科技部補助專題研究計畫成果報告
(□期中進度報告/■期末報告)
思覺失調(精神分裂)症的生物標記、治療成效與成本推估:
多樣本整合研究
計畫類別:■個別型計畫 □整合型計畫 計畫編號:MOST 104-2314-B-006 -032 -MY2
執行期間: 104 年 08 月 01 日至 106 年 07 月 31 日
執行機構及系所:國立成功大學 醫學系精神學科
計畫主持人:楊延光 教授
共同主持人:林君昱 助理教授、李怡慧 副教授、陳柏熹 教授、
陳高欽 副教授、邱南津 教授 計畫參與人員:林思賢 助理研究員
本計畫除繳交成果報告外,另含下列出國報告,共 0 份:
□執行國際合作與移地研究心得報告
□出席國際學術會議心得報告 期末報告處理方式:
1. 公開方式:
■非列管計畫亦不具下列情形,立即公開查詢
□涉及專利或其他智慧財產權,□一年□二年後可公開查詢 2.「本研究」是否已有嚴重損及公共利益之發現:■否 □是
3.「本報告」是否建議提供政府單位施政參考 ■否 □是, (請列舉 提供之單位;本部不經審議,依勾選逕予轉送)
中 華 民 國 106 年 10 月 31 日
附件一
目錄、
中文摘要---P.3 英文摘要---P.4 報告內容
研究目的---P.5 文獻探討---P.6 研究方法---P.16 期末成果與討論(含結論與建議)--- ---P.24 參考文獻---P.37 附錄(已發表論文或投稿中摘要)---P.46
中文摘要(關鍵詞)
思覺失調症的影響咸信是病人及社會沉重負擔,治療的直接與間接成本均很高昂。雖然急性精神 病發作之核心症狀會影響病程且與療效有關之生物指標變化已有報告,但是現行研究大多為回溯式研 究,故記錄未治療時的急性精神病發作之信度有所限制。此外,因此變化可能非線性現象,故在縱貫 性研究中僅設計兩個時間點也可許能有所不足。自從 1998 年起,我們開始招募未用藥的首發思覺失調 症患者進行研究,若干患者另有六個月或兩年的完整追蹤資料,至今我們仍持續招募未用藥的思覺失 調症患者進行整套評估。目前共計有 103 位患者已經被招募,並且得以在尚未投與藥物治療前,針對 若干重要的生物與心理因素上進行完整的評估及檢查,包括了結構性核磁共振、紋狀體多巴胺傳輸體 與 D2/D3 受體可利用率的單光子電腦造影(2004 年前)、認知功能、自律神經功能、事件誘發電位、
功能表現與精神病理等。在本研究中,這些過去未用藥的患者將再重複上述評估及檢查。更重要的此 次還增加 3T 功能性磁振造影配合行為作業(CPT)、功能連結與擴散張量造影等檢查用於評估患者的腦 部功能。而更精準的功能測量,如心理與社會功能,以及治療思覺失調的經濟成本等資料收集。
本研究由三個重要步驟組成,也就是在三年的計畫內同時針對三個群體進行研究,分別是:(A)
未用藥的首發思覺失調症群體;(B)全民健保資料庫中針對初次思覺失調症住院群體(樣本數大於 800)
的 12 年追蹤;(C)成大醫院針對 ICD-9295(思覺失調症)的病歷資料連結死因檔(樣本數大於 400)。
本研究在三個主要領域的發現簡述如下:
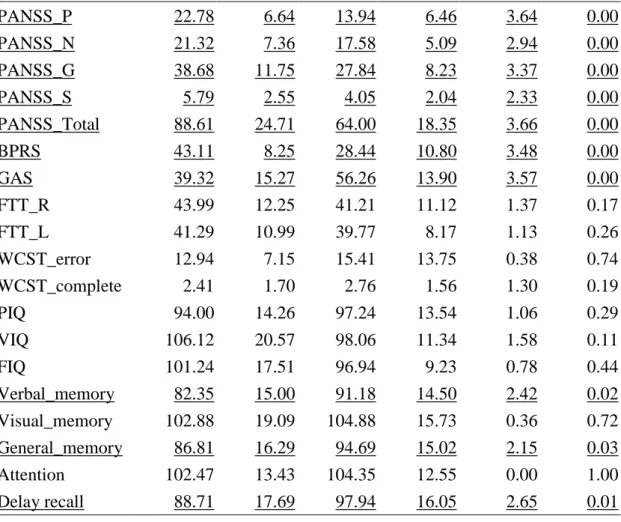
本研究目前分析之結果,可展現症狀以及療效的軌跡變化,病患的症況在各層面上都顯著的緩解,
值得注意的是,雖然在平均八年的治療後,智商沒有變化,但是記憶功能具有明顯的改善。細部分析 上,我們發現發病初期時,由單光子電腦造影測得的多巴胺活動可以顯著的預測療效(論文已發表)。本 研究發展用於功能性磁振造影的連續注意力測驗,效度獲得支持,分析結果更顯示患者在治療後的額 葉腦部活動,與發病初期的多巴胺運轉體可利用率有關,相關機制尚待釐清。其餘的研究目標,尚在 進行分析中。在二手資料分析方面,本研究結果顯示功能性為非常需要注意的課題,特別是關切此一 疾患的經濟成本研究者。針對初次住院之病人其十年後之再住院率很高,出院後四個月內就有 25%再 住院,顯示長期社區追蹤之重要(論文已發表)。終身照護的需求應當特別加以留意。與總人口相比,自 殺是患者風險最高的死因,除此之外,患者在都多生理疾患上的標準化死亡率也都偏高,應當特別留
意。上述資訊將發表(或已經發表),並且整合加入日後用來推估台灣思覺失調證患者醫療成本以及療
效評估的新模型中。
關鍵詞:思覺失調症、未用藥初發患者,神經影像學、經濟成本、療效、功能
英文摘要(關鍵字)
The impact of schizophrenia is known as a huge burden, and treatment/improving outcome is also expensive not only in direct but also in indirect cost. The core symptoms of psychosis contribute towards the progressive biological markers changes reported in schizophrenia. However, the limitation is that a retrospective assessment of the duration of untreated psychosis is less reliable. Meanwhile, it could be inadequate for using only two time points in longitudinal studies because this changes could be a non-linear pattern. Since 1998, we began to recruit drug naïve patients with schizophrenia and some of them had 6-month or 2-year comprehensive followed-up data. Moreover, this recruitment procedure for drug naive patients with schizophrenia is still ongoing till now. Those 103 patients who had been recruited, had received a comprehensive measure on several important biological and psychological variables, included structure MRI (magnetic resonance image) on brain, SPECT (single-photon emission computed tomography) imaging with dopamine transporter and striatal D2/D3 receptor availability (before 2004), cognitive function, ANS (autonomic nervous system) function, ERP (event-related potential) and their psychopathology before initial phase of antipsychotic treatment was administered. In this follow-up study, those previous naïve patients will be reevaluated the above measures. More importantly, the 3T functional MRI with behavior paradigm (Continuous Performance Test), functional connectivity, DTI (diffusion tensor imaging) will be applied to assess the brain function of patients, and more precise functionality outcomes, such as the PSP (Personal and Social Performance scale) and monetary cost of treating schizophrenia will be employed.
