Urban Forestry & Urban Greening 56 (2020) 126863
Available online 28 September 2020
1618-8667/© 2020 The Authors. Published by Elsevier GmbH. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Restorative effects of virtual natural settings on middle-aged and
elderly adults
Chia-Pin Yu
a,b, Hsiao-Yun Lee
c,*
, Wen-Hsin Lu
a, Yu-Chih Huang
d, Matthew H.E.M. Browning
e aSchool of Forestry and Resource Conservation, National Taiwan University, Taiwan, ROCbT.H. Chan School of Public Health, Harvard University, United States
cDepartment of Leisure Industry and Health Promotion, National Taipei University of Nursing and Health Sciences, Taiwan, ROC dDepartment of Tourism, Leisure and Hospitality Management, National Chi-Nan University, Taiwan, ROC
eVirtual Reality and Nature Lab, Department of Parks, Recreation and Tourism Management, Clemson University, United States
A R T I C L E I N F O Handling Editor: Matilda van den Bosch
Keywords: Attention restoration Mood states Natural environments Restorative environments Seniors A B S T R A C T
Previous studies have demonstrated health benefits result from exposure to natural environments. Virtual reality (VR) may offer an alternative to actual outdoor immersion by generating a simulated health-promoting envi-ronment. Given that health issues are more prevalent in older adults, this study investigated the restorative effects of virtual natural settings on middle-aged and elderly adults. A cross-over pretest-posttest design was used to measure changes in participants’ mood levels, physiological and psychological responses, and attentional measures of cognitive functioning (N = 34). Semi-structured interviews after the VR experiences were conducted to evaluate participants’ experiences. Physiological responses to VR did not differ between virtual natural and urban settings. In contrast, participants expressed more positive feelings and lower levels of fatigue and depression after viewing virtual nature settings than after viewing virtual urban settings. Virtual nature settings were also rated as more restorative than virtual urban settings. Further, participants described virtual natural settings as appeasing and relaxing, so much so that they were motivated to travel outdoors to experience the settings shown in VR. Our findings provide additional evidence that viewing simulated natural settings in VR can be beneficial for this population. Perhaps the most promising finding is that VR may motivate older adults to experience nature outdoors, thus promoting synergistic benefits first during virtual exposure and then during actual exposure.
1. Introduction
An increasing amount of evidence demonstrates exposure to natural settings yields health benefits (Chen et al., 2018; Hartig et al., 2014; Markevych et al., 2017; Yu et al., 2017). However, not everyone is able to freely visit natural settings. Simulated natural settings can also be expected to promote mental health primarily through the recovery of attentional resources and reductions in stress (Browning et al., 2020a; Valtchanov et al., 2010; Valtchanov and Ellard, 2010, 2015), as explained in Attention Restoration Theory (ART, Kaplan and Kaplan, 1989) and Stress Recovery Theory (SRT, Ulrich et al., 1991). ART ex-plains how natural environments capture involuntary attention and allow restoration of cognitive capacities (Berto, 2014; Kaplan and Kaplan, 1989). SRT suggests that non-threatening natural settings are
evolutionarily preferred. Therefore, they promote positive affect and decrease physiological arousal (Ulrich et al., 1991).
Advancements in the development of virtual reality (VR) have allowed indoor simulations of health-promoting outdoor scenes and experiences. VR can be described as virtual settings represented through real-time computations that provide one or more sensory stimulations and are interlinked with the user’s behavior. By combining input signals and feedback devices, VR enables humans to interact with virtual set-tings through a human–machine interface (Burdea and Coiffet, 2003; Guti´errez et al., 2008).
Relatively little research has been conducted on therapeutic appli-cations of VR for the psychological health of older adults, despite pro-moting their health being an important area of emphasis (World Health Organization, 2017). Extant research with seniors and VR has focused on * Corresponding author at: Department of Leisure Industry and Health Promotion, National Taipei University of Nursing and Health Sciences, No. 365, Ming-te Road, Peitou District, Taipei City, 11219, Taiwan, ROC.
E-mail address: hsiaoyun07@ntunhs.edu.tw (H.-Y. Lee).
Contents lists available at ScienceDirect
Urban Forestry & Urban Greening
journal homepage: www.elsevier.com/locate/ufughttps://doi.org/10.1016/j.ufug.2020.126863
cognitive training (García-Betances et al., 2014), therapeutic in-terventions for fall prevention (Mirelman et al., 2020), muscular strength and postural balance (Park and Yim, 2016), and rehabilitation (Stone et al., 2014). Yet seniors experience also high levels of psycho-logical distress and mental illness.
We are aware of only two studies that have examined VR’s potential to improve mental health in this population. One study in the United States with 63 assisted living community residents found no difference in mood levels, perceived well-being, or happiness between a two-week VR intervention with travel imagery and this same imagery shown on televisions (Lin et al., 2018). The second study was conducted with 66 Canadian seniors and showed them 6 min of nature-based 360-degree video content in an VR head-mounted display (HMD) (Appel et al., 2020). Pre-post surveys showed that the experience increased positive emotions and decreased negative emotions. Although these results are promising for the therapeutic potential of VR for seniors, both studies are limited by the lack of physiological measures of physical conditions, such as heart rate and blood pressure, and the lack of blinding partici-pants or researchers to experimental treatments to prevent social desirability bias (Joseph et al., 2020). Moreover, these studies did not compare the psychological impacts of differing types of content in VR, which could lead to the actual use of VR—rather than the content shown in VR—causing the reported changes. Therefore, systematic examina-tions of the content shown to participants is a crucial next step in the examination of VR as a therapeutic intervention for seniors (Gaboda et al., 2011; Leontjevas et al., 2013).
The current study aims to fill the gaps in our understanding of the impact of virtual natural settings on senior’s health. Specifically, we evaluate and compare the restorative psychophysiological effects of virtual natural settings (the experimental condition) and virtual urban settings (the control condition) on 34 middle-age and elderly in-dividuals. We employed a mobile, smartphone-based VR system (Sam-sung Gear VR) to provide the high visual quality, ease of use, and affordability that would facilitate the future distribution of VR as a therapeutic intervention and a tool for health promotion. A cross-over, pretest-posttest experimental design allowed us to compare changes in physiological and psychological responses as well as attention perfor-mance between settings before and after exposure. Because research on VR and seniors is still in its early stages, participant’s experiences were documented using semi-structured interviews to understand user per-spectives. Overall, this study provides a step toward exploring the po-tential of using immersive VR applications for health promotion in middle-age and elderly adults.
2. Materials and methods
2.1. Participants
Participants were recruited with a convenience sampling method in March 2019 from social networking platforms (e.g., Facebook, Line, web forums). People who were at least 45 years old and without neuropsy-chiatric disorders, cardiovascular diseases, cognition disorders, or spe-cific visual and hearing problems were eligible to participate. People with common visual problems such as myopia and presbyopia were also eligible to participate, because the VR HMD had a focal adjustment that allowed these people to accurately and safely see content in VR. All participants were instructed to avoid consumption of alcohol and caffeine for at least 12 h prior to the experiment. Each participant was required to complete two experimental sessions and was rewarded 7 USD upon finishing the study. The study ran from March 6th, 2019 to March 26th, 2019. It was approved by Institutional Review Board at National Taiwan University (NTU-REC No. 201906HM013).
