Full Terms & Conditions of access and use can be found at
https://www.tandfonline.com/action/journalInformation?journalCode=wwah20
Women & Health
ISSN: 0363-0242 (Print) 1541-0331 (Online) Journal homepage: https://www.tandfonline.com/loi/wwah20
The Effects of Perceived Stress and Life Style Leading to Breast Cancer
Lee Wang PhD , Wen-Chun Liao PhD , Chung-Jung Tsai PhD , Li-Rong Wang MS , I-Fang Mao PhD , Chun-Chieh Chen MD PhD , Pan-Fu Kao MD MS &
Chung-Chin Yao MD PhD
To cite this article: Lee Wang PhD , Wen-Chun Liao PhD , Chung-Jung Tsai PhD , Li-Rong Wang MS , I-Fang Mao PhD , Chun-Chieh Chen MD PhD , Pan-Fu Kao MD MS & Chung-Chin Yao MD PhD (2013) The Effects of Perceived Stress and Life Style Leading to Breast Cancer, Women &
Health, 53:1, 20-40, DOI: 10.1080/03630242.2012.732680
To link to this article: https://doi.org/10.1080/03630242.2012.732680
Accepted author version posted online: 09 Oct 2012.
Published online: 19 Feb 2013.
Submit your article to this journal
Article views: 706
View related articles
Citing articles: 10 View citing articles
Copyright © Taylor & Francis Group, LLC ISSN: 0363-0242 print/1541-0331 online DOI: 10.1080/03630242.2012.732680
The Effects of Perceived Stress and Life Style Leading to Breast Cancer
LEE WANG, PhD
Department of Public Health, Chung-Shan Medical University, and Department of Family and Community Medicine, Chung-Shan Medical University Hospital, Taichung, Taiwan
WEN-CHUN LIAO, PhD
School of Nursing, Chung-Shan Medical University, Taichung, Taiwan
CHUNG-JUNG TSAI, PhD
Department of Occupational Safety and Health, Chung Hwa University of Medical Technology, Tainan, Taiwan
LI-RONG WANG, MS
Department of Public Health, Chung-Shan Medical University, Taichung, Taiwan
I-FANG MAO, PhD
Department of Occupational Safety and Health, Chung Shan Medical University, Taichung, Taiwan
CHUN-CHIEH CHEN, MD, PhD
Department of Family and Community Medicine, Chung-Shan Medical University Hospital, and School of Medicine, Chung-Shan Medical University, Taichung, Taiwan
PAN-FU KAO, MD, MS
School of Medicine, Chung-Shan Medical University, and Department of Nuclear Medicine, Chung Shan Medical University Hospital, Taichung, Taiwan
CHUNG-CHIN YAO, MD, PhD
School of Medicine, Chung-Shan Medical University, and Department of Surgery, Division of General Surgery, Chung Shan Medical University Hospital, Taichung, Taiwan
Researchers conducted a study in a Taiwanese medical center from June 2009 to June 2011 to investigate the relations of perceived
Received January 22, 2012; revised September 14, 2012; accepted September 14, 2012.
Lee Wang and Chung-Chin Yao contributed equally to this work.
This study was supported by grant CSH-2010-A-03 from Chung-Shan Medical University Hospital, Taiwan.
Address correspondence to Lee Wang, PhD, Department of Public Health, School of Medicine, Chung Shan Medical University, No. 110, Chien-Kuo N Rd, Sec. 1, Taichung, 40242, Taiwan, Republic of China. E-mail: [email protected]
20
stress and lifestyle to breast cancer. A total of 157 cases and 314 controls completed a structured questionnaire. Using multi- ple logistic regression models, high perceived stress (adjusted odds ratio [AOR]= 1.65; 95% confidence interval [CI], 1.10–2.47), less than 1,000 kcal of physical activity expenditure per week (AOR, 2.17; 95% CI, 1.39–3.39), and high intake of fried and stir-fried food (AOR, 1.86; 95% CI, 1.24–2.77) were positively associated with breast cancer. Breast cancer was related to joint interactions between high perceived stress and alcohol intake of 11.0 g or more per day (AOR, 2.91; 95% CI, 1.23–6.86), smoking at least one cigarette per day (AOR, 2.52; 95% CI, 1.16–5.47), intake of less than 100 ml of green tea per day (AOR, 2.47; 95% CI, 1.40–4.38), physical activity of less than 1,000 kcal per week (AOR, 3.36; 95%
CI, 1.77–6.36), high fried and stir-fried food intake (AOR, 3.18;
95% CI, 1.79–5.63), and high meat and seafood intake (AOR, 1.89;
95% CI, 1.09–3.27). Perceived stress, when combined with poten- tially risky lifestyle behaviors, may be a contributing factor to breast cancer.
