Journal of Microbiology, Immunology and Infection
Journal homepage: http://www.e-jmii.comMicrobiology, Infection Immunology
and
Indexed in MEDLINE/Index Medicus, SCIE, BIOSIS, EMBASE, Aidsline, CancerLit, Chemical Abstracts, HealthSTAR
The official journal of
Taiwan Society of Microbiology Chinese Society of Immunology The Infectious Diseases Society of Taiwan Taiwan Society of Parasitology
*Corresponding author. Division of Pediatric Infectious Disease, China Medical University Hospital, 2 Yuh Der Road, 40447 Taichung, Taiwan.
E-mail: [email protected]
†Shu-Yan Yang and Kao-Pin Hwang contributed equally to this work. Article History:
Received: Apr 20, 2010 Revised: May 1, 2010 Accepted: Jun 20, 2010
Original Article
Epidemiology and Clinical Peculiarities of Norovirus and
Rotavirus Infection in Hospitalized Young Children with
Acute Diarrhea in Taiwan, 2009
Shu-Yan Yanga†, Kao-Pin Hwanga,b*†, Fang-Tzy Wuc, Ho-Sheng Wuc, Chao Agnes Hsiungc, Wan-Chi Changd,
Jen-Shiou Line, Shun-Cheng Yange, Sun-Lin Huangf, Yhu-Chering Huangf
aDivision of Pediatric Infectious Disease, Department of Pediatrics, Chang Gung Memorial Hospital, Kaohsiung Medical Center,
Chang Gung University College of Medicine, Kaohsiung, Taiwan.
bDivision of Pediatric Infectious Disease, China Medical University Hospital, China Medical University School of Medicine,
Taichung, Taiwan.
cResearch and Diagnostics, Centers for Disease Control, Department of Health, Taiwan. dInstitute of Population Health Sciences, National Health Research Institute, Taiwan.
eDivision of Pediatric Infectious Disease and Department of Laboratory Medicine, Changhua Christian Hospital,
Changhua, Taiwan.
fDivision of Pediatric Infectious Disease, Chang Gung Children’s Hospital, Chang Gung University College of Medicine,
Taoyuan, Taiwan.
BACKGROUND/PURPOSE: Acute diarrhea is one of the most common morbidities in pediatrics world-wide. We conducted a study to investigate the incidence of norovirus in young children hospitalized with acute diarrhea in Taiwan and its clinical peculiarity compared with rotavirus gastroenteritis.
METHODS: Between January and December, 2009, patients younger than 5 years and admitted to hospital with acute diarrhea were randomly selected; and their stool samples were collected and tested for presence of rotavirus and norovirus by enzyme immunoassay and reverse transcription-polymerase chain reaction, respectively. The clinical manifestations and laboratory findings of the enrolled patients were analyzed.
RESULTS: A total of 989 cases were enrolled with a mean age of 21.6 ± 13.7 months and a male proportion
of 56.0%. Rotavirus and norovirus was detected in 20.2% and 14.6% of all patients, respectively. Genogroup II was the predominant strain of norovirus (80.6%). Children aged 6–36 months accounted for the majority of patients positive for rotavirus and norovirus (73.0% and 81.3%, respectively). The incidences of norovirus
Introduction
Acute diarrhea is one of the most common morbidities among pediatric patients worldwide. Because of easy access to medical services, acute gastroenteritis seldom causes mortality but it remains a significant disease burden for young children and an economic burden in industrial countries. In a questionnaire-based study conducted in Taiwan, 55.78% of children younger than 5 years had ex-perienced acute diarrhea, and the prevalence increased with age, ranging from 15.45% among infants less than 6 months of age to 82.22% among children aged 4–5 years.1
In a study of economic burden, families spent on average US$294 per month for a child admitted with rotavirus gastroenteritis, accounting for nearly 40% of the monthly salary of an unskilled or service worker.2
With the advancement of public health over the past two decades, viral agents have replaced bacteria as the leading cause of infectious diarrhea.3 As shown in a review about gastroenteritis in Taiwan, rotavirus is the leading cause (30.4–48.0%) of infectious gastroenteritis, followed by ad-enovirus (9.1–19.8%), norovirus (8.2–25.0%), astrovirus (2.7–2.9%) and enterovirus (< 5.2%).4 According to the
re-view on rotavirus and norovirus gastroenteritis published by the United States Centers for Disease Control and Prevention, rotavirus was estimated to cause 25 million clinic visits, 2 million hospitalizations and 352,000–592,000 deaths worldwide each year in children younger than 5 years.5 However, it was estimated that norovirus caused
900,000 clinic visits and 64,000 hospitalizations among children in developed countries and up to 200,000 deaths of children younger than 5 years in developing countries each year.6 In recent studies,3,7–9,14,15 norovirus was
recog-nized as the major infectious agent attributed to out-breaks and sporadic cases of infectious gastroenteritis.
