୯ҥᆵεᏢᙴᏢଣᙍૈݯᕍᏢࣴز܌
ᅺγፕЎ
Graduate Institute of Occupational Therapy College of medicine
National Taiwan University Master Thesis
ᙴᕍவΓϐᎦԋၸำύ!
ӕЈᆶճޗՉࣁϐᡂϯ!
The Chronological Change of Empathy and Prosocial Behavior in
Healthcare Professionals
શᇽ Jasin Wong
ࡰᏤ௲Ǻֆࡌቺ റγ Advisor: Chien-Te Wu, Ph.D.
ύ҇୯ 102 ԃ 7 Д July, 2013
ز܌ ܌ ܌ ܌ ܌ ܌ ܌ ܌
୯ҥᆵεᏢᅺγᏢՏፕЎ α၂ہቩۓਜ
ᙴᕍவΓϐᎦԋၸำύӕЈᆶճޗՉࣁϐᡂϯ The Chronological Change of Empathy and Prosocial Behavior in
Healthcare Professionals
ҁፕЎ߯શᇽȐR00429009ȑӧ୯ҥᆵεᏢᙍૈݯᕍ Ꮲسǵ܌ֹԋϐᅺγᏢՏፕЎǴܭ҇୯ 102 ԃΎДϖВ܍Πӈ Ե၂ہቩ೯ၸϷα၂ϷǴԜܴ
α၂ہǺ
ࡰᏤ௲Ǻ
շ௲
α၂ہ ୍ܺᐒᄬᆶӜᆀ
ᎄᖚ
୯ҥܴεᏢઓࣽᏢࣴز܌
ୋ௲
ᎄΚଈ
୯ҥύξεᏢޗᏢس
ୋ௲
Ԣࡏғ
ύѧࣴزଣޗᏢࣴز܌
շࣴز
ᙍૈݯᕍᏢسسЬҺǺ݅լ۸ ЬҺ
ύ҇୯൘ԭ႟ມԃࢠД
!! !
Ў
Ў
Ў
Ў
ठ ठᖴ!
ؒགྷډ೭ᇥߏόߏǴᇥอόอޑٿԃࣴزғఱǴΨಖܭډΑቪठᖴޑਔংǶ ӣགྷ೭ٿԃǴεཷࢂךᏢғఱύനᆒჴǵനٌधΨനזޑࢤਔӀǶ
२ӃǴךाձགᖴӧᅐߏޑᏢၡύ๏ךֹӄЍޑΓ—ךޑРᒃǶΨ ӢࣁԖдǴךωૈคࡕ៝ϐኁޑך഻ޑࣴزǶќѦǴΨाགᖴךޑР҆Ǵ
Ꮲғఱύന߃ޑඵችᏤৣǶ
ځԛǴߚதགᖴךޑࡰᏤ௲—ֆࡌቺԴৣǴд๏Αךനεޑޜ໔วචǵႴ ᓰךوрਣࢎࡘԵǴΨ๏ך߿ֹԋԾρޑགྷǴ٠ӧᜢᗖਔڅЇᏤךǵቍઢךǶ ᗋԖᏼҺךፕЎीฝکፕЎα၂ޑہॺǺᎄᖚԴৣǵᎄΚଈԴৣکԢࡏғԴ
ৣǴգॺޑཀـᔅշךुۓᚒҞǵঅׯჴᡍБݤǵࡘԵࣴزЬᚒǴ٠Їሦךوр
⭩␎ǴᘉεךޑࣚǶᛥ໋зԴৣǺၟᒿԴৣޑङቹǴᡣך࣮ډᙍૈݯᕍޑ
҅ሽॶᆶԾρޑёૈǶӵ݀ؒԖᖴమᡕԴৣӧεΒපଷਔޑЈЇᏤǴךགྷך ёૈΨόΑ೭ࣴز྅ǶᗋԖǴ݅լ۸ԴৣӧεѤᚒፕਔᡣךΑှيࣁ
ঁᏢޣ܌၀ڀഢޑᄊࡋᆶדǶќѦǴယធԴৣᡣךΑှډࣴزჹܭᖏ
ޑख़ा܄ǶќѦǴΨाགᖴ೭ၡഉՔךᅺғఱޑӕᏢॺǺ൛Ǵᖴᖴی೭ ٿԃٰޑ࣬ϕןǴѝԖيࣁӕჴᡍ࠻ޑیёаΑှ೭ځύޑለౡधᇺǶᴜǴ ᖴᖴیᕴࢂࡐ୲ჴޑުᆮǴջਔޑ๏ϒךനޔௗޑࡰЇǶᗋԖጰ൛ᏢۊӧӚБ य़ޑࡌǴ٠ӧр୯ਔගٮಉጕచޑךڐշǶךޑࣴز܌ӕᏢॺǴᖴᖴգॺکך
ଆوၸࣴز܌ᕷख़ԶкჴޑፐำǴӢࣁکգॺଆတΚᐟᕏǴךωૈֹԋ೭ঁ
ࣴزǶ
ௗǴךाձགᖴӧךࣴزගٮڐշǵှൽޑӕᏆॺǶӵ݀ؒԖⓥᏢ ۊޑεΚᔅԆǴךགྷךډӧёૈᗋคݤᗎፎٗሶӭᙍૈݯᕍৣٰୖуჴᡍǴӢ ࣁԖیǴωૈ٬ךޑࣴزीฝбፏჴǶᖴᖴ܃ԋջ٬ӧࣴزғനԆޑਔংǴᗋ ᜫཀਔ໔ձ௲ᏤךၗϩǴ٠๏ךЍǶќѦǴᖴᖴॕഉՔךࡋၸᅺ
ԃޑЈਔӀǴૈک഻ޑΓଆঅፐࢂനזޑ٣Ƕձགᖴֻণǵറ๔ک ࣄǴᖴᖴգॺᜫཀਔ໔ᔅךঅׯ JAVA ำԄǵഉՔךቪΓғύಃঁ matl
abำԄǵคҶคЗޑ debugǴךుޕਔ໔࣮ᔉձΓ܌ቪޑำԄᇟقሡाคКޑऐ
ЈǴ܌аߚதགᖴգॺޑ϶ڐշǼќѦฅᗋԖךޑ toolboxǺഋᴜπڀጃ(ٰ
ྍઓઝǴคݤڗ)Ƕ
Αቪठठठठठठठठᖴޑᖴޑᖴޑᖴޑᖴޑᖴޑᖴޑᖴޑᖴ ਔংਔংਔংਔংਔংਔংਔংਔংǶ ࢤਔӀǶ
ᗋԖाགᖴٗ٤ӧךᅺғఱύ٩ฅჹךόᚆόకޑӳܻ϶ॺǴҏکᑯǴ ᗨฅـय़ޑਔ໔όӭǴՠགྷډیॺΨӧيೀНుОϐύǴ൩ளವӜޑז
Ƕඍ൛ǵࢀᆺᕴࢂࣁךޑғࢲቚబӭઢǴکیॺӧଆ൩ૈᡣךགྷႽрऍ ӳғࢲޑኬᇮ(ؒᒱǼࣴزғғࢲࢂाགྷႽωऍӳǶ) ךޑӳۊۂॺǺᆢীǵ
٫֗کޱǴᖴᖴیॺᕴࢂхךޑँฅѨǴ٠ӧեዊਔӼኃךǶ
ќѦǴགᖴനख़ाޑৎΓǴᖴᖴۊۊکۊϻᕴࢂ໒ᚈЋ߆ௗךډৎ္ۺ(͵
Ͷ)ਜ(Ή)ǶᗋԖᕴࢂᔅךວکЬ҅ကޑǶ
ߚதख़ाӦǴךाགᖴ೭ 121 Տᜫཀਔ໔ǵऐЈޑୖуךޑࣴزޑΓॺǴ ӧךޑЈύǴգॺ൩ࢂٗဂᄋඉǵᜫཀϩ٦ޑΓॺ(คፕჴᡍޑ่݀ӵՖև)Ƕᖴ ᖴ OT98 ୖу୍ܺᏢಞΟޑᏢۂॺǴӢࣁԖգॺǴךωૈགྷр೭ঁࣴزЬᚒǶᖴ ᖴ OT99 ޑ܌ԖӕᏢǴךӧգॺيᕇளࡐӭཥޑࡘԵکྕធޑ϶ǶOT100 ୖу ჴᡍޑεᏢۂॺǴգॺޑપ๓ؼᡣךΑှϙሶॶளࣔெǶ
നࡕाགᖴӧךࣴزሦୱޑ፸ॺǴӢࣁԖգॺޑᄋඉǴךωૈᕇளᙦޑ
ୢڔǵჴᡍीǵჴᡍǵྗϯკТǵၯᔍǵྗϯӷຒǶՠӢԜϩӧ ВࡕፕЎว߄ਔ(ӵ݀Ԗޑ၉)ևǴЪ೭٤ΓΨ࣮όᔉύЎǴࡺᙁाගၸǶ
ाགᖴޑΓϼӭΑǴٯӵᎦךऐЈޑѠεᙴᏢଣ IRB ہǵຠЈࣴزғ
மॐଷВ੮سᓔԶჴࡼޑϦፁεኴૈ෧ᅹࡼǵՉࡹΓόჇځྠޑ௲Ꮴך ൔำׇ…Ǵٗ൩ᖴϺփ (ഋϐ᛫Ǵ1961)Ǽ
კ კ႟!
