Cingulum correlates of cognitive functions in patients with mild cognitive impairment and early Alzheimer’s disease - A diffusion spectrum imaging study
Y.-C. Lin • Y.-C. Shih • W.-Y. I. Tseng • Y.-H. Chu • M.-T. Wu •T.-F. Chen • P.-F. Tang ( ) • M.-J. Chiu ( )
Correspondence to: Dr. Ming-Jang Chiu, No. 7, S. 1, Chung-Shan S. Rd., Department of neurology, National Taiwan University Hospital, College of Medicine, National Taiwan University,Taipei, 100, Taiwan; E-mail: [email protected]; Tel: 886-933929393; Fax: 886-2-23418395 ; Correspondence to: Dr. Pei-Fang Tang, No. 17, XuZhou Rd, School and Graduate Institute of Physical Therapy, College of Medicine, National Taiwan University, Taipei, 100, Taiwan; E-mail: [email protected]; Tel: 33668128; Fax: 886-2-33668161.
Y.-C. Lin • Y.-H. Chu • M.-T. Wu • P.-F. Tang
School and Graduate Institute of Physical Therapy, College of Medicine, National Taiwan University, Taipei, Taiwan
W.-Y. I. Tseng • P.-F. Tang • M.-J. Chiu
Graduate Institute of Brain and Mind Sciences, College of Medicine, National Taiwan University, Taipei, Taiwan
W.-Y. I. Tseng • P.-F. Tang • M.-J. Chiu
Neurobiology and Cognitive Science Center, National Taiwan University Hospital, Taipei, Taiwan
Y.-C. Shih • W.-Y. I. Tseng
Center for Optoelectronic Biomedicine, College of Medicine and Department of Medical 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
Imaging, National Taiwan University Hospital, College of Medicine, Taipei, Taiwan T.-F. Chen • M.-J. Chiu
Department of Neurology, National Taiwan University Hospital, College of Medicine, National Taiwan University, Taipei, Taiwan
Y.-C. Lin
Department of Physical Medicine and Rehabilitation, China Medical University Hospital, Taichung, Taiwan
Y.-C. Shih
Institute of Biomedical Engineering, College of Medicine and Department of Medical Imaging, National Taiwan University Hospital, College of Medicine, Taipei, Taiwan Y.-H. Chu
Department of Physical Therapy and Graduate Institute of Rehabilitation Science, China Medical University, Taichung, Taiwan
M.-T. Wu
Rehabilitation Center, Cardinal Tien Hospital Yunghe Branch, Taipei, Taiwan P.-F. Tang
Physical Therapy Center, National Taiwan University Hospital, Taipei, Taiwan M.-J. Chiu
Institute of Brain and Mind Sciences, Department of Psychology, College of Science, and Graduate Institute of Biomedical Engineering and Bioinformatics, National Taiwan University, Taipei, Taiwan
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
Abstract
Diffusion spectrum imaging (DSI) of MRI can detect neural fiber tract changes. We investigated integrity of cingulum bundle (CB) in patients with mild cognitive impairment (MCI) and early Alzheimer’s disease (EAD) using DSI tractography and explored its relationship with cognitive functions. We recruited 8 patients with MCI, 9 with EAD and 15 healthy controls (HC). All subjects received a battery of
neuropsychological tests to access their executive, memory and language functions. We used a 3.0-tesla MRI scanner to obtain T1- and T2-weighted images for anatomy and used a pulsed gradient twice-refocused spin-echo diffusion echo-planar imaging
sequence to acquire DSI. Patients with EAD performed significantly poorer than the HC on most tests in executive and memory functions. Significantly smaller general
fractional anisotropy (GFA) values were found in the posterior and inferior segments of left CB and of the anterior segment of right CB of the EAD compared with those of the HC. Spearman’s correlation on the patient groups showed that GFA values of the posterior segment of the left CB were significantly negatively associated with the time used to complete color trails test Part II and positively correlated with performance of the logical memory and visual reproduction. GFA values of inferior segment of bilateral CB were positively associated with the performance of visual recognition. DSI
tractography demonstrates significant preferential degeneration of the CB on the left side in patients with EAD. The location-specific degeneration is associated with corresponding declines in both executive and memory functions.
Keywords: diffusion spectrum imaging, cingulum bundle, executive function, memory function, mild cognitive impairment, Alzheimer’s disease
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
Introduction
Diffusion spectrum imaging (DSI), a magnetic resonance imaging (MRI) technique, is a sensitive and reliable tool for detecting structural changes in the fiber tracts of the human brain (Schmahmann et al. 2007). DSI measures the magnitude and direction of water molecule diffusion in the brain tissue. It has been used to reconstruct detailed cerebral fiber pathways, forming a rectilinear three-dimensional grid, and a strength of the technique is its ability to resolve crossing fibers and small fibers (Wedeen et al. 2012). The general fractional anisotropy (GFA) value is an index of the directional consistency of water diffusion in DSI analysis. A higher GFA value indicates a more consistent direction of diffusion of water molecules along fiber tracts, reflecting better integrity of the neural fiber bundles (Basser 1995; Hubbard and Parker 2009).
