzyme into clots significantly affects the rate of fibrinolysis.
Stable cavitation has been shown to play an important role in sonothrombolysis [42,64]. The acoustic pressure used in the present study (1.30 MPa) falls within the range that induces inertial cavitation. Stable cavitation was expected to exert relative- ly insignificant effects in our model. These observations suggest that the type of cavi- tation and its relative contributions on thrombolysis vary with the acoustic pressure and model system. However, our study further indicates the importance of cavitation effects in enzymatic thrombolysis. Future studies should investigate the mechanisms of cavitation in thrombolysis, particularly stable cavitation.
2.5 Conclusions
29
This study has demonstrated the effects of acoustic inertial cavitation in sonothrom- bolysis. The transportation of fibrinolytic enzyme into clots significantly affects the rate of fibrinolysis. Moreover, the ICD is potentially a useful tool for sonothrombo- lysis evaluation, since weight reduction measurement of thrombus is not applicable clinically. Nonetheless, the relative contributions in enzymatic thrombolysis by dif- ferent types of cavitation were still undetermined and require further studies for better understanding.
30
Chapter 3
Combining Radiation Forces with Cavitation for Enhanced Sonothrombolysis
3.1 Introduction
The presence of thrombi or emboli within blood vessels can lead to various clin- ical diseases, including myocardial infarction, peripheral artery disease, deep vein thrombosis, and acute ischemic stroke. Such diseases remain the leading causes of death in many developed countries. Ultrasound has been used for several decades to promote clot breakdown as both a stand-alone treatment and in combination with thrombolytic agents, and more recently in combination with ultrasound contrast agents, both in vitro and in vivo [79,86,107-115]. However, the specific mechanisms have yet to be elucidated, and its safety and efficacy remain to be optimized.
Cavitation is one of the possible mechanisms underlying sonothrombolysis. Re- cent data suggest that stable cavitation is more effective than inertial cavitation for clot lysis [42]. The disadvantages of cavitation-induced sonothrombolysis include damage to the endothelium, perforation of the vessel wall, and platelet activation. It is possible that such problems can be alleviated by making the exposure area smaller using targeted MBs or the “push effect” provided by acoustic radiation forces.In mo- lecular imaging studies, MBs are tagged with an adhesion ligand that binds to molec- ular markers expressed on a diseased endothelium, which retains the contrast agent preferentially at sites exhibiting characteristics such as inflammation, angiogenesis, or thrombus [116–120]. However, the microvascular rheology of several nontargeted
31
microbubble preparations has been shown to be very similar to that of erythrocytes [121–123], and microscopy observations have confirmed that MBs tend to distribute toward the axis of the vessel [124], with only few exceptions [125–127]. Thus, the frequent absence of contrast agent contacting the target surface may be a significant impediment to applications.
Applying low-intensity acoustic energy has been hypothesized as a way to move flowing contrast agents toward the endothelium and named radiation force [54,55].
Acoustic radiation forces (also known as Bjerknes forces) consist of two components:
(1) a primary force directed away from the acoustic source in the direction of wave propagation and (2) a secondary attractive force that acts between individual bubbles.
Dayton and colleagues verified that the primary radiation forces were able to displace nontargeted contrast agent away from the vessel center in a flow chamber [55,56] and in the mouse microcirculation [22]. The use of acoustic radiation forces has also been suggested for enhancing the delivery of therapeutic substances [57,58]. Radia- tion-force-induced displacements may cause shear forces between displaced and non-displaced tissue, and the resulting strain may induce gaps between endothelial cells [59,60] and widen intercellular spaces in epithelial tissue [61,62]. All of these effects of radiation forces provide promise in targeting MBs onto a clot for sono- thrombolysis. However, the characteristics of the shear forces induced by radiation forces are not yet fully understood in the thrombolysis model. Spengler et al. showed that radiation forces push the bubbles together in the fluid [63], while Sakharov et al.
showed that acoustic streaming enhanced thrombolysis by an amount equivalent to that induced by mild stirring of a thrombolytic solution around the thrombus [64].
Nevertheless, the behavior of MBs inside mediums such as blood clots or tissues ex- posed to radiation forces is not fully understood.
