口服中藥槐花散治療有症狀的痔瘡-一個隨機、雙盲、安慰劑對照組之臨床試驗結果; Effects of oral TCM(Sophora Flower Formula) in the treatment of symptomatic hemorrhoids-Results of a Randomized, Double blind and Placebo-Controlled Trial
72
0
0
全文
(2)
(3)
(4) 中文摘要:. 口服中藥槐花散治療有症狀的痔瘡一個隨機、雙盲、安慰劑對照組之臨床試驗結果. 研究生:蔣鋒帆 指導教授: 陳汶吉 中國醫藥大學中西醫結合研究所 台中榮民總醫院大腸直腸外科,中西藥臨床試驗中心. 目的:評估以中藥槐花散治療有症狀的痔瘡療效與安全性. 材料與方法:我們應用雙盲、隨機、安慰劑對照組之前瞻性研究觀察評 估於台中榮總大腸直腸外科門診診斷為有症狀的痔瘡並接受內科保守 治療者在保守藥物治療基礎上用或不用中藥槐花散對有症狀的痔瘡患 者之臨床療效及安全性. 排除條件為第四度痔瘡,懷孕患者,曾接受骨 盆腔電療,明顯凝血功能異常或肝腎功能不佳者,並存大腸直腸疾病者 (如癌症, 克隆氏症, 潰瘍性大腸炎, 肛門廔管, 肛裂, 直腸炎或會 陰皮膚炎症等,六個月內曾接受非保守治療(如橡皮筋結紮術,紅外線 與冰凍療法等)或 或患者使用試驗用藥時間未超過半個療程者. 結果:共有45位有症狀的痔瘡患者參加此次臨床試驗,這些患者經第 三者, 本院中西臨床試驗中心經亂數分組為槐花散治療組與安慰劑 對照組兩組.槐花散治療組的平均年齡為37.34歲(SD=12.66), 男性有 18人, 女性5人.有不正常排便習慣的共12人, 其中9位須使用軟便劑. 在對照組中平均年齡為39.54(SD=13.89), 男性女性比為15比7位.12 位受試者有不正常排便的習慣, 其中需使用軟便劑有5位. 若以所有 主要症狀的分數來比較, 也就是將各次追蹤時間點時(基準點,7. i.
(5) 天,14天28天與56天)流血,疼痛,搔癢與腫脹感的主要症狀分數總和來 比較,在基準點時治療組肛門流血的總和分數為44分而對照組則為 36分, 疼痛方面則是26分比上18分, 肛門搔癢感與腫脹感是12分,20 分比上6分與18分。 兩組最主要的差別在痔瘡流血症狀的改善後較 少復發, 尤其是在服藥兩個至四個禮拜後最明顯優於對照組的 趨勢。 其他如疼痛,搔癢與腫脹感都能很快消退, 只要有傳統排便生 活改善與坐浴, 不管有無服用到有效成分的中藥。 結論: 根據以上的結果證實中藥槐花散可以幫助治療有症狀的痔瘡, 流血較傳統治療能更迅速停止與避免復發。 而其他症狀如疼痛搔 癢與腫脹感, 則在此研究不能顯示出其明顯療效。. 關鍵字:中藥 有症狀的痔瘡 生活品質 槐花散. ii.
(6) Effects of oral TCM(Sophora Flower Formula) in the treatment of symptomatic hemorrhoids – Results of a Randomized, Double blind and Placebo-Controlled Trial Objective: The purpose of this study was to assess the efficacy and safety of Sophora Flower Formula in the treatment of symptomatic hemorrhoids Methods: Under the design of a prospective, double-blind, randomized and placebo-controlled study, patients with symptomatic hemorrhoids were grouped into treatment group who received the formula when the placebo group take the capsule with starch only. The exclusion criteria were grade 4 hemorrhoids, pregnancy, radiation history, obvious impairment of liver and renal function, coexisting anal disease like ulcerative colitis, Crohns disease, anal fissure ,fistula and history of recent invasive procedure for hemorrhoids within six months. Results: There were 45 patients enrolled into this study, they were randomized by the third party. The average age in treatment group were 37.34±12.66, 18 male and 5 female. 12 patients had abnormal bowel movement. In the placebo group, age is 39.54±13.89, 15 male and 7 female. 12 patients had abnormal bowel movement. After 7 days treatment, the main symptoms among the treatment group were subsided 60.86% and improved in 26.08%. When the patients in placebo group 54.54% subsided and 18.18% had persist symptoms. The main superior effect is to maintain stop bleeding in the treatment group. On the other hand, anal pain, itching and tenesmus sensation improved equally in both group. Conclusion: According to this study, Sophora Flower Formula in the treatment of symptomatic hemorrhoids is effective, the main effect is to control and prevent recurrent hemorrhoids bleeding. Keyword:traditional medicine, symptomatic hemorrhoids, Quality of life. iii.
(7) 目錄: 中文摘要 英文摘要 生物醫學論文各章 第一章 前言. 1. 第二章 文獻探討. 2. 第三章 材料與方法. 5. 第四章 結果. 14. 第五章 討論. 27. 第六章 結論. 29. 參考文獻. 30. 附錄 槐花散HPLC分析. 55. 人體試驗委員會通過書. 56. 受試者同意書. 57. 生活飲食衛教書(中文版). 62. 生活飲食衛教書(英文版). 63. i.
(8) 圖目錄:. Figure 3.1 試驗藥物外觀. 8. Figure 3.2 試驗藥物的儲存. 9. Figure 4.1 Comparison of Global symptoms score between treatment and placebo group 19 Figure 4.2. Comparison of anal bleeding symptoms score between treatment and placebo group 20 Figure 4.3 Comparison of anal pain symptoms score between treatment and placebo group 21 Figure 4.4 Comparison of anal pruritus symptoms score between treatment and placebo group 22 Figure 4.5 Comparison of Tenesmus /Mass feeling symptoms score between treatment and placebo group 23 Figure 4.6 過敏患者. 25. ii.
(9) 表目錄: 表4.1 Patients Characteristics in treatment and placebo group. 15. 表4.2 The main Symptoms score after treatment. 16. 表4.3 Comparison of symptom score between Treatment and Placebo group. 18. iii.
(10) 第一章. 前言. 許多人都有痔瘡,雖然是良性疾病,但發作時卻使人相當難受, 坐立難安,嚴重影響生活品質。目前痔瘡的手術治療已多被探討,但並 非所有病患都願意接受手術或不適合手術,保守療法療效之證據強度也 不顯著。在此種情況下,患者之生活品質將受到影響。因此,我們想從 另一角度思考,是否可用別的方式來改善患者之症狀。 使用中藥槐花散治療痔瘡在民間自古即廣為流行,衛生署也早許 可上市,但中英文科學期刊皆無依較嚴謹的臨床研究證明其療效。故設 計此一研究,主要目的在於以嚴謹的態度探討: 中藥槐花散治療有症狀的痔瘡之療效評估. 1.
(11) 第二章 文獻探討 痔瘡是相當普遍的疾病,是由肛門區皮下動靜脈血管欉(Thulesius and Gjores 1973; Loder, Kamm et al. 1994)與由聯合縱走肌肉而來並 穿過內括約肌的帄滑肌共同構成(Thomson 1975; Hansen 1976),提供了 15~20% resting anal pressure 與肛門完整的閉合(Lestar, Penninckx et al. 1989),多項研究發現痔瘡患者有著較高的resting pressure(Read, Read et al. 1982; Sun, Read et al. 1990; Loder, Kamm et al. 1994)。 痔瘡的症狀包括疼痛、流血、脫出與肛門癢(Loder, Kamm et al. 1994), 多因痔瘡組織的腫大或腫大後易受傷的血管欉造成。 其成因目前沒有一個確切的結論, 通常認為是多因子造成的, 我們 詴著統結起來可以由肛門的精巧構造與功能來分析它。 第一, 肛門是主成分是細菌的糞便排出處, 又常受到創傷, 如過 硬的糞便, 衛生紙磨擦等。 所以必需要有一個很好的免疫力來防範細菌 的入侵, 而免疫力則由血液循環來輔助。 故當局部清潔不佳時或產生小 創傷時, 痔瘡容易惡化; 這也就是坐浴能加強局部清潔並避免因衛生紙, 或便秘產生過硬的糞便去磨擦損傷痔瘡區,而能降低局部發炎反應與血管 的過度腫脹並得到療效。 第二, 痔瘡協助提供肛門閉合主要的resting pressure, 故便秘或腹 壓增加常使得痔瘡惡化,更加腫脹肥厚。 痔疾有兩項基本特質,它是一種自我限制性的局部病變,而症狀輕 重不等,其症狀隨時日而緩解。常見治療包括內科治療: 藥物、坐浴與 飲食治療。與外科治療: 又可分為非手術治療的橡皮圈結紮法、局部注 射法等和手術治療。 對於外科治療常有文獻探討,可是少有文獻證據探討較不侵入性 2.
(12) 而安全的內科療法,而就這一方面的共識僅為建議增加飲食纖維、避免 便秘與坐浴。 已有臨床詴驗證據證實以含纖維如 psyllium 等去軟化大 便可以減輕疼痛與流血(Moesgaard, Nielsen et al. 1982),但其他證 據文獻卻無法證實其療效(Broader, Gunn et al. 1974; Webster, Gough et al. 1978; Perez-Miranda, Gomez-Cedenilla et al. 1996),因為 有時腹瀉反更易引起痔瘡發作, 所以在治療上仍有發展的空間。 而目前一方面由於治療準則證據不足,另外臨床上常見痔瘡的發作 與體質與身體狀況有很大的關係。中醫可改善患者體質與身體狀況而對 痔瘡有一定的治療作用已被廣泛探討。傳統上認為痔瘡形成的原因乃由 於 本虛: 肛門靜脈血管壁本身虛弱 氣滯血瘀: 加上經常久站、久坐或便秘,導致肛門周圍組織血液循環 障礙 溼熱下注: 飲食偏好辛辣及嗜酒會加重痔瘡的惡化 槐花散是理血劑中治療便血的常用方劑,清·汪昂〈翳方集解〉理 血之劑內有載,云:“治腸風臟毒下血”。由“槐花炒﹑側柏葉杵﹑荊 芥炒黑﹑枳殼炒,等分為末”組成。 大便下血,前人認為鮮紅者為腸 風,色紫暗者為臟毒。此由風邪熱毒或濕熱壅遏於腸胃血分,血滲腸道 所致。方中槐花清腸涼血止血,側柏葉助槐花涼血止血,荊芥舒風理血, 枳殼寬腸行氣。合用,既可涼血止血,又舒腸中風邪,故可用治上証。 現代研究,槐花含蘆丁等成分,能改善毛細血管功能,可防治其脆 性過大﹑通透性過高而引起的出血。槐花炒炭,蘆丁隨即分解,但仍能 明顯縮短出血時間及凝血時間,亦有止血效果。側柏葉和荊芥均能明顯 縮短出血時間及凝血時間,故能加強槐花止血之效。枳殼可使胃腸運動 的收縮節律增加而有力,有助消除大便秘結。總之,本方止血作用肯定, 較適合於肛腸出血。便血包括便後出血﹑便前下血﹑糞中夾血,本方證 以大便血色鮮紅﹑舌紅脈弦數為辨證要點。如大腸熱盛,可加黃連﹑黃 3.
