Article in Experimental gerontology · March 2017 DOI: 10.1016/j.exger.2017.03.003 CITATIONS 10 READS 88 5 authors, including:
Some of the authors of this publication are also working on these related projects:
CRIS output - dementia and mental health of older adults View project
Integrating physical activity in low resourced mental health settings View project Brendon Stubbs
King's College London
456PUBLICATIONS 5,078CITATIONS
SEE PROFILE
Li- Jung Chen
National Taiwan University of Sport, Taiwan 68PUBLICATIONS 590CITATIONS
SEE PROFILE
Wen- Jung Sun
41PUBLICATIONS 324CITATIONS
SEE PROFILE
Po-Wen Ku
National Changhua University of Education 90PUBLICATIONS 687CITATIONS
future cognitive ability: A longitudinal study among community dwelling older adults
Brendon Stubbs, Li-Jung Chen, Chun-Yi Chang, Wen-Jung Sun, Po-Wen Ku
PII: S0531-5565(16)30296-0
DOI: doi:10.1016/j.exger.2017.03.003
Reference: EXG 10015
To appear in: Experimental Gerontology
Received date: 30 August 2016
Revised date: 24 February 2017
Accepted date: 2 March 2017
Please cite this article as: Brendon Stubbs, Li-Jung Chen, Chun-Yi Chang, Wen-Jung Sun, Po-Wen Ku , Accelerometer-assessed light physical activity is protective of future cognitive ability: A longitudinal study among community dwelling older adults. The address for the corresponding author was captured as affiliation for all authors. Please check if appropriate. Exg(2017), doi:10.1016/j.exger.2017.03.003
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
ACCEPTED MANUSCRIPT
Accelerometer-assessed light physical activity is protective of future cognitive ability:
A longitudinal study among community dwelling older adults
Brendon Stubbs, Li-Jung Chen, Chun-Yi Chang, Wen-Jung Sun*, Po-Wen Ku*
Running title: Accelerometer-assessed light physical Activity and cognitive impairment
Submission to Experimental Gerontology
1st author: Brendon Stubbs, PhD
Physiotherapy Department, South London and Maudsley NHS Foundation Trust, Denmark Hill, London SE5 8AZ, UK
Health Service and Population Research Department, Institute of Psychiatry, Psychology and Neuroscience, King's College London, De Crespigny Park, London, Box SE5 8AF, UK Faculty of Health, Social Care and Education, Anglia Ruskin University, Chelmsford, UK E-mail: [email protected]
2nd Author: Li-Jung Chen, PhD
Department of Exercise Health Science, National Taiwan University of Sport, Taiwan E-mail: [email protected]
3rd Author: Chun-Yi Chang, PhD
Department of Physical Education, National Hsinchu University of Education, Hsinchu, Taiwan
E-mail: [email protected]
4th and corresponding author: Wen-Jung Sun, MD, PhD
Family Medicine Department, Taipei City Hospital Zhongxing Branch, Taiwan E-mail: [email protected]
5th and corresponding Author: Po-Wen Ku, PhD (Epidemiology), PhD (Exercise & Health) Graduate Institute of Sports and Health, National Changhua University of Education, Taiwan Email: [email protected]
TEL: +886 4 7232105 ext. 1991 Fax: +886 4 7211155
ACCEPTED MANUSCRIPT
* Corresponding authorAbstract
Objective (246/250)
Physical activity (PA), especially moderate-to-vigorous intensity, could protect older adults
from cognitive impairment. However, most literature is based on self-reported PA which is
limited by recall bias. Light PA is popular among older adults, but a paucity of objective
longitudinal data has considered the relationship between light PA and cognitive ability. We
examined if a higher level of objectively measured light PA, independent of
moderate-to-vigorous physical activity (MVPA), was prospectively associated with better
cognitive ability in older adults.
Methods
A longitudinal study over 22.12 (±1.46) months including 274 community-dwelling older
adults across 14 regions in Taiwan was undertaken. Cognitive ability was obtained using a
Chinese version of the Ascertain Dementia 8-item Questionnaire (AD8) and light PA and
MVPA captured by 7 days accelerometer positioned on waist. Multivariable negative
ACCEPTED MANUSCRIPT
Results274 participants (74.52 years, 45.6% male) attended the follow-up (96.1%). Higher light PA,
independent from MVPA, was associated with a reduced rate of decline in cognitive ability
(rate ratio 0.75 [0.60-0.92]). MVPA, was also associated with a reduced decline in cognitive
ability (rate ratio 0.85 [0.75-0.95]). Light PA was protective of cognitive ability in
sensitivity analyses removing participants with activities of daily living difficulties,
depressive symptoms and cognitive impairment at baseline.
Conclusion
Our data suggest that light PA may offer a protective influence of future cognitive ability in
community dwelling older adults. The promotion of light PA may be a valuable means to
maintain cognitive ability in older age.
Key words: Cognitive decline, dementia, light physical activity, moderate to vigorous
ACCEPTED MANUSCRIPT
IntroductionDementia is a common neurodegenerative condition among older adults that typically leads to
a loss of independence, reduced quality of life, premature mortality, caregiver burden and
high levels of healthcare utilization and cost (Fiest et al. 2016; Prince et al. 2013). Given the
aging population, the total number of dementia cases will inevitably increase, and there are
pressing calls to prevent cognitive decline and ultimately dementia (Deckers et al. 2015).
