Optical Coherence Tomography in Clinical Practice
Yueh-Hung Lin
1,2, Cheng-Ting Tsai
1,2, and Ta-Chuan Hung
1,21
Division of Coronary and Vascular Intervention, Division of Cardiology, Cardiovascular Center/
Department of Internal Medicine, MacKay Memorial Hospital, Taipei, Taiwan;
2
Department of Medicine, Mackay Medical College, New Taipei City, Taiwan
Abstract
Currently, there are two intracoronary imaging techniques available to complement angiography in the management of coronary artery disease, namely intravascular ultrasound (IVUS) and optical coherence tomography (OCT). Optical coherence tomography (OCT) is a high-resolution arterial wall imaging technique with great versatility of applications. This article reviews the use of OCT for assessment of lesion severity, guidance of intracoronary stenting, and evaluation of long-term results. (J Intern Med Taiwan 2017; 28: 199-205)
Key Words: Optical coherence tomography, Intracoronary imageIntroduction
Optical coherence tomography (OCT) was first described for use in ophthalmology field and was widely used to assess retinal diseases[1]. OCT is a novel invasive diagnostic tool in percutane- ous coronary intervention. First generation OCT is based on a time domain OCT (TD-OCT) imaging method that relies on a moving reference mirror to scan each depth position in the image pixel. Due to several limitations of TD-OCT, second generation of OCT: Fourier-domain OCT systems, also known as frequency domain OCT (FD-OCT) was devel- oped. FD-OCT systems offer faster image acqui- sition speeds, greater scan depths, rapid pullback system and more simple procedure than TD-OCT[2- 7]. OCT images have 10-fold higher resolution (10-
15μm) than intravascular ultrasound (IVUS) images and allow for more accurate assessment of vascular lumen size, vascular pathology, presence of throm- bus, coronary stent strut apposition, and vascular response to previously placed coronary stents.
Clinical Application
Concomitant Medication, Patient, and Lesion Selection
Like IVUS, heparinization is recommend before inserting the guidewire into the coronary artery. To minimize the potential catheter-induced vasospasm, intracoronary nitroglycerin administra- tion is recommended if not contraindicated. While performing OCT, it needs to use contrast medium to flush the coronary artery to clear blood for full vessel visualization. In patients with severe left ven-
Reprint requests and correspondence:Dr. Cheng-Ting Tsai
Address:Division of Cardiology, Cardiovascular Center/Department of Internal Medicine, Mackay Memorial Hospital, No. 92, Chung-Shan North Road, 2nd Section, Taipei, Taiwan
tricular function impairment, a single remaining vessel, renal function impairment or known allergy to the flushing media, OCT should be used care- fully.
Evaluation of Coronary Pathology
Normal Coronary Artery
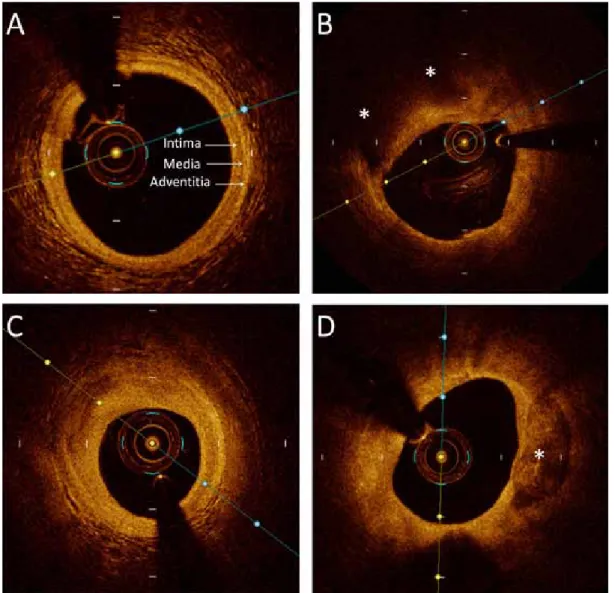
There are three layers in normal coronary arte- rial wall: intima, media and adventitia.
The intima is the innermost layer and is seen as a highly backscattering and signal-rich thin band on OCT (Figure 1A). The media is below the intima and seen as a dark band delimited by the internal elastic lamina (IEL) and external elastic lamina
(EEL). The media layer is low backscattering, signal poor and heterogeneous on OCT.
With OCT, the adventitia layer is heteroge- neous, highly back scattering and signal-rich band.
