BRIEF REPORT
Nationwide surveillance of antimicrobial resistance
among
Haemophilus influenzae and Streptococcus
pneumoniae in intensive care units in Taiwan
S.-S. Jean&P.-R. Hsueh&W.-S. Lee&H.-T. Chang&M.-Y. Chou&I.-S. Chen&J.-H. Wang&C.-F. Lin&J.-M. Shyr&W.-C. Ko&
J.-J. Wu&Y.-C. Liu&W.-K. Huang&L.-J. Teng&C.-Y. Liu
Received: 10 September 2008 / Accepted: 25 February 2009 / Published online: 12 March 2009 # Springer-Verlag 2009
Abstract A nationwide susceptibility surveillance of Strep-tococcus pneumoniae and Haemophilus influenzae isolates collected from patients treated at the intensive care units (ICUs) of ten Taiwanese major teaching hospitals was conducted from September 2005 through November 2005. High rates of resistance (intermediate/resistant) of S. pneumoniae to penicillin (85% resistance), ceftriaxone (46%/20%), and cefepime (43%/15%) by meningitis crite-ria, and in contrast, non-susceptibilities (intermediate/ resistant) to penicillin (0%/0%), ceftriaxone (20%/0%) and cefepime (15%/0%) by non-meningitis criteria were noted
(p values < 0.05) by the Clinical and Laboratory Standards Institute 2008. Resistant rate of S. pneumoniae to azithro-mycin was also high (63%). S. pneumoniae isolates were significantly more susceptible to ertapenem (87%) than to imipenem (39%) and meropenem (44%) (p values < 0.05). Rates of non-susceptibilities of H. influenzae isolates to ampicillin and cefaclor were high (55% and 45%, respec-tively). No β-lactamase-negative ampicillin-resistant (BLNAR) H. influenzae isolates were found. Imipenem has a notably higher MIC90 value (8 μg/ml) for H. influenzae than that of the other two carbapenems.
S.-S. Jean
Departments of Intensive Care and Internal Medicine, Min-Sheng General Hospital,
Taoyuan County, Taiwan P.-R. Hsueh (*)
Departments of Laboratory Medicine and Internal Medicine, National Taiwan University Hospital,
National Taiwan University Medical College, 7 Chung-Shan South Road,
100 Taipei, Taiwan e-mail: [email protected] W.-S. Lee
Department of Internal Medicine, Taipei Municipal WanFang Hospital, Taipei, Taiwan
H.-T. Chang
Department of Internal Medicine, Far Eastern Memorial Hospital, Taipei County, Taiwan
M.-Y. Chou
Department of Internal Medicine, Cheng Hsin Rehabilitation Medical Center, Taipei, Taiwan
I.-S. Chen
Department of Internal Medicine, Cardinal Tien Hospital, Taipei County, Taiwan
J.-H. Wang
Department of Internal Medicine, China Medical College Hospital, Taichung, Taiwan
C.-F. Lin
Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
J.-M. Shyr
Department of Clinical Pathology, Taichung Veterans General Hospital, Taichung, Taiwan
W.-C. Ko
Department of Internal Medicine, National Cheng-Kung University Hospital, Tainan, Taiwan
Tigecycline showed good in vitro activities against these two respiratory pathogens. High rates of resistance among isolates of S. pneumoniae and H. influenzae continue to exist in the ICUs of Taiwan.
Streptococcus pneumoniae and Haemophilus influenzae are the two most frequently encountered, community-acquired pathogens leading to lower respiratory tract infections [1]. Consequently, their resistances are of worldwide concern. The Surveillance of Multicenter Antimicrobial Resistance in Taiwan (SMART) was initiated in 2000. This nationwide programme was designed to longitudinally monitor the antimicrobial resistance of clinically important bacteria. A SMART survey, conducted in 2000, revealed that 58% non-susceptibility to penicillin and 33% non-non-susceptibility to cefotaxime among S. pneumoniae strains evaluated were documented according to the meningitis guidelines of the National Committee for Clinical and Laboratory Standards (NCCLS) in 2000 [2].
