C
HRONIC
H
EPATITIS
B V
IRUS
I
NFECTION
AND
D
YSLIPIDEMIA
Ta-Chen Su,1,2 Yuan-Teh Lee,1 Tsun-Jen Cheng,1,2 Hsu-Ping Chien,2 and Jung-Der Wang1,2
1Department of Internal Medicine, National Taiwan University Hospital, Taipei; 2Institute of Occupational Medicine and
Industrial Hygiene, College of Public Health, National Taiwan University, Taipei, Taiwan. Received: 28 May 2003 Revised: 21 August 2003 Accepted: 9 December 2003
Reprint requests and correspondence to: Dr. Jung-Der Wang, Professor, Institute of Occupational Medicine and Industrial Hygiene, College of Public Health, National Taiwan University, Taipei, Taiwan.
Background and Purpose: The association of chronic hepatitis B virus (HBV) infection and decreased levels of high-density lipoprotein cholesterol (HDL-C) has been well documented. However, the relationship between dyslipidemia and asymptomatic chronic HBV infection is still unclear.
Methods: In 1997, 1330 medical center employees (405 men and 925 women) were recruited to evaluate the effects of chronic HBV infection on serum lipid profile, including total cholesterol (TC), HDL-C, low-density lipoprotein cholesterol, and triglycerides (TG). Among these patients, 195 were found to have chronic HBV infection and 35 (17.9%) of them were found to have elevated alanine aminotransferase (ALT). Multiple linear regression analyses were used to evaluate the effects of chronic HBV infection on serum lipids.
Results: The most significant finding was that levels of TC and HDL-C were decreased by 5.8 and 2.7 mg/dL respectively, among patients with asymptomatic chronic HBV infection (serum ALT < 40 U/L). After controlling for other determinants, male gender, old age, higher body mass index (BMI) and waist-to-hip ratio, current smoking, and hepatitis B surface antigen-negative status with ALT ≥ 40 U/L were associated with lower serum HDL-C and higher TG levels. However, moderate to heavy alcohol drinking, physically active lifestyle, and lower BMI were associated with higher levels of HDL-C.
Conclusions: Asymptomatic chronic HBV infection was associated with lower serum levels of TC and HDL-C. Elevation of ALT was also an indicator of lower levels of HDL-C in patients with chronic hepatitis B and lower serum HDL-C and higher TG levels in patients without HBV infection. These findings also indicated the need to monitor the risk of atherosclerotic diseases in patients with asymptomatic chronic HBV infection, especially those with lower HDL-C levels.
Key words: Alanine aminotransferase; Hepatitis B virus; Dyslipidemia; Lipoprotein, HDL cholesterol
J Formos Med Assoc 2004;103:286-91
Hepatitis B virus (HBV) infection with its high pre-valence and associated morbidity and mortality has been recognized as an important health issue in Taiwan
for more than 3 decades.1 The hepatitis B surface
anti-gen (HBsAg) infection rate in the anti-general
popula-tion is about 10 to 20% in Taiwan.1,2 Hepatoma results
in about 5800 deaths and was the leading cause of
cancer death in Taiwan in 1999.3 People with chronic
HBV infection are at risk for developing sequelae,
including chronic active hepatitis,4 cirrhosis,5 and
hepatocellular carcinoma.6
Chronic hepatitis B and C and cirrhosis of the liver have been associated with impaired lipid me-tabolism, reduced total cholesterol (TC), and reduced high-density lipoprotein cholesterol (HDL-C) in
case-control studies.7,8 Changes in serum lipids were
com-monly found in patients with chronic liver disease,7–9
and a study in China found that prolonged HBV infection was related to low blood cholesterol
con-centration and increased frequency of liver cancer.10
However, the status of serum HDL-C in patients with asymptomatic chronic HBV infection has not been reported. Furthermore, most studies about the influence of blood lipids in patients with hepatitis
were conducted in small series7–9 except for a study
from China,10 and the potential confounding factors
of blood lipid levels were often overlooked,7,8 or only
partially adjusted.9,10
We conducted this study to delineate the effects of HBV infection status and elevation of alanine aminotransferase (ALT) levels on serum lipid profile, especially their association with dyslipidemia (lower levels of HDL-C and/or higher levels of triglyceride).
