Full Article’s Title
Development of Online Diary and Self-Management System on e-Healthcare for Asthmatic Children in Taiwan
Corresponding Author Information
Jing-Long Huang, MD, ([email protected])
Department of Pediatrics, Chang Gung Memorial Hospital and College of Medicine, Chang Gung University
No.5, Fusing St., Gueishan, Taoyuan 333, Taiwan TEL: +886-3-3281200 FAX: +886-3-3285056
Authors and Affiliations
Hsueh-Chun Lin, PhD, ([email protected], 886-4-22070429), Associate Professor, Department of Health Risk Management, China Medical University, 91 Hsueh-Shi Road, Taichung 40402, Taiwan.
Li-Chi Chiang, RN, PhD, ([email protected], 886-2-87923100), Professor,
School of Nursing, National Defense Medical Center, 161 Sec 6, Ming-Chuan East Road, Neihu, Taipei 114, Taiwan
Tzu
-N ing Wen , RN, MS, ([email protected]), Graduate student
Institute of Biomedical Informatics, National Yang-Ming University, No.155, Sec.2, Linong Street, Taipei 112, Taiwan
Kuo-Wei Yeh, MD, ([email protected]), Assistant professor and Chief of Division
Division of Allergy, Asthma and Rheumatology, Department of Pediatrics, Chang Gung Memorial Hospital and College of Medicine, Chang Gung University, No.5, Fusing St., Gueishan, Taoyuan 333, Taiwan
Abstract
Objective: Many regional programs of the countries educate asthmatic children and their
families to manage healthcare data. This study aims to establish a Web-based self-management system, eAsthmaCare, to promote the electronic healthcare (e-Healthcare) services for the asthmatic children in Taiwan. The platform can perform real time online functionality based upon a five-tier infrastructure with mutually supportive components to acquire asthma diaries, quality of life assessments and health educations.
Methods: We have designed five multi-disciplinary portions on the interactive interface
functioned with the analytical diagrams: (1) online asthma diary, (2) remote asthma assessment, (3) instantaneous asthma alert, (4) diagrammatical clinic support, and (5) asthma health education. The Internet-based asthma diary and assessment program was developed for patients to process self-management healthcare at home. In addition, the online analytical charts can help healthcare professionals to evaluate multi-domain health information of patients immediately.
Results: eAsthmaCare was developed by JavaTM Servlet/JSP technology upon Apache
TomcatTM web server and OracleTM database. Forty-one voluntary asthmatic children (and
their parents) were intervened to examine the proposed system. Seven domains of satisfiability assessment by using the system were applied for approving the development. The average scores were scaled in the acceptable range for each domain to ensure feasibility of the proposed system.
Conclusion: The study revealed the details of system infrastructure and developed functions
that can help asthmatic children in self-management for healthcare to enhance communications between patients and hospital professionals.
Keywords: e-Healthcare, self-management healthcare system, real time online analysis,
1. Introduction
In the past decade, World Health Organization (WHO) and Global Initiative for Asthma (GINA) published a global surveillance revealing that asthma has been the most common chronic disease of children in many developed nations due to their official statistics of health data [1][2]. As the viewpoint of healthcare, it implied that the financial burdens of patients and their families and hospital would be heavier due to rising prevalence of childhood asthma. Many regional programs were continuously making progresses for asthma health care over recent decades in a variety of countries to reduce medical expenses [3]-[7]. The well-known ISAAC program, "International Study of Asthma and Allergies in Childhood," comprised three phases for assessments [8] which were followed by past researches to regulate the principles of guidance for preventive care. For example, (1) initiating medications for asthma symptoms by severity, (2) using spirometers for assistance in diagnosis and evaluation, (3) monitoring the asthma morbidity depending upon routine symptom assessments, (4) educating patients by planning self-management asthma care at home, etc. [9] These procedures enabled asthmatic children and their family to manage healthcare data.
In Taiwan, numerous studies of children with asthma established appropriate assessment questionnaires based on the ISAAC procedure to disseminate prevention knowledge regarding health care in the hospital or at home. The findings exhibited that the increase proportion of nation’s population was 20 times and the age of incidence was getting younger in the last four decades [10]-[13]. Therefore, patients were gradually encouraged to extend their awareness of managing, preventing, and controlling illness based on the modern guidelines of asthma health care. The guidelines could afford the education of self-management in clinical practice while the data of asthma control at home have been referred to assess the sufficiency of contemporary treatment [14]. Many patients with chronic illness conditions were invented in the self-management programs for educating them with the helpful skills of self healthcare in
primary care [15][16]. The programs utilized various resources to serve the patients for approaching medical, role, and emotional managements from problem solving, action planning, to decision making [17]. The self-management program of asthmatic health care assisted patients to take care of themselves effectively including measuring health-related quality of life (QOL) and daily asthma condition; i.e., the program provides various impacts to support clinical decisions on the asthmatic treatments [18][19]. As evaluating the asthmatic conditions of the children in clinic visits, their parents were encouraged to share their watches on the fluctuations of peak expiratory flow (PEF) measured in the previous cure period [20]-[23]. For the typical self-management, the asthmatic children were usually asked to write down the daily PEFs twice in the symptom diary at home and show the outcomes in clinic [24][25]. Thus, the computer-based assessment programs could help to improve children’s self-management skills (e.g., assess their asthma symptoms and QOL) and to achieve accurate outcomes (e.g., monitor their functional status and daily PEF) [26][27]. Recently, health services by innovative Internet technique were widely promoted to enhance electronic healthcare (e-Healthcare) for requirements above on self-management of daily traceable illnesses including asthma care [28]-[33].
The Internet-based applications for asthma e-Healthcare herein would be functioned by online education and assessment for users, feedback from patients and health professionals, interaction interface between children and their parents; networking collaboration of clinical data and healthcare records, and supervision on therapeutic scheme and decision support [34]. The major scope targeted to automatically compute self-reported data and assess the asthma diary for improving asthma control with alert criteria and remote monitoring [21][34]. In addition, via Internet, the minority children could obtain more free resources in education, medication, finance, or their social and physical situation [35]-[39]. Similar study has been intervened for kids with asthma in southern Taiwan by proposing an asthma reporting Web
site to provide off-line data analysis [40]. The past research programs exhibited positive results of self-management for e-Healthcare services of asthma but usually lacked a platform with self-developed and analytical modules..
