Prevalence and determinants of workplace violence of health care workers in a psychiatric hospital in Taiwan
6
0
0
全文
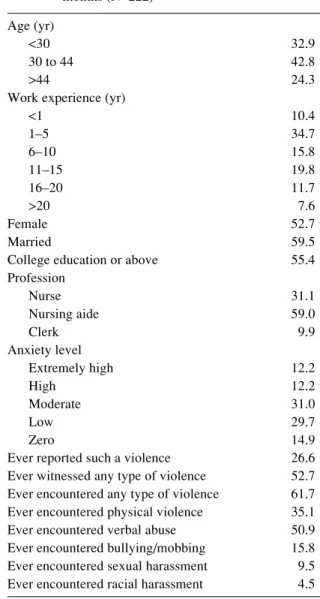
(2) Wen-Ching CHEN, et al.: Prevalence and Determinants of Workplace Violence. perpetrated by patients, so the determinants of workplace violence largely focus on patient profiles, including age, gender, psychotic symptoms, personality, and drug abuse15–19). Several studies have explored staff profiles as a determinant. Anderson reported that nurses with a previous abuse history seemed more vulnerable to physical violence and sexual harassment 20). And Di Martino addressed the relationship between violence and staff feelings of stress21). There is still a gap in the literature of studies exploring the prevalence and determinants of workplace violence against employees caring for long-term institutionalized patients with schizophrenia. We conducted this cross-sectional study to determine the prevalence and the possible risk factors of workplace violence at a large psychiatric institution mainly responsible for the long-term care of schizophrenia patients. In order to compare the results with other similar studies, we used a questionnaire developed by the International Labor Office, International Council of Nurses, World Health Organization, and Public Services International (ILO/ICN/WHO/PSI)5).. Method The hospital and participants This hospital is located in a rural area of eastern Taiwan. It was established as an asylum in 1966 by the government to care for patients with chronic schizophrenia. Following democratic and human rights movements, in the 1990s the asylum was renovated as a modern psychiatric center providing humane, patient-centered, modern services for patients from all over Taiwan. Currently, about 2,400 patients reside in the hospital 22). Once patients are admitted to this hospital, most of them live there for the remainder of their lives. Approximately 85% of the patients have been diagnosed with chronic schizophrenia. All nurses, nursing aides, and clerks with direct care of patients were invited to participate in this study. The main task of the nursing aides in this hospital is helping nurses with medical care, instructing and supervising patients in daily life activities, and keeping the environment clean, while clerks are responsible for accounting and administrative services. Out of the 231 people employed in these three positions at the hospital at the time of data collection, 222 completed valid questionnaires (96% response rate). More than half were female, married, and had a college level education or above. Three-quarters were under 45 yr old. About 60% were nursing aides (Table 1). Study ethics The Institutional Review Board (IRB) at the hospital approved the research protocol including the purpose, method, and use of the data collected. Participants’ privacy was guaranteed. Informed consent to take part in the study was obtained from individual respondents. 289. Table 1. Frequency distributions (in %) of demographics and workplace violence within the last 12 months (N=222) Age (yr) <30 30 to 44 >44 Work experience (yr) <1 1–5 6–10 11–15 16–20 >20 Female Married College education or above Profession Nurse Nursing aide Clerk Anxiety level Extremely high High Moderate Low Zero Ever reported such a violence Ever witnessed any type of violence Ever encountered any type of violence Ever encountered physical violence Ever encountered verbal abuse Ever encountered bullying/mobbing Ever encountered sexual harassment Ever encountered racial harassment. 32.9 42.8 24.3 10.4 34.7 15.8 19.8 11.7 7.6 52.7 59.5 55.4 31.1 59.0 9.9 12.2 12.2 31.0 29.7 14.9 26.6 52.7 61.7 35.1 50.9 15.8 9.5 4.5. when they returned the completed questionnaire. The questionnaire The questionnaire used in this study was translated directly from the one developed by the ILO/ICN/WHO/ PSI joint program on workplace violence in the health sector 5) . First, we formally obtained documented permission to use the questionnaire from the ILO. We then asked 13 experts from all over Taiwan in related fields to evaluate the content validity, including the fit with Taiwanese culture, the rationality of the questions asked, and the appropriateness of the translation. The test-retest reliability (0.85) was assessed with 13 health care workers at the hospital surveyed, with the second test performed two weeks later. The questionnaire was then back-translated to English to verify the accuracy of the Mandarin version..