The internal elastic membrane (IEM) is defined as the border between the intima and media, and the external elastic membrane (EEM) is defined as the border between the media and the adventitia.
Atherosclerotic Plaque Assessment
Table 1 summarizes image characteristics of optical coherence tomography.
Histologically, coronary plaques are generally classified as lipid-rich, fibrous, or calcified plaques
Figure 1. Optical coherence tomography shows the three layer appearance of normal vessel wall (A), lipid plaque (B),
fibrous plaque (C) and calcified plaque (D).
based on their tissue compositions. An atheroscle- rotic plaque is identified as focal thickening or loss of the normal three-layered structure of the vessel wall. OCT has high sensitivity and high specific- ity for lipid plaque, fibrous plaque, and calcified plaque
8.
1. Lipid Plaque
Necrotic lipid pools are low signal, hetero- geneous areas with diffuse edges resulting from backscatter and rapid attenuation from the lipid-con- taining region located below a fibrous cap (Figure 1B). The fibrous cap is typically a homogeneous sig- nal-rich band overlying the signal-poor lipid core.
Lipid plaque is more heterogeneous back scatter- ing than fibrous plaques. There is a strong contrast between lipid-rich cores and fibrous regions within OCT images. The minimal thickness of the fibrous cap is critical for identifying thin-cap fibroathero- mas (TCFAs).
2. Fibrous Plaque
Fibrous plaques consist of homogeneous areas with high reflectivity and low attenuation (Figure 1C). This is distinct from lipid pools which are sig- nal-poor areas with diffuse borders and high attenu- ation
9.
3. Calcified Plaque
The features of calcification within plaques are identified by the presence of well-delineated, low- signal, slow backscattering heterogeneous regions and heterogeneous regions with sharp border (Figure 1D).
Intraluminal and Intramural Pathology
Plaque Rupture
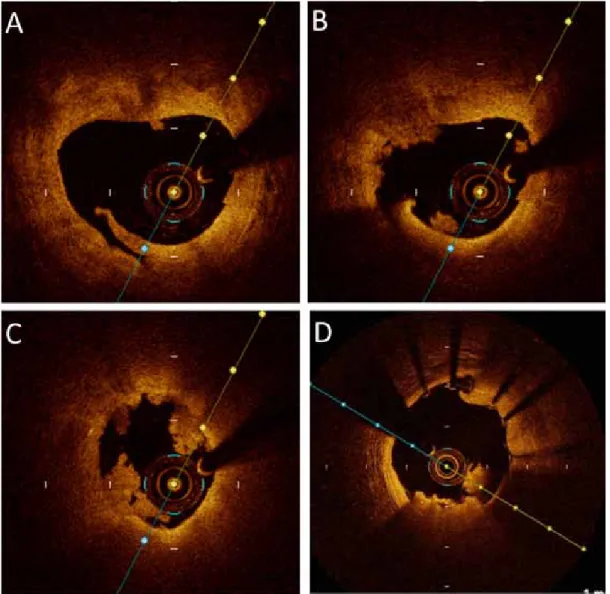
Ruptured plaques are the main mechanism of STEMI and NSTEMI. The features of plaque rupture are intimal tearing, disruption, or dissection of the cap (Figure 2A). When injected with opti- cally transparent crystalloid or contrast media, these defects may have little or no OCT signal and may appear as a cavity.
Thrombus
Thrombi are identified by the presence of irregular masses protruding into the vessel lumen either attached to the vessel wall or free within the vessel lumen. Platelet-rich white thrombi are char- acterized by a homogeneous superficial signal-rich, and low attenuation resulting in minimal shadow- ing
10(Figure 2B, 2C). Red thrombi consist mainly of red blood cells and are characterized as superfi- cial signal rich, low penetration and high attenuation with signal free shadowing (Figure 2D).
Rule of OCT in Coronary Intervention
Pre-stent Deployment
Before stenting, high resolution of OCT makes it a powerful tool to provide accurate assessment of the vessel size, lesion severity, lesion character and lesion length, which provide appropriate stent sizing. OCT also provides information on lesion characteristics such as the presence and type of thrombus, TCFA, plaque ulceration, or superficial calcification that can help to guide the procedure.
