IntroductIons
The occurrence of suicide mirrors closely the status of social and psychological wellbeing of a society. It has been well documented that lack of social integration and anomie status brought about by rapid changes in
Trends in suicide mortality in Taiwan, 1959-2006
Ruoning Wu1, YaWen Cheng1,2,*
Objectives: This study was conducted to examine long-term trends in suicide mortality in
Taiwan from 1959 to 2006 and to analyze the effects of age, time period, and cohort. Methods: Suicide mortality was calculated using official vital statistics data. The effects of age, time period, and cohort on suicide mortality were examined graphically and with Poisson regression models.
Results: An ubiquitous period effect on suicide mortality in both genders across all age groups
was observed, with peak rates in the early 1960s and early 1980s and an upward trend since the mid-1990s. Suicide mortality increased with age, and evidence for an age-by-period interaction was found. Over the past decade, the sharpest increase in suicide mortality was found in middle-aged men. Evidence of cohort effects was less clear, and suicide risk of different cohorts appeared to be associated with period- and age-specific social environmental conditions. Conclusions: The changing patterns of suicide mortality highlight the importance of period- and age-specific social conditions in determining a population’s risk of suicide. Further research is needed to explore the factors involved in such changes. (Taiwan J Public Health. 2008;27(2):110-120)
Key Words: suicide, mortality, trend, Taiwan
1 Department of Public Health, College of Public
Health, National Taiwan University, Taipei, Taiwan, R.O.C.
2 Institute of Health Policy and Management,
College of Public Health, National Taiwan University, No.17 Xu-Zhou Rd.,Taipei, Taiwan, R.O.C.
* Correspondence author. E-mail: [email protected]
Received: Oct 30, 2007 Accepted: Apr 8, 2008
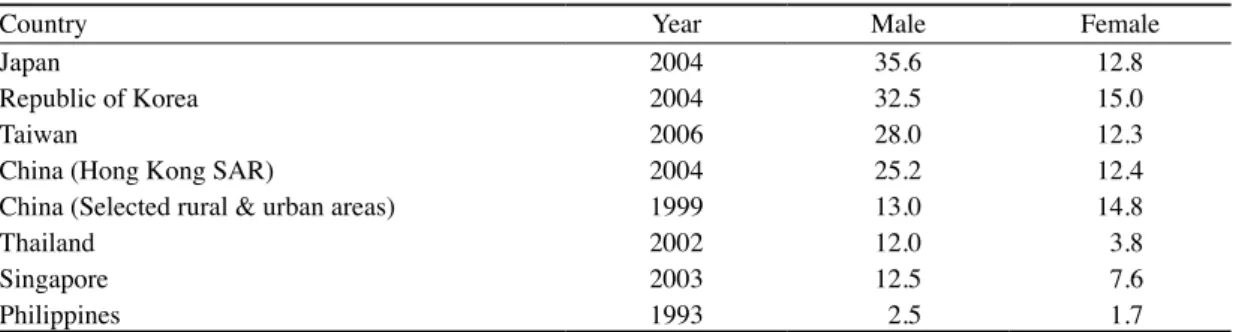
culture, values, and ways of life contribute to a population’s suicide rates [1]. Social and economic variables, such as social support, divorce rate, family integration, lack of participation in organized community activities, unemployment, economic fluctuations and bankruptcies, have been linked to risk of suicide [2-5].Availability of lethal tools, as well as imitative behaviors induced by media reports, have also been found to be promoting factors[6]. In Taiwan, suicide mortality rates have increased sharply in recent years, rising about 2-fold since the mid-1990s. In 2006, deaths from suicide accounted for 3.3% of the total number of deaths, with mortality rates of 28.0 and 12.3 per 100,000 for men and women respectively. As compared to other countries
in the eastern Asian region, Taiwan’s suicide mortality for men ranked only after Japan and South Korea (Table 1). To confront the root causes of suicide from a population perspective, it is crucial to gain a comprehensive understanding of the social distribution of suicide by demographic factors, as well as the changing patterns over a sufficiently long period of time.
