行政院國家科學委員會專題研究計畫 期中進度報告
(子計畫五)腸病毒 71 型宿主基因分析-找尋易感染或抗
感染之基因(2/3)
計畫類別: 整合型計畫 計畫編號: NSC92-3112-B-002-046- 執行期間: 92 年 05 月 01 日至 93 年 04 月 30 日 執行單位: 國立臺灣大學醫學院小兒科 計畫主持人: 張鑾英 共同主持人: 熊昭,張仲明 報告類型: 完整報告 處理方式: 本計畫可公開查詢中 華 民 國 93 年 4 月 22 日
Component Project No. ___5___
NSC Funding Number: NSC 93-3112-B-002-024 (
93年度國科會預核編號) (in Chinese) 中文腸病毒
71 型宿主基因分析--找尋易感染或抗感染之基因
Title of Component Project 子計畫名稱 (in English) 英文Host Genetic Factors of EV71 Infection: Identification of
Host Susceptible or Resistant Genes
(in Chinese) 中文
台灣大學醫學院小兒科
Institution
研究(執行)單位
(in English) 英文
Department of Pediatrics, College of Medicine, National
Taiwan University
(in Chinese) 中文張 鑾 英
Principle Investigator 子計畫主持人 (in English) 英文Luan-Yin Chang
FY
2002 2003 2004 Total
Budget
2,974,400 3,112,800
3,014,100 9,101,300
(in NT dollars: 1USD = 34 NTD)Component Project No. ___5___
((請填入子計畫編號)Progress Report
B1. Response to previous reviewers’ critiques
Please describe the previous reviewers’ critiques and how based on the critiques, you
made modifications to specific aims, experimental design, or resource allocation etc.
1. Previous critique of Reviewer #1
Some initial case-control studies and data collection have been done. However, no significant associations have been found. The candidate gene approach may have some difficulty in this particular case. It seems that some alternative and novel methods are called for.
Suggest to better integrate this line of approach with project 1, 3 and 4.
Response to Reviewer #1’s comments
(1). We have found some genes related to susceptibility of EV71 infection. The data are shown in Tables 4 to 11. The most important genes are Type II TNF-α promoter and HLA-A33.
(2). For other alternative and novel methods, we have better integrated this project with the other. For examples, PCR and sequencing of the second group of candidate genes which have differential expression and significant protein interaction in EV71 infected cells (Project 2, 3 &4), their regulatory genes and EV71 receptor gene. Statistic and bioinformatic analysis of the second group of candidate genes in co-operation with Project 1. Project 2 “Neuropathogenesis Study of Enterovirus 71 Infection via Gene Arrays and
Bioinformatics” revealed that there was significant gene expression of some chemokines, so
we will measure chemokines of the stored serum from EV71 cases to delineate whether chemokines correlate with clinical outcomes. Project 3 “Global Molecular Profiling of
Enterovirus-Host Interaction on Cellular Signaling” revealed some important gene
expression, so we will test whether such differential gene expression occurs in EV71 cases.
2. Previous critique of Reviewer #2
genetic variations. A very impressive effort in patient recruitment for the study is present in the progress report. These recruits include 151 EV71 and 100 control cases, and near 100 families with 100 case-parent trio and 100 sibship pairs. Using this clinical resource, various studies were carried out including the geneotyping of TNF-α and IL-6 promoters. Preliminary results suggested a correlation of Type II TNF-α promoter polymorphism with increase of EV71 infection. However, this polymorphism, together with IL-6 promoter region, has no significant impact on the outcome of the infection. This is very outstanding progress.
Overall, the progress is outstanding. A continuous effort in this approach will yield useful clinical data for this disease. However, this project needs a substantial input from basic scientists regarding to the function of these genetic polymorphisms. It will be interested initially to elucidate the effect of type II TNF-α promoter polymorphism in EV71 infection in vitro.
Response to Reviewer #2’s comments
(1). Indeed, we tried very hard to recruit the EV71 cases and their families. During the case and family recruitment, we have finished the study “Transmission and clinical features of enterovirus 71 infections in household contactsin Taiwan” which will be published in JAMA in Jan 2004. We have also analyzed outcome of all the EV71 cases in Chang Gung Children’s Hospital from 1998 to 2002, and the results will be published in Ped Infect Dis J next year. We still continue to recruit the EV71 cases. We also did other candidate genes and found HLA-A33 is another important susceptible gene of EV71 infection.
(2). Input from basic scientists regarding to the function of these genetic polymorphisms, such as to elucidate the effect of type II TNF-α promoter polymorphism in EV71 infection in vitro. We did
in vitro lymphocyte proliferation and cytokine response after EV71 stimulation in some EV71
Component Project No. _5___
((請填入子計畫編號)B2. Specific Aims
Please state the overall goals of the project, and specific aims, as reviewed and
approved by the Study Section and actually awarded. If these specific aims as
actually funded did not differ in scope from those actually pursued during the grant
period, and if the aims have not been modified, state this. If they have been modified,
give the revised aims.
1. Comparison of gene variants in EV71 cases with different severity and normal
children to find susceptible or resistant genes and genetic polymorphism related
to the clinical outcomes
2. To find the strength of disease associations with different combinations of
polymorphism
3. Pathogenesis of EV71-related fatal pulmonary edema
4. Provide therapeutic guidelines for EV71 infections: to discover genes encoding
novel molecules that fight EV71 infection and to pinpoint critical pathways in
immune regulation, leading to new therapeutic strategies for EV71 infection,
especially fatal pulmonary edema
Component Project No. _5___
((請填入子計畫編號)B3. Progress Summary
Summarize concisely the results obtained for
each specific aim during the past
year (or reporting period)
. Negative results, if any, should also be included and
approaches taken to improve the prospects of the project discussed. (Do not exceed
5 pages
, not including figures and references.)
1.
Case enrollment for EV71 cases and their families, and household EV71 transmission ratesAlthough enterovirus 71 has caused epidemics associated with significant morbidity and
mortality, its transmission has not been thoroughly investigated. From February 2001 to August 2002, we performed a prospective family cohort study to evaluate enterovirus 71 transmission and clinical outcomes within households. These patients and household members underwent clinical evaluations, virologic studies and questionnaire-based interviews (Figure). Enterovirus 71 infection was defined as positive viral isolation, IgM or four-fold change of neutralizing antibody; clinical syndromes defined as asymptomatic, uncomplicated symptomatic and complicated; unfavorable outcome of sequelae or death. We studied 433 family members from 94 families with positive enterovirus 71 isolation (Figure 1). The overall enterovirus 71 transmission rate of household contacts was 52% (176/339): 84% (70/83) siblings, 83% (19/23) cousins, 41% (72/175) parents, 28% (10/36) grandparents and 26% (5/19) uncles/aunts (Table 1). Of 183 infectedchildren, 6% (11/183) were asymptomatic, 73% (133/183) had uncomplicated illnesses of hand, foot and mouth disease, herpangina or nonspecific febrile illness and 21% (39/183) suffered from complications of central nervous system involvement and/or cardiopulmonary failure. During the 6-month follow-up, 10 died and 13 had sequelae of dysfunction in swallowing, cranial nerve palsies, central hypoventilation or limb weakness/atrophy. Age younger than 3 years was the most significant factor associated with unfavorable outcomes in children (P=.004). Among 87 infected adults, 53% (46/87) were asymptomatic, 39% (34/87) had nonspecific illnesses of fever, sore throat or gastrointestinal discomfort and only 8% (7/87) had hand, foot and mouth disease. Enterovirus 71 household transmission rates are high for children, medium for parents and low for
other adults. Serious complications, sequelae and death are associated with young children. (JAMA, 2004;291(2), in press)
2. Clinical syndromes and Outcomes of EV71 cases
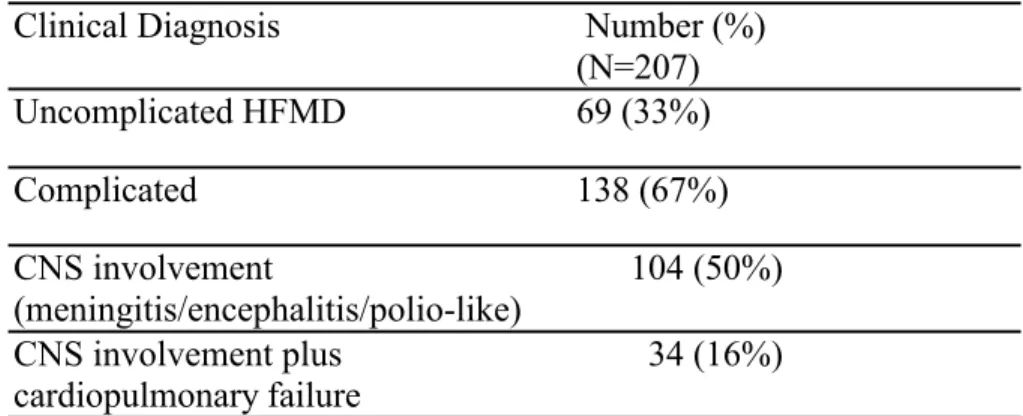
A total of 250 EV71 cases and 140 families were collected; 97 control cases had been collected. We have completed the clinical analyses and gene polymorphism study of 207 EV71 cases and 97 normal control children. The clinical syndromes of the 207 EV71 cases are as the following: 33% (69/207) of the cases were uncomplicated, 67% (138/207) were complicated cases: 50% (104/207) had central nervous system involvement, such as meningitis, myoclonic jerk, encephalitis, polio-like syndrome, etc and 17% (34/207) developed cardiopulmonary failure soon after CNS involvement (Table 2). After intensive resuscitation and medical care, eleven (5%) children died and 46 (22%) children had sequelae of dysphagia, central hypoventilation, cranial nerve palsy and limb weakness/atrophy (Table 3).