ഉՔךٿԃޑჴᡍ࠻ӓ౺ނȋදങ݀এ!
ॺǴҏҏҏҏککککککککᑯᑯᑯᑯᑯᑯᑯᑯᑯǴ ൩
൩ளವளವளವளವளವளವளವளವӜޑӜޑӜޑӜޑӜޑӜޑӜޑӜޑӜ זזזזזזזזז ൩ૈᡣᡣᡣᡣᡣᡣᡣᡣךགྷךགྷךགྷךགྷךགྷךགྷךགྷךགྷႽрႽрႽрႽрႽрႽрႽрႽႽрႽ ऍऍऍऍऍऍऍऍ ӳۊۊۂॺۂ Ǻᆢᆢᆢᆢীǵীǵ
ᄔ ᄔा
ङඳǺӕЈکճдЬကࢂᙴᕍউύਡЈޑሽॶǶၸѐӕȋճдՉࣁଷᇡ ࣁǺΓޑճдՉࣁࢂᙖҗౢғӕдΓϐག܌ЇวޑǶฅԶԜଷ՟Я٠ό
Ҕܭࢌ٤ۓნǴٯӵᙴᕍΓၸࡋᆫขܭੰคݤှޑภधਔǴ٬ᙴ ᕍவΓౢғคΚགǵલЮԾߞЈǴᏤठᙍ॰࡙ǵൿኈੲЮکեғࢲࠔ፦Ǵ
Զ٬ᙴᕍவΓफ़եᙴᕍ࣬ᜢޑշΓՉࣁǶՠҞ٠҂ԖࣴزᙴᕍΓ
ޑӕЈᆶճޗՉࣁٿӢη໔ޑᜢ߯ǴࡺᙶమԜມӢηჹܭᙴᕍவΓՉࣁ ޑቹៜߚதख़ाǶฅԶǴၸѐࣴزӭаԾຑԄୢڔٰຑڙ၂ޣϐӕЈǴԜݤ ҭౢғޗයࡑୃᇤǶќѦǴၸѐࣴزҭӭख़ܭຑᙴᕍவΓϐӕЈǴ ϿԖࣴزᙴᕍΓޑӕЈᆶճޗՉࣁϐ࣬ᜢ܄Ƕ!
ҞޑǺ2/!ϩձ٬ҔόӕޑჴᡍڂጄǴᗦஏޑෳ၂ᙴᕍவΓޑӕЈᆶճޗ
ՉࣁǶ3/!ΑှᙴᕍவΓӧᐕᙴᕍ࣬ᜢ૽ግϷᖏჴಞࡕǴځӕЈᆶճޗ
ՉࣁޑᡂϯǶ!
БݤǺךॺܕԏΑѤಔڙ၂ޣǴಔ 41 ΓǴϩձࣁǺᙍૈݯᕍৣǵᙍૈݯᕍε
ᏢғǵڋಔΓǵڋಔεᏢғǶךॺ௦Ҕᇟნ࣬ᜢϐׯؼࠠᆣў
ཱදჴᡍڂጄຑڙ၂ޣϐӕЈǶќѦǴךॺҭၮҔႝတϯᎿШճޗၯᔍǵ ϷׯؼԾᐱຊޣᖻֽϐਈᒲჴᡍٰෳᡍڙ၂ޣϐճޗՉࣁӛǶ!
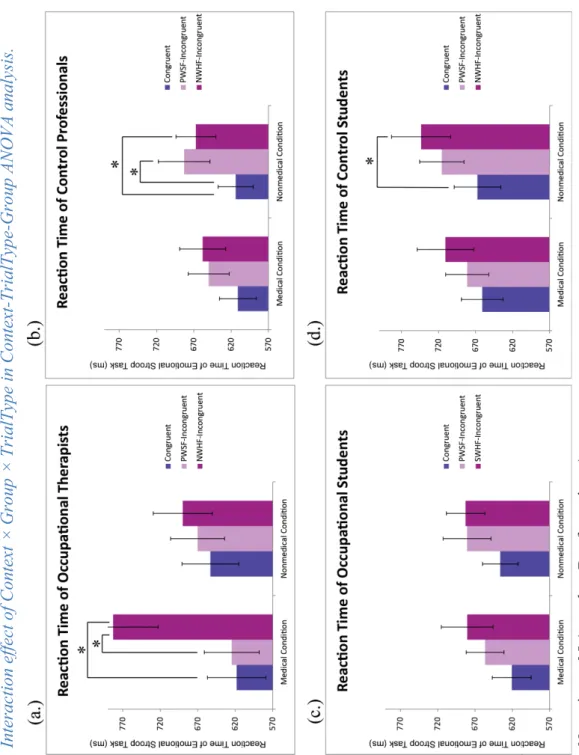
่݀ǺᙴᕍவΓܭᙴᕍ࣬ᜢნύǴफ़եдॺ࣮ډൿᖍϾޑᆣϸᔈǴ ՠԜፓຝ٠όӧᙴᕍคᜢნύ܈זᖍϾύрǶ࣬ჹӦǴԜნۓ ޑᆣፓᐒڋ҂ӸӧܭځдΓ܈ᏢғಔύǶќѦǴᎿШႝတϯၯᔍϷ ਈᒲჴᡍ่݀ᡉҢǺᆶᏢғಔКၨǴᙴᕍவΓᆢଯำࡋޑճޗՉࣁӛ ܭᔕნϷჴሞғࢲნύǴฅԶڋಔΓ࣬ၨܭᏢғಔǴځճޗՉ ࣁޑӛᡉӦफ़եǶջ٬ڋΑᖒၗϷٿঁషౄᡂࡕǴԜ่݀٩ฅᡉǶ!
่ፕǺ่݀ᡉҢǴᙴᕍவΓਥᏵნٰፓдॺჹܭൿნޑᆣϸᔈǶ ќѦǴᙴᕍவΓёаᆢӵᏢғಔኬଯำࡋޑճޗՉࣁǶӕЈکճޗ
ՉࣁӧᙴᕍவΓύ٠҂ᡉ҅࣬ᜢǶԜ่݀ёૈྍܭᙴᕍவΓӧᙴᕍ
ნύวрձޑᆣፓسǴ٬ځխܭၸܭӕᙴᕍ࣬ᜢޑൿ٣ҹࡕౢ
ғޑᆣ֚ᘋϷൿኈੲЮགǴаߥԖճޗՉࣁǴុठΚܭᙴᕍדύǶ!
ᜢᗖຒǺӕЈǴᙍૈݯᕍǴ଼நྣៈǴշΓՉࣁǴճޗՉࣁǴճдЬက!
ȋճдՉдՉдՉдՉдՉдՉдՉдՉࣁଷࣁଷࣁଷࣁଷࣁଷࣁଷࣁଷࣁଷଷଷᇡᇡᇡᇡᇡᇡᇡᇡ Ԝଷଷ՟Я՟Я՟Я՟Я՟Я՟Я՟Я՟Я՟Я٠ό٠ό٠ό٠ό٠ό٠ό٠ό٠ό٠ ޑภधਔ ٬ᙴ
Abstract
Background: Empathy and altruism are two core values of healthcare profession.