Within the last twenty years there has been a rapid increase in interest for the potential of
physical activity to prevent cognitive decline and maintain good cognitive ability (Barnes and
Yaffe 2011; Deckers et al. 2015; Hamer and Chida 2009). Two recent systematic reviews
stipulated that physical activity is one of the top seven modifiable risk factors for cognitive
impairment in older age (Barnes and Yaffe 2011; Deckers et al. 2015). A recent
meta-analysis of longitudinal studies found that higher baseline levels of physical activity
were associated with a 14% reduced risk of future dementia (Relative risk (RR) 0.86, 95% CI
0.76-0.97) (Blondell et al. 2014). The authors (Blondell et al. 2014) only identified one
study capturing physical activity utilizing an objective measurement of physical activity
(Buchman et al. 2012), which found that higher total physical activity was independently associated with a reduced risk of Alzheimer’s disease over 4 years.
ACCEPTED MANUSCRIPT
of altered cognitive ability or cognitive impairment, is challenging. In fact, a recent
systematic review of psychometric and measurement properties of self-report physical activity
measures in older adults noted that most self-report measures have little evidence of any
validity and reliability (Falck et al. 2016). Whilst a small number of cross sectional studies
have investigated objective physical activity and cognition in older age (Doi et al. 2015;
Makizako et al. 2015), there remains a paucity of longitudinal studies investigating
objectively measured physical activity and cognitive impairment/ability. Another key
limitation in the literature is that international physical activity guidelines recommend that
older adults should do at least 150 minutes of moderate-intensity aerobic physical activity or
do at least 75 minutes of vigorous intensity aerobic physical activity throughout the week.
This appears to imply that little or no health benefits can be derived from light physical
activities (World Health Organization 2010). Light physical activity is a popular, relatively
safe and effective form of activity for older adults (Tse et al. 2015). Physical activity
conducted at moderate to vigorous intensity, whilst conferring potentially greater benefits
may also carry a greater risk of injury and potential dropout from exercise (Tse et al. 2015).
Thus, understanding if light intensity physical activity (e.g. casual walking, stretching, and
light yard/house work etc.), independent of moderate-to-vigorous physical activity (MVPA),
might offer protective effects on cognitive ability could provide clinically useful information.
ACCEPTED MANUSCRIPT
physical activity and cognitive abilities using objective devices, the current study examined
whether objectively measured light physical activity, independent of MVPA, is associated
with a reduced risk of decline in cognitive ability in older adults. To test for confounding and
reverse causation, sensitivity analyses were also conducted.
Methods
Study design and sample
The current longitudinal study utilized data from two-waves of a community-based
project conducted in Hunei District, Kaohsiung, which is the second largest city in Taiwan. In
total, 285 community-dwelling older adults who were aged 65 years or older were recruited
and assessed from August to October 2012. Participants were recruited from 14 village
regions, with approximately 20 people being recruited from each community center utilizing
quota sampling in which, participants were drawn based on a national distribution according
to sex and age in 2011 (Taiwan Ministry of Interior 2012). Follow up interviews were
conducted between May to July 2014. From the baseline sample, 274 participants (96.1%)
attended the follow-up after a mean of 22.12 ± 1.46 months. The reasons why participants (n=
11) did not attend the assessment of the second wave included: Inpatient (n= 2), not traceable
(n= 2), deceased cases (n = 4) and refuse to attend (n= 3).
ACCEPTED MANUSCRIPT
ethical approval from National Taiwan University of Sport Institutional Review Board,
Taiwan. All data was collected using a standardized interview format, conducted with
face-to-face interviews at each person’s house.
Measures
Cognitive ability
Cognitive ability was obtained using a Chinese version of the Ascertain Dementia 8-item
Questionnaire (AD8) by participants with a potential range between 0 and 8 (Galvin et al.
2005; Galvin et al. 2007). The AD8 comprises 8 items that ask the respondents to rate
change in memory, problem-solving abilities, orientation, and daily activities (yes=1, no=0).
Higher scores represent cognitive ability decline (Galvin et al. 2005; Ganguli et al. 2014).
The Chinese version of the AD8 has demonstrated adequate reliability and validity among
community-dwelling older Taiwanese adults (Yang et al. 2011). Within the current study,
the Cronbach’s alpha reliability coefficients for the AD8 ranged between 0.79 (first-wave)
and 0.81 (second-wave) across the two waves of data collection.
Objective physical activity
Physical activity were captured using waist worn triaxial accelerometer monitors
(GT3X+, ActiGraph, Pensacola, FL, USA) for 7 days. In order to be included in the study,
participants had to wear the accelerometer for a minimum of 10 hours of monitoring on at
ACCEPTED MANUSCRIPT
software (ActiGraph, Pensacola, FL, USA). Periods of 60 min of consecutive zero counts
were considered as non-wearing time and were excluded from the analyses. Physical activity
parameters were then computed using established cut offs, comprising time spent in light
physical activity (100–1951 counts/min), and moderate-to-vigorous activity (>1951
counts/min) (Gorman et al. 2014), together with total physical activity energy expenditure
(kcal/week). Research evidence has demonstrated that there is a strong correlation between
the indirect calorimetry estimates of energy expenditure and energy expenditure (kcal)
assessed by GT3X+ (r = 0.82) (McMinn et al. 2013). For descriptive purposes, the various
physical activity categories were converted into tertiles, but the primary analyses were
conducted on continuously distributed variables.
