M
ammography usage with relevant factors among women with mental disabilities in Taiwan : a nationwide population-based study
Suh-May Yena, b,c, #Pei-Tseng Kungd, #Wen-Chen Tsaib,*
a. Department of Public Health, China Medical University, Taichung, Taiwan, R.O.C. b. Department of Health Services Administration, China Medical University,
Taichung, Taiwan, R.O.C.
c. Department of Chinese Medicine, Nantou Hospital, Nantou, Taiwan, R.O.C. d. Department of Healthcare Administration, Asia University, Taichung, Taiwan,
R.O.C.
Suh-May Yen:[email protected] Pei-Tseng Kung: [email protected] Wen-Chen Tsai: [email protected]
# Authors equally contributed to this work.
*Correspondence author:Professor Wen-Chen Tsai, Dr.PH
Address:No. 91 Hsueh-Shih Road, Taichung, Taiwan 40402, R.O.C Tel:886-4-22073070
Fax:886-4-22028895
E-mail: [email protected]
Abstract
cancer and are thus in urgent need of breast cancer preventive care. This study examined the use of screening mammography by Taiwanese women with mental disabilities and analyzed factors affecting this use.17,243 Taiwanese women with mental disabilities aged 50–69 years were retrospectively included as study subjects. Linked patient data were obtained from three national databases in Taiwan (the 2008 database of physically and mentally disabled persons, the Health Promotion
Administration’s 2007–2008 mammography screening data, and claims data from the National Health Insurance Research Database). Besides descriptive statistics and bivariate analysis, logistic regression analysis was also performed to examine factors affecting screening mammography use. The 2007–2008 mammography screening rate for Taiwanese women with mental disabilities was8.79% (n=1,515). Variables that significantly influenced screening use were income, education, presence of
catastrophic illness/injury, severity of mental disability, and usage of other preventive care services. Screening was positively correlated with income and education. Those with catastrophic illness/injury were more likely to be screened (odds ratio [OR],1.40; 95% CI=1.15–1.72). Severity of disability was negatively correlated with screening, with very severe, severe, and moderate disability being associated with 0.34–0.69 times the odds of screening as mild disability. In Taiwan, women with mental disabilities receive far less mammography screening than women in general.
Key Words: mental disability; mammography screening; access andutilization; preventive care
M
ammography usage with relevant factors among women with mental disabilities in Taiwan : a nationwide population-based study
1. Introduction
The incidence of breast cancer varies widely across regions of the world, with the age-standardized incidence in 2008 being highest in Western Europe at 89.7 per 100,000 and lowest in Eastern Africa at 19.3 per 100,000(International Agency for
Research on Cancer, 2010). Breast cancer is the leading cause of cancer death in women worldwide (Organization, 2008). In Taiwan, breast cancer is the fourth leading cause of cancer death in women, with the mortality rate from breast cancer nearly doubled over the past 30 years, from 6.0 per 100,000 in 1981 to 11.6 per 100,000 in 2012(Ministry of Health and Welfare, 2013).
Mammography is an important method for the early diagnosis of breast cancer, and regular mammography screening has been shown by many researchers to reduce breast cancer mortality(Hanson, Montgomery, Bakker, & Conlon, 2009; Humphrey, Helfand, Chan, & Woolf, 2002; Kalager, Zelen, Langmark, & Adami, 2010).
Humphrey et al. (2002) found that screening mammography reduced breast cancer mortality by 15%–20% in women aged 40 to 49 years and by 16%–35% in women aged 50 to 59 years(Humphrey, et al., 2002).In Taiwan, women 50 to 69 years of age are eligible to receive free mammography screening once every two years beginning in 2004(K. J. Chang, Kuo, & Wang, 2008). Even with this national screening
program, the breast cancer mortality rate has continued to rise, and improving the early detection of breast cancer has become a top public health issue in Taiwan. A previous study showed that the use of mammographic breast cancer screening by women with disabilities was affected by factors including age, income, health status, and area of residence, marital status, education level, and severity of disability (Kung,
Tsai, & Chiou, 2012). Among all women in the recommended age range for screening in Taiwan, the proportion that had received mammography screening within the past two years increased from 12% in 2008 to 29.3% in 2011(Health Promotion
Administration, 2009, 2012).