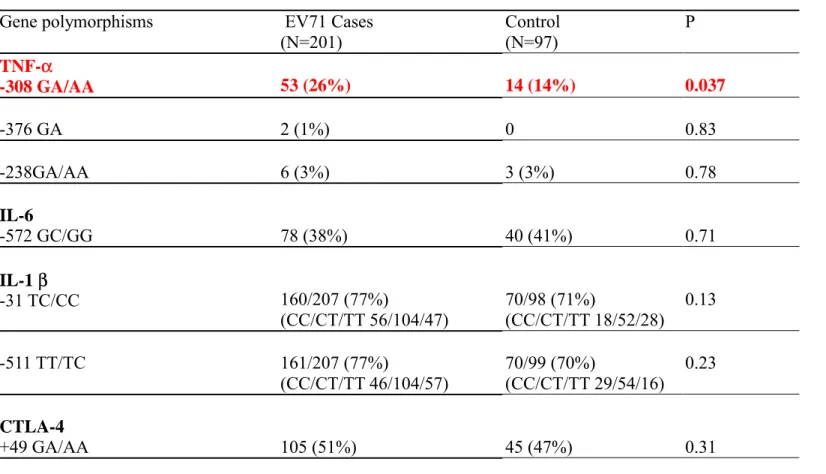
3. Polymorphisms of Candidate Genes, TNF-α promoter, IL6 promoter, IL-1β, CTLA4 and HLA, in EV71 Cases and Normal Control
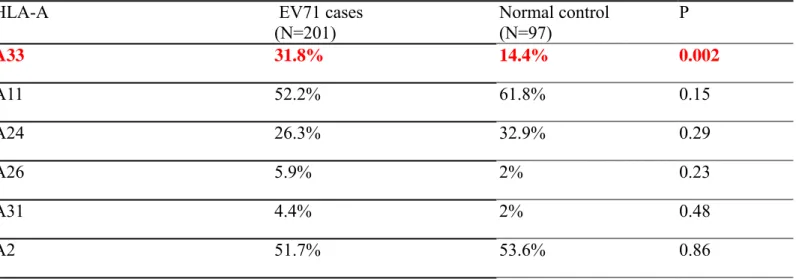
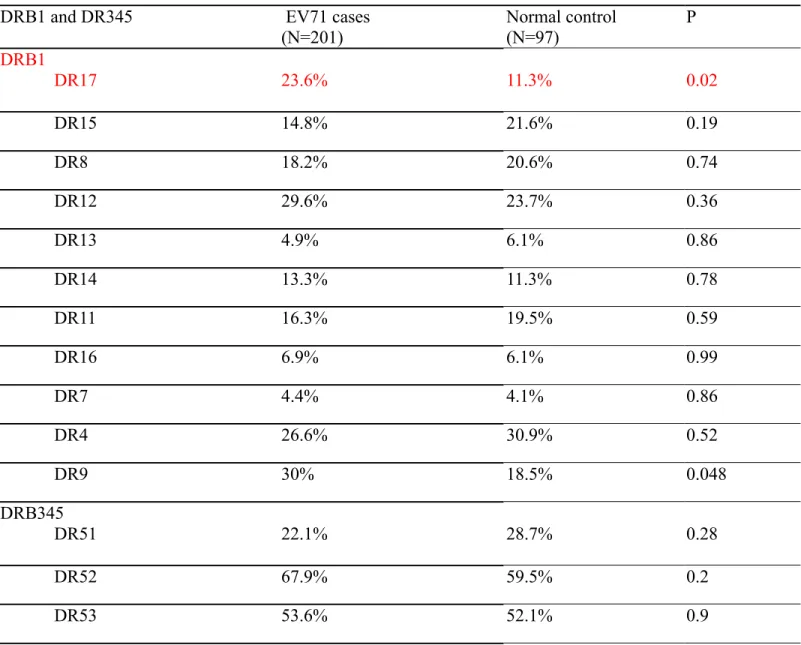
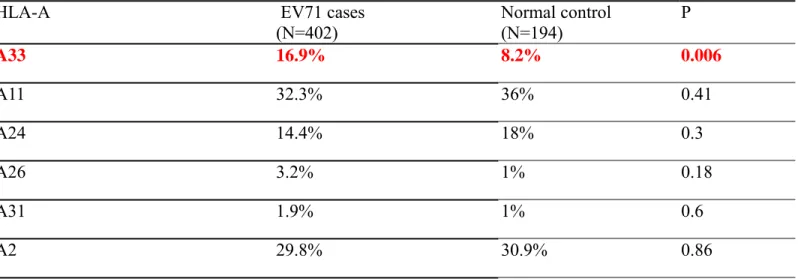
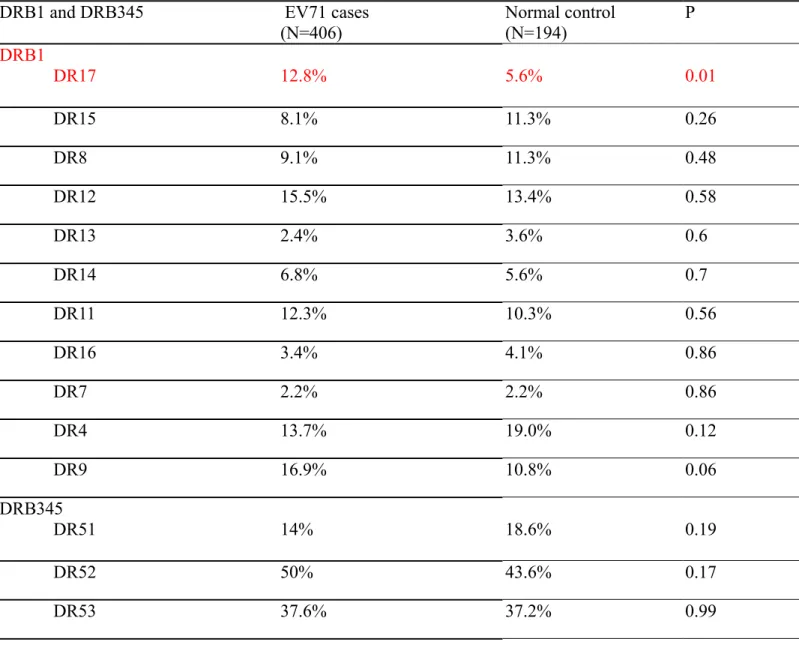
Polymorphisms of candidate genes including TNF-α promoter, IL6 promoter, IL-1β, CTLA4 were detected with PCR, appropriate restriction enzyme and automatic gene sequencing. HLA typing was performed SSP (sequence-specific primer). As Table 4 shows, the incidence (25%, 52/206) of TNF-α type II promoter in EV71 cases was significantly higher than the incidence (15%, 14/96) in normal children (p=0.05); the incidence of IL-1 β promoter -511TT/TC in EV71 cases was higher than normal control children (82% vs. 66%, p=0.014, Table 4). With SSP (sequence-specific primer), the percentage (31.8%, 64/201) of HLA-A33 in EV71 cases was also significantly higher than that (14.4%, /97) in normal children (p=0.002, Table 5). The percentage (23.6%, 48/203) of HLA-DR17 in EV71 cases was also significantly higher than that (11%, 11/97) in normal children (p=0.02, Table 7).The gene frequency of HLA-A33 and DR17 in EV71 cases
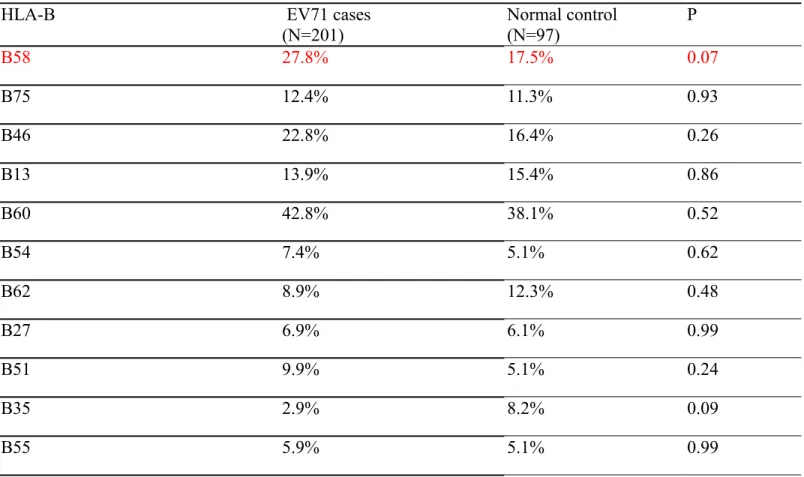
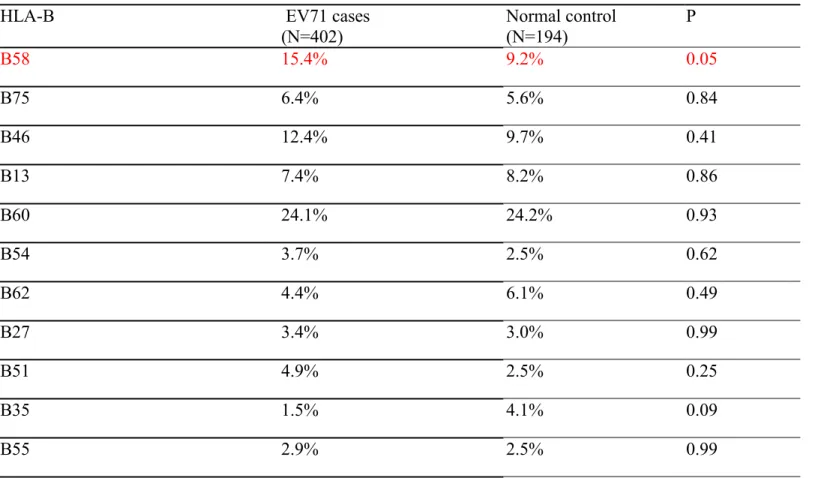
was also higher than that in normal control children (Tables 8 and 10). The gene frequency of HLA-B and HLA-DR345 was not significantly different between EV71 cases and normal control children (Tables 6, 7, 9 and 10).