This study procedure will be constituted by three steps, which means simultaneously three cohorts will be conducted in this three 3-year proposal, including (A) drug naïve cohort, (B) National Health Insurance Research Databank (n>800) of 12-year follow-up cohort for first hospitalization with schizophrenia and (C) the data bank (n>400) connected with National Mortality Registry (NMR) and the medical record databank in National Cheng Kung University Hospital (NCKUH) with ICD-9 295 (schizophrenia).
Our finding demonstrated the trajectory of the symptoms, and outcomes of schizophrenia. Their severity decreased on multiple domains. In particular, the memory function is improved after 8 years treatment, although their IQ remains similar. Baseline dopaminergic activity, measured by SPECT, is predictive to the treatment outcome. Evidence supports the validity of our novel CPT paradigm, which is related with the DAT availability at the baseline. The mechanism of this finding is unclear. We are probing other effects, according to the aims of our study. Our second-hand analysis indicated that the functionality could be an important issue, for those who concern the economic cost of this disorder. The high relapse rate for patients with schizophrenia after first hospitalization was found. A need for lifelong care for patients with schizophrenia should be noticed.
Suicide had the most significantly greater risk of mortality among patients with schizophrenia as compared with the general population. Greater SMRs were also observed for other causes of mortality related to physical illnesses. Patients with schizophrenia are highly vulnerable in terms of increased mortality and require special attention. These information will be published, and integrate for our development of the new model for estimating medical cost/outcome in treating patients with schizophrenia in Taiwan.
Key word: Schizophrenia, drug naïve patient, neuroimaging, monetary cost, outcome, functionality
報告內容
(一) 前言、
The impact of schizophrenia is a huge burden, and treatment is also costly not only in direct cost (13% of total cost) but also in indirect cost (87% of total cost) ( McEvoy, 2007, Lee et al., 2008). Based on our previous study (Lee et al., 2008), its cost will be more than 1 GDP (Gross Domestic Product) per capita in Taiwan.
The ‘outcome’ is the status of the individual at a point in time (end of 2 or 5 or more years) or at the end point. Depending on the length of time for which the patient is followed up, the outcome can vary from one point in time to another. For schizophrenia, it is more relevant to study the outcome at the end of five or more years (Rangaswamy and Greeshma, 2012). Outcome consists of several independent domains, including frequency of hospitalization, medical cost, clinical symptoms, mortality, and social functioning, especially the ability to relate to people and performance at work (including employment, housework and tasks). Family burden and quality of life are other outcome measures were considered important in recent years. Besides, it had been also pointed out the need to add neuropsychological measures such as executive function, attention or memory as outcome indicators, since there is an emerging connection between neurocognitive deficits and poor outcome in schizophrenia (Bowie and Harvey, 2006) (Nuechterlein et al., 2011).
(二) 研究目的、
Three major aims will be explored in this study, the first one is the outcome in drug naïve patients with schizophrenia; the second one is their biological markers; the third one is medical costs of schizophrenia.
These three aims are described in detail as below:
Outcome domain:
1. Which variables assessed at first recruitment point, drug naïve stage, will predict patient’s outcome assessed by this checkpoint, more than three to fifteen years later?
2. To validate our new scale, SRG-PSP, with other functional outcome variables in drug naïve cohort.
Biological domain:
1. All patients’ biological or psychosocial variables will have more than twice measures in this cohort.
The relationship between the changes of these variables and the illness course will be examined in this study. The inter-correlation among these biological variables and psychosocial variables will be tested.
2. Functionality is one of outcome variables such as GAF, PSP, and SRG-PSP. Additionally, fMRI, cognitive function, psychopathology, monetary cost, hospitalization days, frequency of hospitalization, occupational status and mortality cause and age will be also used for as outcome indicators. The above (functionality) variables and biological variables will be examined for their inter-correlation.
3. The biological difference between patients and their matched controls.
Cost domain:
1. Indirect/direct cost of patients with schizophrenia will be calculated using drug naïve cohort.
2. The direct cost of patients with first hospitalization with 12-year follow-up will be calculated using NHIRD.
3. Productivity loss due to mortality will be calculated using the data bank connection with in National Mortality Registry (NMR) in Ministry of Health and Welfare and medical record databank in the NCKUH.
4. To estimate the mortality, death cause and risk factors from the combination of NCKUH medical record databank and deceased registration dataset from National Mortality Registry (NMR).
5. Finally, we will merge the above results to create a new model for estimating medical cost/outcome in treating patients with schizophrenia in Taiwan.
(三) 文獻探討、
Do progressive brain changes parallel the clinical course of illness?
Recent evidence has shown that there are dynamic and progressive brain changes in the early stages of psychosis and schizophrenia (Pantelis et al., 2003; Wood et al., 2009). These changes, which are frequently apparent in frontal and temporal regions, demonstrate that the early stage of schizophrenia is characterized by neuroprogression. Such evidence for neuroprogression is not surprising, based on observations of progressive clinical deterioration, particularly in the earliest stages of schizophrenia and psychosis. It was reported that with every episode of psychotic onset, patients with schizophrenia fail to return to their premorbid level of functioning, and progressively show a poorer clinical response to antipsychotics (Lieberman et al., 2001). In other words, the gradually and progressive clinical downhill course was suspected due to the duration of untreated psychosis (DUP) or repeated psychotic episodes of illness. However, the nature of any associated neurobiological pathology has not been systematically examined. It was proposed that there are two possibilities between the psychopathological and cerebral structure changes observed in schizophrenia. The first one is continuous, characterized by a gradual decline associated with gradual structural and functional brain changes. The second one is the trajectory change fluctuates, with intermittent rapid changes around critical points in the illness (Cropley et al., 2013). The latter might be expected at psychosis onset and with further relapses of psychosis, with partial or incomplete recoveries (Lieberman et al., 2001). It is important to investigate the relationship between clinical course and outcome and patients’ brain changes. It is surprising that only few studies have examined specifically at brain changes associated with illness relapse. It was also noticed that duration of illness and frequency of psychosis could influence the brain structure (Lieberman et al., 2001, Pantelis et al., 2003, Wood et al., 2010). Therefore, it will be better to recruit first episode or drug naive schizophrenic patients with different duration of illness to avoid the above mentioned confounding factors. One of aims of this study is to examine whether progressive brain changes parallel the clinical course of illness/outcome.