Compared with those without mental illness, individuals with mental illness were found to have more medical comorbidities(Cole, 2007; Daumit, Pratt, Crum, Powe, & Ford, 2002), incur greater health care burden,(Caroline P Carney & Laura E Jones, 2006; Insel, 2008) and have 30% higher cancer-related mortality (C. K. Chang, et al., 2010; Kisely, Crowe, & Lawrence, 2013b); they were also less likely to
undergo mammography screening(Pirraglia, Sanyal, Singer, & Ferris, 2004; Steiner, et al., 1998; Vigod, Kurdyak, Stewart, Gnam, & Goering, 2011; Werneke, et al., 2006; Yee, et al., 2011). Masterson et al. (2010) showed a possible correlation
between poor mental health status, such as having feelings of depression and anxiety, and decreased use of regular mammography screening (Masterson, Hopenhayn, & Christian, 2010). Results from past studies have not been entirely consistent with respect to the use of screening mammography among individuals with mental illness. Research conducted by Koroukian et al. (2012) in Ohio State, United States, showed a higher rate of mammographic breast cancer screening for women with than without mental illness (38.1% vs. 31.7%)(Koroukian, Bakaki, Golchin, Tyler, & Loue, 2012). Another study in New Mexico State by Yee et al. (2011) found that women with mental illness were less likely than those without such illness (odds ratio [OR], 0.79) to undergo breast cancer screening(Yee, et al., 2011). Alarmingly, psychiatric patients were shown to have not only a 9.5-fold higher incidence of breast cancer (Halbreich, Shen, & Panaro, 1996) but also a higher risk of breast cancer mortality (rate ratio,
1.27) (Kisely, Crowe, & Lawrence, 2013a) than the general population. Thus, individuals with mental illness as a group are in urgent need of more breast cancer preventive care services.
Little research has focused on screening mammography use by Asian women with mental illness. In Taiwan, 0.51% of the populations (totaling 119,514) were living with mental disabilities in 2012. The aim of this study was to examine the use of mammography screening by Taiwanese women with mental disabilities and analyze factors that affected this use.
2. Materials and methods
2.1 Data source and participants
The study subjects were 17,243 Taiwanese women with mental disabilities aged 50–69 years. Mental disabilities included delusional disorders, affective disorders, schizophrenia, childhood-onset mental disorders, senile and presenile mental disorders, other organic mental disorders, and other nonorganic mental disorders.
A retrospective cohort analysis was conducted using the latest data from the following combination of national databases in Taiwan: the Ministry of the Interior’s 2008 database of physically and mentally disabled persons, the Health Promotion Administration’s 2007–2008 mammography screening data, and claims data from the National Health Insurance Research Database. At the Statistics Center of the Taiwan Ministry of Health and Welfare, patient data from the three databases were linked through patients’ national identification card numbers and then stripped of unique personal identifiers and encrypted in order to protect patient privacy. This study was approved by the institutional review board ofChina Medical University and Hospital (IRB No. CMU-REC-101-012).
2.2 Definition and description of variables
The independent variables analyzed included the following: (i) basic characteristics: age, marital status, and education level; (ii) economic status: premium-based monthly salary, which was categorized into five levels plus the dependent population category; (iii) health status: presence or absence of catastrophic illness/injury, cancer, or diabetes; (iv) neighborhood environment: urbanization level of area of residence, ranging from the most urbanized, or level 1, to the least, or level 8; (v) level of mental disability: classified as very severe, severe, moderate, or mild; and (vi) past usage of other preventive care services: use of the Pap smear test and of adult preventive health care. The dependent variable studied was use of screening mammography during 2007–2008.
The severity of mental disability was categorized as very severe (completely dependent on caretakers or requiring close supervision), severe (requiring
supervision), moderate (capable of self-care and other activities of daily living with partial supervision), and mild (capable of self-care and other activities of daily living without need for supervision), as assessed by nationally recognized psychiatrists. As for economic status, the health insurance premiums under Taiwan’s National Health Insurance system are determined by individuals’ monthly salaries, with non-employed spouses and minor children being considered dependents. Therefore, the insurance premium can be used to represent an individual’s economic status.
2.3 Statistical analysis
Data analysis was performed with the SAS statistical software package, version 9.2. First, descriptive statistics were expressed as percentages of screening
mammography use for the categories of each variable. Next, associations between screening mammography use and other variables were analyzed with the χ2 test.
Finally, logistic regression analysis was performed to determine which of the factors affected screening mammography use. P-values less than 0.05 were regarded as statistically significant.
