以octreotide及低劑量dopamine治療第一型肝腎症候群; Treatment of type I hepatorenal syndrome with octreotide and dopamine
67
0
0
全文
(2) 中文摘要 背景. 肝腎症候群為急性或慢性肝病引發重度肝衰竭和門脈高. 壓所引起的功能性腎衰竭,當患者發生肝腎症候群時,常表示其肝功 能已到了嚴重衰竭的時候,大多數患者在很短的時間內便會死亡。目 前對於肝腎症候群仍未有理想的治療方法。近年來門脈高壓導致內臟 動脈血管擴張便被視為肝腎症候群的起步點,基於此一理論,內臟血 管收縮葯物加上血容積的補充便成為目前對肝腎症候群最有效的藥 物治療。本研究的目的,是要探討內臟血管收縮劑及配合白蛋白的補 充之外,在不同時間加上另一種作用位置不同的藥物,是否更有利於 治療。 方法. 自 2000 年 7 月至 2002 年 3 月間在中國醫藥學院附設醫院住院. 的肝硬化病患如併發第一型肝腎症候群者而符合收納標準者都列 為研究對像。在治療前 5 天停止利尿劑的使用,然後以隨機分組接 受不同的治療:第一組:先以 dopamine 2-4 µg/kg/min 持續注射 5 天,後以 octreotide 100 µg 注射後,25 µg/hr 持續注射 5 天,這 10 天中每天注射 20%白蛋白 50 至 100 毫升。第二組:先以同上劑量 octreotide 注射 5 天,再以 dopamine 注射 5 天,這 10 天中每天也 注射同劑量的白蛋白。第三組:以 dopamine 2-4 µg/kg/min 持續注 射 10 天。第四組:不注射 octreotide 或 dopamine,觀察 10 天。. 2.
(3) 結果. 共有 24 名患者符合本研究的納入標準並同意接受治療,每組個. 案各為 6 人,平均年齡為 50.0 至 55.0 歲(從 36 歲至 69 歲),4 組之 間之基本資料、肝硬化的成因、治療前的肝功能和腎功能並無差異。 經過治療之後,血尿素氮濃度在第一,二組均有顯著下降而第三、四 組卻均有惡化,但第一、二組血尿素氮之改善程度並未達到明顯的不 同。肌酸酐在第一,二組均有顯著下降而第三、四組則均有惡化,且 第二組肌酸酐下降程度顯著地超過第一組(p<0.05)。雖然第一、二組 病患在接受治療後腎功能皆有改善,但無論是血尿素氮或肌酸酐,其 顯著改善的時刻都是出現在使用 octreotide 的時候。PRA、皮質醛酮及 ADH 在第一,二組均隨著腎功能的改善而顯著下降。而 30 天存活率 在第一組為 100%(6/6) 、第二組為 83%(5/6) ,第三組為 67%(4/6), 第 4 組為 33%(2/6)。 結論. 以 octreotide 配合白蛋白的補充而繼之以 dopamine來治療第一. 型肝腎症候群是一個安全而有效的療法;藥物治療 10 天以後可扭轉 肝腎症候群的進展;單獨使用 dopamine 治療不能改善患者的腎功 能,但可短暫性地增加尿量及尿鈉排泄量;進一步的研究仍有必要。. 3.
(4) 目. 錄 頁數. 誌謝……………………………………………………………………1 中文摘要………………………………………………………………2 目錄……………………………………………………………………4 表目錄…………………………………………………………………6 圖目錄…………………………………………………………………7 符號與縮寫……………………………………………………………8 第一章 前言…………………………………………………………9 第一節 何謂肝腎症候群…………………………………9 第二節 歷史回顧…………………………………………10 第三節 流行病學…………………………………………12 第四節 臨床表徵…………………………………………13 第五節 發病原理…………………………………………15 第六節 診斷………………………………………………20 第七節 治療………………………………………………21 第八節 本研究所探討之假說……………………………26 第九節 研究目的…………………………………………27 第二章 研究方法……………………………………………………28. 4.
(5) 第一節. 研究設計…………………………………………28. 第二節 材料………………………………………………29 第三節 方法………………………………………………30 第四節 統計分析…………………………………………32 第三章 研究結果……………………………………………………33 第四章 討論…………………………………………………………36 參考文獻………………………………………………………………55 英文摘要………………………………………………………………65 作者簡歷………………………………………………………………67 著作權聲明……………………………………………………………68. 5.
(6) 表. 目. 錄 頁數. 表 1:肝腎症候群兩個臨床類型的特色………………………………41 表 2:肝腎症候群、腎前氮血症、急性腎衰竭 在尿液生化學及常規檢查上的異同……………………………42 表 3:肝腎症候群的診斷標準…………………………………………43 表 4:四組接受不同治療之肝腎症候群患者的基本資料……………44 表 5:四組接受不同治療之肝腎症候群患者的腎功能變化和預後…45. 6.
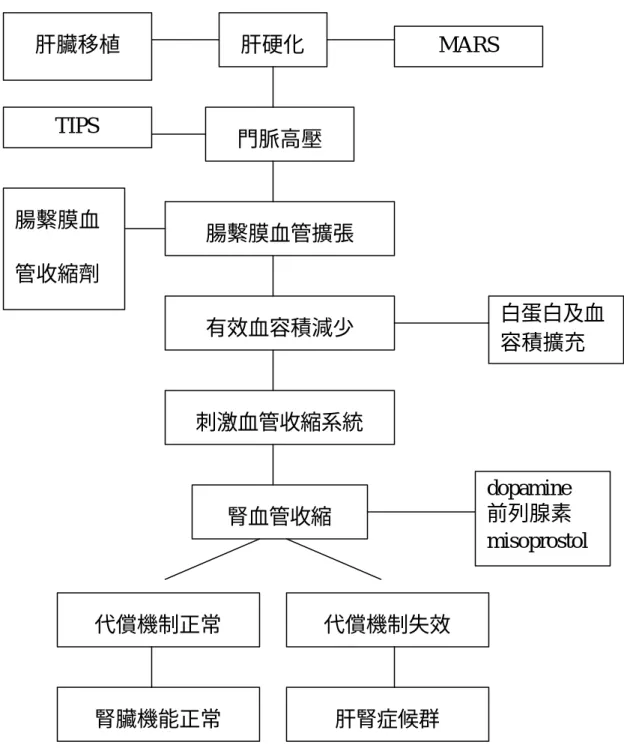
(7) 圖. 目. 錄. 圖 1:由周邊血管擴張理論所推演出的肝腎症候群病理機轉 和它的治療方式………………………………………………46 圖 2:接受 Dopamine 及 Octreotide 治療的患者尿素氮的變化 …47 圖 3:接受 Dopamine 及 Octreotide 治療的患者肌酸酐的變化 …48 圖 4:接受 Dopamine 及 Octreotide 治療的患者肌酸酐廓清率 的變化……………………………………………………………49 圖 5:接受 Dopamine 及 Octreotide 治療的患者 24 小時尿量 的變化……………………………………………………………50 圖 6:接受 Dopamine 及 Octreotide 治療的患者 24 小時尿液 鈉離子排泄量的變化……………………………………………51 圖 7:接受 Dopamine 及 Octreotide 治療的患者血清 renin 活性 的變化……………………………………………………………52 圖 8:接受 Dopamine 及 Octreotide 治療的患者 aldosterone 的變化……………………………………………………………53 圖 9:接受 Dopamine 及 Octreotide 治療的患者血清 antidiuretic hormone 活性的變化……………………………………………54. 7.
(8) 符號與縮寫 ADH: anti-diuretic hormone ALT: alanine aminotransferase AST: aspartate aminotransferase BUN: blood urea nitrogen Cr: creatinine GFR : glomerular filtration rate IL-6: interleukin 6 MARS: molecular adsorbent recirculating system NO: nitric oxide NOS: nitric oxide synthase NSAIDs: non-steroidal anti-inflammatory drugs PRA: plasma renin activity PT: prothrombin time RAAS: renin-angiotensin-aldosterone system RIA: radioimmunoassay SBP: spontaneous bacterial peritonitis SSTR: somatostatin receptor TIPS: transjugular intrahepatic portosystemic shunt TNF: tumor necrosis factors,. 8.
(9) 第一章 第一節. 前言. 何謂肝腎症候群. 急性肝衰竭(包括猛暴性肝炎及慢性肝炎急性惡化)與末期肝硬 化的患者可發生不明原因的少尿性腎衰竭(oliguric renal failure),患 者在臨床上、實驗室或解剖學上並無証據顯示有引發腎衰竭的其他原 因,而腎臟的組織學變化通常是正常的。這種情形被稱為肝腎症候群 (hepatorenal syndrome)﹝1- 3﹞。 1994 年國際腹水研究俱樂部(International Ascites Club)曾為肝 腎症候群下一個定義﹝4﹞:肝腎症候群為急性或慢性肝病引發重度 肝衰竭和門脈高壓所引起的功能性腎衰竭及其伴隨的症候群稱之。肝 腎症候群患者的主要特徵為全身動脈循環之不正常和內生性血管活 躍系統(endogenous vasoactive systems)的活性增加。在腎臟方面主 要發生腎血管的收縮,進而造成腎絲球濾過率(glomerular filtration rate, GFR)降低。然而,在腎臟以外的全身循環則呈現不同的變化: 由於周邊動脈血管的擴張造成全身血管阻力降低,因而引起低血壓。 當患者發生肝腎症候群時,常表示其肝功能已到了嚴重衰竭的時 候,大多數患者在很短的時間內便會死亡。而目前對於肝腎症候群仍 未有理想的治療方法。. 9.
