From the aTaipei Medical University School of Nursing, bNational Health Insurance Department, and cNational College of Physical Education and Sports.
Reprint requests: Chii Jeng, DNSc, RN, 250 Wu Hsing St, Taipei, Taiwan 110, ROC.
Copyright 2002, Mosby, Inc. All rights reserved. 0147-9563/2002/$35.00 + 0 2/1/119403 doi:10.1067/mhl.2002.119403
C
hronic obstructive pulmonary disease (COPD) is a worldwide health problem that has an increasing prevalence and mortality rate.1In Taiwan, COPD is among the 10 leading causes ofdeath. The mortality rate of COPD was 9.37 per 100,000 persons in 1995, with a 5.06% increase in mortality rate compared with 1994.2 In Taiwan, because of the fear of activity-induced dyspnea and a long-term sedentary lifestyle, persons who have COPD could develop low self-efficacy with regard to the performance of daily activities. Kaplan et al3reported that self-efficacy, rather than maximum oxygen uptake (VO2max), partial pressure of oxygen (PaO2), and forced expiratory volume in 1 second (FEV1) was a significant univariate predic-tor of 5-year survival. Gormley et al4demonstrated
Investigation of the difference between
treadmill self-efficacy and actual performance
in Taiwanese patients with chronic obstructive
pulmonary disease
Chii Jeng, DNSc, RN,aHsiao-Chuan Yang, MSN, RN,bPui Man Wai, PhD,cJen Chen Tsai, DNSc, RN,a Ling Ling Wei, MS, RN,aand Su-Ru Chen, MSN, RN,aTaipei, Taiwan
OBJECTIVE: Because overactivity or underactivity may result in inadequate physical responses among patients with chronic obstructive pulmonary disease (COPD), the purpose of this study was to examine the difference between treadmill self-efficacy and actual treadmill performance. Factors that influence self-efficacy and actual performance were also examined.
DESIGN: The design was a descriptive and correlational study.
SETTING: The study took place at the Research Center of Sports Medicine in University. PATIENTS: A total of 48 subjects with COPD were recruited from 4 hospitals.
OUTCOME MEASURES: The outcome measures were treadmill self-efficacy and actual treadmill per-formance.
INTERVENTION: Data were collected by means of treadmill exercise testing and 3 structured ques-tionnaires.
RESULTS: The findings of the study demonstrated that the average maximal functional capacity was 2.94 METs. A positive significant relationship between treadmill self-efficacy and actual performance was observed. However, the majority of subjects (72.9%) underestimated their treadmill performance and only 7 subjects (14.6%) assessed their treadmill performance accurately. Dyspnea was the most common reason for a subject to stop during the exercise testing. The patient’s past experience was the most important predictor for both treadmill self-efficacy and actual treadmill performance.
CONCLUSIONS: These results revealed that patients in Taiwan who have COPD have extremely poor functional capacity and most of them underestimated their exercise performance. An assessment of self-efficacy and exercise performance seems imperative in the development of individualized nursing inter-ventions to help COPD patients. (Heart Lung® 2002;31:150-6.)
that patients who had COPD had self-efficacy per-ceptions that were significantly lower than actual performance.
The theoretical framework for this study was Bandura’s social cognitive theory and his derived self-efficacy theory.5,6 Bandura considers self-effi-cacy perceptions to be the most powerful determi-nants of behavioral change. Efficacy expectation can help one determine whether to engage in a behavior, how much effort to expend, and how long the behavior will last despite possible barriers. Beliefs about personal efficacy develop from cogni-tive appraisal of information, which arises from 4 major sources: performance accomplishment, vicar-ious experience, verbal persuasion, and emotional arousal or physiologic feedback. Performance accomplishment is the most powerful source of effi-cacy information for enhancing self-effieffi-cacy and vic-arious experience is considered the next most powerful method for changing self-perceptions.6
Scherer et al7demonstrated that a rehabilitation program that combines education and exercise training is more effective than education alone to improve long-term self-efficacy related to manag-ing or avoidmanag-ing difficulty in breathmanag-ing in patients with COPD. Gormley et al4 found that COPD patients’ self-efficacy and actual performance became more congruent throughout 12 walking ses-sions. Zimmerman, Brown, and Bowman8found that the use of a group teaching method improved COPD patients’ self-efficacy in self-management.