(13) 蘗以清腸熱;下血多時,可加地榆以加強清腸止血作用;便血日久血虛 者,當加入補血之品。(陳修源 2005/2/14) 槐花散之出典應是許叔微〈普濟本事方〉。許南宋醫學家,字知可。 真州白沙(今江蘇儀征)人。卷第五,“腸風瀉血痔漏臟毒”載:“治腸 風臟毒,槐花散:槐花炒﹑柏葉爛杵焙﹑荊芥穗﹑枳殼去穰細切麩炒黃。 右修事了,方秤等分,細末。用清米飲調下二錢,空心食前服。” 中國傳統醫學使用槐花散(高. [31]. 峰 1997; 楊立成 2001; 陈华良. 2003)治療痔瘡已有很長的一段時間, 最近也常可在中醫雜誌期刊上看 到使用在痔瘡的治療。 通常認為槐花散方以槐花為主藥, 稟天地至陰 之性, 味苦性寒, 入肝及大腸經, 可清泄肝熱及大腸之火熱毒邪; 側 柏葉生而向西, 稟金兌之氣, 苦寒芳香能入血分, 養陰燥濕, 最涼 血分之熱; 槐花側柏相伍, 涼血止血之功更著; 荊芥為風病血病之要 藥, 借其輕揚宣泄之性以散瘀搜風; 枳殼寬腸利氣則邪毒易解。 四藥 所到之處俱可相及, 共奏清腸涼血, 疏風行氣之功, 故其效佳。 治療痔疾的目標以緩解症狀、解除痛苦為第一,其次再考慮如何根 治,防止復發,是以在治療方式的選擇上,以簡單、安全而有效者為優 先。 此研究希望以科學的方法驗證中醫藥既有之驗方口服槐花散治療 痔瘡的效用。. 4.
(14) 第三章. 材料與方法. 從2008年二月至五月, 在台灣台中榮民總醫院的大腸直腸外科門 診應用雙盲、隨機、安慰劑對照組之前瞻性研究觀察評估在保守藥物治 療基礎上用或不用中藥槐花散對有症狀的痔瘡患者之臨床療效及安全 性。我們得到本院人體詴驗委員會的審核通過施行此研究(編 號:C07072)。受詴者必頇簽署同意書,經診斷為痔瘡,並接受內科保守 治療,年齡大於18歲並能配合療程進行者。以下狀況將被排除於此詴驗 之外,包括第四度痔瘡,懷孕患者,曾接受過骨盆腔電療者,明顯凝血 功能異常或肝腎功能不佳者,併存大腸直腸疾病者如癌症、克隆氏症、 潰瘍性大腸炎、肛門廔管、肛裂、直腸炎或會陰皮膚炎症等,六個月內 曾接受非保守治療(如橡皮筋結紮術、紅外線與冰凍療法等), 或用藥 時間未超過半個療程者。 患者將接受飲食與生活型態衛教,排便習慣不佳者輔以藥物治療, 每日早晚4次各10分鐘的泡盆坐浴(建議時間為起床後、下午一點、七點 與睡前)。中藥槐花散或安慰劑藥物服用方式為每日早、中、晚服用三 次,每次2 gram(4顆), 治療間期為2週。. 5.
(15) 評估方式 一般症狀評估 包括流血,疼痛,搔癢與腫脹感, 於治療前、治療中及治療後 紀錄。評估時間點分別是基準點,7,14,28與56天。分數的紀錄為: 原主症狀為2分,其它症狀分數的記錄方式為3分:惡化或症狀變嚴 重;2分:症狀持續或無變化;1分:進步或僅存些微症狀:0分:無症狀。 這些症狀由單一觀察者紀錄評估。受詴者於初診與完成治療回診時 接受肛門鏡檢並記錄觀察所見。若受詴者有症狀持續超過14天,接 受其他治療或肛門鏡發現肛管炎性變化則視為治療失敗,症狀持 續。 實驗室觀測指標 受詴者接受服藥前及服藥後4周共兩次抽血檢查,包括血液常規 與肝腎凝血功能,有生育能力者將接受尿液驗孕,檢體並不留存 依 據台中榮總檢驗科標準程序處理而其檢驗報告將紀錄於台中榮總病 歷與檔案系統中。. 6.
(16) 藥品與治療 藥品 委託順天堂藥廠製成槐花散之藥丸及外型相似之安慰劑,膠囊 額外加上封口。 藥物之HPLC資料附於附錄。所有詴驗藥物包裝上 需註明製藥廠商,臨床詴驗編號,計劃主持人名稱,病患號碼,藥 物數量,服用方法,使用期限,批號,保存方式並標明“臨床詴驗 專用”。所有藥物存放於固定上鎖之地方並由專人保管。詴驗藥物 之有效期需註明於包裝上並確保如以到期則不可使用。詴驗藥物置 於乾燥陰涼處,溫度15至30。C的密閉藥罐。若患者需要藥物調 整排便則視情況開與Normacol 或biofermin。 隨機分配方式 委託台中榮民總醫院中西藥臨床詴驗中心分配藥物。 藥物 交付病人時於分配時當場拆開藥罐封口,取出一顆膠囊作為日 後追蹤備用。 飲食與生活習慣衛教 所有的病人都接受飲食與生活習慣,痔瘡肛門之照顧指導, 如附錄。. 7.
(17) 圖 3.1 詴驗藥物外觀. 8.
(18) 圖3.2 詴驗藥物的儲存. 9.
(19) 臨床不良反應之評估及處理: 安全性評估 1. 觀察生命徵象及臨床檢查結果是否出現重要改變 2. 實驗室數據變化 3. 不良反應事件評估 症狀性不良反應如上腹痛、胃燒灼感等胃腸道症狀 ,頭暈、 嗜睡、耳鳴等神經精神症狀 ,心悸、哮喘等循環呼吸系統 症狀 ;尿少、血尿等泌尿系統症狀 ,皮疹、水腫等。 4.回報方式 所有不良反應事件資料都詳細的建檔 (1)若發生任何諸如死亡、生命受到威脅,永久性傷殘,導致 必頇住院或延長目前的住院狀況、引起先天性的畸形、導 致其他種類癌症的發生或任何因為劑量過高而引起的結果 等嚴重不良反應事件(Serious Adverse Event)時,詴驗主 持人應於24小時內向人體詴驗委員會通報。 (2)一旦發生上述1以外之非嚴重副作用、詴驗主持人填寫不 良反應事件(Addverse Event Form)以個案向人體詴驗委 員會報告。. 10.
(20) 受詴者退出詴驗 受詴者於詴驗施行期間中,可隨時無條件撤回同意,退出詴驗將不 影響醫病關係或任何醫療上的正當權益。但退出詴驗後,仍得要求醫院 提供與受詴者已接受之詴驗相關之必要追蹤檢查。. 11.
(21) 詴驗流程:. 篩選病 人(基準 點). 治. 療. 期. Visit. V1. 追蹤 1,2. V2. 追蹤 3. 週. 0. 1,2. 4. 8. 天. 0. 7, 14±2. 28±2. 56±2. 病人簽署詴驗同意書. X. 納入/排除標準. X. 基本資料. X. 醫療病史. X. 身體評估檢查. X. 生命徵象檢查. X. 尿液驗孕檢查. X. 一般症狀評估表. X. 生活品質評估. X. X. 實驗室檢查數值. X. X. 病患的隨機分派. X. 調配分發詴驗藥品. X. X. X. X. 不良反應事件 收回未服用藥品. X. 完成詴驗/提早結束. X. 生命徵象檢查包括 血壓(收縮壓及舒張壓)、脈搏、身高及體重。. 12. X.
(22) 統計方法 由於我們研究觀察的指標是每位病人皆有的痔瘡症狀, 每個組至少要 有20個病人以上, 其Sample power 證據力等級將到達90%[16]. 連續性變量 (continuous variables) 將提供觀察個數、帄均數、 標準差等敘述統計量。類別性變量 (categorical variables) 則提供 次數與其對應之比例。所有統計檢定將以雙邊 (two-sided),及顯著水 準為0.05之方式執行。療效指標的主要分析母體為intent-to-treat population。 對於受詴者基本資料(demographic) 與各評估指標的基準值 (baseline value),如年齡、體重等連續性變量將以治療組別為因子的 無母數Mann-Whitney U 進行詴驗組與對照組之組間比較。又如性別等 類別性變量則以chi-square test進行組間比較。. 13.
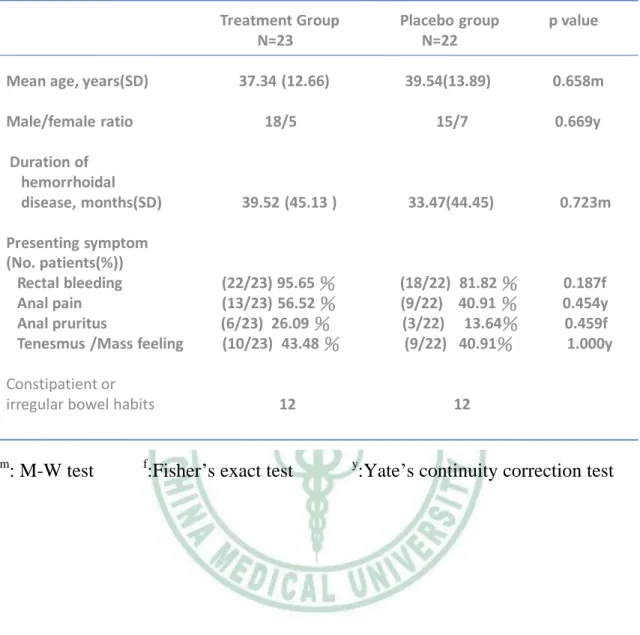
(23) 第四章. 結果. 共有45位有症狀的痔瘡患者參加此次臨床詴驗, 其中有 40 位的主 要症狀是肛門出血, 其餘主要與伴隨症狀則是肛門疼痛 22. 位, 肛門搔. 癢 9 位與腫脹感的 19 位. 這些患者經第三者, 本院中西臨床詴驗中心 經亂數分組為槐花散治療組與安慰劑對照組兩組. 兩組患者的基本資料 可見於table 1. 槐花散治療組的帄均年齡為37.34歲 (SD=12.66), 男性有 18人, 女性5人. 其帄均痔瘡的病史為39.52個月(SD=45.13).. 22位以流血. 為主要表現症狀, 而疼痛,搔癢與腫脹感各有 13,6,10人. 有不正常排便 習 慣 的 共 12 人 , 其 中 9 位 頇 使 用 軟 便 劑 .. 在對照組中帄均年齡為. 39.54(SD=13.89), 男性女性比為15比7位. 其帄均痔瘡的病史為33.47個月 (SD=44.45). 以流血為主要表現症狀的有 18 位, 而疼痛,搔癢與腫脹感 各有 9,3,9 人. 12位受詴者有不正常排便的習慣, 其中需使用軟便劑有 5位. 兩組的痔瘡症狀是相對應的, 都以出血為主要的表現, 治療組有肛門搔癢 的比例則較對照組稍高.. 14.
