Maternal employment and atopic dermatitis in children: A
prospective cohort study
I.J. Wang,*†‡# H.J Wen,§ T.L. Chiang,∥ S.J. Lin, ¶ P.C. ChenΨ and Y.L. Guo§
* Department of Pediatrics, Taipei Hospital, Department of Health, Taipei, Taiwan; † College of Public Health, China Medical University, Taichung, Taiwan;
‡ National Yang-Ming University, Taipei, Taiwan; # Fu Jen Catholic University, Taipei, Taiwan;
§ Department of Environmental and Occupational Medicine, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei, Taiwan
∥Institute of Health Policy and Management, National Taiwan University College of Public Health, Taipei, Taiwan
¶ Department of Pediatrics, National Cheng Kung University Hospital and College of Medicine, National Cheng Kung University, Tainan, Taiwan
ΨInstitute of Occupational Medicine and Industrial Hygiene, National Taiwan University College of Public Health, Taipei, Taiwan
P.C. Chen and Y.L. Guo contributed equally to this article
Running title: Maternal employment and atopic dermatitis
Keywords: atopic dermatitis, pregnancy,employment, occupational exposure Manuscript word: 2654
Table counts: 5
Funding sources: This study was supported by grants from the Bureau of Health Promotion Department of Health (BHP-PHRC-92-4, DOH93-HP-1702) and the National Science Council of Taiwan (NSC 98-2314-B-192 -001-MY3).
Conflicts of interest: None declared. What's already known about this topic?
Whether maternal occupations affect the development of atopic disorders in children remains to be elucidated.
What does this study add?
In addition to work stress during pregnancy, working in professional or technical occupations increased the risk of childhood atopic dermatitis.
Avoiding occupational exposure for pregnant women is important for prevention of atopic disorders in children.
Correspondence: Professor Pau-Chung Chen and Yueliang Leon Guo E-mail: [email protected]; [email protected]
Summary
Background Considering the early onset of atopic dermatitis (AD) which most often arises in the first year of life, risk factors occurring very early in life must be considered. Little is known about the effects of maternal occupational exposure on the development of atopic disorders in children. Objectives The aim of this study was to evaluate associations between maternal employment and childhood AD.
Methods We used multistage stratified systematic sampling to recruit 24,200 mother-newborn pairs from the Taiwan national birth register. Maternal occupation categories, work stress, working time, shift work, and potential confounders during pregnancy were gathered by questionnaires after birth. At 3 years of age, information on the development of AD was assessed via home interviews.
Multiple logistic regression analysis was performed to estimate the association of maternal employment and AD.
Results Overall, 11,962 (61.72%) mothers worked during pregnancy. The children of mothers who worked during pregnancy had an increased risk of AD compared to those whose mothers did not work (OR=1.38, 95%CI=1.25-1.53). The children of mothers with a professional or technical occupation had a higher risk of AD (OR=1.64, 95%CI=1.44-1.87). The risk of AD was found to increase with maternal work stress during pregnancy in a dose-response-manner (p for trend<0.01). The mothers of children with AD had a longer working time than those without AD (p<0.0001). However, no significant association between AD and maternal shift work was found.
Conclusions Working in professional or technical occupations increased the risk of childhood AD in addition to work stress during pregnancy. Ease working conditions and prevent occupational exposure is important for pregnant women.
Introduction
The prevalence of allergic diseases appears to have increased dramatically over the past decade.1 The pathogenesis of allergic diseases is complex and not entirely understood. Considering the early onset of many childhood allergic diseases, and in particular atopic dermatitis (AD) which most often arises in the first year of life, risk factors occurring very early in life must be considered.The prenatal environment can affect the development of the fetus during critical periods of exposure, with a permanent effect in later years.2 This condition is called fetal programming of adult diseases. Programming agents include growth factors, cytokines and hormones, all of which can be altered by stress.3 As a consequence, such stress-modified systems of the offspring are more susceptible to environmental exposure and the development of diseases during later life.