The cingulum bundle (CB) is a complex network structure. It has short association fibers connecting different regions of the cingulate cortices and long association fibers extending to the prefrontal, parietal and temporal cortices (Schmahmann and Pandya 2006). Previous studies using probabilistic tractography and functional connectivity have explored the anatomical and functional connections of the CB (Beckmann et al. 2009; Torta and Cauda 2011). The anterior segment of the CB extends to the
orbitofrontal cortex, dorsolateral prefrontal cortex, amygdala, hippocampus, striatum and hypothalamus (Beckmann et al. 2009). Therefore, the anterior segment of the CB plays a role in emotion, pain perception, attention, and conflict-control functions. The middle segment of the CB connects to the dorsolateral prefrontal cortex, primary motor and premotor cortices, parietal cortex and dorsolateral striatum; hence, this region plays an important role in the execution of motor- and attention-related tasks. The posterior and inferior segments of the CB reach the hippocampus, parahippocampus, and parietal cortex and thus are associated with episodic memory, spatial navigation 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
and attention-shifting tasks. These critical functional connections of the CB prompted us to explore the integrity of the CB in the prodromal and early stages of Alzheimer’s disease (AD) and to elucidate the relationship between CB integrity and the decline in various domains of cognitive function observed with this relentless degenerative disease.
In recent studies, the structural integrity of the posterior segment of the CB displayed early degeneration in patients with mild cognitive impairment (MCI) and in patients with AD (Sexton et al. 2011; Zhang et al. 2007). This degeneration may be related to cognitive dysfunction in these patients because the CB is one of the main associative fibers connecting both the executive control and default mode networks, which control the major neural mechanisms behind executive function, memory and other cognitive functions (Seeley et al. 2007; van den Heuvel et al. 2008).
Therefore, we used DSI to obtain GFA values for the anterior, middle, posterior, and inferior segments of the CB and to examine whether the CB would be degenerated in patients with MCI and early Alzheimer’s disease (EAD). We also explored the
relationship between performance on tests of executive function, memory and language as well as the integrity of different segments of the CB in these patients.
Furthermore, to better elucidate whether the CB plays a specific role in cognitive dysfunction in patients with MCI and EAD, we performed DSI analysis on callosal frontal fibers (CFF) as a comparison and on callosal motor fibers (CMF) as a non-cognitive reference. We also examined the relationship between the fiber integrity of the CFF and CMF and cognitive function.
Participants and Methods Participants 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
In total, we recruited 8 patients with MCI, 9 with EAD and 1 5 elderly healthy controls (HC) in this study. All participants were right-handed, were between 60 and 90 years old and had 6 or more years of education. Participants with AD or MCI were recruited from the memory clinic at the National Taiwan University Hospital. All participants with dementia met the diagnostic guidelines for probable AD dementia proposed by the NIA-AA workgroups in 2011 (Albert et al. 2011). The diagnosis of MCI due to AD was in accordance with the NIA-AA’s diagnostic guidelines (McKhann et al. 2011). To diagnose MCI due to AD, we used a formal cognitive test with the cut-off value set at or below the 4th percentile (i.e., lower than 1.5 SDs) of the scale scores based on
age- and education-matched control participants. All of the patients had decreased hippocampal volume, as measured by either volumetry, with volumes less than 95% of the healthy elderly controls, or the Visual Rating System (Scheltens et al. 1995). The HC were recruited following the principles used in our previous MCI cohort studies (Chen et al. 2009; Chen et al. 2009). Participants who demonstrated contraindication to MRI scanning, other neurological diseases or severe co-morbidities that affect cognitive performance were excluded. This study was approved by the ethics committee and the institutional review board of the university hospital. All participants or their principal caregivers provided their written informed consent.
Neuropsychological tests
All participants received the same neuropsychological test battery, which included the Mini-Mental State Examination (MMSE) (Folstein et al. 1975) to test general
cognitive function; the Modified Card Sorting Test (Nelson 1976) and Color Trails Tests Parts I and II (CTT I and II) (D’Elia et al. 1996) to assess executive function; the logical memory and visual reproduction subtests of the Wechsler Memory Scales, 3rd edition 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
(WMS-III) to assess verbal and visual memory; and the object naming and semantic verbal fluency tests to assess language function (Hua et al. 2005).
MRI data acquisition and analysis
We used a 3.0-tesla MRI scanner (Tim Trio, Siemens, Erlangen, Germany) with a 32-channel head coil to acquire brain images. To obtain an anatomical reference, high resolution T1-weighted imaging with a magnetization-prepared rapid gradient echo (MPRAGE) sequence was performed with a repetition time (TR)/echo time (TE) of 2000 ms/2.98 ms, a flip angle of 9˚, an acquisition matrix of 192 x 256, a field of view (FOV) of 256 x 256 mm, and a slice thickness of 1 mm in the coronal plane. Multiple trans-axial T2-weighted MR images were acquired with a TR/TE of 9430/101 ms, a flip angle of 150°, an acquisition matrix of 256 x 256, a FOV of 248×248 mm, and a slice thickness of 3 mm.