(24) Table 1. Patients Characteristics in treatment and placebo group. Mean age, years(SD) Male/female ratio Duration of hemorrhoidal disease, months(SD). Presenting symptom (No. patients(%)) Rectal bleeding Anal pain Anal pruritus Tenesmus /Mass feeling Constipatient or irregular bowel habits. m. : M-W test. Treatment Group N=23. Placebo group N=22. p value. 37.34 (12.66). 39.54(13.89). 0.658m. 18/5. 15/7. 0.669y. 39.52 (45.13 ). 33.47(44.45). (22/23) 95.65 % (13/23) 56.52 % (6/23) 26.09 % (10/23) 43.48 %. (18/22) (9/22) (3/22) (9/22). 12. 81.82 % 40.91 % 13.64% 40.91%. 0.723m. 0.187f 0.454y 0.459f 1.000y. 12. f. y. :Fisher’s exact test. :Yate’s continuity correction test. 15.
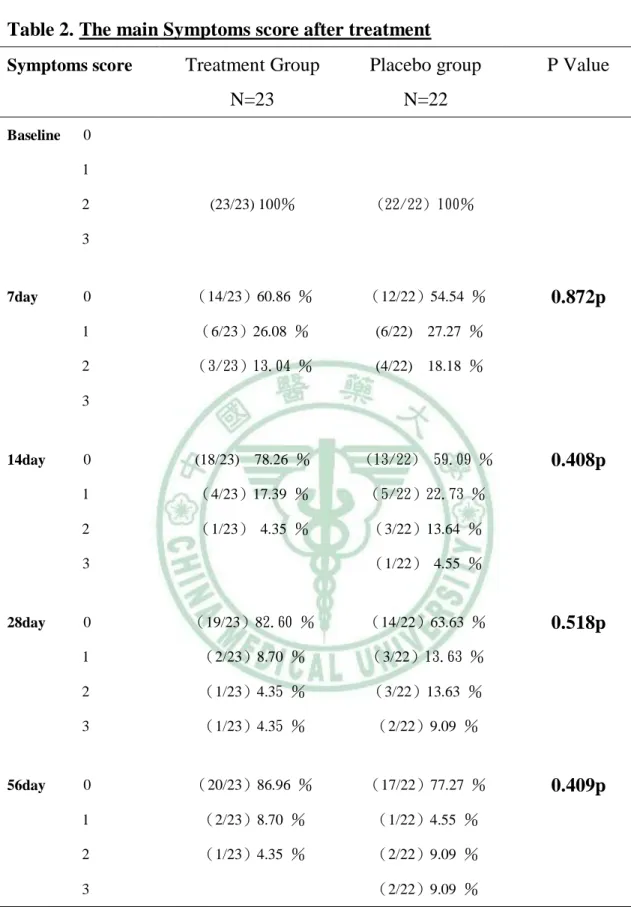
(25) Table 2. The main Symptoms score after treatment Treatment Group. Placebo group. N=23. N=22. (23/23) 100%. (22/22) 100%. 0. (14/23)60.86 %. (12/22)54.54 %. 1. (6/23)26.08 %. (6/22) 27.27 %. 2. (3/23)13.04 %. (4/22) 18.18 %. 0. (18/23) 78.26 %. (13/22) 59.09 %. 1. (4/23)17.39 %. (5/22)22.73 %. 2. (1/23) 4.35 %. (3/22)13.64 %. Symptoms score. Baseline. P Value. 0 1 2 3. 7day. 0.872p. 3. 14day. (1/22) 4.55 %. 3. 28day. 56day. 0.408p. 0. (19/23)82.60 %. (14/22)63.63 %. 1. (2/23)8.70 %. (3/22)13.63 %. 2. (1/23)4.35 %. (3/22)13.63 %. 3. (1/23)4.35 %. (2/22)9.09 %. 0. (20/23)86.96 %. (17/22)77.27 %. 1. (2/23)8.70 %. (1/22)4.55 %. 2. (1/23)4.35 %. (2/22)9.09 % (2/22)9.09 %. 3. P: Pearson Chi-sauare test. 16. 0.518p. 0.409p.
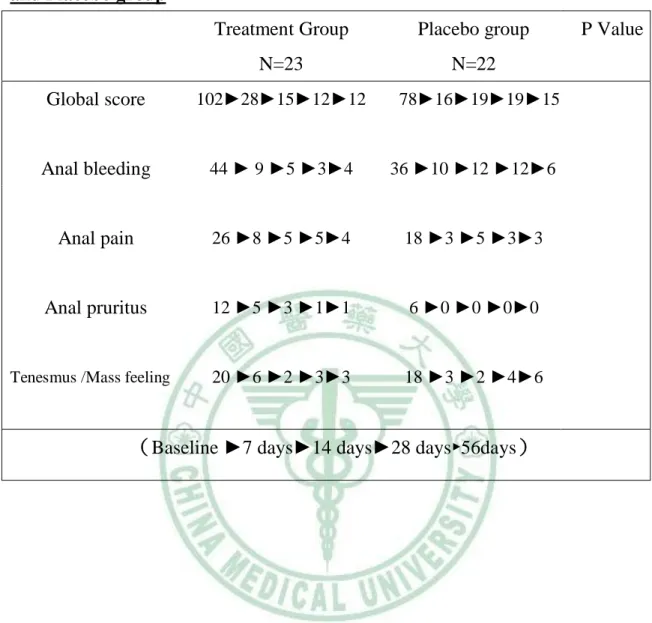
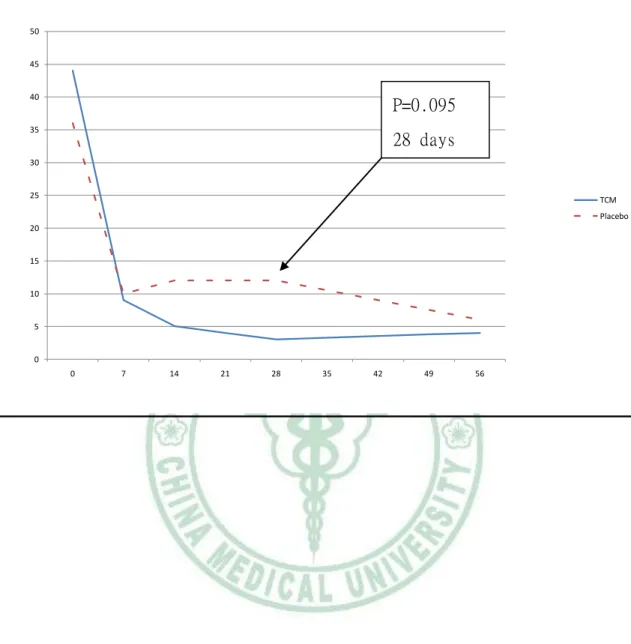
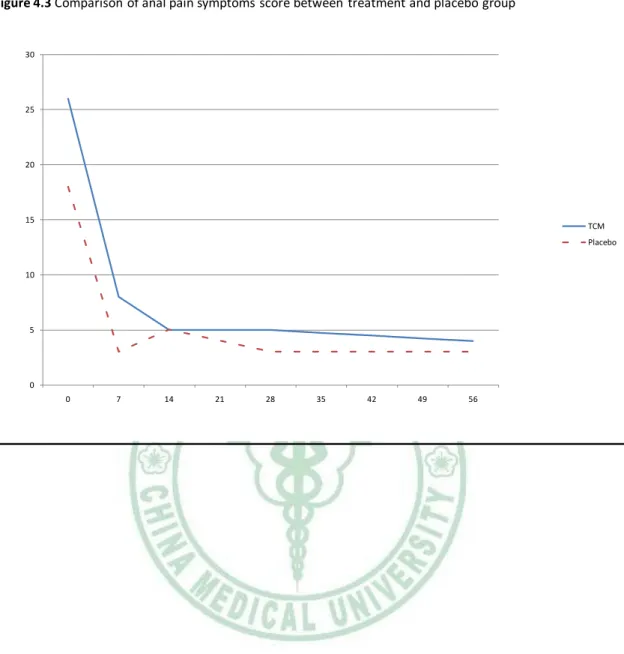
(26) 以受詴者最主要的症狀來分析比較, 在基準點時都以2分為起始判 斷, 在治療後7天已有60.86%症狀消除而26.08%有進步. 對照傳統治療的 結果, 54.54%症狀消除且18.18%的受詴者無轉好跡象,症狀持續. 14天後 則治療組有78.26%無症狀, 對照組則有40.81%殘留症狀. 治療後追蹤的 結果在28天時對照組9.09%症狀惡化, 56天時亦有13.05%治療組痔瘡再發. 帄均主症狀第一次消除的時間在治療組是3.06天, 當對照組是4.47天. 若以所有主要症狀的分數來比較, 也就是將各次追蹤時間點時(基準 點,7天,14天28天與56天)流血,疼痛,搔癢與腫脹感的分數總和來比較, 可 以Table 3來表示. 在基準點時治療組肛門流血的總和分數為44分而對照 組則為36分, 疼痛方面則是26分比上18分, 肛門搔癢感與腫脹感是12 分,20分比上6分與18分。 兩組最主要的差別在痔瘡流血症狀的改善後較 少復發, 尤其是在服藥兩個至四個禮拜後最明顯優於對照組的趨勢。 其 他如疼痛,搔癢與腫脹感都能很快消退, 只要有傳統排便生活改善與坐浴, 不管有無服用到有效成分的中藥。 將症狀分數總和兩組相比較可見得治療組較佳 的低復發趨勢 (FIGURE 1), 流血症狀的改善是其中最有意義的(FIGURE 2). 根據以上的結果證實中藥槐花散可以幫助治療有症狀的痔瘡, 流血 較傳統治療能更迅速停止與避免復發。 而其他症狀如疼痛搔癢與腫脹感, 則在此研究不能顯示出其明顯療效。. 17.