Covariates
A number of covariates were collected at baseline in line with previous literature (Coley
et al. 2008; Hamer and Chida 2009): including (i) socio-demographic factors: sex, age (65-74
years, 75+ years), educational attainment (no formal schooling, primary school, secondary
school+), marital status (married/cohabitating, others), main source of income (from offspring
vs. self [e.g. pension/savings]); (ii) lifestyle behaviors: smoking status (current, never, or
former smokers), alcohol consumption (yes vs. no), and; (iii) health status: body mass index
(BMI) (<18.50, 18.50-23.99, 24-26.99, 27+),(Taiwan Department of Health 2003) number of
ACCEPTED MANUSCRIPT
cancer, chronic obstructive pulmonary disease (COPD), liver disease, renal disease, and
arthritis; difficulties with activities of daily living (ADLs, no difficulties at all vs. some or
great difficulties); depressive symptoms assessed by the 15-item Geriatric Depression Scale
(GDS) using cutoff of 5 (no vs. yes), (Brink et al. 1982; Yesavage and Sheikh 1986); mean
daily accelerometer wear time (Hamer et al. 2014), and baseline AD8 scores.
Data analysis
Descriptive statistics were used to describe the features of the study sample. Given the
violation of normality, Mann Whitney U tests and Kruskal-Wallis tests were adopted to check
for differences in cognitive ability in 2014 across levels of accelerometer-derived parameters
(all in tertiles), and covariates. Previous research indicated that the use of the conventional
level (p-value = 0.05) may fail to identify variables known to be important. Variables with a p
value less than 0.25 were included in the subsequent regression models for adjustment
(Hosmer et al. 2013).
To examine the bi-correlations between objectively assessed physical activity parameters
and subsequent cognitive ability after controlling for accelerometer wear time, partial
correlation coefficients between physical activity energy expenditure (kcal/week as a
continuous variable), time (hours/day as a continuous variable) spent in physical activity at
ACCEPTED MANUSCRIPT
Multivariable negative binomial regression was conducted because the outcome variable
was an over-dispersed count with a highly skewed distribution. All accelerometer-derived
physical activity parameters were log-transformed before conducting regression analyses due
to non-normality (Tudor-Locke et al. 2011). Two separate unadjusted regression models
(single-factor models) for light and moderate-to-vigorous activity were conducted to assess
the associations between each intensity categories and cognitive ability. Then, two separate
multivariable regression models (single-factor models) for light and moderate-to-vigorous
activity (without mutual adjustment) were conducted to assess the associations between each
intensity categories and cognitive ability after adjusting for baseline cognitive ability, wear
time of accelerometer, socio-demographic variables, lifestyle behaviors, and chronic
conditions. Finally, one multivariable regression model (a two-factor model) for light
activity was fitted to examine the relationships in more detail after adjusting for MVPA and
other covariates.
Sensitivity analyses were carried out to evaluate confounding and reverse causation. In