Rotavirus has received considerable attention because it causes more severe clinical symptoms compared with other enteric viruses. Rotavirus is usually identified among nonbacterial gastroenteritis cases by enzyme immunoassay at most hospitals. In contrast, testing for norovirus is not routinely carried out because its clinical symptoms are less severe and testing methods are inefficient. With the increasing popularity of rotavirus vaccines, the incidence of rotavirus infection in patients hospitalized with diarrhea is estimated to have decreased, and the relative importance of norovirus infection is gradually rising.
Previous studies indicate that acute gastroenteritis mainly affected children younger than 5 years of age.10,11 Therefore,
we conducted a hospital-based (3 hospitals) study to in-vestigate the incidence of norovirus among young children hospitalized with acute diarrhea in Taiwan and to com-pare its clinical peculiarity and severity of symptoms with rotavirus gastroenteritis.
Methods
From January to December, 2009, a prospective observa-tional study was conducted in Taiwan; it included three med-ical centers located in the southern, northern and central regions of Taiwan. The hospitals were Chang-Gung Memorial Hospital, Kaohsiung Branch; Chang Gung Memorial Hos-pital, Linko Branch; and Changhua Christian Hospital. The protocol was approved by the local institution review boards of these three hospitals. Enrolled subjects were pa-tients less than 5 years of age, admitted to hospital with acute diarrhea. Diarrhea was defined as the passage of liquid or looser-than-normal stools occurring three or more times daily. Patients with diarrhea for more than 14 days were excluded. After obtaining informed parental consent, stool specimens and demographic information (including age, sex and rotavirus infection were higher during winter and early spring. Most patients with rotavirus and noro-virus diarrhea experienced vomiting (74.9% vs.74.8%, respectively) and fever (94.7% vs. 71.3%, respectively). CONCLUSION: Most young diarrheal patients presenting with vomiting were likely to have norovirus or rotavirus infection. Patients with norovirus diarrhea experienced an absence of, or low-grade fever and longer duration of vomiting compared with those positive for rotavirus infection. A family history of cur-rent gastroenteritis may suggest the possibility of norovirus infection.
and members living together with diarrhea and/or vomiting within 1 week), clinical manifestations (including diarrhea, vomiting, fever and associated upper respiratory symp-toms), and laboratory findings were collected and analyzed. A fecal sample was collected within the first 48 hours after admission and stored at 4ºC before testing. Each fecal sample was tested for the presence of rotavirus by en-zyme immunoassay (Ridascreen; γ − biopharm, Germany).12
The remaining stool specimen was kept frozen at –20ºC in the hospital until delivered to the laboratory at the Centers for Disease Control of Taiwan for norovirus testing by reverse transcription-polymerase chain reaction (RT-PCR) using two sets of PCR primers: G1SKF (5⬘-CTG CCC GAA TTY GTA AAT GA-3⬘) and G1SKR (5⬘-CCA ACC CAR CCA TTR TAC A-3⬘) for GI norovirus, and G2SKF (5⬘-CNT GGG AGG GCG ATC GCA A-3⬘) and G2SKR (5⬘-CCR CCN GCA TRH CCR TTR TAC AT-3⬘) for GII norovirus.13 Statistical analysis
Data were analyzed using SAS version 9.1 (SAS Inc., Cary, NC, USA). The results shown are given as the mean value with standard deviation (SD) or proportion. As for the com-parison of clinical manifestations and laboratory results among diarrheal patients, we categorized subjects into four subgroups according to the laboratory test results for rota-virus and nororota-virus. The percentages were compared using χ2 tests of homogeneity for the four subgroups and a
par-titioning of the χ2 method (Brunden, 1972) for specific
pair-wise comparisons. Kruskal–Wallis one-way analysis of variance by ranks and a multiple-comparison procedure
were used for testing the difference of ordinal variables among the four subgroups. The one-way analysis of variance method with the least significant difference procedure was applied to compare the difference of continuous mea-surements among the four subgroups. Statistical signifi-cance was defined as a p < 0.05 for two-tailed analysis in comparing overall groups and the least significant differ-ence procedure. For each pair-wise comparison, a p < α1 (at
an appropriate threshold) was conducted under a parti-tioning of the χ2 method (α
1 = 0.05/3) or the Kruskal–
Wallis multiple-comparison procedure (α1= 0.05/6).
Results
A total of 989 subjects were enrolled in the study, with a mean age of 21.6 ± 13.7 months and a male proportion of 56.0% (554/989). Children aged 6–36 months were at the highest risk of hospitalization with acute diarrhea (77.4%, 765/989) (Table 1). Overall, the detection rate of rotavirus was 20.2% (200/989) and that of norovirus was 14.6% (144/ 989). Among these patients, 29 cases were tested positive for both rotavirus and norovirus. Among patients positive for norovirus, 116 (80.6%) were genogroup II and 28 (19.4%) were genogroup I. Of the patients that were rotavirus positive, the most common G genotype was G1 (68.7%), followed by G3 (12.8%), G2 (8.0%), and the most common P genotype was P[8] (84.7%), followed by P[4] (9.2%).