(10) 第二節. 歷史回顧. 在 19 世紀末、Frerichs 和 Flint 最早描述慢性肝病合併腎功能不 全的現象,並提出相關生理變化的論點﹝5﹞。他們主要的發現是部 分慢性肝病的病人會合併少尿症,但是他們的腎臟在組織學上是正常 的,且沒有蛋白尿的情形。直至 1956 年 Hecker 和 Sherlock 詳細地描 述肝腎症候群的變化,他們認為這個症候群最主要是因為肝衰竭引起 全身循環的變化所致,而且預後極差﹝6﹞。到了 1960 年代,更多的 研究顯示末期肝硬化患者在肝臟機能日益惡化時會伴隨腎臟血流減 少而 GFR 下降,最終進展成肝腎症候群﹝7-12﹞。由於患者體內之 血漿總容積是增加的,故認為腎功能惡化是因有效血容積(effective blood volume)不足所致﹝13﹞。基於此一假設,在 1960 及 1970 年 代肝腎症候群的治療方式大多著眼於增加循環中的血液容積。其中如 LeVeen 分流管就是其中的代表﹝14﹞,但由於其併發症過多且分流 管容易閉塞而不被廣泛地採用。 在 1970 至 1990 年間,醫學界對肝腎症候群的致病機制有更多的認 知。經由對肝硬化合併腹水患者的內生性血管活性系統(endogenous vasoactive systems)的研究顯示,肝腎症候群是由於腎臟血管收縮因 子,包括 renin-angiotensin-aldosterone 系統(RAAS)、交感神經系統 和抗利尿激素(anti-diuretic hormone,ADH)等的活性上升;而腎臟. 10.
(11) 血管擴張因子,包括前列腺素(prostaglandins)及 bradykinin 等減少 而形成之失衡現象所致﹝15-23﹞。 其後從動物及人體的研究發現,肝硬化患者在血液循環所呈現之 異常變化並不是由於血液容積降低所造成,而是因為動脈血管擴張所 致﹝24-26﹞;並且在 1980 年代末期有研究者提出「周邊動脈血管擴 張學說」(“peripheral arterial vasodilatation theory”)﹝27﹞。 在 1990 年代早期,則有研究者認為一氧化氮(nitric oxide, NO) 在肝硬化患者的循環異常扮演著重要的角色﹝27-29﹞,而血管擴張 的位置就在內臟的血液循環中。因此,門脈高壓導致內臟動脈血管擴 張便被視為肝腎症候群的起步點。基於此一理論,能令內臟血管收縮 的葯物便開始被試用於肝腎症候群的治療﹝30-32﹞。自此,對於從 前被認為預後極差的肝腎症候群,似乎又重燃希望。. 11.
(12) 第三節. 流行病學. 台灣是 B 型肝炎的流行區,成年人口中約五分之一為慢性肝炎 帶原者,約佔三百萬人口﹝33,34﹞。此外 C 型肝炎在台灣地區亦十 分常見,它的盛行率在都會區的正常成人約佔 1%左右﹝35,36﹞,但 在較偏遠地區則盛行率超過 10%,而且仍在蔓延中﹝37,38﹞。因此, 肝硬化及其併發症始終保持在我國十大死亡原因的榜單之上 ﹝39﹞。而根據衛生署西元 2001 年的統計,肝癌佔台灣地區男性癌 症死亡率之第一位,女性則佔第三位,而國人十大死亡原因以惡性腫 瘤為榜首;慢性肝疾病及肝硬化則佔十大死亡原因第六位。又根據統 計,肝硬化合併腹水的患者中每年約有 8%可發生肝腎症候群 ﹝40﹞,因此肝腎症候群是國內肝病醫學界一個並不罕見而又難以處 理的狀況。. 12.
(13) 第四節. 臨床表徵. 肝腎症候群的臨床表徵可分三大方面: (1)肝衰竭; (2)全身循 環異常;及(3)腎衰竭。 在肝衰竭方面,所有肝腎症候群的患者都有腹水,而且通常是非 常大量,並且呈現其它門脈高壓的臨床特徵。至於黃疸或肝腦病變的 程度,則在患者之間有極大的差異。在發生肝腎症候群之前,病人可 能曾遭遇一些會令有效血液容積下降的情況,如大量放出腹水、使用 大量利尿劑來治療腹水、併發自發性細菌性腹膜炎(spontaneous bacterial peritonitis, SBP),或消化道出血等。這些情況到底是誘發肝 腎症候群的因素抑或只是患者因肝衰竭合併大量腹水所引起的伴隨 狀況卻是難以定論。在全身循環異常方面,肝腎症候群的患者常有高 的心輸出量(cardiac output)﹝41,42﹞、低的動脈壓(患者平均動脈 壓在 60 至 80 mmHg 之間)﹝ 43﹞和全身血管阻力( systemic vascular resistance)減少,這會造成血管收縮系統(如:RAAS 和交感神經系 統)的活性。另外在腎血管方面會增加腎血管的阻力,最近更發現在 上肢和下肢血管及腦循環方面也會增加血管阻力﹝44,45﹞。因此大 多數患者的血壓都會稍為偏低,到了末期更會發生顯著的血壓下降。 在腎衰竭方面,肝腎症候群的患者常合併鈉和水份在身體內堆積,形 成腹水、水腫和稀釋性低血鈉血症( dilutional hyponatremia) 。患者腎. 13.
(14) 功能惡化的速度可以非常快速,有些病人原先的腎功能本在正常範圍 以內,卻會在數天內急速惡化。患者的預後甚差,存活時間常在數週 以內,這些病患被歸類為第一型肝腎症候群﹝10﹞。一些在非肝病引 起的急性腎衰竭常見到的情況,如:嚴重高血鉀血症,嚴重代謝性酸 中毒及肺水腫等,在第一型肝腎症候群的患者是較少見的。直至 10 年以前,醫界仍以為只要發生肝腎症候群,病人大多快速死亡。若能 僥倖存活者,便要懷疑病人的腎功能衰竭並非由於肝腎症候群所致, 因為認為肝腎症候群之存活者是非常罕見的,甚至值得作病例報告 ﹝46﹞。然而在近幾年來陸續有報告提出有些肝腎症候群的患者其腎 功能的惡化速度較為緩慢,存活時間可達數個月以上,這種情況被歸 類為第二型肝腎症候群(表 1)。 病患在臨床上除了表現出少尿性腎衰竭之外,最大特色是在尿液 檢查的特徵。患者尿液中的鈉含量甚低而腎仍具有某一程度之濃縮功 能,在尿液生化學檢查與血容積過低(hypovolemia)所造成的腎前 氮血症(prerenal azotemia)不易區分(表 2)。唯一不同者是對於治 療的反應:腎前氮血症患者在給予體液的補充之後,腎功能可穫得改 善,而肝腎症候群者則不會改善。. 14.
(15) 第五節. 發病原理(pathogenesis). 有關肝腎症候群的發病原理至今仍未完全明瞭,但基於下列三個 理由,研究者皆認為肝腎症候群是屬於功能性的腎衰竭,在腎絲球或 腎小管處並無病灶或損傷: (1)肝腎症候群患者的腎臟組織學檢查完 全正常; (2)若將肝腎症候群患者的腎臟移植至沒有罹患肝病的腎衰 竭病人身上,腎臟即可發揮功能﹝47﹞; (3)肝腎症候群患者接受肝 臟移植成功後,其腎功能可逐漸恢復正常﹝48﹞。在目前,一般以為 肝腎症候群與門脈高壓造成之周邊動脈血管擴張甚有關聯﹝27﹞。 1. 周邊動脈血管擴張學說﹝4﹞ 肝硬化的併發症,包括消化道靜脈曲張出血、肝腦病變、腹 水、肝腎症候群及肝肺症候群等,除了與肝細胞數目不足導致功 能衰竭有關外,另一重要的機制就是門脈壓力上升。而門脈高壓 引發上述的併發症,則是透過周邊動脈血管擴張所引發的連鎖效 應而來。 周邊動脈血管擴張學說是敘述肝硬化發生之後,因門脈高壓 導致側枝循環,原先該由肝臟代謝的物質自側枝循環流去而沒有 進入肝臟,因而在體循環的血液中濃度上升,這些物質可直接或 間接地引起周邊血管擴張,導致有效血容積下降。因此,在血流 動力學上出現兩個現象: (1)血壓下降; (2)周邊血管阻力下降。. 15.
(16) 為要因應這些變化所帶來的負面效應,身體便會做出代償反應, 其中包括: (1)增加交感神經系統活性—在心臟的效應是增加心 輸出率,而在皮膚及內臟之血管則會收縮。 (2)RAAS 活性增加, 將水分和鈉儲留體內,以補充身體的有效血容積。但由於體內的 水分和鈉的總量增加,便造成腹水更加嚴重﹝16,49,50﹞。 2. 在腎臟引起的效應 由於周邊動脈血管擴張,導致全身血流動力學的連串變化, 每一個環節都可能對腎臟造成影響: a. 血壓下降:由於平均動脈壓下降,腎的灌注壓也跟著下降, 造成腎血流降低。 b. 交感神經活性增加:會引起腎臟血流及腎絲球率過濾降低。 阻斷腎臟交感神經系統,則可獲得改善﹝51﹞。 c. RAAS 活性增強:除了因 aldosterone 引發留水留鈉的效應 外,具有強力血管收縮功能的 angiotensin II 會造成腎臟血管 的收縮,使腎血流量銳減。 3. 伴隨狀況對腎臟的影響 a. 從周邊動脈血管擴張理論可知,門脈高壓可造成水份和鈉堆 積於體內,因而引發惡性循環,門脈壓力更高,可導致消化 道靜脈曲張出血,情況大多嚴重,常造成血壓下降,腎臟灌. 16.
(17) 流降低而致腎臟受損。 b. 由於腹水的積聚,病人常會接受利尿劑或大量放水治療,可 導致腎臟受損。 c. 伴有大量腹水的肝硬化患者,較一般人容易發生菌血症或自 發性細菌性腹膜炎,常需使用 aminoglycosides 等抗生素,可 能導致腎功能受損。 4. 腎臟本身的代償作用 由於上述的各種狀況,重度肝衰竭或末期肝硬化的患者,其 腎臟經常處於容易受損的狀況。臨床上發生肝腎症候群的患者絕 大多數伴隨有嚴重的腹水;反之,有嚴重腹水的肝病患者卻不一 定有腎功能障礙。由此可以推斷,患有重度肝病及伴隨大量腹水 的患者,其腎臟雖處於危機四伏的環境,但若有充分的代償機制 來避免腎臟血流及腎絲球過濾率的減少,便不會出現腎功能惡化 的情形。但若此代償機制失效,則因腎臟血管過度收縮而終至發 生肝腎症候群。 這些代償機制包括: a. 前列腺素(prostaglandins):代償不良的肝硬化患者中,腎 功能正常者其腎臟產生之前列腺素增加﹝21,22,52﹞。但在 發生肝腎症候群的患者,其尿中前列腺素 E2 和 prostacyclin. 17.