Brain structural changes associated with outcome
The majority of longitudinal MRI studies have reported progressive structural brain changes, notably enlargement of the ventricles and reduced grey matter volumes, in patients with schizophrenia (for reviews, see Hulshoff Pol and Kahn, 2008; Olabi et al., 2011). More recent studies have shown that such progressive structural brain changes are particularly prominent during the earlier stages of the illness (Pantelis and Wood,
2009; Wood et al., 2009), with less prominent changes seen in chronic patients (Hulshoff Pol and Kahn, 2008;
Kempton et al., 2010). But the results between brain changes and clinical symptomatology were inconsistent.
(DeLisi et al., 1998; Nair et al., 1997)
Progressive brain volume loss (particularly in frontotemporal regions) or ventricular enlargement have been associated with greater clinical severity (Mathalon et al., 2001). These different findings may be due to different illness stage, type of symptom, treatment response. Further, these studies provide little information on the nature of the neuroanatomical changes related to psychotic relapse, which may be informative about such discrepancies. In other words, to use a prospective design to map/detect the brain structure changes among different study intervals and different severities of psychopathology will be more appropriate to solve this discrepancy.
Interestingly, by taking into consideration illness state at each neuroimaging assessment, Garver et al.
(2000) have demonstrated specific state-related changes in brain volumes associated with a worsening or a remission of psychotic symptoms. Garver et al hypothesized that brain volumetric increases may accompany DUP, with the subsequent faster rate of volumetric reduction identified in schizophrenia at follow-up reflecting a resolution of such increases, rather than a progressive, ‘atrophic’ process. That means grey matter volumes were influenced not only by duration of untreated psychosis (DUP) but also by state of measurement.
The suggestion that transient brain expansion (‘swelling’) may accompany psychosis exacerbation is intriguing and should be examined more closely. It was proposed that brain expansion (‘swelling’), potentially caused by an active neurochemical or immunological process (such as inflammation or neurotoxicity) associated with periods of the acute psychosis itself.
More importantly, such state-related volumetric changes, assessed near the peak of brain swelling (in psychotic state), may account for the faster rate of brain structural changes identified in schizophrenia patients.
It could be inadequate for using only two time points in longitudinal studies. Because such studies do not allow the elucidation of possible nonlinear brain changes (such as relative ‘swelling’ or ‘shrinking/dips’ in brain volume) and how these relate to psychotic symptom changes. More frequent assessments are required to map/detect the precise trajectory of fluctuating brain structural changes associated with relapse and recovery.
Only few longitudinal studies had specifically explored the association between the duration of active (positive) symptoms of schizophrenia and brain volume changes. Cahn et al. (Cahn et al., 2006) retrospectively assessed the total duration of active psychosis, psychotic remission and recovery over an average of 5 years in a sample of first episode schizophrenia patients. They reported that brain volume change in the first 5 years of illness was related to the length of time that patients were actively psychotic.
Specifically, a longer duration of active psychosis (total period of hallucinations, delusions or conceptual disorganization) was significantly related to greater global grey matter loss and ventricular volume enlargement. This finding is consistent with others (Mathalon et al., 2001; DeLisi and Hoff, 2005; van Haren et al., 2007, 2008).
Regions reported as showing such an association with DUP included the left planum temporale (Takahashi et al., 2007), the left superior temporal gyrus (Keshavan et al., 1998) and the left temporal and occipital cortices (Lappin et al., 2006), but other studies in first episode of schizophrenia failed to confirm the above findings. (Fannon et al., 2000; Ho et al., 2000, 2003, 2005; Hietala et al., 2003).
Taken together, the limitation is that a retrospective assessment of the duration of active (untreated) psychosis is less reliable. It could be inadequate for using only two time points in longitudinal studies. In this proposal, the longer follow-up cohort with different study intervals and some of participants with more than two time measures will be recalled to have the final evaluation.
Striatal dopamine imaging in schizophrenia
Dopamine (DA), particularly increased nigrostriatal DA release, has been considered to play a critical role in the etiology of schizophrenia (for reviews, (Lin et al., 2013)). This inference is due to the shared mechanism of antipsychotic drugs for striatal DA D2 receptor (D2R) occupancy, suggesting that clinical efficacy (traditionally indexed as an antipsychotic potency) is directly related to their affinity for D2R (Seeman and Lee, 1975), and because the repeated use of the DA stimulant amphetamine can induce psychotic symptoms in healthy individuals and patients with schizophrenia (reviewed in Lieberman et al., 1987, (Breier et al., 1997)). Not surprisingly, there is continued interest in DA system neuroimaging with PET and single photon emission computed tomography (SPECT) in patients with schizophrenia.
The DA dysregulation in patients with schizophrenia (for reviews, see Howes et al., 2007; Lyon et al., 2011) and how these abnormalities relate to the positive symptoms of schizophrenia, and specifically, psychosis exacerbation or relapse still remain unclear. However, the most widely replicated DAergic abnormality in schizophrenia is that of elevated presynaptic DA synthesis capacity (Howes et al., 2011a) (Howes et al., 2011b). This elevation of DA in striatum has been found in drug-naïve patients with (Hietala et al., 1995, 1999; Lindstrom et al., 1999; Nozaki et al., 2009). However, the results are inconsistent (Yang et al., 2004). Although our previous study didn’t support that elevated DA in D2/D3 receptor and DAT (dopamine transporter) in drug naïve patients with schizophrenia, however, we demonstrated the striatal D2/ D3 receptor availability, measured by [123I] IBZM SPECT, was positively associated with DAT availability in drug naïve patients with schizophrenia but no association was found in healthy controls (Yang et al., 2004). Even among healthy participants measured by [123I] IBZM SPECT for their striatal D2/D3 receptor availability and by schizotypal personality questionnaire (SPQ) (Raine et al., 1994) for their schizotypal trait, those who with the higher striatal D2/D3 receptor availability was noted to have higher SPQ scores (Abi-Dargham et al., 2004) (Chen et al., 2012). Additionally, elevated striatal F-DOPA uptake has been observed in individuals experiencing prodromal symptoms of psychosis compared with controls (Howes et al., 2009), and a follow-up study (over 3 years) has confirmed that this elevation was specific to individuals who subsequently developed a psychotic disorder (Howes et al., 2011b). This finding is important as it indicates that striatal DA synthesis capacity may be elevated before the first episode of full-blown illness and may represent a biomarker of psychotic episode. Based on this evidence; we suggest that dopaminergic function changes in the brain can be considered as a possible indicator for schizophrenia therapeutic outcome.
Although the detailed mechanism of the dopaminergic activity among schizophrenia could be complex, it is worth to notice that the dopamine D2 receptor occupancy was found to be concurrently associated with clinical response (Kapur et al., 2000); it is unclear that whether the dopaminergic activity before treatment can predict the future functionality/outcome after long-term treatment. This is one of the aims of present study.
Diffusion tension imaging in early stage of schizophrenia
Diffusion tensor imaging (DTI) is a valuable tool for the study of white matte. DTI allows in-vivo quantification of the diffusion characteristics of water molecules (Basser et al., 1994, Taylor et al., 2004).