Empathy-altruism hypothesis claimed that altruistic behaviors are motivated by empathy. However, this hypothesis does not seem to hold in certain contexts. For example, over-emphasizing on patients’ unalleviated suffer may make medical professionals feel helpless and diminish their confidence which could led to burnout, compassion fatigue and low quality of life. These drawbacks could further dampen medical-related prosocial behaviors, which appears to contradict the prediction of the empathy-altruism hypothesis. Most of previous related studies in health care systems focus only on empathy without any discussion on prosocial behaviors. In addition, the traditional questionnaire based evaluation of empathy suffers from serious vulnerability to response bias due to its nature of explicit measurement. Therefore, the relationship between empathy and prosocial behaviors remains unclear.
Objectives: There were two primary aims for the current research: 1. To develop
effective paradigms for implicit evaluation on empathy and prosocial behavior patterns;
2. To investigate the chronological change of the relationship between empathy levels and prosocial behavior patterns in healthcare professionals.
Method: Four groups of participants including occupational therapists, occupational
freshmen, and two corresponding controls participated in the current study. We proposed a novel modified Emotional Stroop paradigm to implicitly evaluate empathy.
Furthermore, we used computerized Zurich Prosocial Game (ZPG) and a donation paradigm modified from dictator games to implicitly evaluate of prosocial behavior patterns.
Results: Health care professionals tended to show reduced emotional responses toward sad facial expression after empathizing medical-related scenarios of negative emotion.
lthcararararararararee eeee ee prprprprprprprprofofofofofofofofffesesesesesesessisssisissisisisionononononononon.
are mom tivated d byby
In contrast, we did not observe similar context-based emotional modulation in other control professionals and student groups. Furthermore, results from ZPG and donation experiment revealed that health care professionals maintained high degrees of prosocial behavior both in virtual game context and in real-world donation, which was not seen in control professionals
Conclusion: Our results therefore suggest that the reduced emotional responses under
empathizing processes of healthcare professionals is contextual oriented. On the other hand, however, they maintain high degrees of prosocial behavioral trait under reduced levels of empathy, which provides evidence against the empathy-altruism hypothesis.
A possible explanation is that health care professionals modulated their empathy toward medical related negative events to protect them from personal distress and enable them to maintain their high degrees of prosocial caring behaviors.
KeywordsǺempathy, occupational therapy, healthcare profession, helping, prosocial behavior, altruism
odulatititiiiiionononononononon iniiiiiiinnnnnn n otototototototother ZPGGG GGG GGanananananand nnd d d d dd ddodododododododonanananananananan titttttttononononononon egreessssss o o o o o o ooofff f f f prprprprprprprprososososososososocococococococociaiiiiiii l ich was not seen in
VII
Contents
α၂ہቩۓਜ ... I
ठᖴ ...II ᄔा ... IV
Abstract ... V Contents ... VII List of Figures ... IX List of Tables ... X
1. Introduction ... 1
1.1 Altruistic Behavior or Prosocial Behavior ... 3
1.2 Models of Prosocial Behavior ... 4
1.2.1 Some Points from Self-serving Prosocial Behavior ... 4
1.2.2 Empathy-altruism Hypothesis ... 10
1.3 The Definition of Empathy ... 12
1.4 Empathy in Healthcare Profession ... 14
1.5 Aims of Current Research ... 17
2. General Methods ... 18
2.1 Apparatus ... 18
2.2 Participants ... 18
2.3 Experiment 1: Implicit Evaluation for Levels of Empathy Using Emotional Stroop Paradigm ... 20
2.3.1 Procedures ... 26
2.3.2 Analysis ... 29 .......IIIIII ...III
VIII
2.3.3 Results ... 30
2.4 Experiment 2: Implicit Evaluation of prosocial behavior - Zurich prosocial game 39 2.4.1 Procedures ... 41
2.4.2 Analysis ... 45
2.4.3 Results ... 46
2.5 Experiment 3: Explicit Evaluation of Prosocial Behaviors ... 49
2.5.1 Materials ... 49
2.5.2 Procedures: ... 50
2.5.3 Analysis ... 51
2.5.4 Results ... 53
3. Discussion ... 56
4. Conclusion ... 66
5. References ... 67
... ...30 - Zuuuuuuuuriririririchchchchchchchch p p p p p pppprorororororororosoosososososososocicicicccaalalaalaa
41
IX
List of Figures
Figure 1... 22
Figure 2... 23
Figure 3... 24
Figure 4... 25
Figure 5... 30
Figure 6... 31
Figure 7... 32
Figure 8... 33
Figure 9... 34
Figure 10... 36
Figure 11 ... 38
Figure 12... 42
Figure 13... 46
Figure 14... 47
Figure 15... 53
Figure 16... 54 ...2222222222 ... 2323
X
List of Tables
Table 1 ... 18 Table 2 ... 48 ... 1818
1. Introduction
Sixteen years have passed since I listened to words that would shape my care of patients. I have witnessed untold tragedies, but through it all my solace has been the gift of a last touch, a last kiss, a last word, and the hope that these moments would alleviate some of the suffering. I pray that other caregivers will learn this lesson sooner than I did and extend not only all that technology has to offer, but all that our hearts have to offer, as well.
Janie K. Ford, 2001 Imagine you are a flight nurse working in aeromedical evacuation. One day you are assigned to airlift a five-year-old child who has stopped breathing. You confront a hysteric mother who is emotionally unstable with worrisome and desperately wants to accompany with her baby. The vital signs of the kid do not look promising, and the condition is so critical that the child requires advance care immediately. Not a single second can be wasted. You also realize that this may be the last chance for this mother to seize her live, warm baby with her arms. What is even worse, the helicopter is too small to bring parents on. Looking at the distraught mother, will you give the chance for the possibly last monetary contact between this mother and her child?
This condition once happened in Janie, a competent flight nurse, and it is the situation that most medical staff in aeromedical evacuation might meet every day in their medical career (Ford, 2001). The patients whom medical staff deliver are so extremely critical that most of them died not having the opportunity to receive the medical technology and therapy. However, their families are still relied on the last hope which is brought by medical workers. Therefore, these experienced medical professionals are obliged to handle this emergency with their well-established skills, concern for the welfare of patients and fulfill the spirit of medical altruism. They were
ould ssssssshahahahahahahahapepepepepepepepe m m m mmmmmmy y y yyy yyy all lmym sollllllllacce
also expected to have the feeling of empathy to imagine the times of patients and to envision the inner experience of its passage. However, these values sometimes come to conflicts that the most effective way to help patients and their families would probably not so humane and lack of emotion-concerned. Further, the feeling of empathy affects the way medical caregivers dealing with life-and-death events and making difficult clinical decisions, which are traditionally thought to be the representation of altruistic behaviors in medicine. It has been long believed that feeling of empathy and compassion toward others could evoke the motivation of altruistic behaviors (Coke, Batson, & McDavis, 1978; Eisenberg & Miller, 1987; Krebs, 1975); however, due to some contradictions in medical helping behavior and empathy, it is critical to determine the relationship again between these two factors of empathy and helping behavior, especially in medical professionals. To examine these two factors, it is necessary to know the cultural evolution of altruism and identified the definitions.
Altruism is a good virtue praised by many cultures and religions. For example, the greatest miracle in Christen was the self-sacrifice behavior of Jesus. This value is even specifically thought to be the core characteristic of medical professionals (Coulter, Wilkes, & Der-Martirosian, 2007; McGaghie, Mytko, Brown, & Cameron, 2002; Sylvia R Cruess & Cruess, 1997), just as the Declaration of Geneva in 2006 stated ‘At the time of being admitted as a member of the medical profession, I solemnly pledge to consecrate my life to the service of humanity.’ The Medical Schools Objectives Project (MSOP) also stated that ‘Physician must be altruistic’ (Medical professionlism in the new millennium: a physician charter., 2002). Not to mention that altruism is the keystone in the Hippocratic Oath which is the initial vows of medical professionals.
Therefore, in traditional view, medical care providers were obligated to be altruistic and of self-sacrifice (Bishop & Rees, 2007; Jack Coulehan, 2005; Jones, 2002; McGaghie et of patttttttieieieieieieiei ntntntntntntntnts sss ss anananananananand nddddddd to ometeteteteteteteteimimimimimmmmeseseseseseseses c c c c c comccomomomomomomomo eeeeeeetototototottoto es wooooooululululululululuddd d d d d prprprprprprprprobobobobobobobobabababababababablyy of empathhy affects
al., 2002).