Although the effectiveness of selected strategies in improvement of self-efficacy has been supported, it is important to explore the related factors that con-tribute to determining one’s self-efficacy because low self-efficacy may deter patients from engaging in activities of daily living. The purpose of this study was to examine differences between treadmill self-efficacy (confidence in a subject’s ability to walk at a maximum level during exercise testing) and actual treadmill performance (actual maximum level achieved during exercise testing) in Taiwanese patients who have COPD. Factors that influence self-efficacy and actual performance also were examined.
METHODS
Research design
This is a descriptive and correlational study. Data were collected by means of graded exercise testing, lung function tests, and 4 questionnaires, which include the Exercise Self-efficacy Scale, Efficacy Sources Inventory, State Trait Anxiety Inventory,9and Self-perceived Dyspnea Scale.10The study was
con-ducted at the Research Center of Sports Medicine in University. Forty-eight volunteers were recruited who had COPD treated on an outpatient basis and who met the selection criteria, which included a stable disease and a referral from their physician. No sub-jects participated in any other pulmonary rehabilita-tion program either before or after discharge.
Exercise testing. A symptom-limited, treadmill-graded exercise test with modified Naughton pro-tocol was used to measure each subject’s functional capacity and to determine the difference between his or her perceived efficacy and actual perfor-mance in exercise testing. The protocol of exercise testing, which included 10 levels, ranged from 1.0 mph, 0% grade (level 1) to 3.0 mph, 12% grade (level 10), with increasing levels in relatively small increments (≤1 MET per stage) every 3 minutes. The test was terminated on the basis of the follow-ing criteria: chest tightness or chest pain, exhaus-tion, severe dyspnea (Borg Scale >3), SaO2 less than 90%, reaching 90% maximal heart rate, abnor-mal electrocardiographic change, or at the request of the subject. The estimated VO2maxfor each sub-ject was calculated by the formula VO2max= speed × 26.8 × (0.1 + [1.8 × % grade]) + 3.5.11This testing was also used to calculate resting heart rate, blood pressure, peak heart rate, and peak blood pressure. Lung function test. Before exercise testing, a spirometer was used to perform a lung function test that measured FEV1and forced vital capacity (FVC). For data analysis, predicted FEV1(FEV1%pred), pre-dicted FVC (FVC%pred), and FEV1/FVC% were com-puted. Predicted FEV1and FVC were calculated by the equations set up in the spirometer software.
Exercise Self-efficacy Scale. This scale, devel-oped by the investigators, was designed on the basis of the calculated workload (speed and % grade) for each stage of the modified Naughton protocol that was used during the exercise testing. This scale was used to measure a subject’s confidence in his tread-mill performance ability. For example, the first item is “Please rate your confidence level in walking on the treadmill with a speed of 1.0 mph and a grade of 0% for 3 minutes without stopping.” Scores for this scale can vary from a minimum of 0 to a maximum of 100. A high score on the scale indicates a high con-fidence level in treadmill performance. Internal consistency of this scale was demonstrated by a Cronbach’s α coefficient of 0.88. Concurrent validity of the scale was supported by the significant corre-lation (r = 0.30, P = .042) between this scale and the Duke Activity Status Index.12
Efficacy Sources Inventory. Developed by the investigators, this inventory consists of 3 parts. Ten
items were designed to measure a subject’s past performance accomplishment in daily activities; 4 items measured vicarious experiences of exercise; and 4 items measured a subject’s verbal persua-sion (ie, verbal exercise encouragement received from others). A standardized score was the obtained score/the maximum score divided by 100. A high score on the scale indicates high self-effica-cy. Internal consistency was demonstrated by the Cronbach α coefficient of 0.82 for the entire scale and ranged from 0.60 to 0.88 for the 3 subscales.
State Trait Anxiety Inventory. This inventory consists of 2 subscales (state anxiety and trait anx-iety) and includes 20 items per subscale. Anxiety states are characterized by subjective feelings of tension, nervousness, and worry. Trait anxiety refers to relatively stable individual differences in predisposition to anxiety. Because anxiety may result in dyspnea, which may in turn influence a patient’s performance during the testing, anxiety level was measured as “emotional arousal” in this study. High scores indicate high anxiety levels. Construct validity of this inventory was supported by its ability to discriminate between psychiatric and nonpsychiatric patients and by a distinct factor structure for items that measure state and trait anx-iety. In this study, the Cronbach α coefficient was 0.88 for state anxiety and 0.87 for trait anxiety.