No significant difference in the affected sex was found between the rotavirus positive and norovirus positive patient groups. The mean age of patients positive for rotavirus
Table 1. Age distribution of all diarrheal cases, rotavirus positive cases and norovirus positive cases from January to December, 2009
Features All AGE (n = 989) Rota (+) (n = 200) Noro (+) (n = 144)
Age (mo) Mean ± SD 21.6 ± 13.7 25.0 ± 14.6 21.3 ± 13.5 Median 17.7 21.3 17.1 Range (mo) 0–5 52 (5.3) 8 (4.0) 5 (3.5) 6–11 233 (23.6) 31 (15.5) 37 (25.7) 12–23 366 (37.0) 71 (35.5) 55 (38.2) 24–35 166 (16.8) 44 (22.0) 25 (17.4) 36–47 100 (10.1) 23 (11.5) 12 (8.3) 48–59 72 (7.3) 23 (11.5) 10 (6.9)
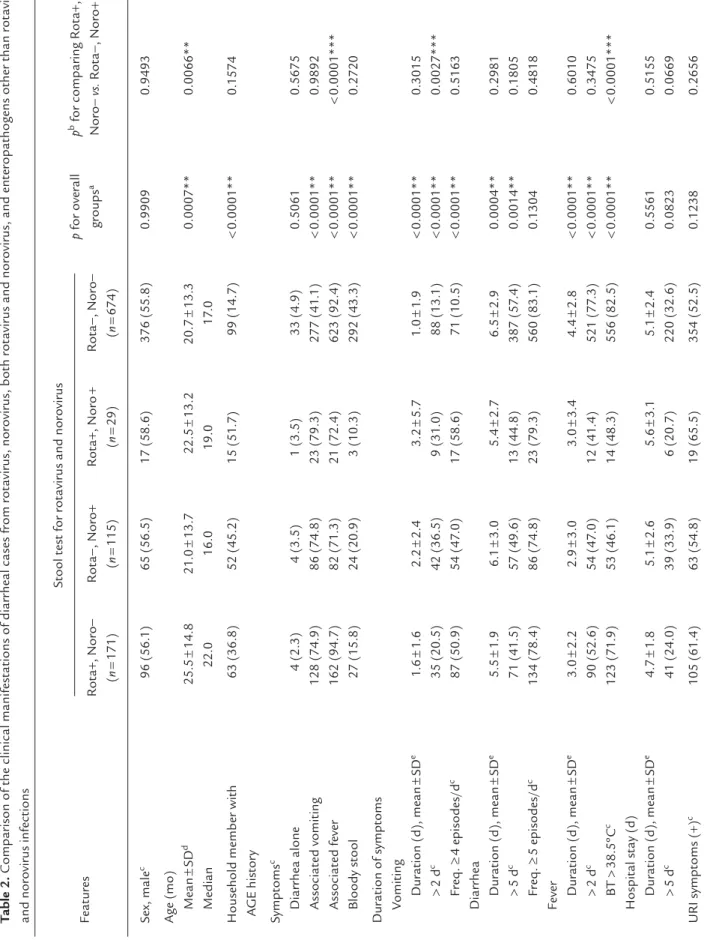
was older than that for norovirus (25.5 ± 14.6 months vs. 21.6 ± 13.7 months, p < 0.01). The cumulative age distribu-tion for rotavirus positive cases was 55.0% (n = 110) for pa-tients younger than 24 months and 77.0% (n = 154) in those younger than 36 months. For norovirus positive cases, 67.4% (n = 97) were younger than 24 months, and 84.7% (n = 122) were younger than 36 months. Compared with other groups of enteropathogens, the history of household members simultaneously suffering from diarrhea and/or vomiting within 1 week was more common among noro-virus and rotanoro-virus infection groups (p < 0.0001) (Table 2). The “other enteropathogens” group refers to those cases that were both rotavirus and norovirus negative.
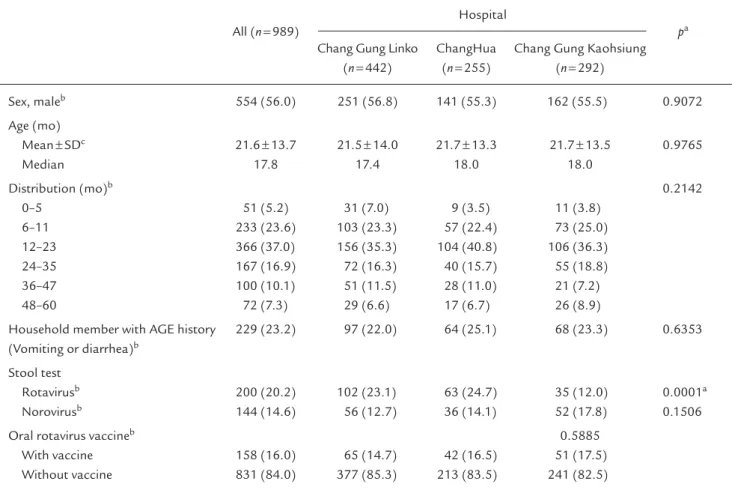
The incidence of rotavirus infection was higher in the northern and central regions of Taiwan compared with the southern region. However, the detection rate of norovi-rus infection was higher in the southern region (Table 3). The seasonal distribution of norovirus gastroenteritis was similar to that of rotavirus gastroenteritis, with higher prev-alence during the winter and early spring months (Figure). The prevalence of norovirus gastroenteritis was observed to peak in January, followed by a peak in rotavirus infections, which occurred in February.