Taiwan has undergone rapid industrialization and economic development over the past few decades. During the process of modernization, the country also experienced dramatic social transformation in many aspects. Some studies have been conducted to investigate the epidemiologic features of suicide in Taiwan. However, many of these studies focused on individual risk factors, such as old age, unemployment, depression, and experiences of major life events [7-9]. While a few studies were conducted to investigate the trends in suicide mortality from a population perspective, information was limited either by restricted periods of time that did not cover the years of recent rise [10-12], restricted regions of observation [13], or specific experiences of certain age groups [9]. Two studies were been carried out using time-series analyses to examine the effects of socio-economic factors on suicide mortality over sufficiently long time periods [11,12]; however, these two studies only presented results from regression models and did not report patterns of changes in suicide mortality by age and sex groups. To our knowledge, the interrelated effects of age, period, and birth cohort on suicide rates in the Taiwanese population had been only studied recently by Lin and Tsai [14]. However, further interpretation of findings from this study was limited because the authors used pooled data for men and women and did not report gender-specific mortality rates.
In western societies, there has been a long
research tradition in longitudinal and historical analysis of suicide rates, and three dimensions of time, i.e., age, period and cohort, have been extensively studied. Age effects refer to the influence of age, such as higher suicide mortality commonly observed in the elderly [1]. Period effects refer to the extent to which living in a particular time period affects suicide mortality in all age and gender groups, for example, the dramatic decrease in suicides in the late 1960s due to the detoxification of the domestic gas supply [6]. Cohort effects refer to the extent that year of birth influence the lifetime risk for suicide, for example, the long-term impact of childhood exposure on lifetime mental health status [15].
Various methodologies have been used to investigate the independent effects of age, period and cohort on suicide. The APC analysis is commonly used, which is based on reclassification of secular mortality data into age-stratified cohort tables, and the changing patterns were examined either graphically or statistically. Poisson regression modeling that attempts to estimate simultaneously all the three effects have also been applied in some studies [16-18]. However, because each of the three dimensions is a function of the other two, it is difficult to untangle the independent effects from each other. Researchers in this field have acknowledged the limitations of APC models, and emphasized the importance of using descriptive data in the interpretation of suicide trends [19,20].
The present study was carried out to investigate the secular trends in suicide mortality in Taiwan during the period from 1959 to 2006, with particular attention given to the effects of age, period, and birth cohort. Descriptive analyses using a graphical approach were performed, which were supplemented with Poisson regression models.
Table 1. Crude mortality (per 100,000) from suicide in selected countries by gender*
Country Year Male Female Japan
Republic of Korea Taiwan
China (Hong Kong SAR)
China (Selected rural & urban areas) Thailand Singapore Philippines 2004 2004 2006 2004 1999 2002 2003 1993 35.6 32.5 28.0 25.2 13.0 12.0 12.5 2.5 12.8 15.0 12.3 12.4 14.8 3.8 7.6 1.7
* Data for other Asian countries were from the World Health Organization[22].
MaterIal and Methods suicide mortality rates
Statistics on causes of death are virtually complete in Taiwan, because by law all deaths must be reported to the local authorities before a permit is issued for cremation or burial. Suicide mortality rates for the period of 1959-2006 were calculated based on data from the Vital Statistics published by the Department of Health and the Demographic Fact Books published by the Department of Provincial Civil Affairs, Executive Yuan of Taiwan. The entire population of Taiwan was included except residences of two offshore isles at a military front (Kinmen and Matsu), for which suicide mortality data were not available until 1994. Cause of suicide death was coded using the International Classification of Disease (ICD) spanning four revisions: in 1959 the ICD-6th Revision was used (E970-979); from
1960 to 1969 the ICD-7th Revision was used
(E970-979); from 1970 to 1980 the ICD-8th Revision was used (E950-959); and from
1981 onwards the ICD-9th Revision was used
(E950-959). The classifications of suicide death swere virtually the same despite of the different revisions. Mortality rates were stratified by sex and age-standardized to the 2000 World Standard Population provided by the World Health Organization.
assessment of age, period, and cohort effects on suicide mortality
The patterns of age, period and cohort ef-fects on suicide mortality were assessed mainly by graphical approaches. Age effects, referring to the influence of age on suicide mortality, were examined by age-specified rates in the following age categories: 15-24; 25-34; 35-44; 45-54; 55-64; and 65+ years old.