However, this traditional value was challenged by the unrealistic expectation of medical professions which would made them to feel overwhelming pressure when they confronted difficult situations they could not handle, and these frustrations may easily cause burnout, distress, compassion fatigue, and low medical caring qualities. Further, the operational definition of altruism in medical field was even obscure due to the concept was too abstract to be measured (Bishop & Rees, 2007; Burks & Kobus, 2012;
Neumann et al., 2011; Wall et al., 1997). Therefore, it is critical to examine the appropriateness of altruism in medicine which advocated other-oriented devotion and self-sacrificed behavior, the effects of altruism when medical professionals contact with patients, and the factors that could impact the helping trends of health care givers.
1.1 Altruistic Behavior or Prosocial Behavior
The word altruism appeared to be initially introduced to scientific field by the philosopher Auguste Comte. The word originated from Latin word ‘alteri’ which means ‘other’. In contrast to ‘egoism’, referring to self-oriented behaviors, altruism corresponds to behaviors of unselfish caring about others’ needs, enhancing their welfares and helping others (Batson et al., 1988; Batson & Shaw, 1991; Comte, 1852;
Coulter et al., 2007). Altruism has traditionally been recognized as the central value of medical professionalism (Coulter et al., 2007; McGaghie et al., 2002); however, there were criticism arguing whether altruism, which includes self-sacrifice and unselfish devotion, is a good virtue in medical profession or not. Further, the definition of altruism in medical field has been still arguing due to the concept of altruism which concerned the inner motivation was too abstract to be measured. Hence medical educators and researchers could not evaluate whether the altruism of students and stic eexexexexeexpepepepepepepepecctctctctctctctatatatatatatatatioioioioioioioioi nnn nnnnn ofofofofofofof f pressurururrrrrree e e e e e e ewhwhwhwhwhwhwhwhenenenenenenenen t t t t t thetthehehehehehehey y rations may easily
trainees improved by medical training process or not. Most of all, it was even not sure whether the altruistic behavior exists in human society because it is difficult to know whether an actioner’s motivation is self-oriented or fully unselfish. Moreover, there was paradox between medical professionalism and altruism due to altruism required the pure other-oriented behavior which could not get money or other benefits from this behavior.
Therefore, we use another border concept to describe the helping behavior: prosocial behavior (Bishop & Rees, 2007; Jaeggi, Burkart, & Van Schaik, 2010; Penner, Dovidio, Piliavin, & Schroeder, 2005). Regardless of an actioner’s motivation, prosocial behavior is defined as behavior that is beneficial to others or societies, including not only altruistic behavior but also some self-directed behaviors like cooperative behavior and reciprocal helping behavior.
1.2 Models of Prosocial Behavior
1.2.1 Some Points from Self-serving Prosocial Behavior
Prosocial behavior was the biggest enigma to Darwin when he propounded the theory of natural selection. He has noticed some individuals in order to ensure the group survival, would make themselves to be eliminated through selection. This phenomenon was incompatible to his theory (Charles Darwin, 1859; Gazzaniga, 2008). When a social group operated adaptably, individuals in the group must have to help each other.
However, these prosocial behaviors seldom maximized the relative adaptability of the individual in the group. Therefore, some evolutionary biologists proposed group selection theory. This theory suggested that selection not only existed in the individual level, but also happened in higher group level. That means although the selfish individual might surpass the altruistic one within group, when it came to group level,
was evevvvvvvvenenenenenenenen notnnnnnnnotototototototot s s s s ssssure s diffffffffffffffffficicicicicculululululululult ttt ttt t tototototoooo k k k k k kkknnnononnnn ww wwwww Moreoveveveveveveveeer,r,rr,r,r,rr, t t t t ttttheheheheheheheherererererererere w w w w was www m requireddthe pure
there were two groups in competition within limited space, food and water resources, the group which had more altruistic individuals would had better opportunities to survive and reproduce than the selfish group; hence, individual not only had to maintain its personal fitness within group, but also presented some altruistic behaviors to enable group survival (David Sloan Wilson & Edward O. Wilson, 2007; Penner et al., 2005). In the process of evolution, individuals must have to achieve a balance between the two extremes of selfishness and altruism. However, there were also some criticisms. The famous evolutionary biologist Williams argued that selection would not react to social interactions, and the meaning of selection was not to avoid the extinction of the whole species but to enhance the survival probability of individuals (Roes, 1998). Therefore, whether group-level selection could surpass individual-level selection has still been debated in evolutionary field. In order to solve the problem, kin selection developed.
This hypothesis suggested that it was more like to pass down the own gene to next generation than to pursue the individual selfish survival. Individuals tended to help and protect their relatives due to they had more genotypes similarity. This could easily been seen in human society that people would choose their children or siblings when they encountered emergency (Hamilton, 1964a, 1964b). However, this theory could not explain why human still helped their friends and even strangers. Further, when speaking of prosocial behaviors within medical professionals, these two evolutionary theories seemed to not be the perfect interpretation because there were often no kinships between patients and medical professionals, and the specificity of altruism in medical professionalism could not be explained by evolution.
To explain the prosocial behaviors between strangers and friends who did not share the same gene, several evolutionary biologists proposed the reciprocal altruism theory.
Human helped others and expected others would help them in return. This action could d wateeeeeeer rrrrr rerererererereresosososososososoururururururuururcecccccc s, r opppppppppppppppporororororororortutututututututuninininininininitititititititititeseseseseseseses t t t tttttoo ooooo nly hadadadadadadadadd t t t t t t to too o o o omamamamamamamamainininininininintatatatatatatatain behaviors to enable
also earn the survival advantages among individuals. However, there were some prerequisites of this reciprocity hypothesis. First, individuals had to remember and recognize the other individuals who had helped them or been helped by them. Second, there were frequent interactions between these two individuals, so that the helper could anticipate feedbacks and the receiver could request to the helper. Third, individual could evaluate the cost-effectiveness of helping, and know this paying was deserved. Fourth, individual had must be able to identify the liars, or they might be exploited by cheaters and lose the advantage of fitness (Leda Cosmides & Tooby, 1992; Shackelford & Buss, 1996; Trivers) .
These behavioral trends were also validated in human societies by economists with game theory. If the two individuals could not trust each other and there were no standard in the social context, these individuals would choose not to cooperate and minimize the goodness of the group. That was the famous Prisoner’s dilemma game (Poundstone, 1992). In order to solid and strengthen the reciprocal helping or cooperation, the game context should be repeated, so that participants could anticipate there were be a feedback (cooperation continue) in next game. However, only repeated the game could not maintain participants’ corporative behavior; in fact it could even decrease the reciprocal helping times in Public Goods Game and Trust Game which took part of participants’ own property in first game and got return until next game. In these games, participants had to endure the risk of not getting the money back and being taken by partners. Therefore, there must be some standards to restrict the behaviors of individuals. In the revised version of iterated Public Goods Game, participants could pay some cost to punish the free rider. Surprisingly, almost all the participants would pay the cost, and the reciprocal corporation could exist continually (Moll & Schulkin, 2009). Therefore, the reciprocal altruism could be developed if the context fulfilled the there wewewewewewewewerererererererere s s s s somsssoooooomo e to rererererererer memememememememembmbmbmbmbmbmbmberererererererere a a a a a andndndndndndnd dd d by thhhhhhhhememememememememe .. . . .. .. SeSeSeSeSeSeSeSecocococococococonndnnnnn , at the helpl er could
requests, and individuals could evaluate the skills of recognizing and remembering.
Some evolutionary biologists also suggested learning social norms from group members was an adaptive behavior of individuals. Many social norms and regulations were benefit to survival for individuals and groups, thus individuals who learned these rules could have fitness for survival. Further, being altruistic and helping reciprocally were the social norms which individuals must learn (Hoffman, 1981; Simon, 1990). As a philosopher, Singer also claimed every society consisted behavioral disciplines to restrict and guide individuals, so ethics were formed naturally in human society progress. Altruism was an inherent characteristic of human as a social creature (Singer, 2011).
Despite all the statements toward reciprocal altruism, these were not quite so competent for describing the prosocial behavior in medical professions because when medical professionals helped patients, they did not often expect the return from patients.