KEYWORDS breast cancer, perceived stress, lifestyle behavior, dietary habits
INTRODUCTION
Like other industrialized countries, the most frequent type of cancer among women in Taiwan is breast cancer. The occurrence of breast cancer has increased steadily in Taiwan in recent years. In 2007, the annual incidence rate of breast cancer was 75.02 per 100,000 women; the rate increased to 81.36 per 100,000 women in 2008 (Taiwan Health Bureau, 2011).
Factors causing breast cancer are many and complex. The circulating level of estrogen in women has been identified as a significant factor con- tributing to the occurrence of breast cancer (Bernstein & Ross, 1993; Toniolo et al., 1995; Persson, 2000). Research results regarding lifestyle factors in relation to the development of breast cancer have been inconsistent. Alcohol consumption (Zhang et al., 2007; Deandrea et al., 2008; Lew et al., 2009), tobacco smoking (Gram et al., 2005; Brown et al., 2010; Deroo et al., 2011), green tea consumption (Wu et al., 2003; Shrubsole et al., 2009; Iwasaki et al., 2010), physical activity (Lahmann et al., 2007; Howard et al., 2009; Smith et al., 2011), consumption of certain foods (Wang et al., 2008; Li et al., 2009; Trichopoulous et al., 2010), and increased weight (Meyskens et al., 2000; Verkasalo et al., 2001; McTiernan et al., 2006) are lifestyle factors that have been considered in relation to the risk of breast cancer. However, the existence and strength of the relationships of these factors to breast cancer
development have been inconsistent. Even though these studies found that certain factors are related to the development of breast cancer, the overall effects observed have been quite small. The lack of agreement in the role of these lifestyle factors affecting breast cancer warrants further study on the matter.
Previous studies have also illustrated a relationship between the risk of breast cancer and psychological stress (Helgesson et al., 2003; Kruk &
Aboul-Enein, 2004; Williams et al., 2009). Psychological stress may pro- mote carcinogens through estrogen synthesis and metabolism, as well as changes in the concentration of circulating estradiol (Gunin, 1996; Kam et al., 2000). Estradiol binds to estrogen receptors, activating gene expression and increasing cell proliferation (Pitot & Dragan, 2001). A woman with a lower concentration of estradiol may have a lower risk of breast cancer compared to a woman with a higher estradiol concentration (Cauley et al., 1999).
A prospective case-control study showed an association between stressful life events and breast cancer risk. In this study, more breast cancer patients consumed alcohol and smoked than did healthy controls, but the difference was not statistically significant (Ollonen, Lehtonen, & Eskelinen, 2005). One cohort and two case-control studies have also shown an asso- ciation of stress with a higher risk of breast cancer (Helgesson et al., 2003;
Lillberg et al., 2003; Kruk & Aboul-Enein, 2004). However, these studies only examined stress in relation to breast cancer risk; they did not analyze any further link between stress and other risk factors or whether the strength of the relationship of stress to breast cancer risk was affected by other factors.
While stress and lifestyle may be associated with breast cancer, few studies have explored the interaction between stress and lifestyle in relation to breast cancer risk. Researchers in the current study designed a hospital- based, case-control study to assess the relationship between perceived stress and lifestyle, and the potential interaction of these on the odds of breast can- cer among women. They hypothesized that perceived stress would increase the odds of breast cancer and that joint effects of perceived stress and spe- cific lifestyle factors might increase the odds of breast cancer among women in Taiwan.