M
ethods
Subjects
In 1997, 1693 health workers in a medical center aged 30 to 65 years were invited to receive an annual
physical examination, which included a general health survey questionnaire, collection of blood for serum lipid profile (TC, triglycerides [TG], HDL-C, and low-density lipoprotein cholesterol [LDL-C]), hepatitis B and C markers, and associated biochemical tests. Among them, 260 subjects with incomplete question-naires, 57 with incomplete data on hepatitis markers, and 25 with previously identified clinical conditions that may affect lipid profile were excluded. In addi-tion, 21 subjects with TG > 400 mg/dL were excluded due to the limitations of the LDL-C calculation by
Friedewald’s formula.11 Finally, 405 men and 925
women were included in this study (78.6%).
Baseline information and medical history
Information about age, gender, type of work, life-styles (smoking and alcohol drinking), medication history, physical activities (including leisure-time and working), and medical and family histories of major diseases was obtained through a self-reported question-naire, and later verified through checking of medic-al charts. Body weight and height, waist-to-hip ratio (WHR), and blood pressure (BP) were measured during the physical examination.
BP measurements were performed with a mercury sphygmomanometer in a standardized fashion. BP was recorded using the mean of 2 measurements taken after 5 minutes of rest in the sitting position. Hypertension was defined according to the criteria established by the Fifth Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (JNC-V). Diabetes mellitus (DM) was defined
as fasting glucose ≥ 140 mg/dL, and/or a history of
use of oral hypoglycemic agents or insulin injection. Body mass index (BMI) was calculated as weight (in kg) divided by height (in meters) squared. Individuals
with BMI ≥ 25 kg/m2 were considered as overweight.
Physical activity index was calculated using the
methods of Paffenbarger et al,12 and computed as an
estimate of energy expended in walking, climbing stairs,
playing sports, yard work, and so on.13 Data on alcohol
use and smoking were self-reported on the question-naire. Amount of alcohol consumed was calculated based on data obtained on frequency and amount, and was summarized as average number of alcoholic drinks consumed per week. An extent of alcohol drinking of 100 to 367.6 g/week was considered a moderate to heavy amount and > 367.6 g/week was considered excessive, as modified from the definition by Lee et al
in a study conducted in Taiwanese.14 Family history of
premature coronary heart disease was indicated by the occurrence of myocardial infarction or sudden death before 55 years of age of an individual’s father or other male first-degree relative, or before 65 years of age of the mother or other female first-degree relative.
Lipid levels, liver function profile and viral
hepatitis markers
Blood samples from patients who had fasted 10 to 14 hours overnight were drawn from the antecubital vein for lipid and glucose determinations with the patient in a seated position. Serum levels of lipids, including TC, HDL-C, and TG were assayed in the central laboratory of National Taiwan University
Hospital.15 The TC and TG levels (determined by
enzymatic methods described elsewhere) were measured with an automatic multichannel chemical analyzer (Hitachi 7450; Hitachi Corp., Tokyo, Japan). HDL-C level was determined by measuring cholesterol in the supernantant after precipitating very
low-density lipoprotein cholesterol and LDL-C with Mg2+/
phosphotungstate reagent. LDL-C was calculated
from Friedewald’s formula.11 Liver function profile,
including serum aspartate aminotransferase (AST), ALT, bilirubin, albumin, and globulin were also deter-mined using routine enzymatic methods. Data on hepatitis markers were collected from chart review and HBsAg and anti-hepatitis C virus (anti-HCV) antibody were rechecked for every participant using radiommunoassays.
Statistical methods
In the data analysis, characteristics and cardiovascular risk factors of study subjects were first compared by hepatitis status, i.e., between HBsAg-positive (+) and -negative (–) status, and between anti-HCV (+) and (–). Variables in interval scales were summarized as
the mean ± standard deviation (SD). The categorical
data on alcohol and smoking habits were expressed as a percentage of positivity. Both t test and ANOVA test were used to make comparisons among these groups.
Multiple linear regression analyses were used to evaluate the determinants of lipid profile and estimate the magnitudes of effects. Because there were only 32 subjects with hepatitis C infection, we excluded these subjects and another 2 cases with coinfections of hepatitis B and C from the multivariate regression analysis.