From September 2005 through November 2005, a total of 85 non-duplicated clinical isolates, including 54 S. pneumoniae and 31 H. influenzae isolates, recovered from the ICU patients of ten major Taiwanese teaching hospitals, were included. Each isolate was obtained from one individual patient. Minimum inhibitory concentrations (MICs) were determined by using the agar dilution method [3], and interpreted by the guidelines recommended by the Clinical and Laboratory Standards Institute (CLSI) 2008 [4]. A total of 23 antimicrobial agents were tested (Table1).
Reference strains including S. pneumoniae ATCC 49619, H. influenzae ATCC 49247, H. influenzae ATCC 49766, and Escherichia coli ATCC 35218 were used as quality control strains for each batch of MIC tests. The H. influenzae isolates were tested for β-lactamase production using the cefinase disk.
The majority of the isolates were cultured from the respiratory tract (80% for S. pneumoniae and 97% for H. influenzae, respectively). The results of antimicrobial susceptibilities are shown in Table 1. For S. pneumoniae isolates, CLSI 2008 meningitis interpretative criteria were used (the susceptible and resistant MIC interpretative breakpoints for penicillin were ≤0.06 and ≥0.12 μg/ml, respectively, and the susceptible, intermediate, and resistant MIC breakpoints, for ceftriaxone and cefepime [4] were≤0.5, 1, and ≥2 μg/ml, respectively). High rates of non-susceptibility for penicillin (85%), ceftriaxone (66%) and cefepime (57%) were demonstrated for ICU S. pneumoniae isolates. However, using the non-meningitis interpretative criteria (MIC interpretative breakpoints for susceptible, intermediate and resistant, respectively, were≤2, 4, and≥ 8 μg/ml for penicillin and ≤1, 2, and ≥4 μg/ml for ceftriaxone and cefepime [4]) in CLSI 2008, penicillin, ceftriaxone and cefepime showed high rates of susceptibility (100% to penicillin, 80% to ceftriaxone, and 85% to cefepime) forS. pneumoniae.
H. influenzae strains exhibited a high rate (55%) of resistance to ampicillin. All isolates intermediate or resistant to ampicillin were positive for β-lactamase production, indicating the absence of β-lactamase-negative ampicillin-resistant (BLNAR) isolates. The susceptibilities of H. influenzae isolates to cefaclor, cefuroxime, cefixime, cefpodoxime, cefotaxime and amoxicillin-clavulanate were 55%, 90%, 100%, 100%, 100% and 100%, respectively. Azithromycin (MIC90value, 4μg/ml) showed significantly better in vitro activity againstH. influenzae than clarithro-mycin (MIC90 value, 32 μg/ml; p=0.0177 [statistical method]).
Levofloxacin and moxifloxacin retained good activi-ties againstS. pneumoniae and H. influenzae isolates, but two (6.5%) of the H. influenzae strains exhibited non-susceptibilities to fluoroquinolones (MIC values of the two isolates for ciprofloxacin/levofloxacin/moxifloxacin were 8/4/8 and 4/4/4 μg/ml, respectively). Isolates of S. pneumoniae and H. influenzae exhibited low MIC90 values (0.03 and 0.25μg/ml, respectively) to tigecycline. Ertapenem showed better activity than imipenem and meropenem (susceptibilities of 87%, 39%, 44%, respec-tively; p values < 0.05) against S. pneumoniae, and the imipenem MIC90 level (8 μg/ml) for H. influenzae was notably higher (64-fold) than that of the other two carbapenems (MIC90 value, 0.12μg/ml).