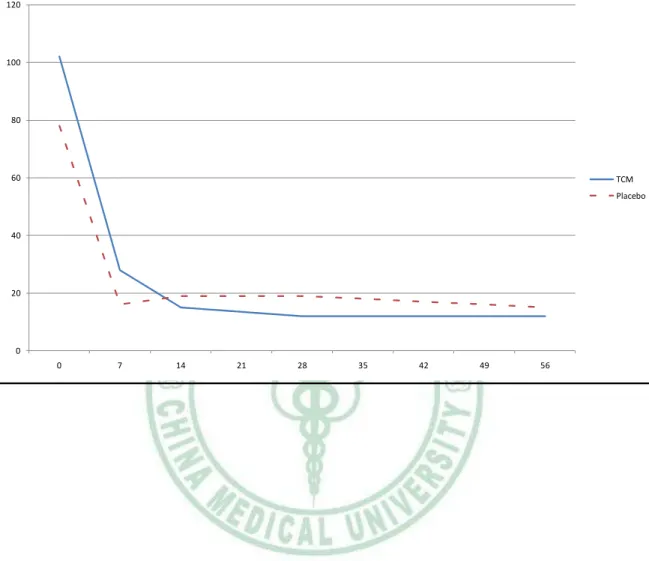
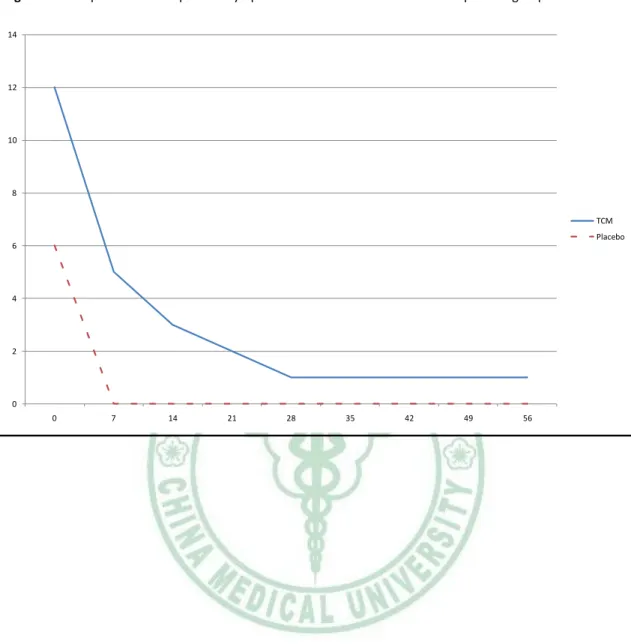
(27) Table 3. Comparison of global and main symptom score between Treatment and Placebo group Treatment Group. Placebo group. N=23. N=22. Global score. 102►28►15►12►12. Anal bleeding. 44 ► 9 ►5 ►3►4. 36 ►10 ►12 ►12►6. Anal pain. 26 ►8 ►5 ►5►4. 18 ►3 ►5 ►3►3. Anal pruritus. 12 ►5 ►3 ►1►1. 6 ►0 ►0 ►0►0. 20 ►6 ►2 ►3►3. 18 ►3 ►2 ►4►6. Tenesmus /Mass feeling. 78►16►19►19►15. (Baseline ►7 days►14 days►28 days►56days). 18. P Value.
(28) Figure 4.1 Comparison of Global symptoms score between treatment and placebo group. 120. 100. 80. 60. TCM Placebo. 40. 20. 0 0. 7. 14. 21. 28. 35. 19. 42. 49. 56.
(29) Figure 4.2 Comparison of anal bleeding symptoms score between treatment and placebo group. 50. 45. 40. P=0.095. 35. 28 days. 30. 25. TCM Placebo. 20. 15. 10. 5. 0 0. 7. 14. 21. 28. 35. 20. 42. 49. 56.
(30) Figure 4.3 Comparison of anal pain symptoms score between treatment and placebo group. 30. 25. 20. 15. TCM Placebo. 10. 5. 0 0. 7. 14. 21. 28. 35. 21. 42. 49. 56.
(31) Figure 4.4 Comparison of anal pruritus symptoms score between treatment and placebo group 14. 12. 10. 8 TCM Placebo 6. 4. 2. 0 0. 7. 14. 21. 28. 35. 22. 42. 49. 56.
(32) Figure 4.5 Comparison of Tenesmus /Mass feeling symptoms score between treatment and placebo group 25. 20. 15. TCM Placebo 10. 5. 0 0. 7. 14. 21. 28. 35. 23. 42. 49. 56.
(33) 退出詴驗 共3位參與詴驗者退出, 有兩位服藥未達一周, 用藥時間未超過半 個療程。在詴驗進行中有一位38歲女性患者在服藥後第九天發生了全身蕁 麻疹、呼吸急促與胸悶的全身性過敏反應, 經緊急通報人體詴驗委員會 與本院中西藥臨床詴驗中心開放此位患者的分組資料,證實為安慰劑對照 組。 患者在皮膚科住院三日後狀況穩定出院,診斷為由於季節環境引起之 非特異性蕁麻疹。 由於肛門仍有間歇出血的狀況,患者於第四週回診時, 我們為患者安排了橡皮筋結紮術。 由於此位患者之分組資料被開放,她 被排除於此一詴驗分析之外。. 24.
(34) 圖4.6 過敏患者. 25.
(35) 毒副作用 在所有的受詴者中並沒有發現在血液與尿液常規、肝腎與凝血功能等 生化檢查於治療前後有異常變化的情形, 其中包括了一位輕微腎功能不 佳的患者(creatinine 1.7mg/dl (0.7- 1.4) )。 在使用槐花散與安慰劑治療的 患者中各有一位敘述非特異性的副作用包括服藥後10 分鐘會有倦怠頭暈 的現象,但都迅速消除,受詴者當時血壓心跳並無明顯變化。. 26.
(36) 第五章 討論 痔瘡是相當普遍的疾病。 臨床上常見痔瘡與體質或身體狀況有很大 的關係,如熬夜 飲酒 暴飲暴食等常會加重或誘發痔瘡發作。 換言之若 能加速身體或免疫力的調節則能降低局部痔瘡的過度充血而使痔瘡這個 臨床症狀早日恢復。 傳統中醫藥如槐花散可改善患者體質與身體狀況, 對痔瘡有一定的治療作用早已被廣泛探討,衛生署並以治療痔瘡為其適應 症許可上市。 但中英文科學期刊皆無依較嚴謹的臨床研究證明其療效。 故設計此一研究,應用雙盲、隨機、安慰劑對照組之前瞻性研究觀察評估 在保守藥物治療基礎上用或不用中藥槐花散對有症狀的痔瘡患者之臨床 療效及安全性,主要目的在於以嚴謹的態度來探討之。 我們納入研究的兩組受詴者不管是治療組或是安慰劑對照組, 均是 較年輕的患者。 他們沒有嚴重的構造改變如嚴重第三度或第四度痔瘡, 因為肥厚鬆弛下降的組織將容易被排便時這個動作或被糞便磨過所受傷 並導致腫脹,流血甚至形成栓塞痔。 在臨床上一般認為這類患者應以較 積極的方式處理包括手術或橡皮筋結紮, 硬化劑注射等方式去減少過度 增生的組織, 或因處置後局部反應將鬆弛下降的組織拉回(Haas, Fox et al. 1984)。 在我們的臨床詴驗受詴者中,以男性居多, 他們較以痔瘡急性發作 表現。 尤其男性骨盆會陰肌肉發達而相對肛管狹長肌肉張力較大者, 稍 微的痔瘡組織腫脹就很容易有明顯的症狀。在這個族群中我們發現現有的 飲食生活排便習慣改變與坐浴皆能有效快速的緩解症狀。 使用中藥槐花散治療組的受詴者中,比起單純只增加飲食纖維攝取, 調整生活與坐浴的安慰劑對照組能有較低的症狀復發, 特別是出血, 且 無明顯的副作用。 其可能的機轉應與調節全身與痔瘡區的細胞素而使血 27.
(37) 管通透性,凝血機轉與淋巴血流壓力獲得改善有關(Szlavy, Repa et al. 1990; Mentes, Gorgul et al. 2001)。 至於服用藥物去治療痔瘡, 目前文獻可以搜尋到的有MPFF(an oral micronized flavonoid compound (Daflon , Les Laboratoires Servier, Gidy, France)(Wadworth and Faulds 1992; Cospite 1994; Godeberge 1994; Meyer 1994; Buckshee, Takkar et al. 1997; Ho and Seow-Choen 2000; Misra and Parshad 2000; La Torre and Nicolai 2004). 與Dobesilate(Szlavy, Repa et al. 1990; Mentes, Gorgul et al. 2001) 兩種。 至於中藥或槐花散則並沒有較完整或證據等級較高的文獻探討。 我們是一個醫學中心且是大腸直腸癌的轉介醫院, 患者常因肛門流 血而來門診希望排除大腸直腸癌的可能性, 所以出血的患者較肛門癢與 腫脹疼痛為多。 原另構想痔瘡手術後的症狀控制與減輕的研究, 由於醫 學倫理與證據醫學的考量, 故先行設計此一研究,下一階段應可考慮施 行於手術後與懷孕的患者使用。 由於痔瘡是一個良性自限性疾病, 臨床上以能夠快速消除症狀並減 少復發, 且副作用少的方式為最佳, 口服藥物合併局部治療與生活飲食 的調整應是很容易被接受的(Misra and Imlitemsu 2005)。 目前證據醫學針 對痔瘡 流血 的保 守治 療建 議是 增加纖 維攝取 避免 便秘 (Alonso-Coello, Guyatt et al. 2005) 而肛門不適與搔癢則可以坐浴來緩解(Shafik 1993) 至於口服藥物, 在Daflon與Dobesilate等藥物之外,我們提供一個新的 選擇,使用中藥槐花散亦初步証實可在治療有症狀的痔瘡得到幫助症狀控 制與低復發的趨勢,而這個結果是由一個雙盲、隨機、安慰劑對照組之前 瞻性研究的結果所支持,包括主觀的病患感受與客觀的肛門鏡檢。 至於如何針對痔瘡在更大規模,更長時間,不同劑量或切除手術後的 症狀控制,不同人種的反應去證實此配方的療效與安全性有待更進一步的 研究。 28.
(38) 結論 從這一個臨床詴驗, 我們觀察到使用槐花散在保守藥物治療基礎 上去處理有症狀的痔瘡的確是傾向有效而安全的, 而對於防止痔瘡流血 再復發的成效最明顯。 使用此非侵犯性,接受度高的口服藥物治療, 能 得到比傳統治療更有助益的成果。. 29.