first stage, we considered the possibility that ADL difficulties might influence physical
activity behaviors at baseline and subsequent cognitive ability, so the negative binomial
regressions were repeated after excluding the 13 participants with impaired ADLs. At the
second stage, we mitigated the potential impact of depressive symptoms on physical activity
ACCEPTED MANUSCRIPT
(Guo et al. 1988). At the third stage, participants with suspected mild cognitive ability or
dementia (i.e. AD8 scores equal or greater than 2) at baseline (n=65) which may have been
not only associated with baseline physical inactivity and subsequent health conditions but also
associated with the accuracy of survey responses. Sensitivity analysis was conducted
excluding those with suspected mild cognitive impairment or dementia at baseline.
All analyses were conducted using IBM SPSS 20.0 software and a p value < 0.05 was
considered statistically significant.
Results
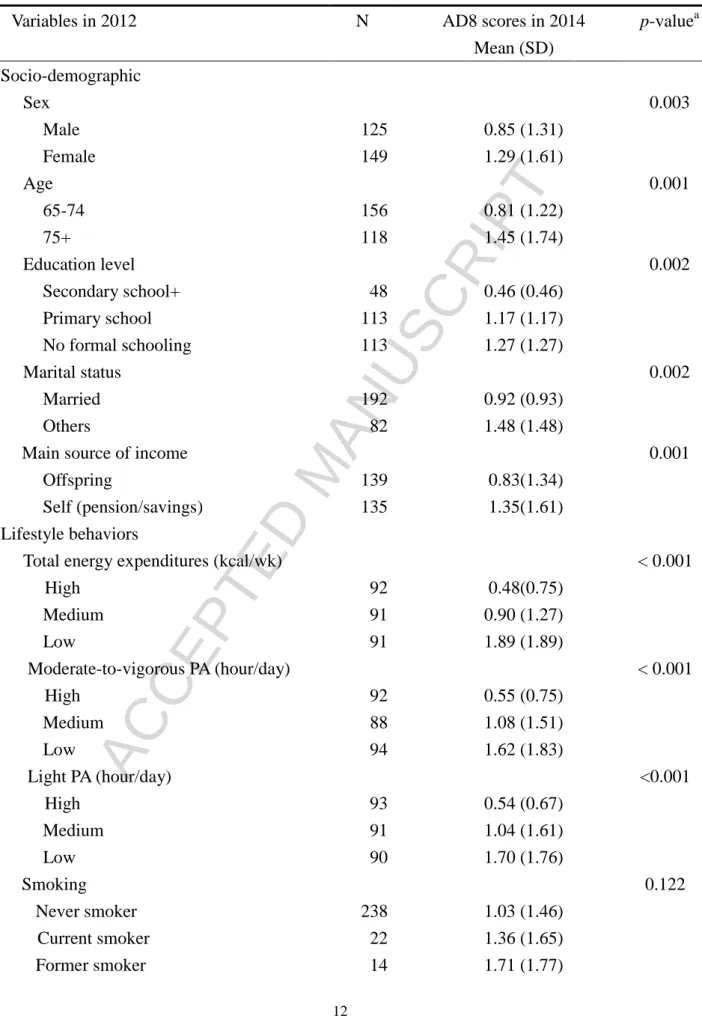
Full details of the sample with follow up data are presented alongside AD8 cognition scores
in Table 1. At baseline, the mean score of AD8 was 0.80 (SD= 0.93). The mean age of the
sample was 74.52 (SD= 6.12) years, just under half of the sample were male (45.6%), while
the majority of the sample did not smoke (86.8% nonsmokers) or drink alcohol (95.2%
non-drinkers). In the univariate analyses, higher AD8 scores at follow-up (i.e. worse
cognition) were associated with female gender, increasing age, lower education status, low
light PA, MVPA, total physical activity, more chronic conditions, and having depressive
ACCEPTED MANUSCRIPT
Table 1 Distribution of cognitive ability in 2014 between levels of descriptors in 2012
Variables in 2012 N AD8 scores in 2014
Mean (SD) p-valuea Socio-demographic Sex 0.003 Male 125 0.85 (1.31) Female 149 1.29 (1.61) Age 0.001 65-74 156 0.81 (1.22) 75+ 118 1.45 (1.74) Education level 0.002 Secondary school+ 48 0.46 (0.46) Primary school 113 1.17 (1.17) No formal schooling 113 1.27 (1.27) Marital status 0.002 Married 192 0.92 (0.93) Others 82 1.48 (1.48)
Main source of income 0.001
Offspring 139 0.83(1.34)
Self (pension/savings) 135 1.35(1.61)
Lifestyle behaviors
Total energy expenditures (kcal/wk) < 0.001
High 92 0.48(0.75) Medium 91 0.90 (1.27) Low 91 1.89 (1.89) Moderate-to-vigorous PA (hour/day) < 0.001 High 92 0.55 (0.75) Medium 88 1.08 (1.51) Low 94 1.62 (1.83) Light PA (hour/day) <0.001 High 93 0.54 (0.67) Medium 91 1.04 (1.61) Low 90 1.70 (1.76) Smoking 0.122 Never smoker 238 1.03 (1.46) Current smoker 22 1.36 (1.65) Former smoker 14 1.71 (1.77)
ACCEPTED MANUSCRIPT
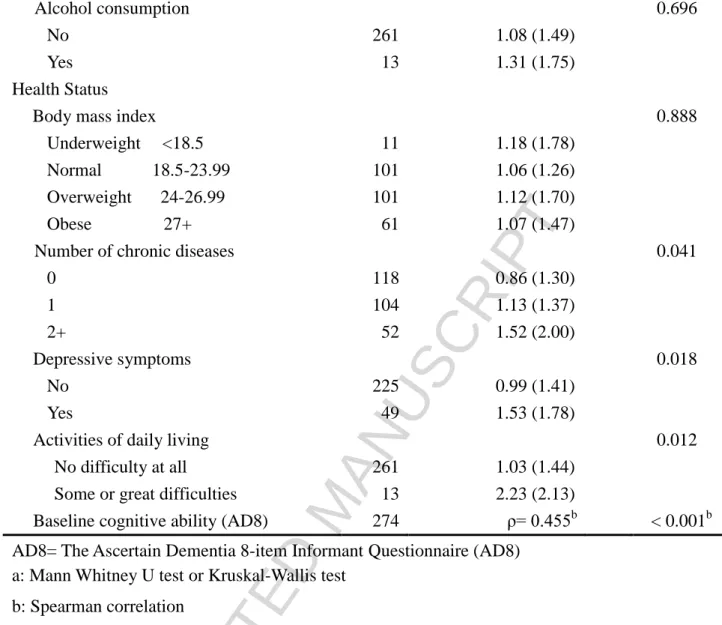
No 261 1.08 (1.49)
Yes 13 1.31 (1.75)
Health Status
Body mass index 0.888
Underweight <18.5 11 1.18 (1.78)
Normal 18.5-23.99 101 1.06 (1.26)
Overweight 24-26.99 101 1.12 (1.70)
Obese 27+ 61 1.07 (1.47)
Number of chronic diseases 0.041
0 118 0.86 (1.30) 1 104 1.13 (1.37) 2+ 52 1.52 (2.00) Depressive symptoms 0.018 No 225 0.99 (1.41) Yes 49 1.53 (1.78)
Activities of daily living 0.012
No difficulty at all 261 1.03 (1.44)
Some or great difficulties 13 2.23 (2.13)
Baseline cognitive ability (AD8) 274 ρ= 0.455b < 0.001b
AD8= The Ascertain Dementia 8-item Informant Questionnaire (AD8) a: Mann Whitney U test or Kruskal-Wallis test