3. Results
3.1 Use of screening mammography by Taiwanese women with mental disabilities
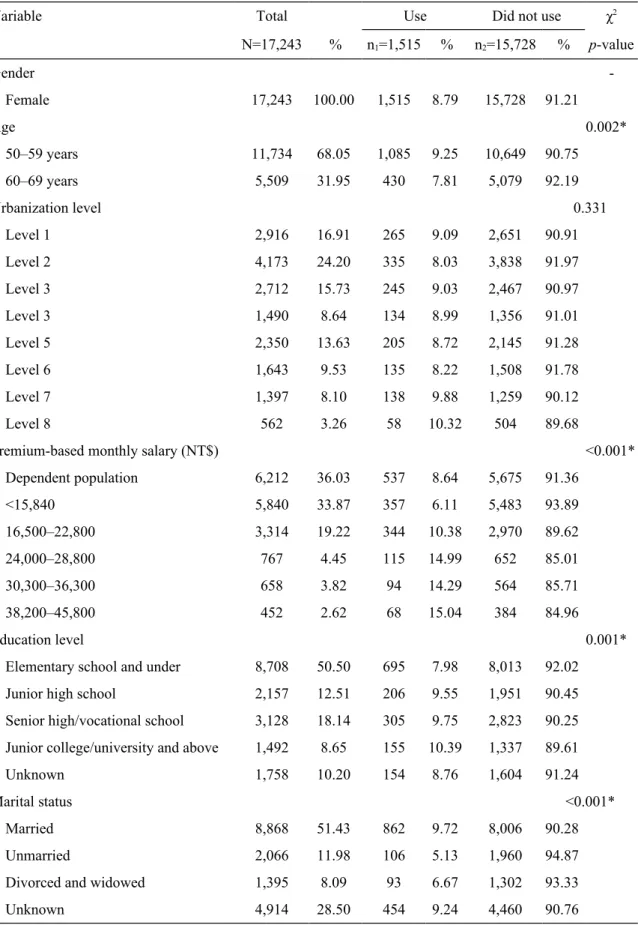
The characteristics of the study subjects, a total of 17,243 women with mental disabilities, are summarized in Table 1. About two-thirds of the women (68.05%) were 50–59 years of age, over half (56.84%) resided in areas within the three highest urbanization levels (levels 1 through 3), nearly nine-tenths (89.12%) had a premium-based monthly salary of NT$16,500–22,800 or less, about half (50.50%) had an education of elementary school or less, and about half (51.43%) were married. With respect to the severity of mental disability, over half of the women (53.02%) had moderate disability, and nearly one-quarter (24.09%) had mild disability. Of all participants, 1,515 (8.79%) used screening mammography during 2007–2008, while the remaining 15,728 (91.21%) did not, indicating that the vast majority of 50–69-year-old Taiwanese women with mental disabilities did not undergo mammography screening for breast cancer during this time period.
The rate of mammography screening among the study participants (1,515 totals screened) varied across different demographic and health-related categories (Table 1). The 50–59-year age group had a somewhat higher screening rate (9.25%) than the 60– 69-year group (7.81%). Among the economic status categories, the highest range of premium-based monthly salary, NT$38,200–45,800, corresponded to the highest screening rate (15.04%). The screening rate increased with increasing education level, with greater participation in mammography screening being observed among those with junior college/university or above education (10.39%) and those with senior
high/vocational school education (9.75%). Married women underwent screening at a higher rate (9.72%) than women in any other marital status category. With respect to the severity of mental disability, the less severe categories, mild disability (14.25%) and moderate disability (8.35%), corresponded to higher screening rates.