2.2. Research design
We employed a cross-over pretest-posttest design over a two-week
period. Participants were randomly (single-blind) assigned to one of two groups (Group A and Group B). Group A was first exposed to the virtual natural setting and then exposed a week later to the virtual urban setting. Group B experienced stimuli in the opposite order. This cross- over design was used to control bias from individual differences, and the week of wash-out was used to avoid carry-over effects.
In accordance with the research designs of previous restorative environment studies (i.e. Bielinis et al., 2018; Ulrich et al., 1991; Yu et al., 2018), virtual natural and urban settings represented the experi-mental condition and the control condition, respectively. We expected that the two conditions would differ in terms of their restorative quality, such that the virtual natural setting was more restorative than the virtual urban setting.
2.3. VR device
We used a Samsung Gear VR head-mounted display (HMD) and a Samsung Galaxy S8 smartphone with iPhone earbuds to view the virtual settings (Fig. 1). The Samsung Gear VR HMD is a commercial product that is compatible with most Samsung smartphones produced since 2016. The HMD presents VR content with a 101◦field of view, 2960 × 1440 resolution, and 60 Hz refresh rate. The HMD is lightweight, cordless, and offers focus adjustment, such that participants with cor-rected vision canview VR content safely and accurately without their glasses. The HMD does not have a cord behind the user’s back con-necting the HMD to a computer; the smartphone provides all the computational power. The latest HMD version (2017) costs approxi-mately 80 USD and, therefore, could be used relatively affordably in many health promotion contexts if users have personal smartphones that are compatible.
2.4. The 360◦videos
Two settings, natural and urban, were captured with 360◦videos and accompanying soundtracks. The selection of the nature and urban sites followed best practices for restorative environmental simulations (Browning et al., 2020a; Yu et al., 2018). Specifically, both settings were within commuting distance for participants and, therefore, could be expected to be generally familiar to them. Also, the two settings were selected to include or exclude specific natural/built environment fea-tures. We used the GoPro Fusion to record the videos. This camera has front and rear fish-eye lenses that capture video feeds at 5.2 K/30 frames per second. Each lens captures 180◦horizontally and vertically, creating a seamless 360◦field of view after stitching together using the GoPro Fusion Studio software. Each video was 10 min in duration.
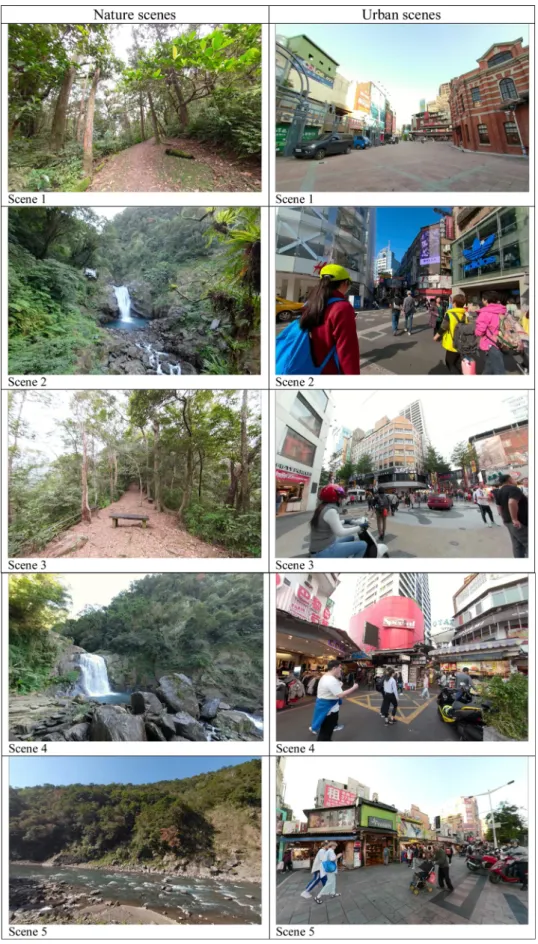
The nature videos were shot at the Neidong National Forest Recre-ation Area in New Taipei City, Taiwan. These videos and their accom-panying soundtracks primarily contained natural elements, including waterfalls, creeks, broad-leaved forests, ferns, and bird songs. Manmade structures, such as roads, fences, and tourists, were not present. The 10- minute video consisted of five scenes. Scene 1 featured a trail in dense forest. Scene 2 featured a small waterfall surrounded by a forest. Scene 3 featured a trail in tall trees with a bench. Scene 4 featured a big waterfall. Scene 5 featured an open forest land with river (see Fig. 2). The urban videos were shot at a Ximending shopping center in Taipei city. Manmade elements, including buildings, signs, crowds, and traffic noises, dominated. Urban street trees were present but accounted for a very small amount of content (<5% of the pixels). Again, the 10-minute video included five scenes. Scene 1 featured an old town setting. Scene 2 featured modern buildings with walking tourists. Scene 3 featured buildings and street trees. Scene 4 featured crowds and signs. Scene 5 featured traffic and noises (see Fig. 2).
2.5. Measures
2.5.1. Physiological indicators of stress
Heart rate (HR), systolic blood pressure (SBP), diastolic blood pres-sure (DBP), activity level of sympathetic nervous system (SNS), and activity level of parasympathetic nervous system (PSNS) were measured using the QHRV (Quantitative Heart Rate Variability, Medeia Ltd. Bulgaria, http://www.vitalscan.es/dtp_realtime.htm). This is a medical device approved by the U.S. Food and Drug Administration (FDA) for measuring heart rate variability (HRV). These physiological measures are commonly assessed in nature and human health studies (Gower and Crick, 2011; Ikei et al., 2017). A high frequency (HF: 0.15–0.40 Hz) calculated from HRV was the indicator of parasympathetic nervous system activity while a low frequency (LF: 0.04–0.15 Hz) and LF/HF ratio were indicators of sympathetic nervous system activity (Camm et al., 1996).
2.5.2. Mood states
The Profile of Mood States (POMS) measured affective valence (Karmanov and Hamel, 2008; Shacham, 1983; Sonntag-¨Ostr¨om et al., 2014). This survey battery includes six constructs: confusion, vigor, fa-tigue, anger, tension, and depression. Survey items were used in isola-tion as well as in a summative score to indicate total mood disturbance (TMD). TMD was calculated by subtracting the total score for positive emotion—vigor—from the total score for the five negative emotions- confusion, fatigue, anger, tension, and depression. A higher score in-dicates a higher level of mood disturbance.
2.5.3. Perceived restorativeness
The Restorative Components Scale (RCS) evaluated whether partic-ipants believed the simulated settings led to feelings of restoration (Herzog et al., 2003). We used an adapted version of the scale from Laumann et al. (2001), which contains four elements of restorative settings - being away, extent, fascination, and compatibility. RCS data were only collected after the VR experience.