The DSI was acquired using a pulsed gradient twice-refocused spin-echo diffusion echo-planar imaging (EPI) sequence (TR/TE= 9600/130 ms, FOV= 200 x 200 mm, matrix= 80 x 80, slice thickness= 2.5 mm, number of slices= 56) in the transverse plane (Reese et al. 2003). A total of 102 diffusion-encoding directions were applied, with a maximum diffusion sensitivity (b max) of 4000 s/mm2, corresponding to the grid points
filled within a half sphere of the q-space, with a radius of three units (Lo et al. 2011). Next, we performed a 3D Fourier transform of the data to obtain a probability
attenuation function at each pixel and calculated the orientation distribution function (ODF) in different radial directions (Wedeen et al. 2005). The generalized fractional anisotropy (GFA) value, which is a quantitative index derived from the ODF equaling the standard deviation of the ODF/root mean square of the ODF, was used to indicate the diffusion anisotropy at each pixel (Tuch, 2004). Therefore, the GFA values in this DSI 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
study are similar to the FA values in DTI studies because both can be used to indicate the microstructural integrity of the white matter fiber tracts (Lo et al. 2011; Tang et al. 2010).
After generating a brain GFA map using in-house DSI studio software (http://dsi-studio.labsolver.org/), we performed multiple-ROI and tract-specific tractography analysis to reconstruct the CB, CFF, and CMF tracts. We primarily used MARINA software (Bender Institute of Neuroimaging, University of Giessen, Germany) to select ROIs for each targeted tract on a Montreal Neurological Institute (MNI) template, except when selecting the ROI for the precentral gyrus. To reconstruct the CB, we selected ROIs on the anterior, middle, and posterior cingulate gyri to reconstruct the superior portion of the CB tract (Fig. 1A, C) and ROIs on the posterior cingulate gyrus and medial temporal lobe to reconstruct the inferior portion of the CB, that is, the portion that enters the medial temporal lobe (Fig. 1B, C). To reconstruct the CFF, we selected ROIs on the bilateral dorsolateral prefrontal cortex (Brodmann’s areas 8, 9, 10, and 46) and the entire corpus callosum (Fig. 1D). To reconstruct the CMF, the ROIs were placed on the medial precentral gyrus (Tang et al. 2010) and the entire corpus callosum (Fig. 1D). After selecting the ROIs, we performed spatial imaging normalization using a two-stage procedure. In this procedure, linear and non-linear transformations of the T2 and DSI image coordinates for the individual participants' brains were utilized to transform images into MNI coordinates using the built-in functions of SPM5 (Wellcome
Department of Imaging Neuroscience, London, UK). In the first stage, we used the T2 weighted image as the reference image and the b0 image (the null image of DSI) as the source image to perform a 3D 12-parameter affine transformation (linear
transformation) and co-registered the diffusion images to the anatomical images. In the second stage, the T2 weighted images of the individual participants were wrapped 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
around the MNI template through non-linear transformation. The coordinates of the ROIs defined in the MNI template were then mapped onto the GFA maps of the individual participants' brains through an inverse transformation by using the
deformation matrix calculated with in-house MATLAB software and DSI studio software. Then, a streamline-based fiber tracking algorithm was performed using DSI studio software to reconstruct the superior portion of the CB, inferior CB, CFF, and CMF tracts.
The way we divided the superior portion of the CB into the anterior, middle and posterior segments was slightly different from Vogt’s definition of the sub-regions of the cingulate gyrus (Fig. 1A) (Vogt 2005). Briefly, the borders of the segments were
determined using the vertical plane at the anterior commissure and the anterior– posterior commissural line. The border between the anterior and middle segments of the CB was defined by the crossing of the vertical line from the anterior commissure and the cingulate sulcus, and the border between the middle and posterior segments of the CB was defined by the extension line of the marginal ramus of the cingulate sulcus. The inferior CB segment was defined as the point where the CB tract enters the medial temporal lobe. Finally, GFA values of the CFF, CMF, and four CB segments were calculated. Higher GFA values indicated greater structural integrity.
Statistical analysis
A one-way ANOVA was used to examine between-group differences in age and years of education, and the Chi-squared test was used for gender and CDR distribution. For the other variables, we used a Kruskal-Wallis test to compare three-group differences (significance level set at 0.05) and a Mann-Whitney U test for pair-wise comparisons, with a correction for multiple comparisons (significance level set at 0.017). The relationships between performance on tests of executive function or memory and the 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
integrity of the various CB segments were examined using Spearman's rank correlation coefficients, and the significance level was set at 0.01 to assure a moderate or strong correlation and a correction for multiple testing. To determine the fiber tract integrity that independently and significantly contributed to neuropsychological performance, we performed stepwise multiple linear regression analysis (criteria: probability-of-F-to-enter <= .050; probability-of-F-to-remove >= .100), controlling for age, with the integrity of the CFF, CMF, and the anterior, middle, posterior, and inferior CB segments as the potential predictors. The significance level was set at 0.05 for multiple regression analysis. All statistical analyses were performed with SPSS version 18.0 software.