In this study, we developed a Web-based self-management system, eAsthmaCare, on e-Healthcare services for the children with asthma in Taiwan. The diagram functions of the system inherited from the core modules of self-developed infrastructure in the previous work. Thus, new database schemes and interfaces were created for instant online analyses correlative to the asthma diary, QOL assessment and health education [41][42]. Five multi-disciplinary portions herein were involved in an interactive interface and functioned with five kinds of analytical diagrams relative to management of asthma health care. The questionnaires were adopted from asthma-related QOL (ARQOL) that includes five dimensions: restrictions of social life, physical disturbances from symptoms, limitations of physical activity, daily inconveniences in managing the disease and emotional distress [43]. In this approach, we focused on the methods of design and development that will be detailed in next section followed by results of system performance. In further, the voluntary asthmatic children (and their parents) were intervened by the e-Healthcare project that was enforced in the pediatrics department of Chang-Gung Hospital at Lin Kou (CGH-LK), Taiwan, to evaluate satisfiablity and feasibility of eAsthmaCare system. The proposed project has been approved by Institutional Review Board of CGH-LK (IRB No. 100-3083A3).
2. Design and Development
The Web-based healthcare and self-management system emphasizes the interactive interfaces for patients, physicians, and professionals to provide remote healthcare services through Internet and avoid burdens of clinical care requiring long distance and duration. In the proposed program, the asthmatic children and their parents would be educated to manage chronic disease with the assistant interface including (1) online asthma diary, (2) remote
asthma assessment, (3) instantaneous asthma alert, (4) asthma health education, and by communicating physicians with (5) diagrammatical clinic support. Herein, the developed system should be able to achieve these multi-disciplinary scopes.
2.1 Infrastructure Design
The design of the proposed asthma e-Healthcare system obeys the model-view-controller (MVC) design pattern [44] to collaborate five mutually supportive tiers (i.e. monitoring, communication, management, analysis, and database) which support healthcare resources reciprocally for patients, physicians, professionals, researchers, and system administrators. The system is programmed by the open-source JavaTM Servlet/JSP technology with reusable
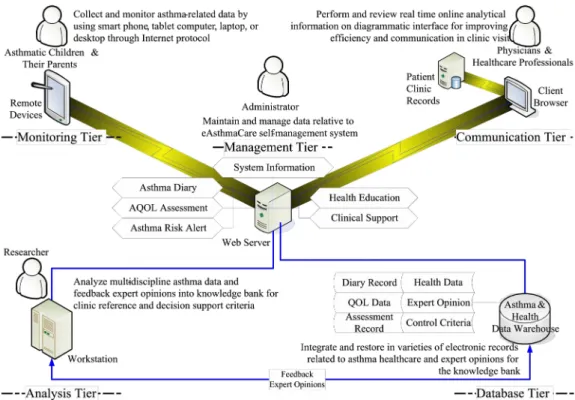
functions, thus the infrastructure is illustrated in Figure 1 followed by detailed description.
Figure 1 Five-tier infrastructure of Web-based e-Healthcare system for children with asthma A. Monitoring Tier. The tier is mainly designed for asthmatic children and their parents to record self-management data. It provides friendly graphical user interface (GUI) for them to collect asthma-related outcomes by using desktop, laptop, tablet computer, or even smart phone through Internet protocol. Meanwhile, the healthcare staffs are allowed to trace asthma
symptoms and conditions of patients. The portal of asthma diary is an entry of routine monitoring and can be examined by assessments for asthma quality of life (AQOL).
B. Communication Tier. The tier is generally established for healthcare professionals and physicians to review electronic health records. It performs interactive components with real time online analytical information on a diagrammatic interface. Through the evident-based diagrammatical interface, communications between physicians and patients can be efficiently improved in clinic visit. Thus the asthma information for self-management can be compared with patient’s clinical records reported by hospital information system.
C. Management Tier. The tier is the center of the infrastructure for system administrators to control necessary electronic resources and varied user privilege. It requires information technique (IT) related to Web services (WS) and software knowledge to maintain and manage the asthma e-healthcare data including asthma diary, AQOL assessment, asthma risk alert, health education, and clinical support records.
D. Analysis Tier. The tier is essentially cooperated with researchers who are experts in asthma studies. It offers them a channel at the backend to feedback expert opinions into the knowledge bank for delivering clinic reference and decision support criteria beyond data analysis. The researchers can compute multi-discipline data through professional software to deliver their expertise for consultants.
E. Database Tier. The tier is usually founded as the base of a knowledge bank storing all asthma healthcare data. It restores a variety of system data and electronic records related to asthma healthcare and expert opinions. Prior to building the knowledge bank, the system is allowed to integrates modules of data query and data mining with auto accessing procedures in daemon for progressing advanced statistics and instantaneous online computation.
2.2 Database Design
According to this MVC-based architecture, a main approach of online analytical process (OLAP) for healthcare informatics can be anticipated. The OLAP mechanism has been widely
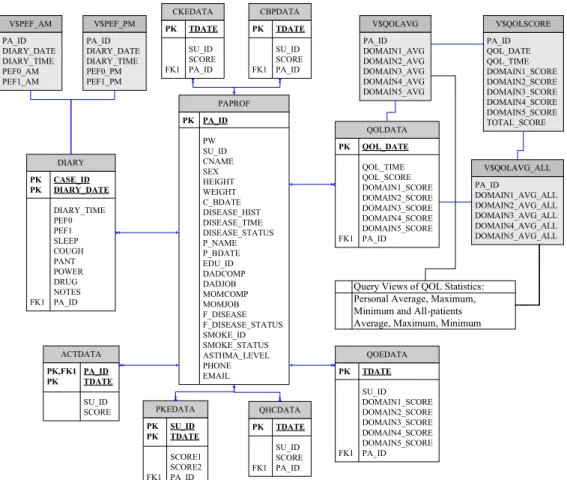
utilized for decision support systems because of offering immediate and online computation algorithms by mining data warehouse [45][46]. Therefore, a well-designed health care data warehouse (HCDW) can fully support the OLAP portal of proposed asthma e-Healthcare system for analyzing complicated data. In this study, we created the foundation of HCDW model by planning a main fact table for health profiles of patients and dimension tables for records of asthma diary and assessments. Thus, the derivative dimensions were schemed by queries corresponding to statistical data from diary and assessment tables. The prototype of HCDW database model as shown in Figure 2 illustrates a star-type schema based on the entity relationship diagram (ERD) of database. Herein, we employed the built-in database functions, which are dynamic view, stored procedure and trigger to control dataflow inside the HCDW. The database transaction scripts are compliant with OracleTM or MySQLTM database and were
pre-stored to enable automatic procedures while integrating diverse data transformation.