Self-perceived Dyspnea Scale. This scale includes 25 items that measure subjects’ degree of dyspnea while they perform daily activities. Subjects rate the level of dyspnea in 5 items that they performed most frequently during the past 2 weeks. The inter-nal reliability and content validity of this scale have been supported by a previous study.10Test-retest reliability (r = 0.60, P = .017) for 6 to 8 weeks has been demonstrated in the current study.
Data collection. Subjects were referred by their physicians and were contacted and scheduled for an orientation session and a graded exercise test. A thorough explanation of the study protocol was pro-vided and a consent form was signed on the orien-tation day. All subjects had to complete the Exercise Self-efficacy Scale, Efficacy Sources Inventory, State Trait Anxiety Inventory, and Self-perceived Dyspnea Scale before the Naughton protocol graded tread-mill test and lung function tests were conducted by the investigators. On the basis of the treadmill test results and the exercise self-efficacy scores, subjects were divided into 3 groups: those who underesti-mated performance, those who accurately estiunderesti-mated performance, and those who overestimated perfor-mance. The maximum performance METs were sub-tracted from the maximum METs of self-efficacy for
each subject to obtain an individual difference value. Subjects with negative values underestimat-ed their performance, such that their self-efficacy was lower than actual performance. Subjects with positive values overestimated their performance, and subjects whose difference value equaled zero accurately appraised their walking ability.
Data analysis. The SPSS/PC+ statistical software package was used for data analysis. Descriptive statistics were computed for demographic data. Differences between self-efficacy and actual performance were determined by t test. One-way analysis of variance (ANOVA) was performed to determine differences in all study variables among the underestimated, the accurately estimated, and overestimated groups. A post hoc analysis of the 3 groups was performed using Scheffe’s test. Step-wise regression analyses were performed to exam-ine what factors were related to self-efficacy and actual performance. With a .05 significance level, the power of the current study was 0.79 for stepwise regression analyses and 0.89 for the t test.
RESULTS
Forty-eight subjects (43 male and 5 female) with COPD volunteered and provided informed consent for the study. The mean age of the sample was 69.83 years (SD, 7.08). Most subjects (92%) were married and retired. The mean number of years of education was 8.79 (SD, 5.04). Twenty-two subjects (54%) had asthma, 11 subjects (23%) had emphyse-ma, and 11 subjects (23%) had chronic bronchitis. The average duration of smoking of the sample was 36.75 years (SD, 18.38), and 11 subjects still smoked during the study period. The average val-ues of FEV1%pred, FVC%pred, and FEV1/FVC% of the sample were 57.57, 69.9, and 60.04, respective-ly. Fourteen subjects’ (29.2%) FEV1%pred were 70% and 20 subjects’ (42%) FEV1%pred were <50% (severe impairment in lung function) (Table I).
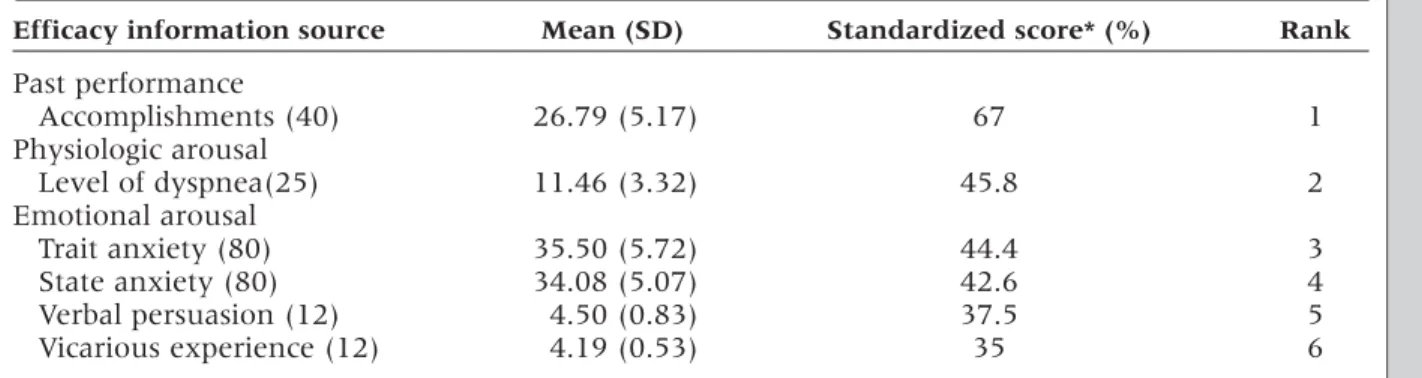