Results
There were no significant between-group differences in gender distribution, age or years of education. General cognitive function, assessed by the total scores on the MMSE, was poorer for the EAD group than for both the MCI and HC groups (p < 0.017; Table 1). The results of the neuropsychological tests showed that patients with EAD performed significantly worse than the HC group on the MCST, with fewer completed categories (p < 0.017) and more perseverative errors (p < 0.017), and the EAD group used more time to complete Parts I (p < 0.017) and II (p < 0.017) of the CTT and generated fewer words in the semantic verbal fluency test (p < 0.017; Table 2). Similarly, memory performance in the EAD group was poorer than that of the HC group for all parameters of the two memory tasks (all p < 0.017, Table 2). Furthermore, immediate and delayed recall of logical memory and recognition of visual reproduction was poorer in the EAD group than in the MCI group (all p < 0.017, Table 2). Comparisons of the GFA values of various segments of the bilateral CBs showed that both the posterior and inferior segments of the left CB and the anterior segment of the right CB were significantly smaller in 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
patients in the EAD group than in patients in the HC group (all p < 0.017; Table 3). There were no significant differences in GFA values of all CB segments, CFF, and CMF between the MCI and EAD groups (Table 3).
The results of the Spearman’s correlation coefficient analyses that were used to assess the relationships between the GFA values of the CB, CFF, and CMF as well as performance on the neuropsychological tests in the patient groups (combining the MCI and EAD groups, n = 17) showed that the GFA value for the posterior segment of the left CB was negatively correlated with the time needed to complete Part II of the CTT (rs =
-0.613, p = 0.009) and positively correlated with the scaled scores of immediate recall on tests of both logical memory (rs = 0.622, p = 0.008) and visual reproduction (rs =
0.684, p = 0.002) and of delayed recall on tests of visual reproduction (rs = 0.606, p =
0.010). GFA values of the inferior segment of both the left and right CB were positively correlated with the scaled scores on the recognition of visual reproduction test (rs =
0.745, p = 0.002 and rs = 0.710, p = 0.004, respectively) (Table 4).
Multiple linear regression models showed that the GFA value for the anterior segment of the left CB explained 39.6 % of the variance in the number of
non-perseverative errors on the Modified Card Sorting Test (p < 0.05; Table 5 and Fig. 2). The GFA value for the posterior segment of the left CB explained28.3 % of the variance in the time needed to complete the CTT Part II and 34.5 % and 71.9 % of the variance in the scaled scores of delayed recall of logical memory and visual reproduction, respectively (all p < 0.05; Table 5 and Fig. 2). The GFA value for the inferior segment of the left CB explained 32.7 % of the variance in the number of perseverative errors on the Modified Card Sorting Test and 50.9 % of the variance in the scaled score for recognition in the test of visual reproduction (both p < 0.05; Table 5 and Fig. 2). Furthermore, the GFA value for the CFF explained 38.5 % of the variance in the time to complete the CTT Part I 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
(p < 0.05; Table 5 and Fig. 2).
Discussion
Recent DTI studies confirmed a significant reduction of FA in the cingulate gyrus in patients with MCI and AD (Teipel et al. 2012; Alves et al. 2012). Other studies further demonstrated that this reduction primarily occurred in the posterior segment of the CB (Zimny et al. 2011; Catheline et al. 2010). However, the decline in FA in the anterior segment of the CB is more controversial because some researchers consider this decline to be a phenomenon of normal aging (Catheline et al. 2010; Kiuchi et al. 2009), whereas others consider the decline to be a process of degenerative change (Mielke et al. 2009). In this study, we found that the GFA values of the right anterior CB and the posterior and inferior segments of the left CB were significantly lower in patients with EAD than in those of the HC group. In short, the integrity of the CB degenerated significantly in the patients with EAD, and the degeneration was more obvious in the left hemisphere, especially in the posterior and inferior segments of the CB. This laterality may be a consequence of more beta amyloid deposition and more white matter degeneration in the left hemisphere (Davatzikos and Resnick 2002; Tosun et al. 2011).
We found that the GFA values of the posterior segment of the left CB were negatively associated with performance on Part II of the CTT. The color trail making tests evaluate attention, visual scanning, visuospatial skills, mental flexibility, inhibition, working memory, and motor skills (Chen et al. 2009; Kortte et al. 2002; Royall et al. 2002). Part II of the CTT has the additional capability of testing cognitive functions related to attention shifting compared to Part I of the CTT (Kortte et al. 2002). During the CTT Part II test, the participants must scan the positions of different numerals with different colors and perform the test by alternately shifting their attention between 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
colors and numerals sequentially. They must also integrate visual information to formulate their action plan on a global level. Previous studies using functional MRI (fMRI) during the trail making tests showed that when right-handed individuals
performed the Trail Making Test- Part B with their dominant hand, there were markedly increased blood oxygenation level dependent responses in the dorsolateral prefrontal cortex, inferior parietal cortex, cingulate cortex, and middle and superior temporal gyri, particularly in the left hemisphere (Moll et al. 2002; Zakzanis et al. 2005).
The posterior cingulate gyrus has strong fiber connections with the posterior parietal lobe, which is involved in smooth pursuit and saccadic eye movement control, sensorimotor integration, motor planning, and set-shifting (Andersen and Buneo, 2002; Asari et al. 2005, Liston et al. 2006). These strong anatomical connections may underlie the executive role of the posterior CB. Furthermore, recent DTI studies in older adults have found that the integrity of the posterior white matter tracts, such as the posterior cingulum and splenium, is associated with not only memory but also executive functions (Kantarci et al. 2011; Voineskos et al. 2012). Therefore, our finding that the integrity of the posterior CB, especially in the left hemisphere, was moderately correlated with CTT Part II performance in patients with MCI and EAD is consistent with previous fMRI and DTI reports. The decline in executive functioning, which is one of the key factors
predicting conversion from MCI to AD, is also a critical factor resulting in impairment when performing instrumental activities of daily living (Marshall et al. 2011; Tabert et al. 2006). Our finding thus emphasizes the importance of examining the integrity of the posterior CB in patients who are in the prodromal stage of or at risk for AD.