Most patients with rotavirus or norovirus diarrhea ex-perienced vomiting (74.9% vs.74.8%, respectively), and the proportion was significantly higher than that of the other enteropathogens group (41.1%). Blood-tinged stools were rarely found in patients with either rotavirus or norovirus diarrhea compared with the other enteropathogens group. Fever was found more commonly in patients with rotavi-rus gastroenteritis than in those with norovirotavi-rus gastroen-teritis (94.7% vs. 71.3%) (Table 2). Concerning the severity of the clinical manifestations between norovirus and rotavi-rus gastroenteritis, more patients with norovirotavi-rus infection experienced a longer duration of vomiting than those with rotavirus infection, but the frequency of vomiting was not found to be significantly different in this study. There was also no difference between the norovirus and rotavirus infected groups with respect to clinical manifestations, including the duration and frequency of diarrhea, dura-tion of fever, and days of hospitalizadura-tion. Of the patients that were rotavirus and norovirus positive, the severity of clinical symptoms was similar to those infected with rota-virus or nororota-virus alone (Table 2). The leukocyte counts and C-reactive protein level in norovirus positive patients
were not significantly different from the rotavirus posi-tive cases. However, a greater number of patients infected with rotavirus were found elevated aspartate aminotrans-ferase levels compared with norovirus infected individuals (30.4% vs. 15.7%), but this difference was not significant (Table 2).
Discussion
In this study, norovirus was detected in 14.6% and rotavirus in 20.2% of all fecal samples. These results indicates that norovirus is a major viral pathogen, secondary to rotavirus, in younger children hospitalized with acute diarrhea in Taiwan. In recent studies,3,7–9,14,15 the increase in the inci-dence of norovirus infection, from 17.3–29.0%, were com-parable with our results. This may be because current testing methods are more sensitive; the incidence of norovirus de-tection nearly doubled when enzyme immunoassays were combined with the more sensitive RT-PCR, as previously proposed by Wu et al.7 Norovirus genogroup II was
pre-dominantly responsible for norovirus gastroenteritis world-wide as shown in most studies,7,8,13,14,16 and our findings are consistent with these results.
Rotavirus is the leading cause of acute gastroenteritis in children worldwide. The incidence of rotavirus gastro-enteritis (25–30%) in recent reports7,8,10,12 was decreased compared with the results of earlier studies,3,15,17–20 with a
range of 35–66%. The surveillance data reported by the Asian Rotavirus surveillance Network (ARSN) also confirm this trend.21,22 The most prevalent genotype was G1P [8] among rotavirus positive cases in our study, consistent with the report of ARSN.12 In the present study, the overall
detection rate of rotavirus (20.2%) was lower, and noticea-bly lower (12%) in the hospital from southern Taiwan. In fact, the detection rates of rotavirus for the two hospitals located in the northern and central regions of Taiwan (23.1% and 24.7%, respectively) in this study were close to the results from the Taiwan surveillance study (25%) of 2005–2007 and the results of other studies in recent years.12 A total of 158 cases from three hospitals received
an oral rotavirus vaccine, accounting for 16% of all cases in this study. The proportion of immunized children was approximately 20% of the eligible infants that received the vaccine in 2007.12 No difference was found between the
T
able 2.