2.5.4. Attention performance
The Sustained Attention to Response Test (SART) is a computer- administered task that measures sustained attention and/or inhibition attention capacity (Berto, 2005; Robertson et al., 1997; Manly and Robertson, 2005; Manly et al., 1999). Here, the SART evaluated par-ticipants’ attentional capacities before and after each VR experience. The test showed 225 digits from one to nine and participants view a random series of single digitals in a computer monitor. Participants were told the digit ‘3’ was the target and the other digits were non-targets. Digits were presented on the computer screen every 900 ms and
remained on the screen for 250 ms. Participants were instructed to press the keyboard any time they saw a non-target digit and to refrain from pressing the keyboard when the target digit appeared. Their attention performance was measured by counting the number of mistakes. A lower score reflects better attention performance.
2.5.5. Participants’ VR experiences
We also conducted semi-structured interviews to evaluate the user experience. Interviews consisted of three questions. The first asked participants whether they experienced physical symptoms, such as cybersickness, dizziness, lightheadedness, or headaches, while watching the videos. If participants indicated they experienced these symptoms, they were asked to describe their symptoms in greater detail. The second question asked participants to describe the perceptions they had while watching the videos. The third question asked participants to share any remaining aspects of the VR experience that was not already covered in the interview or questionnaires.
2.6. Procedures
The day before the experiment, each participant was reminded to abstain from drinking beverages containing alcohol or caffeine for 12 h prior to the experiment. Upon arrival at the research lab, participants were asked to drink a cup of water during a rest period. In the meantime, researchers explained the procedures of the experiment and the purpose of the study and asked participants to sign a consent form. Participants were informed of their right to drop out of the experiment at any time. After the researchers collected the consent forms, participants provided their demographic information and prior VR experience. The total study orientation time was 15 min. Next, the SART test was administered and took 6 min, beginning with a practice test that helped participants get accustomed to the computer task and followed by the formal task. After finishing the SART, participants were asked to complete the POMS questionnaire. Then we collected their physiological indicators (HR, SBP, DBP, and HRV) at baseline. Next, they were exposed to their assigned VR condition – either a natural setting or an urban setting - in any seated position they were comfortable. Afterward, participants’ physiological indicators were measured again and participants were asked to complete follow-up POMS, RCS, interview, and SART measures. Finally, participants were asked to schedule an appointment for one week after the first VR experience to watch the second set of videos. Thus, every participant experienced both conditions during study period. Fig. 3 illustrates the study procedure.
Fig. 1. (a) Samsung Gear VR head-mounted display (HMD); (b) User immersed in the virtual setting via a Samsung Galaxy S8 phone inserted into the front of the HMD.
2.7. Analysis
The data were compiled, coded, and crosschecked. Statistical methods involved descriptive statistics and paired-sample t-tests for examining changes in participants’ physiological and psychological re-sponses. Two-way repeated-measures ANOVAs were conducted to test whether setting (natural or urban) and time (first or second VR experi-ence) influenced physiological and psychological responses. The mini-mum level for statistical significance was 0.05, and the effect size was calculated with Cohen’s d, (1988). Sizes could be small (≤ 0.2), medium (0.3 to 0.7), or large (≥ 0.8). Open-ended responses were analyzed using content analysis with an inductive approach (Lune and Berg, 2017). Two independent researchers examined the data systematically to identify patterns and codes (Lune and Berg, 2017). Each response was coded separately and reviewed for agreement. Codes were sorted based on frequency of expression. All analyses were executed using PASW Sta-tistics 18.0.
3. Results
3.1. Profile of participants and description of study variables
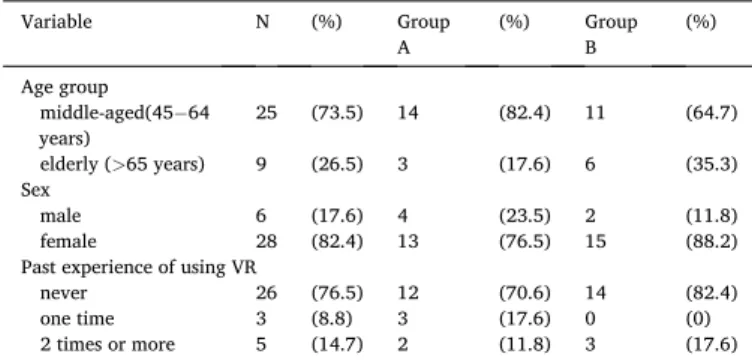
Table 1 displays the descriptive characteristics of the participants. In total, there were 34 participants who completed the experiment. The mean age was 58.76 years (SD = 8.36), with the majority being middle- aged (45-64 years old, 73.5 %) and female (82.4 %). Most of them (76.5 %) had not previously experienced VR.
Table 2 describes the results of the physiological measures, mood levels, attention performance tests, and perceived restorativeness scores. Three participants were excluded from these analyses due to incomplete data from the SART. Also, one participant failed to provide measures of systolic blood pressure and diastolic blood pressure due to device failure.
Fig. 3. Procedure of experiment.
Note: All participants take both VR natural and urban experiments in study period. Table 1 Description of participants. Variable N (%) Group A (%) Group B (%) Age group middle-aged(45− 64 years) 25 (73.5) 14 (82.4) 11 (64.7) elderly (>65 years) 9 (26.5) 3 (17.6) 6 (35.3) Sex male 6 (17.6) 4 (23.5) 2 (11.8) female 28 (82.4) 13 (76.5) 15 (88.2)
Past experience of using VR
never 26 (76.5) 12 (70.6) 14 (82.4)
one time 3 (8.8) 3 (17.6) 0 (0)
2 times or more 5 (14.7) 2 (11.8) 3 (17.6)
Note: each subject was tested in both conditions (nature and urban). Group A was exposed to the virtual nature condition first and then the urban condition; Group B received the opposite order of exposures.
Table 2
Description of all study variables.
Nature Urban Mean SD Mean SD HR (N = 34) Pretest 72.32 7.57 73.65 9.90 Posttest 70.74 7.26 71.21 9.56 SBP (N = 33 a) Pretest 115.70 10.54 118.79 13.16 Posttest 117.21 11.74 120.06 10.95 DBP (N = 33a) Pretest 71.79 5.36 71.94 5.66 Posttest 72.52 6.15 72.70 5.17 LF (N = 34) Pretest 90.15 43.11 104.03 70.82 Posttest 97.15 39.52 105.50 68.20 HF (N = 34) Pretest 97.08 39.79 95.34 43.18 Posttest 98.02 34.47 96.63 42.59 Confusion (N = 34) Pretest 3.44 3.67 3.38 3.74 Posttest 1.53 2.46 3.44 4.36 Vigor (N = 34) Pretest 13.38 6.38 13.59 6.16 Posttest 14.32 6.21 9.44 6.71 Fatigue (N = 34) Pretest 2.76 3.87 3.18 4.34 Posttest 1.71 2.80 5.06 5.73 Anger (N = 34) Pretest 1.59 4.26 1.68 4.31 Posttest 0.65 2.01 2.00 4.58 Tension (N = 34) Pretest 3.29 4.87 3.85 4.45 Posttest 0.85 2.05 3.26 5.22 Depression (N = 34) Pretest 1.82 3.96 2.24 5.18 Posttest 0.97 2.68 2.97 6.12 TMD (N = 34) Pretest −0.47 21.58 0.74 22.79 Posttest −8.62 13.42 7.29 27.70 SART (N = 31b) Pretest 9.03 6.62 8.65 6.39 Posttest 7.45 5.01 7.32 6.03 RCS (N = 34) Being away 33.44 6.11 18.68 8.51 Extent 21.32 3.28 11.12 6.22 Fascination 31.65 3.84 15.85 7.23 Compatibility 24.26 3.61 14.29 5.41
Abbreviations: SBP=systolic blood pressure; DBP=diastolic blood pressure; HR=heart rate; HF=high frequency; TMD=total mood disturbance; RCS= restorative components scale.