The mean estimated VO2maxof this sample was 2.94 METs (SD, 0.89), with an average walking time of 8.88 minutes (SD, 4.42). Most of the subjects ter-minated the testing at stage III because of dyspnea. Table II displays the mean and standardized scores of 4 sources of efficacy information. Past perfor-mance accomplishments were ranked first as the source of efficacy information, whereas vicarious experience and verbal persuasion were ranked sixth and fifth, respectively. To determine which sources of efficacy information might predict tread-mill self-efficacy and actual performance, a series of stepwise multiple regression analyses were per-formed. Table III illustrates that past performance
accomplishment explained 35% of the variance of treadmill self-efficacy (F = 24.82, P < .0001, df = 47) and was the strongest predictor of actual treadmill performance. Together, the past performance accomplishment, resting heart rate, and FEV1/FVC% explained 50% of the variance of actual treadmill performance (F = 14.35, P < .0001).
The difference between actual performance (the maximum performance METs) and treadmill self-efficacy (the maximum METs that the subject had 100% confidence in completing during testing) was computed after exercise testing. A significant dif-ference was observed between treadmill self-effi-cacy (2.20 ± 1.15 METs) and actual performance (2.940.89 METs) (t = –4.28, P < .0001).
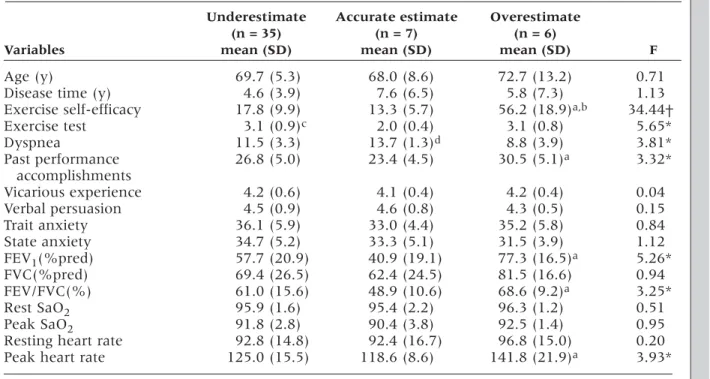
Six subjects (12.5%) overestimated, 7 subjects (14.6%) correctly estimated, and 35 subjects (72.9%) underestimated their actual performance. Table IV presents the comparisons of all study variables among the 3 groups. It was found that treadmill self-efficacy, actual treadmill performance, dysp-nea level, past performance accomplishments, FEV1%pred, FEV1/FVC%, and peak heart rate during testing were significantly different among the 3 groups. Post hoc tests using Scheffes procedure showed that the overestimated group had higher
treadmill self-efficacy, actual treadmill perfor-mance, FEV1%pred, FEV1/FVC%, and peak heart rate during testing, and lower dyspnea level than did the accurate-estimate group. It was also found that the accurate-estimate group had the longest history of disease, and the lowest treadmill self-efficacy, actual treadmill performance, and lung function (FEV1%pred, FVC%pred, FEV1/FVC%).
DISCUSSION
The purpose of this study was to examine differ-ences between treadmill self-efficacy and actual treadmill performance in Taiwanese subjects with COPD. The results reveal that subjects’ self-efficacy was significantly lower than actual performance. Most subjects (72.9%) underestimated their ability in performing treadmill tests, congruent with Gorm-ley’s results4 that most COPD patients have low self-confidence in exercise. Gormley’s study also revealed that self-efficacy and actual performance became more congruent over time, though 44% of the sample continued to underestimate ability to walk relative to actual performance during 12 ses-sions of walking. The most common patterns of changes in self-efficacy and actual performance for subjects across the 12 sessions were increased con-Table I
Demographic characteristics of the sample (N = 48)
Characteristics Mean SD Range
Age (y) 69.83 7.08 49–89
Education (y) 8.79 5.04 0–20
Years of disease 5.21 4.82 0.5–20
Smoking history (y) 36.75 18.38 0–60
FEV1%pred 57.57 21.97 15–107 FVC%pred 69.90 25.28 30–141 FEV1/FVC% 60.04 15.08 32.9–98.2 Sex (No.) Male 43 90% Female 5 10%
Marital status (No.)