The presence or absence of HBsAg (+) or (–) and
status of liver function (serum ALT ≥ 40 U/L or ALT
< 40 U/L) were included to test their contribution to lipid profile. An asymptomatic chronic HBV infection was defined as a positive HBsAg and a normal ALT level (defined as serum ALT < 40 U/L). Serum albumin level was also treated as a potential con-founding factor that might affect the relation between hepatitis and lipid profiles. All statistical analyses were performed with SAS statistical software (Version 8.0, SAS Institute, Cary NC, USA). A p value < 0.05 was considered statistically significant.
R
esults
Baseline characteristics
The prevalence of HBsAg (+) was 17.8% in men and 13.4% in women; anti-HCV (+) status was found in 3.7% of men and 1.9% of women. Table 1 summarizes the reasons for secondary dyslipidemia or decompen-sated liver disease in 25 excluded cases. The character-istics of subjects with and without hepatitis B or C infection are summarized in Table 2. Compared to those without hepatitis B infection, subjects with HBsAg (+) were largely male, had lower levels of TC, HDL-C, and a higher prevalence of abnormal liver
function (defined as levels of ALT ≥ 40 U/L). Among
patients with chronic HBV infection, 17.9% had elevated ALT levels. Compared to those without hepatitis C infection, subjects with anti-HCV (+) status were largely male, older, more obese (higher BMI and WHR), and had a higher prevalence of abnormal liver function.
Effects of chronic hepatitis B infection and
elevated ALT
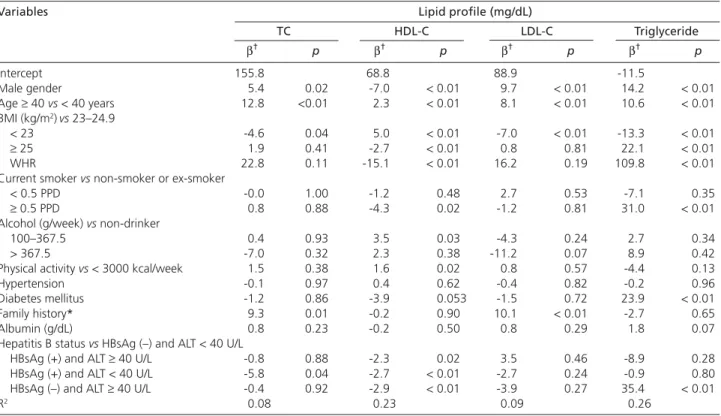
After controlling for potential confounding variables, multiple linear regression analyses showed that asymptomatic chronic HBV infection was correlated with lower TC (-5.8 mg/dL) and HDL-C (-2.7 mg/dL) levels, as shown in Table 3.
However, only a moderate reducing effect on serum HDL-C (-2.3 mg/dL) was found in patients with chronic hepatitis B, defined as HBsAg (+) with
ALT ≥ 40 U/L lasting at least 6 months. Those with
HBsAg (–) and abnormal liver function, defined as
ALT ≥ 40 U/L, had lower HDL-C (-2.9 mg/dL) and
higher TG (+35.4 mg/dL) levels. Serum albumin levels showed no significant association with serum lipids (Table 3).
Effects of cardiovascular risk factors
Table 3 shows that men and older subjects (≥ 40 years
old) had significantly higher TC, LDL-C and TG levels, and lower HDL-C levels. Subjects with higher BMI, WHR, and current smokers of more than 0.5 packs per day (PPD) were associated with lower serum HDL-C and higher TG levels. A family history of premature coronary heart disease was associated with a higher LDL-C level.
However, subjects with moderate to heavy alcohol drinking and subjects who were physically active (defined as physical activity > 3000 kcal/week) were associated with increased HDL-C levels of 3.5 mg/dL and 1.6 mg/dL, respectively. Subjects with DM had a higher TG level and a trend to lower levels of HDL-C. Patterns of diet intake in HBsAg (+) patients were not significantly different from HBsAg (–) patients, and this variable was therefore not included in the multiple linear regression analysis model.
Table 2. Characteristics of subjects with and without hepatitis B or hepatitis C infection.