Period effects and the interrelated effects of age and period were examined by plotting the age- and sex-specific suicide rates in dif-ferent time periods. In order to simplify our graphical presentation, we only presented data in five selected time periods (i.e., 1961-1965, 1971-1975, 1981-1985, 1991-1995, 2001-2005) and omitted the intermediate time periods (i.e., 1966-1970, 1976-1980, etc.). Due to the inter-dependence of period effect and age effect on suicide rates, Poisson regression models were also used to estimate period effect after adjust-ing for age in addition to the graphical analysis. Indicator variables were created for age (in 5-year range) and period (one for each calendar year from 1959 to 2006). The age group 80-84 years and the year of 1993 were used as refer-ence categories. Separated models were fitted for males and females to estimate gender-spe-cific rate ratios (RRs) of each calendar period. All Poisson regression analyses were performed with SAS 9.0.
Cohort effect, referring to the extent that year of birth might influence the lifetime risk for suicide, was examined by categorizing people by their year of birth in 5-year band, and plotting the age-specific suicide mortality rates separately for each of the successive birth cohorts. Since it would be difficult to interpret the data if too many points and lines were dis-played on the same graph, we only reported data from nine selected birth cohorts (1900, 1910, 1920, 1930, and etc.), but the patterns of other birth cohorts were also examined.
results
Period effect on suicide mortality rates
In 2006, suicide mortality in men and women were 28.02/105 and 12.25/105,
respectively. The bold lines in Figures 1(a) & 1(b) indicate the trends of age-standardized mortality for suicide during the period from 1959 to 2006 for men and women, respectively. For both genders, two peaks in suicide mortality were observed, one in the early 1960s and another in the early 1980s. Rising trends have been seen ever since 1993 and are especially apparent for men in the middle-aged groups. The male-to-female mortality ratios, ranging between 1.33 (1965) and 2.29 (2006), have steadily increased throughout the period.
Gender-stratified and age-specific mortality rates for suicide are also shown in Figures 1(a) & 1(b). In general, all age groups experienced similar pattern, with highest suicide mortality rates in the early 1960s, a second peak in the early 1980s, and rising trends since the mid-1990s. The period patterns on suicide variation revealed by the Poisson regression model were similar compared to the results of graphical analyses in both genders. Compared to the reference year of 1993, suicide mortality in the early 1960s was about 3-4 times higher; in the early 1980s, about two times higher; and
in recent years about two times higher in both genders. (Table 2).
age effect on suicide mortality rates
Figures 2(a) and 2(b) display age patterns in suicide mortality in men and women, respectively, in the five selected periods. Each line represents the relationship of age in a five-year interval with the suicide mortality of the corresponding age ranges. For both men and women, suicide mortality rates increased with age, with the highest rates found in people aged 65 years or above. However, unusually high mortality rates for men and women aged younger than 34 were noticed in the early 1960s.
age-by-period interaction on suicide mortality rates
Evidences of some age-by-period interactions were found based on information from Figures 1 and 2. For both genders, during the first epidemic peak in the early 1960s, the youngest group (aged 15-24 years) was found to have substantially higher suicide mortality rates than other age groups, but the rates of this age group became the lowest as compared to other age groups in later periods. In contrast, the middle-aged groups of 35-44 years had lowest rates for suicide in the 1960s, but experienced higher suicide mortality as compared to other age groups in recent years.