b: Spearman correlation
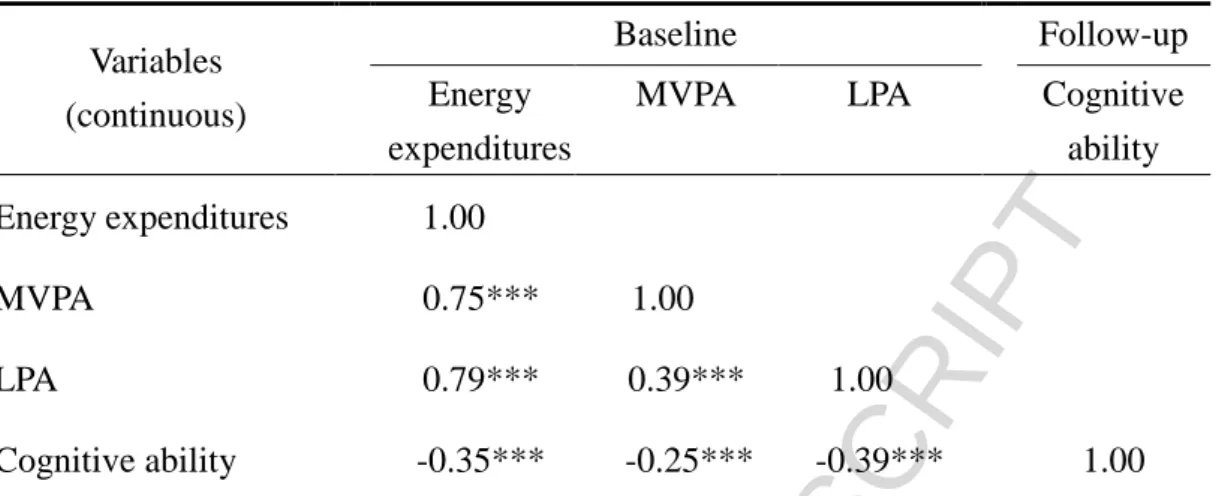
Correlation analyses between physical activity and subsequent cognitive ability
Table 2 summarizes the partial correlations between each physical activity category at
baseline, and subsequent cognitive ability. Briefly, worse cognition was negatively
ACCEPTED MANUSCRIPT
Table 2 Partial correlation coefficients between baseline physical activity parameters and
cognitive ability at follow-up adjusting for mean daily accelerometer wear time (n=274) Variables
(continuous)
Baseline Follow-up
Energy expenditures
MVPA LPA Cognitive
ability
Energy expenditures 1.00
MVPA 0.75*** 1.00
LPA 0.79*** 0.39*** 1.00
Cognitive ability -0.35*** -0.25*** -0.39*** 1.00
MVPA: Moderate-to-vigorous physical activity; LPA: Light physical activity; *** p < 0.001
Multivariate relationship between physical activity and subsequent cognitive score
The crude and adjusted estimates of single and multifactor models are presented in Table 3.
In the crude and adjusted analyses of single-factor models, light physical activity and MVPA
were both significantly associated with a reduced rate of cognitive ability decline. In the
adjusted estimates of two-factor model, light physical activity was independent from MVPA
and associated with a reduced rate of cognitive ability decline with a rate ratio of 0.75
(0.60-0.92). Similarly, MVPA was also independent from light PA and associated with a
ACCEPTED MANUSCRIPT
cognitive ability (n=274)Physical activity (continuous)
Single-factor models Two-factor model
Crude RR (95% CI)a P Adjusted RR (95% CI)b p Adjusted RR (95% CI)c p
MVPA 0.74 (0.66-0.82) < 0.001 0.81 (0.72-0.91) < 0.001 0.85 (0.75-0.95) 0.006
LPA 0.53 (0.45-0.64) < 0.001 0.67 (0.53-0.84) 0.001 0.75 (0.60-0.92) 0.007
RR= rate ratio; MVPA= moderate-to-vigorous physical activity; LPA= light physical activity
a: The two (single-factor) regression models for estimating the crude RR represent the unadjusted association of MVPA or LPA with cognitive impairment without mutual adjustment.
b: The two (single-factor) regression models for estimating the adjusted RR represent the multivariable association of MVPA or LPA with
cognitive ability without mutual adjustment. Covariates in the two models: baseline cognitive scores, sex, age, educational attainment, marital status, income source, smoking, number of chronic diseases, depressive symptoms, activities of daily living, and wear time of accelerometer c: The (two-factor) regression model for estimating the adjusted RR represent the multivariable association of LPA with cognitive ability.
Covariates in the model: baseline cognitive scores, sex, age, educational attainment, marital status, income source, smoking, number of ability chronic diseases, depressive symptoms, activities of daily living, wear time of accelerometer, and MVPA,
ACCEPTED MANUSCRIPT
Sensitivity analyses
The crude and adjusted analyses of single and multifactor models in sensitivity analyses are
shown in Table 4. To examine confounding and reverse causation, sensitivity analyses were
conducted to exclude people with ADL difficulty, people with both ADL difficulty and
depressive symptoms, and those with suspected cognitive impairment at baseline respectively.