32
In this study we examined the ability of acoustic radiation forces to enhance the active targeting of MBs in a cavitation-induced sonothrombolysis model with a flow phantom system. The interaction between MBs and the clot was examined by confo- cal microscopy.
3.2 Materials and Methods
3.2.1 Blood Clot Preparation and Examination
The samples in experiments come from a volunteer after documentation of in- formed consent and institution review board. Freshly drawn human blood was mixed with biotin-NHS (Cayman Chemical, Ann Arbor, MI, USA) (final concentration 0.08%), and 100-μl aliquots added to 200-μl PCR tubes (Scientific Specialties, Lodi, CA, USA). Biotin-NHS binds to proteins on red blood cells (RBC), and makes it pos- sible to trace avidin-albumin MBs in the blood clot after experiments. All samples were kept at 37C in a water bath for 24 hours to ensure that consistent clots were formed. The blood clots were weighed before and after each ultrasound treatment to determine their weight loss.
After ultrasound exposure, the blood clots were fixed with 10% formaldehyde, embedded with paraffin, sliced, fixed on slides, and stained with 0.01% biotin-4-FITC (AnaSpec, San Jose, CA, USA) for confocal microscopy examination (TCS SP2, Leica, Heidelberg, Germany) and photography. Biotin-4-FITC, which binds avidin specifically, was used to visualize the distribution of avidin-albumin MBs after ultra- sound exposure. The photographs from confocal microscope were converted into 8-bit gray-scale images. In each image, we chose 10 lines that were perpendicular to the clots surface for fluorescence study. For each line we calculated the average fluores-
33
cence intensity per unit distance. Then, the intensity and depth data from those lines in each image were averaged for demonstration and further analysis.
3.2.2 Microbubble Preparation
After mixing the human albumin (Octapharma, Lachen, Switzerland) and avidin (ThermoScientific, Rockford, IL, USA) with normal saline at 3% and 0.04%, respec- tively, the solution was ventilated with perfluoropropane and sonicated (S-450D, Branson Ultrasonic Corp, Danbury, CT, USA) in 280 Watt for 2 min, and then incu- bated on ice for 30 min. The concentration of the MBs was more than 8109/ml, and they had a mean diameter of 1.9 μm (range 1.0–4.0 μm) (Multisizer 3, Beckman Coulter, Fullerton, CA, USA), which changed less than 1% over 3 hours at 4C. The MBs were diluted with normal saline to the desired concentration prior to experi- ments.
3.2.3 Flow Cytometry Examination
In order to confirm that avidin integrates into the albumin shell and remains ac- tive after forming avidin-albumin MBs, we added biotin-4-fluorescein (AnaSpec, fi- nal concentration 0.01%) into the avidin-albumin microbubble solution (final concen- tration 0.04% and 1.2%, respectively), incubated at room temperature for 15 min with light protection, washed it with normal saline by centrifugation (1500 rpm for 5 min) for three times, and then used flow cytometry to measure the fluorescence of the MBs.
The avidin that remained active on MBs would bind biotin molecules, and this was counted by flow cytometry. Also, we used streptavidin-FITC (AnaSpec) to determine whether sufficient biotin-NHS molecules binds to red blood cells and remains active.
Freshly drawn human blood was washed with normal saline and centrifuged (1500
34
rpm for 5 min) to remove serum protein. Biotin-NHS was added with final concentra- tion of 0.08%,incubated at room temperature for 1 hour, washed three times by cen- trifugation. The streptavidin-FITC (final concentration 0.04%) was then added, incu- bated at room temperature for 15 min with light protection, washed by centrifugation, and counted by flow cytometry.