3.2 Factors affecting screening mammography use by Taiwanese women with mental disabilities
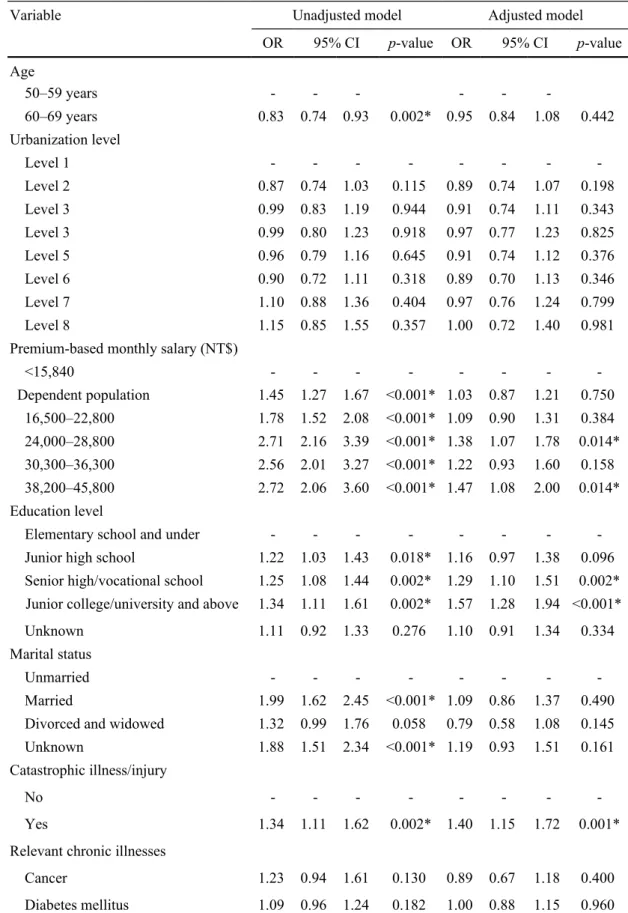
Logistic regression analysis was performed to identify factors that influenced the use of screening mammography among women with mental disabilities. As shown in Table 2, screening mammography use was significantly affected by premium-based monthly salary, education level, presence or absence of catastrophic illness/injury, severity of mental disability, past use of the Pap smear test, and past use of adult preventive health care. With respect to economic status, mammography screening increased with increasing premium-based monthly salary, with the highest odds of screening being observed for the NT$38,200–45,800 category, corresponding to 1.47 times the odds (95% confidence interval [CI], 1.08–2.00) for the reference category, <NT$15,840. Mammography screening also increased with increasing education level, with senior high/vocational school education and junior college/university or more education being associated with 1.29 times (95% CI, 1.10–1.51) and 1.57 times (95% CI, 1.28–1.94) the odds of screening, respectively, relative to elementary school or less education.
As for health-related factors (Table 2), greater use of screening mammography was observed among those with catastrophic illness or injury (OR, 1.40; 95% CI, 1.15–1.72) than among those without it. The severity of disability was negatively correlated with screening use, with the likelihood of screening decreasing from mild disability to very severe disability (OR, 0.34). Having used other preventive health
care services in the past was associated with greater odds of mammography screening. Specifically, those who had received Pap smear tests were 6.42 times as likely (95% CI, 5.55–7.44), and those who had used adult preventive care were 2.20 times as likely (95% CI, 1.96–2.46), to undergo mammography screening as those who had not used the respective service.
4. Discussion
We investigated screening mammography use by Taiwanese women with mental disabilities and found the screening rate in this group to be 8.79%, which is much lower than the 12% screening rate for women in general in Taiwan (Health Promotion Administration, 2009). This result is in agreement with the findings of Carney et al. (2006) and Yee et al. (2011) that women with mental illness were less likely to receive mammography screening(Caroline P. Carney & Laura E. Jones, 2006; Yee, et al., 2011).
Amaddeo & Jones(2007) and Shidhaye & Patel (2010) reported a higher prevalence of mental illness among individuals with lower socioeconomic status (Amaddeo & Jones, 2007; Shidhaye & Patel, 2010). Consistent with this observation, we found that among our study participants with mental disabilities, nearly nine out of ten (89.12%) had a premium-based monthly salary level ≤NT$16,500–22,800 (30 New Taiwan dollars = 1 U.S. dollar), and approximately half (50.5%) had elementary school or less education; we further showed that belonging to these low socioeconomic categories was associated with lower rates of mammography
screening (Table 1). With respect to marital status, we showed that married study participants had the highest rate of mammography screening (Table 1), in agreement with the findings in the past. (Lai, Lai, Chen, & Koo, 2012)
As revealed by our logistic regression modeling (Table 2), the odds of
mammography screening in Taiwanese women with mental disabilities increased with increasing premium-based monthly salary and education level and were higher for those who had used other preventive health care services in the past. These results are similar to those of Kung et al. (2012) for women with disabilities(Kung, et al., 2012). Our results also corroborate the findings of Lai et al. (2012) that low education, low average monthly income, and nonreceipt of complete physical examination were significant independent factors associated with non-utilization of screening mammography(Lai, et al., 2012). Schueler et al. (2008) showed that women who lacked knowledge about breast cancer screening were less likely to undergo
mammography screening (OR, 0.46–0.76), (Schueler, Chu, & Smith-Bindman, 2008) suggesting the importance of improving patients’ health literacy with respect to breast cancer and relevant screening methods.