Overall, disruptions of white matter integrity were found in the cortical, subcortical brain regions and white matter associative and commissural tracts, suggesting that changes of cortical-subcortical white matter integrity were found at an early stage of schizophrenia. These changes in white matter integrity were correlated with specific cognitive deficits ( working memory) as well as psychopathology (positive more than
negative symptoms) in patients with first episode of schizophrenia (reviewed by (Kyriakopoulos and Frangou,
2009, Samartzis et al., 2013), and (Kuswanto et al., 2012)). However, these findings have to be carefullyinterpreted, as most studies have small sample sizes, and need to take into account gender and laterality effects as well as the effects of antipsychotic medications on the findings. One of aims of this study is to explore the combination of DTI findings with clinical course and other variables assessed in this cohort to enhance understanding of the neurobiology of schizophrenia and how these factors affect the white matter neuroplasticity.
Functional brain image changes in schizophrenia
Functional MRI (fMRI), which extract signals from the brain regions that show blood oxygen level dependent (BOLD) changes in cognitive task, has been also used to investigate the altered brain function of schizophrenia. Several tasks have been conducted to test the different domain of malfunction among schizophrenia (Brunet-Gouet and Decety, 2006) (Rubia et al., 2001).
A recent meta-analysis focus on the executive function task indicated an altered activity with deficits in the dorsolateral PFC, ACC, and mediodorsal nucleus of the thalamus (Minzenberg et al., 2009). Among these tasks, continuous performance task (CPT), which could be consider as a go/ no go related task, was a very important tool to investigate the executive function among patients with schizophrenia (Cornblatt et al., 1997).
Schizophrenia tends to have poor performance on CPT, and this poor performance was found to be association with negative symptoms (Nieuwenstein et al., 2001). Our team studied on the performance of community residents (n=1,728) of CPT (Hsieh et al., 2005). In particular, we also found that the performance of CPT is associated with the economic cost of schizophrenia (Ko et al., 2003), and the plasma concentration of risperidone is also associated with the CPT performance in medicated patients with schizophrenia (Chen et al., 2004).
Combining CPT as a challenge task and functional brain image technique has been addressed as a powerful tool for investigating the neurophysiological process (Hager et al., 1998), and a decreased frontal activation in schizophrenia during CPT was found (Volz et al., 1999). Carter et al (2001) reported a group difference on the activity in the anterior cingulate cortex in schizophrenia. A study using both voxel-based morphometry (VBM) and CPT as fMRI protocol reported both structure and functional deficit in the thalamus,
the anterior cingulate and the inferior parietal, which involved in attentional deficit, among schizophrenia (Salgado-Pineda et al., 2004). It was also found that alter brain response among unaffected healthy siblings of schizophrenia (Sepede et al., 2010).
Although the detailed neural network involved in the clinical CPT (e.g. Conners’ CPT) has been investigated (Ogg et al., 2008), the brain activity during CPT among schizophrenia, and its association with other factors, such as disease outcome, ERP (evoke related potentials), DTI and dopaminergic activity, is unclear.
This is one of the aims to explore the relationship among regional changes in fMRI and the above mentioned variables of present study.Event-Related Potentials: P 300 in schizophrenia
The P300 event-related potential (ERP) is a positive deflection of the electroencephalogram following about 300 ms after a participant receives an attended unusual or a task-relevant stimulus. Our previous study, using two isotopes (Tc-99m TRODAT-1 for DAT and I-123 ADAM for SERT), also showed that the P300 measures in auditory oddball paradigm were correlated with DAT and serotonin transporter availabilities (Lee et al., 2011).It has been reported that patients with schizophrenia have lower values in P300 amplitudes (McCarley et al., 1991, Ford et al., 1992, Ozgurdal et al., 2008). Neurophysiological changes such as the reduction in P300 amplitudes begin early in patients with schizophrenia in the prodromal phase, and those
changes are found to run a progressive course, from the prodromal to the chronic phase of schizophrenia (Ozgurdal et al., 2008). Two recent meta-analyses of P300 in auditory oddball paradigms also found large pooled standardized effect size of 0.85 and 0.89 for P300 amplitudes differences between patients with schizophrenia and controls at central (Cz) and parietal (Pz) midline electrode sites(Jeon and Polich, 2003, Bramon et al., 2004). Association of P300 amplitudes with neurodegenerative progression of different cortical regions has also been demonstrated (Martin-Loeches et al., 2001). Although medications have been found to enhance P300 amplitude in some studies (Mathalon et al., 2000, Bramon et al., 2004), P300 amplitude is generally not restored to normal levels (Ford et al., 1994, Hirayasu et al., 1998, Jeon and Polich, 2003).
Therefore, P300 ERPs are thought to be robust vulnerability indicators for schizophrenia.
But, our previous study of drug naïve patients with schizophrenia showed that the P300 ERP is not altered in the early stages of schizophrenia before medication is introduced, and the DAT availability does not influence the P300 ERP amplitude or latency (Chen et al., 2013). The mean P300 ERP showed no significant difference between patients and controls in latency or in amplitude. There was a significant gender effect with females showing greater P300 amplitude than males. The difference between patients and controls in P300 latency became more pronounced with ageing, with latency increasing faster in patients. Our explanation for the above results is that the P300 ERP could be an indicator of the progression of illness and chronicity. It is possible in the early stage of schizophrenia that the ERP could be no difference, compared with their controls.
A significant age by group interaction on P300 latency, whereby the difference between patients and controls in P300 latency became more pronounced with ageing, with latency increasing faster in the patients. The relationship between the latency and age is similar at the other two sites (Cz & Fz). In this proposal, we speculated that ERP P300 could play a partial role in the long-term outcome predicting.
Cognitive functions in early phase of schizophrenia:
The cognitive deficits in patients with schizophrenia were not inversely related to the DUP (Goldberg et al., 2009); other studies even reported patients exacerbated their oculomotor delayed response task performance after 6-week antipsychotic use (Reilly et al., 2006). Since deficits in cognitive function have been demonstrated in studies of drug naïve first-episode schizophrenic patients (Lussier and Stip, 2001), the effectiveness of antipsychotics on the cognitive function may be viewed as an important outcome of schizophrenia.