The posterior and inferior segments of the CB are also highly connected to the medial temporal lobe (Beckmann et al. 2009; Torta and Cauda 2011), which is one of the most vulnerable regions in AD and the principal area involved in episodic memory 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
(Buckner 2004). The medial temporal region contains the hippocampus and
parahippocampus, which play critical roles in the registration, retention and retrieval processes of a memory task. These roles account for the close relationship between performance on a memory task and the integrity of the posterior and inferior segments of the CB found in this study. Finally, the regression analysis results delineated the contribution of the posterior and inferior segments of the left CB to executive and memory functions. This analysis showed that the integrity of these two segments of the left CB explained approximately 30-70% of the variance in executive and memory function, represented by performance on the CTT Part II and tests of logical memory and visual reproduction.
Together, our findings suggest that MCI and EAD are not associated with a universal homogeneous degeneration of all white matter. The preferential degeneration of the left posterior and inferior segments of the CB in the prodromal or early stages of AD may contribute at least in part to the decline in memory and executive function in these patients. However, we acknowledge that the performance of complex
neuropsychological tasks likely requires intricate interactions of complex neural networks. For example, in this study, we found that the CFF explained approximately 40% of the variance in the time needed to complete the CTT I, which evaluates attention, visual scanning, visuospatial skills, working memory, and motor skills. There may be other white matter tracts involved in the neuropsychological functions investigated in this study in addition to the CB. However, the involvement of other potential white matter tracts is beyond the scope of this study.
This study was not without limitations. First, the patient sample size is relatively small, and as a result, some between-group differences may not reach statistical significance, especially when the cognitive change is relatively mild in the prodromal 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
(MCI) or early stage of AD. For example, GFA values for various CB segments in the MCI group were approximately intermediate between those of the HC and EAD groups, but the difference did not reach statistical significance. Similarly, performance on various neuropsychological tests for patients with MCI was intermediate between that of the HC and EAD groups, as expected from a clinical perspective, but the difference did not reach statistical significance. On the other hand, our positive findings for both tests of
cognitive function and GFA measurements from the seemly small number of subjects implied that the differences are robust. Nevertheless, care must be taken when
generalizing the findings of this study. Second, as previously discussed, performance of the complex neuropsychological tasks used in this study requires the cooperation of complex neural networks. There may be other white matter tracts involved in these functions in addition to the CB. However, the involvement of other potential white matter tracts is beyond the scope of this study.
Conclusions
We conclude that the integrity of the CB, derived from the DSI tract-specific
analysis, is compromised in patients with EAD. DSI tractography demonstrated location-specific degeneration of the CB, such that the posterior segment is associated with declines in both executive function and memory, while the inferior segment is associated with memory function in the prodromal and early stages of AD.
Acknowledgments
The research was in part supported by grants from the National Science Committee Taiwan (NSC 99-2314-B-002 -090 and NSC100-2314-B-002-006). 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
References
Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, Gamst A, Holtzman DM, Jagust WJ, Petersen RC, Snyder PJ, Carrillo MC, Thies B, Phelps CH (2011) The diagnosis of mild cognitive impairment due to Alzheimer's disease:
recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 7:270-279
Alves GS, O'Dwyer L, Jurcoane A, Oertel-Knochel V, Knochel C, Prvulovic D, Sudo F, Alves CE, Valente L, Moreira D, Fubetaer F, Karakaya T, Pantel J, Engelhardt E, Laks J (2012) Different patterns of white matter degeneration using multiple diffusion indices and volumetric data in mild cognitive impairment and Alzheimer patients. PLoS One 7:e52859
Andersen RA, Buneo CA (2002) Intentional maps in posterior parietal cortex. Annu Rev Neurosci 25:189-220
Asari T, Konishi S, Jimura K, Miyashita Y. (2005) Multiple components of lateral posterior parietal activation associated with cognitive set shifting. NeuroImage, 26:694-702 Basser PJ (1995) Inferring microstructural features and the physiological state of tissues
from diffusion-weighted images. NMR Biomed 8:333-344
Beckmann M, Johansen-Berg H, Rushworth MF (2009) Connectivity-based parcellation of human cingulate cortex and its relation to functional specialization. J Neurosci 29:1175-1190
Buckner RL (2004) Memory and executive function in aging and AD: multiple factors that cause decline and reserve factors that compensate. Neuron 44:195-208
Catheline G, Periot O, Amirault M, Braun M, Dartigues JF, Auriacombe S, Allard M (2010) Distinctive alterations of the cingulum bundle during aging and Alzheimer's disease. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
Neurobiol Aging 31:1582-1592
Chen TF, Chen YF, Cheng TW, Hua MS, Liu HM, Chiu MJ (2009) Executive dysfunction and periventricular diffusion tensor changes in amnesic mild cognitive impairment and early Alzheimer's disease. Hum Brain Mapp 30:3826-3836
Chen TF, Lin CC, Chen YF, Liu HM, Hua MS, Huang YC, Chiu MJ (2009) Diffusion tensor changes in patients with amnesic mild cognitive impairment and various dementias. Psychiatry Res 173:15-21
Davatzikos C, Resnick SM (2002) Degenerative age changes in white matter connectivity visualized in vivo using magnetic resonance imaging. Cereb Cortex 12:767-771 D'Elia LF (1996) Color Trails Test. Professional manual. Psychological Assessment
Resources, Florida
Folstein MF, Folstein SE, McHugh PR (1975) "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189-198 Hua MS, Chang BS, Lin KN, Yang JM, Lu SR, Chen SY (2005) Wechsler Memory Scale.