4. Specific haplotypes, HLA DR17-TNF-α II-B58-A33 and HLA DR9-TNF-α I-B46-A2 in EV71 cases and normal control
More EV71 cases had the haplotypes of HLA DR17-TNF-α II-B58-A33 and HLA DR9-TNF-α I-B46-A2 than the normal control (9.5% vs. 2.6%, p=0.003; 7.0% vs. 1.5%, p=0.008, respectively, Table 11).
5. Polymorphisms of Candidate Genes, TNF-α promoter, IL6 promoter, IL-1β, CTLA4 and HLA, and Clinical Outcomes of EV71 Cases
Up to now, polymorphisms of the studied candidate genes, TNF-α promoter, IL6 promoter, Il-1 β, CTLA4 and HLA did not affect the clinical outcomes of EV71 cases.
Further case collection, and sequencing of the second group of candidate genes such as EV71 receptor and their regulatory genes will be done in the future. Thereafter, we will compare genetic variants among EV71 cases with different severity and normal children to find susceptible or resistant genes and genetic polymorphism related to clinical outcomes, to find the strength of disease associations with different combinations of polymorphism.
Table 1. Demographic Data and Rates for Isolating EV71, Detecting EV71 IgM, Demonstrating Seropositivity for Neutralizing Antibodies and
Infection Among the Index Cases and Household Contacts Subjects Number Age, mean (SD), y Sex
(Male/ Female) Positive EV71 Isolation Rate Positive EV71 IgM Rate EV71 Seropositivity Rate† Infection Rate
‡ Total subjects* 433 20.9 (18.4) 223/210 28% (119/433) 47% (201/425) 93% (401/429) 62% (270/433) Index case 94 3.1 (2.1) 56/38 72% (68/94) 94% (85/90) 98% (90/92) 100% (94/94) Household contacts 339 25.8 (17.8) 167/172 15% (51/339) 35% (116/335) 92% (311/337) 52% (176/339) Children household contacts 106 4.5 (4.6) 60/46 39% (41/106) 76% (79/104) 95% (99/104) 84% (89/106) Siblings 83 4.4 (3.8) 46/37 40% (33/83) 78% (63/81) 96% (78/81) 84% (70/83) Cousins 23 5.0 (6.8) 14/9 35% (8/23) 70% (16/23) 91% (21/23) 83% (19/23) Adults household contacts 233 35.7 (12.0) 107/126 4.3% (10/233) 16% (37/231) 91% (212/233) 37% (87/233) Parents 175 31.5 (5.4) 83/92 5% (9/175) 17% (29/175) 91% (159/175) 41% (72/175) Grandparents 36 59.3 (10.4) 14/22 0% (0/36) 15% (5/34) 94% (34/36) 28% (10/36) Uncles/aunts 19 27.4 (8.7) 10/9 5% (1/19) 16% (3/19) 84% (16/19) 26% (5/19) Babysitters 3 36.6 (7.7) 0/3 0% (0/3) 0% (0/3) 100% (3/3) 0% (0/3) Abbreviation: EV71, enterovirus 71; SD, standard deviation.
*Total subjects included index cases and household contacts.
† EV71 seropositivity was defined as an EV71 neutralizing antibody titer ≥8 .
Table 2. Clinical Syndromes of EV71 Cases
Clinical Diagnosis Number (%) (N=207) Uncomplicated HFMD 69 (33%) Complicated 138 (67%) CNS involvement (meningitis/encephalitis/polio-like) 104 (50%) CNS involvement plus cardiopulmonary failure 34 (16%)
Table 3. Clinical Outcomes of EV71 Cases
Clinical Outcome Number (%) (N=207) Complete recovery 150 (72%) With sequelae 46 (22%)
Table 4. TNF-α promoter, IL-6 promoter, IL-1 β promoter and CTLA-4 polymorphisms in EV71 Cases and Normal Control
Gene polymorphisms EV71 Cases (N=201) Control (N=97) P TNF-α -308 GA/AA 53 (26%) 14 (14%) 0.037 -376 GA 2 (1%) 0 0.83 -238GA/AA 6 (3%) 3 (3%) 0.78 IL-6 -572 GC/GG 78 (38%) 40 (41%) 0.71 IL-1 β -31 TC/CC 160/207 (77%) (CC/CT/TT 56/104/47) 70/98 (71%) (CC/CT/TT 18/52/28) 0.13 -511 TT/TC 161/207 (77%) (CC/CT/TT 46/104/57) 70/99 (70%) (CC/CT/TT 29/54/16) 0.23 CTLA-4 +49 GA/AA 105 (51%) 45 (47%) 0.31
Table 5. HLA-A Gene percentage for EV71 cases and normal control
HLA-A EV71 cases (N=201) Normal control (N=97) P A33 31.8% 14.4% 0.002 A11 52.2% 61.8% 0.15 A24 26.3% 32.9% 0.29 A26 5.9% 2% 0.23 A31 4.4% 2% 0.48 A2 51.7% 53.6% 0.86
Table 6. HLA-B Gene percentage for EV71 cases and normal control
HLA-B EV71 cases (N=201) Normal control (N=97) P B58 27.8% 17.5% 0.07 B75 12.4% 11.3% 0.93 B46 22.8% 16.4% 0.26 B13 13.9% 15.4% 0.86 B60 42.8% 38.1% 0.52 B54 7.4% 5.1% 0.62 B62 8.9% 12.3% 0.48 B27 6.9% 6.1% 0.99 B51 9.9% 5.1% 0.24 B35 2.9% 8.2% 0.09 B55 5.9% 5.1% 0.99
Table 7. HLA-DRB1 and DR345 Gene percentage for EV71 cases and normal control
DRB1 and DR345 EV71 cases (N=201) Normal control (N=97) P DRB1 DR17 23.6% 11.3% 0.02 DR15 14.8% 21.6% 0.19 DR8 18.2% 20.6% 0.74 DR12 29.6% 23.7% 0.36 DR13 4.9% 6.1% 0.86 DR14 13.3% 11.3% 0.78 DR11 16.3% 19.5% 0.59 DR16 6.9% 6.1% 0.99 DR7 4.4% 4.1% 0.86 DR4 26.6% 30.9% 0.52 DR9 30% 18.5% 0.048 DRB345 DR51 22.1% 28.7% 0.28 DR52 67.9% 59.5% 0.2 DR53 53.6% 52.1% 0.9
Table 8. HLA-A Gene frequency for EV71 cases and normal control
HLA-A EV71 cases (N=402) Normal control (N=194) P A33 16.9% 8.2% 0.006 A11 32.3% 36% 0.41 A24 14.4% 18% 0.3 A26 3.2% 1% 0.18 A31 1.9% 1% 0.6 A2 29.8% 30.9% 0.86
HLA-A Gene frequency for EV71 cases and reference
HLA-A EV71 cases (N=402) Reference- Min-Nan (N=14274) P A33 16.9% 11.56% 0.001 A11 32.3% 34.87% 0.311 A24 14.4% 16.59% 0.272 A26 3.2% 1.31% 0.003 A31 1.9% 1.24% 0.345 A2 29.8% 31.71% 0.449
Table 9. HLA-B Gene frequency for EV71 cases and normal control
HLA-B EV71 cases (N=402) Normal control (N=194) P B58 15.4% 9.2% 0.05 B75 6.4% 5.6% 0.84 B46 12.4% 9.7% 0.41 B13 7.4% 8.2% 0.86 B60 24.1% 24.2% 0.93 B54 3.7% 2.5% 0.62 B62 4.4% 6.1% 0.49 B27 3.4% 3.0% 0.99 B51 4.9% 2.5% 0.25 B35 1.5% 4.1% 0.09 B55 2.9% 2.5% 0.99
HLA-B Gene frequency for EV71 cases and reference control
HLA-B EV71 cases (N=402) Reference- Min-Nan (N=14274) P B58 15.4% 10.66% 0.003 B75 6.4% 3.88% 0.015 B46 12.4% 14.61% 0.243 B13 7.4% 8.32% 0.57 B60 24.1% 20.85% 0.129 B54 3.7% 2.54% 0.197 B62 4.4% 8.65% 0.004 B27 3.4% 2.72% 0.504 B51 4.9% 6.03% 0.404 B35 1.5% 1.51% 0.848 B55 2.9% 2.95% 0.927
Table 10. HLA-DRB1 Gene frequency for EV71 cases and normal control
DRB1 and DRB345 EV71 cases (N=406) Normal control (N=194) P DRB1 DR17 12.8% 5.6% 0.01 DR15 8.1% 11.3% 0.26 DR8 9.1% 11.3% 0.48 DR12 15.5% 13.4% 0.58 DR13 2.4% 3.6% 0.6 DR14 6.8% 5.6% 0.7 DR11 12.3% 10.3% 0.56 DR16 3.4% 4.1% 0.86 DR7 2.2% 2.2% 0.86 DR4 13.7% 19.0% 0.12 DR9 16.9% 10.8% 0.06 DRB345 DR51 14% 18.6% 0.19 DR52 50% 43.6% 0.17 DR53 37.6% 37.2% 0.99
HLA-DRB1 Gene frequency for EV71 cases and reference control
DRB1 and DRB345 EV71 cases (N=406) Reference- Min-Nan (N=14274) P DRB1 DR17 12.8% 8.37% 0.002 DR15 8.1% 9.92% 0.259 DR8 9.1% 9.12% 0.94 DR12 15.5% 14.1% 0.468 DR13 2.4% 3.74% 0.202 DR14 6.8% 6.35% 0.792 DR11 12.3% 7.99% 0.002 DR16 3.4% 3.9% 0.701 DR7 2.2% 2.19% 0.874 DR4 13.7% 14.8% 0.586 DR9 16.9% 15.41% 0.45
Table 11. Specific Haplotypes for EV71 cases and normal control
Haplotype EV71 cases (N=412) Normal control (N=196) P HLA DR17-TNF-α II-B58-A33 9.5% 2.6% 0.003 HLA DR9-TNF-α I-B46-A2 7.0% 1.5% 0.008
Component Project No. ___5___
((請填入子計畫編號)B4. Projected Timeline & Brief Summary of Plans for Next Year
Provide a short paragraph to describe the plans for next year including a realistic
timetable and appropriate milestones for the project, based on the progress reached
so far. (Do not exceed
1 page
.)