From our preliminary data, the group of GAF scores≧60 also showed significantly better cognitive function than the group of GAF scores<60 on cognitive measures. Impaired verbal memory is associated with poor community functioning and poor response to psychosocial rehabilitation programs ( Green et al., 2000, Evans et al., 2004, McGurk et al., 2009). Based on our previous study, those drug naïve patients with schizophrenia (n=33) were noted poorer cognitive function compared with their healthy controls. Eleven participants from our preliminary data received the cognitive assessments at initial enrollment and 6 months later for the analysis, their simultaneous verbal memory and GAF score improvements were observed, though the GAF score change was not significant yet. It seems that the natural course of schizophrenia is progressive downhill. In addition to cognitive deficit in drug naïve patients, our previous study also showed the cognitive difference between health individuals with higher schizotypal score and lower score. The higher schizotypal subgroup showed poorer executive function compared with their lower score group. (Chang TG et al Psychiatry and Clinical Neuroscience 2011)
In schizophrenia, abnormalities are observed in frontotemporal cortical networks during verbal working memory, word encoding, and word recognition (Ragland et al., 2004, Leeson et al., 2009); an abnormality of
prefrontal cortex and its connections to posterior cerebral regions for memory functions has also been supported by brain functional studies (Hazlett et al., 2000). In this proposal, we will continue our work to correlate among the cognitive functions, DTI, structure changes (fMRI & VBM), DAT availability and ERP in the naturalistic treatment effectiveness follow-up cohort.
Functionality measures
Social functionAs we mentioned before that outcome consists of several independent domains, social functionality is one of the most important outcomes in patients with schizophrenia.
Before the development of the Personal and Social Performance (PSP) scale, the main and popular measure instrument of social function was the Global Assessment of Functioning Scale (GAF) which was hard to represent the different psychosocial aspects since its' global rating natural and not at all sensitive to variation in social cognition (Robertson et al., 2013). To fulfill the need to supplement the measurement of psychosocial function using the GAF in clinical practice with functional measures that are more sensitive to deficits in social cognition, the PSP scale was designed to measure psychosocial functioning within four domains: socially useful activities, personal and social relationships, self-care, and disturbing and aggressive behavior (Morosini et al., 2000) both for patients with acute (Patrick et al., 2009) or chronic psychotic symptoms (Nasrallah et al., 2008). Our previous investigation also found that PSP score having good reliability for cognitive function and Activities of Daily Living (ADL) evaluation (Hsieh et al., 2011).
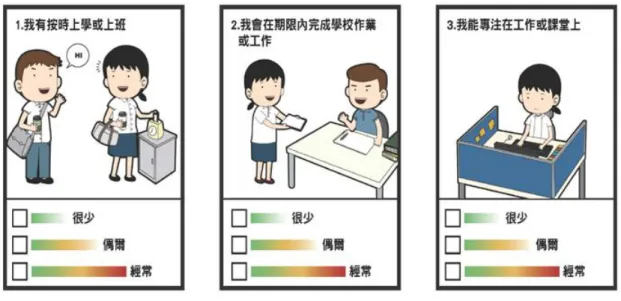
However, due to limited time for clinicians to assess patients’ psychosocial function in their daily practice, a self-rating scale for measuring functionality could be helpful. Regarding the prominent cognitive deficits in executive function, processing speed and verbal memory, but less impairment in visual/spatial perception/memory, were noted in individuals with schizophrenia. A self-reported version of graphic PSP (SRG-PSP) was developed which was revised from the PSP (Bai et al 2014). We proposed that it could be helpful and better, particularly in a large sample survey.
These graphic items (Figure 1) were cartoon-like pictures which the participant is easy to catch the meaning of each item by patients with schizophrenia. At first, there were 12 items for each single domain, after the scale has been reviewed by 10 senior psychiatrists for its content validity; the final version was 22 items in total. The Cronbach's alpha coefficient was 0.83.
Global Assessment of Functioning (GAF) scale:
The GAF scale may be particularly useful in tracking the clinical progress of individuals in global terms using a single measure (Flyckt et al., 2006). We plan to use scores on the GAF scale for correlation analyses supplemented to psychosocial function and outcome. According to the DSM –IV, a GAF cut-off point of 60 generally well distinguishes between good and poor socio-occupational function (Goldman et al., 1992); we therefore choose it as the cut-off point for good/poor outcome. The inter-correlation between SRG-PSP and GAF and its monetary cost will be explored in this proposal.
Figure 1. The example of SRG-PSP (Bai et al Schizophrenia Research, 2014)
Monetary cost of schizophrenia
The global burden of schizophrenia is heavy. According the newest estimation, schizophrenia accounted for 7.4% of DALYs caused by mental and substance use disorder (Whiteford et al., 2013), and the all ages years lived with disability (YLDs) increased 47.5% between 1990 to 2010 (Vos et al., 2012). Since the YLDs estimation correlated to the prevalence rate, even acute schizophrenia had the highest disability weight of all disorders in that study but did not rank highly as major depressive disorder or anxiety disorder, which represent the possibility to underestimate the cost of schizophrenia to individual and society by DALYs.
The monetary costs related to schizophrenia have demonstrated a wide variation across countries (Chan et al., 2003, Yao and Wu, 2005, Brissos et al., 2008, Lee et al., 2008, Williams et al., 2008, Yen et al., 2008), it is difficult to compare estimates from these cost-of-illness studies due to differences in the methods, scope of analyses and the range of costs covered. In the human capital approach, the only common result across the studies was that the major cost came from the indirect costs, ranged from 51% (Law et al., 2005) to 87% (Lee et al., 2008). The indirect costs scope varied by studies, but mainly estimated for reported productivity losses of patients and families, the losses might also include joblessness, the premature mortality, and the family care-giving.
Most cost estimate studies derived from either survey or national statistic, however, the scale of survey were often too small to be representative, and some information such as the cost of family caregiver were limited from the national statistic data, or might limited to the variety of secondary sources and some official
data publicly available was not the latest.
To increase the preciseness, recent studies were more likely to aggregate the data from different levels.Our team had estimated the cost of schizophrenia outpatients based on survey couple years ago (Lee et al., 2008). The results showed that indirect cost was 87% of the total cost which patient’s poor work performance and their caregiver’s joblessness are major loss. Additionally, we found that the patient's age and global functions had a significantly negative relationship with the direct costs. To improve patients'
functionality and decreasing caregivers' burden are essential to reducing costs. However, due to the small sample, participants characteristic and recall bias, the medical cost estimation might not be precise. For better estimation, we would like to focus on these patients with schizophrenia who was first hospitalization with 12-year follow-up cohort and calculate their direct medical cost, based on nationwide claim data bank.
Relapse and medical cost of first hospitalization schizophrenia
First episode psychosis of schizophrenia occurs mostly during young adulthood. The chronic and deteriorated course of schizophrenia led to remarkable impairment in mental health, cognitive function and socio-occupational function (Lieberman et al., 1996). The impact extends from personal to family and social level and makes heavy caring burden, medical cost and decline in labor productivity.