The employment rate for married women and mothers with young children has risen sharply since the mid-1970s.4 Ever-increasing competition and occupational demands affect women to a growing extent. Women who remain in their jobs at childbearing age have an increased potential occupational exposure to chemical, physical, and biological agents as well as to physical exertion and psychosocial stress. Maternal working conditions during pregnancy are considered to be associated with birth outcome in their children.5 Furthermore, certain occupations with a high hapten and irritant chemical exposure during pregnancy are significantly associated with atopic disorders in the offspring.6 Elevated risks of childhood asthma have been reported to be related to occupational groups such as bakers, needleworkers, and dental assistants, who may be exposed to agents commonly associated with occupational asthma.6 At present, over 250 work related agents have been reported to cause allergies, a number of them by inducing IgE mediated responses.7
Whether the increasing employment rate or occupational exposure for pregnant women is linked to the unfavorable trend of atopy prevalence in recent decades is not clear.8 Little is known about maternal occupational exposure that occurs prenatally as a risk factor for childhood atopic disorders. Moreover, data obtained from women are scanty, because psychoneuroimmunologic research has traditionally included more men than women. Since AD is the first step of atopic march, we wanted to explore the effects of maternal employment during pregnancy on the
Methods
Study population and sampling strategy
The Taiwan Birth Cohort Study is a national prospective longitudinal cohort study. In this study, we used a multistage stratified systematic sampling design to obtain representative samples from the Taiwan national birth registration data in 2005. We categorized a total of 369 towns in Taiwan into 12 strata according to the administrative division (four strata) and the total fertility rate (three strata). Using the principle of probability proportional to size, we randomly sampled 90 out of the 369 towns. A total of 24,200 pairs of mothers and newborns from these 90 towns were recruited. All study participants provided written informed consent. The study protocol was approved by the institutional review board of National Taiwan University and complied with the principles outlined in the Helsinki Declaration.
We then conducted home interviews with the postpartum women 6 and 36 months after delivery using a structured questionnaire as previously described.9,10A total of 2,952 cases were lost to follow-up because of refusal to participate, relocation, incorrect addresses, infant deaths, and others. After excluding subjects that were loss to follow-up, these cases, 21,248 postpartum women were interviewed when their children were 6 months of age, and the completed interview rate was thus 87.8%. We then excluded multiple gestations (N = 561) (twins, triples, etc.), and 1306 cases that were lost to follow-up during interviews when the children were 36 months of age. Other exclusion criteria included the inability to answer questions in Chinese, and plans to move out of the area after delivery,. A a final total of 19,381 participants (80.1%) were included in this study (Fig. 1). All study participants provided written informed consent. The study protocol was approved by the institutional review board of National Taiwan University and complied with the principles outlined in the Helsinki Declaration.
Exposure
industry, work stress, work schedule, working days per week, working hours per day, and working hours per week. The type of occupation was classified into six groups: professional, technical; administrative, managerial; superintendents, clerical; sales; fabricators, operators, etc.; and others according to the Taiwan Standard Occupational and Industrial Classification system.11 The type of industry was divided into six groups: manufacturing, construction, mining; wholesale and retail trade; personal services; public administration and defense; professional services; and others.11 The work stress was measured through the question, “How much stress did you feel when working during pregnancy? Very high, high, intermediate, low, or not at all.”
Outcomes
Cases of AD were defined as physician-diagnosed AD through the question, “Have you ever been informed by a doctor that your child has eczema?’’ The questionnaire-diagnosed AD was defined as, “Has your child ever had a recurrent itchy rash for at least 6 consecutive half-month periods over the elbows, knees, face, wrists, neck, periauricular and eyebrow areas during his/her lifetime?’’ according to the International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire via home interviews.10
Potential confounders
Questions about potential confounders and prenatal and postnatal risk factors were asked when the children were 6 months of age, including maternal age at delivery, education, ethnicity, family income, maternal history of atopy, maternal smoking or drinking during pregnancy, diet and supplements during pregnancy, duration of breast feeding, age of introduction of solid foods, number of siblings, day care, owning pets, carpets at home, environmental tobacco smoke, fungi on the walls of the residence, and place of residence. From the records of the collaborating hospitals, we collected neonatal health data at birth, including gender, head circumference, birth body weight, height, weeks of gestation, parity, type of delivery, and vaccination history.
Statistical analysis
For the association between maternal employment status and AD in children, odds ratios (ORs) with 95% confidence intervals (95% CIs) were calculated by logistic regression models. For the effect of working time during pregnancy on AD in children, value SE was also calculated by logistic regression models. Analyses were performed in both univariate and multivariate models. Potential confounders were taken into consideration. Variables were included in the model if they changed the univariate point estimate by at least 10%. All hypothesis testing was two-sided at the significance level of 0.05, and was performed using JMP statistical software version 5.0.1 (SAS Institute Inc., Cary, NC, U.S.A.).
Results
In total, 11,962(61.8 %) mothers worked during pregnancy. The prevalence rates of having questionnaire-diagnosed AD during the child’s lifetime and physician-diagnosed AD were 6.9%(1,340) and 10.5%(2,033), respectively. Among the mothers who were employed during pregnancy, 2,275(19.0%) were in the professional and technical group, 1,456(12.2%) in
administrative and managerial, 5,036(42.2%) in superintendents and clerical, 948(7.9%) in sales, 1,345(11.3%) in fabricators and operators, and 887(7.4%) in others when classifying by occupation. When classifying by type of industry, 3,353(28.1%) were in the manufacturing, construction, and mining group, 3,135(26.3%) in wholesale and retail trade, 1,502(12.6%) in personal services, 406(3.4%) in public administration and defense, 3,191(26.7%) in professional services, and
359(3.0%) in others. As to the scale of workplace, 5,288(44.2%) had fewer than 30 employees and 6,620(55.4%) had more than 30 employees.