cohort effect and the age-period-cohort interaction on suicide mortality rates
To examine whether any particular birth cohort carried an increased predisposition to suicide, we categorized people by their year of birth in five-year band and calculated the age-specific suicide mortality for each group of birth cohort. Only half of the successive five-year birht cohorts are presented alternately for
Table 2. Age-adjusted rate ratios for suicide mortality by calendar year for males and females Year of death Rate ratio Males95% confidence Rate ratioFemales95% confidence
interval interval 1959 3.28 2.99 - 3.61 4.01 3.56 - 4.53 1960 3.30 3.01 - 3.62 4.26 3.78 - 4.80 1961 3.86 3.53 - 4.22 3.98 3.53 - 4.49 1962 4.00 3.67 - 4.37 4.66 4.15 - 5.23 1963 4.05 3.71 - 4.41 4.78 4.27 - 5.37 1964 4.35 4.00 - 4.74 4.53 4.04 - 5.08 1965 3.49 3.20 - 3.81 4.57 4.08 - 5.12 1966 3.30 3.02 - 3.61 4.04 3.60 - 4.53 1967 2.98 2.72 - 3.26 3.27 2.90 - 3.69 1968 2.74 2.50 - 3.00 3.35 2.98 - 3.77 1969 2.75 2.52 - 3.01 3.19 2.83 - 3.59 1970 2.59 2.37 - 2.83 2.89 2.57 - 3.26 1971 2.19 2.00 - 2.40 2.53 2.24 - 2.86 1972 2.30 2.10 - 2.52 2.48 2.20 - 2.80 1973 1.96 1.79 - 2.15 2.32 2.05 - 2.62 1974 1.76 1.60 - 1.94 2.14 1.89 - 2.42 1975 1.84 1.68 - 2.02 2.10 1.86 - 2.38 1976 1.60 1.45 - 1.76 1.97 1.74 - 2.23 1977 1.73 1.58 - 1.90 2.15 1.90 - 2.42 1978 1.69 1.54 - 1.85 2.30 2.04 - 2.59 1979 1.72 1.57 - 1.89 2.16 1.92 - 2.43 1980 1.65 1.50 - 1.81 2.28 2.03 - 2.56 1981 1.85 1.69 - 2.02 2.55 2.27 - 2.86 1982 2.09 1.92 - 2.28 2.55 2.28 - 2.86 1983 2.08 1.91 - 2.27 2.34 2.09 - 2.62 1984 1.81 1.66 - 1.98 2.21 1.97 - 2.48 1985 1.97 1.80 - 2.14 2.36 2.11 - 2.65 1986 1.95 1.79 - 2.12 2.20 1.96 - 2.47 1987 1.57 1.44 - 1.72 1.75 1.56 - 1.98 1988 1.48 1.35 - 1.62 1.64 1.46 - 1.85 1989 1.26 1.15 - 1.38 1.43 1.27 - 1.62 1990 1.08 0.98 - 1.19 1.20 1.06 - 1.36 1991 1.17 1.07 - 1.29 1.19 1.05 - 1.35 1992 1.11 1.01 - 1.22 1.01 0.89 - 1.15 1993 1.00 Reference 1.00 Reference 1994 1.12 1.02 - 1.23 1.02 0.90 - 1.16 1995 1.17 1.06 - 1.28 1.21 1.07 - 1.37 1996 1.38 1.26 - 1.51 1.22 1.08 - 1.38 1997 1.58 1.45 - 1.72 1.45 1.29 - 1.64 1998 1.52 1.40 - 1.66 1.44 1.28 - 1.62 1999 1.62 1.49 - 1.76 1.40 1.24 - 1.57 2000 1.68 1.54 - 1.83 1.53 1.37 - 1.72 2001 1.92 1.77 - 2.08 1.60 1.43 - 1.80 2002 2.12 1.95 - 2.29 1.69 1.51 - 1.89 2003 2.11 1.95 - 2.28 1.84 1.64 - 2.05 2004 2.27 2.10 - 2.45 1.95 1.74 - 2.17 2005 2.85 2.64 - 3.07 2.24 2.01 - 2.49 2006 2.88 2.67 - 3.11 2.20 1.98 - 2.45
Figure 1. Age-adjusted* and age-specific mortality from suicide in Taiwan during the period from 1959 to 2006: (a) males; (b) females.
*Direct standardization using the 2000 world standard population.