For those with first episode psychosis, to stabilize and control symptoms effectively is important. The relapse of psychotic symptoms would lead to further impairment, and the stability of disease in the first five years after onset could be predictor of prognosis (Emsley et al., 2012a, Emsley et al., 2013b). Previous studies showed that more than 80% of patients suffered from symptoms relapse in five years following first episode psychosis ( Robinson et al., 1999). About 20% of those with continuous treatment would experience relapse in one year, but the percentage rise to 60~90% in those without continuous treatment (Wunderink et al., 2007, Boonstra et al., 2011). However, around half of the patients’ adherence became irregular after 1~2 years of treatment in estimation (Perkins et al., 2008, Emsley et al., 2012b). The risk of relapse is also associated with character of symptoms, family support and insight, baseline adaptation ability and patient’s insight, and comorbidity (Miller et al., 2011, Tiihonen et al., 2011, Alvarez-Jimenez et al., 2012, Emsley et al., 2013a).
However, those mentioned studies focused on the first 1 to 5 years course. The study for longer course is still scarce. Although, the medical service, national health insurance system, for patients with schizophrenia is comprehensive in Taiwan, considering the limited resources of health insurance, the medical expenditure must be re-organized and regulated. Appropriate and efficient medical services utility model thus becomes essential issue.
Previous studies had explored risk of relapse, medical service utilization, and the association between them in schizophrenia patients (Shek et al., 2009, Marshall et al., 2011, Killaspy et al., 2013). One study reported correlation between duration of hospitalization and re-admission rate one month after discharge: the lesser days of hospitalization, the higher risk of re-admission (Lin et al., 2006). Considering differences in geographical area, the public opinion and awareness of psychiatric illness, pattern of medical services utilization, and insurance system, it is worth conducting such study for Taiwanese patients with schizophrenia.
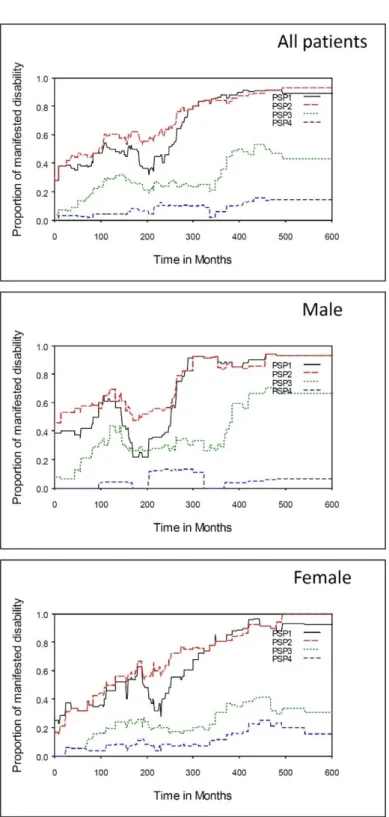
Our preliminary data show, using National Health Insurance Research Databank (NHIRD), subgroup with more relapse episode would more likely to become chronicity in a 10-year follow-up cohort after first hospitalization.
Mortality, cause of death and life expectancy in patients with schizophrenia
It is well known that patients with schizophrenia have at least two to three-fold higher mortality rates compared with the general population (Ö sby et al., 2000, Saha et al., 2007a, Hsiung et al., 2010), corresponding to a 10- to 25-year reduction in life expectancy (Laursen, 2011, Laursen et al., 2012). The excess mortality among schizophrenia patients, from both natural and unnatural causes (Ö sby et al., 2000, Hsiung et al., 2010, Laursen et al., 2012), suicide and other unnatural causes used to be considered the riskiest death cause (Hsiung et al., 2010), however, recent studies has found that the main cause of excess deaths was natural causes (Ö sby et al., 2000, Laursen, 2011, Laursen et al., 2012), and one of the leading cause was
cardiovascular disease (Ö sby et al., 2000, Crump et al., 2013).
Recent studies showed that the differential mortality gap has worsened in recent decades (Saha et al., 2007a). It has been suggested that main reasons for the excess mortality and reduced life expectancy of schizophrenia, except the high risk of suicide and accidents, the suboptimal lifestyles, the adverse effects of antipsychotic drugs, and the diagnosed late and treated insufficiently of physical illnesses (
Laursen et al., 2012). Regarding these reasons, the effect of second-generation antipsychotic medications was controversial (Saha et al., 2007b, Tiihonen et al., 2011), and the medical care accessibility issues for under treatment was also difficult to explain since the continuing excess mortality still remains after implementation of NHIRD (Hsiung et al., 2010) and finding in Scandinavian area (Ö sby et al., 2000, Laursen, 2011, Crump et al., 2013). Therefore, it is still necessary to review the medical records for deceased patients with schizophrenia carefully, to find the details of their treatment, adherence, co-morbidity, and demographic related to the death cause.
In this proposal, we'll analyze the mortality, cause of death and the risk factor of NCKUH schizophrenia cohort (1998-2010). There were 4, 377 patients with schizophrenia identified from NCKUH medical record, and 408 of them, identified from individuals’ mortality cause in National Mortality Registry (NMR), were deceased until the end of 2011. The preliminary results were showed that 339 patients with schizophrenia died, based on the NMR data base. The SMR (standardized mortality ratio) in this cohort is similar to those of previous studies (Ö sby et al., 2000, Saha et al., 2007a, Hsiung et al., 2010). The loss years of life expectance was prominent in patients with schizophrenia.(Table 8, Table 9) The following predictors for mortality will be explored using the medical chart reviewing method.
Naturalistic cohort follow-up: the duration of study—longer will be better
Course and outcome of patients with schizophrenia have been studied by the World Health Organization (WHO) in international studies, and the global assessment of functioning scale (GAF) have widely been used as a standard outcome measure (Hopper and Wanderling, 2000, Harrison et al., 2001) . The prospective cohort studies of drug naïve patients have reported their metabolic changes after antipsychotic use (Correll et al., 2009, Perez-Iglesias et al., 2009). A significant brain volume change was also observed after early treatment in drug naive patients in a 8- week naturalistic study (Deng et al., 2009). Drug naïve patients with schizophrenia improved the functioning in the anterior cingulate cortex after 4-week antipsychotic use on their event-related brain functional MRI (Snitz et al., 2005), it suggested that anterior cingulate cortex functioning may be especially sensitive to remedial antipsychotic treatment effects (Snitz et al., 2005). One 3-year prospective study also reported that although the quantity of neurological soft signs does not significantly change in the 3 years that follow the first episode, but the relationship between neurological soft signs and negative symptoms does not become apparent until 1 year after the initial episode (Chen et al., 2005). Even an 18–month community outreach follow–up study for untreated patients, which included drug naïve cases (27%), showed improvement on their psychotic symptoms, disability and family burden after received outreach services (Srinivasa Murthy et al., 2005). Beside aforementioned short term observations on pharmacological and brain structure changes of drug naïve patients; like the 2-year naturalistic Belgian schizophrenia outcome survey on patients stabilized on medication, the results showed that functional impairment become more significant in this longer follow-up survey. (Peuskens et al., 2009). In summary, it seems a longer observational duration is needed for the outcome evaluation.