It will suggest the need for ancillary devices or for dedicated stents. Plaque dissections are common Table 1. Image characteristics of optical coherence
tomography
Tissue type Image characteristics
Lipid Low signal, Homogenous, Diffuse edges, high reflectivity, high attenuation Fibrotic High signal, Homogeneous, Poorly delin-
eated, high reflectivity, Low attenuation Calcium Low signal, Heterogeneous, Well-lin-
eated, Sharp border, Low reflectivity, Low attenuation
Red thrombus Superficial signal rich, low penetration,
signal-free shadowing, high attenuation
White thrombus Superficial signal rich, more penetration than for red thrombus, low attenuation
findings after balloon angioplasty and are associ- ated with ruptured plaques visualized by OCT. They are identified as rims of tissue protruding into the lumen.
Immediate Post-stent Deployment
One of the key points of a successful inter- vention is adequate stent expansion resulting in a well-apposed stent. OCT can accurately and quickly provide information on expansion, sizing, and appo- sition of the stent after stent implantation.
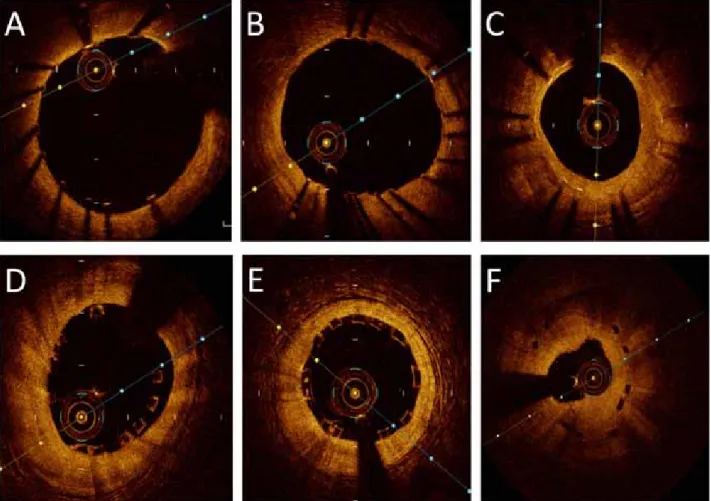
Stent malapposition is defined as the distance from the stent strut to the vessel wall greater than
the nominal stent strut thickness (Figure 3A). Stent underexpansion is minimum stent area (MSA) lower than both the nominal stent and distal reference vessel areas. Stent undersizing is MSA lower than the reference vessel area higher than the nominal stent area. OCT can measure MSA and lumen area of the reference vessel semi-automatically that gives a quick and accurate estimation of the expansion and sizing of the stent. In OCT, metallic stent struts are highly reflective and generate a strong signal with shadowing behind the stent strut. Bioresorb- able Vascular Scaffold are made of polylactide, a crystallised translucent polymer that can be pene-
Figure 2. Example of a patient admitted for myocardial infarction and optical coherence tomography showed a super-
ficial ruptured plaque (A) and white thrombus (B,C). Red thrombus is superficial signal rich, low penetration
and high attenuation with signal free shadowing (D).
trated by optical radiation and do not cause shadow- ing (Figure 3D, 3E). Absorbable stents with metallic scaffolds appear similar to typical metal stents at implantation but overtime become less reflective and lose the blooming effect. In addition to inad- equate stent expansion, OCT frequently identifies vessel dissection (a disruption in the vessel surface), intra-stent thrombus, and tissue prolapse (protru- sion of tissue between stent struts) post intervention.
Late Stent Evaluation
In long-term stent follow up, OCT is a useful examination after stent implantation.
An ideal coronary stent would allow for a thin layer of stent coverage without significant neointi- mal hyperplasia. Delayed coverage or failure to
cover an exposed stent with neointima or regener- ated endothelium could cause late stent thrombosis.
Neoatherosclerosis is pathologically distinct from neointimal hyperplasia and characterized by presence of calcification and lipid pools within the intima and formation of fibroatheromas. OCT can identify in-stent restenosis and characteristics with homogeneous appearance and a smooth lumen contour (Figure 3C, 3F). In addition to the stent strut coverage, stent strut apposition, tissue coverage, neointimal growth and are also important in long- term follow-up of stents.
Limitation of OCT
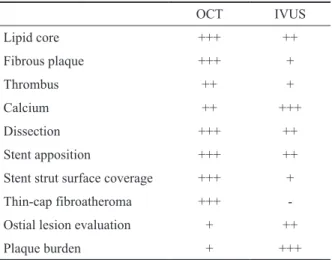
Table 2 summarize comparisons of Character- ization of Pathology Using OCT and IVUS.