Figure 2. Age-pattern of mortality from suicide in Taiwan in different periods: (a) males; (b) females.
the sake of simplicity. Figures 3(a) and 3(b) display the age patterns of suicide mortality rates for the nine separate birth cohorts, in men and women, respectively. The patterns of the omitted birth cohorts were generally represented by their adjacent birth cohorts.
In general, suicide mortality increased with age, but the shape of the relationship between age and suicide mortality varied substantially by year of birth. For the cohorts who were born before 1950, a bimodal relationship between age and suicide mortality was found: the first peaks occurred at different age in different birth cohorts, but all occurred during the suicide epidemic in the 1960s (indicated by downward arrows in the Figures). For the cohorts who were born in the 1950s and 1960s, suicide mortality rates appeared to peak at 20-24 years of age, decline in late 20s, and rise again in the third decade of life. For the birth cohorts of 1970s and 1980s, a linear relationship of age and suicide mortality was observed for both genders,
yet, the length of observation was too short to make conclusive statements.
dIscussIons
Our findings indicated that throughout the study period there has been an ubiquitous period effect on suicide mortality in both genders and across all age groups, with peak rates observed in the early 1960s and early 1980s, and since the early 1990s, a rising trend has been noted in all age groups and in both genders, especially for middle-aged men. Older age was found to be associated with higher suicide mortality in all periods.
Our findings concerning period effects suggested that period-specific social conditions play a major role in determining suicide risk in Taiwan. Echoing the findings from a previous study that reported the trends of suicide in Taiwan from 1946 to 1990 [10], we also observed a peak in the early 1960s. Figure 3. Age-specific mortality from suicide by birth cohort in Taiwan from 1900-1904 to
1980-1984: (a) males; (b) females. *The downward arrows indicate the peak year
It has been suggested that the observed rapid surge in suicide during the 1950s and up to the mid-1960s was related to great social disorganization induced by the massive influx of immigrants from the mainland China right after the World War II [10]. Mass migration over a short period of time caused dramatic demographic changes, as well as social, political and cultural conflicts in Taiwan, which had been a Japanese colony during the first half of the 20th century. Chinese migrants, especially
those who had experienced the Sino-Japanese War and consequential civil conflicts in China, might have been highly susceptible for mental health problems [21]. In addition, major social and economic reforms that occurred in the 1950s also led to changes in family structures, values, and ways of life. On the other hand, the subsequent downward trend observed in the late 1960s and through the 1970s might be linked to greater political stability as well as dramatic improvement in economic conditions, resulting from the country’s rapid industrialization.
The second peak in suicide mortality observed in the early 1980s and the decline afterwards coincided with changes in unemployment rates. In the early 1980s, as many labor-intensive manufacturing factories left Taiwan and relocated in developing neighboring countries, substantial rises in unemployment were noted, rising from <2% throughout the 1970s up to the highest point of 2.9% in 1985. After 1985 and until 1995, unemployment rates were below <2%, but again increased steadily afterwards. The sharp increase in suicide rates observed since the mid-1990s seemed to correlate closely with rising unemployment and economic recession. In other Asian countries, substantial increases in suicide mortality since the 1990s were also reported, including Japan and South Korea [22],and have been associated with economic downturns [23,24].
Some social variables that reflect family integration, such as divorce rate and female labor participation, have also been reported as important risk factors for suicide in earlier periods in Taiwan [12]. However, the contributions of various economic and social factors to the recent rise in suicide mortality in Taiwan have not been well investigated and deserve further studies.
Consistent with most of the existing literature [1,9,19,25,26], we found that suicide mortality increased with age, with highest mortalities observed in the age group of 65 years and older throughout the studied period. Earlier studies have suggested that higher mortality from suicide in the elderly might be related to prolonged duration of chronic physical illnesses; in addition, poverty, feelings of meaninglessness, loss of spouse, social isolation, lack of life control, and even fear of the inability to influence their own dying might attribute to a higher risk for old-age suicide [26,27].