Comparison of the clinical manif
est ations of diarr heal cases fr om r ot avirus, nor ovirus, both r ot
avirus and nor
ovirus, and ent
er
opathogens other than r
ot avirus and nor ovirus inf ections Stool t est f or r ot
avirus and nor
ovirus Rot a+ , Nor o− Rot a− , Nor o+ Rot a+ , Nor o + Rot a− , Nor o− p f or over all p b f or comparing Rot a+ , Featur es ( n = 171) (n = 115) (n = 29) (n = 674) gr oups a Nor o− vs. Rot a− , Nor o+ Se x, male c 96 (56. 1) 65 (56.5) 17 (58.6) 376 (55.8) 0.9909 0.9493
Age (mo) Mean
± SD d 25.5 ± 14.8 21 .0 ± 13.7 22.5 ± 13.2 20.7 ± 13.3 0.0007** 0.0066** Median 22.0 16.0 19.0 17 .0
Household member with
63 (36.8) 52 (45.2) 15 (51 .7) 99 (14.7) < 0.0001** 0. 1574 A GE histor y Symptoms c Diarr hea alone 4 (2.3) 4 (3.5) 1 (3.5) 33 (4.9) 0.5061 0.5675 Associat ed vomiting 128 (74.9) 86 (74.8) 23 (79.3) 277 (41 .1) < 0.0001** 0.9892 Associat ed f ever 162 (94.7) 82 (71 .3) 21 (72.4) 623 (92.4) < 0.0001** < 0.0001*** Bloody stool 27 (15.8) 24 (20.9) 3 (10.3) 292 (43.3) < 0.0001** 0.2720 Dur ation of symptoms V omiting Dur ation (d), mean ± SD e 1 .6 ± 1 .6 2.2 ± 2.4 3.2 ± 5.7 1 .0 ± 1 .9 < 0.0001** 0.3015 > 2 d c 35 (20.5) 42 (36.5) 9 (31 .0) 88 (13. 1) < 0.0001** 0.0027*** Fr eq. ≥ 4 episodes/d c 87 (50.9) 54 (47 .0) 17 (58.6) 71 (10.5) < 0.0001** 0.5163 Diarr hea Dur ation (d), mean ± SD e 5.5 ± 1 .9 6. 1 ± 3.0 5.4 ± 2.7 6.5 ± 2.9 0.0004** 0.2981 > 5 d c 71 (41 .5) 57 (49.6) 13 (44.8) 387 (57 .4) 0.0014** 0. 1805 Fr eq. ≥ 5 episodes/d c 134 (78.4) 86 (74.8) 23 (79.3) 560 (83. 1) 0. 1304 0.4818 Fever Dur ation (d), mean ± SD e 3.0 ± 2.2 2.9 ± 3.0 3.0 ± 3.4 4.4 ± 2.8 < 0.0001** 0.6010 > 2 d c 90 (52.6) 54 (47 .0) 12 (41 .4) 521 (77 .3) < 0.0001** 0.3475 BT > 38.5ºC c 123 (71 .9) 53 (46. 1) 14 (48.3) 556 (82.5) < 0.0001** < 0.0001*** Hospit al st ay (d) Dur ation (d), mean ± SD e 4.7 ± 1 .8 5. 1 ± 2.6 5.6 ± 3. 1 5. 1 ± 2.4 0.5561 0.5155 > 5 d c 41 (24.0) 39 (33.9) 6 (20.7) 220 (32.6) 0.0823 0.0669 URI symptoms ( +) c 105 (61 .4) 63 (54.8) 19 (65.5) 354 (52.5) 0. 1238 0.2656 (Contd )
hospitals (Table 3). Several studies found a higher preva-lence of rotavirus disease at colder temperatures, low rela-tive humidity and in dry weather.23–26 This may be because
families are more likely to stay indoors in cold weather, leading to an increase in contact transmission, with the dry conditions encouraging aerosol formation of virus-laden particles from a patient’s feces. The regional differences of incidence could possibly be the result of shorter colder months (January and February) and higher relative hu-midity (77–81%) in the southern regions compared with the climate of northern and central Taiwan (colder weather during January and April, relative humidity of 68–74%). In contrast, the incidence of norovirus infection was slightly higher in the southern region compared with the north-ern and central regions of Taiwan.
To the best of our knowledge, norovirus can be easily be transmitted via contaminated food or drinking water, lead-ing to diarrheal outbreaks. We speculate that this difference is probably due to poor hygiene as a higher proportion of grandparents serve as primary caregivers in southern Taiwan, likely increasing the risk of norovirus transmission.
Rotavirus is the leading cause of gastroenteritis in infants and younger children, with the findings of most studies consistently demonstrating that rotavirus mainly affects younger children aged less than 5 years and the propor-tion of rotavirus infecpropor-tions among younger children was higher than that in the older age groups.3,7,15,27,28 The
gen-eral belief is that norovirus is a major pathogen leading to diarrheal outbreaks and causes symptomatic infections in older children and adults. However, some studies12,14,15 demonstrated that norovirus also has an impact on children younger than 24 months, which is consistent with the finding of the current study. This study showed children hospitalized with rotavirus and norovirus infection were around the same age and, in the main, younger than 36 months. The proportion of rotavirus positives among different age groups was increased from 13.7% to 26.6% as the age increased, but the proportion of norovirus positives was maintained around 12.8–15.0% in each age group. Because the current study is focused on hospital-ized patients with acute diarrhea and limited to subjects aged less than 5 years, this study indicates that rotavirus infection might possibly cause more intense diarrhea and/ or vomiting than norovirus, leading to older children still requiring hospitalization. However, norovirus infection