DIARY PK CASE_ID PK DIARY_DATE DIARY_TIME PEF0 PEF1 SLEEP COUGH PANT POWER DRUG NOTES FK1 PA_ID QOLDATA PK QOL_DATE QOL_TIME QOL_SCORE DOMAIN1_SCORE DOMAIN2_SCORE DOMAIN3_SCORE DOMAIN4_SCORE DOMAIN5_SCORE FK1 PA_ID QOEDATA PK TDATE SU_ID DOMAIN1_SCORE DOMAIN2_SCORE DOMAIN3_SCORE DOMAIN4_SCORE DOMAIN5_SCORE FK1 PA_ID ACTDATA PK,FK1 PA_ID PK TDATE SU_ID SCORE CKEDATA PK TDATE SU_ID SCORE FK1 PA_ID QHCDATA PK TDATE SU_ID SCORE FK1 PA_ID CBPDATA PK TDATE SU_ID SCORE FK1 PA_ID PKEDATA PK SU_ID PK TDATE SCORE1 SCORE2 FK1 PA_ID V$PEF_AM PA_ID DIARY_DATE DIARY_TIME PEF0_AM PEF1_AM V$QOLSCORE PA_ID QOL_DATE QOL_TIME DOMAIN1_SCORE DOMAIN2_SCORE DOMAIN3_SCORE DOMAIN4_SCORE DOMAIN5_SCORE TOTAL_SCORE V$QOLAVG PA_ID DOMAIN1_AVG DOMAIN2_AVG DOMAIN3_AVG DOMAIN4_AVG DOMAIN5_AVG V$QOLAVG_ALL PA_ID DOMAIN1_AVG_ALL DOMAIN2_AVG_ALL DOMAIN3_AVG_ALL DOMAIN4_AVG_ALL DOMAIN5_AVG_ALL V$PEF_PM PA_ID DIARY_DATE DIARY_TIME PEF0_PM PEF1_PM
Query Views of QOL Statistics: Personal Average, Maximum, Minimum and All-patients Average, Maximum, Minimum
PAPROF PK PA_ID PW SU_ID CNAME SEX HEIGHT WEIGHT C_BDATE DISEASE_HIST DISEASE_TIME DISEASE_STATUS P_NAME P_BDATE EDU_ID DADCOMP DADJOB MOMCOMP MOMJOB F_DISEASE F_DISEASE_STATUS SMOKE_ID SMOKE_STATUS ASTHMA_LEVEL PHONE EMAIL
In the schema, the main fact table “PAPROF” restores personal health data of asthmatic children and their parents that include basic personal data, disease history and status of family members, education degree, and asthma factors. In addition, due to the design, the attributes denote (a) patient’s identification (PA_ID) that is a primary key to control all dimension tables; (b) patient’s birthday (C_BDATE), sex, and height that affect the threshold of asthma control test (i.e. ACTDATA table); (c) disease factors named with “DISEASE,” “SMOKE,” “ASTHMA,” etc. that adapt with relations of AQOL assessments and asthma diary (i.e. QOLDATA and DIARY); (d) the prefixes “EDU_,” “DAD_,” and “MOM_” etc. that imply patient’s and parent’s education for evaluating healthcare knowledge and self-management ability assessments scored in tables of QHEDATA, PKEDATA, CKEDATA, and CBPDATA (i.e. quality of healthcare education, parent's knowledge evaluation, children knowledge evaluation, and children behavior process, respectively).
Furthermore, the gray entities named by prefix V$ mean the query views obtained from three kinds of built-in database functions. The DIARY table provides twice-daily PEF data (measured in both of the morning and evening) while the QOLDATA table contains multi-domain AQOL scores (measured in every several months). They both can be applied for investigation with respect to daily averages and statistical information. Therefore the views of V$PEF_AM and V$PEF_PM give queries about average of PEFs in the morning and evening. Thus V$QOLAVG and V$QOLAVG_ALL are the views queried for average AQOL domain scores of individuals and all-patients, respectively, and similar to computation of other domain scores for presenting the maximum and minimum values. Particularly, these query views can be integrated with the AQOLDATA table to carry out total scores immediately for each domain so that synthetic cross-comparison can be engaged in OLAP functionality.
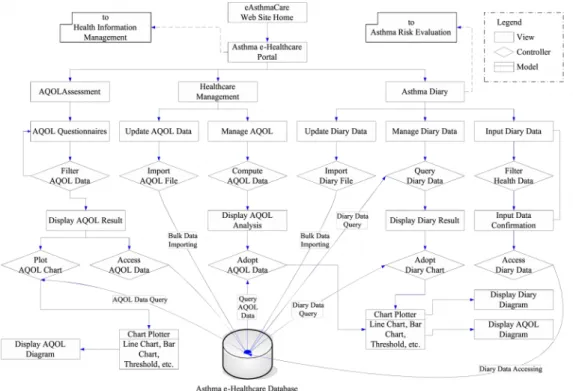
The interactive interface was developed upon an MVC-based architecture, which consists of reusable and extractable components for mutually functional supports, to achieve the five primary scopes of self-management. Figure 3 demonstrates objective dataflow of system data transportation with respect to operation relationships of major components as the roles in “model,” “view,” and “controller” based on the MVC design pattern.
Figure 3 Objective dataflow of eAsthmaCare data transportation: (a) Asthma diary, AQOL assessment, and healthcare management interfaces
(b) Asthma risk evaluation and health information management interfaces
Herein, Figure 3(a) presents that the portions under asthma e-Healthcare portal imply the scopes to patients’ asthma diary, AQOL assessment and healthcare management with diagrammatical clinical support; thus 3(b) shows other parts corresponding to managing risk evaluation and health information. In which, the rectangle blocks represent the view-related components while the double-square and the rhombus blocks stand for the model- and controller-related components, respectively. The developed components are addressed below by following proposed scopes.
(1) Online asthma diary: As considering the daily PEF report, children with asthma were asked to record their asthma conditions twice every day through the online asthma diary page. The diary components are functionally separated by data input, update, and management. The data input function requests the PEF values, asthma symptoms and medicine records entered by patients in the morning and evening every day. If patients could not finish entries because of the personal reasons such as travel, off network, etc., they were able to compose the diary
later by data update function for bulk loading the electronic records with specific data format. In addition, the interface offers management functions for healthcare users to query and review diary data. The controller components “Filter Health Data,” “Import Diary File,” and “Query Diary Data” will transmit dataflow of correspondent interfaces into the correct process. As managing data input or data query, a view page of result for confirming progression will be displayed before accessing database or performing online diagrams. Furthermore, the model component “Chart Plotter” is created for the chart functions of Web-based diagrams that can be recruited by other long-term monitoring programs. For instance of the rehabilitation care, the daily rehabilitation activity record is similar to asthma diary and the diary-related model can be modified for suitable format of input data.