Chinese Behavioral Science Corporation, Taipei
Hubbard PL, Parker GLM (2009) Validation of tractography. In: Johansen-Berg H and Behrens TEJ (eds) Diffusion MRI: from quantitative measurement to in-vivo neuroanatomy. Academic Press, London, pp 353-376
Kantarci K, Senjem ML, Avula R, Zhang B, Samikoglu AR, Weigand SD, Przybelski SA, Edmonson HA, Vemuri P, Knopman DS, Boeve BF, Ivnik RJ, Smith GE, Petersen RC, Jack CR, Jr. (2011) Diffusion tensor imaging and cognitive function in older adults with no dementia. Neurology 77:26-34
Kiuchi K, Morikawa M, Taoka T, Nagashima T, Yamauchi T, Makinodan M, Norimoto K, Hashimoto K, Kosaka J, Inoue Y, Inoue M, Kichikawa K, Kishimoto T (2009)
Abnormalities of the uncinate fasciculus and posterior cingulate fasciculus in mild 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
cognitive impairment and early Alzheimer's disease: a diffusion tensor tractography study. Brain Res 1287:184-191
Kortte KB, Horner MD, Windham WK (2002) The trail making test, part B: cognitive flexibility or ability to maintain set? Appl Nneuropsychol 9:106-109
Liston C, Matalon S, Hare TA, Davidson MC, Casey BJ (2006) Anterior cingulate and posterior parietal cortices are sensitive to dissociable forms of conflict in a task-switching paradigm. Neuron 50:643-53
Lo YC, Soong WT, Gau SS, Wu YY, Lai MC, Yeh FC, Chiang WY, Kuo LW, Jaw FS, Tseng WY (2011) The loss of asymmetry and reduced interhemispheric connectivity in adolescents with autism: a study using diffusion spectrum imaging tractography. Psychiatry Res 192:60-66
Marshall GA, Rentz DM, Frey MT, Locascio JJ, Johnson KA, Sperling RA (2011) Executive function and instrumental activities of daily living in mild cognitive impairment and Alzheimer's disease. Alzheimers Dement 7:300-308
McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR, Jr., Kawas CH, Klunk WE, Koroshetz WJ, Manly JJ, Mayeux R, Mohs RC, Morris JC, Rossor MN, Scheltens P, Carrillo MC, Thies B, Weintraub S, Phelps CH (2011) The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Aging-Alzheimer's disease. Alzheimers Dement 7:263-269
Mielke MM, Kozauer NA, Chan KC, George M, Toroney J, Zerrate M, Bandeen-Roche K, Wang MC, Vanzijl P, Pekar JJ, Mori S, Lyketsos CG, Albert M (2009) Regionally-specific diffusion tensor imaging in mild cognitive impairment and Alzheimer's disease. Neuroimage 46:47-55
Moll J, de Oliveira-Souza R, Moll FT, Bramati IE, Andreiuolo PA (2002) The cerebral 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
correlates of set-shifting: an fMRI study of the trail making test. Arq Neuropsiquiatr 60:900-905
Nelson HE (1976) A modified card sorting test sensitive to frontal lobe defects. Cortex 12:313-324
Reese TG, Heid O, Weisskoff RM, Wedeen VJ (2003) Reduction of eddy-current-induced distortion in diffusion MRI using a twice-refocused spin echo. Magn Reson Med 49:177-182
Royall DR, Lauterbach EC, Cummings JL, Reeve A, Rummans TA, Kaufer DI, LaFrance WC, Jr., Coffey CE (2002) Executive control function: a review of its promise and
challenges for clinical research. A report from the Committee on Research of the American Neuropsychiatric Association. J Neuropsychiatry Clin Neurosci 14:377-405 Scheltens P, Barkhof F, Leys D, Wolters E, Ravid R, Kamphorst W (1995). Histopathologic
correlates of white matter changes on MRI in Alzheimer’s disease. Neurology 45:883–888
Schmahmann J, Pandya D (2006) Fiber pathways of the brain. Oxford University Press, New York
Schmahmann JD, Pandya DN, Wang R, Dai G, D'Arceuil HE, de Crespigny AJ, Wedeen VJ (2007) Association fibre pathways of the brain: parallel observations from diffusion spectrum imaging and autoradiography. Brain 130:630-653