However, the effect of light physical activity on subsequent cognitive ability remained. The
patterns of physical activity with cognitive ability at follow-up were similar to those in Table
ACCEPTED MANUSCRIPT
subsequent cognitive abilityStage 1: Excluding participants with ADL difficulties at baseline (n= 261)
Physical activity (continuous)
Single-factor models Two-factor model
Crude RR (95% CI)a p Adjusted RR (95% CI)b p Adjusted RR (95% CI)c p
MVPA 0.73 (0.65-0.82) < 0.001 0.81 (0.71-0.92) 0.002 0.85 (0.74-0.97) 0.018
LPA 0.53 (0.44-0.64) < 0.001 0.68 (0.54-0.86) 0.001 0.74 (0.58-0.95) 0.017
Stage 2: Excluding participants with ADL difficulties and depressive symptoms at baseline (n= 216)
Physical activity Crude RR (95% CI)a
p Adjusted RR (95% CI)b p Adjusted RR (95% CI)c p
MVPA 0.75 (0.67-0.85) < 0.001 0.81 (0.70-0.94) 0.005 0.86 (0.74-0.99) 0.043
LPA 0.50 (0.39-0.64) < 0.001 0.62 (0.45-0.84) 0.002 0.69 (0.51-0.94) 0.018
Stage 3: Excluding participants with suspected cognitive impairment at baseline (n=209)
Physical activity Crude RR (95% CI)a
p Adjusted RR (95% CI)b p Adjusted RR (95% CI)c p
ACCEPTED MANUSCRIPT
LPA 0.57 (0.45-0.74) < 0.001 0.60 (0.44-0.81) 0.001 0.69 (0.51-0.95) 0.021
RR= rate ratio; MVPA= moderate-to-vigorous physical activity; LPA= light physical activity
a: The two (single-factor) regression models for estimating the crude RR represent the unadjusted association of MVPA or LPA with cognitive ability without mutual adjustment.
b: The two (single-factor) regression models for estimating the adjusted RR represent the multivariable association of MVPA or LPA with cognitive ability without mutual adjustment. Covariates in the two models: baseline cognitive scores, sex, age, educational attainment, marital status, income source, smoking, number of chronic diseases, depressive symptoms, activities of daily living, and wear time of accelerometer
c: The (two-factor) regression model for estimating the adjusted RR represent the multivariable association of LPA with cognitive ability. Covariates in the model: baseline cognitive scores, sex, age, educational attainment, marital status, income source, smoking, number of chronic diseases, depressive symptoms, activities of daily living, wear time of accelerometer, and MVPA.
ACCEPTED MANUSCRIPT
The current study established that objective light physical activity offers a protective
effect from future decline in cognitive abilities over approximately two years among
community dwelling older adults. The protective effects of light physical activity were
independent of MVPA and the results remained robust in sensitivity analyses removing those
people with difficulties with ADL, depressive symptoms and suspected mild cognitive
impairment at baseline.
With the rapidly growing number of older people across the world, our data that objective
light physical activity confers a protective effect for future cognitive abilities are welcome and
has potential public health implications. Previous reviews (Blondell et al. 2014; Hamer and
Chida 2009; Paterson and Warburton 2010) have repeatedly highlighted the absence of
studies considering objective physical activity data and future cognitive impairment. Thus,
the overwhelming reliance of self-report physical activity from previous studies has infiltrated
a bias within the literature and such questionnaires cannot accurately disentangle the potential
individual benefits of different intensities of physical activity. The unique protective
influences of light physical activity on cognition are welcome for a number of reasons. First,
light physical activity such as casual walking, gardening and household chores are a preferred
method of accumulating physical activity for older people (Farren et al. 2015). Moreover,
ACCEPTED MANUSCRIPT
and friends and reduce the risk of social isolation. In addition, light physical activity is
associated with better wellbeing, physical health (Buman et al. 2010; Ku et al. 2016) and
improvements in other health outcomes such as reducing blood pressure, body fat, cholesterol
and improving cardiorespiratory fitness (Hanson and Jones 2015). Moreover, the risk of
injury and adverse outcomes are typically less with light physical activity versus more
vigorous intensities (Paterson and Warburton 2010). However, there are clearly benefits for
engaging in higher intensity physical activity and our data also establish that MVPA has a
protective effect on future cognitive impairment. In particular, higher intensity physical
activity that improves cardiorespiratory fitness confers particular benefits on health and brain
function (Erickson et al. 2014; Erickson et al. 2012).
The potential mechanisms by which physical activity confers a cognitive benefit in older age
are yet to be fully disentangled. One potential mechanism is through improving brain
structure and grey matter volume and in particular stimulating hippocampal neurogenesis,
with more recent evidence also suggesting the caudate nucleus and thalamus may be
positively impacted (Erickson et al. 2014; Erickson et al. 2012; Erickson et al. 2011; Kramer
and Erickson 2007). There is also accumulating evidence that participating in exercise may
improve cognitive outcomes through numerous biomarkers. In particular, recent data
ACCEPTED MANUSCRIPT
dehydroepiandrosterone may be associated with improved cognition and reduced dementia
risk following exercises in older age (Jensen et al. 2015; Maass et al. 2016). Clearly, future
research utilizing objective measures of physical activity are required to disentangle potential
mechanistic changes associated with cognitive status in older age.
Whilst our data are novel, one should note the observation nature of the data, which cannot
make claims regarding causality. The study follow up time was relatively short. Future
longitudinal research of longer duration is required to verify our findings. In addition, future
interventional work should seek to establish if changing physical activity levels can improve
cognitive (and other) outcomes. Another potential limitation is that objectively assessed
physical activity was only measured at baseline, which clearly limits the ability to explore the
reciprocal relationships between light physical activity and cognitive ability. Furthermore,
there is heterogeneity of comorbid conditions or health status in the population aged 65 or
above (e.g., different age groups). Future studies are encouraged to assess the relationships of
objectively measured physical activity with cognition, stratified by age groups. In addition,
we included some participants at baseline who had some degree of cognitive impairment,
which may influence the physical activity status at baseline. However, the independent
impact of light physical activity was evident in sensitivity analyses when such participants
ACCEPTED MANUSCRIPT
with and without such participants may actually increase representativeness, given the high
numbers of older people who are affected by cognitive impairment. This is the first
longitudinal paper to investigate light intensity physical activity and cognitive ability in older
adults. Strengths of our paper include the objective measurement of physical activity,
adjustment for multiple underlying confounders (e.g. baseline cognitive status, depressive
symptoms, and ADL difficulties) known to influence both physical activity and cognitive
ability, and test for reverse causation.