1. PCR and sequencing of candidate genes for the siblings and parents to test whether there is
gene transmission distortion with STDT and TDT tests, which will be performed in cooperation with Project 1.
2. PCR and sequencing of the second group of candidate genes which have differential expression and significant protein interaction in EV71 infected cells (Project 2, 3 &4), their regulatory genes and EV71 receptor gene.
3. Statistic and bioinformatic analysis of the second group of candidate genes in co-operation with Project 1
4. Project 2 “Neuropathogenesis Study of Enterovirus 71 Infection via Gene Arrays and
Bioinformatics” revealed that there was significant gene expression of some chemokines,
so we will measure chemokines of the stored serum from EV71 cases to delineate whether chemokines correlate with clinical outcomes.
5. Project 3 “Global Molecular Profiling of Enterovirus-Host Interaction on Cellular
Signaling” revealed some important gene expression, so we will test whether such
Component Project No. __5____
((請填入子計畫編號)B5. Personnel
Summarize the
personnel involved in the project during the grant period
. List
the personnel in accordance to the following categories: (1) senior investigators,
including visitors; (2) postdoctoral fellows; (3) graduate students; (4) technicians or
research assistants. Specify for each individual the period of involvement and the
percentage commitment of effort.
Name
In Chinese In English Position Title
Education
Degree % of effort Job Description or Responsibilities
張鑾英 熊昭 張俊明 張憶壽 陳光武 施信如 莊志立 施修明 林奏延 方翠嬿 王詩欣 蔡佳良 Luan-Yin Chang Chao A. Hsiung Chung-Ming Chang I-Shou Chang Guang-Wu Chen Shin-Ru Shih Jyh-Lyh Juang Hsiu-Ming Shih Tzou-Yien Lin Cui-Yen Fang Principal investigator Co- Investigator Co- Investigator Co- Investigator Co- Investigator Co- Investigator Co- Investigator Co- Investigator Co- Investigator Research Assistant Research Assistant Research Assistant M.D., Ph.D. Ph.D. Ph.D. Ph.D. Ph.D. Ph.D. Ph.D. Ph.D. M.D. BA MS MS 100% 30% 10% 20% 20% 20% 20% 20% 30% 100% 100% 100%
Attending; Chief of Division of Pediatric Infectious Diseases, Chang Gung Children’s Hospital
Director; National Health Research Institutes Director; National Health Research Institutes
Research fellow; National Health Research Institutes Research associate; National Health Research Institutes Associate professor; Chang Gung University
Assistant Research Fellow; National Health Research Institutes
Assistant Research Fellow; National Health Research Institutes
Superintendent, Chang Gung Children’s Hospital
Case/control/family cohort collection and follow-up DNA extraction, gene
polymorphism, HLA serotyping DNA extraction, gene
Component Project No. ___5___
((請填入子計畫編號)B6. Publications and/or Patents
B6a. Publications
List the title and complete references (author(s), journal or book, year, page number) of
all publications
directly resulting from studies supported by the project (i.e., with
citation of this grant in the acknowledgement section)
. List the publications for the
project in accordance to the following categories: (1) manuscripts published and
accepted for publications; (2) manuscripts submitted; and (3) conference proceedings.
Provide one copy of each publication not previously reported to the National Science
Council in the Appendix.
(1) Manuscripts published and accepted for publications
1. Chang LY, Tsao KC, Hsai SH, et al. Transmission and clinical features of enterovirus 71 infections in household contactsin Taiwan. JAMA 2004;291(2). (in press)
2. Chang LY, Hsia SH, Wu CT, et al. Outcome of EV71 Infections with or without Stage-based Management, 1998 – 2002. Ped Infect Dis J (accepted).
(3) Manuscript under preparation
TNF-α Type II promoter and HLA-A33 are related to susceptibility of EV71 infection
(4). Conference proceedings
1. Chang LY, Lu HK, Hsia SH, et al. TNF-α promoter polymorphism is not related to the severity of EV71 Infection. Acta Paediatrica Sinica 2002;43 (suppl A):115-6.
2. Luan-Yin Chang, Chao A. Hsiung, Lin-Min Huang, I-Shou Chang, Guang-Wu Chen, Shin-Ru Shih, Jyh-Lyh Juang, Hsiu-Ming Shih, Tzou-Yien Lin, Chung-Ming Chang, Chin-Yun Lee.
TNF-α Type II promoter and HLA-A33 are related to susceptibility of EV71 infection: possible susceptible genes? Acta Paediatrica Sinica 2003;44 (suppl B):239.
Component Project No. ___5___
((請填入子計畫編號)B6b. Patents
List all inventions disclosed, patents filed, and patents granted. Please note the
inventors, assignee, title of patent, country or area where patent applied for, filing or
issued number and date.
Appendix
1. Transmission and Clinical Features of EV71 Infections in Household Contacts in Taiwan (JAMA,
2004;291, in press, SCI, IF 16.783)
2. Outcome of Enterovirus 71 Infections with or without Stage-based Management, 1998 – 2002 (Ped Infect Dis J, accepted, SCI, IF 2.376)
Transmission and Clinical Features of EV71 Infections in Household Contacts in Taiwan
Luan-Yin Chang, MD, PhD, Kou-Chien Tsao, BS, Shao-Hsuan Hsia, MD, Shin-Ru Shih, PhD, Chung-Guei Huang, MS, Wing-Kai Chan, MD, Kuang-Hung Hsu, PhD, Tsui-Yen Fang, RN, Yhu-Chering Huang, MD, PhD, Tzou-Yien Lin, MD
Division of Pediatric Infectious Diseases (Drs Chang, Huang and Lin, Rn Fang), and Division of Pediatric Critical Care and Emergency Medicine (Dr Hsia), Department of Pediatrics, Chang Gung Children’s Hospital; Clinical Virology Laboratory, Chang Gung Memorial Hospital (Bs Tsao and Ms Huang); School of Medical Technology (Dr Shih), Laboratory for Epidemiology and Department of Health Care Management (Dr Hsu), Chang Gung University; Department of Medical Research (Dr Chan), National Taiwan University Hospital
Dr Chang is now with Department of Pediatrics, National Taiwan University Hospital, College of Medicine, National Taiwan University.
Corresponding Author and Reprints: Tzou-Yien Lin, MD,
Department of Pediatrics, Chang Gung Children’s Hospital, Chang Gung University, 5, Fu-Hsing Street, Kweishan, Taoyuan 333, Taiwan
Tel: 886-3-3281200 ext 8002; Fax: 886-3-3288957; E-mail: [email protected]
Short title: Household Transmission of Enterovirus 71 Word count: 2995.
Abstract
Context Although enterovirus 71 has caused epidemics associated with significant morbidity and mortality, its transmission has not been thoroughly investigated. Objective To evaluate enterovirus 71 transmission and clinical outcomes within households.
Design, Setting, and Subjects From February 2001 to August 2002, we performed a prospective family cohort study to investigate patients and family members of patients who had signs and symptoms suggestive of enterovirus 71. These patients and
household members underwent clinical evaluations, virologic studies and questionnaire-based interviews.
Main Outcome Measures Enterovirus 71 infection was defined as positive viral isolation, IgM or four-fold change of neutralizing antibody; clinical syndromes defined as asymptomatic, uncomplicated symptomatic and complicated; unfavorable outcome of sequelae or death.
Results We studied 433 family members from 94 families with positive enterovirus 71 isolation. The overall enterovirus 71 transmission rate of household contacts was 52% (176/339): 84% (70/83) siblings, 83% (19/23) cousins, 41% (72/175) parents, 28% (10/36) grandparents and 26% (5/19) uncles/aunts. Of 183 infected children, 6% (11/183) were asymptomatic, 73% (133/183) had uncomplicated illnesses of hand, foot and mouth disease, herpangina or nonspecific febrile illness and 21% (39/183) suffered from complications of central nervous system involvement and/or cardiopulmonary failure. During the 6-month follow-up, 10 died and 13 had sequelae of dysfunction in swallowing, cranial nerve palsies, central hypoventilation or limb weakness/atrophy. Age younger than 3 years was the most significant factor associated with unfavorable outcomes in children (P=.004). Among 87 infected adults, 53% (46/87) were
asymptomatic, 39% (34/87) had nonspecific illnesses of fever, sore throat or gastrointestinal discomfort and only 8% (7/87) had hand, foot and mouth disease. Conclusions Enterovirus 71 household transmission rates are high for children, medium for parents and low for other adults. Serious complications, sequelae and death are associated with young children.