Characteristic* HBsAg (+) HBsAg (–) Anti-HCV (+) Anti-HCV (–) (n = 195) (n = 1135) (n = 32) (n = 1298) Age (years) 40.44 (7.54) 41.12 (8.25) 48.13 (7.81) 40.85 (8.08)‡ Male (%) 36.9 29.3† 43.8 30.1† Current smoker (%) 8.7 6.9 3.1 7.2 Alcohol habit (%)‡ 9.2 6.3 3.1 6.9 ALT ≥ 40 U/L (%) 17.9 6.9‡ 25.0 8.1‡
Body mass index (kg/m2) 23.54 (3.24) 23.45 (3.12) 24.80 (3.59) 23.43 (3.12)†
Waist-to-hip ratio 0.86 (0.08) 0.85 (0.07) 0.89 (0.05) 0.85 (0.07)‡ Physical activity index (/1000 kcal/week) 3.09 (1.61) 3.24 (1.43) 3.55 (1.45) 3.21 (1.46) TC (mg/dL) 181.7 (29.8) 186.8 (33.3)† 187.9 (35.2) 186.0 (32.9) HDL-C (mg/dL) 53.4 (11.6) 56.5 (13.5)‡ 54.9 (15.1) 56.1 (13.1) LDL-C (mg/dL) 108.7 (25.9) 109.4 (28.6) 108.3 (26.3) 109.4 (28.2) Triglyceride (mg/dL) 99.2 (54.0) 102.7 (57.6) 125.8 (71.7) 101.9 (56.7)† Fasting sugar (mg/dL) 92.2 (24.7) 91.0 (17.5) 91.8 (17.6) 91.1 (18.7) * Values are presented as mean (SD), except gender, current smoker, alcohol habit and ALT ≥ 40 U/L. Alcohol habit means alcohol consumption ≥ 100 g/week. †p < 0.05.
‡ p < 0.01.
ALT = alanine aminotransferase; TC = total cholesterol; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol; HBsAg = hepatitis B surface antigen; HCV = hepatitis C virus.
Table 1. Clinical conditions and laboratory findings that may
affect lipid profile in excluded subjects.
Condition No. of cases
Clinical conditions* Pregnancy 12 Hyperthyroidism 3 Chemotherapy 1 Steroid use 1 Laboratory findings† Albumin < 3.5 g/dL 4 Total bilirubin > 2 mg/dL 4 Total 25
* Clinical conditions associated with secondary dyslipidemia. † Laboratory findings that define decompensated liver disease or poor nutrition status.
D
iscussion
To our knowledge, this study is the first to document that asymptomatic chronic HBV infection has a significant effect in lowering HDL-C and TC. The additional finding of decreased serum levels of HDL-C in chronic hepatitis B in this study is compatible
with previous studies.7,8 Because most of the measured
HDL-C is synthesized in the liver,16 major injuries to
hepatocytes, such as those caused by alcohol con-sumption, chronic viral hepatitis or cirrhosis of liver, might produce abnormal liver function and moderate
decrease in levels of HDL-C and TC.7,8 In patients with
chronic liver disease, the lower level of cholesterol indicated the severity of liver cell injury, which was associated with impairment of the synthetic ability of the liver.17
Male gender, old age,18,19 obesity,20 and DM21 were
reported to be associated with dyslipidemia among Caucasians. This study had similar findings, as shown in Table 3, which corroborated the above hypotheses
in ethnic Chinese from our previous studies.22,23 The
lower HDL-C and higher TG levels in subjects with
current smoking ≥ 0.5 PPD is similar to previous
findings.24 This and other studies have observed that
alcohol drinkers have higher HDL-C levels than
non-drinkers,25 and physically active subjects had higher
levels of HDL-C.26 All of these consistent findings
strongly support the validity of this study.
The detailed mechanism responsible for the HDL-C-reducing effect of chronic HBV infection remains to be elucidated. An enzyme involved in the biotransformation of HDL, lecithin-cholesterol acyl-transferase (LCAT), was reported to be reduced in pa-tients with advanced chronic liver disease or cirrhosis,
probably because of impaired hepatic synthesis.7,27,28
This reduction may also decrease HDL-C and TC in the case of mild hepatic damage that is not reflected in serum ALT level. Since our study did not perform abdominal sonography or measure hepatitis B e anti-gen, we could not differentiate the exact clinical stage of the HBV infection for each patient, which limits the inference potential of this study.