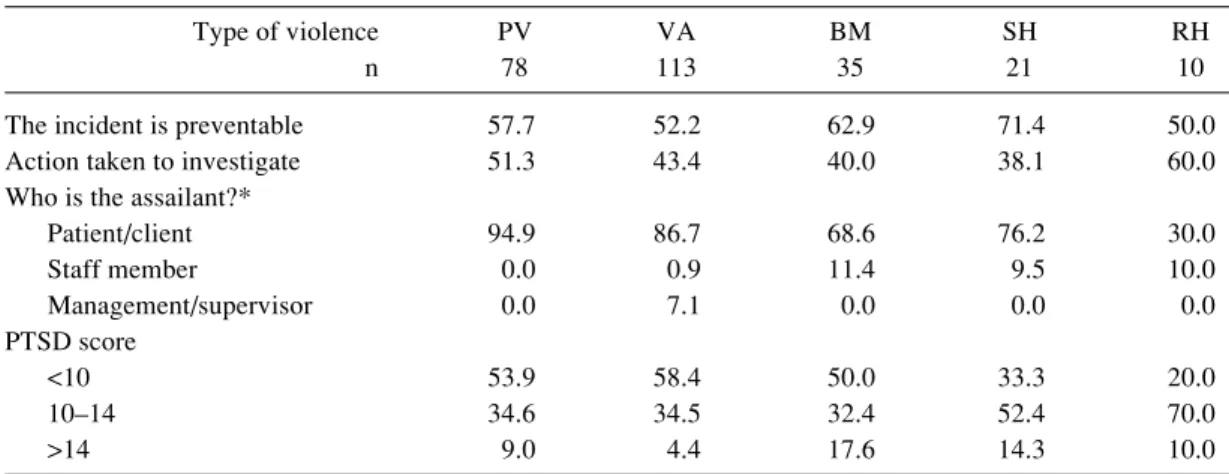
(3) 290. The questionnaire contains three parts. The first part requests personal data and includes a question about the level of anxiety about workplace violence, 1=not worried at all, 5=very worried. Next are the questions about experiences within the last 12 months with physical violence, which is defined as an intentional behavior that harms another person physically. The third part addresses the last 12 months experiences of psychological violence including verbal abuse (the behavior that humiliates, degrades, or otherwise a lack of respect for the dignity and worth of an individual), bullying/mobbing (repeated and over time offensive behavior, vindictive, cruel, or malicious attempts to humiliate or undermine an individual), sexual harassment (any unwanted, unreciprocated and unwelcome behavior of a sexual nature that is offensive to person involved, and causes that person to feel threatened, humiliated or embarrassed), and racial harassment (any threatening conduct that is based on race, color, language, religion, and minority). For each kind of violence, there is a post-traumatic stress disorder (PTSD) scale containing four items (rehearsal, avoidance, hyper-arousal, and effort) asking the victim to indicate how much he or she was bothered by the incident, 1=not at all, 5=extremely. These items are compatible to the diagnostic criteria of PTSD described in DSM-IV, which includes persistent reexperiencing of the traumatic event, such as thoughts, images, dreams, or percepts, persistent avoidance of stimuli associated with the trauma and numbing of general responsiveness, persistent symptoms of increased arousal, such as difficulty in falling or staying asleep, irritability, and difficulty in concentrating, and disturbances causing clinically significant distress or impairment in functioning23). Survey procedure In June 2003, we delivered the questionnaires to the nurses and asked them to fill them out, enclose and seal them with the provided envelope, and return them to the head nurse within one week in exchange for a small gift, a ball-point pen worth about US$ 2 dollars. In addition, we took advantage of two on-the-job training classes for nursing aides and clerks to collect questionnaires. The same gift was given in exchange for a completed questionnaire. Statistical analysis We coded the data in Excel ®, and asked another member of our team to verify all keyed-in data. SAS 8.2 was used to conduct statistical analyses. To evaluate the degree of PTSD, we summed scores on each PTSD item. In addition to simple analysis of frequencies, multiple logistic models were constructed for the two major types of violence, physical and verbal, by taking the following factors into consideration: gender, job duration, marital status, educational level, profession, and level of anxiety.. J Occup Health, Vol. 50, 2008. Through analysis, we found no statistically significant difference in gender, marital status, and educational level, so we did not put them into the model. Because age and job duration showed a high correlation, we deliberately included the latter in the model. In addition, because the hospital was restructured in 1990, staff recruited after that time were all required to have formal education and training, and thus are more qualified than those employed before 1990. We expected the staff whose job duration ranged 11–15 yr to be less vulnerable to violence and so we used them as the reference group. For the variables of profession and anxiety level, we chose clerk and zero level as the reference, respectively. The sample size of victims in the BM, SH, and RH categories was too small to conduct a logistic analysis in this study.. Results About a quarter of the participants reported workplace violence during the past year. Over half had witnessed such an incident, and over 60% had personally encountered at least one kind of violence at some time during their employment. About 55% had a moderate level of anxiety about workplace violence. The one-year prevalence rates of PV, VA, BM, SH, and RH