Key words: enterovirus 71; hand, foot and mouth disease; herpangina; household transmission; risk factors; outcomes
INTRODUCTION
Outbreaks of enterovirus 71 (EV71) have been documented since it was recognized in California in l969.1 Forty-four fatalities have been reported in Bulgaria (1975), 47 in Hungary (1978) and 30 in Malaysia (1997).2-4 The largest and most severe EV71 epidemic occurred in Taiwan in 1998.5-10 During the 1998 epidemic in Taiwan, out of over hundred thousands cases of hand, foot, and mouth disease or herpangina (HFMD/HA), 405 suffered severe neurologic complications such as encephalitis, meningitis, polio-like syndrome, encephalomyelitis and/or pulmonary edema. 9 Among the 405, 78 children died.9
In a seroepidemiological study before and after the 1998 outbreak, we found that pre-epidemic and post-epidemic EV71 seroprevalence rates in adults and children older than 6 years ranged from 57% to 67%.11 The post-epidemic EV71-seropositive rates among children below 3 years old ranged from 0% to 36%.11 An increased incidence of EV71 infection in young children occurred more often in geographic areas with increased mortality rates.11 For the 3 to 6-year-old children, the seropositive rates were between 26% and 51%. Interestingly, only 29% of preschool children infected with EV71 developed HFMD/HA. Combining the information of the clinical and seroepidemiological studies together, 1-6,8,9,11 we found that the clinical syndromes and severity of EV71 infection are very diverse, ranging from asymptomatic to fatal diseases.
In another Taiwanese seroepidemiological study, Lu CY et al. examined serial serum antibody titers to EV71 in blood samples from 81 children born in 1988.12 Samples were obtained yearly from 1989 to 1994 and from 1997 to 1999. EV71 seroconversion occurred with a yearly incidence of 3% to 11% between 1989 and 1997. By 1997, 68% of the 81 children at the age of 9 had serologic evidence of EV71 infection.12 A seroepidemiological study in Singapore also demonstrated that the EV71 seroprevalence rate in the general population was as high as 60% to 70%.13 It is evident that EV71 infection is not uncommon and that documented cases do not accurately reflect the actual number of infections.
Why the 1998 EV71 outbreak in Taiwan was so large is not clear.9,10 EV71 seropositivity was found to be concordant among siblings in our previous seroepidemiological study, suggesting that household transmission plays an important role on EV71 spread.11 The secondary household transmission rates of enteroviruses vary, including those for poliovirus, enterovirus 70 and coxsackievirus A24.14-16 The two adult fatalities that have been reported in Bulgaria and Singapore indicate that adults can also suffer serious complications from EV71 infections.2,17 However, the impact and outcomes of EV71 infections in adults and disease transmission among household family members need further investigation.
Since vaccination programs have almost eliminated poliovirus infection, EV71 infections may become one of the most important enteroviral diseases associated with significant sequelae and mortalities among young children. To date, EV71 transmission and outcomes within households of EV71 infection have not been studied. Data on household transmission of EV71 are necessary to help control, manage and prevent future EV71 infections. Therefore, the objective of this study is to investigate EV71 transmission and clinical outcomes within households of EV71-infected patients.
METHODS
Patient Selection and Family Surveillance
At Chang Gung Children’s Hospital in Taiwan, we studied patients who were suspected of having EV71 illnesses, such as HFMD or herpangina, and their household family members from February 2001 to August 2002. Institutional Review Board approval was obtained for this study and informed consents were obtained from all subjects or their parents.
Study flowchart is shown in Figure. If patients at the emergent service, outpatient clinic or inpatient ward had clinical syndromes suggestive of EV71 infection, they and their household family members were asked to participate in the study. Throat and rectal swabs for virus isolation, and the first blood sample for EV71 IgM, tested by µ-capture enzyme-linked immunoassay (ELISA),18 and neutralizing antibodies were obtained from the suspected cases of EV71 treated at Chang Gung Children’s Hospital. Clinical manifestations, courses and outcomes were recorded. If at any point the patients suspected of infection displayed clinical symptoms, the other family members in the same household were asked to undergo screening by virus isolation of throat swabs, and received the first blood sample for EV71 IgM and neutralizing antibodies. Questionnaire-based interviews were used to collect information including demographic data, the number of bedrooms in the households, contact time, pattern and presence of current/recent signs and symptoms (ulcers, sore throat, rash, fever, abdominal pain and diarrhea) and preceding contact history with extra-household people who had clinical syndromes suggestive of EV71 infection. Follow-up telephone interviews repeated questions about signs and symptoms at 2, 4 and 8-week intervals. If any household family member reported experiencing signs or symptoms suggesting of EV71 infection during the follow-up period, clinical assessment and repeated laboratory investigation for EV71 were performed.
If the suspected case or any household family member tested positive for EV71 isolation, a second blood sample was obtained from the suspected cases and all their household family members 4 weeks after the first blood sample obtained. Household EV71 transmission rates and clinical outcomes were analyzed only for families with at
least a member for positive EV71 isolation.
Definitions of EV71 Infection, Clinical Syndromes, Outcomes and Identified
Source of Infection
Laboratory evidence of EV71 infection was defined as the isolation of EV71, the presence of EV71 IgM or a four-fold change in EV71 neutralizing antibody serotiters between acute and convalescent sera. EV71 seropositivity was defined as a serotiter ≥ 8.
In uncomplicated cases, evidence of HFMD infections included oral ulcers on the tongue and buccal mucosa and a vesicular rash on the hands, feet, knees or buttocks. Evidence of herpangina included oral ulcerations on anterior tonsillar pillars, soft palate, buccal mucosa or uvula. Nonspecific febrile illness was defined as rectal temperature greater than 38oC without other symptoms. Enteritis was defined as diarrhea with or without abdominal pain. Upper respiratory tract infection was defined as sore throat, coryza or cough without herpangina or rash.
In complicated cases, aseptic meningitis was defined as a clinically compatible illness with cerebrospinal fluid (CSF) pleocytosis (>5 leukocytes/mm3 in patients older than one month or >25 leukocytes/mm3 in neonates) and negative bacterial cultures. Encephalitis was characterized by an altered level of consciousness accompanied by CSF pleocytosis. Evidence of a poliomyelitis-like syndrome included acute limb weakness with diminished reflexes and muscular strength. A diagnosis of encephalomyelitis was made when there was evidence of encephalitis and poliomyelitis-like syndrome. Cardiopulmonary failure was defined as pulmonary edema/hemorrhage with left ventricle failure requiring inotropic support. Unfavorable outcome was defined as death or sequelae, and favorable outcome was defined as complete recovery after 6 months of follow-up.
The index cases were the first members of the household to have clinically apparent illness confirmed by laboratory EV71 diagnosis. The secondary cases were defined as other family members whose EV71 symptoms occurred later than the index cases’ illness. Identified source of EV71 infection to the household was defined as “the first case in the household who displayed clinical apparent disease and who had had clear contact history with extra-household people who had illnesses suggestive of EV71 infection, such as HFMD or herpangina”. The infection transmission interval was defined as the time between the onset of disease for the first case in the household and the onset of disease in secondary case. Crowded household was defined as the ratio of the number of household members to the number of bedrooms over 1.5.
Laboratory Methods
Virus Isolation and Serotyping
Throat swabs, rectal swabs or stool samples were submitted for virus isolation. Samples were inoculated into human embryonic fibroblast, LLC-MK2, HEp-2 and rhabdomyosarcoma (RD) cell cultures. When enteroviral cytopathic effect involved more than 50% of the cell monolayer, cells were scraped and subjected to indirect fluorescent antibody staining with panenteroviral antibodies (Chemicon International Inc., Temecula, CA). Isolates were identified as EV71 by immunofluorescence with EV71 monoclonal antibodies (Chemicon International Inc., Temecula, CA).
EV71 Neutralizing Antibodies
Laboratory methods for measuring EV71 neutralizing antibody followed standard protocol of the neutralization test on microtiter plates.19,20 Serum and 50ul of EV71, containing one hundred 50% tissue culture infective doses (TCID50) of EV71 strain TW/2272/98 (GenBank accession number AF119795), were mixed and incubated onto the microtiter plates with RD cells at 35℃ in a 5% CO2 incubator. Each tested sample was run simultaneously with cell control, serum control and virus back titration. Cytopathic effect (CPE) was observed under an inverted microscope after an incubation period of 2 to 7 days, and the neutralizing antibody titer was determined at the time when CPE was observed in one TCID50 of the virus back titration. The neutralizing antibody titer was defined as the highest dilution of serum that would prevent the occurrence of CPE. Seropositivity was defined as a neutralizing antibody titer ≥8.
EV71 IgM Detection
EV71 isolate TW/2086/98 was amplified and purified as an antigen for µ-capture ELISA. In comparison with standard method of conventional virus culture, sensitivity and specificity for µ-capture ELISA were 91.5% and 93.1%, respectively.18
Statistical Analysis
Data were analyzed with the SAS Statistical Package (Version 8.2, SAS Institute, Cary, North Carolina). We used Student’s t test for continuous variables and χ 2 test for categorical data. After univariate analysis screened statistically significant variables, forward stepwise multiple logistic regression analysis was performed to adjust confounders simultaneously and to calculate multivariate-adjusted odds ratios for risk factors of EV71 infection and an unfavorable outcome in children. Corrected risk ratio was measured by using the formula of Zhang J and Yu KF to correct the adjusted odds ratios obtained from logistic regression if the incidence of an outcome was over 10%
in the study subjects.21 The α level of model selection was set at 0.15 for in-and-out models. P<.05 was considered statistically significant.
Results
Demography, Source of Infection, and Transmission Rates
One hundred and seventy-three suspected cases of EV71 and their household member (343 children and 441 adults) were surveyed from February 2001 to August 2002. The flowchart describing the selection of 94 families with positive EV71
isolation and the source of EV71 infection are shown in Figure. The source of infection to the 94 families was only identified in 47% (44/94): 19% from relatives, 13% from schoolmates, 11% from neighbors and 4% from friends. Because of the difficulties in identifying the source of EV71 infection to the families, we failed to find the source of infection to 53% (50/94) of the families (Figure).
The EV71 infection transmission interval ranged from 1 to 15 days. Median transmission interval was 3 days and mean (SD) interval was 3.7 (2.6) days.