METHODS Study Population
This hospital-based, matched-pair, case-control study was carried out in Chung-Shan Medical University Hospital, a medical center and teaching hos- pital in central Taiwan. The period of study was from June 2009 to June 2011. A total of 471 participants were involved in the research with two participants in the control group matched on age to each participant in the breast cancer case study group.
Patients in the case study group were diagnosed by physicians of the breast surgical department, with histological confirmation of carcinoma in the breast tissue of all case study participants. These new breast cancer patients were about 2% of all patients seen in the breast surgical depart- ment during the period of the investigation. Of the 162 new cases (new cases were defined as cases diagnosed within one month of the study), 5 patients refused to be interviewed, and 157 patients (96.31%) took part in this study. Three hundred fourteen controls were recruited from outpa- tients seen in the family medicine and physical check-up departments. Two controls were matched to each case study on age (± 2 years). Matched par- ticipants were interviewed during the same time period (within one month) as the cases. Participants in the control group were screened by physicians of the family medicine and physical examination center; no control partici- pants had cancer, a previous history of cancer, a previous case of a benign tumor, or a reproductive system disease. Generally speaking, participants in the control group tended to suffer from colds, gastric problems, diabetes, hypertension, coronary disease, liver disease, and nephritis, or they had come to the hospital for a general health check-up. These controls com- prised about 4% of all patients visiting the outpatient family medicine and physical check-up departments. Of the 334 participants selected to be in the control group, 20 women did not agree to be interviewed, and 314 women (95.93%) participated in the control group.
Data Collection
All participants resided in central Taiwan and were personally interviewed face-to-face by an interviewer using a structured questionnaire that collected information about lifestyle and stress. Interviewers were not masked as to which group each interviewee belonged. Participants were asked about their daily routines and stress levels prior to any illnesses. Before interviewing the cases, interviewers would tell respondents to answer all questionnaire questions, including lifestyle and perceived stress, retrospectively—that is how they felt in the past. If the information given by the respondents was incomplete, the questionnaire was excluded from the study. All respondents were clear-minded without any mental impairment.
The study protocol was approved by the ethics committee of Chung- Shan Medical University Hospital. All participants gave their written and signed informed consent.
Instruments
The structured questionnaire was designed to collect personal informa- tion from respondents, including demographic and breast cancer-relevant
characteristics, perceived stress level, individual behavior, and dietary habits.
Demographic and breast cancer-relevant characteristics included educational level, marital status, self-reported weight and height to calculate body mass index (BMI), age at menarche, age at menopause, family history of breast cancer, and previous use of menopausal hormone therapy. BMI was cal- culated as weight (kg) per height squared (m2). BMI was categorized into normal/underweight, <25 kg/m2; overweight and obese, ≥25 kg/m2 (National Heart Blood Lung Institute, 1998).
PERCEIVED STRESS LEVEL
The survey on perceived stress consisted of 14 questions from the perceived stress scale (PSS) that measured one’s perception of stress related to one’s daily life (Cohen, Kamarck, & Mermelstein, 1983). The Chinese version of PSS had a test-retest reliability (r = 0.76 over a 4-week interval). The construct validity was assessed by factor analysis. Two factors, life being uncontrol- lable and life being unpredictable and overloaded, were assessed. The total variance accounted for by these two factors was 49.5% (Chen, 1993). The PSS asked respondents to evaluate their lives for stress levels during the preced- ing month. The PSS items were designed to provide a way for respondents to express how unpredictable, uncontrollable, and overloaded they felt that their lives were. The measure was sensitive to the nonoccurrence of events and ongoing life circumstances, not for a particular situation. On the PSS, a 5-level Likert scale was used to measure perceived stress levels (0= Never;
4= Very often). The total possible range of scores was from 0 to 56. Higher scores indicated higher levels of stress. In this study, the range of PSS scores among participants was assessed as above (high stress) or below (low stress) the median score. The median score of 23 was the cut-off value.