3.2.4 Ultrasound System
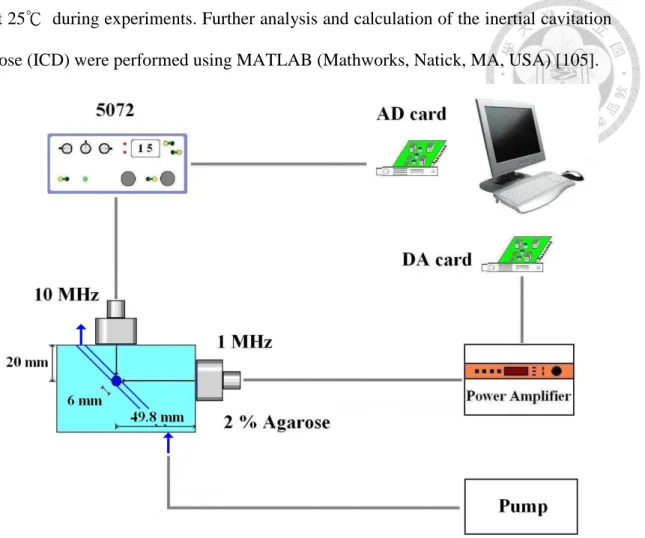
The acoustic measurement setup is shown in Fig. 7. A 1.0-MHz transducer (V302, Panametrics-NDT, Waltham, MA, USA) with a diameter of 25.4 mm and a focal length of 49.8 mm. was used for transmission. The transmitted waveforms were generated by a digital-to-analog converter (DA card) (CompuGen 1100, GaGe Ap- plied Technologies, Lachine, QC, Canada) and amplified by a power amplifier (250A250A, Amplifier Research, Souderton, PA, USA). The acoustic signals were detected by an unfocused 10-MHz transducer (V312, Panametrics-NDT) and sent to a receiver (5072PR, Panametrics-NDT). Pulsed waves were used in this study with a repetition frequency of 100 Hz, pulse duration of 10 cycles, exposure time of 1.5 sec, and acoustic pressures of about 1.32 MPa for cavitation settings [115]. A 2% agarose phantom was constructed with a cylindrical cavity (5 mm in diameter and 2.5 cm deep) to hold the blood clot and a tilting tunnel (2.7 mm in diameter) passing through the cavity. A continuous flow (5 ml/min) of MBs solution was provided by a syringe pump (KD Scientific, Holliston, MA, USA) to simulate the human arterial blood flow [128]. The microbubble solution comes out from the orifice of the flow phantom (shown by the arrow on the left of the 10-MHz transducer). It is lower than the orifice of sample cavity to make sure the flow rate is consistent within the system. Both transducers were positioned with their focuses within the cavity. Temperature remains
35
at 25℃ during experiments. Further analysis and calculation of the inertial cavitation dose (ICD) were performed using MATLAB (Mathworks, Natick, MA, USA) [105].
Fig. 7. Experimental setup.
3.2.5 Radiation Force Setting
Before experiments, we used the phantom model mentioned above to find out the radiation-force acoustic settings. A 6.7 MHz probe (10L, GE, Tokyo, Japan) of an ul- trasound machine (LOGIQ 500, GE, Tokyo, Japan) was placed opposite to the 10 MHz transducer to evaluate the movement of MBs. Radiation force produced by 1 MHz transducer was imaged by the GE system as the MBs pushed away from the transducer. Minimal cavitation effect presented in ICD was recorded. The radiation force settings included a pulse wave with a repetition frequency of 100 Hz, pulse du-
36
ration of 100 cycles, exposure time of 1.5 sec, and acoustic pressures of about 0.12 MPa.
3.2.6 Experimental Design
The experiments were divided into four groups [control, radiation forces, cavita- tion, radiation forces combined with cavitation (RF+Cav)], with the ten data samples collected within each group averaged to reduce human and system errors. The RF+Cav group was exposed to acoustic radiation forces followed by cavitation set- tings, and repeated these two acoustic exposures for 10 times (in order to maximize the effect). The radiation-force group and the cavitation group were also exposed 10 times to their respective stimuli to allow accurate comparisons. Different microbubble concentrations were used in the experiments. The samples in the control group with- out ultrasound exposure were immersed in a solution containing MBs at a concentra- tion of 4107/ml.
3.2.7 Statistics
Kruskal-Wallis one-way ANOVA was used to statistically compare between the experimental groups, with a P value of less than 0.05 considered to be indicative of significance.