(39) 參考文獻. Alonso-Coello, P., G. Guyatt, et al. (2005). "Laxatives for the treatment of hemorrhoids." Cochrane Database Syst Rev(4): CD004649. BACKGROUND: Symptomatic hemorrhoids are a common medical condition, which increase in prevalence in women during pregnancy and postpartum. Although the evidence appears to be inconclusive, narrative reviews and clinical practice guidelines recommend the use of laxatives (and fiber) for the treatment of hemorrhoids and relief of symptoms. This is due to their safety and low cost. OBJECTIVES: To evaluate the impact of laxatives on a wide range of symptoms in people with symptomatic hemorrhoids. SEARCH STRATEGY: We searched the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library Issue 2, 2005), MEDLINE (1966 to 2005), EMBASE (1980 to 2005), CINAHL (1982 to 2005), BIOSIS, and AMED (Allied and Alternative Medicine Database), for eligible trials (including conference proceedings). We sought missing and additional information from authors, industry, and experts in the field. SELECTION CRITERIA: We selected all published and unpublished randomised controlled trials that compared any type of laxative to placebo or no therapy in any patient population. DATA COLLECTION AND ANALYSIS: Two authors independently screened studies for inclusion and retrieved all potentially relevant studies. Data were extracted from studies that met 30.
(40) our selection criteria on study population, intervention used, pre-specified outcomes, and methodology. We extracted methodological information for the assessment of internal validity: existence and method of generation of the randomization schedule, and method of allocation concealment; blinding of caregivers and outcomes assessors; numbers of and reasons for participants lost to follow up; and use of validated outcome measures. MAIN RESULTS: Seven randomised trials enrolling a total of 378 participants to fiber or a non-fiber control were identified. Meta-analyses using random-effects models showed that laxatives in the form of fiber had a beneficial effect in the treatment of symptomatic hemorrhoids. The risk of not improving hemorrhoids and having persisting symptoms decreased by 53% in the fiber group (risk reduction (RR) 0.47, 95% CI 0.32 to 0.68). These results are compatible with large treatment effects regarding prolapse, pain, itching, although the pooled analyses showed a tendency toward no-effect for these parametres. The effect on bleeding showed a significant difference in favour of the fiber (RR 0.50, 95% CI 0.28 to 0.89). Studies including data on multiple follow ups (usually after six weeks and three months) showed consistent results over time. However, we have to stress two possible limitations of this review: the risk of publication bias, and only moderate study quality. AUTHORS' CONCLUSIONS: The 31.
(41) use of fiber shows a consistent beneficial effect for relieving overall symptoms and bleeding in the treatment of symptomatic hemorrhoids. Broader, J. H., I. F. Gunn, et al. (1974). "Evaluation of a bulk-forming evacuant in the management of haemorrhoids." Br J Surg 61(2): 142-4. Buckshee, K., D. Takkar, et al. (1997). "Micronized flavonoid therapy in internal hemorrhoids of pregnancy." Int J Gynaecol Obstet 57(2): 145-51. OBJECTIVE: To assess the safety, efficacy and acceptability of a micronized flavonoid formulation in the treatment of internal hemorrhoids of pregnancy. METHODS: In an open study on hospital outpatients, we studied therapy with micronized diosmin 90% and hesperidin 10% for a median of 8 weeks before delivery and 4 weeks after delivery, in 50 women with acute hemorrhoids. The outcome measures were symptoms and signs of hemorrhoids; adverse effects; and acceptability of treatment. RESULT: On intention to treat analysis, 66% (95% confidence interval, range 79.1-52.9) had relief from acute symptoms by the 4th day; 53.6% (95% confidence interval, range 70-37.1, P < 0.001) fewer patients had relapse in the antenatal period. Treatment was well accepted, and did not affect pregnancy, fetal development, birth weight, infant growth and feeding. CONCLUSION: In the short term, micronized diosmin 90% and hesperidin 10% is 32.
(42) safe, acceptable, and effective in the treatment of hemorrhoids of pregnancy. Cospite, M. (1994). "Double-blind, placebo-controlled evaluation of clinical activity and safety of Daflon 500 mg in the treatment of acute hemorrhoids." Angiology 45(6 Pt 2): 566-73. One hundred patients with a history of hemorrhoidal disease and suffering from an acute hemorrhoidal attack were randomized into two parallel groups and treated with Daflon 500 mg* (D500) or placebo (PL) under double-blind conditions. Daflon 500 mg was administered at the dosage of three tablets bid the first four days and two tablets bid the following three days. Overall improvement of symptoms was greater in the D500 group than in the PL group, from D2 up to D7. The clinical severity of proctorrhagia, anal discomfort, pain, and anal discharge diminished in both groups but to a greater extent in the D500 group (P < 0.001 for all parameters except protorrhagia, P = 0.006). Inflammation, congestion, edema, and prolapse were more markedly improved in the D500 group than in the PL group. Duration and severity of the current hemorrhoidal episode, as assessed by patient self-evaluation, were less important in the D500 group as compared with previous episodes. Use of analgesics and topical medications diminished in both groups, with a major reduction in the D500 group from D4 (P < 0.001). Acceptability was 33.
(43) good in both groups: no patient experienced major side effects. In summary, treatment with D500 resulted in a quicker and more pronounced relief of signs and symptoms of acute hemorrhoids than with the placebo. Godeberge, P. (1994). "Daflon 500 mg in the treatment of hemorrhoidal disease: a demonstrated efficacy in comparison with placebo." Angiology 45(6 Pt 2): 574-8. Hemorrhoidal disease (HD) is a trophic disorder of the anal canal characterized by recurrent, self-resolving acute episodes. The author reports the results of a double-blind, placebo-controlled trial of the efficacy of Daflon 500 mg in the treatment of acute and chronic symptoms of hemorrhoids. One hundred and twenty outpatients (54 men, 66 women) suffering from an acute episode of HD during the previous two months were included. They received Daflon 500 mg (group D, n = 60) or placebo (group P, n = 60) two tablets daily for two months. The patients were examined at entry (T0) and at two months (T2). At T0, the two groups did not differ in terms of age, sex, weight, height, history of symptoms of HD; 7 patients were excluded from analysis because of treatment failure (group D, n = 2; group P, n = 3), or lost to follow-up (group P, n = 2). In group D, 40% of patients had an attack during the trial with a mean duration of 2.6 days and 34.
(44) a mean severity of 1.1 scored on a scale from 1 to 3. These values were significantly different (P < 0.01) from the corresponding values in the P group: 70%, 4.6 days and 1.6 respectively. Each symptom and sign was scored on a scale of severity. The overall symptom score, scored from 0 to 15, decreased from 6.6 (group D) and 6.1 (group P) (NS) to 1.1 and 4.0 respectively (P < 0.01) at the end of treatment.(ABSTRACT TRUNCATED AT 250 WORDS) Haas, P. A., T. A. Fox, Jr., et al. (1984). "The pathogenesis of hemorrhoids." Dis Colon Rectum 27(7): 442-50. The structure of the anal canal was examined in histology slides. Hemorrhoids are normal features of the human anatomy. They are pads that bulge into the lumen. Hemorrhoids have three parts: 1) the lining, which can be mucosa or anoderm; 2) the stroma with blood vessels, smooth muscle, and supporting connective tissue; and 3) the anchoring connective tissue system, which secures the hemorrhoids to the internal sphincter and the conjoined longitudinal coat. The anchoring and supporting connective tissue system deteriorates with aging. The hemorrhoids not only bulge, but descend into the lumen. This becomes observable in the third decade of life, with individual differences. The veins become distended as they lose their support. The descended loose lining becomes more sensitive to pressure from 35.
(45) straining and to trauma from the stool. There can be a stasis in the veins, with clot formations and swelling, or erosions of the lining, with bleeding. The hemorrhoids become symptomatic. Hansen, H. H. (1976). "[The importance of the Musculus canalis ani for continence and anorectal diseases (author's transl)]." Langenbecks Arch Chir 341(1): 23-37. The functional morphology of the M. canalis ani is described. Hitherto this muscle has not been studied in detail. The M. canalis ani is located inside of the M. sphincter ani internus and reaches through the spatium submucosum et subcutaneum of the analcanal. This muscle is part of a described "organ of continence". Its importance in the course of anorectal disease is shown. Ho, Y. H. and F. Seow-Choen (2000). "Randomized clinical trial of micronized flavonoids in the early control of bleeding from acute internal haemorrhoids." Br J Surg 87(12): 1732-3. La Torre, F. and A. P. Nicolai (2004). "Clinical use of micronized purified flavonoid fraction for treatment of symptoms after hemorrhoidectomy: results of a randomized, controlled, clinical trial." Dis Colon Rectum 47(5): 704-10. PURPOSE: The aim of this study was to evaluate if the 36.
(46) combination of micronized purified flavonoid fraction with short-term routine antibiotic and anti-inflammatory therapy was better at reducing the intensity of postoperative symptoms and wound bleeding after a Milligan-Morgan's open hemorrhoidectomy than antibiotic and anti-inflammatory treatment alone. METHODS: Fifty patients were randomly assigned to receive routine antibiotic and anti-inflammatory treatment alone (control patients) or a combination of micronized purified flavonoid fraction with identical antibiotic and anti-inflammatory treatment (micronized purified flavonoid fraction patients). The evolution of symptoms (pain, tenesmus, pruritus, and bleeding) during the postoperative period was assessed by means of patients' self-questionnaires. Each symptom was scored on a graded severity scale from 0 to 3, daily during the first three days of the immediate postoperative period, then at regular intervals (about every 14 days) until postoperative day 60. A global score for evaluation of each postoperative symptom and bleeding was used. The global score for each symptom was the sum of scores for each patient over the study period. The global score for each symptom was compared between the two groups with the Mann-Whitney U test. RESULTS: No significant differences in age, gender distribution, and stage of disease between the two groups were noticed at baseline. Posthemorrhoidectomy symptoms 37.