In fact, it was prohibited receiving extra gifts from their clients in medicine ethics.
According to above evolutionary theories, prosocial behavior seemed to be developed to enhance benefits and fitness of individuals or to maximize the advantage of the species group. Therefore, prosocial behavior should be based on self-concerned or so-called egoistic. Some psychologists and scientists expended this view, incorporated some economical hypothesis such as marginal utility and supply-and-demand relationship, and form the social exchange theory. They claimed that human behavior was built on reward pursuing and cost preventing. Individuals rationally chose the most reword, avoided punishment and minimized expends. The reword and punishment not only included physical materials but also contained psychological needs like love, satisfactions, self-esteem, and preventing negative feelings (Homans, 1961; John W Thibaut & Harold H Kelley, 1959). Speaking of
rememmmmmmbebebebebebeberieririririririringngngngngngngng. .... normmmmmmmms sss frfrfrfrfrfrfrfromomomomomomomom g g g g g g grogrrorororororoupupupupupupupup ms andndndndndndndndd r r r r r r r regegegegegegegegululululululululatatatatatatatatioioioioioioioions who learned these
helping, there were several advantages when individual presented prosocial trait. First, previous studies revealed prosocial behaviors could raise happiness and live healthier life of helpers, such as donors and volunteers (Dunn, Aknin, & Norton, 2008; Haidt, 2006; Post, 2009). Dunn et al. (2008) found that when sent money to participants and manipulated the way they spend money, participants who used the money on others would have higher score in happiness index than participants who spent money on themselves. Further, Moll et al. (2006) revealed that when participants made charitable donation, the mesolimbic reward system was activated, which area was highly correlated with getting monetary rewards. Besides, medial orbitofrontal–subgenual and lateral orbitofrontal areas also activated, which was important to social attachment. This similar result was also supported by James K. Rilling et al. (2002). They found nucleus accumbens, the caudate nucleus, ventromedial frontal/orbitofrontal cortex, and rostral anterior cingulate cortex which were correlated to reward processing were also engaged in reciprocal altruistic behaviors. These studies suggested that because helping others could make actioner happy, they would maintain prosocial behavior to enhance these social rewards such as establishing good image, health and wellbeing. Second, reciprocity also could be another motivation for individuals to perform prosocial behaviors. As mentioned above, human helped others might motivate by anticipating the receivers paying back whenever they were in need, although the rewards might not be received immediately. Third, prosocial behavior could be occurred to avoid negative results of not helping. For example, people would help victims to reduce sadness, social pain and to prevent guilty (Eisenberg & Fabes, 1991; Masten, Morelli, & Eisenberger, 2011). Fourth, helpers could also earn some social rewards such as social pronunciation and status. This motivation also had some supporting evidence in evolution which suggested that if an individual performed high cost altruistic behavior, which meant the
rosocialalalalalalal t tttttttrarararararararaitititititititit. . FiFFiFiFiFiFiFirst, and d dd dd d dd lililililiveveveveveveveve h h h h h hhheaeaeaeaeaeaeaeaaltltltltltltltlthihhhhhhererererererer orton, 222222222000000000000000088888888;;;;;;;; HaHaHaHaHaHaHaHaididididididididt, to participants and
individual had more abilities and survival advantages. Therefore prosocial behaviors might be an adaption indicator in sexual selection which could make the individual more attractive to opposites.
Hanson (1991) also adopted evolutionary theory and this social exchange view into medicine. He claimed that in hunter-gatherer stage, our ancestors took care about sick or injured associates in order to get more allies, gain more prestige, and expect to receive more aids when they encountered crisis or got injured. The reciprocity and better social status could make prosocial care and medical-related concern altruism (he did not mean the truly altruistic behaviors in this thesis) occurred in human society.
Along with all the advantages of prosocial behaviors, the cost of helping and self-sacrifice also came. Individuals had to weigh up the gains and losses then made the best decision. Hence supporters of social exchange theory claimed human would only help others when they thought it was good to them, and there was no purely other-oriented altruistic behavior.
Although self-centered prosocial behaviors seemed to explain almost all the helping behaviors in daily lives, it still could not explain some self-sacrifice and life-serving behaviors; for example, there have been countless heroes who sacrificed their life to rescue their countries and tried to make better future for their people in every cultural history. We can still see numberless suicide bombers attack to realize their ideals for protecting their own countries. Further, it was not the value to encourage medical professionals to help their patients by balancing the pro and cons first. We do not expect medical students to be hesitated helping only because they think it is not worthy for themselves. Therefore, is there exist truly pure altruistic behavior? Do human help others only because of themselves?
rosocialalalalalaaa b b b b bbbbehehehehehehehehavhavavavavavaavavioiiiiii rs ake tttttttheheheheheeee i i i i iiiindndndndndndndndivivivivivivivivvididididididididuaual aaaaall
exchange view into
1.2.2 Empathy-altruism Hypothesis
Opposite to the view of a more self-centered motivation underlying prosocial behaviors, some researchers propose that there are helping behaviors, or so-called altruistic behaviors, without any self-centered motivations. In this view, it is possible for people to help others or even sacrifice their benefits simply because they want to enhance others’ wellbeing. The empathy-altruism hypothesis proposed by Toi and Batson (1982) was one example. They suggested that altruism is a natural behavior that focuses on other individuals, and empathy is an intrinsic emotional response enabling people to understand other individuals’ psychological experience.
According to this hypothesis, altruistic behaviors occur due to emotional sharing with other individuals. To test their hypothesis, Toi and Batson developed a social psychological experiment which let participants (college students in general psychology) hear a piece of record from a victim who broke her legs from a serious traffic accident and could not attend to class. Participants were requited to use different views (high empathy vs. low empathy) to listen to the record. Immediately after participants listened to the record, the experimenter would ask participants whether they were willing to meet the victim and share their class notes with her. In addition, there were two types of cost conditions. In the high cost condition, participants learned that the victim would come back to the class and join them, however, she would be unable to keep up with other classmates. In other words, if participants chose not to help her, they would have to bear the guiltiness for rejecting to provide help whenever they saw the girl. In the low cost condition, participants would be told that the victim would not join the class at this semester. The results showed that in the low empathy condition, participants would have lower helping rate when they did not have to meet the victim again. Contrarily, in the high empathy condition, participants tended to show higher
de
d rllllllllyiyiyiyiyiyiyiyingngngngngngngng p p ppppppprorororororororor sosososososososociciciciciciciciaaalaalaala viors, ororororororororo s s s s s s ssso-o-o-o-o-o-o-o-cacacacacacacacalllllllllllllllledd
helping rate both in the high and low cost situation. These results suggested that when people could not have empathy with the needy, their prosocial behaviors would be determined by the cost-and-earns evaluation. Human decided whether to help or not according self-oriented social exchange theory. However, if human felt empathetic toward the pain of others, their altruistic behaviors have nothing to do with personal benefits or costs. Their findings thus suggest the view that altruistic behaviors can be non-self-centered (Batson et al., 1988; Batson & Shaw, 1991; C. Daniel Batson et al., 1991; Toi & Batson, 1982; but see Robert B. Cialdini et al., 1987).
. Further, some studies also revealed that when people encountered social exclusion by the group they cared about, they would do less charity donate, join volunteers or helping others. That meant the participants would repress their emotion or sad feelings to outward events to prevent the social pain caused by being rejected. Therefore, they could not have deep empathy to the needy person and adopted other-oriented view so their prosocial behavior trait would be lower (DeWall & Baumeister, 2006; Twenge, Baumeister, DeWall, Ciarocco, & Bartels, 2007).
McGaghie et al. (2002) also built up a model of altruism based on compassion within health promoted professions. They argued that altruism was a kind of explicit behaviors which was motivated by individuals’ inner companionate core. The companionate core was composed of human inner resources such as cognitive abilities, emotions, moral belief and awareness of self and others. This core would interact with life experiences which they called ‘accumulated wisdom’. The two levels of personal characteristics combined formed the basis of altruistic attitude toward outer world.