Our study found that individuals with lower income had a lower likelihood of using mammography screening. However, cancer screening services are available at nearly no cost to patients under Taiwan’s universal health insurance system and
should not pose a financial barrier, indicating that other reasons may exist for lower-income individuals’ receiving less cancer screening in Taiwan. A similar phenomenon was observed in a Swiss study by Cullati et al. (2009). As breast cancer screening is covered under the health insurance system in Switzerland, the authors interpreted the lower likelihood of screening among lower-income individuals as being largely mediated by a link between income and attitudes toward cancer screening (Cullati, Charvet-Bérard, & Perneger, 2009).
Previous studies identified several factors that were significantly associated with lower screening mammography use by individuals with mental illness. These factors include poor integration of psychiatric and other medical services(Druss &
Rosenheck, 1997); stigmatization and negative perceptions toward persons with mental illness, which influence the care provided by medical personnel(Penn & Martin, 1998) inability of patients with severe psychiatric conditions to adequately communicate with their physicians(Bunce, Jones, Badger, & Jones, 1982); fear or anxiety toward breast cancer screening results(Kash & Dabney, 2001); and embarrassment or fear of adverse mammography experience(Owen, Jessie, & De Vries Robbe, 2002).Research by Friedman et al. (2005) (Friedman, Puryear, Moore, & Green, 2005) and Schueler et al. (2008)(Schueler, et al., 2008) showed that recommendation by physicians or other medical personnel can increase patients’ use of screening mammography. Because women with psychiatric disorders tend to have greater trust in psychiatrists whom they see on a regular basis, psychiatrists are in a unique position to encourage their patients to undergo cancer screening. According to Friedman et al.’s study in the United States, about one-quarter of patients with
psychiatric disorders cited psychiatrists, rather than other physicians, as their primary recommenders of medical care services(Friedman, et al., 2005). Therefore, it would be helpful for psychiatrists and psychiatric medical personnel to become familiarized with cancer preventive care services so that they can provide timely education and encouragement to their patients on cancer screening and reduce the patients’ cancer risks.
4.1Limitations
In this study, the use of screening mammography by women with mental disabilities was investigated by analyzing data from secondary databases. Because these databases did not include information on the study participants’ health literacy and lifestyle or whether the participants were living in institutions, these factors were not included in our analysis. Also, the premium-based monthly salary, used as a proxy for economic status in this study, does not necessarily represent an individual’s entire income.
5. Conclusion
Our results show that relative to Taiwanese women in general, Taiwanese women with mental disabilities are far less likely to undergo mammography screening. Higher likelihoods of screening mammography use in this group are associated with higherincome, higher education level, presence of catastrophic illness/injury, and experience with other preventive health care services.
List of abbreviations CI: Confidence interval;
NT$: New Taiwan Dollar; OR: Odds Ratio;
SAS:Statistics Analysis System;
Acknowledgements
This study was supported by grants (CMU101-ASIA-14) from China Medical University and Asia University, and grants (No.9805006A) from the Health
Promotion Administration. The preventive health care files were obtained from the Health Promotion Administration, Ministry of Health and Welfarein Taiwan. We are also grateful for use of the National Health Insurance Research Database provided by the Ministry of Health and Welfare, Taiwan. The interpretations and conclusions contained herein do not represent those of the Health Promotion Administration in Taiwan.
Reference
Amaddeo, F., & Jones, J. (2007). What is the impact of socio-economic inequalities on the use of mental health services? Epidemiologia E Psichiatria Sociale, 16, 16-19.
Bunce, D. F., 2nd, Jones, L. R., Badger, L. W., & Jones, S. E. (1982). Medical illness in psychiatric patients: barriers to diagnosis and treatment. Southern Medical Journal, 75, 941-944.
Carney, C. P., & Jones, L. E. (2006). The influence of type and severity of mental illness on receipt of screening mammography. Journal Of General Internal Medicine, 21, 1097-1104.
Carney, C. P., & Jones, L. E. (2006). Medical comorbidity in women and men with bipolar disorders: a population-based controlled study. Psychosomatic Medicine, 68, 684-691.
Chang, C. K., Hayes, R. D., Broadbent, M., Fernandes, A. C., Lee, W., Hotopf, M., & Stewart, R. (2010). All-cause mortality among people with serious mental illness (SMI), substance use disorders, and depressive disorders in southeast London: a cohort study. BMC Psychiatry, 10, 77-77.