(2) Remote asthma assessment: The 35-question ARQOL questionnaire is adopted as the main AQOL assessment for evaluating quality of life of the asthmatic children. This approved questionnaire involves five domains such as “influence of symptoms in life,” “influence of asthma in life,” “influence of asthma during social learning,” “management of asthma control,” and “influence of emotion upon relationship with parents,” during the past four weeks. Additionally, we designed other questionnaires for assessing the influences in health condition and home environment with respect to AQOL. Similar to the diary entry procedure, the interface of AQOL assessment employs the controller component to filter AQOL data (or users’ answers) and display AQOL results on the view page; then, further confirmation is validated prior to data access in database. Herein, assessment questions are formatted in WS-enabled files to reduce frequency of database access and increase flexibility of maintenance. Because of the “Chart Plotter” model, the assessment diagrams can be presented on Web sites remotely for evaluating asthma and healthcare information.
(3) Instantaneous asthma alert: The “Asthma Threshold” model is the core component of asthma risk evaluation to support criteria as processing “Check Threshold” controller.
Behind displaying the history of health outcomes derived from the asthma diary, the evaluation interface induces the “Risk Compute” controller to analyze asthma-related data by retrieving the database reciprocally for online calculation or manual statistics. This process stands for the feedback of the expert opinions towards the database for updating the risk threshold. Similar to traditional asthma control test (ACT) alert in red, yellow, or green indication, the controller uses the “Chart Plotter” model to highlight the risk zones on the diagram for instantaneous asthma alert. The function can be further adaptive with short message service (SMS) programs to inform healthcare staffs at emergent moment.
(4) Asthma health education: The interface of health information management extends the portal of asthma e-Healthcare system to provide information of personal health and education for patients and their families. The health profile stores necessary asthma-related data including family disease history and parent’s education level. Herein, the “Health Information” model offers general health information data by linking with the “Access Health Data” controller to educate patients and their family. Besides, three types of questionnaires are designed to assess children behaviors in managing asthma symptoms and to investigate asthma awareness of children and their parents after learning the health information. The format of questionnaire files is identical to AQOL assessment which requires filtering and accessing processes to ensure correct data entries of the eAsthmaCare database.
(5) Diagrammatical clinic support: The physicians or healthcare professionals are authorized to track AQOL assessment reports and asthma diaries of patients through the interface of healthcare management. When patients complete the assessment, the “Compute AQOL Data” controller will provide OLAP functions to display analytical results on the view page. The “Adopt AQOL Data” controller searches database and performs these diagrams with the help of the “Chart Plotter” model. Meanwhile, the components can crossly compare asthma diary data with designed “query view” (the database function mentioned above) for
decision support. Then, the authorized people can study either AQOL or PEF variations on the online diagrams in clinic visits. Furthermore, the healthcare professionals can help the patients who are inconvenient for online assessment to update their AQOL data. The “Import AQOL File” controller can assist in importing bulk data to update database.
The proposed asthma e-Health system provides a login portal to assign permission to various users for operating authorized Web pages. Meanwhile, the user-friendly interface with “keep in simple, stupid (KISS)” design for non-IT users is scoped to decrease complexity and increase feasibility of the system.
3. Implementation and Presentation
In this section, we present the major functional pages to prove the self-developed system and explain the intervention procedure to the participant patients for further discussion.
3.1 Practice of Functionality
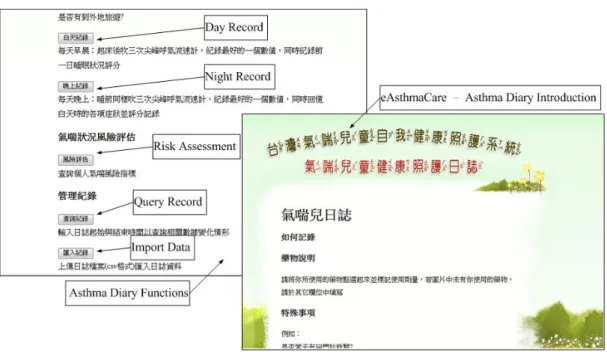
The self-management functions of eAsthmaCare are shown in the serial figures (a) to (f) of Figure 4. Figure 4(a) presents the portal of asthma diary with functional KISS interface that includes readable introductions with Chinese phonetic notations for the school-age children and simple function-oriented page with clear browser layout for the uses. Figure 4(b) shows the main form of asthma diary input interface while the entry results notice primary PEF data as well as traceable asthma risk indexes and medicine information for healthcare requirement. In which, the index indicates status of sleep, cough, pant, and activity power scaled by the value of 1(occurrence), 0(none) or -1(no entry). The history of diary records is shown in Figure 4(c) that can compare daily PEF values (in dash line) with relative asthma symptom risk indexes. Meanwhile, the indexes with daily PEFs can provide three-level risk and four-level severity information for critical asthma alert diagrams as shown in Figure 4(d).
Furthermore, the online assessment interface helps healthcare professionals to remotely collect responses of participant patients and to immediately obtain analytical results in cross
comparison with all patients. The result page and score diagram as shown in Figure 4(e) list the evaluation date and duration; in the meantime, five-domain AQOL scores of assessment are also displayed on the bar chart. Figure 4(f) performs two types of comparative diagrams that the multiple bar charts compare current personal AQOL scores with average, maximum, and minimum values of the past AQOL scores of the individual; thus, the bar-line chart evaluates the current personal AQOL versus statistics of the AQOL scores of all patients.
Figure 4 Implementation of diagrammatic interfaces of the eAsthmaCare system (a) KISS interface of asthma diary portal and function-oriented page
(b) Input interface corresponding to entry results of asthma diary
(d) Level-based critical alerts in asthma risk and severity
(f) Online AQOL assessment and real time cross-comparison diagrams
The proposed system was finally integrated with hospital information system as the part of the Pediatric Department of CGH-LK. In order to ensure continuous update of knowledge, the online education for asthma health information was hence engaged with hospital web site in Chinese (http://www1.cgmh.org.tw/chldhos/intr/c4a80/06index001-1-01.htm) that is related to pediatric asthma healthcare.