Unexpectedly, findings of this study revealed that in the early1960s, young people, especially those between 15-24 years old, exhibited high mortality from suicide. Such an unusual binomial age pattern observed in the 1960s in Taiwan was also documented by an earlier study [10], in which the authors suggested that a boom in birth rate during the post-war era and disrupted social and familial support for the youth during that period might be explanations. High risk for suicide death among the young people disappeared however during the following years.
With regard to gender difference in suicide mortality, we found that suicide mortality rates were higher in men than women throughout the studied period and across all age groups. This finding is consistent with findings from most of the other countries [22].This could be explained by higher levels of social distress,
lower levels of social support, less adequate coping behaviors, and higher lethality of suicide methods in men than in women.
Strengths of this study include its comprehensive coverage of population and the long-term data based on official vital statistics. However, there is a limitation in this study. Since mortality data for suicide were traced over a long span of more than four decades and across all age groups, we are not certain whether suicide deaths were recognized and recorded in a systematic manner across different periods and populations. In Taiwan, suicide is still regarded as a sensitive issue and is highly stigmatized. It is possible that some suicide deaths or events were not reported as suicide, but instead as accident or other causes.
Concerns are mounting as Taiwan’ s suicide rates have increased rapidly in recent years. It is extremely worrisome that the sharpest increase was found in middle-aged men. Marked increases in suicide among middle-aged men were also reported in Japan and South Korea, and had been associated with changes in social and economic factors such as divorce, economic crisis, and labor market conditions [24,28-30]. While many people agree that effective public health actions should be taken to stop this alarming trend, there is little consensus on what preventative measures are most efficient and applicable. Currently, the Department of Health of Taiwan Govenment has adopted preventative strategies, such as providing mental health counseling services, setting up suicide hotline services, advocating screening programs and psychiatric treatment for depression. However, we argue that such individual-based approaches might only be palliative and unlikely to alter the trend of suicide. Findings of our study highlight the importance of period- and age-specific social couditions in determining a population’s risk of suicide. We suggest that further research should
be conducted to identify social and economic determinants of suicide risk and design more appropriate preventative policy to tackle such an urgent public health problem.
acknowledgeMents
This study was supported by a research grant from the National Science Council (NSC 95-2627-H-002-001-MY2), Taiwan. We appreciated Dr. Wanyu Yeh’s assistance in statistical analyses. We were also grateful to two anonymous reviewers for giving us constructive suggestions, and to Dr. Linda M. Ewers for proof-reading this paper.
references
1. Sainsbury P. The epidemiology of suicide. In: Roy A ed. Suicide. Baltimore: Williams & Wilkins, 1986:17-40.
2. Crawford MJ. Increasing rates of suicide in young men in England during the 1980s: the importance of social context. Soc Sci Med 1999;49:1419-23. 3. Johansson SE. Unemployment is an important risk
factor for suicide in contemporary Sweden: an 11-year follow-up study of a cross-sectional sample of 37,789 people. Public Health 1997;111:41-5.
4. Lewis G. Suicide, deprivation, and unemployment: record linkage study. BMJ 1998;317:1283.
5. Preti A, Miotto P. Suicide and unemployment in Italy, 1982-1994. J Epidemiol Comm Health 1999;53:694-701.
6. Gunnell D, Middleton N, Frankel S. Method availability and the prevention of suicide--a re-analysis of secular trends in England and Wales 1950-1975. Soc Psychiatry Psychiatr Epidemiol 2000;35:437-43.
7. Cheng A, Chen T, Chen C, Jenkins R. Psychosocial and psychiatric risk factors for suicide: case-control psychological autopsy study. Br J Psychiatry 2000;177:360-5.
8. Chou YJ, Huang N, Lee C, et al. Suicides after the 1999 Taiwan earthquake. Int J Epidemiol 2003;32:1007-14.
9. Liu HL, Wang HC, Yang MJ. Factors associated with an unusual increase in the elderly suicide rate in Taiwan. Int J Geriatr Psychiatry 2006;21:1219-21.