Table 1 shows demographic data and the rates for isolating EV71, detecting EV71 IgM and demonstrating seropositive neutralizing antibodies among index cases and household contacts. The enterovirus 71 transmission rate of household contacts was 52% (176/339): 84% (70/83) siblings, 83% (19/23) cousins, 41% (72/175) parents, 28% (10/36) grandparents and 26% (5/19) uncles/aunts. The transmission rate was 84% (89/106) among household children, and 37% (87/233) among household adults (P<.001). The 39% (41/106) EV71 isolation rate from children household contacts was also significantly higher than the 4.3% (10/233) EV71 isolation rate from adult
household contacts (P<.001).
EV71 infection rates declined as age increased (Table 2). Furthermore, 100% (71/71) of children younger than 2 years were infected with EV71. Among children, no significant difference in the infection rate existed between siblings and cousins. Among adults, parents had a higher infection rate (41%, 72/175) than other adults (26%, 15/58) (P =.05). Infection rate for mothers (43%, 40/92) was similar to that for fathers (39%, 32/83) (P =.61). EV71 seropositive rates for all family members were as high as 93% (401/429).
Factors Associated with EV71 Infection in Children
Table 3 shows factors associated with EV71 infection in children. Male sex and age less than 6 years of age were associated with increased risk of EV71 infection. Children attending kindergarten or school had a lower incidence of EV71 infection. More household members, more children in the household and having a more crowded household did not significantly increase the risk of infection. Forward stepwise
associated with infection in children were age less than 6 years (adjusted OR=9.11, 95% confidence interval=2.90-28.65, P<.001; corrected risk ratio=2.37, 95% CI=1.74-2.68) and male gender (adjusted OR=4.11, 95% confidence
interval=1.19-14.15, P=.03; corrected risk ratio=1.13, 95% CI=1.02-1.19).
Clinical Syndromes and Outcomes in Children
Clinical syndromes and outcomes for infected children and adults are shown in Table 4. Children had significantly higher rates than adults for complications (21% vs. 0%, P<.001), long-term sequelae and fatalities (13% vs. 0%, P=.001).
Ten children (5%, 10/183) died: 6 patients died within 24 hours of hospitalization due to brainstem encephalitis plus fulminant cardiopulmonary failure, 3 patients died within 2 to 7 weeks of hospitalization due to brainstem encephalitis plus deep coma, and 1 with sequelae of dysphagia plus central hypoventilation died at home due to ventilator dysfunction 4 months after onset of illness.
At 6 months of follow-up, thirteen (7%, 13/183) children suffered from long-term sequelae that involved the CNS. Magnetic resonance imaging findings revealed
abnormal signal intensity in the brainstem and/or the spinal cord on T2-weighted images. Five patients had limb weakness/atrophy, 5 patients had swallowing dysfunction plus central hypoventilation plus limb weakness/atrophy, 1 patient had swallowing dysfunction plus central hypoventilation, 1 patient had limb
weakness/atrophy plus abducens palsy, and 1 patient had abducens palsy alone. Unfavorable outcomes including sequelae or deaths occurred in 23 (13%, 23/183) children. Table 5 shows factors associated with unfavorable outcomes in infected children based on univariate analyses. Age less than 3 years was the most significant factor. The clinical outcome of the secondary cases was not significantly different from that of the index cases (P=.09). Contact history with HFMD/HA, more household members, more children in the household and crowded household were not associated with a significantly higher unfavorable outcome rate. Children in kindergarten and school had lower unfavorable outcome rates. Forward stepwise multiple logistic regression analysis indicated that the most significant factor associated with an
unfavorable outcome in infected children was age less than 3 years (adjusted OR=6.19, 95% confidence interval=1.77-21.6, P=.004; corrected risk ratio=5.18, corrected 95% CI=1.72-12.2). However, in the less-than-3-year-old age group, we did not find any fatal cases in young infants less than 3 months of age.
Clinical Syndromes and Outcomes in Adults
Of 87 EV71-infected adults, 53% (46/87) were asymptomatic. All symptomatic adults recovered completely from uncomplicated illnesses, which included HFMD, herpangina, fever, upper respiratory tract infection and viral exanthema.
COMMENT
In this prospective family cohort study, we found that EV71 infections in young children to be associated with serious diseases; we also found a high household
transmission rate for children and a high ratio of asymptomatic adults. Long periods of viral shedding may account for widespread transmission of enteroviral diseases, which is certainly the case for polio and coxsackievirus infections.14 In a previous study, we found EV71 to be present in the stool of infected patients for up to 5 weeks.22 Previous research has demonstrated a higher rate of EV71 isolation from throat swabs than from rectal swabs or stool: 90% vs. 32%, respectively.23 We speculate that respiratory transmission by large droplet from the oral cavity may explain the high secondary infection rate within households in Taiwan, despite hand washing precautions in practice since 1998.24 Therefore, isolation of infected patients within single rooms and masks for the patients and the close contacts may be recommended for the prevention of respiratory droplet transmission of EV71.
New York Virus Watch data indicate that secondary coxsackievirus infections are more frequent in mothers (78%) than fathers (47%).15 However, the EV71 infection rates in the mothers and fathers in this study were similar: 43% and 39%, respectively (Table 1). EV71 infection rates for parents (41%, 72/175) were higher than for other adults (26%, 15/58), suggesting that close or longer contact facilitated EV71
transmission.
EV71 seropositive rates for all family members were as high as 93% (Table 1), which were significantly higher than those (57% to 67%) for the general population in a previous seroepidemiological study,11 therefore, it is likely that almost all the
susceptible family members were infected once EV71 had been introduced. Table 3 shows that EV71 infection rate increases as age decreases, so the most susceptible households have the highest EV71 infection rates. The high infectivity of EV71 is similar to that of poliovirus.14
Among children, household transmission produced a higher rate of clinical symptoms (94%) compared to extra-household transmission (29%) in our previous EV71 seroepidemiological study.11 Viral load or host genetic factors may account for this difference. Because the rate of asymptomatic infection with EV71 after social contact is high (about 71%),11 it was difficult to identify the source of primary
infections to the family. We were successful in determining the sources in only 47% of the cases.
EV71 infections in adults were less serious than those in children. Although EV71 infection is a differential consideration in cases of adult encephalitis, unexplained pulmonary edema or cardiopulmonary failure and although two deaths have occurred in adults,2,17 most infected adults in the present study were asymptomatic or suffered mild
upper respiratory tract infections. Why adults or older children have less severe
illnesses needs further study. One possible reason for the reduced severity might be that most adults and older children have antibody to this virus or a related virus, whereas younger children may incur primary infections. Another possible reason is that inadequate hygiene of younger children may increase a higher viral load and subsequently more severe diseases. EV71 transmission by infected adults who are asymptomatic or mildly symptomatic is a likely source of many infections. In some families whose source of infection could not be identified, we speculate that EV71 infections might be introduced into the family by an asymptomatic adult.
In conclusion, EV71 household transmission rates are high for children, medium for parents and low for other household adults. EV71 infections in children, especially those younger than 3 years old, are associated with serious complications, long-term sequelae and death. Adult EV71 infection can be characterized as having a high ratio of asymptomatic adults or nonspecific mild illnesses.
Author Contributions:
Study concept and design: Chang, Lin.
Acquisition of data: Chang, Tsao, Hsia, Shih, CG Huang, Hsu, Fang, YC Huang. Analysis and interpretation of data: Chang, Tsao, Hsia, Chan, Hsu, Lin
Drafting of the manuscript: Chang, Lin.
Critical revision of the manuscript for important intellectualcontent: Chang, Tsao, Hsia, Shih, CG Huang, Chan, Hsu, Fang, YC Huang, Lin.
Statistical expertise: Chang, Hsu. Obtained funding: Chang, Lin.
Administrative, technical, or material support: Tsao, Shih, Huang, Lin. Study supervision: Lin.
Funding/Support: This study was supported by grants from the Chang Gung
Memorial Hospital (CMRP1089) and National Science Council (NSC 90-2314-B-002-463 and NSC 91-3112-B-002-029).
Acknowledgement: We thank Mr. James Steed for his critical review on this
REFERENCES
1. Schmidt NJ, Lennette EH, Ho HH. An apparently new enterovirus isolated from patients with disease of the central nervous system. J Infect Dis. 1974;129:304-309. 2. Shindarov LM, Chumakov MP, Voroshilova MK, et al. Epidemiological, clinical and
pathomorphological characteristics of epidemic poliomyelitis-like disease caused by enterovirus 71. J Hyg Epidemiol Microbiol Immunol. 1979;23:284-295.
3. Nagy G, Takatsy S, Kukan E, Mihaly I, Domok I. Virological diagnosis of
enterovirus type 71 infections: experiences gained during an epidemic of acute CNS diseases in Hungary in 1978. Arch Virol. 1982;71:217-227.
4. Chan LG, Parashar UD, Lye MS, et al. Deaths of children during an outbreak of hand, foot, and mouth disease in Sarawak, Malaysia: Clinical and pathological
characteristics of the disease. Clin Infect Dis. 2000;31:678-683.
5. Chang LY, Huang YC, Lin TY. Fulminant neurogenic pulmonary oedema with hand, foot and mouth disease. Lancet. 1998;352:367-368.
6. CDC. Deaths among children during an outbreak of hand, foot and mouth
disease—Taiwan, Republic of China, April-July 1998. MMWR Morb Mortal Wkly Rep. 1998;47:629-632.
7. Wu TN, Tsai SF, Li SF, et al. Sentinel surveillance of enterovirus 71, Taiwan, 1998. Emerg Infect Dis. 1999;5:458-460.
8. Chang LY, Lin TY, Hsu KH, et al. Clinical features and risk factors of pulmonary oedema after enterovirus 71-related hand, foot, and mouth disease. Lancet. 1999;354:1682-1686.