3.2 Practice of Intervention
The self-developed eAsthmaCare system was transferred into the computer center of CGH-LK in July 2011 for security tuning and database immigration prior to adaption of the hospital information system. The authorized web and database servers are Apache TomcatTM 6
and Oracle 8iTM, respectively. After one-month in-site test, the system was published on the
website "http://www.cgmh.org.tw:8056/eAsthmaCare/" in August 2011 for forty-one children and their parents to begin the asthma self-management project. The voluntary participants were intervened in using the eAsthmaCare system to manage and report their health condition
till February 2012. They measured their PEF twice in the morning and evening daily while two PEF values (before and after taking drugs) are required for each measurement to record the asthma diary in eAsthmaCare. Meanwhile, they were asked to input medicine and symptom conditions for asthma control monitored by healthcare professionals. Besides of routine records, they would report their quality of life by filling up online AQOL assessment and reply other evaluations regarding knowledge of asthma management every three months. In order to encourage patients to use the online diary, they would get awards due to the diary score that accumulates a point for each daily record entry.
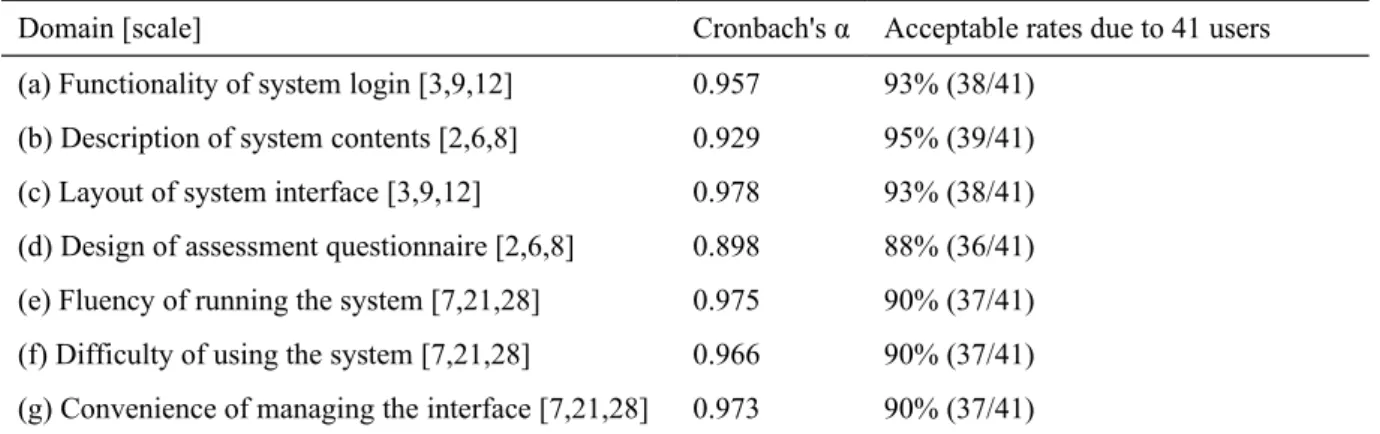
Table 1 Reliability test for assessments of satisfiability on using eAsthmaCare Domain [scale] Cronbach's α Acceptable rates due to 41 users (a) Functionality of system login [3,9,12] 0.957 93% (38/41)
(b) Description of system contents [2,6,8] 0.929 95% (39/41) (c) Layout of system interface [3,9,12] 0.978 93% (38/41) (d) Design of assessment questionnaire [2,6,8] 0.898 88% (36/41) (e) Fluency of running the system [7,21,28] 0.975 90% (37/41) (f) Difficulty of using the system [7,21,28] 0.966 90% (37/41) (g) Convenience of managing the interface [7,21,28] 0.973 90% (37/41)
Average α: 0.979; Low reliability: α<0.35; General reliability: 0.35≤α<0.7; High reliability: α>0.7;
[scale]: [min points, threshold, max points], each question in a domain is given by 1, 2, 3, 4 points for very agreeable, agreeable, not very agreeable but acceptable, and very disagreeable, respectively
In order to evaluate user’s satisfiability in system performance, we studied the reliability of seven-domain questionnaire inspected by Cronbach’s α test. The results in Table 1 shows that thirty-three questions were all approved by average of α reaching 0.979 while reliability of each domain was qualified by the criterion (i.e. α > 0.7). Thus, we would like to discuss the responses of patients about their experiences in using the eAsthmaCare system.
4. Results and Discussion
The past study had contributed practical discussions as facilitating guideline system with computerized methods for feasible approaches of asthma healthcare and management in the
clinical department [47]. In order to understand feasibility of the developed system, we evaluated eight asthma-related variables with respect to seven domains (ordered by (a) to (g) in Table 1) of satisfiability while using eAsthmaCare. Each domain gives some questions thus each question is scaled in range of 1 point to 4 points (i.e., very agreeable, agreeable, not very agreeable but acceptable, and very disagreeable). In this approach, the satisfiability of each domain will be acceptable if the average score is less than three fourths of the max scale (i.e., the threshold). For an example, scale of the three-questionnaire domain should be ranged between 3 and 12 thus the average score less than 9 (i.e., threshold) is satisfactory. It performs that the acceptable rates of 41 users for domain (a) to (g) approximately reach 93%, 95%, 93%, 88%, 90%, 90%, and 90% in order. In general, around 40-50% of the users completely agreed the developed functions but 5-10% of them did not feel convenient while using the system. Some participants responded valuable opinions regarding difficulties for operating the system and that will be discussed in later paragraphs. Besides, six groups of independent variables including (G1) sex of child, (G2) asthma outbreak due to emotional changes, (G3) parent’s age, (G4) child’s age, (G5) parent’s education level, and (G6) severity level of asthma, are examined by non-parametric statistical hypothesis tests to study how feasible the system is for various user groups and illness conditions.