In conclusion, our data suggest that engagement in light intensity physical activity,
independent of MVPA, is associated with a reduced rate of cognitive ability decline in
community dwelling older adults. In addition, objectively assessed MVPA is associated with
better cognitive status. This extends the existing evidence for the benefits of physical
ACCEPTED MANUSCRIPT
AcknowledgementsThe authors declare no conflicts of interest and acknowledge funding support from Taiwan
Ministry of Science and Technology (104-2410-H-018-028).
Conflict of interest statement
ACCEPTED MANUSCRIPT
ReferencesBarnes, D.E.; Yaffe, K. The projected effect of risk factor reduction on Alzheimer's disease
prevalence. Lancet Neurol. 10:819-828; 2011
Blondell, S.J.; Hammersley-Mather, R.; Lennert Veerman, J. Does physical activity prevent
cognitive decline and dementia?: A systematic review and meta-analysis of
longitudinal studies. BMC Public Health. 14:1036-1061; 2014
Brink, T.L.; Yesavage, J.A.; Lum, O.; Heersema, P.H.; Adey, M.; Rose, T.L. Screening tests
for geriatric depression. Clin Gerontol. 1:37-43; 1982
Buchman, A.S.; Boyle, P.A.; Yu, L.; Shah, R.C.; Wilson, R.S.; Bennett, D.A. Total daily
physical activity and the risk of ad and cognitive decline in older adults. Neurology.
78:1323-1329; 2012
Buman, M.P.; Hekler, E.B.; Haskell, W.L.; Pruitt, L.; Conway, T.L.; Cain, K.L. Objective
light-intensity physical activity associations with rated health in older adults. Am J
Epidemiol. 172:1155-1165; 2010
Coley, N.; Andrieu, S.; Gardette, V.; Gillette-Guyonnet, S.; Sanz, C.; Vellas, B.; Grand, A.
Dementia prevention: Methodological explanations for inconsistent results.
Epidemiologics Review. 30:35-66; 2008
Deckers, K.; van Boxtel, M.P.; Schiepers, O.J.; de Vugt, M.; Munoz Sanchez, J.L.; Anstey,
ACCEPTED MANUSCRIPT
Yaffe, K.; Irving, K.; Verhey, F.R.; Kohler, S. Target risk factors for dementia
prevention: A systematic review and delphi consensus study on the evidence from
observational studies. Int J Geriatr Psychiatry. 30:234-246; 2015
Doi, T.; Makizako, H.; Shimada, H.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Park, H.;
Suzuki, T. Objectively measured physical activity, brain atrophy, and white matter
lesions in older adults with mild cognitive impairment. Exp Gerontol. 62:1-6; 2015
Erickson, K.I.; Leckie, R.L.; Weinstein, A.M. Physical activity, fitness, and gray matter
volume. Neurobiol Aging. 35:S20-S28; 2014
Erickson, K.I.; Miller, D.L.; Weinstein, A.M.; Akl, S.L.; Banducci, S.E. Physical activity and
brain plasticity in late adulthood: A conceptual review. Ageing Research. 3:34-47;
2012
Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.;
Heo, S.; Alves, H.; White, S.M.; Wojcicki, T.R.; Mailey, E.; Vieira, V.J.; Martin, S.A.;
Pence, B.D.; Woods, J.A.; McAuley, E.; Kramer, A.F. Exercise training increases size
of hippocampus and improves memory. PNAS Proceedings of the National Academy
of Sciences of the United States of America. 108:3017-3022; 2011
Falck, R.S.; McDonald, S.M.; Beets, M.W.; Brazendale, K.; Liu-Ambrose, T. Measurement of
physical activity in older adult interventions: A systematic review. Br J Sports Med.
ACCEPTED MANUSCRIPT
Farren, L.; Belza, B.; Allen, P.; Brolliar, S.; Brown, D.R.; Cormier, M.L.; Janicek, S.; Jones,
D.L.; King, D.K.; Marquez, D.X.; Rosenberg, D.E. Mall walking program
environments, features, and participants: A scoping review. Prev Chronic Dis. 12:E129;
2015
Fiest, K.M.; Jette, N.; Roberts, J.I.; Maxwell, C.J.; Smith, E.E.; Black, S.E.; Blaikie, L.;
Cohen, A.; Day, L.; Holroyd-Leduc, J.; Kirk, A.; Pearson, D.; Pringsheim, T.;
Venegas-Torres, A.; Hogan, D.B. The prevalence and incidence of dementia: A
systematic review and meta-analysis. Can J Neurol Sci. 43 Suppl 1:S3-s50; 2016
Galvin, J.; Roe, C.; Powlishta, K.; Coats, M.; Muich, S.; Grant, E.; Miller, J.; Storandt, M.;
Morris, J. The AD8: A brief informant interview to detect dementia. Neurology.
65:559; 2005
Galvin, J.E.; Roe, C.M.; Coats, M.A.; Morris, J.C. Patient's rating of cognitive ability: Using
the AD8, a brief informant interview, as a self-rating tool to detect dementia. Arch
Neurol. 64:725-730; 2007
Ganguli, M.; Lee, C.-W.; Snitz, B.; Hughes, T.; McDade, E.M.; Chang, C.-C.H. How well do
MCI criteria predict progression to severe cognitive impairment and dementia?