Seeley WW, Menon V, Schatzberg AF, Keller J, Glover GH, Kenna H, Reiss AL, Greicius MD (2007) Dissociable intrinsic connectivity networks for salience processing and executive control. J Neurosci 27:2349-2356
Sexton CE, Kalu UG, Filippini N, Mackay CE, Ebmeier KP (2011) A meta-analysis of diffusion tensor imaging in mild cognitive impairment and Alzheimer's disease. Neurobiol Aging 32:2322 e2325-2318
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
Tabert MH, Manly JJ, Liu X, Pelton GH, Rosenblum S, Jacobs M, Zamora D, Goodkind M, Bell K, Stern Y, Devanand DP (2006) Neuropsychological prediction of conversion to Alzheimer disease in patients with mild cognitive impairment. Arch Gen Psychiatry 63:916-924
Tang PF, Ko YH, Luo ZA, Yeh FC, Chen SH, Tseng WY (2010) Tract-specific and region of interest analysis of corticospinal tract integrity in subcortical ischemic stroke: reliability and correlation with motor function of affected lower extremity. Am J Neuroradiol 31:1023-1030
Teipel SJ, Wegrzyn M, Meindl T, Frisoni G, Bokde AL, Fellgiebel A, Filippi M, Hampel H, Kloppel S, Hauenstein K, Ewers M (2012) Anatomical MRI and DTI in the Diagnosis of Alzheimer's Disease: A European Multicenter Study. J Alzheimers Dis
Torta DM, Cauda F (2011) Different functions in the cingulate cortex, a meta-analytic connectivity modeling study. Neuroimage 56:2157-2172
Tosun D, Schuff N, Mathis CA, Jagust W, Weiner MW (2011) Spatial patterns of brain amyloid-beta burden and atrophy rate associations in mild cognitive impairment. Brain 134:1077-1088
Tuch DS (2004) Q-ball imaging. Magn Reson Med 52:1358-1372
van den Heuvel M, Mandl R, Luigjes J, Hulshoff Pol H (2008) Microstructural organization of the cingulum tract and the level of default mode functional connectivity. J Neurosci 28:10844-10851
Voineskos AN, Rajji TK, Lobaugh NJ, Miranda D, Shenton ME, Kennedy JL, Pollock BG, Mulsant BH (2012) Age-related decline in white matter tract integrity and cognitive performance: a DTI tractography and structural equation modeling study. Neurobiol Aging 33:21-34
Vogt BA (2005) Pain and emotion interactions in subregions of the cingulate gyrus. Nat 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
Rev Neurosci 6:533-544
Wedeen VJ, Hagmann P, Tseng WY, Reese TG, Weisskoff RM (2005) Mapping complex tissue architecture with diffusion spectrum magnetic resonance imaging. Magn Reson Med 54:1377-1386
Wedeen VJ, Rosene DL, Wang R, Dai G, Mortazavi F, Hagmann P, Kaas JH, Tseng WY (2012) The geometric structure of the brain fiber pathways. Science 335:1628-1634 Zakzanis KK, Mraz R, Graham SJ (2005) An fMRI study of the Trail Making Test.
Neuropsychologia 43:1878-1886
Zhang Y, Schuff N, Jahng GH, Bayne W, Mori S, Schad L, Mueller S, Du AT, Kramer JH, Yaffe K, Chui H, Jagust WJ, Miller BL, Weiner MW (2007) Diffusion tensor imaging of cingulum fibers in mild cognitive impairment and Alzheimer disease. Neurology 68:13-19
Zimny A, Szewczyk P, Trypka E, Wojtynska R, Noga L, Leszek J, Sasiadek M (2011)
Multimodal imaging in diagnosis of Alzheimer's disease and amnestic mild cognitive impairment: value of magnetic resonance spectroscopy, perfusion, and diffusion tensor imaging of the posterior cingulate region. J Alzheimers Dis 27:591-601 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
Figure Legends
Fig 1. Shows tractography from diffusion spectrum imaging (A) superior cingulate bundle containg anterior segment in the anterior cingulate cortex (magenta), middle segment in the middle cingulate cortex (green), posterior segment in the posterior cingulate cortex (yellow); (B) inferior segment in the temporal cortex (amerald) ; (C) combined superior and inferior cingulate bundles; (D) callosal frontal fibers leading to dorsolateral prefrontal cortex (gold) and callosal motor fibers leading to primary motor cortex (red).