Chang, K. J., Kuo, W. H., & Wang, M. Y. (2008). The epidemiology of breast cancer in Taiwan. Journal of Oncology Society, 24, 85-93.
Cole, M. G. (2007). Does depression in older medical inpatients predict mortality? A systematic review. General Hospital Psychiatry, 29, 425-430.
Cullati, S., Charvet-Bérard, A. I., & Perneger, T. V. (2009). Cancer screening in a middle-aged general population: factors associated with practices and attitudes. BMC Public Health, 9, 118.
Daumit, G. L., Pratt, L. A., Crum, R. M., Powe, N. R., & Ford, D. E. (2002).
Characteristics of primary care visits for individuals with severe mental illness in a national sample. General Hospital Psychiatry, 24, 391-395.
Druss, B. G., & Rosenheck, R. A. (1997). Use of medical services by veterans with mental disorders. Psychosomatics, 38, 451-458.
Friedman, L. C., Puryear, L. J., Moore, A., & Green, C. E. (2005). Breast and colorectal cancer screening among low-income women with psychiatric disorders. Psycho-Oncology, 14, 786-791.
Halbreich, U., Shen, J., & Panaro, V. (1996). Are chronic psychiatric patients at increased risk for developing breast cancer? The American Journal Of Psychiatry, 153, 559-560.
mammography participation in Canada: an integrative review of the literature. Current Oncology (Toronto, Ont.), 16, 65-75.
Health Promotion Administration, M. o. H. a. W. (2009). Bureau of Health Promotion Annual Report 2008-2009. In (Vol. 2014): Health Promotion Administration, Ministry of Health and Welfare
Health Promotion Administration, M. o. H. a. W. (2012). Bureau of Health Promotion Annual Report 2012. In (Vol. 2014): Health Promotion Administration, Ministry of Health and Welfare
Humphrey, L. L., Helfand, M., Chan, B. K. S., & Woolf, S. H. (2002). Breast cancer screening: a summary of the evidence for the U.S. Preventive Services Task Force. Annals of Internal Medicine, 137, 347-360.
Insel, T. R. (2008). Assessing the economic costs of serious mental illness. The American Journal Of Psychiatry, 165, 663-665.
International Agency for Research on Cancer, I. (2010). GLOBOCAN 2008:Breast Cancer Incidence, Mortality and Prevalence Worldwide in 2008. In (Vol. 2013).
Kalager, M., Zelen, M., Langmark, F., & Adami, H.-O. (2010). Effect of screening mammography on breast-cancer mortality in Norway. The New England Journal Of Medicine, 363, 1203-1210.
Kash, K. M., & Dabney, M. K. (2001). Psychological aspects of cancer screening in high-risk populations. Medical And Pediatric Oncology, 36, 519-524.
Kisely, S., Crowe, E., & Lawrence, D. (2013a). Cancer-related mortality in people with mental illness. JAMA Psychiatry, 70, 209-217.
Kisely, S., Crowe, E., & Lawrence, D. (2013b). Cancer-related mortality in people with mental illness. JAMA Psychiatry (Chicago, Ill.), 70, 209-217.
Koroukian, S. M., Bakaki, P. M., Golchin, N., Tyler, C., & Loue, S. (2012). Mental illness and use of screening mammography among Medicaid beneficiaries. American Journal Of Preventive Medicine, 42, 606-609.
Kung, P. T., Tsai, W. C., & Chiou, S. J. (2012). The assessment of the likelihood of mammography usage with relevant factors among women with disabilities. Research In Developmental Disabilities, 33, 136-143.
Lai, C. Y., Lai, C. M., Chen, C. Y., & Koo, M. (2012). [Factors associated with non-utilization of mammographic screening services in middle-aged and elderly women in Taiwan]. Hu Li Za Zhi The Journal Of Nursing, 59, 61-71.
Masterson, E. A., Hopenhayn, C., & Christian, W. J. (2010). Self-reported mental health status and recent mammography screening. Journal Of Women's Health (2002), 19, 1569-1576.
In (Vol. 2013). Taipei, Taiwan: Ministry of Health and Welfare.
Organization, W. H. (2008). World cancer report 2008. In (Vol. 2013): World Health Organization.
Owen, C., Jessie, D., & De Vries Robbe, M. (2002). Barriers to cancer screening amongst women with mental health problems. Health Care For Women International, 23, 561-566.