3.2. Physiological indicators of stress
The results of two-way repeated-measures ANOVAs are shown in Table 3. None of the interactions were significant with one exception; a significant difference was found in time factors for heart rate (F = 61.416, p < .001, ηp2 =0.482).
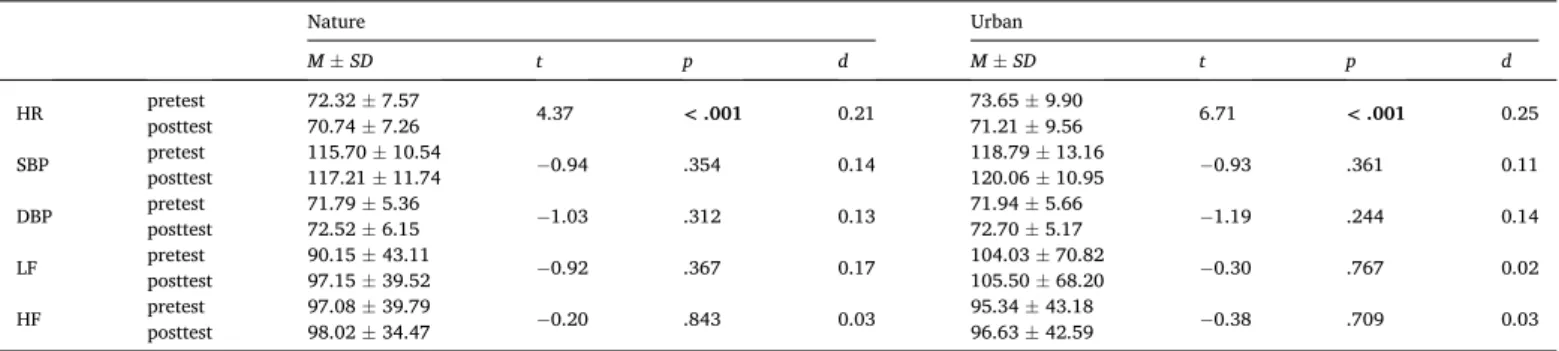
Table 4 displays the results of paired-sample t-tests regarding phys-iological responses. Significant differences were observed between the pretest and the posttest mean heart rates of the virtual nature setting (t (33) = 4.37, p < .001, d = 0.21) and the virtual urban setting (t(33) = 6.71, p < .001, d = 0.25), see Fig. 4.
Table 5 displays the comparisons in the physiological response change scores between the two virtual settings. There were no observed differences between settings.
3.3. Mood states changes
The results of two-way repeated-measures ANOVAs are shown in Table 6. There were significant interactions between the effects of time and setting on confusion (F = 7.427, p = .008, ηp2 =0.101), vigor (F = 16.448, p < .001, ηp2 = 0.199), fatigue (F = 13.091, p = .001, ηp2 = 0.166), and total mood disturbance (TMD, F = 12.347, p < .001, ηp2 = 0.158).
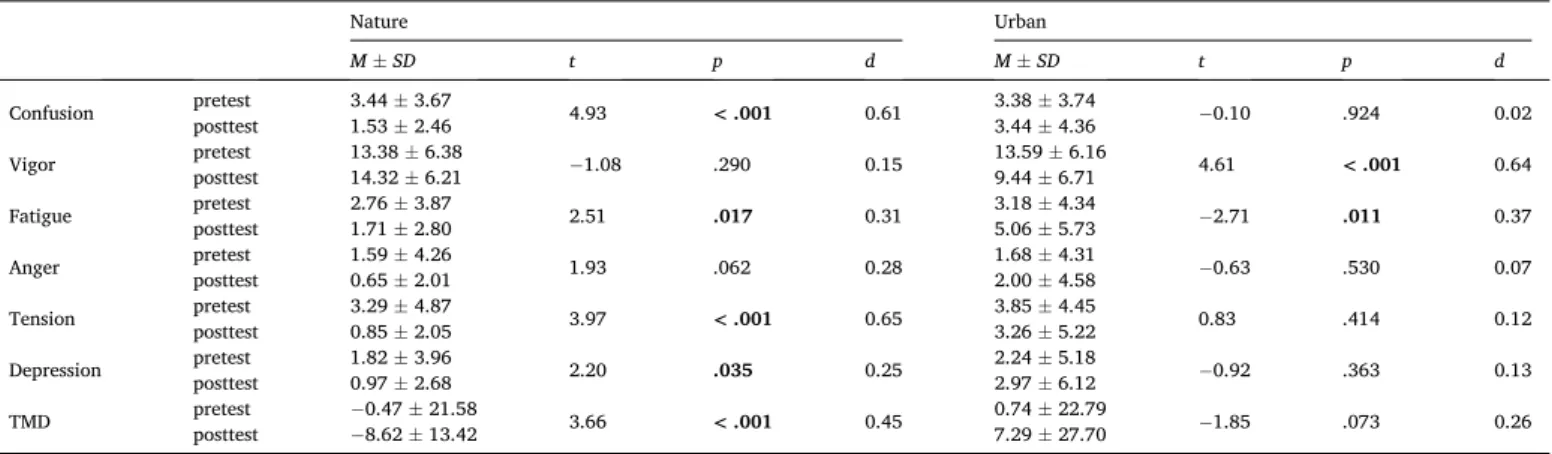
Table 7 presents the results regarding the six constructs of the profile of mood states. Significant differences were observed between pretest and posttest in all variables except vigor and anger for the virtual natural setting [confusion: t(33) = 4.93, p < .001, d = 0.61; fatigue: t(33) = 2.51, p = 0.017, d = 0.31; tension: t(33) = 3.97, p < .001, d = 0.65; depression: t(33) = 2.20, p =0.035, d = 0.25; TMD: t(33) = 3.66, p < .001, d = 0.45]. Specifically, the posttest scores of confusion, fatigue, tension, depression, and TMD were lower than the pretest scores (Fig. 5). In the virtual urban setting, a significant difference was observed between the pretest and the posttest in vigor and fatigue [vigor: t(33) = 4.61, p < .001, d = 0.64; fatigue: t(33) = -2.71, p =0.011, d = 0.37] (Table 7). The posttest score of vigor was lower than the pretest score, and the posttest score of fatigue was higher than the pretest score (see Fig. 6).