ALCOHOL CONSUMPTION, HABITUAL SMOKING, GREEN TEACONSUMPTION,
AND PHYSICALACTIVITY
To assure content validity in the questionnaire section on alcohol consump- tion, habitual smoking, green tea consumption, and physical activity, the questionnaires were reviewed by three experts in the fields of epidemiology, nutrition, and health education. The content validity (correlation coefficient) was 0.90 and the test-retest reliability was 0.93 in this section. Alcohol con- sumption was measured as average alcohol consumption (times per day or week) and amount of alcohol ingested (dependent upon the type of bever- age). Total alcohol intake was 11.0 g of ethanol for 120 ml of wine, 14.0 g for 45 ml of liquor, 12.8 g for 360 ml of regular beer, or 11.3 g for 360 ml of light beer (Zhang et al., 2007). Alcohol consumption was categorized as “no”
if a participant’s average ingested alcohol amount was less than the above
criterion every day and “yes” otherwise. Habitual smoking was measured as number of cigarettes smoked per day and intensity of inhalation. Habitual smoking was categorized as “no” if it was less than once daily on average and “yes” otherwise. Green tea intake was categorized as “no” if it was less than one cup per day on average and “yes” otherwise. The volume of a cup of green tea was assumed to be 100 ml (Kuriyama et al., 2006). Physical activity was measured by calculating a given activity’s metabolic equivalent by multiplying the number of physical activities each week with the duration of the activity and the person’s weight (Ainsworth et al., 2000). In this study, a physically active individual was defined as one who had physical energy consumption of more than 1,000 kcal/week.
DIETARY HABITS
To assure content validity for food intake, the questionnaires were reviewed by three experts in the fields of epidemiology, nutrition, and health educa- tion. The content validity (correlation coefficient) was 0.89 and the test-retest reliability was 0.92. The food-frequency questionnaire estimated the fre- quency of an individual person’s normal intake of food. The food items included 18 different types of food: rice, pasta, cake, poultry, red meat, processed meat (sausage/bacon), fried meat, stir-fried meat, fish, fried fish, stir-fried fish, seafood (shrimp/clams/oysters), eggs, soybean products, dairy products, green/leafy vegetables, dark yellow vegetables, and fruits. The response consisted of food items in 5 frequency of consumption categories, which were separated as never, seldom (2–3 times/month), occasionally (1–2 times/week), usually (4–6 times/week), and always (at least one time/day). The responses were scored from 0 (never) to 4 (always). Factor analysis was used to analyze the frequencies of food intake for these food items. Researchers used an orthogonal rotation to identify dietary factor groupings using eigen values, the scree plot, and interpretability.
Factor loadings above 0.6 were considered to be the factors. With 61.06%
of variance explained, three food categories were formed: fried/stir-fried foods, meat/seafood, and vegetables/fruits. The fried/stir-fried foods group included the following foods and factor loadings: stir-fried fish, 0.88; fried fish, 0.83; stir-fried meat, 0.80; and fried meat, 0.78. The meat/seafood group included foods and factor loadings as follows: poultry, 0.85; red meat, 0.84;
seafood (shrimp/clams/oysters), 0.67; and fish, 0.60. The vegetables/fruits group included the following foods with these factor loadings: green/leafy vegetables, 0.91; dark yellow vegetables, 0.90; and fruits, 0.71. By summing the frequency of consumption scores for each food in each food category weighted by its factor loading, researchers were able to calculate food group scores. They distributed participant food scores for each food category into percentiles. Using the 50th percentile (median) of the distribution as a cut- off point, they separated frequency of intake into low and high intake. The
fried/stir-fried foods and meat/seafood groups thus each contained four food items, and the total possible sum of scores for each of these two food groups was 16. Three food items were in the vegetables/fruits group, which pro- duced a total possible summed score of 12. The median cut-off scores and ranges for each of these three food groups were fried/stir-fried foods, median
= 3.44 and range = 0–11.45; meat/seafood, median = 6.27 and range = 0–11.17; and vegetables/fruits, median = 9.00 and range = 2.52–10.08.