Lipids have been considered to play an important
role in the host immune response to infections.29
Lipo-proteins can bind a variety of viruses and reduce their
toxic effect.30 Thus, decreased levels of TC and HDL-C
in patients with asymptomatic chronic HBV infection may reduce their antiviral response. Because an association between low levels of cholesterol and liver
cancer has been observed in chronic HBV infections,10
Table 3. Multiple linear regression analyses to evaluate the predictive effects of viral hepatitis B infection and other
deter-minants on serum lipid profile.
Variables Lipid profile (mg/dL)
TC HDL-C LDL-C Triglyceride β† p β† p β† p β† p Intercept 155.8 68.8 88.9 -11.5 Male gender 5.4 0.02 -7.0 < 0.01 9.7 < 0.01 14.2 < 0.01 Age ≥ 40 vs < 40 years 12.8 <0.01 2.3 < 0.01 8.1 < 0.01 10.6 < 0.01 BMI (kg/m2)vs 23–24.9 < 23 -4.6 0.04 5.0 < 0.01 -7.0 < 0.01 -13.3 < 0.01 ≥ 25 1.9 0.41 -2.7 < 0.01 0.8 0.81 22.1 < 0.01 WHR 22.8 0.11 -15.1 < 0.01 16.2 0.19 109.8 < 0.01
Current smoker vs non-smoker or ex-smoker
< 0.5 PPD -0.0 1.00 -1.2 0.48 2.7 0.53 -7.1 0.35
≥ 0.5 PPD 0.8 0.88 -4.3 0.02 -1.2 0.81 31.0 < 0.01
Alcohol (g/week) vs non-drinker
100–367.5 0.4 0.93 3.5 0.03 -4.3 0.24 2.7 0.34
> 367.5 -7.0 0.32 2.3 0.38 -11.2 0.07 8.9 0.42
Physical activity vs < 3000 kcal/week 1.5 0.38 1.6 0.02 0.8 0.57 -4.4 0.13
Hypertension -0.1 0.97 0.4 0.62 -0.4 0.82 -0.2 0.96
Diabetes mellitus -1.2 0.86 -3.9 0.053 -1.5 0.72 23.9 < 0.01 Family history* 9.3 0.01 -0.2 0.90 10.1 < 0.01 -2.7 0.65
Albumin (g/dL) 0.8 0.23 -0.2 0.50 0.8 0.29 1.8 0.07
Hepatitis B status vs HBsAg (–) and ALT < 40 U/L
HBsAg (+) and ALT ≥ 40 U/L -0.8 0.88 -2.3 0.02 3.5 0.46 -8.9 0.28 HBsAg (+) and ALT < 40 U/L -5.8 0.04 -2.7 < 0.01 -2.7 0.24 -0.9 0.80 HBsAg (–) and ALT ≥ 40 U/L -0.4 0.92 -2.9 < 0.01 -3.9 0.27 35.4 < 0.01
R2 0.08 0.23 0.09 0.26
*Family history means family history of premature coronary artery disease. †β means regression coefficient.
BMI = body mass index; WHR = waist-to-hip ratio; PPD = packs per day; HBsAg = hepatitis B surface antigen; ALT = alanine aminotransferase; TC = total cholesterol; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol.
patients with asymptomatic chronic HBV infection with decreased HDL-C and TC should be followed due to their increased risk of developing liver cancer in the future.
A previous study showed that elevated ALT was associated with higher levels of BMI, glucose, and uric acid in a large cohort of 8501 men and women with hyperlipidemia, and this combination of clinical
fea-tures was designated as plurimetabolic syndrome.31
High ALT is also associated with impaired insulin
sensitivity and is a predictor of type 2 DM.32 Elevation
of ALT in non-alcoholic subjects without HBV and HCV infections is often associated with liver steatosis, which had a strong relationship with obesity, DM
and hypertriglyceridemia in a previous study.33 In
this study, we demonstrated an association between elevated serum levels of ALT and lower levels of C in patients with HBsAg (+), and lower levels of HDL-C and higher levels of TG in patients with HBsAg (–). These findings suggest that liver steatosis and a clustering of symptoms indicative of a metabolic syn-drome might be the cause of elevated ALT levels.