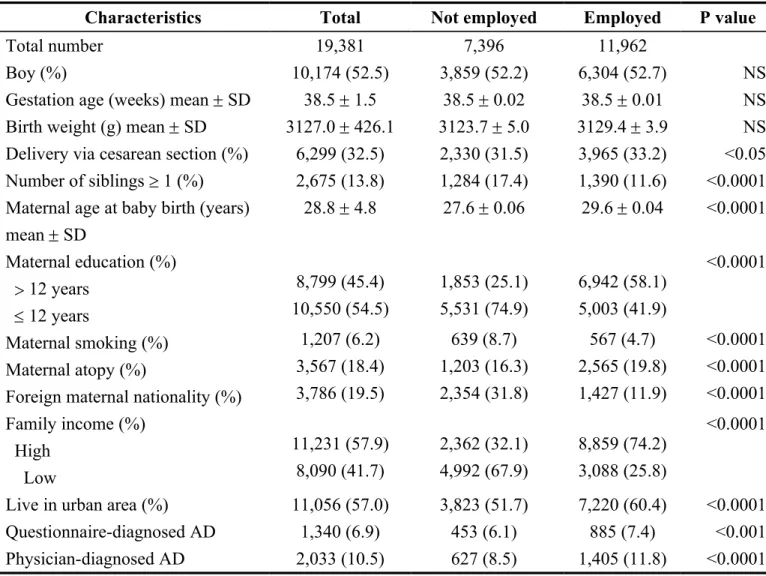
The children of mothers who were employed tended to have questionnaire-diagnosed AD, physician-diagnosed AD, be delivered via cesarean section, have fewer siblings, live in urban areas, and have a higher family income. The mothers who were employed were older at the birth of their baby, received a higher education and had a higher atopy history, but a lower prevalence of smoking and foreign nationality than those who were not employed (Table 1).
The children of the mothers who worked during pregnancy had an increased risk of physician-diagnosed AD compared to those whose mothers did not work (OR=1.38, 95%CI=1.25-1.53), after adjusting for gender, maternal atopy, maternal education level, maternal smoking, family income, number of siblings, and residence location (Table 2). Within the occupational category, the children of mothers with professional or technical, and administrative or managerial, and superintendent and clerical occupations had a higher risk of childhood physician-diagnosed AD (OR=1.64,
95%CI=1.42-1.90; OR= 1.52, 95%CI= 1.27-1.81; OR=1.59, 95%CI= 1.42-1.79) and questionnaire-diagnosed AD (OR=1.34, 95%CI=1.13-1.60; OR= 1.32, 95%CI= 1.07-1.63; OR=1.26, 95%CI= 1.09-1.45) (Table 2). As for the category of industry, an increased risk of questionnaire- and physician-diagnosis AD was found for the children whose mothers work involved professional
services (OR=1.31, 95%CI=1.12-1.54; OR= 1.64, 95%CI= 1.44-1.87). The risk of questionnaire- and physician-diagnosed AD was found to increase with maternal work stress during pregnancy in a dose-response-manner after adjusting for potential confounders (p for trend<0.01) (Table 2).
However, no significant association between AD and maternal night or shift work during pregnancy was found.
The mothers of the children with physician-diagnosed AD had longer working days per week and working hours per day than those without AD (p<0.0001) (Table 3). The same results were found for children with questionnaire-diagnosed AD, although not all factors were statistically significant. After adjusting for potential confounders, working days per week and working hours per day were positively associated with the risk of physician-diagnosed AD [β (S.E.) = 0.0428 (0.009); 0.0308 (0.006)].