(18) 的代謝物 6-oxo-PGF1α均減少﹝53,54﹞。此外,使用非類固 醇抗發炎藥(non-steroidal anti-inflammatory drugs, NSAIDs) 可能導致伴有大量腹水的肝硬化病人出現腎功能衰竭 ﹝55﹞。 b. Kallikrein-kinin 系統:腎臟產生 kallikrein 是防範肝腎症候群 發生的代償機制之一,若 kallikrein 產生不足,便可能導致 腎功能的衰竭﹝23﹞。 5. 參與肝硬化患者腎灌流調節的其他重要因子 a. NO:在 1990 年代 NO 被視為引發肝硬化患者循環異常的重 要因素﹝28,29,56﹞。它會引起內臟循環之動脈血管擴張, 但卻在肌肉、皮膚、腎臟及腦部呈現血管收縮﹝44,57-59﹞。 肝硬化患者內臟血管內皮細胞之 NO 合成? (nitric oxide synthase, NOS)活性增加,因而產生較多的 NO﹝60﹞。對 正常動物和人類短時間地抑制 NOS 活性會引起腎血管收縮 和腎血流減少﹝61,62﹞;但在肝硬化合併腹水的老鼠,抑制 NOS 的活性並不會影響腎血流和腎功能﹝63,64﹞。這是由 於 肝 硬 化 老 鼠 的 NOS 受 抑 制 時 腎 臟 會 產 生 較 多 的 prostacyclin 作為代償;若同時抑制 NO 及 prostacyclin 則會 令腎臟血流明顯下降﹝63﹞。由此可知,在發生肝硬化時,. 18.
(19) 身體的腎臟血流係由 prostacyclin 及 NO 來合作維持。 研究顯示,nitrite 在門脈高壓老鼠腎絲球的合成增加 ﹝65﹞,在肝臟患者尤其合併腹水者的尿中 nitrate 的分泌也 上升﹝66﹞。並有證據指出肝硬化合併腹水的病人腎臟微循 環(microcirculation)的 NO 是不敏感的﹝28﹞。對於肝硬 化合併腹水的患者,注射一氧化氮的類似物 L-arginine 會引 起 natriuresis,並且會增加尿液中的 nitrate 及 nitrite﹝67﹞。 b. Natriuretic peptides:肝硬化患者在腎功能仍正常時,血中 natriuretic peptides 濃度上升﹝68﹞。在動物實驗中,正常老 鼠的 natriuretic peptides 受體(receptor)若被阻斷,其腎臟 血流將會減少;而此種情況在肝硬化合併腹水的老鼠則更為 嚴重﹝69﹞。若使用 acetylcysteine 使 natriuretic peptides 增 加,則可使肝腎症候群患者腎血流增加而腎功能改善 ﹝70﹞。 c. Endothelin-1:曾有研究報告指出 endothelin 與肝硬化及肝腎 症候群有關﹝71,72﹞,然而,endothelin 卻與這些病患腎功 能 惡 化 並 無 關 聯 ﹝ 73﹞ 。 使 用 經 頸 肝 內 門 脈 全 身 分 流 (transjugular intrahepatic portosystemic shunt, TIPS)治療 後,腎功能改善與 endothelin 也沒有相關性﹝74﹞。. 19.
(20) 第六節 診斷 肝腎症候群並無特異性的診斷方法( specific diagnostic tests) ,其 診斷的標準如表 3 所示﹝4﹞。依據診斷標準,患者除罹患急性或慢 性肝病並導致嚴重肝衰竭(常伴隨大量腹水)和門脈高壓外,還須符 合下列各項: (1)腎絲球濾過率下降、血肌酸酐值大於 1.5 mg/dl 或 在沒有利尿劑的治療作用下 24小時肌酸酐清除率小於 40 ml/min。 (2) 必須排除其它引起腎衰竭的原因,如:休克、細菌性感染、大量體液 流失、最近使用腎毒性藥物(如非類固醇抗發炎藥或 aminoglycosides)。(3)即使給予大量輸液或血漿製劑注射亦無法改 善腎功能。 (4)每天排泄的尿蛋白小於 500 毫克,且沒有阻塞性腎病 變或間質性腎疾病。但必須注意的是,由於末期肝硬化患者常伴隨營 養不良,全身的肌肉質量顯著減少,故血中肌酸酐濃度在腎功能正常 時便低於常人。因此,若以血清肌酸酐濃度來作為腎功能的指標,常 會低估腎功能惡化的程度。 以上是診斷的主要條件,必須全部符合。此外,還有一些附加條 件,雖然在診斷上不需完全符合,但可加強診斷的支持度。附加條件 包括: (1)每天尿量小於 500 毫升;(2)尿中鈉含量小於 10 meq/l; (3)尿中滲透壓大於血漿中滲透壓; (4)每一高倍鏡視野下尿中紅 血球數小於 50 ;(5)血漿中鈉的濃度小於 130 meq/l。. 20.
(21) 第七節 治療 在 1990 年代中期以前,醫學界均認為肝腎症候群是一種預後極 差且無法以葯物來治癒的「不可逆」情況。過去數十年來曾經被嘗試 使用的葯物包括:dopamine﹝75﹞、前列腺素﹝76,77﹞、misoprostol ﹝77﹞、norepinephrine﹝78﹞、metaraminol﹝79﹞,以及 fenoldopan、 saralasin、phentolamine、dazoxiban 和 ocatpressin 等﹝80﹞血管活性 葯物,但均無法顯著或持續地改善患者的腎功能。故一般認為肝臟移 植是肝腎症候群最有效的治療方式﹝48,81﹞。然而,由於肝腎症候 群患者接受肝臟移植的併發症較多而存活較低﹝82,83﹞,並不能讓 人滿意;加上對肝腎症候群的發病原理有更深入的了解而令研究者對 藥物治療的發展較具信心,故近年來醫學界對於肝腎症候群的處理又 再燃起新的希望,因此不斷地嘗試用內科治療方式來改善肝腎症候群 病患的腎功能,使病患的肝臟移植的成功率較高或是使病患等待較適 宜的肝臟來移植。 目前對於肝腎症候群的治療可分為四類:(1)藥物治療、(2) TIPS、(3)分子吸附劑再循環系統(molecular adsorbent recirculating system, MARS) 、 (4)肝臟移植。 (圖 1) 1. 藥物治療 基於周邊動脈血管擴張學說,肝腎症候群的起源是因門脈高. 21.
(22) 壓導致內臟血管擴張而造成全身有效血容積不足,故補充血容積 再配合血管收縮劑( volume expansion and vasoconstrictors)便成了 目前對肝腎症候群藥物治療的主流,曾被使用的藥物包括 vasopressin、ornipressin、terlipressin 及 octreotide 等,其療效及副 作用分述如下: a. Ornipressin Ornipressin 為 vasopressin-l receptor agonist,是最早被用作 治療肝腎症候群的腸繫膜血管收縮劑﹝30-32,75,84﹞,通常合 併血漿容積擴張劑(如 albumin)來使用。Ornipressin 能有效地 抑制 RAAS 和交感神經系統,長時間注射雖能改善腎血流量和 腎功能,但是由於有血管缺血的副作用(包括內臟缺血及致命 性的心律不整)而限制了它的臨床使用﹝75,84﹞。 b. Terlipressin Terlipressin 也是 vasopressin-l receptor agonist,短期的治療 即能增加肌酸肝的廓清率和增加每日之尿排出量﹝85﹞,經過 5 至 15 天治療之後,RAAS 的活性也被抑制,而且病人沒有血 管 缺 血 的 副 作 用 ﹝ 86,87﹞ , 部 分 患 者 在 停 藥 後 沒 有 復 發 ﹝87﹞,因此認為 terlipressin 的安全性比 ornipressin 好。在 2001 年,Ginés 等人﹝88﹞研究發現使用 terlipressin 來治療肝腎症候. 22.
(23) 群必須配合白蛋白的補充才能發揮效果。 c. Vasopressin 由於 terlipressin 及 ornipressin 均具有療效,故理論上以 vasopressin 來治療肝腎症候群也應有效。但從使用 terlipressin 及 vasopressin 來治療食道及胃靜脈曲張的經驗,vasopressin 之 安全性及方便性均比不上 terlipressin﹝89-91﹞,故目前僅有以 低劑量及短療程的臨床試驗,顯示治療後病人尿液排出有明顯 改善﹝92﹞。 d. Octreotide Octreotide 為 長 效 型 的 somatostatin 衍 生 物 , 它 作 用 在 somatostatin receptor l(SSTR1)和 SSTR4,使血管平滑肌收縮 ﹝93,94﹞。由於它可選擇性地使腸繫膜血管收縮,因此能降低 門脈壓,使血液回流至全身血管中。單獨使用 octreotide 來治療 肝腎症候群,能令肌酸酐和肌酸酐廓清率皆有改善,但是停藥後 肝腎症候群容易得復發﹝95﹞。若以 octreotide 合併 midodrine (一種α-adrenergic agonist)和白蛋白來治療,則較 dopamine 合併白蛋白更能明顯地增加患者的腎血流量和腎絲球濾過率、降 低 RAAS 的活性,而且沒有血管缺血的副作用﹝96﹞。 從上述研究可推斷:(1)合併使用靜脈注射白蛋白和血管收. 23.