3.3 Results
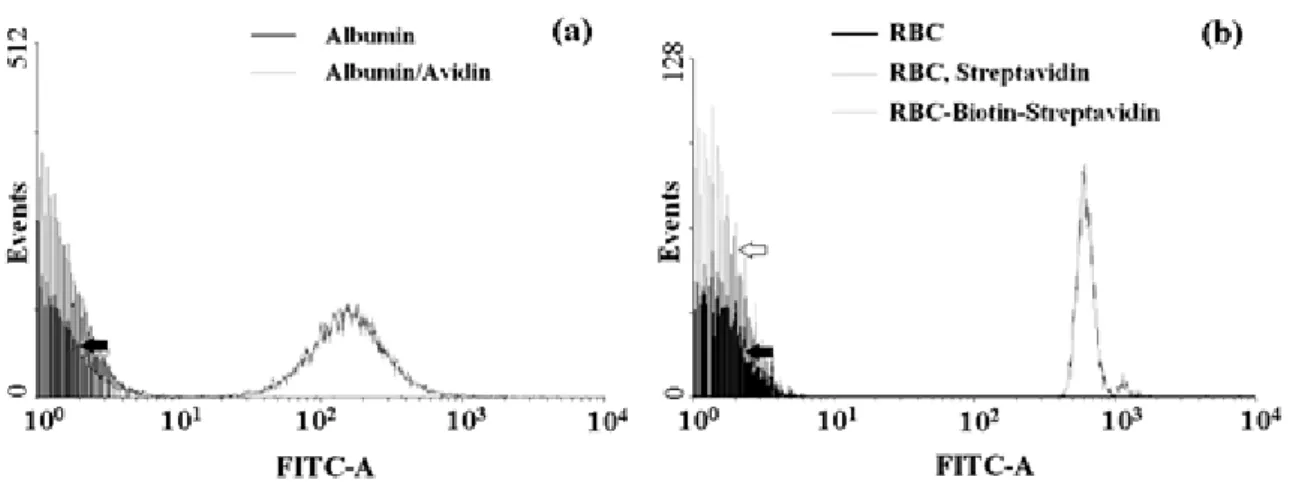
Fig. 8 shows the flow cytometry results of avidin on albumin MBs and the bind- ing condition of biotin-NHS on red blood cells. The black line (solid arrow) in Fig. 8(a) indicates that no biotin-4-fluorescein could bind albumin MBs without avi-
37
din, while the gray line indicates fluorescence on MBs. This figure indicates that avi- din did integrate into the albumin shell of the MBs and remains active. The gray line on the right side of Fig. 8(b) indicates that biotin-NHS was detected on red blood cells, while the gray line on the left side of the figure (hollow arrow) indicates the fluores- cence staining of red blood cells without biotin-NHS binding. The black line (solid arrow) indicates the background fluorescence of the cells. This figure indicates that biotin-NHS binds to red blood cells and remains active.
Fig. 8. Flow cytometry results. (a) Avidin and albumin MBs. (b) Biotin-NHS and red blood cells
(RBC).