Hence there were continuous interactions between the companionate core and the external-situational world which the inner empathy drove altruistic behaviors, and the behavioral reinforcement would enhance the companionate core and increase the
uggesteeeeeeed dddddddththththththththatatatatatatatat w w w w w whewwwhhhhh n ehaviviviviviviviviororororrrrss ssss s s wowowowowowowowoululululululululud d d dd d dd bebebebebebbebe her to oooooo hehehehehehehehelplplplplplplplp o o o o o o o or r r r r r r r nnnonnnn t an felt empathetic
motivation for future helping behaviors. McGaghie claimed this was the reason medical professionals maintain their compassion and altruistic behaviors. This hypothesis was also supported by some philosophical base that sympathy could establish the best clinical relations and provide both patients and physicians by maintaining their authenticity in health caring professions (Bardes, 2006). However, promoting altruism within medicine also confronted some opposite opinions due to the following reasons: 1.
The definition of altruism in medicine field was still obscure, and it was impossible to evaluate the empathy trait of medical students and professionals due to the difficulty to determine their motivation was truly other-interested. 2. It was unrealistic to promote altruism in medical career because medical professionals would repressed their empathy during medical practice training when medical students faced increasing work loading and turned their attitude to more technological-oriented acknowledgements to avoid burnout and self-protected (Bishop & Rees, 2007; Burks & Kobus, 2012).
To summarize previous theories and hypothesis of helping behaviors, it seemed to be still unclear what the mechanism of medical professionals’ prosocial behaviors.
Although medical professionals were required to be altruistic, what motivated medical caregivers dedicate their life to health promotion and maintain their prosocial behaviors in this career? Is that purely self-serving? Or they helped patients other-oriented and motivate by their affective toward patients and their empathy according to empathy-altruism hypothesis?
1.3 The Definition of Empathy
In order to investigate the relationship between empathy and prosocial behaviors in medicine, the definition of the term of empathy must be clarified. Empathy is a multi-dimensional concept whose meaning varied with different people and various the reaaaaaaasososososososononnnnnn n memememememememediedididididididical his hhhhhhhhhypypypypypyypypotototototototothehehehehehehehesisisisisisisisiiss s ss sss wawawawawawawwass sssss establblblblblblbllisisisisisisisisi hhh h h h h ththththththththe e e eee ee bebebebebebebebest maintaining their
cultures. Empathy mainly occurs when an actioner takes measures to understand the others’ feelings, situations and perspective, image the time of others, and see the inner experience of its’ passage (Charon, 2001). Some previous studies suggested that empathy could be divided into two parts: cognitive empathy and affective empathy.
Cognitive empathy refers to the ability to recognize a context from another person’s perspective in order to identify the person’s experience, thoughts and feeling at that time.
And affective empathy was termed as the ability physically and mentally shares another person’s emotional state and induce similar emotion reactions (Fields et al., 2011;
Hemmerdinger, Stoddart, & Lilford, 2007; Konrath, O'Brien, & Hsing, 2011). Moreover, some researchers subdivided the concept of empathy into multiple mental processing levels; for example, Davis (1980) suggested there were four sub items in empathy which were Empathetic Concern: the feelings aroused from others’ difficulty, Perspective Taking: to cognitively and more rationally understand others’ situations and perspectives, Fantasy: the tendency to imagine the fictional stories and novels, and Personal distress: the distress when oneself saw the misfortune of others. Lately, Decety & Lamm proposed a social cognitive model of empathy to describe the mechanism underlying how empathy is invoked and modulated (Decety & Lamm, 2006). The model includes two levels of processing: 1. a bottom-up processing that involves with implicit and autonomic behaviors or emotional sharing invoked by simply observing another individual’s behavior, and 2. a top-down processing that involves with perspective-taking and emotional regulation. They further pointed out that the interaction of the two processing affect the development of empathy in that the bottom-up processing continuously renews external information and the top-down processing regulates induced emotion (Cacioppo & Berntson, 1992; Stroop, 1935).
Previous studies of medicine often focused on cognitive empathy and perspective taking to undddddddderererererererrststststststststanananananananandnddddddddddd the , anddddddddd s s ssseeeeeeeeeeeeeeee ttttttthehehehehehehehee i i i i i iiinnnnnnnnnnnnn ererererererer es suuuuuuggggggggggggggggg esesesesesesesesteteteteteteteted d d d d dd d ththththththththat affective empathy
aspect. Therefore, in traditional view, empathy could promote medical professionals to understand patients’ needs. However, this view would easily neglect the other aspect of empathy, affective empathy or empathetic concern, might have some bad impact on emotional distress and fatigue of medical workers (Chen, Lew, Hershman, & Orlander, 2007; Fu & Chen, 2011; Neumann et al., 2011). Further, the drawback of personal distress seemed not to be avoided when empathy occurred at a certain level (Eisenberg, Shea, Carlo, & Knight, 1991). Therefore, empathy should be discussed with affective concern in medical field. de Vignemont and Singer (2006) gave a clear description of empathy which empathy occurred when an actioner had a similar affective state of others when they imagined or noticed other’s affective state. And the actioner would know their emotional state was caused by the feelings of another person. In current research, we corporate the definitions mentioned above and form the term as: ‘an ability to recognize another person’s mental, and emotional states from the person’s perspective, which induce an isomorphic affective experience as the person’ (Cacioppo
& Berntson, 1992; de Vignemont & Singer, 2006; Stroop, 1935).
1.4 Empathy in Healthcare Profession
Empathy is no doubt one of the most important central values for healthcare professionals (Bardes, 2006; Bishop & Rees, 2007; Norman, 2007; Shapiro, 2008). It can not only help establish a better patient-physician relationship, but also create the broader connections with the community. This good relationship would improve patients’ adherence, treatment compliance and enhance satisfaction with medical services (Burks & Kobus, 2012; Hall, Epstein, DeCiantis, & McNeil, 1993; M Robin DiMatteo et al., 1993; McGaghie et al., 2002; Ong, Dehae, Hoos, & Lammes, 1995).
Empathy may also help encourage patients to be more willing to report their symptoms cal proffffffffesesesesesessisssisisisisisisiononononononononalalaalalalalalals ssssss to the ototootototooheheheheheheher er r rr r rrasasasasasasaspespepepepepepepep ctcctctctcctct oooooooff ffffff me baaaaaaaadd dd d d d dd imimimimimimimimpapapapapapapapactctctctctctctct ooon hman & Orlander
in details, which would increase the accuracy of diagnosis (Chen et al., 2007;
Hemmerdinger et al., 2007; Neumann et al., 2011). Furthermore, a better communication between patients and medical professionals could even reduce the severity of symptoms and decrease blood pressure, blood glucose levels or anxiety levels of patients (Griffin et al., 2004; Neumann et al., 2007; M. A. Stewart, 1995; M.
Stewart et al., 2000).
Compared to physicians, therapists (e.g., clinical psychologists, physical therapists, occupational therapists, speech therapists) usually have longer and more frequent contact with patients or clients. For example, stroke patients in average spend half to one hour per day in their acute stage and at least one hour per week in their sub-acute or chronic stage in a rehab clinic with occupational therapist. In addition, empathy has been an essential core for healthcare professionals to apply ‘client-centered’ approaches in daily practices (Brown et al., 2010; Dalia Sachs, 1994; McAuliffe & Barnett, 2009;
McKenna, Adri-Anne Scholtes, Fleming, & Gilbert, 2001; Norman, 2007; Stachura &
Garven, 2007).
Although empathy is an important focus in the education of healthcare professions, several studies show that the levels of empathy of medical students declined as their medical education years increases. The declination is even more prominent when they are in their senior grades and start their clinical training (Bardes, 2006; Chen et al., 2007;
Neumann et al., 2011; Williams et al., 2012). Additional evidence also shows that medical students may not have more empathy than other students, and their empathy even decays when they contact clinical patients (Au & Man, 2006; Brown et al., 2010;
McAuliffe & Barnett, 2009; Stachura & Garven, 2007). Surprisingly, one cross-campus study even reported that business students show greater altruistic attitudes than medical and law students, suggesting that medical students do not necessarily
hen et t tt t tt alalalalalalalal.,,, 2 2222222200000000000 7;
hermmmmmmmoororooroo e,e,ee,e,e,e,e, a a a a a a ba b b bebbbbeteteeetetetteeeeeeerr rrrrr d even nnnnnnn rerererererereredudududududududucececececececece t t thettttthhhhhhh
levels or anxiety
exhibit more altruistic behavior than other students (Coulter et al., 2007).