9. Ho M, Chen ER, Hsu KH, et al. An epidemic of enterovirus 71 infection in Taiwan. N Engl J Med. 1999;341:929-935.
10. Dolin R. Enterovirus 71—emerging infections and emerging questions. N Engl J Med. 1999;341:984-985.
11. Chang LY, King CC, Hsu KH, et al. Risk factors of enterovirus 71 infection and associated hand-foot-mouth-disease/herpangina in children during an epidemic in Taiwan. Pediatrics. 2002;109:e88.
12. Lu CY, Lee CY, Kao CL, et al. Incidence and case-fatality rates resulting from the 1998 enterovirus 71 outbreak in Taiwan. J Med Virol. 2002;67:217-223.
13. Ooi EE, Phoon MC, Ishak B, Chan SH. Seroepidemiology of human enterovirus 71, Singapore. Emerg Infec Dis. 2002;8:995-997.
14. Gelfand HM, LeBlanc DR, Fox JP, Conwell DP. Studies on the development of natural immunity to poliomyelitis in Louisiana. II. Description and analysis of episodes of infection observed in study group households. Am J Hyg.
1957;65:367-385.
continuing surveillance of viral infections in metropolitan New York families. VII. Observations on viral excretion, seroimmunity, intrafamilial spread and illness association in coxsackie and echovirus infections. Am J Epidemiol. 1969;89:51-61. 16. Morens DM, Pallansch MA, Moore M. Polioviruses and other enteroviruses. In:
Belshe RB, ed. Textbook of Human Virology, 2nd ed. St. Louis, MO: Mosby Yearbook; 1991:427-497.
17. Chan KP, Goh KT, Chong CY, Teo ES, Lau G, Ling AE. Epidemic hand, foot and mouth disease caused by human enterovirus 71, Singapore. Emerg Infec Dis. 2003;9:78-85.
18. Tsao KC, Chan EC, Chang LY, et al. Responses of IgM for enterovirus 71 infection. J Med Virol. 2002;68:574-580.
19. Grandien M, Fosgren M, Ehrnst A. Enterovirus. In: Lennette EH, Lennette DA, Lennette ET, eds. Diagnostic Procedures for Viral, Rickettsial and Chlamydial Infections. 7th ed. Washington, DC: American Public Health Association; 1995:279-298.
20. Schnurr D. Enterovirus. In: Lennette EH, ed. Laboratory Diagnosis of Viral Infections. 2nd ed. New York, NY: Marcel Dekker Inc; 1992:351-364.
21. Zhang J, Yu KF. What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA. 1998;280:1690-1691.
22. Chung PW, Huang YC, Chang LY, Lin TY, Ning HC. Duration of enterovirus shedding in stool. J Microl Immunol Infect. 2001;34:167-170.
23. Chang LY, Lin TY, Huang YC, et al. Comparison of enterovirus 71 and
coxsackievirus A16 clinical illnesses during the Taiwan enterovirus epidemic, 1998. Ped Infect Dis J. 1999;18:1092-1096.
24. Lin TY, Twu SJ, Ho MS, Chang LY, Lee CY. Enterovirus 71 outbreaks, Taiwan: occurrence and recognition. Emerg Infect Dis. 2003;9:291-293.
Table 1. Demographic Data and Rates for Isolating EV71, Detecting EV71 IgM, Demonstrating Seropositivity for Neutralizing Antibodies and
Infection Among the Index Cases and Household Contacts Subjects Number Age, mean (SD), y Sex
(Male/ Female) Positive EV71 Isolation Rate Positive EV71 IgM Rate EV71 Seropositivity Rate† Infection Rate‡ Total subjects* 433 20.9 (18.4) 223/210 28% (119/433) 47% (201/425) 93% (401/429) 62% (270/433) Index case 94 3.1 (2.1) 56/38 72% (68/94) 94% (85/90) 98% (90/92) 100% (94/94) Household contacts 339 25.8 (17.8) 167/172 15% (51/339) 35% (116/335) 92% (311/337) 52% (176/339) Children household contacts 106 4.5 (4.6) 60/46 39% (41/106) 76% (79/104) 95% (99/104) 84% (89/106) Siblings 83 4.4 (3.8) 46/37 40% (33/83) 78% (63/81) 96% (78/81) 84% (70/83) Cousins 23 5.0 (6.8) 14/9 35% (8/23) 70% (16/23) 91% (21/23) 83% (19/23) Adults household contacts 233 35.7 (12.0) 107/126 4.3% (10/233) 16% (37/231) 91% (212/233) 37% (87/233) Parents 175 31.5 (5.4) 83/92 5% (9/175) 17% (29/175) 91% (159/175) 41% (72/175) Grandparents 36 59.3 (10.4) 14/22 0% (0/36) 15% (5/34) 94% (34/36) 28% (10/36) Uncles/aunts 19 27.4 (8.7) 10/9 5% (1/19) 16% (3/19) 84% (16/19) 26% (5/19) Babysitters 3 36.6 (7.7) 0/3 0% (0/3) 0% (0/3) 100% (3/3) 0% (0/3) Abbreviation: EV71, enterovirus 71; SD, standard deviation.
*Total subjects included index cases and household contacts.
† EV71 seropositivity was defined as an EV71 neutralizing antibody titer ≥8 .
Table 2. EV71 Infection Rates in Different Age Groups
Age Group, y EV71 Infection Rates Adjusted Odds Ratio* (95% CI)
Corrected Risk Ratio† (95% CI) P Value* <6 96% (159/165) 1.0 1.0 - 7-18 72% (26/36) 0.10 (0.03-0.3) 0.74 (0.46-0.91) <.001 19-40 39% (71/181) 0.025 (0.01-0.06) 0.39 (0.20-0.61) <.001 >40 27% (14/51) 0.014 (0.005-0.04) 0.26 (0.11-0.51) <.001 Abbreviation: EV71, enterovirus 71; CI, confidence interval.
*Adjusted odds ratio and P value were calculated by using the age≤6 group as the reference group and adjusted by sex. †Corrected risk ratio was measured by using the formula of Zhang J and Yu KF to correct the adjusted odds ratio obtained from logistic regression.21
Table 3. Factors Associated With EV71 Infection in Children
Factors Infected (n=183) Not Infected (n=17) P Value Male/female ratio 1.57 (112/71) 0.31 (4/13) <.01 Age, mean (SD), y 3.3 (2.4) 10.0 (7.6) <.01 Age<6 years 86% (158/183) 35% (6/17) <.01 No. of household members>6 52% (95/183) 53% (9/17) .94 No. of children>3* 45% (82/183) 59% (10/17) .27Crowded household† 64% (118/183) 53% (9/17) .34 Kindergarten or school attendance 34% (62/183) 71% (12/17) <.01 Abbreviation: EV71, enterovirus 71; SD, standard deviation.
*No. of children was the number of children in the same household.
†Crowded household was defined as the ratio of the number of household members to the number of bedrooms over 1.5.
Table 4. Clinical Syndromes and Outcomes of EV71-infected Children and Adults Children (n=183) Adults (n=87) P Value Clinical Syndromes Asymptomatic 11 (6%) 46 (53%) - Symptomatic 172 (94%) 41 (47%) <.001* Uncomplicated symptomatic 133 (73%) 41 (47%) - HFMD 90 (49%) 7 (8%) - Herpangina 19 (10%) 8 (9%) - Nonspecific febrile illness 4 (2%) 1 (1%) - Upper respiratory tract infection 16 (9%) 18 (21%) - Enteritis 2 (1%) 2 (2%) - Viral exanthema 2 (1%) 5 (6%) -
Complicated symptomatic† 39 (21%) 0 <.001† HFMD plus meningitis 9 (5%) 0 - HFMD plus encephalitis 11 (6%) 0 - HFMD plus polio-like syndrome 5 (3%) 0 - HFMD plus encephalomyelitis and
cardiopulmonary failure 14 (8%) 0 -
Outcomes
Unfavorable outcomes (sequelae or deaths) 23 (13%)‡ 0 .001 Abbreviation: EV71, enterovirus 71; HFMD, hand, foot, and mouth disease.
* P Value was measured with Pearson χ2test to compare the rates of symptomatic cases between infected children and infected adults.
† P Value was measured with Pearson χ2 test to compare the rates of complications between infected children and infected adults.
Table 5. Factors Associated With Unfavorable Outcomes in EV71-infected
Children
Factors Children With Unfavorable Outcomes* (n=23) Children With Favorable Outcomes (n=160) P Value Age<3 years 87% (20/23) 52% (83/160) <.01 Males 65% (15/23) 61% (97/160) .67 Secondary case in family 26% (6/23) 46% (68/149) † .09 Contact history with HFMD/HA 52% (12/23) 71% (110/160) .11 No. of household members>6 48% (11/23) 53% (84/160) .68 No. of children>3‡ 43% (10/23) 45% (72/160) .89 Crowded household§ 65% (15/23) 64% (103/160) .94
Kindergarten or school attendance 9% (2/23) 38% (60/160) .01 Abbreviation: EV71, enterovirus 71; HFMD/HA, hand, foot, and mouth disease or herpangina.
*Unfavorable outcomes were defined as death or having log-term sequelae, and favorable outcomes as complete recovery.
† Because 11 out of 160 infected children with favorable outcomes were asymptomatic, these 11 cases could not be defined as primary or secondary.
‡No. of children was the number of children in the same household.
§Crowded household was defined as the ratio of the number of household members to the number of bedrooms over 1.5.