(47) were relieved more rapidly in the micronized purified flavonoid fraction group; during the first three postoperative days, the global score for each symptom was significantly more reduced in the micronized purified flavonoid fraction group. The global scores for each symptom are as follows: pain after 3 days, 6.16 (SD = 1.9) in the control group vs. 3.48 (SD = 1.8) in the micronized purified flavonoid fraction group (P < 0.0001); tenesmus, 5.36 (SD = 1.8) in the control group vs. 1.48 (SD = 1.5) in the micronized purified flavonoid fraction group (P < 0.0001); pruritus, 4.04 (SD = 1.9) in the control group vs. 1.84 (SD = 1.4) in the micronized purified flavonoid fraction group (P < 0.0001); bleeding, 4.4 (SD = 2.1) in the control group vs. 2.0 (SD = 1.3) in the micronized purified flavonoid fraction group (P < 0.0001). A significant difference (P < 0.0001) between groups was also shown in favor of micronized purified flavonoid fraction patients when global scores were calculated over the entire study period (60 days). CONCLUSION: Micronized purified flavonoid fraction used in combination with short-term antibiotic and anti-inflammatory treatment can reduce both the duration and extent of postoperative symptoms and wound bleeding following hemorrhoidectomy. Lestar, B., F. Penninckx, et al. (1989). "The composition of anal basal pressure. An in vivo and in vitro study 38.
(48) in man." Int J Colorectal Dis 4(2): 118-22. The maximal anal basal pressure (MABP) was measured with probes of 0.3, 1, 2 and 3 cm diameter in 21 subjects, 60 years old, without anal pathology. The components of MABP were analyzed by inducing a maximal internal sphincter (IS) relaxation, taking pressure measurements in the conscious state and during narcosis with curarization. In seven cases pressure measurements were done on isolated anorectum after abdominoperineal rectum amputation. MABP increases with probe diameter before as well as during anaesthesia with curarization. The contribution of the striated sphincter tonic activity is constant within the range of probe diameters used. At rest, i.e. when the 0.3 cm diameter pressure recording probe is used, 30% of MABP is made up by striated sphincter tonic activity, 45% of it is due to nerve induced IS activity, 10% to purely myogenic IS activity and 15% can be attributed to the expansion of the haemorrhoidal plexuses. Although MABP is mainly based on active forces generated by the smooth and striated sphincter apparatus, the presence of the anal cushions is essential for perfect anal continence, as they have to fill the gap within the IS ring to hermetically close the anal canal. The global IS activity, contributing 50-60% of MABP at rest, can completely be inhibited by a maximal rectoanal inhibitory reflex. Stretching of passive elements starts at 1 cm anal distension, but 39.
(49) steeply increases thereafter, accounting for 65% of the MABP at 3 cm anal distension. It is deduced that optimal stool diameter is about 2 cm. Loder, P. B., M. A. Kamm, et al. (1994). "Haemorrhoids: pathology, pathophysiology and aetiology." Br J Surg 81(7): 946-54. Haemorrhoidal disease is the consequence of distal displacement of the anal cushions, which are normal structures with an important role in continence. The causes of haemorrhoidal disease are unknown; constipation and abnormal bowel habit are commonly blamed despite largely contrary evidence. The most consistently demonstrated physiological abnormality is an increased maximum resting anal pressure. Most evidence points to this being a secondary phenomenon rather than the cause of haemorrhoidal disease. Among the many unexplored areas are the function of the longitudinal muscle in relation to haemorrhoidal disease, the description and pharmacological responsiveness of the anal subepithelial muscle, and the clinical role of specific pharmacological agents that might reverse some of the observed physiological changes. Mentes, B. B., A. Gorgul, et al. (2001). "Efficacy of calcium dobesilate in treating acute attacks of hemorrhoidal disease." Dis Colon Rectum 44(10): 1489-95. 40.
(50) PURPOSE: A randomized, double-blind, controlled study was conducted to investigate the efficacy of oral calcium dobesilate therapy in treating acute attacks of internal hemorrhoids. METHODS: Twenty-nine well-documented adult patients with first- or second-degree internal hemorrhoids were treated with calcium dobesilate for two weeks, while16 patients received only a high-fiber diet to serve as control. Both symptoms and anoscopic inflammation were scored on a scale from 0 to 2 before (T0) and two weeks after treatment (T2). RESULTS: A success rate of 86.21 percent with cessation of bleeding plus lack of severe anitis anoscopically at two weeks were achieved with calcium dobesilate. The pretreatment symptom score of 2 fell significantly to 0.45 +/- 0.13, and the pretreatment anitis score of 1.69 +/- 0.09 fell to 0.55 +/- 0.12 at T2 (P = 0.0001 for both comparisons). The symptom and anoscopic inflammation scores obtained with calcium dobesilate treatment were also significantly better than those with diet only (P = 0.0017 and P = 0.0013, respectively). CONCLUSION: Together with recommendations about diet and bowel discipline, oral calcium dobesilate treatment provides an efficient, fast, and safe symptomatic relief from acute symptoms of hemorrhoidal disease. This symptomatic healing is associated with a significant improvement in the anoscopically observed inflammation. 41.
(51) Meyer, O. C. (1994). "Safety and security of Daflon 500 mg in venous insufficiency and in hemorrhoidal disease." Angiology 45(6 Pt 2): 579-84. Daflon 500 mg is a new flavonoid vasoprotector venotonic agent whose active principle is micronized and contains 90% diosmin and 10% flavonoids expressed as hesperidin. In animal studies, the safety of Daflon 500 mg is shown by an LD50 (lethal dose 50) of more than 3 g/kg, ie, 180 times the daily therapeutic dose, as well as by the absence of any toxic effect after repeated oral dosing for thirteen and twenty-six weeks, using a dose representing 35 times the daily dosage, in the rate and primate. Daflon 500 mg has no mutagenic action nor any significant effect on reproductive function. Gastrointestinal tolerance is good when administered orally in the rat. Transplacental passage and passage into breast milk are minimal. In the rat, 0.003% of the administered dose has been found in each fetus and 1% in breast milk. Clinical trials fulfill international scientific requirements and have collected more than 2850 patients treated with Daflon 500 mg at the dosage of two tablets per day for six weeks to one year. The proportion of patients with side effects (10% of those treated), essentially of a gastrointestinal or autonomic nature and leading to a rate of only 1.1% trial dropouts, is less than described in 225 patients given a placebo (13.9%) in 42.
(52) controlled trials. Satisfactory clinical acceptability already confirmed in the short term was equally found in long-term treatment. Hemodynamic parameters (systolic and diastolic blood pressure) as well as laboratory parameters (hematology, liver and renal function, metabolic) were uninfluenced even by prolonged treatment for one year at the dosage of two tablets per day.(ABSTRACT TRUNCATED AT 250 WORDS) Misra, M. C. and Imlitemsu (2005). "Drug treatment of haemorrhoids." Drugs 65(11): 1481-91. Drug treatment for various anorectal conditions has been known since ancient times. Today, modern as well as traditional drugs are being increasingly used in all grades of symptomatic haemorrhoids. These drugs (oral and local) are used as a part of conservative management or as an adjuvant to invasive outpatient procedures. Flavonoids, in the new formulation of micronised purified flavonoid fraction (MPFF) or as part of the ancient traditional medicine derivative of the Ginkgo tree, are used for relief of acute symptoms (for control of bleeding and re-bleeding in all grades of haemorrhoids). MPFF has been recommended for control of acute bleeding in patients waiting for a definitive outpatient treatment. Similarly, better known drugs such as calcium dobisilate (used in diabetic retinopathy and chronic venous insufficiency), nitrates and nifedipine have 43.
(53) also been effective and well tolerated in the medical treatment of haemorrhoids. However, drug treatment is not aimed at curing haemorrhoids. The prime objective of drug therapy is to control the acute phase (bleeding) so that definitive therapy (banding, injection sclerotherapy, infrared photocoagulation, cryotherapy or surgery) can be scheduled at a convenient time. Misra, M. C. and R. Parshad (2000). "Randomized clinical trial of micronized flavonoids in the early control of bleeding from acute internal haemorrhoids." Br J Surg 87(7): 868-72. BACKGROUND: Patients with acute bleeding from internal haemorrhoids often have to be referred by the general practitioner to the surgeon for definitive treatment with invasive outpatient procedures. At the initial consultation, patients frequently seek postponement of immediate surgery to a more convenient time. Effective and rapid non-invasive control of acute bleeding could be of practical use in scheduling surgery to a time convenient to both patient and surgeon. METHODS: In a 90-day randomized, double-blind study treatment with a micronized purified flavonoid fraction (MPFF) was compared with placebo, in 100 outpatients who presented for treatment of acute internal haemorrhoids of less than 3 days' duration. The primary endpoint was cessation of bleeding on the 44.
(54) third day of treatment. RESULTS: Of 50 patients randomized to each group, acute bleeding ceased by the third day in 40 (80 per cent) who received MPFF compared with 19 (38 per cent) who had placebo (P < 0.01). Mean(s.d. ) duration of acute bleeding from onset to cessation of 4.9(1.6) days was 2.1 (95 per cent confidence interval 1.2-2.9) days less than that in patients receiving placebo (P < 0.01). Continued treatment in patients with no bleeding prevented a relapse in 30 of 47 patients, compared with 12 of 30 receiving placebo (P < 0.05). CONCLUSION: Patients with acute internal haemorrhoids treated with MPFF had rapid cessation of bleeding and a reduced risk of relapse. This could be of value in the more convenient timing of treatment with invasive outpatient procedures. Moesgaard, F., M. L. Nielsen, et al. (1982). "High-fiber diet reduces bleeding and pain in patients with hemorrhoids: a double-blind trial of Vi-Siblin." Dis Colon Rectum 25(5): 454-6. Perez-Miranda, M., A. Gomez-Cedenilla, et al. (1996). "Effect of fiber supplements on internal bleeding hemorrhoids." Hepatogastroenterology 43(12): 1504-7. BACKGROUND/AIMS: The aim of this study is to assess prospectively the effect of fiber additions on internal bleeding hemorrhoids. MATERIALS AND METHODS: 45.
(55) Fifty patients with bleeding internal hemorrhoids are studied and randomized in two groups. Patients in the study group were treated with a commercially available preparation of Plantago Ovata and those in the control group were treated with a placebo. Endoscopy was performed on every patient before and after treatment to establish: a) the degree of hemorrhoidal prolapse, b) the number of congested hemorrhoidal cushions and c) contact bleeding hemorrhoids. RESULTS: During the 15 days of treatment, the average number of bleeding episodes was 4.8 +/3.8 for the study group versus 6.4 +/- 3 for the control group (n.s.). During the following 15 days, it decreased to 3.1 +/- 2.7 in the study group versus 5.5 +/- 3.2 (p < 0.05) in the control group and in the last 10 days of treatment a further reduction to 1.1 +/- 1.4 was found in the study group versus 5.5 +/- 2.9 (p < 0.001). The number of congested hemorrhoidal cushions diminished from 2.6 +/- 1 to 1.6 +/- 2.2 after fiber treatment (p < 0.01) and no differences were found in the control group. In the fiber group, hemorrhoids bled on contact in 5 out of 22 patients before treatment and in none after treatment; no differences were found in the control group. No modification of the degree of prolapse was observed after treatment. CONCLUSION: Addition of dietary fiber may improve internal bleeding hemorrhoids although with no immediate effect. Fiber addition should be ensured in patients who refuse 46.