Table 8 displays the differences in psychological response change
scores between the two virtual settings. There were significant differ-ences in confusion, vigor, fatigue, anger, and TMD [confusion: t(33) = -2.77, p = 0.009, d = 0.66; vigor: t(33) = 5.10, p < .001, d = 0.98; fa-tigue: t(33) = -3.48, p =0 .001, d = 0.88; anger: t(33) = -2.05, p =0.049,
d = 0.43; TMD: t(33) = -3.56, p =0 .001, d = 0.85], see Fig. 7.
3.4. Attention performance
Regarding the analysis of SART, three participants were excluded due to incomplete test data. Consequently, 31 responses remained for further analysis.
There were no significant changes between the pretest and posttest scores in the virtual nature setting (t(30) = 1.65, p = 0.109, d = 0.27) or the virtual urban setting (t(30) = 1.92, p = 0.065, d = 0.21). To test for differences between settings, another paired-sample t-test was per-formed. The results show there was no difference in change scores be-tween the two settings (t(30)= -0.21, p = 0.833, d = 0.06).
3.5. Perceived restorativeness
Table 9 presents the results of paired sample t-tests on the RCS. Mean scores of the four components in the virtual nature setting were higher than those in the virtual urban setting [being away: t(33) = 8.53, p < .001, d = 1.99; extent: t(33) = 8.48, p < .001, d = 3.11; fascination: t(33) =9.89, p < .001, d = 2.73; compatibility: t(33) = 8.77, p < .001, d = 2.17].
3.6. Qualitative assessment
The study had a 0% dropout rate. Four of the 34 participants (11.8 %) and six of the 34 participants (17.6 %) reported feeling uncomfort-able (dizziness or facial pressure) during the virtual nature setting and virtual urban setting, respectively. Participants generally agreed that the virtual urban setting was stressful, oppressive, clamorous, noisy, and boring. In contrast, the majority of participants described the virtual natural setting as appeasing, refreshing, delightful, relaxing, and calm-ing; the water, sounds of the waterfall and stream, mountains, and for-ests were considered most restorative (see Table S1). Some respondents felt free and at ease in the virtual nature setting and thought the setting could comfort their body and mind. Participants also indicated their desire to be in physically present in the outdoor nature settings so that they could inhale fresh air and feel cool water. Illustrative comments of the latter sentiments included:
“…feel like to do exercise and take a walk there.” “…make me want to visit Nei-dong.”
“…the environment was comfortable…really want to inhale the fresh air and feel the cold water.”
4. Discussion
4.1. Physiological responses to virtual settings
The goal of this study was to advance our understanding of the restorative effects of virtual natural settings in middle-aged and older adults. Unexpectedly, we observed few physiological changes over the course of exposure to virtual natural or urban settings, and we observed no differences in physiological responses between these two settings. Therefore, our findings do not support prevailing theories regarding psychological relaxation from immersion specifically in natural settings. However, the posttest results for heart rate in both settings were lower than pretest measurements, showing that virtual settings - regardless of content - can induce restorative physiological effects. This conclusion is reinforced by another study with younger adults Yu et al. (2018).
Also unexpectedly, blood pressure slightly increased (albeit minorly Table 3
Physiological results of two-way repeated-measures ANOVAs.
F p ηp2 HR Time (T) 61.416 <0.001*** 0.482 Setting (S) 0.185 0.668 0.003 T x S 2.752 0.102 0.04 SBP Time 1.733 0.193 0.026 Setting 1.243 0.269 0.019 T x S 0.013 0.909 <0.001 DBP Time 2.429 0.124 0.037 Setting 0.017 0.898 <0.001 T x S 0.001 0.975 <0.001 LF Time 0.864 0.356 0.013 Setting 0.72 0.399 0.011 T x S 0.368 0.564 0.006 HF Time 0.146 0.703 0.002 Setting 0.028 0.867 <0.001 T x S 0.004 0.952 <0.001 LF/HF Time 2.129 0.149 0.031 Setting 1.325 0.254 0.02 T x S 0.182 0.671 0.003
Note: ηp2 =partial eta squared (effect size); *:p < 0.05; **:p < 0.01; ***:p < 0.001; ANOVA with Bonferroni adjustment; LF/HF=ratio of low frequency and high frequency
and not significantly) over the course of VR exposure to both urban and natural settings. This slight increase may be because participants were excited about experiencing VR since the majority had limited prior experience, which could have resulted in increased blood pressure with the posttest measurement. We suggest future studies conduct longer- term experiments that involve several waves of VR experiences to avoid any potential disturbance of excitement in the results.
Another explanation for our unexpected physiological responses may involve the duration of the experiment. The total time of immersion was 10 min. This may be too brief to activate sympathetic and/or para-sympathetic nervous system responses in older adults.
4.2. Psychological responses to virtual settings
In contrast to the physiological results, our psychological results were as expected. Participants reported more positive feelings and lower levels of fatigue and depression after a virtual nature setting than after a
virtual urban setting. This finding is in accordance with several other studies, such as Lee et al. (2011), Song et al. (2017) and Ulrich (1981). Furthermore, in the current study, participants’ emotions were restored after exposure to virtual natural settings and worsened after exposure to virtual urban settings. Such results support the argument that a natural setting is not only conducive to psychological restoration but the opposite of a natural setting - a built urban environment with little or no natural elements - degrades psychological states. Importantly, the psy-chological measurements employed in this study were similar to those from previous research studies (e.g., van den Berg, 2009; Yu et al., 2018), further substantiating the hypothesis that virtual natural settings evoke stronger positive effects in middle-aged and elderly people than do virtual urban settings.
4.3. Attention restoration and perceived restorativeness of virtual settings
This study measured the number of mistakes participants made in the SART as an indicator of participants’ levels of attention before and after exposure to virtual settings. The results show participants made fewer Table 4
Results of paired-sample t-tests regarding physiological responses in the two virtual settings.
Nature Urban M ± SD t p d M ± SD t p d HR pretest posttest 72.32 ± 7.57 70.74 ± 7.26 4.37 < .001 0.21 73.65 ± 9.90 71.21 ± 9.56 6.71 < .001 0.25 SBP pretest 115.70 ± 10.54 −0.94 .354 0.14 118.79 ± 13.16 −0.93 .361 0.11 posttest 117.21 ± 11.74 120.06 ± 10.95 DBP pretest 71.79 ± 5.36 −1.03 .312 0.13 71.94 ± 5.66 −1.19 .244 0.14 posttest 72.52 ± 6.15 72.70 ± 5.17 LF pretest 90.15 ± 43.11 −0.92 .367 0.17 104.03 ± 70.82 −0.30 .767 0.02 posttest 97.15 ± 39.52 105.50 ± 68.20 HF pretest 97.08 ± 39.79 −0.20 .843 0.03 95.34 ± 43.18 −0.38 .709 0.03 posttest 98.02 ± 34.47 96.63 ± 42.59
Note: Statistically significant differences shown in bold, p < .05. HR = heart rate; SBP = systolic blood pressure; DBP = diastolic blood pressure; LF = sympathetic nervous system activity (SNS); HF = parasympathetic nervous system activity (PSNS); d=Cohen’s d.