(24) 縮劑能使第一型肝腎症候群情況逆轉; (2)但單獨使用任何一種 均無效;(3)ornipressin 會併發缺血性併發症; (4)這些治療方法 可增進存活率及使較多的病人能等到肝臟移植﹝3﹞。 2.. TIPS 由於門脈高壓被認為是肝腎症候群的起始步驟,以分流方法 降低門脈壓力來作為治療肝腎症候群是一個合理的構思。雖然曾 經有些病例報告敘述有病人在接受分流手術之後其肝腎症候群得 到改善﹝97,98﹞,但肝腎症候群患者大多數無法承受這些重大的 手術。因此,TIPS 被引用至臨床治療之後,便受到評估是否適合 用來治療肝腎症候群。 當 TIPS 成功地置入之後,除了可以降低門脈壓,並且可以改 善病人的腎功能、﹝74,99-103﹞,但約有近半的患者產生肝腦病 變或原有的肝腦病變呈現惡化。雖然初步的研究顯示 TIPS 與藥物 治療均可改善肝腎症候群,但至於何者較優及如何選擇病患,則 仍有待進一步的研究。. 3.. 分子吸附劑再循環系統 MARS 是一種特殊的透析方法,利用含有白蛋白的透析液選 擇性地移除與白蛋白結合的物質,包括許多毒素及腫瘤壞死因子 (tumor necrosis factors, TNF)和第六間白質(interleukin 6, IL-6). 24.
(25) 等細胞激素(cytokines)﹝104,105﹞。傳統的透析對肝腎症候群 並無顯著效益,而接受有 MARS 相輔的透析者除了血清膽紅素下 降外,腎功能及存活時間均獲改善﹝106﹞。然而,由於 MARS 耗費甚高且效果短暫,目前僅考慮作為等候肝臟移植的橋樑及仍 規範於臨床試驗中使用。 4.. 肝臟移植 肝臟移植仍是肝腎症候群的首選療法﹝81,107-110﹞。在移植 手術完成之後,患者的腎功能會更為惡化,其中約有三分之一需 要透析治療。肝腎症候群患者在肝臟移植之後會較沒有肝腎症候 群的患者有較高之術後死亡率,但在情況穩定之後其長期存活率 則不差,三年存活率可達 60% ﹝81,107-110﹞。 但由於第一型肝 腎症候群患者常在兩週內死亡,能等到捐贈的肝臟機會甚微,因 此,仍必須研發其他有效的治療來延長這類病人的生命,使能有 較大的機會接受肝臟移植。. 25.
(26) 第八節. 本研究所探討之假說. 從過往研究所得的結論包括: (1) 第一型肝腎症候群患者常在兩週內死亡,能等到捐贈的肝 臟機會甚微,因此,有效的藥物療法仍亟待研發。 (2) 合併使用靜脈注射白蛋白和血管收縮劑是目前已知最能使 第一型肝腎症候群情況逆轉之搭配。但單獨使用任何一種 均無效。 (3) 如 ornipressin 及 vasopressin 會併發缺血性併發症,選擇用 藥時必須考慮安全性。 (4) 這些治療方法似乎可以增進存活率及使較多的病人能等到 肝臟移植,但目前的藥物搭配仍未達理想。 基於上述論點,我們有下列兩個假設: (1) 最佳的藥物搭配組合除了包括一種安全而有效的內臟血管 收縮劑及配合白蛋白的補充之外,還應加上另一種作用位 置不同的藥物(圖 1)。 (2) 兩類藥物並非必須同時給予,應按照其作用機制來考量用 藥的時機。. 26.
(27) 第九節. 研究目的. (1) 研發對第一型肝腎症候群更有效的藥物治療(使用 octreotide 及 低劑量 dopamine)。. 27.
(28) 第二章 第一節. 研究方法. 研究設計. 本研究是採前瞻性隨機控制研究。. 28.
(29) 第二節. 材料. 1. 病人 自 2000 年 7 月至 2002 年 3 月間在中國醫藥學院附設醫院住院的 肝硬化病患如併發第一型肝腎症候群者都列為研究對象。肝硬化的診 斷主要是根據臨床症狀、實驗室數據、腹部超音波或電腦斷層,第一 型肝腎症候群的診斷則如前所述(表 3)﹝4﹞。患者如有下列情形, 則排除在本研究之外: 甲、 患者最近有腸胃道出血,肝腦病變,感染等併發症。 乙、 發現肝癌或其它器官之惡性腫瘤。 丙、 出現嚴重心衰竭,非常難控制的糖尿病或其它非常嚴重的全 身性疾病。 丁、 不願配合本研究流程的患者。 戊、 患者有休克,大量體液流失,最近使用腎毒性藥物治療。 2. 藥物 除了給予白蛋白的補充外,用作治療的藥物包括: 甲、 Octreotide(諾華、巴塞爾、瑞士) 乙、 Dopamine(Orion、Espoo、芬蘭). 29.
(30) 第三節. 方法. 對於符合條件的患者,先予病人或家屬解釋本研究的醫療過程, 待獲得同意並簽署同意書後以隨機分配方式分為四組,在治療前 5 天 停止利尿劑的使用,然後接受不同的治療: 第一組:先以 dopamine 2-4 µg/kg/min 持續注射 5 天,後以 octreotide 100 µg 注射後,25 µg/hr 持續注射 5 天,這 10 天中每天注射 20% 白蛋白 50 至 100 毫升。 第二組:先以同上劑量 octreotide 注射 5 天,再以 dopamine 注射 5 天, 這 10 天中每天也注射同劑量的白蛋白。 第三組:以 dopamine 2-4 µg/kg/min 持續注射 10 天。 第四組:不注射 octreotide 或 dopamine,觀察 10 天 四組病人均於治療前後抽血檢查肝功能和腎功能,包括氨基丙酸 胺基轉移酵素(alanine aminotransferase, ALT )、天門冬酸胺基轉移酵 素(aspartate aminotransferase, AST)、膽紅素(bilirubin)、凝血酵素 原時間( prothrombin time, PT) 、白蛋白( albumin)和氨(ammonia); 以及血尿素氮(blood urea nitrogen, BUN)、肌酸酐(creatinine, Cr) 和肌酸酐清除率等。並且計算病人的每日尿液總量。第一、二組加抽 血液測定血漿腎素活性( plasma renin activity, PRA)、皮質醛酮 (aldosterone)、抗利尿賀爾蒙(anti-diuretic hormone, ADH)濃度,. 30.
(31) 並留 24 小時尿液來測算尿鈉含量。 在治療期間的追蹤包括:每 6 小時測量病人血壓、心跳;每天計 算病人尿液總量;每天測量病人體重並記錄病人的副作用,第 5 天和 第 10 天抽血追蹤病人的肝功能和腎功能。在治療期間,鹽份和水份 的攝取均予嚴格限制(水每天≤ 1 公升,鈉≤ 40 meq/天) ,若需要腹水 釋放,則每天以小於 5 公升為原則,且每釋放 1 公升腹水,必需注射 5 公克白蛋白。 PRA、aldosterone 及 ADH 血中濃度的偵測係以放射免疫分析法 (radioimmunoassay, RIA)測量。其中 PRA、ADH 之檢體收集方式 為:抽血(PRA 3 ml,ADH 10 ml)置入 EDTA 管在 4℃保存,後用 3000xg 離心 15 分鐘,取 plasma。Aldosterone 之檢體收集方式為:抽 血 3 ml 置入 SST Gel 管,在室溫下用 3000xg 離心 15 分鐘,取 serum。 • 測 aldosterone 的試劑為 SPAC-S Aldostorone Kit ( Daichii,日本) • 測 PRA 的試劑為 plasma renin activity RIA Kit ( Dia Sorin,日本) • 測 ADH 的試劑為 ADH RIA Kit ( Dia Sorin,日本). 31.
(32) 第四節. 統計分析. 1. t 檢定(Student’s t test):檢定兩組間連續數據的差異。 2. 配對 t 檢定(Paired t test):檢定同一組別在治療過程中連續數據 的變化。 3. Kruskal-Wallis ANOVA:檢定各組間連續數據的差異。 4. Student-Newman-Keuls method:各組間以 ANOVA 檢定呈 p 值<0.05 時採用為組與組間相互多次比較。 5. p 值<0.05 視為具有統計學的意義,連續數據以 mean ± SD 來表示。. 32.
(33) 第三章. 研究結果. 一、病人的基本資料及狀況 共有 24 名患者符合本研究的納入標準並同意接受治療,經隨機 分配每組個案各為 6 人(表 4)。其中 21 名為男性,3 名為女性;平 均年齡為 50.0 至 55.0 歲(從 36 歲至 69 歲),4 組之間並無差異。肝 硬化的成因中 12 名為 B 型肝炎,5 名為 C 型肝炎,7 名為酒精性肝 炎,在 4 組中肝硬化的原因沒有明顯的差別。住院時 4 組的肝功能 (ALT、AST、白蛋白、膽紅素、凝血酵素原時間)及腎功能(血尿 素氮,肌酸酐)均沒有明顯差異(表 4)。. 二、腎功能之變化 四組接受不同治療的患者其腎功能變化如表 5 所示。血尿素氮濃 度在第一,二組均有顯著下降而第三、四組則均有惡化。但第一、二 組血尿素氮濃度之改善程度並未達到明顯的不同。但在肌酸酐方面, 同樣是在第一,二組均有顯著下降而第三、四組則均有惡化,與血尿 素氮不同的是第二組肌酸酐之下降程度顯著地超過第一組 (p<0.05)。雖然第一、二組病患在接受治療後腎功能皆有改善,但 無論是血尿素氮或肌酸酐,其顯著改善的時刻都是出現在使用 octreotide 的時候。如第一組在前 5 天接受 dopamine 治療,在第 5 天. 33.
(34) 之血尿素氮濃度、肌酸酐濃度和肌酸酐清除率等均與治療前並無顯著 差異,直至使用 octreotide 5 天之後,此 3 項腎功能檢查才明顯地進 步(圖 2 - 4) 。第二組患者在前 5 天使用 octreotide,在第 5 天之血尿 素氮濃度、肌酸酐濃度和肌酸酐清除率均較治療前呈現顯著改善,在 第 6 至 10 日使用 dopamine,則各項腎功能指標呈現繼續進步的趨勢 (圖 2 - 4)。 雖然第一組患者在前 5 日使用 dopamine 時各項腎功能指標並未 進步,但患者的排尿量與尿鈉排泄量均已顯著上升;而無論在第一或 第二組,這兩項指標的改善程度在使用 octreotide 時尤為顯著(圖 5、 6)。. 三、相關激素的變化 無論是 PRA、皮質醛酮或 ADH,其中的變化與腎功能的變化相 似:如第一組在前 5 天接受 dopamine 治療,在第 5 天之 PRA、皮質 醛酮和 ADH 均與治療前並無顯著差異,直至使用 octreotide 5 天之 後,此 3 項檢查才明顯地進步(圖 7 - 9)。第二組患者在前 5 天使用 octreotide,在第 5 天之 PRA、皮質醛酮和 ADH 均較治療前呈現顯著 改善,在第 6 至 10 日使用 dopamine,則各項指標呈現繼續進步的趨 勢(圖 7 - 9)。. 34.