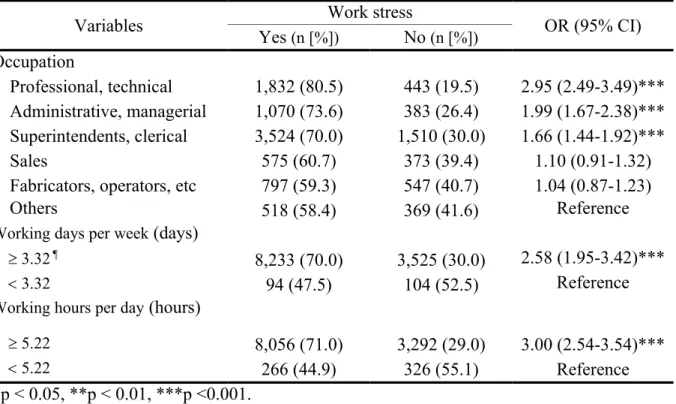
Pregnant women with professional or technical occupations and administrative or managerial occupations had higher work stress than other fields (OR=2.95, 95%CI=2.49-3.49) (Table 4). A longer working days per week and working hours per day were also correlated with higher work stress (OR=2.58, 95%CI=1.95-3.42; OR=3.00, 95%CI=2.54-3.54). Since maternal professional
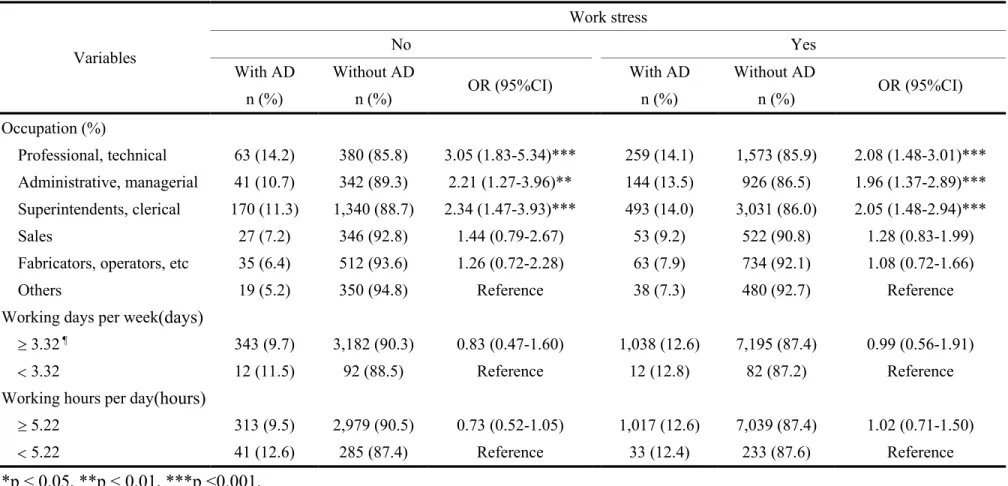
occupation, high work stress, and long working time were related to an increased risk of childhood atopic disorders, and since work stress may be correlated with the other two risk factors, we further investigated whether work stress alone could account for all of the effect on atopic disorders. After stratification by work stress, the effect of job category on AD still existed (OR=3.05, 95%CI=1.83-5.34 for those without work stress). However, the effect of longer working time on AD disappeared (Table 5).
Discussion
Associations between mothers who work and atopic diseases among their offspring have not been previously reported, and thus merit further investigation. In our study, significant associations between childhood AD and maternal employment status and occupational category were found. In addition, the risk of AD was found to increase with maternal work stress and working time during pregnancy. After stratification by maternal work stress, the effect of occupational category on AD still existed, however, the effect of working time on AD disappeared. Therefore, maternal
occupational category was the risk factor for childhood AD in addition to work stress. This study adds important knowledge to the fact that maternal occupational exposure during pregnancy have significant effects on the development of atopic disorders in their offspring.
We found that the children of mothers who worked during pregnancy had an increased risk of AD compared to those whose mothers did not work. With the increased participation of fertile women in working life, this increase may be due to working conditions having an impact on
reproductive health. The general stress of combining family life and household responsibilities with a full time job can also have a negative impact on daily well being, particularly during pregnancy. Several studies have reported that the children of working women have higher risks of developing asthma, which may result from a high physical workload and psychological stress.3,12,13
Consistent with a survey from Statistics Canada, which reported that most employed women work in traditionally female jobs including nursing and health-related occupations, we found that the most two common maternal occupation groups were the superintendents or clerical groups and professional or technical groups.4 Interestingly, we observed that the children of the mothers with professional or technical occupations had a higher risk of AD. A possible explanation is that mothers with professional or technical occupations may have an increased exposure to certain allergens or chemicals, leading to atopic disorders in their offspring.6,8 It is consistent with the ‘hapten-atopy’ hypothesis, which postulates that increased hapten and irritant chemical exposure during maternal pregnancy when there is already a natural tendency to Th2 immunological bias contributes to the subsequent development of atopic disorders in children.14 Work-related
exposures were reported to be associated with AD.15 Occupational exposure to gas, dust or fumes appeared to be a strong risk factor for AD.16 It is interesting that cooking with wood and biomass has also shown an increased risk for AD, further emphasizing the influence of environmental exposures.17 In addition, more and more studies have reported associations between prenatal exposure to environmental chemicals and childhood atopic disorders.18,19 Prenatal exposure to organic solvents may confer immune modulation or program the immune function, and increase the risk of allergic manifestations.20 Therefore, it is reasonable that maternal occupational exposures may contribute to a Th1/Th2 imbalance in pregnancy and lead to the development of atopic diseases.21
We found that the risk of AD increased with maternal work stress during pregnancy in a dose-response-manner. Exposure to stress during pregnancy has been reported to be associated with an increased risk of respiratory and skin diseases in the offspring, and to be related with elevated cord blood IgE and the change of Th1/Th2 balance.22,23 In our previous study, maternal nerve growth factor levels during pregnancy, a kind of stress related neuropeptide, were significantly higher in AD children compared with controls.24 It has also been reported that maternal stress during pregnancy is associated with alterations of blood cortisol responses, a stress related hormone, measured 10 years later in preadolescent children.25 Maternal stress may affect fetal immune development either through hormonal regulation of fetal genes or through modification of placental and uterine functions.25 Another possible mechanism for a prenatal programming effect is through epigenetic regulation of the glucocorticoid receptor gene. Emerging evidence suggests that
environmental variables may alter methylation profiles of other genes of relevance to atopic diseases, opening the possibility that maternal stress may operate through direct epigenetic effects, as well as indirect effects mediated through neuroendocrine dysregulation.26 By these mechanisms, prenatal stress may lead to reprogramming or imprinting of the two stress pathways (hypothalamic– pituitary–adrenal axis and the sympathetic nervous system), which modulate immune function and lead to increased vulnerability to allergies.27
that women who work more than 50 hours a week without taking antenatal leave from work tend to have small-for-gestational-age births.28 However, the effect of maternal working time on childhood AD disappeared after stratification by work stress in our study. Shift work is associated with hormonal disturbances through changes in circadian rhythm and stress, affecting fetal
development.29 A slightly raised odds ratio for asthma was observed in the children of shift workers in one study.6 However, most studies investigating the effect of work schedule on the reproductive health of women have reached equivocal conclusions.30 Although no associations between work schedules and AD in children were established in our study, public health concerns and the previously reported data warrant continued research.