were 35.1, 50.9, 15.8, 9.5, and 4.5%, respectively (Table 1). Of the PV incidents, 7.7% involved a weapon, such as chopsticks or a chair, and about 46.2% resulted in a physical injury, of which 30.8% needed medical treatment. About one-third of victims took time off from work due to an assault, of which more than one-third were off work for more than three days. About 70% of such incidents occurred in the daytime between 7:00 am and 18:00 pm. Over 80% of respondents had forgotten on which day of the week the incident had occurred. Table 2 summarizes the characteristic of each type of workplace violence. More than half of the PV and RH incidents were investigated, but less than half of the other three types were investigated. The most common perpetrators were patients, but a few co-workers or supervisors were perpetrators of VA, BM, SH, and RH. Fewer than 20% of the victims suffered from noteworthy PTSD symptoms for all types of workplace violence. More than half the respondents considered these events to be preventable. The results of the multiple logistic analyses are summarized in Table 3, which shows that anxiety above a moderate level tended to increase the likelihood of physical and/or verbal violence after adjustment for other risk factors. In addition, PV was associated with nurses and nurse aids, while VA was associated nurses and duration of employment of less than 5 yr or more than 20 yr.. Discussion Our findings suggest that not only the physical violence and verbal abuse but also bullying/mobbing, sexual.
(4) Wen-Ching CHEN, et al.: Prevalence and Determinants of Workplace Violence. 291. Table 2. Frequency distributions (in %) for physical violence (PV), verbal abuse (VA), bullying/mobbing (BM), sexual harassment (SH), and racial harassment (RH) experienced by 222 psychiatric care workers over the past one year Type of violence n The incident is preventable Action taken to investigate Who is the assailant?* Patient/client Staff member Management/supervisor PTSD score <10 10–14 >14. PV 78. VA 113. BM 35. SH 21. RH 10. 57.7 51.3. 52.2 43.4. 62.9 40.0. 71.4 38.1. 50.0 60.0. 94.9 0.0 0.0. 86.7 0.9 7.1. 68.6 11.4 0.0. 76.2 9.5 0.0. 30.0 10.0 0.0. 53.9 34.6 9.0. 58.4 34.5 4.4. 50.0 32.4 17.6. 33.3 52.4 14.3. 20.0 70.0 10.0. *The sum may be less than 100% because of the missing data.. Table 3. Frequency distributions (n) stratified by risk factors, crude odds ratio (COR), and the adjusted odds ratio (AOR) with a 95% confidence interval (CI) estimated by multiple logistic regression of physical violence and verbal abuse Physical violence n=78. Job duration (yr) <1 1–5 6–10 11–15 16–20 >20 Professional group Nurse Nursing aide Clerk Anxiety level Extremely high High Moderate Low Zero. Verbal abuse n=113. No. Yes. COR. AOR. 95% CI. No. Yes. COR. AOR. 95% CI. 20 40 26 31 18 9. 3 37 9 13 8 8. 0.4 2.2 0.8 1.0 1.1 2.1. 0.3 1.6 0.5 1.0 1.3 1.4. 0.1, 1.2 0.6, 4.2 0.1, 1.5. 15 29 15 30 14 6. 8 48 20 14 12 11. 1.1 3.5 2.9 1.0 1.8 3.9. 1.2 3.2 2.1 1.0 2.2 4.2. 0.4, 3.7 1.3, 7.9 0.7, 5.7. 36 88 20. 33 43 2. 9.2 4.9 1.0. 8.4 7.0 1.0. 1.4, 49.1 1.4, 34.5. 18 75 16. 51 56 6. 7.6 2.0 1.0. 5.9 2.5 1.0. 1.7, 21.2 0.8, 7.3. 12 9 42 53 28. 15 18 27 13 5. 7.0 11.2 3.6 1.4 1.0. 6.8 9.3 2.9 1.1 1.0. 1.8, 25.9 2.4, 36.1 0.9, 9.3 0.3, 3.6. 11 12 24 37 25. 16 15 45 29 8. 4.5 3.9 5.9 2.4 1.0. 2.9 2.3 4.3 1.8 1.0. 0.9, 9.3 0.7, 7.6 1.5, 11.8 0.7, 4.9. harassment, and racial harassment existed in the hospital among nurses and nursing aides. Gerberich et al.24) made a similar finding. The prevalence rate of 35.1% for physical violence in this hospital was much higher than the rates found in studies conducted at general hospitals with the same questionnaire, 3–17%7), or with different questionnaires 5.3–21%8–10). This finding corroborates the hypothesis that psychiatric units are one of the most frequent sites of workplace violence25). The level of verbal. 0.4, 4.3 0.4, 5.6. 0.8, 6.4 1.1, 15.8. abuse found in this study is consistent with that found in other studies8–10). Bullying was much lower in this study than reported in a Hong Kong study9), but the level of sexual harassment was comparable7, 9). An important finding in this study was that the higher the level of anxiety about workplace violence, the more vulnerable the healthcare workers were to PV. Hurell mentioned that a high level of anxiety can be a precedent for violence26). However, since a high level of anxiety.