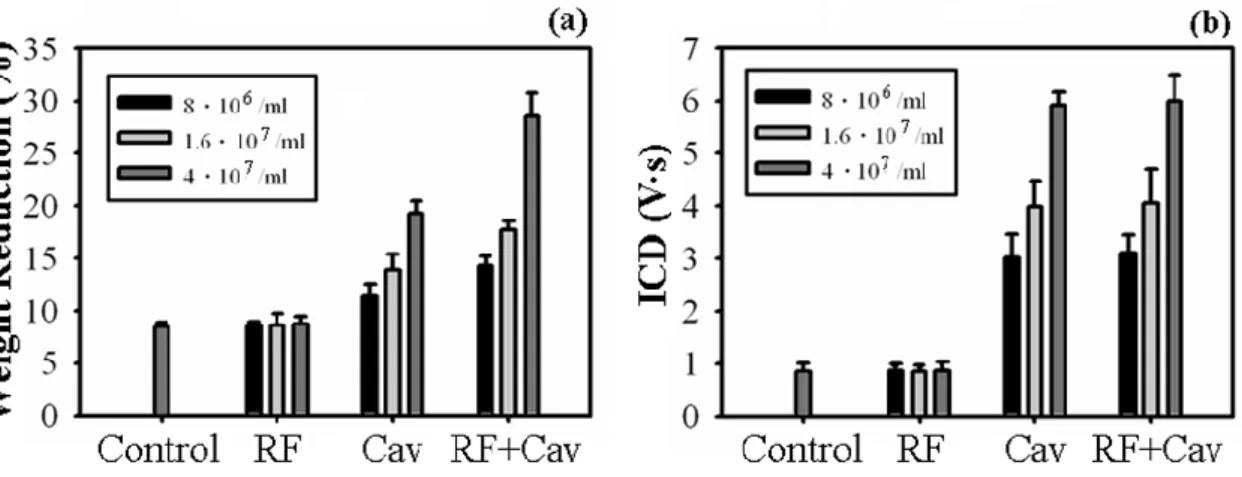
Fig. 9(a) shows the effects of radiation forces, cavitation, and radiation forces combined with cavitation on blood clots for different microbubble concentrations based on measurements of the weight reduction.Fig 9(b) indicates the cavitation in- tensity during the same set of experiments. The weight reduction produced by cavita- tion increased with the bubble concentration [Fig. 9(a)], as did the cavitation effect as evaluated by the ICD [Fig. 9(b)], relative to the control group. The ICD of control group represents the background level of cavitation for comparison. Both results are
38
statistically significant (p<005). The radiation forces alone exerted minimal effects on the weight reduction of the blood clot and ICD, relative to the control group, even if the bubble concentration increases. The statistics are insignificant. However, the RF+Cav group showed additional 3–9% weight reductions of thrombi relative to the cavitation group as the microbubble concentration increased and statistically signifi- cant (p<005). The ICD differences between the RF+Cav and cavitation group in the same bubble concentration are statistically insignificant. The discrepancy in weight reduction and ICD results between RF+Cav and cavitation groups is explained by the radiation force applied before cavitation effect in RF+Cav group.
Fig. 9. Effects of radiation forces (RF), cavitation, and radiation forces combined with cavitation
(RF+Cav) on thrombolysis for different microbubble concentrations. (a) Weight measurement. (b) ICD
evaluation.
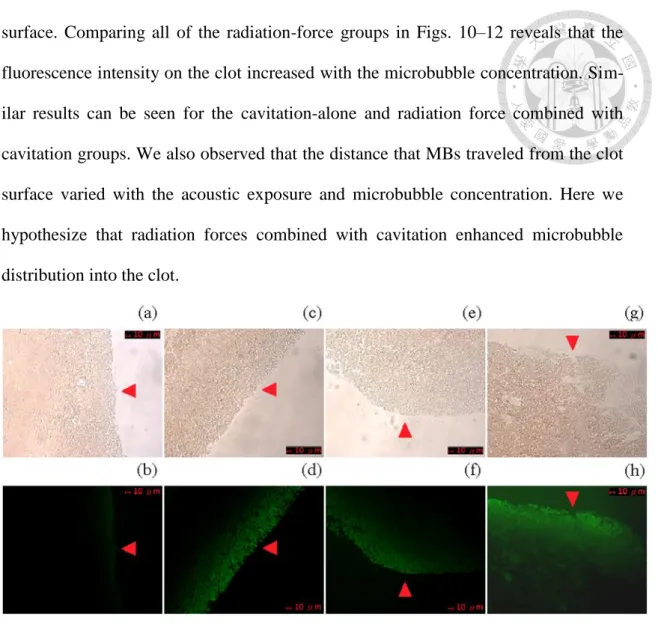
Figs. 10–12 demonstrate the fluorescence distribution and intensity of blood clots after ultrasound exposure. The fluorescence on the clot presents the distribution of avidin-albumin MBs, but it does not record the total acoustic effects ever exposed in individual experimental group (including sonothrombolysis). The distribution of MBs on the clot is described by the fluorescence intensity and depth from the clot
39
surface. Comparing all of the radiation-force groups in Figs. 10–12 reveals that the fluorescence intensity on the clot increased with the microbubble concentration. Sim- ilar results can be seen for the cavitation-alone and radiation force combined with cavitation groups. We also observed that the distance that MBs traveled from the clot surface varied with the acoustic exposure and microbubble concentration. Here we hypothesize that radiation forces combined with cavitation enhanced microbubble distribution into the clot.