Fig. 4. Pretest and posttest heart rate comparisons between the two vir-tual settings.
Table 5
Comparison of physiological response change scores between virtual natural and urban settings. Setting M ± SD t p d ΔHR Nature Urban −−1.59 ± 2.12 2.44 ± 2.12 2.00 .054 0.40 ΔSBP Nature Urban 1.52 ± 9.26 1.27 ± 7.89 0.10 .920 0.03 ΔDBP Nature 0.73 ± 4.06 − 0.03 .976 0.01 Urban 0.76 ± 3.67 Δ LF Nature Urban 7.00 ± 44.66 1.47 ± 28.79 0.60 .554 0.25 Δ HF Nature 0.94 ± 27.43 − 0.06 .955 0.02 Urban 1.29 ± 19.89 Note: Δ=posttest-pretest. Table 6
Psychological results of two-way repeated-measures ANOVAs.
F p ηp2 Confusion Time 6.567 0.013* 0.09 Setting 1.338 0.252 0.02 T x S 7.427 0.008* 0.101 Vigor Time 6.529 0.013* 0.09 Setting 2.747 0.102 0.04 T x S 16.448 <0.001*** 0.199 Fatigue Time 1.026 0.315 0.015 Setting 3.813 0.055 0.055 T x S 13.091 0.001** 0.166 Anger-hostility Time 0.768 0.384 0.012 Setting 0.662 0.419 0.01 T x S 3.22 0.077 0.047 Tension Time 10.374 0.002** 0.136 Setting 2.505 0.118 0.037 T x S 3.881 0.053 0.056 Depression Time 0.018 0.895 <0.001 Setting 1.341 0.251 0.02 T x S 3.213 0.078 0.046 TMD Time 0.144 0.706 0.002 Setting 3.047 0.086 0.044 T x S 12.347 0.001** 0.158
Note: ηp2 =partial eta squared (effect size); *:p < 0.05; **:p < 0.01; ***:p < 0.001; ANOVA with Bonferroni adjustment.
mistakes after exposure than before, regardless of the content (natural or urban settings) shown in VR; however, these changes were not statisti-cally significant. Further, we observed no difference in change scores between the virtual natural settings and virtual urban settings.These findings might be explained by participants’ increased familiarity with the SART after the pre-exposure task, and therefore, learning effects that artificially increased scores after exposure. Such learning effects may have been compounded by our use of a cross-over design, which allowed participants to complete the SART a total of four times. We recommend
future research consider alternative measures of attention restoration to overcome such possible limitations.
In contrast, the two virtual settings exhibited marked differences in perceived restorativeness. Specifically, nature settings were rated higher than urban settings, which is mostly consistent with a large body of Table 7
Results of paired-sample t-tests in the six constructs of POMS and total mood disturbance (TMD) for the two virtual settings.
Nature Urban M ± SD t p d M ± SD t p d Confusion pretest 3.44 ± 3.67 4.93 < .001 0.61 3.38 ± 3.74 −0.10 .924 0.02 posttest 1.53 ± 2.46 3.44 ± 4.36 Vigor pretest 13.38 ± 6.38 −1.08 .290 0.15 13.59 ± 6.16 4.61 < .001 0.64 posttest 14.32 ± 6.21 9.44 ± 6.71 Fatigue pretest 2.76 ± 3.87 2.51 .017 0.31 3.18 ± 4.34 −2.71 .011 0.37 posttest 1.71 ± 2.80 5.06 ± 5.73 Anger pretest 1.59 ± 4.26 1.93 .062 0.28 1.68 ± 4.31 −0.63 .530 0.07 posttest 0.65 ± 2.01 2.00 ± 4.58
Tension pretest posttest 3.29 ± 4.87 0.85 ± 2.05 3.97 < .001 0.65 3.85 ± 4.45 3.26 ± 5.22 0.83 .414 0.12
Depression pretest 1.82 ± 3.96 2.20 .035 0.25 2.24 ± 5.18 −0.92 .363 0.13
posttest 0.97 ± 2.68 2.97 ± 6.12
TMD pretest − 0.47 ± 21.58 3.66 < .001 0.45 0.74 ± 22.79 −1.85 .073 0.26
posttest − 8.62 ± 13.42 7.29 ± 27.70
Note: Statistically significant differences shown in bold, p < .05. TMD = total mood disturbance.
-25 -20 -15 -10 -5 0 5 10 15 20 25
Confusion Vigor Fatigure Anger Tension Depression TMD
Sc or es o f P O M S pretest posttest *** * *** * ***
Fig. 5. Pretest and posttest mood states comparisons in the virtual na-ture condition.
Fig. 6. Pretest and posttest mood states comparisons in the virtual urban setting.
Table 8
Differences of mood and total mood disturbance response change scores be-tween virtual nature and urban settings.
Setting M ± SD t p d
Δ Confusion Nature − 1.91 ± 2.26 −2.77 .009 0.66
Urban 0.06 ± 3.56
Δ Vigor Nature Urban 0.94 ± 5.10 − 4.15 ± 5.24 5.10 < .001 0.98
Δ Fatigue Nature − 1.06 ± 2.46 −3.48 .001 0.88 Urban 1.88 ± 4.05 Δ Anger Nature − 0.94 ± 2.84 −2.05 .049 0.43 Urban 0.32 ± 2.97 Δ Tension Nature − 2.44 ± 3.59 −1.70 .098 0.48 Urban − 0.59 ± 4.15 Δ Depression Nature − 0.85 ± 2.26 −1.93 .062 0.44 Urban 0.74 ± 4.65 Δ TMD Nature − 8.15 ± 12.97 −3.56 .001 0.85 Urban 6.56 ± 20.67
Note: Statistically significant differences shown in bold, p < .05. TMD = total mood disturbance.
Fig. 7. Comparisons of the mood state change scores between virtual nature and urban settings.
environmental psychology research (Browning et al., 2020a; Hartig et al., 2003; Wang et al., 2016). Natural settings appear to better meet the attributes of restorative environments, as outlined in attention restoration theory (Kaplan, 1995). Interestingly, although our results demonstrated that virtual natural settings showed higher restorative scores than virtual urban settings, these subjective scores were not re-flected in improvements in physiological or attentional performance measures, as explained above. It remains unclear how the properties of virtual environments trigger physical and cognitive processes or to what extent physiological and cognitive responses can be influenced by environmental attributes specifically with older adults.
4.4. Implications for therapeutic uses of VR with middle-aged and elderly adults
The current study highlights the therapeutic potential of VR expe-riences amongst middle-aged and elderly adults. Participants reported feeling pleasant, calm, delighted, relaxed, free, refreshed and comfort-able in virtual nature settings. They were attracted to running water, waterfall sounds, mountains, and forests. Further, they described these natural elements as vivid and motivators for going outdoors into nature. Few participants reported feelings of dizziness or facial pressure from the VR HMD. Accordingly, ongoing research on the therapeutic imple-mentation of VR with this population is supported.