Currently married 44 92% Widowed 4 8% Diagnosis (No.) Asthma 26 54% Emphysema 11 23% Chronic bronchitis 11 23% Employment (No.) Retired 44 92% Work full-time 4 8%
gruency and consistent underestimation. Ewart et al13 demonstrated that even a single session of exercise tests could improve a subject’s self-effica-cy. Therefore, to decrease the differences between self-efficacy in exercise and actual performance, an exercise test or a period of exercise training should be arranged for COPD patients.
Although a relationship between FEV1and peak VO2max has been demonstrated, pulmonary func-tion does not accurately predict exercise perfor-mance in patients with COPD.14 In the current study, subjects with poor lung function (FEV1%pred and FEV1/FVC%), negative exercise experience, and higher level of dyspnea tended to more accu-rately estimate their ability. On the contrary, sub-jects with higher lung function tended to underes-timate or overesunderes-timate their exercise ability. Because underestimation may result in decreased daily activities and overestimation may result in severe physical symptoms during exercise,
inter-ventions should be directed at helping individuals with COPD to judge their exercise ability accurate-ly, even when their lung function is good.
The average estimated VO2maxof this study sam-ple during exercise testing was 2.94 METs and 71% of the sample had <3 METs, which is much lower than the report (4.6-6.2 METs) of a previous study.15 This suggests that functional capacity in Taiwanese subjects who have COPD is extremely poor and may limit their daily activity performance because 5 METs is considered to be the minimal fitness level needed to independently perform daily activities.
Dyspnea was also found to be the most common reason (27 subjects) that participants stopped dur-ing the exercise testdur-ing, but the SaO2values of all 27 subjects were >90%. Nevertheless, 27% of the sample (13 subjects) terminated the testing because their SaO2 was <90%, but this dyspnea level was mild (<3). During exercise testing, SaO2 decreased from 95.0% to 91.67%. The decrease in Table II
Mean and standard deviation of source of efficacy information
Efficacy information source Mean (SD) Standardized score* (%) Rank
Past performance Accomplishments (40) 26.79 (5.17) 67 1 Physiologic arousal Level of dyspnea(25) 11.46 (3.32) 45.8 2 Emotional arousal Trait anxiety (80) 35.50 (5.72) 44.4 3 State anxiety (80) 34.08 (5.07) 42.6 4 Verbal persuasion (12) 4.50 (0.83) 37.5 5 Vicarious experience (12) 4.19 (0.53) 35 6
*Standardized score = Obtained score/the maximum score divided by 100.
Table III
Stepwise regression analysis of treadmill exercise efficacy and actual performance model indicators
Dependent Independent
variables variables B R2 Cumulative R2 F P
Exercise self-efficacy Past performance 1.94 0.59 0.35 0.35 24.82 .0001 accomplishment
Actual performance Dyspnea –0.10 –0.368 0.336 0.336 13.50 .0001
Resting heart rate –0.02 –0.32 0.068 0.404
SaO2significantly correlated with dyspnea at rest (r = –0.385, P = .007). However, in contrast to the find-ings of Chodosowska and Zielinski,16a weak corre-lation (r = –0.252, P = .084) between degree of dys-pnea and SaO2during exercise was observed in this study. Differences in modes of exercise tests (6-minute walking test or treadmill exercise test) and severity of disease (resting SaO2, 92% or 95%) between these 2 studies may be possible reasons for the discrepancy. In the future, more research is needed to support the relationship between degree of dyspnea and SaO2.
Negative relationships between dyspnea level and actual performance (r = –0.58, P < .0001) as well as between dyspnea level and exercise self-efficacy (r = –0.496, P < .0001) were observed in the current study. These results suggest that dyspnea rather than SaO2was a significant factor in determining exercise performance among patients who have COPD. Similar to previous findings,17dyspnea was the most important predictor in exercise
perfor-mance. However, a low test-retest correlation coeffi-cient (r = 0.6, P = .017) for the Self-perceived Dysp-nea Scale might influence the stability of the data.