In contrast, the declination trend of empathy in students of occupational therapy does not appear to be significant (Brown et al., 2010). The results, however, remain inconclusive in that the survey used in the study was designed for physicians (Jefferson Scale of Physician Empathy (JSPE)) and may not be suitable for evaluating empathy traits of occupational therapy students (Brown et al., 2010). Data from senior students, who were in their clinical training year, were also missing, which minimize the interpretation power of the study. Furthermore, like most studies, they used self-report assessments, which lack reliability and validity and could show social expectation bias effect (Fields et al., 2011; Hemmerdinger et al., 2007). . Previous research also suggested that these questionnaires have not enough sensitivity to detect the difference between individuals and could only be used as a screening tool to identify the low empathy one (Hemmerdinger et al., 2007). Hence, it is essential to use an indirect approach to assess students’ empathy with reduced interference from social expectation bias effect.
Several reasons could explain the declination of empathy observed in medical students: distress from heavy workload, sleep deprivation, poor interaction with patients and feeling of helplessness with difficult medical situations (Chen et al., 2007;
Maudsley, Williams, & Taylor, 2010; Neumann et al., 2011). Surprisingly, despite health caregivers trained to be promote health , there were high rates of psychiatric morbidity and stress within medical professions (Firth-Cozens & Payne, 1999; Wall et al., 1997). Further, when medical students faced with clinical reality such as painful illness and death, they might decrease their feelings toward patients to avoid emotional distress, protect themselves and tried to be more rational on their duties (Chen et al., 2007; Hojat et al., 2004). A recent ERP study investigated physicians’ response to
07).
cupatataatatatatatioioioioiooonanananananananall ll llll ththththththththhererererererererapapapapapapppyy yyyyy , howwwwwwwweveveveveveveveve erererererererer, rerererererereremamammamammamain ysicians (J( efferson
pictures representing body parts in contact with painful or non-painful objects, and demonstrated that, compared to the control group, physicians seemed to suppress their emotional reaction through early affective processing when they saw others in pain (Decety, Yang, & Cheng, 2010). Therefore, the observed common declination of empathy in physicians could be an emotional regulation mechanism to keep them away from work-related distress, burnout or fatigue and help them make rational clinical decisions. It is possible that empathy decline is a necessary and normal process to adjust to the clinical reality and medical surroundings when medical professionals pass through medical practice training. According to these findings, there seems to be some discrepancies between empathy regulation and helping behavior in healthcare professionals.
1.5 Aims of Current Research
Although several factors have been assumed to explain the declination of empathy in healthcare professionals, very few studies can provide the evidence that supports these assumptions. In terms of empathy evaluation, previous research also suffered from robust vulnerability to response bias due to the nature of explicit measurement by empathy questionnaires (Fields et al., 2011; Hemmerdinger et al., 2007). Furthermore, most of previous research focused only on the empathy declination, the relationship between empathy level and prosocial behavior patterns in healthcare professionals remains unclear. Therefore, there are two aims for the current research:
1. To develop experimental paradigms to implicitly evaluate both the level of empathy and prosocial behavior patterns.
2. To investigate the chronological change of the relationship between empathy levels and prosocial behavior patterns in healthcare professionals.
ainful obobobobobobobobjejejejejejejejectctctctctctctcts,s,s,s,s,s,s,s, a a aaaaaandd d tooooooo s s ssupupupupupupupprpprprprprprprpresesesesesesess ss s sss ss s thtththththththeeeiriririririirir
aw ototottttttheheheheheheheheh rsrsrsrsrsrsrsrs in iiiiiiin n nnnn papapapapapapapain mon decliination of
2. General Methods
2.1 Apparatus
A Win XP PC with Matlab installed and a 21” CRT monitor of up to 100 Hz were needed to present experimental paradigms and collecting behavioral data. All experiment scripts were written in Matlab using the Psychophysics Toolbox extensions (Brainard, 1997; Kleiner, Brainard, & Pelli, 2007; Pelli, 1997)
2.2 Participants
Table 1
Demographic Data
Gender portion (Female/ male)
Age (y/o)
Formal education year
Professional training year
Seniority
Professional
controls 19 / 11 27.27± 3.39 16.83± 1.80 4.60± 1.22 3.15± 1.97
Occupational
therapists 20 / 10 27.63± 4.30 16.23± .553 4.33±.71 4.37± 3.27
t - -0.367 1.74 1.03 -1.75
p - 0.715 0.087 0.305 0.086
Occupational
freshmen 22 / 8 18.73± .79 12.03± .183 0 0
Freshmen
controls 23 / 7 18.47± .51 12.00± .000 0 0
t - 1.56 1 - -
p - 0.124 0.321 - -
We recruited 120 healthy volunteers to participate the current study. Since it is important to conceal the true purpose of the present experiments before participants finish all tasks, all participants signed one informed consent before the start of experiments and signed another form which revealed true experimental aims after they completed the experiments. The experimental protocol was approved by Research Ethic Committee at National Taiwan University (201209HS004).
All participants were categorized as one of the following four groups with 30 participants for each group:
Naive Occupational Therapy students: 30 freshmen in the school of occupational therapy at National Taiwan University. (22 female, mean age ± S.D. = 18.7 ± 0.8 y/o).
Naive control students: 30 freshmen who do not major in healthcare or social work related undergraduate program at National Taiwan University (23 female, mean age ± S.D. = 18.5 ± 0.5).
Senior Occupational Therapists: 30 registered occupational therapists who have worked full-time for more than 2 years in Taiwan (19 female, mean age ± S.D. = 27.3 ± 3.4).
Senior professional controls: 30 adult participants who have a full-time job in other professions, excluding anything related to health care or social work, for more than 2 years in Taiwan (20 female, mean age ± S.D. = 27.6 ± 4.2).
Since the proportion of male occupational therapists and occupational students generally lies between 1/3 to 1/4, we tried to recruit similar gender proportion of participants for each group (Sylvia R Cruess & Cruess, 1997). The demographic information of all participants was listed in Table 1.
studydydydydydydydy. .. S S S S SinSSSininininininncecececececececec i i i i i i it tttt isisisisisiisis before eeeeee papapapapapapapartrtrtrtrtrtrtrticicicicicicicicipipipipipipipanpanaaanananants efore the start of
2.3 Experiment 1: Implicit Evaluation for Levels of Empathy Using Emotional Stroop Paradigm
The levels of empathy was traditionally evaluated by administering psychometric questionnaires such as Jefferson scale of physician empathy, Empathy quotient, Davis' interpersonal reactivity index, Empathy construct rating scale. However, it was not rare to observe response biases favoring empathetic decisions resulting from social expectation effect (i.e., people tend to respond in terms of what a society expect an empathetic person would do) (Neumann et al., 2011). To downgrade the interference from social expectation effect, we used a novel version of emotional Stroop paradigm to implicitly evaluate participants’ level of empathy. The traditional Stroop paradigm required participants to selectively respond to a given feature (e.g., colors) of stimuli (e.g., colored words of “colors”) while suppressing the distraction from another feature of the same stimuli (e.g., the semantic meaning of words) (Stroop, 1935). The Stroop effect occurs as participants respond with longer reaction times (RT) and prone to report more errors when the two features of a stimulus are incongruent (e.g., a “Red” written in green color) than when the two features are congruent (e.g., a “Red” written in red color). The size of the effect, usually measured as the RT difference between congruent vs. incongruent trials, represents the degrees of interference from distracting features.
The Emotional Stroop, modified from the traditional Stroop paradigm, combines emotional words and emotional facial expression pictures to create an emotional interference (see Figure 1) (Haas, Omura, Constable, & Canli, 2006; Hofelich &
Preston, 2012; Hu, Liu, Weng, & Northoff, 2012; Monk et al., 2003; Preston &
Hofelich, 2012; Preston & Stansfield, 2008) and the Emotional Stroop effect occurs
r r
r L L L L L L L L L L L L L L L L L L L Le e e e e e e e e e e e e e e e e e e e ev v v v v v v v v v v v v v v ve e e e e e e e el l l l l l l l l l l ls s s s s s s s s s s s s o o o o o o o o o o o o o o o o o o o o of f f f f f f f f f f f f f g
g g g g g g g g g g g gm m m m m m m m m m m m m m m m m m m
ering psychommeterirc
when the valence of the words is incongruent with the valence of the facial expression.