A more systematic longitudinal study could potentially be informative about the way in which the relationship between neurobiological changes and symptoms/outcome might evolve over time. It was
proposed that altered dopaminergic system among schizophrenia has been established as a pivot mechanism of schizophrenia (Carlsson, 1988, Howes and Kapur, 2009, Howes et al., 2009), comprehensive evidence on the longitudinal change on their dopaminergic activity, as well as their neuropsychological function (Rund, 1998), and event-related potential (ERP) (Ozgurdal et al., 2008) is needed to further study. Meanwhile, little is known about the inter-correlation between the mentioned variables and the brain activity during the cognitive task among schizophrenia (Snitz et al., 2005). Functional magnetic resonance imaging (fMRI) could be a potential safety tool to identify the potential biomarker that concurrently associated with the treatment outcome and their functionality. Therefore, in this project, we are especially interested in the patients’ changes of brain structure, neurotransmitter (DA), neurobiological (ERP) and cognitive functions, and psychosocial adaptation after a longer therapeutic intervention; therefore we wish to design a longer
duration follow-up study. Meanwhile, as fMRI could be considered as a non-invasive and safety tool to assess the brain structure and function during specific task, we propose to conduct a structural and task-dependent (CPT) fMRI, to probe the potential surrogate markers of schizophrenia. Advance resting state analysis, such as functional connectivity, voxel-based morphometry (VBM), and diffusion tensor imaging, will be employed.
The niche of this drug naïve cohort in this proposal
Since 1998, we began to recruit drug naïve patients with schizophrenia in our clinics and some of them had 6-month or 2-year comprehensive followed-up data. Moreover, this recruitment procedure for drug naive patients with schizophrenia is still ongoing till now. At first, these patients received a comprehensive research protocol including MRI, SPECT imaging with DAT and striatal D2/D3 receptor availability(before 2004), cognitive function, auto nervous system (ANS) function, ERP and their psychopathology measures before initial phase of treatment. The comparisons between drug naïve patients and their controls were reported in several famous journals such as Am J of Psychiatry, Schizophrenia Bulletin or Psychological Medicine (Yang et al., 2004, Chen et al., 2013, Chen et al., 2014).The rest of mentioned results are still in the process of submission (Hsu et al., J Affective Disorder, revised, for cognitive deficit Chang et al. 2014, for ERP in gender difference). Currently, we have recruited more than 103 drug naïve patients with schizophrenia Some of them also received 6-month and/or 2-year follow-up reevaluation, depended on different protocols. In this comprehensive naturalistic cohort study, we will not only reevaluate the above mentioned variables but also conduct a fMRI study with well-established cognitive task (CPT) and their functionality variables and monetary cost during this period. Regarding the outcome measures, in addition to using treatment response, such as psychopathological changes during follow-up period, the functionality changes during follow-up period will be also emphasized. The advantage of this cohort is that the assessment of recruitment at the beginning stage is quite comprehensive, moreover, some of these participants were assessed more than two times, and the final assessment will be more comprehensive, including fMRI. Therefore, not only different outcome but also its inter-correlation among different biological variables and psychosocial variables could be tested in this study. Finally, we will merge the above results, combined with the results from the other data mining results which will be mentioned as follows, to create a new model for estimating medical cost/outcome in treating patients with schizophrenia in Taiwan.
Using two data banks to explore 12-year outcome and causes of mortality of schizophrenia
As the cost-effectiveness for the treatment for schizophrenia is an important issue, identifying the factors that can predict the severity after treatment could be important (Milev et al., 2005). Regarding the patient’s
number being small in drug naïve cohort, large sample size with the long-term outcome and the causes of mortality in patients with schizophrenia will be explored in this study. Two data banks will be used, the first one is the National Health Insurance Research Databank (NHIRD), and the second one is connection between data banks of nationwide deceased individuals’ mortality cause in National Mortality Registry (NMR) and the medical record in National Cheng Kung University Hospital (NCKUH) with ICD-9 295 (schizophrenia).
(三) 研究方法
This study procedure will divide into three parts. It means simultaneously three cohorts will be conducted by this research team in this 3-year proposal, included:
(A) Drug naïve cohort,
(B) NHIRD of 12-year follow-up cohort for first hospitalization with schizophrenia,
(C) Mortality cause cohort for the data bank connected with National Mortality Registry (NMR) and NCKUH for causes of mortality in patients with schizophrenia.
I. Methods for (A) drug naïve cohort
We will conduct a follow-up study, in which the individuals had participated in previous studies (Atomic Energy Council, N3I102 (1998-99), 90NU-7-006-004(2001-02), 91NU-7-006-004(2002-03), and National Science Council, NSC 99-2314-B-006 -019 -MY3 (2010-2013) as drug naïve schizophrenia will be recalled.
In the previous studies, the SPECT, ERP, cognitive function, and psycho-social function had been assessed.
Currently, its potential sample size will be more than
103
participants. In this follow-up study, we will conduct a retest on these variables. Meanwhile, a fMRI and more functionality measures will be employed in this study. These data will be analyzed as a naturalistic cohort study, and the clinical severity measured, used standard instrument (i.e. GAF, BPRS, PANSS, ESRS, AIMS) will be probed.1. Sample:
A total of 103 patients with schizophrenia, who participated in our previous study, will be recalled from the psychiatric outpatient clinic of National Cheng Kung University Hospital (NCKUH) or community. The healthy controls will be excluded, if any medical condition was noted and they will be interviewed by a senior psychiatrist using MINI to rule out any psychiatric morbidity. We estimate at best only 75 % of our previous participants could be recalled. Their age and gender matched healthy controls (n=75) will be recruited from community via advertisement. Our previous criteria for patients are showed as below:
1.1 Inclusion criteria:
1. Patients should fulfill with Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria and they are diagnosed and interviewed by experienced psychiatrists who have been practicing more than 5 years.
2. Age between 18 and 65.
3. No physical illness and with stable vital signs and no evidence of substance abuse/dependence as assessed during the clinical interview with the research psychiatrist at the time of enrollment.
4. Never received any antipsychotic or antidepressant treatment and were free of any psychotropic medication at the time of testing.
5. Patient or his (her) legal caregiver have signed an informed consent document, indicating that they understand the purpose and procedures of the study.
1.2 Exclusion Criteria:
1. Other co-morbid psychiatric illnesses, substance abuse/dependence, or neurological illnesses.
2. Mental retardation.
3. Pregnant patients or patients are suspected to be pregnant. Childbearing age female patients should agree an acceptable form of contraceptive use during the conduct of the study in order to be included.
4. In the judgment of the investigator, the patient is at risk of suicide/ harming, precautions against suicide/ harming risk must be employed.
5. Patients who have been assessed by the investigator not to be suitable to enter this study due to some other reasons.
2. Objective Measurements:
Before participating this study, the participants should sign the inform consent which was approved by local IRB at NCKUH. Currently, NCKUH IRB had approved this proposal in (2014-07-01, the approval number is A-BR-103-017.)