10. Chong MY, Cheng TA. Suicidal behaviour observed in Taiwan:trends over four decades. In: Lin TY, Tseng WS, Yeh EK eds. Chinese Societies and Mental Health. Hong Kong: Oxford University Press, 1995;209-18.
11. Chuang HL, Huang WC. A reexamination of "sociological and economic theories of suicide: a comparison of the U.S.A. and Taiwan". Soc Sci Med 1996;43:421-3.
12. Yang B, Lester D, Yang CH. Sociological and economic theories of suicide: a comparison of the U.S.A. and Taiwan. Soc Sci Med 1992;34:333-4. 13. Lin JJ. Changes of method-specific suicide trends
in Taipei City,1971-2004. Taipei City Med J 2006;3:962-9.
14. Lin CY, Tsai YJ. Suicide trend in Taiwan,1976-2001. Taiwan Family Med Res 2005;3:28-38.
15. Hjern A, Allebeck P. Suicide in first- and second-generation immigrants in Sweden: a comparative study. Soc Psychiatry Psychiatr Epidemiol 2002;37:423-9.
16. Allebeck P. Are suicide trends among the young reversing? Age, period and cohort analyses of suicide rates in Sweden. Acta Psychiatr Scand 1996;93:43-8. 17. Morrell S, Page A, Taylor R. Birth cohort effects in
New South Wales suicide, 1865-1998. Acta Psychiatr Scand 2002;106:365-72.
18. Ajdacic-Gross V, Bopp M, Gostynski M, Lauber C, Gutzwiller F, Rossler W. Age-period-cohort analysis of Swiss suicide data, 1881-2000. Eur Arch Psychiatry Clin Neurosci 2006;256:207-14.
19. Snowdon J, Hunt GE. Age, period and cohort effects on suicide rates in Australia, 1919-1999. Acta Psychiatr Scand 2002;105:265-70.
20. Gunnell D, Middleton N, Whitley E, Dorling D, Frankel S. Influence of cohort effects on patterns
of suicide in England and Wales, 1950-1999. Br J Psychiatry 2003;182:164-70.
21. Carta MG, Bernal M, Hardoy MC, Haro-Abad JM. Migration and mental health in Europe (the state of the mental health in Europe working group: appendix 1). Clin Pract Epidemol Ment Health 2005;1:13. 22. WHO. Country reports and charts. http://www.who.
int/mental_health/prevention/suicide/country_reports/ en/index.html. Accessed, October 30 2007.
23. Aihara H, Iki M. An ecological study of the relations between the recent high suicide rates and economic and demographic factors in Japan. J Epidemiol 2003;13:56-61.
24. Kim H, Song YJ, Yi JJ, Chung WJ, Nam CM. Changes in mortality after the recent economic crisis in South Korea. Ann Epidemiol 2004;14:442-6.
25. Yip PS. Suicides in Hong Kong, Taiwan and Beijing. Br J Psychiatry 1996;169:495-500.
26. Erlangsen A, Bille-Brahe U, Jeune B. Differences in suicide between the old and the oldest old. J Gerontol B Psychol Sci Soc Sci 2003;58:S314-22.
27. Chochinov HM, Wilson KG, Enns M, et al. Desire for death in the terminally ill. Am J Psychiatry 1995;152:1185-91.
28. Yamasaki A, Sakai R, Shirakawa T. Low income, unemployment, and suicide mortality rates for middle-age persons in Japan. Psychol Rep 2005;96:337-48. 29. Inoue K, Tanii H, Abe S, et al. Causative factors as
cues for addressing the rapid increase in suicide in Mie Prefecture, Japan: comparison of trends between 1996-2002 and 1989-1995. Psychiatry Clin Neurosci 2006;60:736-45.
30. Aihara H, Iki M. Effects of socioeconomic factors on suicide from 1980 through 1999 in Osaka Prefecture, Japan. J Epidemiol 2002;12:439-49.
1 台灣大學公共衛生系 2 台灣大學衛生政策與管理研究所 * 通訊作者:鄭雅文 聯絡地址:台北市徐州路十七號 E-mail: [email protected] 投稿日期:96年10月30日 接受日期:97年4月8日