(35) 四、預後 在治療期間沒有一人發生任何不良副作用和併發症。雖然 4 組患 者的住院平均天數沒有明顯差異(表 5) ,但 30 天存活率則並不相同: 第一組有 6 位(100%)、第二組 5 位(83%),第三組 4 位(67%), 第 4 組 2 位(33%) 。而存活大於 6 個月以上者,第一組有 3 位(50%) , 第二組 3 位(50%),第三組 1 位(17%),第 4 組 0 位。. 35.
(36) 第四章. 討 論. 依據周邊動脈血管擴張學說﹝4﹞及過去幾年來以內臟血管收縮 劑治療肝腎症候群的療效﹝31-33,81-86,90,93,94﹞,本研究的假設是 (1)肝腎症候群的理想藥物治療應包括血液容積的補充(靜脈注射 白蛋白)加上兩種作用機制不同的藥物治療。 (2)藥物給予的時間並 非一定要同時給予,可依其作用機制不同而在不同時機給藥。 接受治療的四組病人之中以第二組療效最為顯著,他們是先接受 5 天的 octreotide 然後再接著接受 5 天的 dopamine。在注射 octreotide 期間無論是腎功能(血尿素氮、肌酸酐及肌酸酐清除率)、尿量及尿 鈉排泄量,以及相關的激素(PRA、aldosterone 及 ADH)均有顯著 的改善,顯見 octreotide 對肝腎症候群是具有療效的。在隨後的 5 天, 給予低劑量的 dopamine,結果顯示病患的腎功能等繼續獲得改善, 可見肝腎症候群患者在接受門靜脈減壓之後接著使用增加腎臟血流 的藥物,後者仍能發揮治療的效果。而相對地,第一組患者在前 5 天 接受 dopamine 及第三組病患連續 10 天使用 dopamine 的期間,均未 見腎功能獲得明顯的改善,再度證實單獨使用 dopamine 來配合白蛋 白的補充,並不能產生實際療效﹝71﹞。 較為特別的發現,是第一組患者在前 5 天使用 dopamine 時,雖 然腎功能並沒有改善,但亦未有顯著惡化,在第 6 至 10 天使用. 36.
(37) octreotide 後腎功能即有明顯好轉的現象,而且預後並不比第二組差, 顯示當肝腎症候群發病之初,使用低劑量 dopamine 仍具有短暫保護 腎臟的效用,待加上或改用內臟血管收縮劑時情況便得到改善。但發 生肝腎症候群至開始使用內臟血管收縮劑的時間間格不宜過長,否 則 在發病 10 天以後腎功能便更益惡化,此時預後便會更差。 此外,另一個顯示 dopamine 具有潛在保護效益的證據是在使用 dopamine 期間病人的尿量及尿鈉排泄量會增加,但這種保護的效益 能維持多久仍有待進一步的探討。 本研究的血管收縮劑採用 octreotide 主要是基於安全性的考量。 由於 ornipressin 會引起缺血性併發症的機率頗高,已被認為不宜廣泛 地使用﹝81,82﹞;而 vasopressin 具有相同的不良副作用,故亦少被 採用。目前報告得最多的是 terlipressin,主要是因其安全性及方便性 皆優於 ornipressin 和 vasopressin﹝84,85,87-89﹞。至於另一種到近年 才被用作治療消化道靜脈曲張出血的藥物 octreotide,目前全世界對 其使用於治療肝腎症候群的經驗十分有限,而且並未有比較其與 terlipressin 對肝腎症候群治療的效益及副作用的研究報告。但基於使 用 octreotide 及 terlipressin 來治療消化道靜脈曲張出血的經驗, octreotide 的安全性優於 terlipressin,而且價格比較便宜,因此我們採 用 octreotide﹝111,112﹞。而從本研究的結果顯示,octreotide 的安全. 37.
(38) 性甚高,受試患者中並無一人發生血管缺血的副作用。 雖然在過去的研究顯示,單獨使用 dopamine 並不能扭轉肝腎症 候群患者的預後﹝71﹞,但低劑量的 dopamine 能增加腎臟的血流卻 是不爭的事實﹝113-115﹞。本研究採用 dopamine 作為輔助藥物,發 現在使用血管收縮劑(octreotide)5 天之後,在門脈高壓下降及腎功 能漸漸改善的時候換用 dopamine 繼續使用 5 天,竟能令腎功能持續 地進步,前後用藥共 10 天,大多數病患的病情都能逆轉回來。至於 可否採用其他能改善腎臟血流的藥物來取代 dopamine 以期產生相同 或更佳的效果,則有待進一步的探討。 就以往的經驗顯示,無論是採用任何一種血管收縮劑,少於 5 天 的治療只能令肝臟症候群患者的情況暫為的改善,不久即會再度惡化 ﹝81,93﹞。故一般建議用藥起碼要超過 5 天,甚至用到 15 天。然而, 上述提及曾用來治療肝腎症候群的血管收縮劑均非常昂貴;而且,大 多有缺血性的併發症,若使用 10 天或更久,則除了醫療費用大增之 外,亦可能增加副作用的機會。因此,若從本研究的結果推論,使用 octreotide 10 天甚有可能發揮與第二組用藥同樣的療效,但在醫療花 費及副作用的考量下似乎並不值得推薦。 此外,還有一種用藥在搭配沒有在本研究中採用,就是在最初開 始治療的 5 天即合併使用 octreotide 及 dopamine。此種合併用藥的可. 38.
(39) 能優點有兩個: (1)療效更快出現,便可減少病人住院的天數; (2) 療效更加顯著,增進病人的預後。但從本研究的結果顯示,雖然四組 患者的預後不同,但住院天數相近,正反映出發生肝腎症候群的病 患,除了腎功能衰竭之外,還有許多與肝衰竭相關的情況需要照顧, 除了死亡病例以外,大多數不會在短期內出院。因此,合併使用 octreotide 和 dopamine 恐怕不容易達成減少住院天數的目標。而在第 一和第二組病人的預後來看,以這兩種組合治療的效果已經很好,故 同時使用 octreotide 及 dopamine 似難有更佳的結果。然而,本研究當 初設計時並沒有採用同時使用 octreotide 及 dopamine 的主要理由是希 望能更明確地釐清兩種藥物各自的治療效益,故會在第一和第二組分 開用藥的時間。當然,如果加入第五組來採用同時合併治療將會有更 確實的數據支持我們上述的論點,但由於在設計本研究時已考量到病 患的收納不容易,若分為 5 組則可能無法在預訂期間內完成計畫,故 仍只分為四組。在未來的研究中我們將會把此一議題加以進一步的評 估。雖然本研究的結果能清楚地呈現出 octreotide 及 dopamine 的療 效,但因個案數目仍嫌偏低,故必須有進一步較大規模的研究來確認 及推廣本研究的及對肝腎症候群的致病機制。 本研究的結論為:(1)以 octreotide 配合白蛋白的補充及繼之以 dopamine 來治療第一型肝腎症候群是一個安全而有效的療法;(2) 39.
(40) 藥物治療 10 天以後可扭轉肝腎症候群的進展; (3)單獨使用 dopamine 治療不能改善患者的腎功能,但可短暫性地增加尿量及尿鈉排泄量; (4)進一步的研究仍有必要。. 40.
(41) 表 1. 肝腎症候群兩個臨床類型的特色 第一型肝腎症候群 •腎功能快速惡化 •兩星期內血漿肌酸酐升至 2.5 mg/dl 以上或 24 小時肌酸酐廓清 率小於 20 ml/min •存活時間約數週 第二型肝腎症候群 •腎功能慢慢惡化 •存活時間約數個月. 41.
(42) 表 2. 肝腎症候群,腎前氮血症,急性腎衰竭在尿液生化學及常規檢 查上的異同 肝腎症候群. 腎前氮血症. 急性腎衰竭. 尿鈉濃度(meq/l). <10. <10. >30. 尿/血漿肌酸酐比例. >30:1. >30:1. <20:1. 尿液滲透度. 比血漿滲透 度至少超過 100 mOsm. 比血漿滲透 度至少超過 100 mOsm. 與血漿滲透 度相同. 尿液沈澱物. 正常. 無顯著異常. 有細胞柱及 壞死物. 42.
(43) 表 3. 肝腎症候群的診斷標準[4]* 主要條件 •低的腎絲球濾過率,血漿中肌酸肝大於 1.5 mg/dl 或 24 小時肌酸酐 清除率小於 40 ml/min •沒有休克,細菌性感染,大量體液流失,最近使用腎毒性的藥物 •停用利尿劑和血漿製劑注射 1.5 公升後,腎功能沒有改善(肌酸酐 沒有小於 1.5 mg/dl 或 24 小時肌酸酐清除率沒有大於 40 ml/min) •蛋白尿小於 500 毫克/天,且沒有阻塞性腎病變或間質性腎疾病 附加條件 •每天尿量小於 500 毫升 •尿中鈉含量小於 10 meq/l •尿中滲透壓大於血漿中滲透壓 •每一高倍鏡視野下尿中紅血球數小於 50 •血漿中鈉的濃度小於 130 meq/l *主要條件必須全部符合,附加條件在診斷上不需要符合但可加強診 斷支持度. 43.