(5) 292. can also result from workplace violence, the association cannot be clarified in a cross-sectional study such as this one. A follow-up study is needed. If the hypothesis of high anxiety level is verified, we shall recommend the hospital to provide a training program for high risk groups to reduce workplace violence. Although only 7.7% of the PV incidents involved the use of a weapon, they deserve our attention as PV incidents may lead to serious injuries. The fact that over one-third of PV incidents required medical treatment may be a warning sign for more serious workplace violence. In addition, about one-third of the PV victims needed to take sick leave. Thus, we recommend the precautionary measure of instituting a mandatory check for any dangerous tools during admission to the hospital or coming back after patients leave the ward. Only a moderate level of anxiety, not the two higher levels, was significantly related to an increased risk of verbal abuse. Perhaps VA is so frequently encountered in psychiatric wards that it might not be perceived as a major concern for injury and a source of worry. Nurses, not nursing aides, were the group most at risk of verbal abuse probably because the tasks carried out by nurses, such as giving medication and drawing blood samples, cause them to come into direct contact with patients more frequently than nursing aides. Privitera et al. indicated that work experience is a protective factor against violence12). In this study, the group with 1 to 5 yr of employment was at increased risk of VA, which seems to corroborate Privitera’s findings. People who had been employed for less than one year also had a shorter period of exposure, which might have had some impact on the prevalence rate. However, staff employed at the hospital for more than 20 yr had been working in this hospital since the asylum era. They are used to using authority to instruct patients and seemed more likely to encounter VA. Less than 10% of the employees surveyed reported sexual harassment over the past year. This figure might be accurate, or it might be an underestimation reflecting a difficulty in sharing such a private matter with others. There was a low rate (38%) of taking action to investigate SH as compared to other types of violence. Peek-Asa and Jenkins classified the following four types of workplace violence: criminal intent, customer or client, worker on worker, and personal relationship27). Table 2 shows that the majority (over 80%) of perpetrators were patients in the hospital. Only a small proportion of VA, BM, and SH incidents were conducted by supervisors or staff members. This finding is different from the findings of national case studies7), in which a substantial percentage of the perpetrators of psychological violence, including VA, BM, SH, and RH were staff. In this study, about one-third to half of the victims suffered PTSD symptoms. A PTSD score over 14 fits the DSM-IV diagnostic criteria of PTSD, which means. J Occup Health, Vol. 50, 2008. that about 10% of victims developed this disorder. A similar incidence has been reported among violence victims28). Over half of the affected staff regarded the event as preventable. Namely, had they taken proactive prevention measures, a substantial proportion of violence could have been avoided. Active training of employees in high-risk groups, especially those with a moderate or high level of anxiety, may reduce workplace violence in psychiatric hospitals. Among many aggression management programs29), a training program of Nonviolent Crisis Intervention has been introduced to this hospital for all staff. It contains instruction on a series of skills for coping with assault situations including how to avoid kicking, hitting and how to escape when