Statistical Analysis
Data were analyzed using SPSS17.0 (Chicago, IL, USA). Univariate logistic regressions were used to test the association of breast cancer and demo- graphics with relevant characteristics comparing cases and controls. Crude and adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were cal- culated for each variable. Variable(s) significantly differing between cases and controls were considered to be confounding factor(s), using statistical significance as p < 0.10. The main effect in conditional multiple logistic regression analysis was used to examine the differences of perceived stress and lifestyle factors between breast cancer cases and controls, considering statistical significance to be p< 0.05. Spearman correlation coefficients were used to assess the relation of perceived stress and each lifestyle variable. After identification of the main effects in the logistic regression models, two-way interaction factors (perceived stress and lifestyle factors) were tested with multiple logistic regression models. Variables eligible for inclusion in the models included those with variable(s) significant at p < 0.10 in Spearman correlations between perceived stress and each lifestyle factor and demo- graphic characteristics. The final models were checked for goodness of fit with the Hosmer and Lemeshow test to ensure the models fit the data well.
RESULTS Characteristics of Participants
The mean age of participants was 54.67± 10.95 years, and ages ranged from 32 to 76 years. Due to matching, the age distributions were very similar for cases and controls (Table 1). No significant differences between breast cancer cases and controls were observed in education level, marital status, BMI, late menopause, family history of breast cancer in first degree relatives, or use of hormone therapy. However, the OR for education level ≤ 9 years (OR
= 1.40; 95% CI, 0.95–2.06), menarche before age 12 years (OR = 1.84; 95%
CI, 1.21–2.81), and past hormone therapy for ≥ 3 months (OR = 1.59; 95%
CI, 0.97–2.61) were increased and were retained in the main effect model and interaction model as confounding variables per the selection criterion (p< 0.10).
TABLE 1 Unadjusted OR and 95% CI for Demographic and Breast Cancer-Relevant Characteristics in Breast Cancer Patients as Compared with Control Participants
Cases Controls Total
Characteristics (n= 157) (n = 314) (n = 471) OR (95% CI) Education level≤ 9 years; n (%) 91 (58.0) 156 (49.7) 247 (52.4) 1.40 (0.95–2.06) Married/live together vs. single; n (%) 117 (74.5) 236 (75.2) 353 (74.9) 0.97 (0.62–1.50) BMI≥ 25/overweight & obese vs.
normal weight; n (%)
45 (28.7) 73 (23.2) 118 (25.1) 1.33 (0.86–2.05) Menarche before age 12 years; n (%) 34 (21.7) 41 (13.1) 75 (15.9) 1.84 (1.11–3.04) Age at menopause≥ 55 years; n (%) 16 (10.2) 38 (12.1) 54 (11.5) 0.82 (0.49–1.68) First-degree family history of breast
cancer; n (%)