Penn, D. L., & Martin, J. (1998). The stigma of severe mental illness: some potential solutions for a recalcitrant problem. The Psychiatric Quarterly, 69, 235-247. Pirraglia, P. A., Sanyal, P., Singer, D. E., & Ferris, T. G. (2004). Depressive symptom
burden as a barrier to screening for breast and cervical cancers. Journal Of Women's Health (2002), 13, 731-738.
Schueler, K. M., Chu, P. W., & Smith-Bindman, R. (2008). Factors associated with mammography utilization: a systematic quantitative review of the literature. Journal of Women's Health (15409996), 17, 1477-1498.
Shidhaye, R., & Patel, V. (2010). Association of socio-economic, gender and health factors with common mental disorders in women: a population-based study of 5703 married rural women in India. International Journal Of Epidemiology, 39, 1510-1521.
Steiner, J. L., Hoff, R. A., Moffett, C., Reynolds, H., Mitchell, M., & Rosenheck, R. (1998). Preventive health care for mentally ill women. Psychiatric Services (Washington, D.C.), 49, 696-698.
Vigod, S. N., Kurdyak, P. A., Stewart, D. E., Gnam, W. H., & Goering, P. N. (2011). Depressive symptoms as a determinant of breast and cervical cancer
screening in women: a population-based study in Ontario, Canada. Archives Of Women's Mental Health, 14, 159-168.
Werneke, U., Horn, O., Maryon-Davis, A., Wessely, S., Donnan, S., & McPherson, K. (2006). Uptake of screening for breast cancer in patients with mental health problems. Journal Of Epidemiology And Community Health, 60, 600-605. Yee, E. F. T., White, R., Lee, S. J., Washington, D. L., Yano, E. M., Murata, G., Handanos,
C., & Hoffman, R. M. (2011). Mental illness: is there an association with cancer screening among women veterans? Women's Health Issues: Official Publication Of The Jacobs Institute Of Women's Health, 21, S195-S202.
Table 1 Use of screening mammography among women with mental disabilities: basic characteristics and bivariate analysis.
Variable Total Use Did not use χ2
N=17,243 % n1=1,515 % n2=15,728 % p-value Gender -Female 17,243 100.00 1,515 8.79 15,728 91.21 Age 0.002* 50–59 years 11,734 68.05 1,085 9.25 10,649 90.75 60–69 years 5,509 31.95 430 7.81 5,079 92.19 Urbanization level 0.331 Level 1 2,916 16.91 265 9.09 2,651 90.91 Level 2 4,173 24.20 335 8.03 3,838 91.97 Level 3 2,712 15.73 245 9.03 2,467 90.97 Level 3 1,490 8.64 134 8.99 1,356 91.01 Level 5 2,350 13.63 205 8.72 2,145 91.28 Level 6 1,643 9.53 135 8.22 1,508 91.78 Level 7 1,397 8.10 138 9.88 1,259 90.12 Level 8 562 3.26 58 10.32 504 89.68
Premium-based monthly salary (NT$) <0.001*
Dependent population 6,212 36.03 537 8.64 5,675 91.36 <15,840 5,840 33.87 357 6.11 5,483 93.89 16,500–22,800 3,314 19.22 344 10.38 2,970 89.62 24,000–28,800 767 4.45 115 14.99 652 85.01 30,300–36,300 658 3.82 94 14.29 564 85.71 38,200–45,800 452 2.62 68 15.04 384 84.96 Education level 0.001*
Elementary school and under 8,708 50.50 695 7.98 8,013 92.02 Junior high school 2,157 12.51 206 9.55 1,951 90.45 Senior high/vocational school 3,128 18.14 305 9.75 2,823 90.25 Junior college/university and above 1,492 8.65 155 10.39 1,337 89.61
Unknown 1,758 10.20 154 8.76 1,604 91.24
Marital status <0.001*
Married 8,868 51.43 862 9.72 8,006 90.28
Unmarried 2,066 11.98 106 5.13 1,960 94.87
Divorced and widowed 1,395 8.09 93 6.67 1,302 93.33
Table 1 (continued)
Variable Total Use Did not use χ2
N=17,243 % n1=1,515 % n2=15,728 % p-value
Catastrophic illness/injury 0.002*
Yes 15,408 89.36 1,389 9.01 14,019 90.99
No 1,835 10.64 126 6.87 1,709 93.13
Relevant chronic illnesses
Cancer 0.129 Yes 589 3.42 62 10.53 527 89.47 No 16,654 96.58 1,453 8.72 15,201 91.28 Diabetes mellitus 0.181 Yes 3,628 21.04 339 9.34 3,289 90.66 No 13,615 78.96 1,176 8.64 12,439 91.36 Severity of disability <0.001* Mild 4,154 24.09 592 14.25 3,562 85.75 Moderate 9,142 53.02 763 8.35 8,379 91.65 Severe 3,607 20.92 151 4.19 3,456 95.81 Very severe 340 1.97 9 2.65 331 97.35
Other preventive health care usage
Pap smear <0.001*
Yes 7,315 42.42 1,270 17.36 6,045 82.64
No 9,928 57.58 245 2.47 9,683 97.53
Adult preventive health care <0.001*
Yes 4,496 26.07 722 16.06 3,774 83.94
No 12,747 73.93 793 6.22 11,954 93.78
Table 2 Logistic regression models for screening mammography use among women with mental disabilities.