Fig. 2 Results of the multiple linear regression analysis of determining the significant contributors of white matter integrity of the investigated fiber tracts to the performance of different executive and memory functions. MCST= Modified Card Sorting Test, CTT= color trails test, LM= logical memory, VR= visual reproduction, aCB= anterior CB segment, mCB= middle CB segment, pCB= posterior CB segment, iCB= inferior CB segment, GFA= generalized fractional anisotropy, LH= left
hemisphere, R= right hemisphere. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
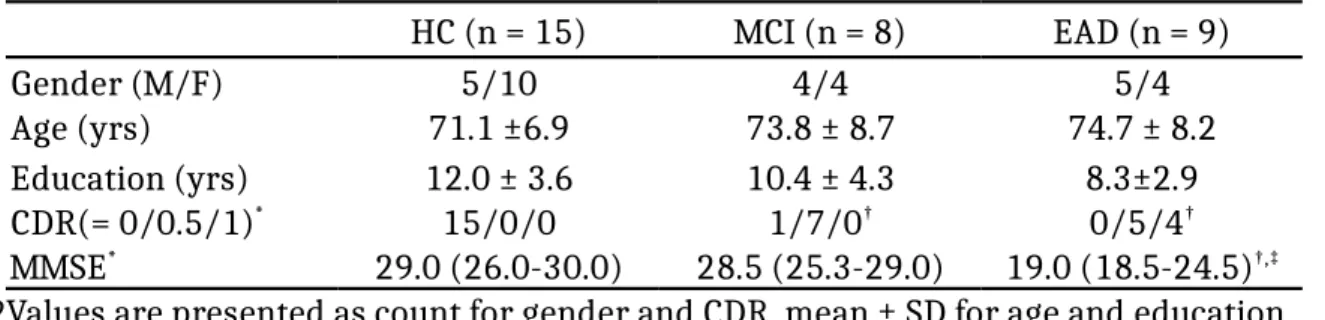
Table 1. Demographic data of the participants HC (n = 15) MCI (n = 8) EAD (n = 9) Gender (M/F) 5/10 4/4 5/4 Age (yrs) 71.1 ±6.9 73.8 ± 8.7 74.7 ± 8.2 Education (yrs) 12.0 ± 3.6 10.4 ± 4.3 8.3±2.9 CDR(= 0/0.5/1)* 15/0/0 1/7/0† 0/5/4† MMSE* 29.0 (26.0-30.0) 28.5 (25.3-29.0) 19.0 (18.5-24.5)†,‡
Values are presented as count for gender and CDR, mean ± SD for age and education, and median (25th -75th percentile) for MMSE.
M= male, F= female, MMSE= Mini-Mental State Examination, CDR= Clinical Dementia Rating, HC= healthy control, MCI= mild cognitive impairment, EAD= early Alzheimer’s disease. Kruskal-Wallis test was performed for three group comparison, *p < 0.05.
Mann-Whitney U was performed for follow-up paired-wise comparison with adjusted
significance level, †significantly different from HC, p<0.017; ‡significantly different from
MCI, p < 0.017. 1 2 3 4 5 6 7 8 9
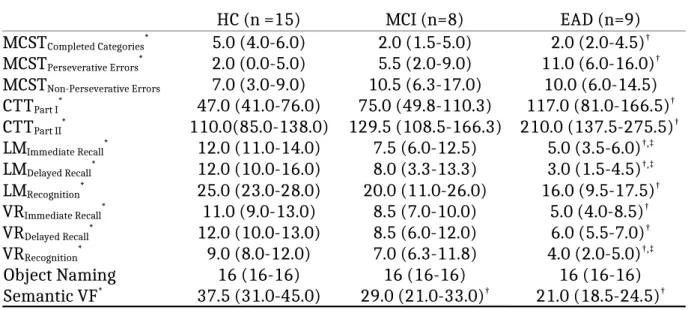
Table 2. Performance of neuropsychological tests of the participants HC (n =15) MCI (n=8) EAD (n=9) MCSTCompleted Categories* 5.0 (4.0-6.0) 2.0 (1.5-5.0) 2.0 (2.0-4.5)† MCSTPerseverative Errors* 2.0 (0.0-5.0) 5.5 (2.0-9.0) 11.0 (6.0-16.0)† MCSTNon-Perseverative Errors 7.0 (3.0-9.0) 10.5 (6.3-17.0) 10.0 (6.0-14.5) CTTPart I* 47.0 (41.0-76.0) 75.0 (49.8-110.3) 117.0 (81.0-166.5)† CTTPart II* 110.0(85.0-138.0) 129.5 (108.5-166.3) 210.0 (137.5-275.5)† LMImmediate Recall* 12.0 (11.0-14.0) 7.5 (6.0-12.5) 5.0 (3.5-6.0)†,‡ LMDelayed Recall* 12.0 (10.0-16.0) 8.0 (3.3-13.3) 3.0 (1.5-4.5)†,‡ LMRecognition* 25.0 (23.0-28.0) 20.0 (11.0-26.0) 16.0 (9.5-17.5)† VRImmediate Recall* 11.0 (9.0-13.0) 8.5 (7.0-10.0) 5.0 (4.0-8.5)† VRDelayed Recall* 12.0 (10.0-13.0) 8.5 (6.0-12.0) 6.0 (5.5-7.0)† VRRecognition* 9.0 (8.0-12.0) 7.0 (6.3-11.8) 4.0 (2.0-5.0)†,‡ Object Naming 16 (16-16) 16 (16-16) 16 (16-16) Semantic VF* 37.5 (31.0-45.0) 29.0 (21.0-33.0)† 21.0 (18.5-24.5)†
Values are presented as median (25th -75th percentile).
HC= healthy control, MCI= mild cognitive impairment, EAD= early Alzheimer’s disease, LM= logical memory, VR= visual reproduction, MCST= Modified Card Sorting Test, CTT= color trails test, VF= verbal fluency. Kruskal-Wallis test was performed for three group comparison, *p < 0.05. Mann-Whitney U test was performed for follow-up pair-wise comparison with adjusted significance level, †significantly different from HC, p<0.017; ‡significantly different from MCI, p < 0.017.
1 2 3 4 5 6 7 8 9 10