13 (8.3) 23 (7.3) 36 (7.6) 1.14 (0.56–2.32) Past hormone therapy for≥
3 months; n (%)
33 (21.0) 45 (14.3) 78 (16.6) 1.59 (0.97–2.61)
Main Effects of Perceived Stress and Risk Factors in Breast Cancer Patients Compared with Controls
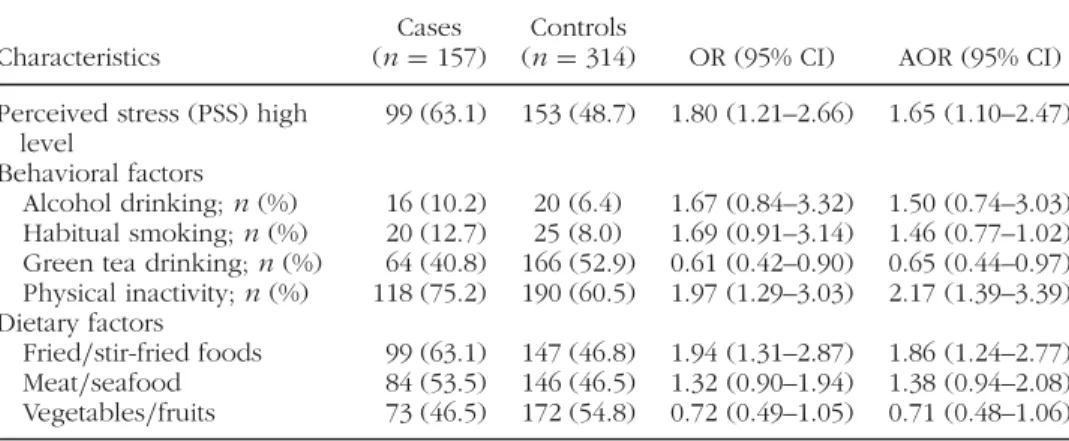
Fifty-four percent (n = 252) of the population reported high levels of perceived stress. High level of perceived stress was significantly positively associated with risk of breast cancer (Table 2). The AOR for high perceived stress, adjusted for education level, age at menarche, and past hormone therapy was 1.65 (95% CI, 1.10–2.47) and for being less physically active (<1,000 kcal/week) was 2.17 (95% CI, 1.39–3.39). Among the dietary fac- tors, consumption of fried/stir-fried foods was associated with a significantly increased odds of breast cancer (AOR= 1.86; 95% CI, 1.24–2.77). No asso- ciation was found between breast cancer and any of the following: alcohol consumption, habitual smoking, green tea consumption, or consumption of meat/seafood or vegetables/fruits.
TABLE 2 Unadjusted OR and AOR and 95% CI for Perceived Stress and Behavioral and Dietary Risk Factors in Breast Cancer Patients Compared with Control Participants
Cases Controls
Characteristics (n= 157) (n = 314) OR (95% CI) AOR (95% CI) Perceived stress (PSS) high
level
99 (63.1) 153 (48.7) 1.80 (1.21–2.66) 1.65 (1.10–2.47) Behavioral factors
Alcohol drinking; n (%) 16 (10.2) 20 (6.4) 1.67 (0.84–3.32) 1.50 (0.74–3.03) Habitual smoking; n (%) 20 (12.7) 25 (8.0) 1.69 (0.91–3.14) 1.46 (0.77–1.02) Green tea drinking; n (%) 64 (40.8) 166 (52.9) 0.61 (0.42–0.90) 0.65 (0.44–0.97) Physical inactivity; n (%) 118 (75.2) 190 (60.5) 1.97 (1.29–3.03) 2.17 (1.39–3.39) Dietary factors
Fried/stir-fried foods 99 (63.1) 147 (46.8) 1.94 (1.31–2.87) 1.86 (1.24–2.77) Meat/seafood 84 (53.5) 146 (46.5) 1.32 (0.90–1.94) 1.38 (0.94–2.08) Vegetables/fruits 73 (46.5) 172 (54.8) 0.72 (0.49–1.05) 0.71 (0.48–1.06)
Correlation Coefficients for Perceived Stress and Each Risk Factor Perceived stress was positively correlated with alcohol consumption (r = 0.092, p = 0.046), habitual smoking (r = 0.109, p = 0.017), physical inactivity (r = 0.118, p = 0.010), fried/stir-fried food (r = 0.114, p = 0.013) and meat/seafood (r = 0.091, p = 0.048), and inversely correlated with green tea consumption (r = –0.103, p = 0.026), and vegetables/fruits (r = –0.093, p = 0.044). Alcohol drinking was correlated with habitual smoking (r = 0.131, p = 0.004) and fried/stir-fried food (r = 0.133, p
= 0.004). Habitual smoking was correlated with fried/stir-fried food (r = 0.161, p < 0.001) and meat/seafood (r = 0.119, p = 0.010). Physical inac- tivity was correlated with fried/stir-fried foods (r = 0.099, p = 0.033) and meat/seafood (r = 0.127, p = 0.006) and inversely correlated with green tea (r = –0.194, p < 0.001) (Table 3). In this study, all variables were not collinear.