Dyslipidemia (lower HDL-C levels and/or higher TG levels), defined as the major component of
meta-bolic syndrome according to the NCEP-ATP III,34 was
strongly associated with HBV infection and elevated ALT levels in this study. Dyslipidemia is also well known as a major risk factor for cardiovascular disease
(CVD).34 Thus, measurements of HBsAg markers and
serum ALT levels at the time of health examinations could provide valuable information, especially in subjects at increased risk for CVD.
Clinical and experimental trials have shown that decreased levels of HDL-C increase the risk of CVD.35,36 A hospital-based study in Taiwan also revealed that a lower HDL-C level was an important independent risk factor for coronary artery disease in patients with
low serum TC and TG levels.15 Low serum HDL-C level
was also found to be associated with subclinical left ventricular systolic dysfunction in Chinese patients with stable angina whose serum levels of TC and TG were
relatively low.37 A recent study demonstrated HBsAg (+)
was positively associated with carotid plaque with an odds ratio of 1.57 (95% CI, 1.10 to 2.24) compared with HBsAg (–), which may suggest a possible role of chronic HBV infection in the pathogenesis of carotid
arterio-sclerosis.38 Chronic infection and inflammation have
been suggested to be associated with atherosclerotic
disease in recent studies.39,40 Thus, the long-term effect
of lowering levels of HDL-C in patients with chronic HBV infection deserves further investigation.
ACKNOWLEDGMENT: A grant from National Taiwan
University Hospital (NTUH-N87104) supported this study.
R
eferences
1. Sung JL, Chen DS, Lai MY, et al: Epidemiological study on hepatitis B virus infection in Taiwan. Chin J Gastroenterol 1984; 1:1-9.
2. Hsu HY, Chang MH, Chen DS, et al: Baseline seroepidemiology of hepatitis B virus infection in children in Taipei, 1984: a study just before the mass hepatitis B virus vaccination program in Taiwan. J Med Virol 1986;18:301-7.
3. Department of Health, Executive Yuan: Health and Vital Statistics II of the Republic of China, 1999. Taipei, Republic of China. 4. Redeker AG: Viral hepatitis: clinical aspects. Am J Med Sci 1975;
270:9-16.
5. Yu MW, Hsu FC, Sheen IS, et al: Prospective study of hepato-cellular carcinoma and liver cirrhosis in asymptomatic chronic hepatitis B virus carriers. Am J Epidemiol 1997;145:1039-47. 6. Beasley RP, Lin CC, Hwang LY, et al: Hepatocellular carcinoma
and hepatitis B virus. A prospective study of 22,707 men in Taiwan. Lancet 1981;2:1129-33.
7. Kanel GC, Radvan G, Peters RL: High-density lipoprotein cholesterol and liver disease. Hepatology 1983;3:343-8. 8. Cicognani C, Malavolti M, Morselli-Labate AM, et al: Serum
lipid and lipoprotein patterns in patients with liver cirrhosis and chronic active hepatitis. Arch Intern Med 1997;157:792-6. 9. Fabris C, Federico E, Soardo G, et al: Blood lipids of patients
with chronic hepatitis: differences related to viral etiology. Clin
Chim Acta 1997;261:159-65.
10. Chen Z, Keech A, Collins R, et al: Prolonged infection with hepatitis B virus and association between low blood cholesterol concentration and liver cancer. BMJ 1993;306:890-4. 11. Friedewald WT, Levy RI, Fredrickson DS: Estimation of
concent-ration of low density lipoprotein cholesterol in plasma without preparative ultracentrifuge. Clin Chem 1972;18:499-502. 12. Paffenbarger RS, Hyde RT, Wing AL, et al: Physical activity,
all-cause mortality, and longevity of college alumni. N Engl J Med 1986;314:605-13.
13. Ainsworth BE, Haskell WL, Leon AS, et al: Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc 1993;25:71-80.
14. Lee TK, Huang ZS, Ng SK, et al: Impact of alcohol consumption and cigarette smoking on stroke among the elderly in Taiwan.
Stroke 1995;26:790-4.
15. Lien WP, Lai LP, Shyu KG, et al: Low-serum, high-density lipoprotein cholesterol concentration is an important coronary risk factor in Chinese patients with low serum levels of total cholesterol and triglyceride. Am J Cardiol 1996;77:1112-5. 16. Levy RI, Rifkind BM: The structure, function and metabolism of
high-density lipoproteins: a status report. Circulation 1980;62 (Suppl IV):4-8.