Alzheimer Dis Assoc Disord. 28:113-121; 2014
Gorman, E.; Hanson, H.; Yang, P.; Khan, K.; Liu-Ambrose, T.; Ashe, M. Accelerometry
ACCEPTED MANUSCRIPT
review and data analysis. Eur Rev Aging Phys Act. 11:35-49; 2014Guo, N.W.; Liu, H.C.; Wong, P.F.; Liao, K.K.; Yan, S.H.; Lin, K.P.; Chang, C.Y.; Hsu, T.C.
Chinese version and norms of the Mini-Mental State Examination. Journal of
Rehabilitation Medicine Association:52-59; 1988
Hamer, M.; Chida, Y. Physical activity and risk of neurodegenerative disease: A systematic
review of prospective evidence. Psychol Med. 39:3-11; 2009
Hamer, M.; Coombs, N.; Stamatakis, E. Associations between objectively assessed and
self-reported sedentary time with mental health in adults: An analysis of data from the
Health Survey for England. BMJ Open. 4; 2014
Hanson, S.; Jones, A. Is there evidence that walking groups have health benefits? A systematic
review and meta-analysis. Br J Sports Med. 49:710-715; 2015
Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied logistic regression. NJ: John Wiley &
Sons; 2013
Jensen, C.S.; Hasselbalch, S.G.; Waldemar, G.; Simonsen, A.H. Biochemical markers of
physical exercise on mild cognitive impairment and dementia: Systematic review and
perspectives. Front Neurol. 6:187; 2015
Kramer, A.F.; Erickson, K.I. Capitalizing on cortical plasticity: Influence of physical activity
on cognition and brain function. Trends in Cognitive Sciences. 11:342-348; 2007
ACCEPTED MANUSCRIPT
assessed physical activity at different intensities with subjective well-being in older
adults. Quality of Life Research. 25:2909–2919; 2016
Maass, A.; Duzel, S.; Brigadski, T.; Goerke, M.; Becke, A.; Sobieray, U.; Neumann, K.;
Lovden, M.; Lindenberger, U.; Backman, L.; Braun-Dullaeus, R.; Ahrens, D.; Heinze,
H.J.; Muller, N.G.; Lessmann, V.; Sendtner, M.; Duzel, E. Relationships of peripheral
igf-1, vegf and bdnf levels to exercise-related changes in memory, hippocampal
perfusion and volumes in older adults. Neuroimage. 131:142-154; 2016
Makizako, H.; Liu-Ambrose, T.; Shimada, H.; Doi, T.; Park, H.; Tsutsumimoto, K.; Uemura,
K.; Suzuki, T. Moderate-intensity physical activity, hippocampal volume, and memory
in older adults with mild cognitive impairment. J Gerontol A Biol Sci Med Sci.
70:480-486; 2015
McMinn, D.; Acharya, R.; Rowe, D.A.; Gray, S.R.; Allan, J.L. Measuring activity energy
expenditure: Accuracy of the GT3X+ and Actiheart monitors. Int J Exerc Sci.
6:217-229; 2013
Paterson, D.H.; Warburton, D.E. Physical activity and functional limitations in older adults: A
systematic review related to Canada's physical activity guidelines. Int J Behav Nutr
Phys Act. 7:38; 2010
Prince, M.; Bryce, R.; Albanese, E.; Wimo, A.; Ribeiro, W.; Ferri, C.P. The global prevalence
ACCEPTED MANUSCRIPT
Journal Of The Alzheimer's Association. 9:63-75.e62; 2013Taiwan Department of Health. Identification, evaluation, and treatment of overweight and
obesity in adults in Taiwan. Taipei: Taiwan Department of Health; 2003
Taiwan Ministry of Interior. Monthly bulletin of interior statistics: Resident population by age
group. Taipei: Taiwan Ministry of Interior; 2012
Tse, A.; Wong, T.W.; Lee, P.H. Effect of low-intensity exercise on physical and cognitive
health in older adults: A systematic review. Sports Medicine-Open. 1:1-13; 2015
Tudor-Locke, C.; Leonardi, C.; Johnson, W.D.; Katzmarzyk, P.T.; Church, T.S. Accelerometer
steps/day translation of moderate-to-vigorous activity. Prev Med. 53:31-33; 2011
World Health Organization. Global recommendations on physical activity for health. Geneva:
World Health Organization; 2010
Yang, Y.-H.; Galvin, J.E.; Morris, J.C.; Lai, C.-L.; Chou, M.-C.; Liu, C.-K. Application of
AD8 questionnaire to screen very mild dementia in Taiwanese. Am J Alzheimer's Dis
Other Dementias. 26:134-138; 2011
Yesavage, J.A.; Sheikh, J.I. Geriatric depression scale (gds): Recent evidence and
development of a shorter version. in: Brink T.L., ed. Clinical gerontologist: A guide to
assessment and intervention. New York: The Haworth Press; 1986
ACCEPTED MANUSCRIPT
29
Highlight Points
A paucity of studies have considered objective longitudinal physical activity and future cognitive ability decline in older adults.
Our data suggests that higher light physical activity, independent of
moderate-to-vigorous physical activity, is associated with a reduced risk of future
cognitive decline.
This is the first longitudinal paper to investigate light intensity physical activity and cognitive decline in older adults.
This extends the existing evidence for the benefits of physical activity for preventing cognitive deterioration in later life.