White et al. (2018) reviews the risks, benefits, and cost efficiency of applying VR technology in health care systems. A research opportunity exists in regard to the evidence-based benefits of simulated natural settings. Because of the short history of consumer-grade immersive VR technology, our study provides only preliminary evidence of the restorative experience of VR for older adults. Immersive VR technology is particularly important for people with mobility constraints, people without easy access to actual natural settings, and urban dwellers engaging in social/physical distancing. Moreover, the positive impact of simulated nature settings could benefit elderly populations within resi-dential care facilities or clinical settings (Ba˜nos et al., 2013; Hoffman et al., 2000). Our findings suggest that virtual nature experiences might serve as an alternative approach to going outside but also as a channel for motivating people to visit nature outdoors.
5. Conclusion
VR equipment was used in this study to show virtual natural and urban settings to middle-aged and older adults and to study changes in their physiological, psychological, and attention performance changes. Although we did not observe changes in the physiology, we did see virtual natural settings (but not virtual urban settings) promoted psy-chologically restorative effects. The content of the virtual setting should be considered if VR is used to improve the physical and mental condi-tions of elderly and middle-aged people.
Funding
This research was supported by a grant from the Ministry of Science
and Technology of Taiwan [109-2410-H-002-109].
CRediT authorship contribution statement
Chia-Pin Yu: Conceptualization, Methodology, Writing - review &
editing, Supervision, Funding acquisition. Hsiao-Yun Lee: Conceptu-alization, Methodology, Formal analysis, Validation, VisuConceptu-alization, Writing - original draft. Wen-Hsin Lu: Investigation, Data curation, Formal analysis, Writing - original draft, Project administration. Yu-
Chih Huang: Validation, Writing - review & editing. Matthew H.E.M. Browning: Validation, Writing - review & editing.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Appendix A. Supplementary data
Supplementary material related to this article can be found, in the online version, at doi:https://doi.org/10.1016/j.ufug.2020.126863.
References
Appel, L., Appel, E., Bogler, O., Wiseman, M., Cohen, L., Ein, N., et al., 2020. Older adults with cognitive and/or physical impairments can benefit from immersive virtual reality experiences: a feasibility study. Front. Med. 6, 329. https://doi.org/10.3389/ fmed.2019.00329.
Ba˜nos, R.M., Espinoza, M., García-Palacios, A., Cervera, J.M., Esquerdo, G., Barraj´on, E., Botella, C., 2013. A positive psychological intervention using virtual reality for patients with advanced cancer in a hospital setting: a pilot study to assess feasibility. Support. Care Cancer 21, 263–270.
Berto, R., 2005. Exposure to restorative environments helps restore attentional capacity. J. Environ. Psychol. 25 (3), 249–259. https://doi.org/10.1016/j.jenvp.2005.07.001.
Berto, R., 2014. The role of nature in coping with psycho-physiological stress: a literature review on restorativeness. Behav. Sci. 4, 394–409.
Bielinis, E., Takayama, N., Boiko, S., Omelan, A., Bielinis, L., 2018. The effect of winter forest bathing on psychological relaxation of young Polish adults. Urban For. Urban Green 29, 276–283.
Browning, M.H.E.M., Saeidi-Rizi, F., McAnirlin, O., Yoon, H., Pei, Y., 2020a. The role of methodological choices in the effects of experimental exposure to simulated natural landscapes on human health and cognitive performance: a systematic review. Environ. Behav. 7 (1), 1–43.
Burdea, G.C., Coiffet, P., 2003. Virtual Reality Technology, second edition. Wiley-IEEE Press, New Jersey, USA.
Camm, A.J., Malik, M., Bigger, J.T., Breithardt, G., Cerutti, S., Cohen, R.J., et al., 1996. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 17, 354–381.
Chen, H.-T., Yu, C.-P., Lee, H.-Y., 2018. The effects of forest bathing on stress recovery: evidence from middle-aged females of Taiwan. Forests 9 (7), 403. https://doi.org/ 10.3390/f9070403.
Cohen, J., 1988. Statistical Power Analysis for the Behavioral Sciences. Lawrence Earlbaum Associates, Hillsdale, NJ.
Gaboda, D., Lucas, J., Siegel, M., Kalay, E., Crystal, S., 2011. No longer undertreated? Depression diagnosis and antidepressant therapy in elderly long-stay nursing home residents, 1999 to 2007. J. Am. Geriatr. Soc. 59 (4), 673–680. https://doi.org/ 10.1111/j.1532-5415.2011.03322.x.
García-Betances, R.I., Jim´enez-Mixco, V., Arredondo, M.T., Cabrera-Umpi´errez, M.F., 2014. Using virtual reality for cognitive training of the elderly. Am. J. Alzheimer’s Disease Other Dementiasr. 30 (1), 49–54. https://doi.org/10.1177/
1533317514545866.
Gower, A.L., Crick, N.R., 2011. Baseline autonomic nervous system arousal and physical and relational aggression in preschool: the moderating role of effortful control. Int. J. Psychophysiol. 81 (3), 142–151. https://doi.org/10.1016/j.ijpsycho.2011.06.001. Guti´errez, A., M. A, Vexo, F., Thalmann, D., 2008. Stepping into virtual reality. Stepping
Into Virtual Reality. https://doi.org/10.1007/978-1-84800-117-6.
Hartig, T., Evans, G.W., Jamner, L.D., Davis, D.S., G¨arling, T., 2003. Tracking restoration in natural and urban field settings. J. Environ. Psychol. 23 (2), 109–123. https://doi. org/10.1016/S0272-4944(02)00109-3.
Hartig, T., Mitchell, R., de Vries, S., Frumkin, H., 2014. Nature and health. Annu. Rev. Public Health 35 (1), 207–228. https://doi.org/10.1146/annurev-publhealth- 032013-182443.
Herzog, T.R., Colleen, Maguire, P., Nebel, M.B., 2003. Assessing the restorative components of environments. J. Environ. Psychol. 23 (2), 159–170. https://doi.org/ 10.1016/S0272-4944(02)00113-5.
Table 9
Difference between perceived restorativeness scores between virtual nature and urban settings.
Setting M ± SD t p d
Being away Nature 33.44 ± 6.11 8.53 <.001*** 1.99
Urban 18.68 ± 8.51 Extent Nature 21.32 ± 3.28 8.48 <.001*** 3.11 Urban 11.12 ± 6.22 Fascination Nature 31.65 ± 3.84 9.89 <.001*** 2.73 Urban 15.85 ± 7.23 Compatibility Nature 24.26 ± 3.61 8.77 <.001*** 2.17 Urban 14.29 ± 5.41
Hoffman, H.G., Patterson, D.R., Carrougher, G.J., 2000. Use of virtual reality for ad- junctive treatment of adult burn pain during physical therapy: a controlled study. Clin. J. Pain 16, 244–250.