There are limitations to our study. First, we used occupational groups to assess exposure. This probably results in potential non-differential misclassification of job exposure due to differences in work tasks within the groups. A classification of occupations according to allergen or chemical exposure would have been of interest, however, occupational grouping by exposure was not feasible for such a large epidemiological study. Furthermore, standard occupational and industrial
classification system of occupational grouping for exposure assessment has previously been used in many epidemiological studies.5,31,32 Second, our study was limited by the use of questionnaires for ascertaining AD, which may not be as accurate as the standard diagnostic criteria used by a
dermatologist. Nevertheless, maternal reports of physician-diagnosed AD with typical morphology and atopic distribution have been validated versus clinical examinations in studies performed in the United States and Denmark, and have been used by many epidemiological studies.9,10,33,34
The strengths of our study include the large sample size and the population based prospective cohort design. Because of the large sample size, we were able to control for numerous potential confounders in the statistical analysis. The consistency across different outcome measures (questionnaire-diagnosed AD, physician-diagnosed AD) and the evidence for a dose-response relationship between work stress severity and AD raises the possibility that this association may be causal. Therefore, we are fairly confident about our results. In addition, this is the first contribution to the literature linking the association between different characteristics of prenatal maternal
employment exposure and subsequent AD development during childhood. Moreover, the multistage stratified systematic sampling including urban, suburban, and rural populations may enhance the generality. Since the follow-up rate was high, selection bias was not a major problem in our study. Finally, there were no significant differences in most of the variables in those lost to follow-up and in those who completed the followed-up.
In summary, working in professional or technical occupations increased the risk of childhood AD in addition to work stress during pregnancy. Since the intrauterine environment plays a pivotal role for health across life, transferring pregnant women to a safe work environment is important. As worldwide fertility rates continue to decrease, action must be taken by governments to ease working conditions and prevent exposure to occupational hazards for female workers, particularly during pregnancy. Further research should provide more insight into the magnitude of exposure
responsible for detrimental effects.There is an urgent need to further clarify which environmental exposures during pregnancy will influence the subsequent development of allergic diseases in children.
References
1. Yan DC, Ou LS, Tsai TL et al . Prevalence and severity of symptoms of asthma, rhinitis, and eczema in 13- to 14-year-old children in Taipei, Taiwan. Ann Allergy Asthma Immunol 2005;95:579-85.
2. Barker DJ. The fetal origins of adult disease. Proc Biol Sci 1995;262: 37–43.
3. Knackstedt MK, Hamelmann E, Arck PC. Mothers in stress: consequences for the offspring. Am J Reprod Immunol 2005;54:63-9.
4. McIntosh Jeff. Percentage of working mothers has doubled in 30 years: StatsCan. Canadian Press.
http://www.parentcentral.ca/parent/newsfeatures/article/904143--percentage-of-working-mothers-has-doubled-in-30-years-statscan Accessed 2012.
5. Herdt-Losavio ML, Lin S, Chapman BR, et al. Maternal occupation and the risk of birth defects: an overview from the National Birth Defects Prevention Study. Occup Environ Med 2010;67:58-66.
6.Magnusson LL, Wennborg H, Bonde JP et al. Wheezing, asthma, hay fever and atopic eczema in relation to maternal occupations in pregnancy. Occup Environ Med 2006; 63:640–6.
7.Chan-Yeung M, Malo JL. Occupational asthma. N Engl J Med 1995;333:107–12.