17. Vergani C, Trovato G, Delu A et al: Serum total lipids, lipoprotein cholesterol, and apolipoprotein A in acute viral hepatitis and chronic liver disease. J Clin Path 1978;31:772-8.
18 Miller VT: Lipids, lipoproteins, women and cardiovascular disease.
19. Brown SA, Hutchinson R, Morrisett J, et al: Plasma lipid, lipoprotein cholesterol, and apoprotein distribution in selected US communities. Arterioscler Thromb 1993;13:1139-58. 20. Van Itallie TB: Health implications of overweight and obesity in
the United States. Ann Intern Med 1985;103:983-8.
21. Howard BV: Lipoprotein metabolism in diabetes mellitus. J Lipid
Res 1987;28:613-28.
22. Torng PL, Su TC, Sung FC, et al: Effects of menopause and obesity on lipid profiles in middle-aged Taiwanese women—The Chin-Shan Community Cardiovascular Cohort Study. Atherosclerosis 2000;153:413-21.
23. Chien KL, Lee YT, Sung FC, et al: Hyperinsulinemia and related atherosclerotic risk factors in the population at risk: community-based study. Clin Chem 1999;45:838-46.
24. Craig WY, Palomaki GE, Haddow JE: Cigarette smoking and serum lipid and lipoprotein concentrations: an analysis of published data. BMJ 1989;298:784-8.
25. Castelli WP, Doyle JT, Gordon T, et al: Alcohol and blood lipids. The Cooperative Phenotying Study. Lancet 1977;2:153-5. 26. Krauss RM: Exercise, lipoproteins, and coronary artery disease.
Circulation 1989;79:1143-5.
27. Floren CH, Chen CH, Franzen J, et al: Lecithin: cholesterol acyl-transferase in liver disease. Scand J Clin Lab Invest 1987;47: 613-7.
28. Nestel PJ, Tarda N, Fidge NH: Increased catabolism of high-density lipoprotein in alcoholic hepatitis. Metabolism 1980;29:101-4. 29. Grunfeld C, Feingold KR: Tumor necrosis factor, interleukin, and
interferon induced changes in lipid, metabolism as part of host defense. Proc Soc Exp Biol Med 1992;200:224-7.
30. Leong JC, Kane JP, Oleszko O, et al: Antigen specific non-immunoglobulin factor that neutralizes xenotropic virus is associated with mouse serum lipoproteins. Proc Natl Acad Sci
USA 1977;74:276-80.
31. Bruckert E, Giral P, Ratziu V, et al: A constellation of cardio-vascular risk factors is associated with hepatic enzyme elevation in hyperlipidemic patients. Metabolism 2002;51:1071-6. 32. Vozarova B, Stefan N, Lidsay RS, et al: High alanine
amino-transferase is associated with decreased hepatic insulin sensitivity and predicts the development of type 2 diabetes. Diabetes 2002; 51:1889-95.
33. Angelico F, DelBen M, Conti R, et al: Non-alcoholic fatty liver syndrome: a hepatic consequence of common metabolic diseases. J Gastroenterol Hepatol 2003;18:588-94.
34. National Institutes of Health. Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Bethesda, Md. National Institutes of Health; 2002. NIH Publication 02-5215.
35. Gordon DJ, Rifkind BM: High-density lipoprotein—the clinical implications of recent studies. N Engl J Med 1989;321:1311-6. 36. Rubins HB, Robins SJ, Collins D, et al: Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. N Engl J Med 1999;341:410-8.
37. Wang TD, Lee CM, Wu CC, et al: The effects of dyslipidemia on left ventricular systolic function in patients with stable angina pectoris. Atherosclerosis 1999;146:117-24.
38. Ishizaka N, Ishizaka Y, Takahashi E, et al: Increased prevalence of carotid atherosclerosis in hepatitis B virus carriers. Circulation 2002;105:1028-30.
39. Danesh J, Collins R, Peto R: Chronic infections and coronary heart disease: is there a link? Lancet 1997;350:430-6. 40. Libby P, Ridker PM, Maseri A: Inflammation and atherosclerosis.