Lab dat a on admission WBC (1 ,000/ μ L), mean ± SD d 11 .4 ± 5.2 11 .5 ± 6. 1 12.3 ± 6.0 10.4 ± 5. 1 0.0177** 0.8802 > 15 cf 33 (19.4) 17 (15.2) 6 (20.7) 101 (15. 1) 0.4925 0.3633 missing dat a 1 (0.6) 3 (2.6) 0 (0) 5 (0.7) 0. 1537 Plat elet (1 ,000/ μ L), mean ± SD d 304.6 ± 90.9 332.4 ± 122.0 355.6 ± 83.7 273.5 ± 102.6 < 0.0001** 0.0266** missing dat a 1 (0.6) 3 (2.6) 0 (0) 5 (0.7) 0. 1537 CRP (mg/L), mean ± SD d 21 .0 ± 40.0 17 .1 ± 28. 1 14.8 ± 20.0 58.9 ± 66.8 < 0.0001** 0.6178 missing dat a 27 (15.8) 22 (19. 1) 9 (31 .0) 52 (7 .7) 0.4630 AS T (U/L), mean ± SD d 49.8 ± 22.8 47 .5 ± 27 .7 42.8 ± 10.6 47 .6 ± 50.3 0.9718 0.7893 missing dat a 115 (67 .3) 64 (55.7) 20 (67 .0) 378 (56. 1) aSt atistically signif icant, p < 0.05** f
or the least signif
icant dif fer ence pr ocedur e; bp < α1 *** (an ap pr opriat e thr eshold) f or each pair
-wise comparison between Rot
a + , Nor o– vs. Rot a–, Nor o + , under a par titioning of the χ 2 method ( α1 = 0.05/3) or Krusk al-W allis multiple-comparison pr ocedur e ( α1 = 0.05/6); cχ 2 t est f
or the comparison of cat
egorical dat a, and a par titioning of the χ 2 method (Brunden, 1972) f or each pair -wise comparison; done-way analy
sis of variance with the least signif
icant dif fer ence pr ocedur e f or continuous dat a; eKrusk al-W
allis one-way analy
sis of variance by r
anks with a multiple-comparison pr
ocedur
e in ordinal dat
a;
fthe percent
age was calculat
ed by number of events divided by number of r
emaining samples
af
ter e
xcluding number of missing. A
GE = acut e gastr oent eritis; AS T = aspar tat e aminotr ansf er ase; BT = body t emper atur e; CRP = c-r eactive pr ot ein; SD = st andard de viation; URI = up per respi-rator y inf ection; WBC = whit e blood cell.
could indeed be more frequent in older children and adults but not severe enough to require hospitalization.
One review study demonstrated that norovirus gastro-enteritis predominantly occurs in cold weather between
November and March in the northern hemisphere.29 How-ever, the prevalent season of norovirus infection was highly variable in different regions as shown in some studies.8,15,30
A study conducted in China showed that norovirus infection
0 5 10 15 20 25 30 35 40 45 50
Virus positive cases (%)
Rotavirus Norovirus
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Figure. Monthly distribution of norovirus and rotavirus among hospitalized young children with acute diarrhea in Taiwan, 2009.
Table 3. Comparison of epidemiology of diarrheal cases in three Taiwanese hospitals
All (n = 989)
Hospital
pa
Chang Gung Linko ChangHua Chang Gung Kaohsiung (n = 442) (n = 255) (n = 292) Sex, maleb 554 (56.0) 251 (56.8) 141 (55.3) 162 (55.5) 0.9072 Age (mo) Mean ± SDc 21.6 ± 13.7 21.5 ± 14.0 21.7 ± 13.3 21.7 ± 13.5 0.9765 Median 17.8 17.4 18.0 18.0 Distribution (mo)b 0.2142 0–5 51 (5.2) 31 (7.0) 9 (3.5) 11 (3.8) 6–11 233 (23.6) 103 (23.3) 57 (22.4) 73 (25.0) 12–23 366 (37.0) 156 (35.3) 104 (40.8) 106 (36.3) 24–35 167 (16.9) 72 (16.3) 40 (15.7) 55 (18.8) 36–47 100 (10.1) 51 (11.5) 28 (11.0) 21 (7.2) 48–60 72 (7.3) 29 (6.6) 17 (6.7) 26 (8.9)
Household member with AGE history 229 (23.2) 97 (22.0) 64 (25.1) 68 (23.3) 0.6353 (Vomiting or diarrhea)b
Stool test
Rotavirusb 200 (20.2) 102 (23.1) 63 (24.7) 35 (12.0) 0.0001a
Norovirusb 144 (14.6) 56 (12.7) 36 (14.1) 52 (17.8) 0.1506
Oral rotavirus vaccineb 0.5885
With vaccine 158 (16.0) 65 (14.7) 42 (16.5) 51 (17.5)
Without vaccine 831 (84.0) 377 (85.3) 213 (83.5) 241 (82.5)
ap < 0.05 for the χ2 test or ANOVA; bχ2 test for comparison of categorical data; cOne-way analysis of variance (ANOVA) for continuous data.
peaked in autumn (August–November). It has been reported that norovirus is prevalent all year around in Hong Kong and during the warmer months in Indonesia. Some studies indicate that the prevalence of rotavirus infection is higher during cooler months in temperate zones.9,11,13,17–20,52,56–59
However, infection shows less distinct seasonality but has a peak during the dry months in tropical countries. This study demonstrates that the detection rates of rotavirus and norovirus were both higher during winter and early spring (December–April) in Taiwan but the peak incidence of norovirus occurred earlier than that of rotavirus.