J.-J. Wu
School of Medical Technology,
National Cheng-Kung University College of Medicine, Tainan, Taiwan
Y.-C. Liu
Department of Clinical Pathology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
W.-K. Huang
Department of Internal Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
L.-J. Teng
School of Medical Technology, National Taiwan University Hospital,
National Taiwan University College of Medicine, Taipei, Taiwan
C.-Y. Liu
Department of Internal Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
Table 1 Antimicrobial susceptibilities ofS. pneumoniae and H. influenzae isolates recovered from patients treated at the intensive care units of ten major teaching hospitals in Taiwan in 2005
Antimicrobial agent MIC (μg/ml) No. (%) of isolatesa
Range MIC50 MIC90 S I R
S. pneumoniae (54) Penicillin 0.03–2 1 2 8 (15) NAc 46 (85)b 54 (100) 0 (0) 0 (0)c Ceftriaxone 0.03–2 1 2 18 (33) 25 (46) 11 (20)b 43 (80) 11 (20) 0 (0)c Cefepime 0.03–2 1 2 23 (43) 23 (43) 8 (15)b 46 (85) 8 (15) 0 (0)c Imipenem 0.03–1 0.25 0.5 21 (39) 32 (59) 1 (2) Meropenem 0.03–2 0.5 0.5 24 (44) 27 (50) 3 (6) Ertapenem 0.03–8 1 2 47 (87) 6 (11) 1 (2) Azithromycin 0.03– >128 8 >128 18 (33) 2 (4) 34 (63) Levofloxacin 0.06–16 1 2 52 (96) 0 (0) 2 (4) Moxifloxacin 0.03–4 0.12 0.25 52 (96) 1 (2) 1 (2) Vancomycin 0.03–0.5 0.25 0.5 54 (100) 0 (0) 0 (0) Linezolid 0.06–1 0.5 1 54 (100) 0 (0) 0 (0) Telithromycin 0.03–0.25 0.03 0.06 54 (100) 0 (0) 0 (0) Tigecycline 0.03 0.03 0.03 NA NA NA H. influenzae (31) Ampicillin 0.25–128 2 64 14 (45) 2 (7) 15 (48) Amoxicillin 0.25–128 4 64 NA NA NA Amoxicillin-clavulanate 0.25–4 1 4 31 (100) NA 0 (0) Cefaclor 4–64 8 64 17 (55) 6 (19) 8 (26) Cefuroxime 0.5–8 1 4 28 (90) 3 (10) 0 (0) Cefixime 0.03–0.5 0.06 0.12 31 (100) NA NA Cefpodoxime 0.03–0.25 0.12 0.25 31 (100) NA NA Cefotaxime 0.03 0.03 0.03 31 (100) NA NA Imipenem 0.12–16 1 8 26 (84)d NA NA Meropenem 0.03–0.5 0.06 0.12 31 (100) NA NA Ertapenem 0.03–0.25 0.06 0.12 31 (100) NA NA Azithromycin 1–4 2 4 31 (100) NA NA Clarithromycin 1–128 16 32 10 (32) 16 (52) 5 (16) Ciprofloxacin 0.03–8 0.03 0.25 29 (94)e NA NA Levofloxacin 0.03–4 0.03 0.12 29 (94)e NA NA Moxifloxacin 0.03–8 0.03 0.12 29 (94) NA NA TMP-SMX 1–>128 16 128 11 (35) 6 (19) 14 (45) Tigecycline 0.12–0.5 0.25 0.25 NA NA NA
MIC minimum inhibitory concentration, S susceptible, I intermediate, R resistant, NA not available, TMP-SMX trimethoprim-sulfamethoxazole a
Some interpretative MIC breakpoints of susceptibility categories were not available (NA) [4]
b ForS. pneumoniae isolates, the rates of susceptibilities to penicillin, ceftriaxone, and cefepime were calculated as percentages by meningitis
criteria (the susceptible and resistant MIC interpretative breakpoints for penicillin were≤0.06 and ≥0.12 μg/ml, respectively, and the susceptible,
intermediate, and resistant MIC breakpoints, for ceftriaxone and cefepime were≤0.5, 1, and ≥2 μg/ml, respectively) [4]
c ForS. pneumoniae isolates, the rates of susceptibilities to penicillin, ceftriaxone, and cefepime were calculated as percentages by non-meningitis
criteria (the MIC interpretative breakpoints for susceptible, intermediate and resistant were, respectively,≤2, 4, and ≥ 8 μg/ml for penicillin and ≤1, 2,
and≥4 μg/ml for ceftriaxone and cefepime) [4]
d Five isolates ofH. influenzae were not susceptible to imipenem
e
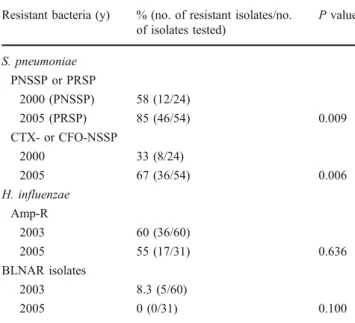
Compared to the data of previous surveillances, signif-icantly increasing prevalences of penicillin-resistant S. pneumoniae (PRSP, evaluated by the meningitis criterion of CLSI 2008) and the third-generation cephalosporins (cefotaxime, ceftriaxone)-non-susceptible S. pneumoniae (by using meningitis criteria; p=0.009 and 0.006, respec-tively) between 2000 [2] and 2005 in Taiwanese ICUs were noted. Also, a decline in the rate of BLNAR (evaluated by chi-square test; p=0.100) for H. influenzae between 2003 [1] and 2005 (Table2) was seen.