8. McFadden JP. The great atopic diseases epidemic: does chemical exposure play a role? Br J Dermatol 2012;166:1156-7.
9. Wang IJ, Guo YL, Weng HJ et al. Environmental risk factors for early infantile atopic dermatitis. Pediatr Allergy Immunol 2007;18:441-7.
10. Choi WJ, Ko JY, Kim JW et al. Prevalence and Risk Factors for Atopic Dermatitis: A Cross-sectional Study of 6,453 Korean Preschool Children. Acta Derm Venereol 2011. Nov 24. doi: 10.2340/00015555-1252. [Epub ahead of print]
11. Li CY, Chang KH, Feng CK et al. Inter-rater agreement on the classification of job titles. Chinese J Public Health 1999;18:255–61.
12. Ball TM, Anderson D, Minto J et al. Cortisol circadian rhythms and stress responses in infants at risk of allergic disease. J Allergy Clin Immunol 2006;117:306-11.
13. Barreto do Carmo MB, Neves Santos D, Alves Ferreira Amorim LD et al. Minor psychiatric disorders in mothers and asthma in children. Social Psychiatry Psychiatric Epidemiology
2009;44:416-20.
14. McFadden JP, Dearman RJ, White JML et al. The hapten-atopy hypothesis II: the ‘cutaneous hapten paradox’. Clin Exp Allergy 2011; 41:327–37.
15. Rönmark EP, Ekerljung L, Lötvall J et al. Eczema among adults: prevalence, risk factors and relation to airway diseases. Results from a large-scale population survey in Sweden. Br J Dermatol 2012;166:1301-1308.
16. Meding B, Ahman M, Karlberg AT. Skin symptoms and contact allergy in woodwork teachers. Contact dermatitis 1996; 34:185–90.
17. Kurt E, Metintas S, Basyigit I et al. Prevalence and Risk Factors of Allergies in Turkey (PARFAIT): results of a multicentre cross sectional study in adults. Eur Respir J 2009; 33:724–33.
18. Miller RL, Garfinkel R, Horton M et al. Polycyclic aromatic hydrocarbons, environmental tobacco smoke, and respiratory symptoms in an inner-city birth cohort. Chest 2004;126:1071–8. 19. Sherriff A, Farrow A, Golding J et al. Frequent use of chemical household products is
associated with persistent wheezing in pre-school age children. Thorax 2005;60:45–9.
20. McMartin KI, Chu M, Kopecky E et al. Pregnancy outcome following maternal organic solvent exposure: a meta-analysis of epidemiologic studies. Am J Ind Med 1998;34:288–92.
21. Warner JA. Primary sensitization in infants. Ann Allergy Asthma Immunol 1999;83:426–30. 22. Lin YC, Wen HJ, Lee YL et al. Are maternal psychosocial factors associated with cord
immunoglobulin E in addition to family atopic history and mother immunoglobulin E? Clin Exp Allergy 2004;34:548-54.
23. Tegethoff M, Greene N, Olsen J et al. Stress during pregnancy and offspring pediatric disease: A National Cohort. Environ Health Perspect 2011;119:1647-52.
24. Wang IJ, Hsieh WS, Guo YL et al. Neuro-mediators as predictors of pediatric atopic dermatitis. Clin Exp Allergy 2008;38:1302-8.
25. O'Connor T, Ben-Shlomo Y, Heron J et al. Prenatal anxiety predicts individual differences in cortisol in pre-adolescent children. Biol Psychiatry 2005;58:211–7.
26. Oberlander T.F, Weinberg J, Papsdorf M et al. Prenatal exposure to maternal depression, neonatal methylation of human glucocorticoid receptor gene (NR3C1) and infant cortisol stress responses. Epigenetics 2008;3:97–106.
27. Wright RJ. Stress and atopic disorders. J Allergy Clin Immunol 2005;116:1301–6.
28. Ceròn-Mireles P, Harlow SD, Sànchez-Carrillo CI. The risk of prematurity and small-for-gestational-age birth in Mexico city: the effects of working conditions and antenatal leave. Am J Public Health 1996;86:825-31.
29. Yamauch H, Iwamoto M, Harada N. Physiological effects of shift work on hospital nurses. J Hum Ergol 2001;30:251-4.
30. Nurminen T. Shift work and reproductive health. Scand J Work Environ Health 1998;24:28-34. 31. Chang PJ, Chu LC, Hsieh WS et al. Chuang YL, Lin SJ, Chen PC. Working hours and risk of
gestational hypertension and pre-eclampsia. Occup Med (Lond) 2010;60:66-71.
32. Stocks SJ, Turner S, McNamee R et al., Carder M, Hussey L, Agius RM. Occupation and work-related ill-health in UK construction workers. Occup Med (Lond) 2011;61:407-15.
33.Moore MM, Rifas-Shiman SL, Rich-Edwards JW et al. Perinatal predictors of atopic dermatitis occurring in the first six months of life. Pediatrics 2004;113:468-74.