Figure. Flowchart of Family Surveillance Study and Identified Sources of EV71 Infection to the Family
Virus isolation
1st blood sample for EV71 antibodies Questionnaire-based investigation Telephone interview +/– clinical assessment
94/173 (54%) families (200 children and 233 adults) (+) for EV71 isolation
50/173 (29%) families (88 children and 136 adults) (–) for EV71 isolation
29/173 (17%) families (55 children and 72 adults) (+) for non-71 enterovirus
Excluded from study 2nd blood sample for EV71 antibodies
Clinical outcome assessment Data analysis
The first EV71-infected cases in 44/94 (47%) families had identified source of infection
Source of infection was not identified in 50/94 (53%) families Identified source of infection Relatives 19% (18/94) Schoolmates 13% (12/94) Neighbors 11% (10/94) Friends 4% (4/94)
Outcome of Enterovirus 71 Infections with or without Stage-based Management, 1998 -
2002
Luan-Yin Chang, MD, PhD; Shao-Hsuan Hsia, MD; Chang-Teng Wu, MD; Yhu-Chering Huang, MD, PhD; Kuang-Lin Lin, MD; Tsui-Yen Fang, BS; Tzou-Yien Lin, MD
Division of Pediatric Infectious Diseases (LYC, YCH, TYF, TYL), Division of Pediatric Critical Care and Emergency Medicine (SHH, CTW), Divison of Pediatric Neurology (KLL), Department of Pediatrics, Chang Gung Children’s Hospital, Chang Gung University, Taoyuan, Taiwan
*Dr. Chang’s current affiliation is Department of Pediatrics, National Taiwan University Hospital, College of Medicine, National Taiwan University.
Running Title: Outcome of EV71 Infection
Correspondence and Reprint Requests to: Dr. Tzou-Yien Lin
Division of Pediatric Infectious Diseases, Department of Pediatrics, Chang Gung Children’s Hospital, Chang Gung University,
5, Fu-Hsing Street, Kweishan, Taoyuan, Taiwan Tel: 886-3-3281200 ext 8002; Fax: 886-3-3288957; E-mail: [email protected]
Abstract
Background: Enterovirus 71 (EV71) infection may progress through four stages, one
of which is cardiopulmonary failure. In Taiwan in 1998, almost all the EV71 patients with cardiopulmonary failure died. To improve clinical outcome of EV71 patients, we developed a stage-based management program in 2000.
Methods: The medical records of 196 EV71 patients who did not have stage-based
management (1998-1999) and of 331 EV71 patients who did (2000-2002) at Chang Gung Children’s Hospital were reviewed for demographic characteristics, clinical syndromes, case-fatality rates and sequelae. We compared and analyzed the results for the two groups.
Results: Of the patients who did not receive stage-based management, 83% (15/18) of
cases with both central nervous system (CNS) involvement and cardiopulmonary failure died during the acute stage of the infection. Two patients died at convalescence and one had sequelae of dysphagia and limb weakness. By contrast, of the patients who received stage-based management, 33% (12/36) of cases with CNS and
cardiopulmonary failure died during the acute stage, 8% (3/36) died at convalescence, 14% (5/36) recovered completely and 43% (16/36) had severe sequelae of central hypoventilation, dysphagia, and limb weakness (p<0.001). For cases with CNS and cardiopulmonary failure, multivariate analysis showed that age older than 2 years and cerebrospinal fluid white cell count over 100/uL were associated with a increase in acute mortality (95% CI 1.9 to 105.3, p=0.001; 95% CI 1.1 to 66.6, p=0.04,
respectively) but stage-based management was significantly associated with a reduction in acute mortality (95% CI 0.007 to 0.24; p=0.0004). Stage-based management did not affect the outcome of cases with CNS involvement alone.
Conclusions: Stage-based management reduced the case-fatality rate of EV71-related
cardiopulmonary failure, but two-thirds of the survivors had severe sequelae.
Introduction
There were large outbreaks of enterovirus 71 (EV71) infection resulting in dozens of deaths in Bulgaria in 1975,1 Hungary in 1978,2 and Malaysia in 1997,3 and in the largest and most severe EV71 epidemic, to date, in Taiwan in 1998.4 During the 1998 Taiwan EV71 epidemic, almost all the patients with cardiopulmonary failure died.4,5 This outcome may have been the result of lack of previous experience in managing such patients or delayed parental or medical recognition of how critical the patients were at that time.
According to our clinical studies, enterovirus 71 (EV71) infection can progress through four stages: hand, foot, and mouth disease (HFMD)/herpangina (Stage 1), CNS involvement (Stage 2), cardiopulmonary failure (Stage 3), and convalescence (Stage 4). In 1998 in Taiwan almost all the patients with cardiopulmonary failure died.5 In 2000, to improve the survival, we developed a disease management program that varied according to the different stages of EV71 infection.6,7 This study was conducted to compare case-fatality rates and sequelae of EV71 infection before and after stage-based management was developed.
Patients and Methods
Definition of clinical syndromes and stages
From 1998 to 2002, we identified all the EV71 patients at Chang Gung Children’s Hospital. These patients were clinically diagnosed as having the disease if their viral cultures showed EV71 or positive EV71 IgM or if a four-fold rise in EV71 neutralizing antibody serotiters was found between the acute and convalescent sera. We reviewed all their charts to find out what their current states of health were. Complicated cases with sequelae were followed up either as inpatients or outpatients and some complicated cases with complete recovery were followed up as outpatients.
We defined the clinical diseases as follows: Stage 1, HFMD, were found to have oral ulcers and vesicular rash appearing on the hands, feet, knees, and/or the buttocks, or herpangina including oral ulceration over anterior tonsillar pillars, the soft palate, buccal mucosa or uvula; Stage 2, CNS involvement: aseptic meningitis with headache, irritability or myoclonic jerk and CSF pleocytosis (>5x106 leukocytes/L) but without altered level of consciousness and focal signs, or encephalitis with altered level of consciousness plus CSF pleocytosis, or poliomyelitis-like syndrome with acute limb weakness and decreased reflex and muscle strength, or encephalomyelitis with the occurrence of both encephalitis and poliomyelitis-like syndrome. Stage 3, cardiopulmonary failure, was defined as pulmonary edema or hemorrhage with decreased ejection fraction of left ventricle as assessed by echocardiography necessitating inotropic agent support. Pulmonary edema was defined as alveolar
congestion on a chest radiography and pink frothy fluid from the endotracheal tube; pulmonary hemorrhage as evidenced by alveolar congestion on a chest radiography or fresh blood from the endotracheal tube; Stage 4, convalescence, was defined as recovery from cardiopulmonary failure.
Stage-based Therapeutic Strategy
Between 1998 and 1999, cases of EV71 were managed with various symptom-control treatments and with no special strategy. In 2000, with the approval of Taiwan’s Enterovirus Ad Hoc Committee and the Center for Disease Control in Taiwan, we developed a treatment program based on the four stages of EV71 infection. Since that time, all EV71 cases at Chang Gung Children’s Hospital have received this stage-based management.
The clinical stages and the disease management of these stages have been published previously.6,7 Patients with Stage 1 required treatment of symptoms only. Patients identified as having Stage 2 were hospitalized and their treatment included fluid restriction and administration of osmotic diuretics for those with signs of increased intracranial pressure (IICP) and furosemide for those suspected having fluid overload. Intravenous immunoglobulin (IVIG) was administered and blood pressure, oximeter, coma scale and blood sugar were closely monitored. Patients were managed in the ICU if they were found to have tachypnea/apnea, hypertension/hypotension, signs of IICP, or hyperglycemia.
Patients identified as having Stage 3 were identified when they required ventilator support and inotropic agents. We subdivided these patients into Stage 3A as having hypertension and pulmonary edema and Stage 3B as having hypotension. Treatment of Stage 3B was as follows: their intensive care management included continuous fluid restriction, administration of milrinone to control severe hypertension and to increase cardiac output, early intubation with positive pressure mechanical ventilation with increased positive end expiratory pressure for pulmonary edema. High frequency oscillatory ventilator was considered if pulmonary edema or hemorrhage persisted or if they developed severe hypoxemia. When a patient’s blood pressure drops below the normal range for his or her age, the disease was considered to be in stage 3B. In some cases, blood pressure is very unstable, requiring fine adjustments of inotropic agents such as dopamine and epinephrine.
For Stage 4 patients, rehabilitation is provided for limb weakness/atrophy, dysphagia, diaphragm dysfunction, apnea or central hypoventilation.
Outcome assessment
onset of the disease, and a convalescent stage fatality if death occurred more than 8 weeks after onset of the disease. Sequelae included residual neurologic deficits, seizures, need for tracheostomy with or without ventilator support, need for nasogastric tube or other disabilities after 6 months of follow-up.
Laboratory methods for virus isolation, EV71 IgM, and neutralizing antibody
Throat swabs, rectal swabs, cerebrospinal fluid, vesicular fluid or autopsy tissue were submitted for virus isolation. Samples were inoculated into human embryonic
fibroblast (MRC-5), LLC-MK2, HEp-2, RD cell cultures. Once enteroviral cytopathic effect involved more than 50% of the cell monolayer, the cells were scraped. Indirect fluorescent antibody staining with panenteroviral antibody (Chemicon International, Inc., Temecula, CA) was performed to identify enterovirus. These isolates were subsequently identified as EV71 by immunofluorescence with EV71 monoclonal antibody (Chemicon International, Inc., Temecula, CA).
To test EV71 IgM, an EV71 isolate, TW/2086/98, was amplified and purified as an antigen for use in µ-capture enzyme-linked immunosorbent assay (ELISA), whose diagnostic sensitivity and specificity for acute EV71 infection have been reported to be 91.5% and 93.1% respectively when compared with conventional virus culture methods.8
The measurement of EV71 neutralizing antibody was done in microtiter plates following standard protocol.9,10 Seropositivity was defined as serotiter equal to or greater than 8.
Statistical Analysis
Data are expressed as mean ±standard deviation. Chi-square test was used for analysis of categorical data, and student t-test for continuous variables. A multiple logistic regression analysis was performed for the calculation of multivariate-adjusted odds ratios for risk factors. P values less than 0.05 were considered significant.
Results
Clinical Syndromes
There were a total of 527 EV71 cases. Of these 527 EV71 cases, 509 cases were diagnosed by positive EV71 isolation plus positive EV71 neutralization antibody; the remaining 18 cases were diagnosed by positive EV71 IgM and positive EV71
neutralization antibody.