Ikei, H., Song, C., Miyazaki, Y., 2017. Physiological effects of wood on humans: a review. J. Wood Sci. 63 (1), 1–23. https://doi.org/10.1007/s10086-016-1597-9. Joseph, A., Browning, M., Jiang, S., 2020. Using immersive virtual environments (IVEs)
to conduct environmental design research: a primer and decision framework. Herd Health Environ. Res. Des. J. 10 https://doi.org/10.1177/1937586720924787, 193758672092478–27.
Kaplan, S., 1995. The restorative benefits of nature: toward an integrative framework. J. Environ. Psychol. 15, 169–182.
Kaplan, R., Kaplan, S., 1989. The Experience of Nature: a Psychological Perspective. Cambridge University Press, Cambridge.
Karmanov, D., Hamel, R., 2008. Assessing the restorative potential of contemporary urban environment(s): beyond the nature versus urban dichotomy. Landsc. Urban Plan. 86 (2), 115–125. https://doi.org/10.1016/j.landurbplan.2008.01.004. Laumann, K., Garling, T., Stormark, K.M., 2001. Rating scale measures of restorative
components of environments. J. Environ. Psychol. 21 (1), 31–44. https://doi.org/ 10.1006/jevp.2000.0179.
Lee, J., Park, B.-J., Tsunetsugu, Y., Ohira, T., Kagawa, T., Miyazaki, Y., 2011. Effect of forest bathing on physiological and psychological responses in young Japanese male subjects. Public Health 125 (2), 93–100.
Leontjevas, R., Gerritsen, D.L., Smalbrugge, M., Teerenstra, S., Vernooij-Dassen, M.J., Koopmans, R.T., 2013. A structural multidisciplinary approach to depression management in nursing-home residents: a multicentre, stepped-wedge cluster- randomised trial. Lancet 381 (9885), 2255–2264. https://doi.org/10.1016/S0140- 6736(13)60590-5.
Lin, C.X., Lee, C., Lally, D., Coughlin, J.F., 2018. Impact of virtual reality (VR) experience on older adults’ well-being. Proceedings of the International Conference on Human Aspects of IT for the Aged Population 89–100.
Lune, H., Berg, B.L., 2017. Qualitative Research Methods for the Social Sciences. Pearson.
Manly, T., Robertson, I.H., 2005. The sustained attention to response test (SART). Neurobiology of Attention. Academic Press.
Manly, T., Robertson, I.H., Galloway, M., Hawkins, K., 1999. The absent mind: further investigations of sustained attention to response. Neuropsychologia 37, 661–670.
Markevych, I., Schoierer, J., Hartig, T., Chudnovsky, A., Hystad, P., Dzhambov, A.M., et al., 2017. Exploring pathways linking greenspace to health: theoretical and methodological guidance. Environ. Res. 158, 301–317.
Mirelman, A., Maidan, I., Shiratzky, S.S., Hausdorff, J.M., 2020. Virtual reality training as an intervention to reduce Falls. In: Montero-Odasso, M., Camicioli, R. (Eds.), Falls and Cognition in Older Persons, pp. 309–321. https://doi.org/10.1007/978-3-030- 24233-6_18.
Park, J., Yim, J., 2016. A new approach to improve cognition, muscle strength, and postural balance in community-dwelling elderly with a 3-D virtual reality kayak program. Tohoku J. Exp. Med. 238 (1), 1–8. https://doi.org/10.1620/tjem.238.1.
Robertson, I.H., Manly, T., Andrade, J., Baddeley, B.T., Yiend, J., 1997. Oops!’: performance correlates of everyday attention failures in traumatic brain injured and normal subjects. Neuropsychologia 35 (6), 747–758.
Shacham, S., 1983. A shortened version of the Profile of Mood States. J. Pers. Assess. 47 (3), 305–306.
Song, C., Ikei, H., Kobayashi, M., Miura, T., Li, Q., Kagawa, T., et al., 2017. Effects of viewing forest landscape on middle-aged hypertensive men. Urban For. Urban Green. 21, 247–252. https://doi.org/10.1016/j.ufug.2016.12.010.
Sonntag-¨Ostr¨om, E., Nordin, M., Lundell, Y., Dolling, A., Wiklund, U., Karlsson, M., et al., 2014. Restorative effects of visits to urban and forest environments in patients with exhaustion disorder. Urban For. Urban Green. 13 (2), 344–354. https://doi.org/ 10.1016/j.ufug.2013.12.007.
Stone, R., Small, C., Knight, J., Qian, C., Shingari, V., 2014. Virtual natural environments for restoration and rehabilitation in healthcare. In: Ma, M., Jain, L.C., Anderson, P. (Eds.), Virtual, Augmented Reality and Serious Games for Healthcare 1, pp. 497–521. https://doi.org/10.1007/978-3-642-54816-1_24.
Ulrich, R.S., 1981. Natural versus urban scenes: some psychophysiological effects. Environ. Behav. 13 (5), 523–556.
Ulrich, R.S., Simons, R.F., Losito, B.D., Fiorito, E., Miles, M.A., Zelson, M., 1991. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 11, 201–230.
Valtchanov, D., Ellard, C., 2010. Physiological and affective responses to immersion in virtual reality: Effects of nature and urban settings. J. Cybertherapy Rehab. 3 (4), 359–373.
Valtchanov, D., Ellard, C., 2015. Cognitive and affective responses to natural scenes: effects of low level visual properties on preference, cognitive load and eye- movements. J. Environ. Psychol. 43, 184–195.
Valtchanov, D., Barton, K.R., Ellard, C., 2010. Restorative effects of virtual nature settings. Cyberpsychol. Behav. Soc. Netw. 13 (5), 503–512.
van den Berg, A.E., 2009. Restorative effects of nature: towards a neurobiological approach. Proceedings of 9th Congress of Physiological Anthropology 132–138. Wang, X., Rodiek, S., Wu, C., Chen, Y., Li, Y., 2016. Stress recovery and restorative effects
of viewing different urban park scenes in Shanghai, China. Urban For. Urban Green. 15, 112–122. https://doi.org/10.1016/j.ufug.2015.12.003.
White, M.P., Yeo, N.L., Vassiljev, P., Lundstedt, R., Wallergård, M., Albin, M., L˜ohmus, M., 2018. A prescription for “nature” - the potential of using virtual nature in therapeutics. Neuropsychiatr. Dis. Treat. 14, 3001–3013. https://doi.org/ 10.2147/NDT.S179038.
World Health Organization, 2017. Global Strategy and Action Plan on Ageing and Health. https://apps.who.int/iris/bitstream/handle/10665/329960/97892415 13500-eng.pdf.
Yu, C.-P., Lin, C.-M., Tsai, M.-J., Tsai, Y.-C., Chen, C.-Y., 2017. Effects of short forest bathing program on autonomic nervous system activity and mood states in middle- aged and elderly individuals. Int. J. Environ. Res. Public Health 14 (8), 897. https:// doi.org/10.3390/ijerph14080897.
Yu, C.-P., Lee, H.-Y., Luo, X.-Y., 2018. The effect of virtual reality forest and urban environments on physiological and psychological responses. Urban For. Urban Green. 35, 106–114. https://doi.org/10.1016/j.ufug.2018.08.013.