(44) 表 4. 四組接受不同治療之肝腎症候群患者的基本資料 項目 第一組 第二組 第三組 第四組 p值 (n=6) (n=6) (n=6) (n=6) 年齡 55.0 ± 12.4 50.7 ± 12.3 50.0 ± 8.4 51.7 ± 9.3 N.S. 性別(男/女) 5/1 6/0 5/1 5/1 肝硬化病因 B 型肝炎 C 型肝炎 酒精性肝病 住院時之肝功能 白蛋白 (g/dL) 膽紅素 (mg/dL) 凝血酵素原時間 (秒) ALT (U/L) AST (U/L) 住院時之腎功能. 3 2 1. 3 1 2. 3 1 2. 3 1 2. 2.4 ± 0.1 12.8 ± 3.1 20.5 ± 1.5 60.4 ± 18.4 57.2 ± 19.5. 2.4 ± 0.3 13.9 ± 6.0 21.2 ± 2.9 48.8 ± 17.0 75.5 ± 30.9. 2.3 ± 0.3 11.6 ± 3.8 18.4 ± 0.9 53.8 ± 17.9 61.3 ± 17.4. 2.3 ± 0.2 13.3 ± 3.4 18.7 ± 2.1 61.2 ± 18.7 57.8 ± 14.3. N.S. N.S. N.S. N.S. N.S.. 血尿素氮 (mg/dL) 49.2 ± 9.0 44.8 ± 12.5 40.3 ± 2.9 49.7 ± 5.7 N.S. 肌酸酐 (mg/dL) 3.0 ± 0.3 2.9 ± 0.2 3.1 ± 0.4 3.2 ± 0.3 N.S. N.S. = 未達具統計意義之差異;ALT = alanine aminotransferase;AST = aspartate aminotransferase。. 44.
(45) 表 5. 四組接受不同治療之肝腎症候群患者的腎功能變化和預後 項目 第一組 第二組 第三組 第四組 p值 (n=6) (n=6) (n=6) (n=6) 血尿素氮之變化 (mg/dL) -12.77 -14.00 12.67 a,b 11.83 a,b 0.009 c c,d c,d 肌酸酐之變化 (mg/dL) -0.88 -1.30 1.92 2.02 < 0.001 住院天數(日) 18.0 ± 2.4 24.3 ± 12.6 26.2 ± 16.6 20.7 ± 6.6 N.S. 預後(存/歿) 30 天 6/0 5/1 4/2 2/4 6 個月 3/3 3/3 1/5 0/6 a 與第一組血尿素氮之變化相較 p 值<0.05; b 與第二組血尿素氮之變化相較 p 值 <0.05; c 與第一組肌酸酐之變化相較 p 值<0.05; d 與第二組肌酸酐之變化相較 p 值 <0.05。. 45.
(46) 肝臟移植. 肝硬化. TIPS. 腸繫膜血. MARS. 門脈高壓. 腸繫膜血管擴張. 管收縮劑 有效血容積減少. 白蛋白及血 容積擴充. 刺激血管收縮系統 dopamine 前列腺素 misoprostol. 腎血管收縮. 代償機制正常. 代償機制失效. 腎臟機能正常. 肝腎症候群. 圖 1. 由周邊血管擴張理論所推演出的肝腎症候群病理機 轉和它的治療方式。 MARS=molecular absorbent recirculating system。. 46.
(47) 47.
(48) 48.
(49) 49.
(50) 50.
(51) 51.
(52) 52.
(53) 53.
(54) 54.
(55) 參考文獻 1. Helwing FC, Schutz CB. A liver— kidney syndrome. Surg Gynecol Obstet 1932;55:570-80. 2. Conn HO. A rational approach to the hepatorenal syndrome. Gastroenterology 1973;65:321-40. 3. Arroyo V, Guevara M, Ginès P. Hepatorenal syndrome in cirrhosis: pathogenesis and treatment. Gastroenterology 2002;122:1658-76. 4. Arroyo V, Ginès P, Gerbes A, Dudley FJ, Gentilini P, Laffi G, et al. Definition and diagnostic criteria of refractory ascites and hepatorenal syndrome in cirrhosis. Hepatology 1996;23:164-76. 5. Arroyo V, Batalleer R. Historical notes on ascites in cirrhosis. In: Arroyo V, Ginès P, Rodes J, Schrier RW, eds. Ascites and Renal Dysfunction in Liver Disease: Pathogenesis, Diagnosis, and Treatment. Malden, MA: Blackwell Science, 1999:3-13. 6. Hecker R, Sherlock S. Electrolyte and circulatory changes in terminal liver failure. Lancet 1956;2:1221-5. 7. Lancestremere RG, Davidson PL, Earley LE, O’Brien FJ, Papper S. Renal failure in Laennec’s cirrhosis. II. Sinmultaneous determination of cardiac output and renal hemodynamics. J Clin Invest 1962;41: 1922-7. 8. Baldus WP, Summerskill WHJ, Hunt JC. The kidney in cirrhosis. II. Disorders in renal function. Ann Intern Med 1964;60:366-77. 9. Baldus WP, Summerskill WHJ, Hunt JC, Maher FT. Renal circulation in cirrhosis: observations based on catheterization of renal vein. J Clin Invest 1964;43:1090-7. 10. Shear L, Hall WP, Gabuzda GJ. Renal failure in patients with cirrhosis of the liver. II. Factors influencing maximal urinary flow rate. Am J Med 1965;39:199-209. 11. Schroeder ER, Shear L, Sancetta SM, Gabuzda GJ. Renal failure in patients with cirrhosis of the liver. Evaluation of intrarenal blood flow by para-aminohippurate extraction and response to angiotensin. Am J Med 1967;43:887-96. 12. Epstein M, Berk DP, Hollenberg NK, Adams DF, Chalmers TC, Abrams HL, Merril JP. Renal failure in the patient with cirrhosis. The role of active vasoconstriction. Am J Med 1970;49:175-85. 13. Lieberman FL, Reynolds TB. Plasma volume in cirrhosis of the liver. 55.
(56) Its relation to portal hypertension, ascites and renal failure. J Clin Invest 1967;46:1293-308. 14. LeVeen HH, Christoudias G, Ip M, Luft R, Falk G, Gorsberg S. Peritoneo-venous shunting for ascites. Ann Surg 1974;180:580-90. 15. Schroeder ET, Eich RH, Smulyan H, Gould AB, Gabuzda GJ. Plasma renin levels in hepatic cirrhosis. Relationship to functional renal failure. Am J Med 1970;49:186-91. 16. Arroyo V, planas R, Gaya J, Deulofeu R, Rimola A, Pérez-Ayuso RM, et al. Sympathetic nervous activity, renin-angiotensin system and renal excretion of prostaglandin E2 in cirrhosis. Relationship to functional renal failure and sodium and water excretion. Eur J Clin Invest 1983;13:271-8. 17. Ring-Larsen H, Hesse B, Henriksen JH, Christensen NJ. Sympathetic nervous activity and renal and systemic hemodynamics in cirrhosis: plasma norepinephrine concentration, hepatic extraction, and renal release. Hepatology 1982;2:304-10. 18. Bichet DG, Van Putten VJ, Schrier RW. Potential role of increased sympathetic activity in impaired sodium and water excretion in cirrhosis. N Engl J Med 1982;307:1552-7. 19. Zipser RD, Hoefs JC, Speckart PF, Zia PK, Horton R. Prostaglandins: modulators of renal function and pressor resistance in chronic liver disease. J Clin Endocrinol Metab 1979;8:895-900. 20. Rimola A, Ginès P, Arroyo V, Camps J, Pérez-Ayuso RM, Quintero E, et al. Urinary excretion of 6-keto-prostaglandin F1-alpha, thromboxane B2 and prostaglandin E2 in cirrhosis with ascites. Relationship to functional renal failure (hepatorenal syndrome). J Hepatol 1986;3:111-7. 21. Pérez-Ayuso RM, Arroyo V, Camps J, Rimola A, Gaya J, Costa J, et al. Evidence that renal prostaglandins are involved in renal water metabolism in cirrhosis. Kidney Int 1984;26:72-80. 22. Arroyo V, Ginès P, Rimola A, Gaya J. Renal function abnormalities prostaglandins and effects of nonsteroidal anti-inflammatory drugs in cirrhosis with ascites. An overview with emphasis on pathogenesis. Am J Med 1986;81:104-22. 23. Pérez-Ayuso RM, Arroyo V, camps J, Rimola A, Costa J, Gaya J, et al. Renal kallikrein excretion in cirrhotics with ascites: relationship to renal hemodynamics. Hepatology 1984;4:247-52. 24. Jiménez W, Martinex A, Arroyo V, Bruix J, Rimola A, Gaya J, et al. 56.
(57) Temporal relationship between hyperaldosteronism, sodium retention and ascites formation in rats with experimental cirrhosis. Hepatology 1985;5:245-50. 25. Camps J, Sola J, Arroyo V, Pérez-Ayuso RM, Gaya J, Rivera F, Rodés J. Temporal relationship between the impairment of free water excretion and antidiuretic hormone hypersecretion in rats with experimental cirrhosis. Gastroenterology 1987;93:498-505. 26. López C, Jiménez W, Arroyo V, Clariá J, Lavilla G, Albert M, et al. Temporal relationship between the decrease in arterial pressure and sodium retention in hypertensive rats with carbon tetrachloride induced cirrhosis. Hepatology 1991;13:585-9. 27. Schrier RW, Arroyo V, bernardi M, Epstein M, Henriksen JH, Rodés J. Peripheral arterial vasodilation hypothesis: a proposal for the initiation of renal sodium and water retention in cirrhosis. Hepatology 1988;8:1151-7. 28. Martin PY, Ginés P, Schrier RW. Role of nitric oxide as mediator of hemodynamic abnormalities and sodium and water retention in cirrhosis. N Engl J Med 1998;339:533-41. 29. Wiest R, Groszmann RJ. Nitric oxide and portal hypertension: its role in the regulation of intrahepatic and splanchnic vascular resistance. Semin Liver Dis 1999;19:411-26. 30. Lenz K, Druml W, Kleinberger G, Hortnagl H, Laggner A, Schneeweiss B, Deutsch E. Enhancement of renal function with ornipression in a patient with decompensated cirrhosis. Gut 1985;26:1385-6. 31. Lenz K, Hortnagl H, Druml W, Grimm G, Laggner A, Schneeweiss B, Kleinberger G. Beneficial effect of 8-ornithine vasopressin on renal dysfunction in decompensated cirrhosis. Gut 1989;30:90-6. 32. Lenz K, Hortnagl H, Druml W, Reither H, Schmid R, Schneeweiss B, et al. Ornipressin in the treatment of functional renal failure in decompensated liver cirrhosis. Gastroenterology 1991;101:1060-7. 33. Chen DS, Sung JL. Hepatitis B virus infection on Taiwan. N Engl J Med 1997;297:668-9. 34. Chen DS, Sung JL. Hepatitis B virus infection and its sequelae in Taiwan. Gastroenterol Jpn 1984;19:363-6. 35. Lee SD, Chan CY, Wang YJ, Wu JC, Lai KH, Tsai YT, Lo KJ. Seroepidemiology of hepatitis C virus in infection in Taiwan. Hepatology 1991;13:830-3. 57.