34.Benn CS, Wohlfahrt J, Aaby P et al. Breastfeeding and risk of atopic dermatitis, by parental history of allergy, during the first 18 months of life. Am J Epidemiol 2004;160:217-23.
Table 1 Characteristics of the study subjects by maternal employment during pregnancy (n = 19,381)
Characteristics Total Not employed Employed P value
Total number 19,381 7,396 11,962
Boy (%) 10,174 (52.5) 3,859 (52.2) 6,304 (52.7) NS
Gestation age (weeks) mean SD 38.5 1.5 38.5 0.02 38.5 0.01 NS Birth weight (g) mean SD 3127.0 426.1 3123.7 5.0 3129.4 3.9 NS Delivery via cesarean section (%) 6,299 (32.5) 2,330 (31.5) 3,965 (33.2) <0.05 Number of siblings 1 (%) 2,675 (13.8) 1,284 (17.4) 1,390 (11.6) <0.0001 Maternal age at baby birth (years)
mean SD 28.8 4.8 27.6 0.06 29.6 0.04 <0.0001 Maternal education (%) 12 years 12 years 8,799 (45.4) 10,550 (54.5) 1,853 (25.1) 5,531 (74.9) 6,942 (58.1) 5,003 (41.9) <0.0001 Maternal smoking (%) 1,207 (6.2) 639 (8.7) 567 (4.7) <0.0001 Maternal atopy (%) 3,567 (18.4) 1,203 (16.3) 2,565 (19.8) <0.0001
Foreign maternal nationality (%) 3,786 (19.5) 2,354 (31.8) 1,427 (11.9) <0.0001 Family income (%) High Low 11,231 (57.9) 8,090 (41.7) 2,362 (32.1) 4,992 (67.9) 8,859 (74.2) 3,088 (25.8) <0.0001
Live in urban area (%) 11,056 (57.0) 3,823 (51.7) 7,220 (60.4) <0.0001
Questionnaire-diagnosed AD 1,340 (6.9) 453 (6.1) 885 (7.4) <0.001
Physician-diagnosed AD 2,033 (10.5) 627 (8.5) 1,405 (11.8) <0.0001 NS, not significant.
Table 2 The effect of maternal employment status and work stress during pregnancy on questionnaire- and physician-diagnosed AD in 3-year-old children (n = 19,381)
Factors (n) Questionnaire-diagnosed AD Physician-diagnosed AD
n (%) OR (95%CI) ¶ n (%) OR (95%CI) ¶ Employed Yes (11,962) No (7,396) 885 (7.4)453 (6.1) 1.18 (1.05-1.33)**Reference 1,405 (11.8)627 (8.5) 1.38 (1.25-1.53)***Reference Occupation Professional, technical (2,276) Administrative, managerial (1,456) Superintendents, clerical (5,036) Sales (948)
Fabricators, operators, etc. (1,346) Others (888) Non-employed (7,396) 198 (8.7) 120 (8.2) 394 (7.8) 49 (5.2) 79 (5.9) 45 (5.1) 453 (6.1) 1.34 (1.13-1.60)** 1.32 (1.07-1.63)** 1.26 (1.09-1.45)** 0.81 (0.59-1.08) 0.95 (0.74-1.21) 0.81 (0.58-1.10) Reference 322 (14.2) 185 (12.7) 663 (13.2) 80 (8.4) 98 (7.3) 57 (6.4) 627 (8.5) 1.64 (1.42-1.90)*** 1.52 (1.27-1.81)*** 1.59 (1.42-1.79)*** 0.96 (0.75-1.22) 0.84 (0.67-1.05) 0.73 (0.55-1.00) Reference Industry
Manufacturing, construction, mining (3,355) Wholesale and retail trade (3,135)
Personal service (1,502) Professional service (3,191)
Public administration and defense (406) Others (359) Non-employed (7,396) 234 (7.0) 230 (7.3) 100 (6.7) 271 (8.5) 27 (6.7) 22 (6.1) 453 (6.1) 1.14 (0.96-1.34) 1.17 (0.99-1.38) 1.06 (0.85-1.33) 1.31 (1.12-1.54)*** 1.06 (0.69-1.56) 1.01 (0.63-1.54) Reference 336 (10.0) 375 (12.0) 145 (9.7) 450 (14.1) 57 (14.0) 41 (11.4) 627 (8.5) 1.19 (1.03-1.37)* 1.42 (1.24-1.63)*** 1.12 (0.93-1.36) 1.64 (1.44-1.87)*** 1.72 (1.27-2.28)*** 1.41 (0.99-1.95)* Reference Work schedule Day (8,825) Night (308) Shift/All day (2,815) Non-employed (7,396) 687 (7.8) 19 (6.2) 177 (6.3) 453(6.1) 1.25 (1.01-1.41)* 1.04 (0.62-1.66) 0.98 (0.82-1.18) Reference 1,093 (12.4) 30 (9.7) 281 (10.0) 627 (8.5) 1.47 (1.33-1.63)* 1.04 (0.68-1.52) 1.14 (0.99-1.33) Reference Work stress Very high/high (4,386) Intermediate (3,941) Low/Not at all (3,629) 382 (8.7) 286 (7.3) 217 (6.0) 1.43 (1.20-1.70)*** 1.20 (1.00-1.45)* Reference 581 (13.3) 469 (11.9) 355 (9.8) 1.34 (1.16-1.54)*** 1.22 (1.05-1.41)** Reference ¶adjusted for gender, maternal atopy, maternal education level, maternal smoking, family income, number of siblings, and residence location.