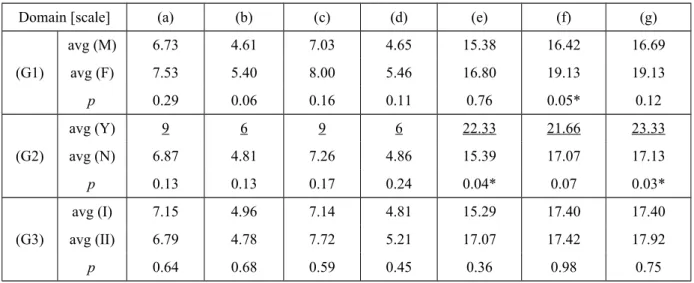
Table 2 Satisfiability on using eAsthmaCare related to six groups of independent variables
Domain [scale] (a) (b) (c) (d) (e) (f) (g)
(G1) avg (M) 6.73 4.61 7.03 4.65 15.38 16.42 16.69 avg (F) 7.53 5.40 8.00 5.46 16.80 19.13 19.13 p 0.29 0.06 0.16 0.11 0.76 0.05* 0.12 (G2) avg (Y) 9 6 9 6 22.33 21.66 23.33 avg (N) 6.87 4.81 7.26 4.86 15.39 17.07 17.13 p 0.13 0.13 0.17 0.24 0.04* 0.07 0.03* (G3) avg (I) 7.15 4.96 7.14 4.81 15.29 17.40 17.40 avg (II) 6.79 4.78 7.72 5.21 17.07 17.42 17.92 p 0.64 0.68 0.59 0.45 0.36 0.98 0.75
(G4) avg (7) 6.87 4.80 7.46 4.93 15.06 17.73 17.93 avg (8) 8.50 5.66 8.50 5.66 10.33 17.83 16.83 avg (9) 6.17 4.83 7.50 4.16 12.83 16.16 17.00 avg (10) 7.33 4.66 7.16 5.00 18.66 19.16 17.66 avg (11) 6.63 4.75 6.50 5.00 17.37 16.12 17.87 p 0.480 0.667 0.551 0.635 0.440 0.690 0.989 (G5) avg (H) 7.50 5.08 7.58 4.83 16.58 16.25 16.50 avg (P) 7.79 5.21 7.85 5.14 17.57 19.21 18.50 avg (U) 5.42 4.25 6.50 4.75 12.83 16.00 16.75 avg (G) 8.00 5.33 8.00 5.33 17.66 19.33 21.00 p 0.03* 0.22 0.38 0.89 0.17 0.15 0.42 (G6) avg (L) 7.11 4.92 7.47 4.86 16.00 17.50 17.50 avg (M) 4.50 4.00 5.00 6.00 15.00 14.00 17.50 avg (S) 9.00 6.00 9.00 6.00 14.00 21.00 21.00 p 0.27 0.44 0.20 0.50 0.92 0.38 0.79 Notes:
G1: Sex of child (Male/Female); G2: Is asthma breakout due to emotional changes? (Yes/No) G3: Parent's age (I:41-50 years old, II:51-60 years old); G4: Child’s age from 7 to 11 years old; G5: Parent’s education level, H = high school, P = professional school, U = bachelor by university, G = master or doctor by graduate school; G6: Severity of children asthma, L = light intermittent asthma, M = light continuous asthma, S = severe continuous asthma; p = p-value in statistics, where, *p<0.05; avg = average points in statistics;
Avg with underline: identical to or under the acceptable threshold
According to the results shown in Table 2, most of the variables indicate that average values of the groups in each domain are not over the acceptable thresholds of satisfiability scales. It implies the participant patients would like to accept the asthma e-Healthcare services for daily self-management of the disease. Some of they probably had difficulties or never experienced in using a novel Web-based system due to age level, but the group (G3) and (G4) show no significant difference to operate the simple-design interface. However, due to the threshold data with underline in group (G6), the system could not completely satisfy the users who have asthma outbreak due to emotional changes or are severe in asthma status. Furthermore, a significant difference (i.e. p≤0.05) can be found in group (G1) for domain (f) (p=0.05), and group (G2) for (e) (p=0.04), (g) (p=0.03). It infers that the children in various
sexes have various difficulties in using the system. Fluency of running the system and convenience of managing the interface are both domains affected by the children with asthma in emotional changes. Particularly, age and severity of children as well as age and education level of parents do not respond any significant differences in fluency of running the system, difficulty of operating the system, and convenience of managing the interface (i.e., the domain (e), (f), (g)). We learned that the health conditions and sexes of children probably effect their attempt to enforce self-management capabilities through the eAsthmaCare system.
Regarding those unsatisfactory returns, we shared the experiences with the participants, including patients, physicians and healthcare professionals, through the routine healthcare seminars for problem solving. The discussion discovered positive and negative feedback that can be referred to the past studies for improving patient-physician communication and chronic illness care [48]-[50]. The positive groups were aware of advantages of healthcare in self-management by monitoring asthma data routinely and remotely with the Web-based e-Healthcare system that offers online query and statistics of health informatics from hospital. The physicians and healthcare professionals were benefited by realizing more detailed morbidity of patients because of real-time online analytical and diagrammatical reports. However, the opposite groups revealed a few thinkable difficulties. For example, the children usually felt uncomfortable when finishing the diary under supervision of parents (otherwise they would rather play online game); the parents, who were under heavy daily workloads, wanted pure diary input but against the management interface with complicated functions; the patients, who were used to managing records and were familiar with paper diary, had barrier to accept new technique. Both of groups provided supportive suggestions for continuous development.
In summary, the use of the proposed asthma e-Healthcare system was feasible to help the asthmatic children and their parents to enhance capability of self-management for monitoring
health conditions. Thus, the system design would be upgraded by more user-friendly interface for convenient mobile devices in future study to eliminate the discussed conflicts and improve the practical strategy.
5. Conclusion Remarks
In this study, we designed a Web-based self-management system, eAsthmaCare, on e-Healthcare services for the children with asthma in Taiwan. The system was constructed by five-tier framework with real time clinical decision support functions for immediate online analyses by asthma diary, QOL assessment and health educations. Five multi-disciplinary portions, including online asthma diary, remote asthma assessment, instantaneous asthma alert, asthma health education, and diagrammatical clinic support, were created by online diagram in an expandable infrastructure. Details of the design and development methodology are explained in this paper, thus the diagrammatical interfaces are performed as the results. The proposed system was implemented in hospital to examine satisfiability and feasibility of the self-management functions. Thus, an assessment of satisfiability within the using system was offered for approving the development. As a result, the average scores of seven domains were scaled in the acceptable range to ensure feasibility of the system. In conclusion, the developed system can enhance healthcare in self-management for asthmatic children and their parents.
Authors and Contributions
Hsueh-Chun Lin: conceived of the study, and contributed in system design, development and manuscript writing.
Li-Chi Chiang: collaborated to advise the graduate student for professional studies and plan the healthcare schedule.
Tzu-Ning Wen: interacted with patients to collect the clinical data and perform the statistical analysis.
Kuo-Wei Yeh: participated in the clinical practice integration and consulted the knowledge of asthma medicine and healthcare.