Fig. 10. Confocal microscopy photographs of blood clots. Upper and lower rows are in color and FITC
fluorescence mode, respectively. Microbubble concentration is 4×107/ml. Red arrowheads indicate the
clot surface. (a) and (b) are control group. (c) and (d) are radiation force group. (e) and (f) are cavita-
tion group. (g) and (h) are radiation force combined with cavitation group. The photographs in the
same experimental group are from the same slice.
40
Fig. 11. Confocal microscopy photographs of blood clots. Upper and lower rows are in color and FITC
fluorescence mode, respectively. Microbubble concentration is 1.6107/ml. Red arrowheads indicate the clot surface. (a) and (b) are radiation force group. (c) and (d) are cavitation group. (e) and (f) are
radiation force combined with cavitation group. The photographs in the same experimental group are
from the same slice.
41
Fig. 12. Confocal microscopy photographs of blood clots. Upper and lower rows are in color and FITC
fluorescence mode, respectively. Microbubble concentration is 8106/ml. Red arrowheads indicate the clot surface. (a) and (b) are radiation force group. (c) and (d) are cavitation group. (e) and (f) are radia-
tion force combined with cavitation group. The photographs in the same experimental group are from
the same slice.
In order to quantify the fluorescence while minimizing observational bias, we converted the fluorescence images in Fig. 10–12 into 8-bit grayscale values (from 0 to 255) and then calculated the fluorescence intensity (as the difference between the re- gion of interest and the average background) and depth (distance from clot surface traveled by the MBs). Fig. 13(a) shows an example of fluorescence curve sampled from the images in the lower panels of Fig. 10 that had been converted into grayscale images. Fig. 13(b) and 13(c) present the results of fluorescence calculation. The dashed line in Fig. 13(a) represents the calculated depth and the grayscale value used when calculating the average fluorescence intensity. The results of Fig. 13(b) and (c)
42
represent the distribution of avidin molecules within the clots. We noticed that, after possible thrombolysis presented in Fig. 9, the fallen part of the clot cannot provide fluorescence here. In other words, the fluorescent intensity and depth here would not be interpreted as another presentation of weight reduction or total effect of thrombo- lysis. The fluorescence intensity on the clot increased with the microbubble concen- tration in each type of experimental groups, as shown in Fig. 13(b) and (c) and statis- tically significant (p<0.05). Fig. 13(b) shows that the fluorescence intensities in the radiation-force group were 1.9, 2.5, and 4.4 times (p<0.05) higher than that in the control group for microbubble concentrations of 8106/ml, 1.6107/ml, and 4107/ml, respectively, which was suggested by the total effect that active targeting of the avi- din-biotin system assisted by the shear forces induced by the acoustic radiation forces.
The corresponding fluorescence intensities in the cavitation group were 1.9, 3.5, and 4.2 times higher than that in the control group and statistically significant (p<0.05), which was explained by the shear forces associated with the effects of cavitation. Fi- nally, the corresponding fluorescence intensities in the RF+Cav group were 1.6, 2.2, and 5.4 times higher than that in the control group and statistically significant (p<0.05), which was explained by the shear forces produced by radiation forces and cavitation. Note that the fluorescence depths are not comparable between the groups with different acoustic exposures and the same bubble concentration. However, MBs did travel further (typically by 10~20 μm) than in the control group after being ex- posed to radiation forces, cavitation, or both. Also the statistics are significant (p<0.05).
43
Fig. 13. Calculations about fluorescence intensity and distribution in depth. (a) Example fluorescence
curve sampled from fluorescence images in Fig. 10, 11, 12 converted into grayscale values. The dashed
line represents the calculated depth and the grayscale value used when calculating the average fluores-
cence intensity. (b) Average fluorescence intensity. (c) Fluorescence distribution in depth from clot
surface. Data in panels b and c are mean and SD values.