Table 3 The effect of working time during pregnancy on questionnaire- and physician-diagnosed AD in 3-year-old children (n = 19,381)
Physician-diagnosed AD With (n = 2,032) Without (n = 17,323) p-value value SE ¶
Working days per week (days) mean SE 3.62 0.06 3.28 0.02 <0.0001 0.0428 0.009*** Working hours per day (hours) mean SE 5.80 0.10 5.16 0.03 <0.0001 0.0308 0.006*** Questionnaire-diagnosed AD With (n = 1,340) Without (n = 18,041)
Working days per week (days) mean SE 3.46 0.07 3.31 0.02 0.0514 0.0151 0.01
Working hours per day (hours) mean SE 5.58 0.12 5.20 0.03 0.0017 0.0165 0.007* ¶ adjusted for gender, maternal atopy, maternal education level, maternal smoking, family income, number of siblings, and residence location.
* p < 0.05, ** p < 0.01, *** p< 0.001.
Table 4 The effect of maternal occupations and working time during pregnancy on work stress
Variables Work stress OR (95% CI)
Yes (n [%]) No (n [%]) Occupation Professional, technical 1,832 (80.5) 443 (19.5) 2.95 (2.49-3.49)*** Administrative, managerial 1,070 (73.6) 383 (26.4) 1.99 (1.67-2.38)*** Superintendents, clerical 3,524 (70.0) 1,510 (30.0) 1.66 (1.44-1.92)*** Sales 575 (60.7) 373 (39.4) 1.10 (0.91-1.32)
Fabricators, operators, etc 797 (59.3) 547 (40.7) 1.04 (0.87-1.23)
Others 518 (58.4) 369 (41.6) Reference
Working days per week (days)
3.32 ¶ 8,233 (70.0) 3,525 (30.0) 2.58 (1.95-3.42)***
3.32 94 (47.5) 104 (52.5) Reference
Working hours per day (hours)
5.22 8,056 (71.0) 3,292 (29.0) 3.00 (2.54-3.54)***
5.22 266 (44.9) 326 (55.1) Reference *p < 0.05, **p < 0.01, ***p <0.001.
¶The cutoff value was the mean working time
Table 5 The effect of maternal occupations and working time during pregnancy on questionnaire- and physician-diagnosed AD in 3-year-old children after stratification by maternal work stress
Variables Work stress No Yes With AD n (%) Without AD n (%) OR (95%CI) With AD n (%) Without AD n (%) OR (95%CI) Occupation (%) Professional, technical 63 (14.2) 380 (85.8) 3.05 (1.83-5.34)*** 259 (14.1) 1,573 (85.9) 2.08 (1.48-3.01)*** Administrative, managerial 41 (10.7) 342 (89.3) 2.21 (1.27-3.96)** 144 (13.5) 926 (86.5) 1.96 (1.37-2.89)*** Superintendents, clerical 170 (11.3) 1,340 (88.7) 2.34 (1.47-3.93)*** 493 (14.0) 3,031 (86.0) 2.05 (1.48-2.94)*** Sales 27 (7.2) 346 (92.8) 1.44 (0.79-2.67) 53 (9.2) 522 (90.8) 1.28 (0.83-1.99) Fabricators, operators, etc 35 (6.4) 512 (93.6) 1.26 (0.72-2.28) 63 (7.9) 734 (92.1) 1.08 (0.72-1.66) Others 19 (5.2) 350 (94.8) Reference 38 (7.3) 480 (92.7) Reference Working days per week(days)
3.32 ¶ 343 (9.7) 3,182 (90.3) 0.83 (0.47-1.60) 1,038 (12.6) 7,195 (87.4) 0.99 (0.56-1.91)
3.32 12 (11.5) 92 (88.5) Reference 12 (12.8) 82 (87.2) Reference
Working hours per day(hours)
5.22 313 (9.5) 2,979 (90.5) 0.73 (0.52-1.05) 1,017 (12.6) 7,039 (87.4) 1.02 (0.71-1.50) 5.22 41 (12.6) 285 (87.4) Reference 33 (12.4) 233 (87.6) Reference
*p < 0.05, **p < 0.01, ***p <0.001.
¶The cutoff value was the mean working time