In this Taiwanese ICU surveillance, the markedly high prevalence of penicillin resistance (meningitis criteria) for ICUS. pneumoniae was noted. Because of the rapidly rising prevalence of PRSP, which also have a high likelihood of exhibiting co-resistance to non-β-lactam antimicrobials [5], institution of a stricter control policy for the administration of β-lactams in Taiwanese ICUs is mandatory. No BLNAR isolate in this survey was found, which is different from that of a previous Taiwanese study [1].
In this study, imipenem and meropenem showed poorer in vitro activities against S. pneumoniae isolates than that of ertapenem. Hilliard et al. demonstrated that S. pneumoniae strains with intermediate susceptibility to imipenem and meropenem were likely (>80% probability) to be susceptible to ertapenem [6], and the susceptibilities of amoxicillin-clavulanate and ceftriaxone to S. pneumoniae were
well-correlated with that of ertapenem [6], which were consistent with our findings on the similarity between the susceptibility of ceftriaxone (by non-meningitis criterion) and ertapenem to pneumococci. Besides, our H. influenzae isolates had a significantly lower imipenem susceptibility (84%) than that of the other two carbapenems (p values < 0.05). Different entry routes of imipenem from meropenem [7] and decreased imipenem affinity to penicillin-binding protein in mutatedH. influenzae isolates [8] were the presumed mechanisms resistant to imipenem. Notably, our H. influenzae isolates displayed remarkable differences in their susceptibilities to azithromycin and clarithromycin. However, the clinical applicability of this MIC data suggestive of the superiority of azithromycin to clarithromycin is controversial because the synergistic effect of the 14-OH metabolite of clarithro-mycin is not routinely tested in the MIC determination of clarithromycin [9]. The tigecycline MIC90 value for our S. pneumoniae is lower than that of a previous global study [10], and similar to that of the same global survey for H. influenzae [10].
In conclusion, high penicillin non-susceptibility and marked differences concerning the susceptibilities of Taiwa-nese ICUS. pneumoniae isolates for penicillin and cefotax-ime/ceftriaxone through the evaluation by meningitis and non-meningitis criteria were clearly documented. Imipenem and meropenem showed high non-susceptibilities to pneu-mococci. With regards to Taiwanese H. influenzae strains, ampicillin, cefaclor, clarithromycin and trimethoprim-sulfamethoxazole showed poor activities by in vitro suscep-tibility data, and the suscepsuscep-tibility of imipenem was inferior to that of the other carbapenems. Alarmingly, higher β-lactam-non-susceptible rates (meningitis criteria) among S. pneumoniae isolates and the persistently high prevalence of ampicillin- non-susceptible H. influenzae isolates in comparison with prior Taiwanese data were noted. Tigecy-cline and respiratory fluoroquinolones are promising agents with potent activity against both S. pneumoniae and H. influenzae isolates. However, prudent use of these agents to prevent the potential emergence of resistance is warranted.