Part 1 measurements:
Brain imaging examinations
1. Brain image studies with [99mTc] TRODAT-1 single positron emission computed tomography (SPECT), and functional magnetic resonance imaging (fMRI).
SPECT, [99mTC] TRODAT-1
A single bolus injection of 740 MBq (20 mCi) [99mTc]TRODAT-1(a radio labeled form of tropane derivative for selectively labeling dopamine transporter) is administered, we use a triple-headed rotating gamma camera (Multispect3; Siemens, Hoffman Estates, Illinois, USA) with ultra high-resolution fan-beam collimators, with an energy window of 15% centered on 140 keV for technetium-99m. Imaging of [99mTc]
TRODAT-1 is initiated approximately 240 minutes after injection of [99mTc] TRODAT-1.
An experienced nuclear medicine specialist draws the regions of interest manually on the basis of the individual magnetic resonance images (GE Sigma CV-I, 1.5 T, General Electric Systems, Milwaukee). The ratio of the radioactivity in the striatum to that in the cerebellum is derived by dividing the average counts per pixel in the striatum by the average counts per pixel in the cerebellum. The density of dopamine transporter (DAT) is measured by the ratio. T-1 weighted MRI will be obtained on the same day or later in axial planes on a Megaton 1.5 Tesla scanner. The SPECT and MRI images are registered using internal markers. It is very important for MRI in [99mTc] TRODAT-1 SPECT study because the MRI will be served as a reference for defining the area of striatum/cerebellum of the SPECT image which DAT was located.
fMRI of the brain
The fMRI will constitute with a resting-state fMRI (van den Heuvel and Hulshoff Pol, 2010) for the functional connectivity (Aertsen et al., 1989, Friston et al., 1993), diffusion tensor imaging (DTI) and VBM (Salgado-Pineda et al., 2004), and CPT for assessing the brain function during decision making. A structural MRI will be collected as well for coregistration.
Resting-state fMRI
Resting-state fMRI is an advance technique to exploring the default mode network (DMN). The brain network could be defined as functional connectivity within brain areas. Conventional fMRI is focused on the spatially distributed brain areas, while resting-state fMRI could analysis the temporal dependency of neuronal activation patterns of anatomically separated brain regions (van den Heuvel and Hulshoff Pol, 2010).
Resting-state fMRI has been applied to assessing the association between default mode network with behavior, emotion, and social response as well as some psychiatric disorders (Buckner et al., 2008, Greicius, 2008).
During the resting-state fMRI procedure, the subject will be instructed to close eyes and rest, while avoid any
movement as possible. The echoplanar imaging sequence (EPI) will be conducted for data acquisition for 5 minutes (TR/TE = 2000/50 ms, 32 axial slices, voxel dimensions = 3.1×3.1×4 mm to cover the whole brain).
A voxel-wise and ROI-wise method will both be conducted for data analysis.
Diffusion tension imaging
DTI data were obtained on the same 3T fMRI. Single-shot spin-echo planar imaging (EPI) with a twice-refocused balance echo sequence to reduce eddy current distortions will be used. TR/TE=6,300/85 ms, field of view=220 m, b=1,000 s/mm2 along 32 directions, 45 contiguous slices, three imaging series, and a voxel size of 1.7×1.7×3 mm. All data processing was executed at Hartford by investigators who were blind to diagnosis and used the same methods and quality thresholds. Data were checked for noise, motion, and artifacts (seven subjects at Hartford and 34 at Baltimore were excluded). FSL software (www.fmrib.ox.ac.uk/fsl) was used for standard analysis including motion correction and eddy current correction, with coregistration to the B0 image with gradient directions corrected. Fractional anisotropy was used to assess white matter integrity. To enhance reproducibility and overlap of white matter fibers, we calculated a common white matter skeleton and used tract-based spatial statistics (Smith et al., 2006).
fMRI with CPT
The paradigm is similar to the blocked fMRI design of Ogg et al. (Ogg et al., 2008). Acquisitions were made during a 5 minutes run contained 15 blocks. The “watch” block started firstly and then pictures shuffled the pixel from the same digital stimuli employed in task block appeared on the screen for 50 ms with 950 ms interstimulis interval. Participants did not need to respond for any stimuli during this block. In the “task”
block, Single digit stimuli (0 tough 9) were presented for 50 ms, with a 950 ms interstimulus interval. The participants were instructed to press a “target” button as fast and as accurately as possible with their right thumb finger when the target digit “9” followed by digit “1”.
fMRI data acquisition
Image will be acquired using a 3.0 T GE MR750 MRI scanner system at Mind Research and Imaging Center in NCKU, a new center for fMRI study funding by NSC. Functional data will be acquired with a T2*-weighted gradient-echo EPI using BOLD contrast (TR = 2000ms, TE = 50 ms, flip angle = 90 degree, slice thickness = 4 mm, interslice interval = 0 mm, field of view = 230 × 230 mm2, 64 × 64 × 32 matrix, whole brain coverage). The first five images of each session were discarded from the analysis. The anatomical image was acquired using a high-resolution T1-weighted 3D gradient-echo pulse sequence (TR = 88.1ms, TE
= 4.12 ms, TI = 650 ms, flip angle = 90 degree, slice thickness = 1.5mm, field of view = 230 × 230 mm2, 256× 256 × 128 matrix).
Data process and analysis
Image and statistical analysis will be processed with SPM8 (Welcome Departament of Cognitive Neurology, London, UK). Scans will be realigned, time corrected, coregistered, normalized, and spatially smoothed with a 4 mm full-width-at-half-maximum Gaussian Kernal with SPM. Generalized Linear Model will be used to model the event timecourse of each subjects. Regional differences were statistically thresholded at p < .05, FDR corrected for multiple comparison, voxel extent (k) > 10, in within-subject analysis. A random-effect model will be applied for second-level random effects group analysis.
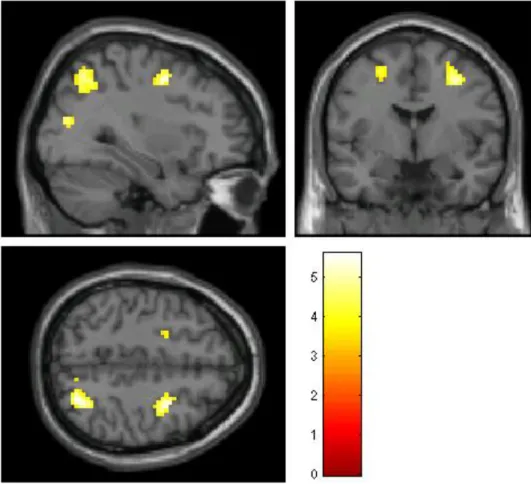
Currently, the software of CPT in fMRI had been settled down in our team. The preliminary results for fMRI with CPT in healthy participants showed anterior cingulate cortex and frontal cortex regions activation which is similar to previous research.
2. Event-related potentials (ERP) study