Figure 3. Optical coherence tomography images immediately post-PCI and follow-up imaging of coronary stents. (A)
malapposed stent, (B) Well-apposed stent, (C) In-stent restenosis, (D) malapposed bioresorbable vascular
scaffold (BVS) restenosis, (E)Well-apposed BVS, (F) BVS restenosis.
Though OCT offer high-resolution arterial wall imaging, there are some limitations.
The main limitation of OCT is poor penetra- tion power and provide between 0.5 and 1.5 mm of imaging depth. If the thickness of plaque burden exceeds than 1.5 mm, it does not allow visualiza- tion of the media and adventitia well and hampers the evaluation of vessel wall remodeling
11-13. The second limitation OCT is that OCT requires clear- ing or flushing blood from the lumen. In severe ste- nosis lesion, the probe of OCT may occlude vessels and disturb image acquisition and interpretation.
In addition, measurement of severity of plaques in large-diameter vessels located at aorto-ostial loca- tions is difficult to assess with the current stage of technology.
References
1. Huang D, Swanson EA, Lin CP, et al. Optical coherence tomography. Science 1991; 254: 1178-81.
2. Gonzalo N, Tearney GJ, Serruys PW, et al. Second-generation optical coherence tomography in clinical practice. High-speed data acquisition is highly reproducible in patients undergoing percutaneous coronary intervention. Rev Esp Cardiol 2010;
63: 893-903.
3. Herrero-Garibi J, Cruz-Gonzalez I, Parejo-Diaz P, et al.
Optical coherence tomography: its value in intravascular diagnosis today. Rev Esp Cardiol 2010; 63: 951-62.
4. Abtahian F, Jang IK. Optical coherence tomography: basics, current application and future potential. Curr Opin Pharmacol 2012; 12: 583-91.
5. Gutierrez-Chico JL, Alegria-Barrero E, Teijeiro-Mestre R, et al. Optical coherence tomography: from research to practice.
Eur Heart J Cardiovasc Imaging 2012; 13: 370-84.
6. Tearney GJ, Regar E, Akasaka T, et al. Consensus standards for acquisition, measurement, and reporting of intravascu- lar optical coherence tomography studies: a report from the International Working Group for Intravascular Optical Coher- ence Tomography Standardization and Validation. J Am Coll Cardiol 2012; 59: 1058-72.
7. Terashima M, Kaneda H, Suzuki T. The role of optical coher- ence tomography in coronary intervention. Korean J Intern Med 2012; 27: 1-12.
8. Kume T, Akasaka T, Kawamoto T, et al. Assessment of coro- nary arterial plaque by optical coherence tomography. Am J Cardiol 2006; 97: 1172-5.
9. Kume T, Akasaka T, Kawamoto T, et al. Measurement of the thickness of the fibrous cap by optical coherence tomography.
Am Heart J 2006; 152: 755 e1-4.
10. Kume T, Akasaka T, Kawamoto T, et al. Assessment of coro- nary arterial thrombus by optical coherence tomography. Am J Cardiol 2006; 97: 1713-7.
11. Bezerra HG, Attizzani GF, Sirbu V, et al. Optical coherence tomography versus intravascular ultrasound to evaluate coro- nary artery disease and percutaneous coronary intervention.
JACC Cardiovasc Interv 2013; 6: 228-36.
12. Waksman R, Kitabata H, Prati F, et al. Intravascular ultra- sound versus optical coherence tomography guidance. J Am Coll Cardiol 2013; 62: S32-40.
13. Magnus PC, Jayne JE, Garcia-Garcia HM, et al. Optical coherence tomography versus intravascular ultrasound in the evaluation of observer variability and reliability in the assess- ment of stent deployment: the OCTIVUS study. Catheter Car- diovasc Interv 2015; 86: 229-35.
Table 2. Comparison of characterization of pathology using OCT and IVUS
OCT IVUS
Lipid core +++ ++
Fibrous plaque +++ +
Thrombus ++ +
Calcium ++ +++
Dissection +++ ++
Stent apposition +++ ++
Stent strut surface coverage +++ +
Thin-cap fibroatheroma +++ -
Ostial lesion evaluation + ++
Plaque burden + +++
+++ = excellent capability; ++ = good capability; + = poor
capability; - = impossible.光學同調斷層掃瞄在臨床上的應用
林岳鴻1,2 蔡政廷1,2 洪大川1,2
1
馬偕紀念醫院 心血管中心冠狀動脈暨周邊介入醫學科
2