With respect to 4 sources of efficacy information, the results of this study reveal that subjects’ past performance accomplishment was the most impor-tant predictor of treadmill self-efficacy and actual performance. This result supports Bandura’s social cognitive theory that past performance is the most powerful source of efficacy information for enhanc-ing self-efficacy. However, vicarious experience and verbal persuasion were not correlated with tread-mill self-efficacy in this study. A low score in vicari-ous experience and verbal persuasion was observed, which indicates that exercise-related encouragement and instructions from others might be insufficient or have limited impact.
Physiologic indicators of level of dyspnea, FEV1%pred, and FEV1/FVC% were significantly cor-related with treadmill self-efficacy supporting the findings of Graydon and Ross.17However, a
signifi-Table IV
Differences in study variables among 3 groups
Underestimate Accurate estimate Overestimate
(n = 35) (n = 7) (n = 6)
Variables mean (SD) mean (SD) mean (SD) F
Age (y) 69.7 (5.3) 68.0 (8.6) 72.7 (13.2) 0.71
Disease time (y) 4.6 (3.9) 7.6 (6.5) 5.8 (7.3) 1.13
Exercise self-efficacy 17.8 (9.9) 13.3 (5.7) 56.2 (18.9)a,b 34.44†
Exercise test 3.1 (0.9)c 2.0 (0.4) 3.1 (0.8) 5.65* Dyspnea 11.5 (3.3) 13.7 (1.3)d 8.8 (3.9) 3.81* Past performance 26.8 (5.0) 23.4 (4.5) 30.5 (5.1)a 3.32* accomplishments Vicarious experience 4.2 (0.6) 4.1 (0.4) 4.2 (0.4) 0.04 Verbal persuasion 4.5 (0.9) 4.6 (0.8) 4.3 (0.5) 0.15 Trait anxiety 36.1 (5.9) 33.0 (4.4) 35.2 (5.8) 0.84 State anxiety 34.7 (5.2) 33.3 (5.1) 31.5 (3.9) 1.12 FEV1(%pred) 57.7 (20.9) 40.9 (19.1) 77.3 (16.5)a 5.26* FVC(%pred) 69.4 (26.5) 62.4 (24.5) 81.5 (16.6) 0.94 FEV/FVC(%) 61.0 (15.6) 48.9 (10.6) 68.6 (9.2)a 3.25* Rest SaO2 95.9 (1.6) 95.4 (2.2) 96.3 (1.2) 0.51 Peak SaO2 91.8 (2.8) 90.4 (3.8) 92.5 (1.4) 0.95
Resting heart rate 92.8 (14.8) 92.4 (16.7) 96.8 (15.0) 0.20
Peak heart rate 125.0 (15.5) 118.6 (8.6) 141.8 (21.9)a 3.93*
aOverestimate group > accurate-estimate group. bOverestimate group > underestimate group. cUnderestimate group > accurate-estimate group. dAccurate-estimate group > overestimate group. *P < .05.
cant relationship between anxiety (emotional arousal) and exercise self-efficacy was not support-ed even though this relationship also had been demonstrated in the study of Graydon and Ross.17In the current study, it was observed that subjects had the highest anxiety level as soon as testing began, perhaps because most subjects were unfamiliar with the machine and because measures were complet-ed before testing began rather than during testing.
CLINICAL IMPLICATIONS
In summary, this study demonstrates that the majority of subjects who have COPD in this study in Taiwan have extremely poor functional capacity and underestimated their treadmill exercise per-formance. The overestimated group and the under-estimated group tended to have higher treadmill self-efficacy, actual treadmill performance, lung function, peak heart rate during testing, and lower dyspnea level. However, the accurate-estimate group tended to have the longest history of dis-ease, and the lowest treadmill self-efficacy, actual treadmill performance, and lung function. The sub-ject’s past exercise experience was the most impor-tant predictor for treadmill self-efficacy, whereas dyspnea was the most important predictor in actu-al treadmill performance.