patients grasp hair or clothes. Limitations In contrast to the country case studies using the questionnaire developed by ILO/ICN/WHO/PSI5) that were conducted in many types of facilities around the world, this study was conducted at only one psychiatric hospital that mainly provides care for long-term institutionalized chronic schizophrenia patients. Thus, our results on prevalence cannot be generalized to other hospitals, but the exploration of risk factors might be valuable for control of workplace violence in a large psychiatric hospital. In addition, our data was collected retrospectively, and may suffer from recall bias, misunderstanding of the definitions of violence, or a lack of willingness to share private information. However, since the questionnaire only asked participants to recall experiences from the past year and the test-retest reliability was 85%, it seems that the contents of the questionnaires were clearly understood by our participants. Furthermore, the 96% response rate also indicates excellent cooperation from our target group. Thus, the potential bias mentioned above might be small. Since the anxiety level may be a result of former experience of violence or a reflection of some workplace atmosphere, future studies should also consider these factors.. Conclusions The result of high anxiety level being associated with violence needs further examination. The prevalence of physical violence in this study was higher than those in other countries’ health sectors. We thus recommend the management of the hospital in our study to consider providing suitable training programs for the high-risk groups which might possibly reduce workplace violence. Acknowledgments: This study was partially supported by grant No. 93042 from the Hospital Administration Commission, and grant No. NHRI- EX 95-9204PP from the National Health Research Institutes of the Department.
(6) Wen-Ching CHEN, et al.: Prevalence and Determinants of Workplace Violence. of Health, Executive Yuan, Taiwan. The authors thank Ms. Chiou-Tau Lin and Ms. Shuen-Tzu Yang for their assistance with data collection and data management. We presented part of this paper at the 37th APACPH Conference in Conjunction with the 2005 Asia-Pacific Health Forum which was held on November 19–23 in Taipei, Taiwan.. References 1) DHHS (NIOSH) Publication 2002-101. Violence: occupational hazards in hospitals. Washington, DC: National Institute of Occupational Safety and Health, 2002. 2) Wilkinson CW: The role of the occupational health professional in preventing workplace violence. Clin Occup Environ Med 3, 659–672 (2003) 3) Shen HC, Cheng Y, Tsai PJ, Lee SH and Guo YL: Occupational stress in nurses in psychiatric institutions in Taiwan. J Occup Health 47, 218–225 (2005) 4) Wright RJ and Steinbach SF: Violence: an unrecognized environmental exposure that may contribute to greater asthma morbidity in high risk inner-city populations. Environ Health Persp 109, 1085–1089 (2001) 5) ILO/ICN/WHO/PSI. Framework guidelines for addressing workplace violence in the health sector. Geneva: ILO/ICN/WHO/PSI Joint Programme on Workplace Violence in Health Sector, 2002. 6) OSHA (NIOSH) Report 3148. Guidelines for preventing workplace violence for health care and social service workers. Washington, DC: US Department of Labor, 1996. 7) Di Martino V. Workplace violence in the health sectorcountry case studies Brazil, Bulgaria, Lebanon, Portugal, South Africa, Thailand, plus an additional Australian study: synthesis report. Geneva: ILO/ICN/ WHO/PSI Joint Programme on Workplace Violence in Health Sector, 2002. 8) Whittington R, Shuttleworth S and Hill L: Violence to staff in a general hospital setting. J Adv Nurs 24, 326– 333 (1996) 9) Kwok RP, Law YK, Li KE, Ng YC, Cheung MH, Fung VK, Kwok KT, Tong JM, Yen PF and Leung WC: Prevalence of workplace violence against nurses in Hong Kong. Hong Kong Med J 12, 6–9 (2006) 10) Chen ZH, Wang SY and Jing CX: Prevalence of workplace violence in staff of two hospitals in Guangzhou. Chinese J Prev Med 37, 358–360 (2003) (in Chinese) 11) May DD and Grubbs LM: The extent, nature, and precipitating factors of nurse assault among three groups of registered nurses in a regional medical center. J Emergency Nursing 28, 11–17 (2002) 12) Privitera M, Weisman R, Cerulli C, Tu X and Groman A: Violence toward mental health staff and safety in the work environment. Occup Med (Lond) 55, 480– 486 (2005) 13) Atawneh FA, Zahid MA, Al-Sahlawi KS, Shahid AA and Al-Farrah MH: Violence against nurses in. 14). 