Variable Unadjusted model Adjusted model
OR 95% CI p-value OR 95% CI p-value Age 50–59 years - - - -60–69 years 0.83 0.74 0.93 0.002* 0.95 0.84 1.08 0.442 Urbanization level Level 1 - - - -Level 2 0.87 0.74 1.03 0.115 0.89 0.74 1.07 0.198 Level 3 0.99 0.83 1.19 0.944 0.91 0.74 1.11 0.343 Level 3 0.99 0.80 1.23 0.918 0.97 0.77 1.23 0.825 Level 5 0.96 0.79 1.16 0.645 0.91 0.74 1.12 0.376 Level 6 0.90 0.72 1.11 0.318 0.89 0.70 1.13 0.346 Level 7 1.10 0.88 1.36 0.404 0.97 0.76 1.24 0.799 Level 8 1.15 0.85 1.55 0.357 1.00 0.72 1.40 0.981 Premium-based monthly salary (NT$)
<15,840 - - - Dependent population 1.45 1.27 1.67 <0.001* 1.03 0.87 1.21 0.750 16,500–22,800 1.78 1.52 2.08 <0.001* 1.09 0.90 1.31 0.384 24,000–28,800 2.71 2.16 3.39 <0.001* 1.38 1.07 1.78 0.014* 30,300–36,300 2.56 2.01 3.27 <0.001* 1.22 0.93 1.60 0.158 38,200–45,800 2.72 2.06 3.60 <0.001* 1.47 1.08 2.00 0.014* Education level
Elementary school and under - - -
-Junior high school 1.22 1.03 1.43 0.018* 1.16 0.97 1.38 0.096 Senior high/vocational school 1.25 1.08 1.44 0.002* 1.29 1.10 1.51 0.002* Junior college/university and above 1.34 1.11 1.61 0.002* 1.57 1.28 1.94 <0.001* Unknown 1.11 0.92 1.33 0.276 1.10 0.91 1.34 0.334 Marital status
Unmarried - - -
-Married 1.99 1.62 2.45 <0.001* 1.09 0.86 1.37 0.490 Divorced and widowed 1.32 0.99 1.76 0.058 0.79 0.58 1.08 0.145 Unknown 1.88 1.51 2.34 <0.001* 1.19 0.93 1.51 0.161 Catastrophic illness/injury
No - - -
-Yes 1.34 1.11 1.62 0.002* 1.40 1.15 1.72 0.001* Relevant chronic illnesses
Cancer 1.23 0.94 1.61 0.130 0.89 0.67 1.18 0.400 Diabetes mellitus 1.09 0.96 1.24 0.182 1.00 0.88 1.15 0.960
Table 2 (continued)
Variable Unadjusted model Adjusted model
OR 95% CI p-value OR 95% CI p-value Severity of disability Mild - - - -Moderate 0.55 0.49 0.61 <0.001* 0.69 0.61 0.78 <0.001* Severe 0.26 0.22 0.32 <0.001* 0.45 0.37 0.55 <0.001* Very severe 0.16 0.08 0.32 <0.001* 0.34 0.17 0.69 0.002* Other preventive health care usage
Pap smear
No - - -
-Yes 8.30 7.22 9.56 <0.001* 6.42 5.55 7.44 <0.001* Adult preventive health care
No - - -
-Yes 2.88 2.59 3.21 <0.001* 2.20 1.96 2.46 <0.001*