(56) invasive treatment, waiting for a more defined form of treatment, or with contraindications. Read, M. G., N. W. Read, et al. (1982). "A prospective study of the effect of haemorrhoidectomy on sphincter function and faecal continence." Br J Surg 69(7): 396-8. The effect of haemorrhoidectomy on anal sphincter manometry and continence to faeces and rectally infused saline was investigated in 24 unselected patients with third-degree haemorrhoids. Haemorrhoidectomy resulted in the abolition of ultra-slow waves and significant decreases in basal and squeeze pressures, though these were reduced to normal values from abnormally high levels. Pressures remained at normal levels up to a year after surgery. An association was found between mucous soiling following surgery and an abnormally low postoperative squeeze pressure. There was no alteration in the function of the recto-anal inhibitory reflex following surgery. Only two patients developed incontinence to rectally infused saline for the first time following surgery. The addition of four-finger dilatation of the anal canal to the operative procedure did not cause any significant differences in sphincter manometry. Shafik, A. (1993). "Role of warm-water bath in anorectal conditions. The "thermosphincteric reflex"." J Clin 47.
(57) Gastroenterol 16(4): 304-8. Why anorectal pain is relieved by sitting in a warm-water bath was investigated in 18 healthy volunteers and 28 patients with painful anorectal disease (18 patients with fissures and 10 with hemorrhoids). Investigations consisted of measuring rectal and interstitial sphincter temperature, rectal and rectal neck pressures, and electromyographic activity of both the external and internal anal sphincters before and after the subjects sat in a warm-water bath at temperatures of 40, 45, and 50 degrees C for 10 min each time. Pain relief was more evident and lasted longer at higher bath temperatures. The rectal and interstitial sphincter temperatures were unchanged before and after bath in both the healthy volunteers and patients. The rectal neck pressure and internal and sphincter electromyographic activity dropped significantly in the bath, but increased gradually to pretest levels 25-70 min after exiting the bath. The higher the bath temperature, the greater the drop in rectal neck pressure and internal sphincter EMG activity, and the longer the time needed to return to pretest levels. Pain relief after Sitz bath seems to be the result of internal anal-sphincter relaxation with a resulting diminution of the rectal neck pressure. The relaxation of the internal sphincter following the warm bath postulates a relationship, but direct action was ruled out. A 48.
(58) neural pathway through a "thermosphincteric reflex" seems most likely. Sun, W. M., N. W. Read, et al. (1990). "Hypertensive anal cushions as a cause of the high anal canal pressures in patients with haemorrhoids." Br J Surg 77(4): 458-62. Anorectal manometry and electrophysiology studies were conducted in 25 men with non-prolapsing haemorrhoids, ten men with prolapsing haemorrhoids, and 20 age-matched normal men. Mean(s.e.m.) minimum basal pressures were significantly higher in patients with non-prolapsing haemorrhoids than in normals (61(5) versus 43(7) cmH2O; P less than 0.05) or patients with prolapsing haemorrhoids (55(4) cmH2O; P less than 0.05). There were no significant differences in maximum basal pressures and maximum squeeze pressures. During rectal distension, all normal subjects showed relaxation in all anal channels. However, 92 per cent of patients with non-prolapsing haemorrhoids and 40 per cent of patients with prolapsing haemorrhoids showed no relaxation in the outer anal channels, even when relaxation occurred in the inner anal channels; internal sphincter electrical slow waves were suppressed and the integrated electrical activity of the external sphincter had returned to predistension values. Maximum residual anal pressures during balloon distension were significantly higher in 49.
(59) patients with non-prolapsing haemorrhoids than normals (75(7) versus 45(7) cmH2O; P less than 0.01), or patients with prolapsing haemorrhoids (53(3) cmH2O; P less than 0.05). When subjects increased intra-abdominal pressure rectal pressure was significantly higher in patients with non-prolapsing haemorrhoids than in normal subjects (157(10) versus 105(15) cmH2O; P less than 0.05), but not in patients with prolapsing haemorrhoids (126(14) cmH2O). Resting anal cushion pressures in patients with non-prolapsing or prolapsing haemorrhoids were much higher than normal capillary or venous pressure and significantly higher than those recorded in normals (median 35, 35 versus 10 cmH2O; P less than 0.0001). Pressures recorded during coughing (60, 60 versus 30 cmH2O) and straining (78, 80 versus 55 cmH2O) were also significantly higher (P less than 0.0001) in patients than in normals. Pressures after straining were higher than those recorded before (38 versus 29 cmH2O; P less than 0.05) in 60 per cent of patients but no normal subjects and took 18-36 s to return to baseline. This study suggests that the abnormally high pressures in the anal canal in patients with haemorrhoids may be related to an increased vascular pressure in the anal cushions. Szlavy, L., I. Repa, et al. (1990). "Calcium dobesilate (CLS 2210) protects the myocardium in early acute myocardial infarction: a preliminary randomized, 50.
(60) double-blind, placebo-controlled study of its effects on biochemical markers." J Cardiovasc Pharmacol 15(1): 89-95. To determine the effect of calcium dobesilate (CLS 2210) on biochemical markers of acute myocardial infarction, and thereby assess its action in limiting myocardial necrosis, this compound was administered intravenously by a randomized, double-blind technique to 23 of 41 patients suffering their first infarction. The remaining 18 patients received a placebo. Administration was begun within 3 h of onset of symptoms and continued for 72 h. Before and during treatment, blood samples were taken for measurement of the serum activity of creatine kinase and its isoenzyme MB, and the serum and urinary concentrations of myoglobin and glycosaminoglycans. Serum creatine kinase and serum and urinary myoglobin were significantly lower in the CLS 2210-treated patients than in the placebo patients throughout the 72 h (p = 0.01, 0.005, and 0.004, respectively). Serum creatine kinase MB and serum glycosaminoglycan in the CLS 2210 patients were initially higher than in the controls, but fell below the control levels between the 40th and 55th hours (p = 0.89 and 0.02, respectively). The glycosaminoglycan urinary concentrations alone were higher in the CLS 2210 group than in the placebo group throughout (p = 0.0005). These findings suggest that CLS 2210 reduces myocardial infarct size in human subjects, as it is 51.
(61) already known to do in animals. Thomson, W. H. (1975). "The nature of haemorrhoids." Br J Surg 62(7): 542-52. An anatomical and clinical study aimed at uncovering factors likely to be helpful in understanding the true nature of haemorrhoids is described. The main finding was of specialized 'cushions' of submucosal tissue lining the anal canal; it is argued that piles are merely the result of their displacement. Thulesius, O. and J. E. Gjores (1973). "Arterio-venous anastomoses in the anal region with reference to the pathogenesis and treatment of haemorrhoids." Acta Chir Scand 139(5): 476-8. Wadworth, A. N. and D. Faulds (1992). "Hydroxyethylrutosides. A review of its pharmacology, and therapeutic efficacy in venous insufficiency and related disorders." Drugs 44(6): 1013-32. Hydroxyethylrutosides is a standardised mixture of semisynthetic flavonoids, mainly mono-, di-, tri-, and tetrahydroxyethylrutosides, which acts primarily on the microvascular endothelium to reduce hyperpermeability and oedema. In patients with chronic venous insufficiency or diabetes, hydroxyethylrutosides improves microvascular perfusion and microcirculation, and reduces erythrocyte aggregation. The preparation also has a 52.
(62) possible protective effect on the vascular endothelium. In short to medium term placebo-controlled studies (up to 6 months) hydroxyethylrutosides therapy improved signs and symptoms of chronic venous insufficiency, including venous insufficiency associated with pregnancy and lymphoedema, and was well tolerated. However, the long term effects of hydroxyethylrutosides administration have yet to be demonstrated. The preparation also alleviated symptoms in patients with severe haemorrhoids, although there were no corresponding objective improvements. Hydroxyethylrutosides administration has been associated with reductions in retinal vascular permeability in patients with diabetic retinopathy but has no apparent effect on signs of retinal haemorrhage, although a reduction in oedema and haemorrhage has been reported in other patients receiving oral hydroxyethylrutosides in the acute phase of central retinal vein occlusion. There are only limited effective pharmacological treatment options for patients with chronic venous insufficiency or lymphoedema, and hydroxyethylrutosides clearly improves signs and symptoms of these disorders. While its role in diabetic retinopathy and haemorrhoids requires some clarification, hydroxyethylrutosides therapy shows promise as a useful additional option for the management of oedema and other symptoms of chronic 53.
(63) venous insufficiency. Webster, D. J., D. C. Gough, et al. (1978). "The use of bulk evacuant in patients with haemorrhoids." Br J Surg 65(4): 291-2. Fifty-three patients with symptomatic haemorrhoids have been studied in a double-blind cross-over trial of a bulk forming agent (ispaghula husk) against a placebo. Although only 11 per cent of patients ocmplained of constipation, a significant benefit in symptoms and improved bowel habit was demonstrated. 高. 峰, 孫. 江., 黃如華. (1997). "槐花散加味治療肛門下 鮮血 360 例." Fujian Journal of TCM 28(6): 2.. 陳 修 源 . (2005/2/14). " 槐 花 散 的 出 典 ." from http://www.mintong.com.tw/art/list.asp?unid=456. 楊立成, 于., 閆玉印. (2001). "槐花散合腸風湯治療內痔出 血 156 例." 中国民间疗法 9(8): 1. 陈华良 (2003). "加味槐花散治疗内痔 162 例疗效观察." 云 南中医中药杂志 24(6): 2.. 54.
(64) 附錄 槐花散HPLC分析. 55.
(65) 人體詴驗委員會通過書. 56.
(66) 台中榮民總醫院人體詴驗計畫受詴者同意書 本自願書由受詴者本人簽署 本自願書由法定代理人簽署 計畫名稱:口服中藥槐花散治療有症狀的痔瘡 計畫執行單位:中西藥臨床詴驗中心 計畫主持人姓名:蔣鋒帆 緊急聯絡人:蔣鋒帆 受詴者姓名:. 職稱:主治醫師 職稱:主治醫師. 性別:. 年齡:. 24小時緊急電話:0919710446 病歷號碼:. 通訊地址:. 法定代理人姓名:. 電話:. 性別:. 年齡:. 通訊地址:. 電話:. (醫療法第七十九條規定:受詴者為無行為能力或限制行為能力人,應得其法 定代理人之同意) 敬啟者: 為增進醫學新知及提高醫療技術,進而服務社會,承蒙您自願接受(法定代 理人同意)為本詴驗計畫之主要受詴對象,為能使您完全瞭解本計畫施行人體詴 驗部分主要內容及方法,敬請詳閱以下各項資料。倘若您對本詴驗進行的方法 及步驟仍有疑問,本計畫有關人員願意提供進一步解釋,以期您能充分瞭解。. 本自願書以下列方式敘述理由:□ 口述. 57. □ 筆述.