15). 16). 17). 18). 19). 20). 21). 22). 23). 24). 25). 26). 27). 28). 29). 293. hospitals: prevalence and effects. Br J Nurs 12, 102– 107 (2003) Lin YH and Liu HE: The impact of workplace violence on nurses in South Taiwan. Int J Nurs Stud 42, 773– 778 (2005) Lam JN, McNiel DE and Binder RL: The relationship between patients’ gender and violence leading to staff injuries. Psychiatr Serv 51, 1167–1170 (2000) Lowenstein M, Binder RL and McNiel DE: The relationship between admission symptoms and hospital assaults. Hosp Community Psychiatry 41, 311–313 (1990) Miller R, Zadolinnyj K and Hafner RJ: Profiles and predictors of assaultiveness for different psychiatric ward populations. Am J Psychiatry 150, 1368–1373 (1993) Nijman H, Merckelbach H, Evers C, Palmstierna T and Campo J: Prediction of aggression on a locked psychiatric admissions ward. Acta Psychiatr Scand 105, 390–395 (2002) Wessely SC, Castle D, Douglas AJ and Taylor PJ: The criminal careers of incident cases of schizophrenia. Psychol Med 24, 483–502 (1994) Anderson C: Workplace violence: are some nurses more vulnerable? Issues Ment Health Nurs 23, 351– 366 (2002) Di Martino V. Relationship of work stress and workplace violence in health sector. Geneva: ILO/ICN/ WHO/PSI Joint Programme on Workplace Violence in Health Sector, 2002. Chen WC, Wang JD, Lew-Ting CY, Chiu HJ and Lin YP: Workplace violence on workers caring for longterm institutionalized schizophrenic patients in Taiwan. J Occup Health 49, 311–316 (2007) Frances A. Diagnostic and statistical manuals of mental disorders, fourth edition (DSM-IV). Washington, DC: American Psychiatric Association, 1994. Gerberich SG, Church TR, McGovern PM, Hansen HE, Nachreiner NM, Geisser MS, Ryan AD, Mongin SJ and Watt GD: An epidemiological study of the magnitude and consequences of work related violence: the Minnesota Nurses’ Study. Acta Psychiatr Scand 61, 495–503 (2004) Eriksen W: Practice area and work demands in nurses’ aides: a cross-sectional study. BMC Public Health 6, 97 (2006) Hurrell JJ. Job stress, gender and workplace violence: analysis of assault experiences of state employees. In: VandenBos GR, Bulatao EQ, eds. Violence on the job. Washington, DC: Americal Psychological Association, 1997. Peek-Asa C and Jenkins L: Workplace violence: how do we improve approaches to prevention? Clin Occup Environ Med 3, 659–672 (2003) Caldwell MF: Incidence of PTSD among staff victims of patient violence. Hosp Community Psychiatry 43, 838–839 (1992) Farrell G and Cubit K: Nurses under threat: a comparison of content of 28 aggression management programs. Int J Ment Health Nurs 14, 44–53 (2005).
(7)
數據
相關文件
Using Books and Reading to Create a Healthy Workplace‖, Journal of the Canadian Health Libraries Association,
( Framework Directive 89/391/EEC On the introduction of measures to en- courage improvements in the safety and health of workers at
政府頒佈「Guideline to develop the mental health of workers in the workplace」. 要求雇主必須建立「心理健康發展計畫」(mental health
Article 40 and Article 41 of “the Regulation on Permission and Administration of the Employment of Foreign Workers” required that employers shall assign supervisors and
To offer foreign fisherman employed to work in Taiwan sounder care and impose obligations on employers to manage foreign fishermen for the purpose of improving their
The path to a healthy workplace, a critical review linking healthy workplace practices, employee well-being, and organiztion improvements.. Confirmatory factor analysis of the
Australian Government, Department of Education, Employment and Workplace Relations. Evaluation strategy for Job Services Australia
6 《中論·觀因緣品》,《佛藏要籍選刊》第 9 冊,上海古籍出版社 1994 年版,第 1