Because of lack of regular exercise and overpro-tection by family compared with Westerners, most patients with COPD in Taiwan lead a sedentary lifestyle that would avoid activity-induced dyspnea or other symptoms and they have a poor quality of life. There are few trained professionals in pul-monary rehabilitation and very few hospitals that provide pulmonary rehabilitation programs. To improve the quality of care for COPD patients in Taiwan, a pulmonary rehabilitation center should be established as soon as possible. The findings of this study have implications for improving physical performance and self-confidence of COPD patients. An assessment of treadmill self-efficacy and maxi-mal functional capacity seems imperative in the development of individualized nursing interven-tions to help COPD patients attain optimal health status. A routine treadmill exercise test should be arranged before COPD patients’ hospital discharge in order to improve confidence in their ability to exercise. In addition, teaching COPD patients how to monitor the level of dyspnea during exercise may help subjects become more aware of their ability to exercise without dyspnea.
According to Bandura’s theory, performance accomplishment, vicarious experience, verbal per-suasion, and emotional arousal or physiologic
feedback are 4 major sources of efficacy informa-tion to enhance self-efficacy. Because most of the subjects underestimated their self-efficacy, use of appropriate strategies such as encouraging exer-cise at an adequate intensity level during daily activities (performance accomplishment), introduc-ing model cases to patients (vicarious experience), and providing verbal persuasion may improve the patient’s self-efficacy. For further research, a ran-dom control study will be needed to determine the effectiveness in improving self-efficacy of the above strategies.
REFERENCES
1. ATS Statement. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1995;152(Suppl):S77-121.
2. Department of Health the Executive Yuan, ROC (1996). Health and vital statistics Republic of China; 1995.
3. Kaplan RM, Ries AL, Prewitt LM, Eakin E. Self-efficacy expec-tations predict survival for patients with chronic obstructive pulmonary disease. Health Psychol 1994;13:336-8.
4. Gormley JM, Carrieri-Kohlman V, Douglas MK, Stulbarg MS. Treadmill self-efficacy and walking performance in patients with COPD. J Cardiopulm Rehabil 1993;13:424-31.
5. Bandura A. Social foundation of thought and action. Prentice-Hall; 1977.
6. Bandura A. Self-efficacy: toward a unifying theory of behav-ioral change. Psychol Rev 1977;84:191-215.
7. Scherer YK, Schmieder LE, Shimmel S. The effects of education alone and in combination with pulmonary rehabilitation on self-efficacy in patients with COPD. Rehabil Nurs 1998;23:71-7. 8. Zimmerman BW, Brown ST, Bowman JM. A self-management program for chronic obstructive pulmonary disease: relation-ship to dyspnea and self-efficacy. Rehabil Nurs 1996;21:253-7. 9. Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA.
Manual for the state-trait anxiety inventory. Palo Alto (CA): Consulting Psychologists Press; 1983.
10. Hsu, NT. Compliance behavior to breathing control strategies in patients with chronic obstructive pulmonary disease [mas-ter’s thesis]. Taipei, ROC: Kaohsiung Medical College Gradu-ate Institute of Nursing; 1994.
11. American College of Sports Medicine. Guidelines for exercise testing and prescription. Philadelphia: Lea & Febiqer; 1991. 12. Hlatky MA, Boineau RE, Hogginbotham MB, Lee KL, Mark DB,
Califf RM, et al. A brief self-administered questionnaire to determine functional capacity (the Duke activity status index). Am J Cardiol 1989;15:651-4. p.p. 293-5.
13. Ewart CK, Taylor CB, Reese LB, DeBusk RF. Effects of early post myocardial infarction exercise testing on self-perception and subsequent physical activity. Am J Cardiol 1983;51:1076-80. 14. Ortega F, Montemayor T, Sanchez A, Cabello F, Castillo J. Role of
cardiopulmonary exercise testing and the criteria used to deter-mine disability in patients with severe chronic obstructive pul-monary disease. Am J Respir Crit Care Med 1994;150:747-51. 15. Punzal PA, Ries AL, Kaplan RM, Prewitt LM. Maximum
inten-sity exercise training in patients with chronic obstructive pul-monary disease. Chest 1991;100:618-23.
16. Chodosowska E, Zielinski J. Evaluation of the relations between exercise tolerance, dyspnea and pulmonary function in patients with chronic obstructive lung diseases. Pneu-monologia I Alergologia Polska 1992;60:54-61.
17. Graydon JE, Ross E. Influence of symptoms, lung function, mood, and social support on level of functioning of patients with COPD. Res Nurs Health 1995;18:525-33.