(67) 一、詴驗目的及方法: 許多人都有痔瘡,雖然是良性疾病,但發作時卻使人相當難受,坐立難安,嚴 重影響生活品質。目前痔瘡的手術治療已多被探討,但並非所有病患都願意接受手 術或不適合手術,而保守療法方面其療效之證據強度也不顯著。在此種情況下,患 者之生活品質將受到影響。因此,我們想從另一角度思考,是否可用別的方式來改 善患者之症狀。 臨床上常見痔瘡的發作與體質與身體狀況有很大的關係。 中醫對 痔瘡有一定的治療作用,並可改善患者體質與身體狀況已被廣泛探討。而使用中藥 槐花散治療痔瘡在民間自古即廣為流行,衛生署也早許可上市,但中英文科學期刊 皆無依較嚴謹的臨床研究證明其療效。故設計此一研究,主要目的在於以嚴謹的態 度探討: 1. 中藥槐花散治療有症狀的痔瘡之療效評估 2. 痔瘡患者生活品質〈Quality of life〉改善之評估 研究方法: 我們將研究評估在保守藥物治療基礎上,花費約兩個月的時間在台中榮總大腸 直腸外科門診收集約200人使用與追蹤中藥槐花散治療有症狀的痔瘡患者其臨床療 效及安全性。如果您符合進行詴驗條件,您將被分配到治療組或安慰劑組:我們的 研究方法分為兩組,您可能加入治療組接受槐花散加泡盆,但也可能是對照組服用 的是安慰劑。在服藥期間我們也會按時檢查您身體的狀況。此藥物為中醫之經方, 經長期之使用經驗並未發現有嚴重之副作用。 您有可能拿到不含有效成分的安慰劑作為您的詴驗用藥,各有一半一半的機 會,您或您的醫師都不會知道您拿的是槐花散或安慰劑。在追蹤詴驗期間,我們將 與你聯絡,以收集有關您在詴驗中的經驗或是健康及生活品質問卷。 您完全是自 願參加本詴驗,您可以拒絕參加,或加入後也可在任何時候終止參加,不會對您應 有權益有何影響。 治療組:槐花散 + 泡盆 安慰劑組:安慰劑 + 泡盆 觀查組: 不願服用中藥但同意症狀資料收集 服用方式:每日早、中、晚服用三次,每次2 gram(4顆), 服用2週 泡盆:每日早晚4次各10分鐘,共2週(建議時間為起床後、下午一點、七 58.
(68) 點與睡前) 評估方式以一般症狀評估表〈治療前、治療中及治療後〉生活品質評估 表 參與資格: 1. 於台中榮總大腸直腸外科門診診斷為痔瘡並接受內科保守治療者 2. 您必頇同意遵守計劃書的規定,並且在詴驗進行前簽署受詴者同意書 3. 年齡 > 18 4. 您必頇配合醫師安排的回診時間 如果您有下列任何情形,您將無法參與本實驗 1. 第四度痔瘡(痔瘡脫出無法推回) 2. 懷孕患者 3. 曾接受骨盆腔電療 4. 明顯凝血功能異常或肝腎功能不佳者. 5. 並存大腸直腸疾病者(如癌症, 克隆氏症, 潰瘍性大腸炎, 肛門廔管, 肛 裂, 直腸炎或會陰皮膚炎症等) 7. 6個月內曾接受非保守治療(如橡皮筋結紮術,紅外線與冰凍療法等). 二、預期詴驗效果:可能有下列成效 1. 症狀改善 2. 生活品質改善 三、可能產生之併發症、副作用、危險及其處理方法: 此次詴驗之中藥為中醫之固有成方,已服用於人體上百年,並未有嚴重副 作用之報告。現也為中醫臨床常用方,但仍有可能造成一些副作用發生如煩熱、 咽乾口燥、舌紅。醫院將盡力維護貴受詴者在詴驗施行期間之權益,並善盡醫 療上必要之注意。若於詴驗期間發現影響受詴者權利、安全與福祉之相關最新 資訊,會盡快聯絡並告知受詴者。 四、詴驗可能造成的不適: 您將在服食中藥(槐花散或安慰劑)前及服藥後四周於門診接受身體評估, 生理檢查和抽血檢查<血液常規與肝腎功能,約10cc〉兩次與服食中藥。若您是 59.
(69) 有生育能力之婦女亦將接受尿液驗孕。檢體並不留存,依據台中榮總檢驗科標準 程序處理而其檢驗報告將紀錄於台中榮總病歷與檔案系統中。由於對胎兒的影 響未知故懷孕婦女將被排除併建議服藥期間避孕.此除此之外,您將於第一,二 與第八週被電話訪問要求回答一些有關您的醫病史、健康狀況及生活品質問題 以幫助評估。 五、其他可能之治療方法及說明: 您不一定要參與本詴驗才能治療您的疾病,仍有其他治療方式,包括手術 及橡皮筋結紮術等。您的詴驗主持醫師會與您討論這些治療與方法。 六、詴驗經費來源及所有參與詴驗之機構: 台中榮民總醫院大腸直腸外科,中西藥臨床詴驗中心 中國醫藥大學中西結合研究所(專題討論研究並提供監督建議) 順天堂製藥廠提供藥物 七、受詴者之禁忌、限制與應配合之事項: 如果您符合進入詴驗資格,您將花費約兩個月的時間完成一次回診與三次電話 追蹤。詴驗所得資料可能將發表於學術性雜誌,但受詴者姓名將不會公布,同時 受詴者之隱私將給予絕對之保密。受詴者於詴驗過程中可隨時退出本計畫,並請 暫時停止其他藥物服用或與您的醫師討論。 八、本詴驗受詴者之權益將受到下列保護: (一) 本計畫所用藥物由順天堂製藥廠提供,醫院將盡力維護貴受詴者在詴驗施 行期間之權益,並善盡醫療上必要之注意。如造成任何傷害該代理商願負全 責,本院並願協助受詴人向代理商索取賠償。 順天堂製藥廠總公司 地址:台北市羅斯福路二段11號3樓 消費者服務專線: (02)2327-8185 E-mail :[email protected] (二)如依本研究所訂詴驗計畫,足以證明因本案處置而使您的健康受到任何傷 害,本醫院願依法負損害賠償責任。 (三)本詴驗已經得到醫院人體詴驗委員會審查通過,該委員會的審查重點即是 對受詴者是否有適當的保護。 (四)詴驗所獲得資料之使用或發表,醫院將對受詴者之隱私(例如:姓名、得 以辨識受詴者身分之照片等資料)絕對保密。 (五)貴受詴者於詴驗施行期間中,可隨時無條件撤回同意,退出詴驗。但退出 60.
(70) 詴驗後,仍得要求醫院提供與受詴者已接受之詴驗相關之必要追蹤檢查。 (六)受詴者退出詴驗,將不影響醫病關係或任何醫療上的正當權益。. 九、若您對於參與本臨床詴驗的相關權益有所疑問,您可與本院人體詴驗委員會 之承辦人聯絡,聯絡電話:04-23592525轉4006,傳真:04-23592525轉4408 ,E-mail:[email protected] 十、經本詴驗計畫主持人或其代理人向本人說明上列事項後,本人已明瞭其內 容;有關本詴驗之疑問,亦得到詳細解答,本人係在完全自主,未被詐欺、 脅迫或利誘之情形下,同意參加本詴驗,並知悉在詴驗期間本人有權隨時無 條件退出詴驗,且本藥物對孕婦及胎兒作用不明,正值生育年齡而有懷孕可 能之婦女不宜參加本詴驗,如參加詴驗中途懷孕應主動對主持人說明並退出 詴驗。詴驗內容如有變更,將先取得本人同意。 受詴者簽名:. 日期:. (法定代理人簽名:. 日期:. 計畫主持人簽名:. 日期:. 說明人簽名:. 日期:. 61. ).
(71) 生活飲食衛教書(中文版). 生活飲食衛教書(英文版). 62.
(72) Suggestions for Local Care of the Anus. 1. Diet: Eat a balance diet and avoid ”stimulating” food such as alcohol, hot peppers, and hard to chew foods. 2. Keep Bowel Movement(BM)Schedule: Avoid constipation, and increase intake of fruits, vegetables, honey, or milk. 3. Adequate Exercise:. Take laxatives if necessary.. avoid keeping the same posture too long such as. standing, sitting, squatting.. Increase exercises in relaxing/constricting. anal sphincter. Do not spend extra time on the commode during BM . 4. Avoid using excessive force while wiping afterwards. 5. Washing your bottom is more important than washing your face.. Use. warm water to wash your anus after BM . 6. Patients with hemorrhoids, anal fistula, anal fissures should have Sits bath (soaking the anus in warm water)frequently. This helps to improve blood flow and improve symptoms. Best when done after a BM. There is no limitation on the frequency. The more the merrier. Sits bath method – use a large basin of a bath tub and fill it warm water that is deep enough to cover the entire anus area. Sit in the basin/tub for 5 to 10 minutes Wipe dry gently afterwards. 7. If you continue to have blood in the stool or have poor bowel habits, seek the care of a physician.. 63.
(73)
數據

+7

Outline
相關文件
SF12219A#9 陳得源 一項第 3 期、隨機分配、雙盲、安 慰劑對照詴驗,評估 Belimumab 搭
In the fourth quarter of 2003, 4 709 acts of deed were notarized on sales and purchases of real estate and mortgage credits, representing a variation of +19.6% in comparison with
4-7 The photocopy of the letter of agreement between Business Incubation Center of Feng Chia University and the applied company over the operations and cultivations.. 4-8
MR CLEAN: A Randomized Trial of Intra-arterial Treatment for Acute Ischemic Stroke. • Multicenter Randomized Clinical trial of Endovascular treatment for Acute ischemic stroke in
A Phase 2/3 Multicenter, Open-label, 3-arm, 2-stage Randomized Study of ASP2215 (Gilteritinib), Combination of ASP2215 Plus Azacitidine and Azacitidine Alone in the Treatment
4-7 The photocopy of the letter of agreement between Business Incubation Center of Feng Chia University and the applied company over the operations and cultivations.. 4-8
Therefore, the current research evaluated oral health condition, salivary flow, and halitosis across the different stages of leprosy treatment and compared the results with those
Figure 3: Comparison of the partitioning of the hemisphere effected by a VQPCA-based model (left) and a PPCA mixture model (right). The illustrated boundaries delineate regions of