The intensity of the emotional interference is therefore measured by the RT differences between congruent and incongruent trials. The paradigm appears to be an efficient behavioral probe for implicitly evaluating emotional responses. For example, patients with major depressive disorder suffered greater interference from negative words than positive words in Emotional Stroop (Hu et al., 2012).
In the current experiment, we aimed to use the Emotional Stroop paradigm to implicitly evaluate participants’ empathizing capability. Specifically, we compared the Emotional Stroop Effect under three different contexts of empathy: Empathy Induction (see Figure 2), Cognitive Interference (see Figure 3), and Neutral Viewing conditions (see Figure 4). In the Empathy Induction (EI) condition, participants were required to look at a picture and made efforts to empathize the emotional contents in the picture before performing the Emotional Stroop tasks (see Figure 2). If a participant possesses a higher level of empathy, the picture will presumably induce higher emotional valence and subsequently amplify the emotional interference effects (i.e., larger RT differences between incongruent trials vs. congruent trials). In order to further investigate if there is any difference of modulation effects between medical and non-medical empathy contexts, the emotional content pictures were separated into non-medical contexts and medical contexts during analyses. The Cognitive Interference condition (CI) served as an empathy baseline condition in which we aimed to suppress top-down empathizing processing by introducing an additional working memory task (see Figure 3). Accordingly, the Emotional Stroop effect contrast between the EI and CI presumably reflects the modulation of empathy upon Emotional Stroop effects. It is possible that the Emotional Stroop effect in both EI and CI conditions, if any, could result from some bottom-up emotional responses by simply e facial l l l ll exexexexexexexxprprprprprprprpresesesesesesesessissisisissisision.
the RRRRRRRRT T T T T T Tdidididididididiffffffffffffffffererererererererrenenenenenenenenceeeeeees ssssss to be eeeee anananananananan e e e eeeeefffffffffffffffficicicicicicicicieieieieieieieient r example patients
viewing emotional contents. Therefore, the Neutral Viewing (NU) condition further served as a general emotion baseline measurement in which emotional pictures were replaced by non-meaningful pixel-shuffled pictures from the same set of pictures used in the EI condition (see Figure 4).
Figure 1
Three stimulus examples in the Emotional Stroop Experiment.
Here we show three examples of emotional face-word pairs for the Emotional Stroop paradigm. Picture (a) represents a typical emotionally congruent trial (Con) in which the facial expression (happy) matches the double-character descriptions (happy). In contrast, picture (b) and (c) show two typical emotionally incongruent trial in which the facial expression does not match the double-character descriptions. Picture (b) shows happy-word-sad-face (PWSF) incongruent trial, and picture (c) shows sad-word-happy-face (NWHF) incongruent trial.
) condididididididititititititiionononononononon f f f f f furfffurururururuururthttttttt er onal l ll l l ll pipipipipipipictctctctctctctcturuururururururesesesesesesesess w w w w w w w werrrrrrre eeeeee et of pipipipipipipipiicctctctctctctcturururururururureseseseseseseses u u u uuuuussssessss d
Figure 2
The sequence of a typical trial for the Empathy Induction Condition.
Empathy Induction condition (EI): In this condition (Figure 2), participants were required to empathize the person’s situation of the emotional context from a given picture. Specifically, participants were instructed to imagine what they feel if they undergo the same emotional incident and also imagine how the incident may influence their life in the future. There were four emotional context categories with six pictures in each context. Each context category (i.e., an experiment block) started with a 4 sec context description followed by a 2 sec task instruction. Subsequently, 6 trials of emotional Stroop were presented. Each trial started with a 4 sec emotional context picture followed by a picture containing a pair of double-character word and an emotional facial expression with a 1 sec latency. The next trial would not start until participants made a response.
onnnnnnnnnn......
Figure 3
The sequence of a typical trial for the Cognitive Interference Condition.
Cognitive Interference condition (CI): In this condition (Figure 3), a working memory task was introduced to presumably prevent participants’ automatic empathizing processes, if any, induced by emotional context pictures. The working memory task required participants to remember an 8 digit number presented before the emotional context picture. Following the picture presentation, a pair of memory test numbers was presented and participants needed to indicate which number matches the content of their working memory. Note that the distracting number and the correct number differed from each other with only one digit, maintaining a reasonable load for working memory. After the memory test, participants performed the regular Emotional Stroop task.
di di di d d d d d d di d d di dtititttttitooonononoononooooooon.. .
Figure 4
The sequence of a typical trial for the Neutral Viewing Condition.
Neutral Viewing Condition (NU): In this condition (see Figure 4), participants were required to look at neutral pictures naturally without any extra effort as if they were sitting on the sofa, reading a magazine and coming across to these images (Rameson, Morelli, & Lieberman, 2011). For each trial, a pixel-shuffled picture was presented for 4 sec and was followed by a picture containing a pair of double-character word and an emotional facial expression with a 1 sec latency. The next trial would not start until participants made a response.
.
2.3.1 Procedures
2.3.1.1 Stimuli and Materials
The emotional context pictures were selected from the International Affective Picture System (IAPS) (Van Lange, 2008) and the picture repertoire used in a previous study (Rameson et al., 2011). All the pictures were subdivided into 16 sets according to their contexts and reevaluated subjective empathy valance, arousal level and emotional valance in our study. The facial expression pictures were selected from 12 (6 men and 6 female) actors in Taiwan emotional standard stimuli database (Farnand et al., 2009) . One happy face and one sad face expression were chosen form each actor.
The 12 double-character emotional words (ǵඍ৹ǵࢲΚǵݒ഻ǵ഻ǵזǵ ൿኌǵኁǵݪ഼ǵൿࠉǵधඊǵЈ) were drawn from the emotional standard Chinese phrase database developed by Lee et al (Lee & Lee, 2011). There were no significant differences between arousal level, concreteness, familiarity, frequency and stoke count in chosen words.
2.3.1.2 Tasks
Emotional Stroop
A typical trial of Emotional Stroop started with an emotional (or neutral) context picture presented for 4 sec. One second after the offset of the emotional context picture, a picture of a face paired with a double-character word was presented and last until participants made responses. The two characters were displayed at the cheek level so that they would not cover the eyes of faces. The face could be either a happy or a sad facial expression, and the double-character word could describe either a positive or a negative emotion. The combination of face-word pairs was
natioionan l Affeectivve
pseudorandomly presented in three different kinds of trial types: congruent (Con) (happy face with positive words or sad face with negative words), negative words with happy face incongruent (NWHF) and positive words with sad face incongruent (PWSF) trial types (see Figure 1) (Hofelich & Preston, 2012; Preston & Stansfield, 2008; Rameson et al., 2011). Participants were instructed to press one key for happy face and another key for sad face as soon and accurate as possible. After the response, there would be a feedback signal (500 ms) with a green square around the face picture for correct responses and a red square for incorrect responses. The Emotional Stroop effect was defined as longer reaction times for the incongruent trials than the congruent trials.
In the current experiment, participants performed emotional Stroop task under 5 different empathy contexts including neutral viewing condition, medical cognitive interference condition, medical empathy induction condition, non-medical cognitive interference condition and non-medical empathy induction condition. There were four blocks for each empathy context with each block contained six pictures belonging to a single emotional context. To prevent the emotional Stroop task of neutral viewing condition from interference by other EI and CI conditions, the neutral viewing condition was presented first and then the other 4 conditions would show in random order. For any medical condition, we used pictures with contexts that health care professionals might encounter in their daily works, such as “This person is suffering from a serious disease” or “This person's father was just taken to the hospital due to a serious accident”. On the other hand, for any non-medical condition, we used pictures with contexts that had nothing to do with health care, such as “This person just lost a career-changing sporting event” or “This person was just fired from a job they really need”. Participants were informed that all emotional context pictures were selected from newspaper, magazines,
congggggrururururururuuenenenenenenenentt tttttt (C(C(C(C(C((C(C(Conooooo ) egag titititititititivevevevevveve w w w wwwwworororororororo dsdsdsdsdsdsdsdsds wwwwwwwwitttttttthh hhhhhhh
face iiiiiiiiincncncncncncncnconononononononongrgrgrgrgrgrgrgrueueueueuueueuent ston & StSansfield