As shown in many previous studies,7,15,32,33 rotavirus
infection typically manifested as fever and vomiting, followed by profuse diarrhea. Norovirus infection results in a higher rate of vomiting in children but diarrhea in adults, and usually a shorter course of disease, around 1–3 days. Our findings show that patients with norovirus gastroenteritis presented with a low grade fever, or no fever at all, and a longer duration of vomiting compared with those with ro-tavirus gastroenteritis. We found the severity of diarrhea and days of hospitalization for patients positive for noro-virus were not less than those infected with rotanoro-virus. These findings differ from those of studies in northern Taiwan3,7
that demonstrated patients with rotavirus gastroenteritis had a longer course than those with norovirus diarrhea. An explicit finding of this study indicated a far higher pro-portion of diarrheal patients infected by either norovirus or rotavirus was associated with vomiting (74.8% and 74.9%, respectively) compared with the other enteropathogens group. Some studies in northern Taiwan3,7 demonstrated that higher levels of C-reactive protein along with variable leukocytosis were noted in patients with rotavirus diarrhea compared with those with norovirus diarrhea. However, no apparent difference in the laboratory findings was found between patients with rotavirus and norovirus diarrhea in our study.
Our study had several limitations. First, only patients suffering from acute diarrhea were enrolled, and this en-rolled criteria possibly underestimated the true occurrence rate of enteropathogen infection if patients initially pre-sented with vomiting and less intense diarrhea. The severity of gastroenteritis for hospitalized pediatric patients was roughly estimated by duration and frequency of vomiting and diarrhea, and no apparent difference was found between norovirus and rotavirus diarrheal cases. A more objective
dehydration scale should be introduced to assess the se-verity of gastroenteritis resulting from different infectious pathogens.
In conclusion, norovirus was one of the major infectious agents, secondary only to rotavirus, which caused hospi-talization of children less than 5 years of age with acute diarrhea in Taiwan. The prevalent season for norovirus gastroenteritis was similar to that of rotavirus gastroen-teritis, i.e. winter and the early spring months. We found it difficult to differentiate norovirus from rotavirus ac-cording to the laboratory findings and the clinical symp-toms; however, norovirus infection came with a lower grade fever and longer duration of vomiting. A history of house-hold members simultaneously suffering from gastroen-teritis might hint at the possibility of norovirus infection.
References
1. Chang CW, Chen PY, Huang FL. Epidemiology of diarrhea among young children: a questionnaire-based study in Taiwan.
J Microbiol Immunol Infect 2009;42:265–70.
2. Chen KT. Fana SF, Huang YF, Lee PI, Chen PY, Tang CW. Hospital-based study of the economic burden associated with rotavirus diarrhea in Taiwan. Vaccine 2007;25:4266–72.
3. Chen SM, Ni YH, Chen HL, Chang MH. Microbial etiology of acute gastroenteritis in hospitalized children in Taiwan. J Formos
Med Assoc 2006;105:964–70.
4. Lu TM, Tsai HT, Cheng YW, Chin LW, Yang CC. Gastroenterovi-ruses infection in Taiwan. The Open Infect Diss J 2009;3:37–43. 5. Parashar UD, Hummelman EG, Bresee JS, Miller MA, Glass RI.
Global illness and deaths caused by rotavirus disease in children.
Emerg Infect Dis 2003;9:565–72.
6. Patel MM, Widdowson MA, Glass RI, Akazawa K, Jan Vinjé, Parashar UD. Systematic literature review of role of noroviruses in sporadic gastroenteritis. Emerg Infect Dis 2008;14:1224–31. 7. Wu TC, Liu HH, Chen YJ, Tang RB, Hwang BT, Yuan HC.
Comparison of clinical features of childhood norovirus and rota-virus gastroenteritis in Taiwan. J Chin Med Assoc 2008;71:566–70. 8. Cheryl S.Y.Li, Paul K.S. Chan, and Julian W. Tang. Prevalence of
diarrhea viruses in hospitalized Children in Hong Kong in 2008.
J Med Virol 2009;81:1903–11.
9. Junquera CG, de Baranda CS, Mialdea OG, Serrano EB, Sánchez-Fauquier A. Prevalence and clinical characteristics of norovirus gastroenteritis among hospitalized children in Spain. Pediatr
Infect Dis J 2009;28:604–7.
10. Chen SY, Chang YC, Lee YS, Chao HC, Tsao KC, Lin TY, et al. Molecular epidemiology and clinical manifestations of viral gas-troenteritis in hospitalized pediatric patients in Northern Taiwan.
11. Lu CY, Lauderdale TL, Fang YH, Wang CY, Ho YH, Hung CL. Disease burden and related medical costs of rotavirus infections in Taiwan. BMC Infectious Diseases 2006;6:176.