3.4 Discussion
We have found that combining radiation forces with cavitation can reduce the damage to the surrounding tissue and improve the efficacy of sonothrombolysis. Cav- itation-related tissue damage after microbubble destruction has been demonstrated at high doses of MBs and high acoustic pressures (greater than those used clinically) [129,130]. One possible way of reducing unwanted cavitation-induced tissue damage is to localize MBs to the target area. Our results in Fig. 9 demonstrate that combining
44
radiation forces with cavitation provided an additional 3–10% weight reduction of the thrombus relative to cavitation alone. We attribute this to cavitation occurring inside the blood clot after the targeting of MBs was enhanced by the radiation forces.
Devcic-Kuhar et al. showed both theoretically and experimentally that the effects of radiation forces on sonothrombolysis are much less than those of microstreaming [131]. They used thrombolytic agent recombinant t-PA exposed to standing and trav- elling waves for their study and no microbubble was added. They concluded that acoustic streaming and shear stress are probably the most important mechanisms of ultrasound contributing to thrombolysis enhancement. In our experiments the radia- tion forces exerted minimal effects on thrombolysis with added MBs but without thrombolytic enzyme. However, combining radiation forces with cavitation effects produced an additional weight reduction of the thrombus relative to the cavitation group, with this being evident even for lower microbubble concentrations. These findings look promising for reducing the unwanted damage produced by cavitation when using radiation forces to enhance the targeting and localization of MBs.
Figs. 10–13 show that the MBs were distributed at greater depths (by 10~20 μm) in all of the experimental groups than in the control group. The microbubble distribu- tion on the clot surface in the cavitation group are likely due to microjetting and mi- crostreaming phenomena, while the shear forces produced by the radiation forces are suggested to explain the results obtained in the radiation-force group. Many previous studies have focused on the shear forces produced by radiation forces in a fluid [22,54–56]. Our results provide evidence that radiation forces can be used to enhance the movement and targeting of MBs inside tissues such as a thrombus. Such en- hancement of targeting could be employed to deliver drugs across the leaky vessels in tumors and inflammatory tissues, as suggested by Hashizume et al. [132]. The spatial
45
selectivity provided by radiation forces has substantial potential to improve the local- ization of delivery and reduce systemic toxicity [133]. Nonspecific endothelium or vessel-wall damage produced by cavitation could also be reduced by localizing MBs using radiation forces [56,134–137]. The combined application of radiation forces and cavitation provides better effects in sonothrombolysis than do radiation forces or cav- itation alone, as shown in Fig. 9.
3.5 Conclusions
Acoustic radiation forces facilitate the targeting of MBs to blood clots, and this study has demonstrated that combining radiation forces and cavitation provides better effects in sonothrombolysis than do radiation forces or cavitation alone.
46
Chapter 4
Albumin Acts Like TGF-β1 in Microbubble-Based Drug De- livery
4.1 Introduction
Chemotherapy is one of the most important approaches for treating breast cancer patients. However, chemotherapeutic drugs such as paclitaxel (PTX) and doxorubicin lack cytotoxicity selectivity between cancer cells and normal cells, which frequently leads to serious side effects. Also, the poor water solubility of PTX makes it difficult to administer in clinical applications. Drug resistance and limited access of the drug often results in the drug concentration not been sufficiently high to kill malignant cancer cells [65, 66]. Therefore, localized drug delivery looks promising in reducing systemic toxicity and maximizing tumor exposure [67]. Drug-loaded-MBs destruction in combination with ultrasound has recently become one of the most promising ther- apeutic applications in drug delivery [68], since drug-loaded MBs can be manipulated and destroyed by ultrasound applied at the tumor site, causing localized release of the drug [69-72]. In addition, combining MBs with ultrasound can increase the permea- bility of physiologic barriers such as the blood–brain barrier, capillary endothelium, and the cell membrane for macromolecules or even colloidal particles [73, 74]. Sever- al investigations on the application of ultrasound contrast agents as tumor drug deliv- ery systems have recently been reported. Kang et al. showed an antitumor effect of docetaxel-loaded lipid-shelled MBs combined with ultrasound-targeted MB activation on VX2 rabbit liver tumors [75]. Xing et al. demonstrated the effective treatment of