Jing-Long Huang (corresponding author): coordinated the hospital and institution for the research program and consulted the medical informatics in pediatrics.
Acknowledgement
The authors would like to appreciate the research support from the Ministry of Science and Technology (former National Science Council) in Taiwan with the Grant numbered NSC 100-2625-M-039-001 and NSC 101-2625-M-039-001.
Conflict of interest statement
None declared
References
[1] World Health Organization, Global surveillance, prevention and control of chronic respiratory diseases: a comprehensive approach (2007). [online] http://www.who.int/gard/publications/GARD_Manual/en/index.html
[2] M. Masoli, D. Fabian, S. Holt, R. Beasley, GINA Program, The global burden of asthma: executive summary of the GINA Dissemination Committee Report. 59 Allergy. (2004) 469–478. [online] http://www.ginasthma.org/reports-global-burden-of-asthma.html) [3] N.M. Clark, C.H. Feldman, D. Evans, M.J. Levison, Y. Wasilewski, R.B. Mellins, The
impact of health education on frequency and cost of health care use by low income children with asthma. 78(1 Part 1) J. Allergy and Clinical Immunology. (1986) 108–115 [4] M.S. Blaiss, Outcomes analysis in asthma. 278 JAMA. (1997) 1874–1880.
[5] K.-H. Hsieh, J.-J. Shen, Prevalence of Childhood Asthma in Taipei, Taiwan, and Other Asian Pacific Countries. 25(2) J. Asthma. (1988) 73-82.
[6] L. J. Akinbami, K. C. Schoendorf, Trends in Childhood Asthma: Prevalence, Health Care Utilization, and Mortality. 110(2) Pediatrics. (2002) 315-322.
[7] J.A. Blackman, M.J. Gurka, Developmental and Behavioral Comorbidities of Asthma in Children. 28(2) J. Developmental & Behavioral Pediatrics. (2007) 92-99.
[8] M.I. Asher, U. Keil, H.R. Anderson, R. Beasley, J. Crane, F. Martinez, E.A. Mitchell, N. Pearce, B. Sibbald, A.W. Stewart and et al., International Study of Asthma and Allergies in Childhood (ISAAC): rationale and methods. 8(3) Europ. Respirat. J. (1995) 483-491. [9] L.M. Bell, R. Grundmeier, R. Localio, J. Zorc, A.G. Fiks, X. Zhang, T. B. Stephens, M.
Swietlik, J.P. Guevara, Electronic Health Record-Based Decision Support to Improve Asthma Care: A Cluster-Randomized Trial. 125(4) Pediatrics. (2010) e770-e777.
[10] C.C Kao, J.L. Huang, L.S. Ou, L.C. See, The prevalence severity and seasonal variation of asthma, rhinitis and eczema in Taiwan schoolchildren. 16(5) Pediatric Allergy Immunology. (2005) 408-415.
[11] D.-C. Yan, L.-S. Ou, T.-L. Tsai, W.-F. Wu, J.-L. Huang, Prevalence and severity of symptoms of asthma, rhinitis, and eczema in 13- to 14-year-old children in Taipei, Taiwan. 95(6) Annals of Allergy, Asthma & Immunology. (2005) 579–585.
[12] M.-F. Liao, J.-L. Huang, L.-C. Chiang, F.-Y. Wang, C.-Y. Chen, Prevalence of Asthma, Rhinitis, and Eczema from ISAAC Survey of Schoolchildren in Central Taiwan. 42(10) J. Asthma. (2005) 833-837.
[13] L.-C. Chiang, Y.-H. Chen, K.-C. Hsueh, J.-L. Huang, Prevalence and Severity of Symptoms of Asthma, Allergic Rhinitis, and Eczema in 10- to 15-Year-Old Schoolchildren in Central Taiwan. 25 Asian Pacific J. Allergy and Immunol. (2007) 1-5. [14] B.P. Yawn, S.K. Brenneman, F.C. Allen-Ramey, M.D. Cabana, and L.E. Markson,
Assessment of Asthma Severity and Asthma Control in Children. 118(1) Pediatrics. (2006) 322-329.
[15] K. Lorig, D.S. Sobel, A.L. Stewart, B.W. Jr. Brown, A. Bandura, P. Ritter, V.M. Gonzalez, D.D. Laurent, H.R. Holman, Evidence Suggesting That a Chronic Disease Self-Management Program Can Improve Health Status While Reducing Hospitalization: A Randomized Trial. 37(1) Medical Care. (1999) 5-14.
[16] T. Bodenheimer, K. Lorig, H. Holman, K. Grumbach, Patient Self-management of Chronic Disease in Primary Care. 288(19) JAMA. (2002) 2469-2475.
[17] K.R. Lorig, H.R. Holman, Self-management education: History, definition, outcomes, and mechanisms. 26(1), Annals of Behavioral Medicine. (2003) 1-7.
[18] S. Tousman, H. Zeitz, L.D. Taylor, C. Bristol, Development, Implementation and Evaluation of a New Adult Asthma Self-Management Program. 24(4) J. Community Health Nursing. (2007) 237-251.
[19] E.S. Ford, D.M. Mannino, D.M. Homa, C.Gwynn, S.C. Redd, D.G. Moriarty, A.H. Mokdad, Self-Reported Asthma and Health-Related Quality of Life: Findings From the Behavioral Risk Factor Surveillance System. 123(1) Chest. (2003) 119 - 127.
[20] N. Connolly, S. Godfreym, Assessment of the Child With Asthma. 8(1) J. Asthma Research. (1970) 31-36.
[21] P.V. Burkhart, J.M. Dunbar-Jacob, J.M. Rohay, Accuracy of children's self-reported adherence to treatment. 33(1) J. Nursing Scholarship. (2001) 27-32.
[22] W.M. Vollmer, L.E. Markson, E. O’Connor, E. Ann Franzier, M. Berger, A. Sonia Buist, Association of Asthma Control with Health Care Utilization. 165 American Journal of Respiratory Critical Care Medicine. (2002) 195–199.
[23] C.-M.I. UGent, K. Desager, R.D.K. Ugent, Fractional order model parameters for the respiratory input impedance in healthy and in asthmatic children. 101(3) Computer Methods and Programs in Biomedicine. (2011) 315-323.
[24] D. Wensley, M. Silverman, Peak Flow Monitoring for guided self-management in childhood asthma. 170 American J. Respiratory Critical Care Medicine. (2004) 606-612. [25] P.V. Burkhart, M. Kay Rayens, M.G. Oakley, D.A. Abshire, M. Zhang, Testing an
Intervention to Promote Children's Adherence to Asthma Self-Management. 39(2) J. Nursing Scholarship. (2007) 133–140.