(58) 36. Chen DS, Wang JT, Chen PJ, Wang TH, Sung JL. Hepatitis C virus infection in Taiwan. Gastroenterol Jpn 1991;26(suppl 3):164-6. 37. Chang SJ, Chen HC, Ying J, Lu CF, Ko YC. Risk factors of hepatitis C virus infection in a Taiwanese aboriginal community. Kaohsiung J Med Sci 1996;12:241-7. 38. Lu SN, Chue PY, Chen IL, Wang JH, Huang JF, Peng CF, et al. Incidence of hepatitis C infection in a hepatitis C endemic township in southern Taiwan. Kaohsiung J Med Sci 1997;13:605-8. 39. Lee SD, Lo KJ. Control of hepatitis b virus infection by vaccination : the Taiwan experience. Zhonghua Yi Xue Za Zhi (Taipei) 1998;61:501-6. 40. Ginés A, Escorsell A, Ginés P, Salo J, Jimenez W, Inglada L, et al. Incidence, predictive factors, and prognosis of hepatorenal syndrome in cirrhosis. Gastroenterology 1993;105:229-36. 41. Bernardi M, Fornale L, Di Marco C, Trevisani F, Baraldin M, Gasberrini A, De Collibus C. Hyperdynamic circulation of advanced cirrhosis: a re-appraisal based on posture-induced changes in hemodynamic. J Hepatol 1995;22:309-18. 42. Groszmann RJ. Hyperdynamic circulation of liver disease 40 years later: pathophysiology and clinical consequences. Hepatology 1994;20:1359-63. 43. Albillos A, Colombato LA, Groszmann RJ. Vasodilation and sodium retention in prehepatic portal hypertension. Gastroenterology 1992;102:931-5. 44. Maroto A, Ginès P, Arroyo V, Ginès A, Salo J, Claria J, Jimènez W, et al. Brachial and femoral artery blood flow in cirrhosis: relationship to kidney dysfunction. Hepatology 1993: 17;788-793. 45. Guevara M, Bru C, Ginès P, Fermandez-Esparrach G, Sort P, Bataller R, Jimenez W. Increased cerebrovascular resistance in cirrhotic patients with ascites. Hepatology 1998:28;39-44. 46. Goldstein H, Boyle JD. Spontaneously recovery from the hepatorenal syndrome. Repost of four cases. N Engl J Med 1965; 272:895. 47. Koppel MH, Coburn JN, Mims MM, Goldtein H, Boyle H, Rubini ME. Transplantation of cadaveric kidneys from patients with hepatorenal syndrome. Evidence for the functional nature of renal failure in advanced liver disease. N Engl J Med 1969;280:1367-71. 48. Iwatsuki S, Popovtzer MM, Corman JL, Ishikawa M, Putnam CW, Katz FH, Starzl TE. Recovery from hepatorenal syndrome after orthotopic liver transplantation. N Engl J Med 1973;289:1155-9. 58.
(59) 49. Bosch J, Arroyo V, Betriu A, Mas A Carrilho F, Rivera F, et al. Hepatic hemodynamics and the renin-angiotensin aldosterone system in cirrhosis. Gastroenterology 1992;102:2114-9. 50. Arroyo V, Bosch J, Mauri M, Viver J, Mas A, Rivera F, Rodès J. Renin, aldosterone and renal hemodynamics in cirrhosis with ascites. Eur J Clin Invest 1979;9:69-73. 51. Solis-Herruzo JA, Duran A, Favela G, Castellano G, Madrid JL, Munoz-Yague MT, et al. Effects of lumbar sympathetic block on kidney function in cirrhotic patients with hepatorenal syndrome. J Hepatol 1987;5:167-73. 52. Laffi G, La Villa G, Pinzani M, Ciabattoni G, Patrignani P, Mannelli M, et al. Altered renal and platelet arachidonic acid metabolism in cirrhosis. Gastroenterology 1986;90:274-82. 53. Moore K, Ward PS, Taylor GW, Williams R. Systemic and renal production of thromboxane A2 and prostacyclin in decompensated liver disease and hepatorenal syndrome. Gastroenterology 1991; 100:1069-77. 54. Govindarajan S, Nast CC, Smith WL, Koyle MA, Daskalopoulos G, Zipser RD. Immunohistochemical distribution of renal prostaglandin endoperoxidase synthase and prostacyclin synthase: diminished endoperoxidase synthase in the hepatorenal syndrome. Hepatology 1987;7:654-9. 55. Boyer T, Zia P, Reynolds TB. Effect of indomethacin and prostaglandin A1 on renal function and plasma rennin activity in alcoholic liver disease. Gastroenterology 1979;77:215-22. 56. Bomzon A, Blendis LM. The nitric oxide hypothesis and the hyperdynamic circulation in cirrhosis. Hepatology 1994;20:1343-50. 57. Vorobioff J, Bredfeldt JE, Groszmann RJ. Increased blood flow through the portal system in cirrhotic rats. Gastroenterology 1984;87:1120-6. 58. Kotelanski B, Groszmann RJ, Cohn JN. Cirrculation times in the splanchnic and hepatic beds in alcoholic liver disease. Gastroenterology 1972;63:102-11. 59. Fernández-Seara J, Prieto J, Quiroga J, Zozaya JM, Cobos MA, Rodriguez-Eire JL, et al. Systemic and regional hemodynamics in patients with liver cirrhosis and ascites with and without functional renal failure. Gastroenterology 1989;97:1304-12. 60. Guarner C, Soriano G, Tomas A, Bulbena O, Novella MT, Balanzo J, et al. Increased serum nitrite and nitrate levels in patients with cirrhosis: relationship to endotoxemia. Hepatology 1993;18:1139-43. 61. Raij L, Baylis C. Glomerular actions of nitric oxide. Kidney Int 59.
(60) 1995;48:20-32. 62. Bech JN, Nielsen CB, Pedersen EB. Effects of systemic nitric oxide synthesis inhibition on renal plasma flow, glomerular filtration rate, urinary sodium excretion, and vasoactive hormones in healthy humans. Am J Physiol 1996;270:F845-51. 63. Ros J, Claria J, Jimenez W, Bosch-Marce M, Angeli P, Arroyo V, et al. Role of nitric oxide and prostacyclin in the control of renal perfusion in experimental cirrhosis. Hepatology 1995;22:915- 20. 64. Atucha NM, Garcia-Estan J, Ramirez MC, Perez MC, Quesada T, Romero JC. Renal effects of nitric oxide synthesis inhibition in cirrhotic rats. Am J Physiol 1994;267:R1454-60. 65. Criado M, Flores O, Ortiz MC, Hidalgo F, Rodriguez-Lopez AM, Eleno N, et al. Elevated glomerular and blood mononuclear lymphocyte nitric oxide production in rats with chronic bile duct ligation: role of inducible nitric oxide synthase activation. Hepatology 1997;26:268-76. 66. Campillo B, Bories PN, Benvenuti C, Dupeyon C. Serum and urinary nitrate levels in liver cirrhosis: endotoxemia, renal function and hyperdynamic circulation. J Hepatol 1996;24:707-14. 67. Tajiri K, Miyakawa H, Izumi N, Marumo F, Sato C. Systemic hyoptensoin and diuresis by L-arginine in cirrhotic patients with ascites: role of nitric oxide. Hepatology 1995;22:1430-5. 68. Gülberg V, Moller S, Henriksen JH, Gerbes AL. Increased renal production of C-type natriuretic peptide (CNP) in patients with cirrhosis and functional renal failure. Gut 2000;47:852-7. 69. Angeli P, Jimenez W, Arroyo V, Mackenzie HS, Zhang PL, Claria J, et al. Renal effects of natriuretic peptide receptor blockade in cirrhotic rats with ascites. Hepatology 1994;20:948-51 70. Holt S, Goodier D, Marley R, Patch D, Burroughs A, Fernando B, Harry D, Moore K. Improvement in renal funcition in hepatorenal syndrome with N-acetylcysteine. Lancet 1999;353:294-5. 71. Uchihara M, Izumi N, Sato C, Marumo F. Clinical significance of elevated plasma endothelin concentration in patients with cirrhosis. Hepatology 1992;16:75-99. 72. Moore K, Wendon J, Frazer M, Karani J, Williams R, Badr K. Plasma endothelin immunoreactivity in liver disease and the hepatorenal syndrome. N Engl J Med 1992; 327:1774-8. 73. Salo J, Fernandez-Esparrach G, Ginés P, Ginés A, Guevara M, Sort P et al. Urinary endothelin like immunoreactivity in patients with cirrhosis. J Hepatol 1997; 27: 810-6. 74. Guevara M, Ginés P. Bandi JC, Gilabert R, Sort P, Jinénez W, et al. 60.