References
1. Lau YJ, Hsueh PR, Liu YC, Shyr JM, Huang WK, Teng LJ, Liu CY, Luh KT (2006) Comparison of in vitro activities of
tigecycline with other antimicrobial agents againstStreptococcus
pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis
in Taiwan. Microb Drug Resist 12:130–135. doi:10.1089/
mdr.2006.12.130
2. Hsueh PR, Liu YC, Yang D, Yan JJ, Wu TL, Huang WK, Wu JJ, Ko WC, Leu HS, Yu CR, Luh KT (2001) Multicenter surveillance of antimicrobial resistance of major bacterial pathogens in intensive care units in 2000 in Taiwan. Microb Drug Resist
7:373–382. doi:10.1089/10766290152773383
Table 2 Differences in the prevalences of antibiotic resistance of
penicillin- non-susceptible S. pneumoniae (PNSSP) in 2000,
penicillin-resistantS. pneumoniae (PRSP) (evaluated by the
meningi-tis criterion of CLSI 2008) in 2005, and the third-generation cephalosporins (cefotaxime [CTX], ceftriaxone
[CFO])-non-suscepti-bleS. pneumonia (CTX- or CFO-NSSP) isolates from the Taiwanese
intensive care units between 2000 and 2005 with ampicillin-resistant
(Amp-R) and β-lactamase-negative ampicillin-resistant (BLNAR) H.
influenzae isolates between 2003 and 2005
Resistant bacteria (y) % (no. of resistant isolates/no.
of isolates tested) P value S. pneumoniae PNSSP or PRSP 2000 (PNSSP) 58 (12/24) 2005 (PRSP) 85 (46/54) 0.009 CTX- or CFO-NSSP 2000 33 (8/24) 2005 67 (36/54) 0.006 H. influenzae Amp-R 2003 60 (36/60) 2005 55 (17/31) 0.636 BLNAR isolates 2003 8.3 (5/60) 2005 0 (0/31) 0.100
3. CLSI (2005) Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically, 6th edn. Approved standard M7-A6. Clinical and Laboratory Standards Institute, Wayne, PA, USA
4. CLSI (2008) Performance standards for antimicrobial susceptibility testing, 15th informational supplement. Supplemental tables M100-S18. Clinical and Laboratory Standards Institute, Wayne, PA, USA
5. Whitney CG, Farley MM, Hadler J, Harrison LH, Lexau C, Reingold A, Lefkowitz L, Cieslak PR, Cetron M, Zell ER, Jorgensen JH, Schuchat A, Active Bacterial Core Surveillance Program of the Emerging Infections Program Network (2000)
Increasing prevalence of multidrug-resistant Streptococcus
pneu-moniae in the United States. N Engl J Med 343:1917–1924. doi:10.1056/NEJM200012283432603
6. Hilliard NJ, Johnson CN, Armstrong SH, Quarles S, Waites KB (2002) In vitro activity of ertapenem (MK-0826) against
multi-drug resistantStreptococcus pneumoniae compared with 13 other
antimicrobials. Int J Antimicrob Agents 20:136–140. doi:10.1016/
S0924-8579(02)00129-2
7. Yourassowsky E, Van der Linden MP, Crokaert F (1991) Antibacterial effects of meropenem and imipenem against
Haemophilus influenzae. Chemotherapy 37:38–42. doi:10.1159/
000114345
8. Cerquetti M, Giufrè M, Cardines R, Mastrantonio P (2007) First characterization of heterogeneous resistance to imipenem in
invasive nontypeableHaemophilus influenzae isolates. Antimicrob
Agents Chemother 51:3155–3161. doi:10.1128/AAC.00335-07
9. Hardy DJ, Swanson RN, Rode RA, Marsh K, Shipkowitz NL, Clement JJ (1990) Enhancement of the in vitro and in vivo
activities of clarithromycin againstHaemophilus influenzae by
14-hydroxy-clarithromycin, its major metabolite in humans.
Anti-microb Agents Chemother 34:1407–1413
10. Hoban DJ, Bouchillon SK, Johnson BM, Johnson JL, Dowzicky MJ, Tigecycline Evaluation and Surveillance Trial (TEST Pro-gram) Group (2005) In vitro activity of tigecycline against 6792 Gram-negative and Gram-positive clinical isolates from the global Tigecycline Evaluation and Surveillance Trial (TEST Program,
2004). Diagn Microbiol Infect Dis 52:215–227. doi:10.1016/j.