12. Wu FT, Liang SY, Tsao KC, Huang CG, Lin CY, Lin JS, et al. Hospital-based surveillance and molecular epidemiology of rotavirus infection in Taiwan, 2005–2007. Vaccine 2009; 27S:F50–4. 13. Wu FT, Oka T, Katayama K, Wu HS, Donald Jiang DS, Miyamura
T, et al. Genetic diversity of noroviruses in Taiwan between November 2004 and March 2005. Arch Virol 2006;151:1319–27. 14. Victoria M, Carvalho-Costa FA, Heinemann MB, Leite JP,
Miagostovich M. Prevalence and molecular epidemiology of noroviruses in hospitalized children with acute gastroenteritis in Rio de Janeiro, Brazil, 2004. Pediatr Infect Dis J 2007;26:602–6. 15. Subekti D, Lesmana M, Tjaniadi P, Safari N, Frazier E,
Simanjuntak C, et al. Incidence of Norwalk-like viruses, rotavi-rus and adenovirotavi-rus infection in patients with acute gastroenteritis in Jakarta, Indonesia. FEMS Immunol Med Microbiol 2002;33:27–33. 16. O’Ryan ML, Lucero Y, Prado V, Santolaya ME, Rabello M, Solis Y, et al. Symptomatic and asymptomatic rotavirus and norovirus infections during infancy in a Chilean birth cohort. Pediatr Infect
Dis J 2009;28:879–84.
17. Mamdoh M. Meqdam1, Ibrahim R. Thwiny. Prevalence of group a rotavirus, enteric adenovirus, norovirus and astrovirus infections among children with acute gastroenteritis in Al-Qassim, Saudi Arabia. Pak J Med Sci 2007;23:551–5.
18. Nguyen VM, Nguyen VT, Huynh PL, Dang DT, Nguyen TH, Phan VT, et al. Vietnam Rotavirus Surveillance Network. The epidemiology and disease burden of rotavirus in Vietnam: sentinel surveillance at 6 hospitals. J Infect Dis 2001;183:1707–12. 19. Bresee J, Fang ZY, Wang B, Nelson EA, Tam J, Soenarto Y, et al.
Asian Rotavirus Surveillance Network. First report from the Asian Rotavirus Surveillance Network. Emerg Infect Dis 2004;10:988–95. 20. Karadag A, Acikgoz ZC, Avci Z, Catal F, Gocer S, Gamberzade S,
et al. Childhood diarrhoea in Ankara, Turkey: epidemiological and clinical features of positive versus rotavirus-negative cases. Scand J Infect Dis 2005;37:269–75.
21. Nelson EA, Widdowson MA, Kilgore PE, Steele D, Parashar UD. A decade of the Asian Rotavirus Surveillance Network: achieve-ments and future directions. Vaccine 2009;27(Suppl 5):F1–3.
22. Nelson EA, Bresee JS, Parashar UD, Widdowson MA, Glass RI; Asian Rotavirus Surveillance Network. Rotavirus epidemiology: the Asian Rotavirus Surveillance Network. Vaccine 2008;26:3 192–6.
23. Brandt CD, Kim HW, Rodriguez WJ, Arrobio JO, Jeffries BC, Parrott RH. Rotavirus gastroenteritis and weather. J Clin Microbiol 1982;16:478–82.
24. Levy K, Hubbard AE, Eisenberg JN. Seasonality of rotavirus disease in the tropics: a systematic review and meta-analysis. Int J
Epidemiol 2009;38:1487–96.
25. Atchison CJ, Tam CC, Hajat S, van Pelt W, Cowden JM, Lopman BA. Temperature-dependent transmission of rotavirus in Great Britain and The Netherlands. Proc Biol Sci 2010;277:933–42. 26. Morris OP, Edward AE. Influence of humidity on rotavirus
prevalence among Nigerian infants and young children with gastroenteritis. J Clin Microbiol 1982;15:212–5.
27. Xu J, Yang Y, Sun J, Ding Y, Su L, Fang Z, Glass R. Molecular epidemiology of rotavirus infections among children hospitalized for acute gastroenteritis in Shanghai, China, 2001 through 2005.
J Clinl Virol 2009;44:58–61.
28. Chiu TF, Lee CN, Lee PI, Kao CL, Lin HC, Lu CY, et al. Rotavirus gastroenteritis in children: 5-year experience in a medical center.
J Microbiol Immunol Infect 2000;33:181–6.
29. Mounts AW, Ando T, Koopmans M, Bresee JS, Noel J, Glass RI. Cold weather seasonality of gastroenteritis associated with Norwalk-like viruses. J Infect Dis 2000;181(Suppl 2):S284–7. 30. Xu J, Yang Y, Sun J, Ting Y. Molecular epidemiology of norovirus
infection among children with acute gastroenteritis in Shanghai, China, 2001–2005. J Clin Virol 2009;81:1826–30.
31. Mast TC, Chen PY, Lu KC, Hsu CM, Lin HC, Liao WC, et al. Epidemiology and economic burden of rotavirus gastroenteritis in hospitals and paediatric clinics in Taiwan, 2005–2006. Vaccine 2010;28:3008–13.
32. Cheng AC, McDonald JR, Thielman NM. Infectious diarrhea in developed and developing countries. J Clin Gastroenterol 2005;39: 757–73.
33. Narkeviciute I, Tamusauskaite I. Peculiarities of norovirus and rotavirus infections in hospitalised young children. J Pediatr