(61) Tramsjagular intrahepatic postosystemic shunt in hepatorcnal syndrome: effect on renal function and vasoactive systems. Hepatology 1998; 28: 416-422. 75. Gülberg V, Bilzer M, Gerbes AL. Long-term therapy and retreatment of hepatorenal syndrome type 1 with ornipressin and dopamine. Hepatology 1999;30:870-5. 76. Zusman RM, Axelrod L, Tolkoff-Rubin N. The treatment of hepatorenal syndrome with intra-renal administration of prostaglandin E1. Prostaglandins 1977;13:819-30. 77. Ginès A, Salmeron JM, Ginès P, Arroyo V, Jimènez W, Rivera F, Rodés J. Oral misoprostol or intravenous prostaglandin E2 do not improve renal function in patients with cirrhosis and ascites with hyponatremia or renal failure. J Hepatol 1993;17:220-6. 78. Badalamenti S, Borroni G, Lorenzano E, Incerti P, Salerno F. Renal effects in cirrhotic patients with avid sodium retention of atrial natriuretic factor injection during norepinephrine infusion. Hepatology 1992;15:824-9. 79. Lancestremere RG, Klinger EL, Jr, Frisch E, Papper S. Simultaneous determinations of cardiac output and renal function in patients with Laennec’s cirrhosis during the administration of the pressor amine, metaraminol. J Lab Clin Med 1963;61:820-5. 80. Arroyo V. Treatment of hepatorenal syndrome in cirrhosis. In: Arroyo V, ed. Ascites and Renal Dysfunction in Liver Disease. Malden, MA: Blackwell Science, 1999;492-510. 81. Gonwa TA, Morris CA, Goldstein RM, Husberg BS, Klintmalm GB. Long-term survival and renal function following liver transplantation in patients with and without hepatorenal syndrome: experience in 300 Patients. Transplantation 1991;51:428-30. 82. Brown RS Jr, Lombardero M, Lake JR. Outcome of patients with renal insufficiency undergoing liver or liver-Kidney transplantation. Transplantation 1996;62:1788-93. 83. Jeyarajah DR, Gonwa TA, McBride M, Testa G, Abbasoglu O, Husberg BS, et al. Hepatorenal syndrome: combined liver kidney tramsplants versus isolated liver transplant. Transplantation 1997;64:1760-5. 84. Guevara M, Ginés P, Fernandez-Esparrach G, Sort P, Salmeron JM, Jimenez W, et al. Reversibility of hepatorenal syndrome by prolonged administration of ornipressin and plasma volume expansion. Hepatology 1998;27:35-41. 85. Hadengue A, Gadano A, Moreau R, Giostra E, Durand F, Valla D, et al. Beneficial effects of the 2-day administration of terlipressin in patients 61.
(62) with cirrhosis and hepatorenal syndrome. J Hepatol 1998;29:565-70. 86. Uriz J, Ginés P, Cárdenas A, Sort P, Jiménez W, Salmerón JM, Bataller R, et al. Terlipressin plus albumin infusion: an effective and safe therapy of hepatorenal syndrome. J Hepatol 2000;33:43-48. 87. Mulkay JP, Louis H, Donckter V, Bourgeois N, Adler M, Deviere J, Le Moine O. Long-term terlipressin administration improves renal function in cirrhotic patients with type 1 hepatorenal syndrome: a pilot study. Acta Gastroenterol Belg 2001;64:15-9. 88. Ginés P, Ortega R, Uriz J, Calahorra B, Cárdenas A, De Las Heras D, et al. Effect of terlipressin administration with and without albumin in hepatorenal syndrome. A phase-II study. Hepatology 2001;34:186(A). 89. Freeman JG, Cobden I, Lishman AH, Record CO. Controlled trial of terlipressin ('Glypressin') versus vasopressin in the early treatment of oesophageal varices. Lancet 1982;2:66-8. 90. D'Amico G, Traina M, Vizzini G, Tine F, Politi F, Montalbano L, et al. Terlipressin or vasopressin plus transdermal nitroglycerin in a treatment strategy for digestive bleeding in cirrhosis. A randomized clinical trial. Liver Study Group of V. Cervello Hospital. J Hepatol 1994;20:206-12. 91. Chiu KW, Sheen IS, Liaw YF. A controlled study of glypressin versus vasopressin in the control of bleeding from oesophageal varices. J Gastroenterol Hepatol 1990;5:549-53. 92. Eisenman A, Armali Z, Enat R, Bankir L, Baruch Y. Low-dose vasopressin restores diuresis both in patients with hepatorenal syndrome and in anuric patients with end-stage heart failure. J Int Med 1999;246:183-190. 93. Lamberts SW, van der Lely AJ, de Herder WW, Hofland LJ. Octreotide. N Engl J Med 1996;334:246-54. 94. Chatila R, Ferayorni L, Gupta T, Groszmann RJ. Local arterial vasoconstriction induced by octreotide in patients with cirrhosis. Hepatology 2000;31:572-6. 95. Kaffy F, Borderie C, Chagneau C, Ripault MP, Larzilliere I, Silvain C, Beauchant M. Octreotide in the treatment of the hepatorenal syndrome in cirrhotic patients. J Hepatol 1999;30:174. 96. Angeli P, Volpin R, Gerunda G, Craighero R, Romero P, Merenda R, et al. Reversal of type 1 hepatorenal syndrome with the administration of midodrine and octreotide. Hepatology 1999;29:1690-7. 97. Schroeder ET, Numann PJ, Chamberlain BE. Functional renal failure in cirrhosis. Recovery after portacaval shunt. Ann Intern Med 1970;72:293-8. 98. Ariyan S, Sweeney T, Kerstein MD. The hepatorenal syndrome: 62.
(63) recovery after portacaval shunt. Ann Surg 1975;181:847-9. 99. Brensing KA, Textor J, Perz J, Schiedermaier P, Raab P, Strunk H, et al. Long term outcome after transjugular intrahepatic postosystemic stent shunt in non-transplant cirrhotics with hepatorenal syndrome: a phase II study. Gut 2000;47:288-95. 100. Brensing KA, Textor J, Strunk H, Klehr HU, Schild H, Sauerbruch T. Transjugular intrahepatic portosystemic stent-shunt for hepatorenal syndrome. Lancet 1997;349:697-8. 101. Spahr L, Fenyves D, N’Guyen VV, Roy L, Legault L, Dufresne MP, Pomier-Layrargues G. Improvement of hepatorenal syndrome by transjugular intrahepatic portosystemic shunt. Am J Gastroenterol 1995;90:1169-71. 102. Alam I, Bass NM, LaBerge JM, Ring E, Somberg KA. Treatment of hepatorenal syndrome with the transjugular intrahepatic shunt (TIPS). Gastroenterology 1995;108:A1024. 103. Ochs A, Rössle M, Haag K, Gerbes A, Morgenroth A, Deibert P, et al. TIPS for hepatorenal syndrome. Hepatology 1994;20:114A. 104. Awad SS, Sawada S, Soldes OS, Ricj PB, Klein R, Alarcon WH, Bartlett RH. Can the clearance of tumor necrosis factor and interleukin 6 be enhanced using an albumin dialysate hemodiafiltration system ASAIO J 1999;45:47-9. 105. Rahman TM, Hodgson HJF. Liver support systems in acute hepatic failure. Aliment Pharmacol Ther 1999;13:1255-72. 106. Mitzner SR, Stange J, Klammt S, Risler T, Erley CM, Bader BD, et al. Improvement of hepatorenal syndrome with extracorporeal albumin dialysis MARS: results of a prospective randomized, controlled clinical trial. Liver Transpl 2000;6:277-86. 107. Lerut J, Goffette P, Laterre PF, Donataccio M, Reynaert MS, Otte JB. Sequential treatment of hepatorenal syndrome and posthepatic cirrhosis by intrahepatic portosystemic shunt (TIPS) and liver transplantation. Hepatogastroenterology 1995;42:985-7. 108. Gonwa TA, Klintmalm GB, Jennings LS, Goldstein RM, Husberg B. Impact of pretransplant renal function on survival after liver transplantation. Transplantation 1995;59:361-5. 109. Seu P, Wilkinson AH, Shaked A, Busuttil BW. The hepatorenal syndrome in liver transplant recipients. Am Surg 1991;57:806-9. 110. Rimola A, Gavaler JS, Schade RR, el-Lankany S, Starzl TE, van Thiel DH. Effects of renal impairment on liver transplantation. Gastroenterology 1987;93:148-5. 111. Pedretti G, Elia G, Calzetti C, Magnani G, Fiaccadori F. Octreotide versus terlipression in acute variceal hemorrhage in liver 63.
(64) cirrhosis. Emergency control and prevention of early rebleeding. Clin Investig 1994;72:653-9. 112. Silvain C, Carpentier S, Sautereau D, Czernichow B, Metreau JM, Fort E, et al. Terlipressin plus transdermal nitroglycerin vs. octreotide in the control of acute bleeding from esophageal varices: a multicenter randomized trial. Hepatology1993;18:61-5. 113. Lin SM, Lee CS, Kao PF. Low-dose dopamine infusion in cirrhosis with refractory ascites. Int J Clin Pract 1998; 52:533-6. 114. Bennett WM, Keeffe E, Melnyk C, Mahler D, Rosch J, Porter GA. Response to dopamine hydrochloride in the hepatorenal syndrome Arch Intern Med 1975;135:964-71. 115. Barnardo DE, Baldus WP, Maher FT. Effects of dopamine on renal function in patients with cirrhosis. Gastroenterology 1970;58:524-31.. 64.
數據


相關文件
28 Specifically, in this study we determined that (1) individuals having comorbid OSA and MetS, that is SZ, have a greater prevalence of calcified carotid artery atherosclerotic
Wheeled in a pram by her mother, she attended the Pediatric Dentistry Clinic, Faculty of Dentistry, Khon Kaen University, because of dental caries and poor oral hygiene..
This retrospective magnetic resonance imaging study of patients under 21 years of age found that these young patients are susceptible to all stages of disk displacement and that
6 M 30 Palmar and/or plantar pits, skin cysts, one basal cell carcinoma, milia, neurofibroma, jaw cysts, calcification of the falx cerebri, scoliosis, missing/malformed
pylori in pathogenesis of oral mucosal lesions or ulcerations is still unclear, it seems that patients with oral lesions as leukoplakia and oral lichen planus, and concurrent
Introduction Casereport Abstract Thetreatmentofdiffusesclerosingosteomyelitiswithoralbisphosphonates
A case of SAPHO syndrome with dif- fuse sclerosing osteomyelitis of the mandible treated successfully with prednisolone
Radiomorphometric indices can be used to deter- mine the existence of a porous structure in the man- dible on panoramic images of patients who have scleroderma and may have a high
Objectives This study investigated the clinical effectiveness of intervention with an open-mouth exercise device designed to facilitate maximal interincisal opening (MIO) and