[26] S. Guendelman, K. Meade, M. Benson, Y.Q. Chen, S. Samuels, Improving Asthma Outcomes and Self-management Behaviors of Inner-city Children: A Randomized Trial of the Health Buddy Interactive Device and an Asthma Diary. 156(2) Archive of Pediatrics & Adolescent Medicine. (2002) 114 - 120.
[27] D.S. Chan, C.W. Callahan, S.J. Sheets, C.N. Moreno, F.J. Malone, An internet-based store-and-forward video home telehealth system for improving asthma outcomes in children. 60(1) American Journal of Health-System Pharmacy. (2003) 1976-1981.
[28] D. Giansanti, S. Morelli, G. Maccioni, M. Brocco, Design, construction and validation of a portable care system for the daily telerehabiliatation of gait. 112(1) Computer Methods and Programs in Biomedicine. (2013) 146-155.
[29] J.L.G. Perales, Development of a new software for comprehensive management and traceability of hospital radiopharmacies. 112(1) Computer Methods and Programs in Biomedicine. (2013) 166-172.
[30] V. Rialle, J.-B. Lamy, N. Noury, L. Bajolle, Telemonitoring of patients at home: a software agent approach. 72(3) Computer Methods and Programs in Biomedicine. (2003) 257-268.
[31] D.S. Chan, C.W. Callahan, V.B. Hatch-Pigott, A. Lawless, H.L. Proffitt, N.E. Manning, M. Schweikert, F.J. Malone, Internet-based home monitoring and education of children with asthma is comparable to ideal office-based care: results of a 1-year asthma in-home monitoring trial. 119(3) Pediatrics. (2007) 569-78.
[32] H. Meischke, P. Lozano, C. Zhou, M.M. Garrison, D. Christakis, Engagement in “My Child's Asthma”, an interactive web-based pediatric asthma management intervention. 80(11) International Journal of Medical Informatics. (2011) 765-774.
[33] J.W. Dexheimer, T.J. Abramo, D.H. Arnold, K.B. Johnson, Y. Shyr, F. Ye, K.-H. Fan, N. Patel, D. Aronsky, An asthma management system in a pediatric emergency department. 82(4) International Journal of Medical Informatics. (2013) 230-238.
[34] A.M. Patel, Using the Internet in the management of asthma. 7(1) Current Opinion in Pulmonary Medicine. (2001) 39-42.
[35] M.E. Mansour, B.P. Lanphear, T.G. DeWitt, Barriers to Asthma Care in Urban Children: Parent Perspectives. 106(3) Pediatrics. (2000) 512-519.
[36] L.G Kun, Telehealth and the global health network in the 21st century. From homecare to public health informatics. 64(3) Computer Methods and Programs in Biomedicine. (2001) 155-167.
[37] L.-C. Chiang, J.-L. Huang, J.-L., S.-Y. Chao, A comparison by quantitative and qualitative methods, between the self-management behaviors of parents with asthmatic children in two hospitals. 13(2) J. Nursing Research. (2005) 85-96.
[38] V. van der Meer, H.F. van Stel, S.B. Detmar, W. Otten, P.J. Sterk, J.K. Sont, Internet-Based Self-Management Offers an Opportunity to Achieve Better Asthma Control in Adolescents. 132(1) Chest. (2007) 112 - 119.
[39] T.-N. Wen, H.-C. Lin, J.-L. Huang, L.-C. Chiang, An Internet-Based Self-Management Program on Children with Asthma. 19(4) Changhua Nursing. (2012) 25-32.
[40] R.-L. Jan, J.-Y. Wang, M.-C. Huang, S.-M. Tseng, H.-J. Su, L.-F. Liu, An Internet-Based Interactive Telemonitoring System for Improving Childhood Asthma Outcomes in Taiwan. 13(3) Telemedicine and e-Health. (2007) 257-268.
[41] H.-C. Lin, H.-C. Wu, C.-H. Chang, T.-C. Li, W.-M. Liang, J.-Y. Wang, Development of a Real-Time Clinical Decision Support System upon the Web MVC-based Architecture for Prostate Cancer Treatment. 11(16) BMC Med. Informatics and Decision Making. (2011).
[42] H.-C. Lin, H.-C. Wu, C.-H. Chang, T.-C. Li, W.-M. Liang, C.-Y. Wang, A Real Time Online Assessment System with Modelized Architecture on Clinical Infometrics for Patient Reported Outcomes of Prostate Cancer. 106(3) Computer Methods and Programs in Biomedicine. (2012) 249-259.
[43] L.-C. Chiang, L.-F. Tzeng, L.-S. Fu, J.-L. Huang, Testing a questionnaire to measure asthma-related quality of life among children. 38(4) J. Nurs. Scholarsh. (2006) 383-386. [44] E. Gamma, R. Helm, R. Johnson, J. Vlissides, Design Patterns: Elements of Reusable
Object-Oriented Software. Addison-Wesley. (1994).
[45] S. Chaudhuri, U. Dayal, An Overview of Data Warehousing and OLAP Technology. 26 ACM SIGMOD Record. (1997) 65-74.
[46] C.-H. Lee, J.C.-Y. Chen, V.S. Tseng, A novel data mining mechanism considering bio-signal and environmental data with applications on asthma monitoring. 101(1) Computer Methods and Programs in Biomedicine. (2011) 44-61.
[47] D.L. Sanders, W. Gregg, D. Aronsky, Identifying asthma exacerbations in a pediatric emergency department: A feasibility study. 76(7) Int’l J. Medical Informatics. (2007) 557-564.
[48] S.B. Detmar, M.J. Muller, J.H. Schornagel, L.D.V. Wever, N.K. Aaronson, Health-related quality-of-life assessments and patient-physician communication: a randomized controlled trial. 288(23) JAMA. (2002), 3027-3034.
[49] E.H. Wagner, B.T. Austin, C. Davis, M. Hindmarsh, J. Schaefer, A. Bonomi, Improving Chronic Illness Care: Translating Evidence Into Action. 20(6) Health Affairs (2001) 64-78.
[50] C.K.L. Or, B.-T. Karsh, A Systematic Review of Patient Acceptance of Consumer Health Information Technology. 16(4) J. Am. Med. Inform. Assoc. (2009) 550-560 doi: 10.1197/jamia.M2888