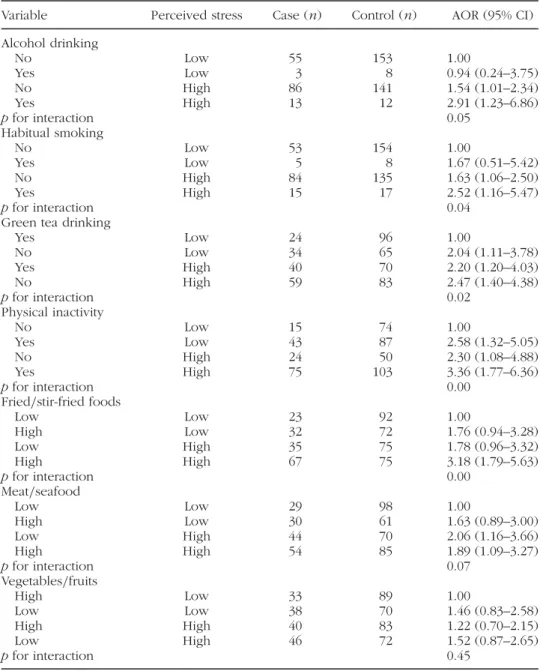
Interaction Effects of Breast Cancer Associated with Risk Factors and Perceived Stress
The ORs for the interactions of perceived stress and lifestyle factors were adjusted for menarche before age 12 years in the multiple logistic regres- sion models (Table 4). Compared to those with low perceived stress who abstained from excessive alcohol consumption, those with high perceived stress and high amounts of alcohol intake had higher odds of breast cancer (AOR, 2.91; 95% CI, 1.23–6.86). An interaction was also observed between stress and smoking behavior, with those having high perceived stress and habitual smoking habits having higher odds of breast cancer (AOR, 2.52;
95% CI, 1.16–5.47). Stress and green tea intake also showed an interaction:
Those with low green tea intake and high levels of perceived stress had a higher odds of breast cancer (AOR, 2.47; 95% CI, 1.40–4.38). Another interaction, one for stress and physical activity, was observed such that those who were less active physically and reported higher levels of per- ceived stress had a higher odds of breast cancer (AOR, 3.36; 95% CI, 1.77–6.36) than those who were more physically active and reported lower levels of perceived stress. Finally, stress and food showed an interaction:
Those who ate large amounts of fried or stir-fried food and reported high levels of stress had higher odds of breast cancer (AOR, 3.18; 95% CI, 1.79–5.63) than those with low stress and low fried food intake, as did those who reported high stress and ingested high amounts of meat and seafood (AOR, 1.89; 95% CI, 1.09–3.27) compared to those who reported low stress and lower intake of meat and seafood. Model fit of the data in each model was not significant (p> 0.05); therefore, the null hypothesis was not rejected.
TABLE3CorrelationCoefficientsforPerceivedStressandBehavioralandDietaryRiskFactors(n=471) Perceived stressAlcohol drinkingHabitual smokingGreentea drinkingPhysical inactivityFried/stir-fried foodsMeat/ seafoodVegetables fruits Perceivedstress1 Alcoholdrinking.092∗1 Habitualsmoking.109∗.131†1 Greenteadrinking−.103∗−.084−.0491 Physicalinactivity.118∗.009.049−.194‡1 Fried/stir-friedfoods.114∗.133†.161‡−0.86.099∗1 Meat/seafood.091∗.047.119∗−.011.127†.0561 Vegetables/fruits−.093∗−.007−.051.049−.066−.084−.0501 ∗p<.05,†p<.01,‡p<.001.
29
TABLE 4 Interaction Effects of Breast Cancer Associated with Risk Factors and Perceived Stress
Variable Perceived stress Case (n) Control (n) AOR (95% CI) Alcohol drinking
No Low 55 153 1.00
Yes Low 3 8 0.94 (0.24–3.75)
No High 86 141 1.54 (1.01–2.34)
Yes High 13 12 2.91 (1.23–6.86)
p for interaction 0.05
Habitual smoking
No Low 53 154 1.00
Yes Low 5 8 1.67 (0.51–5.42)
No High 84 135 1.63 (1.06–2.50)
Yes High 15 17 2.52 (1.16–5.47)
p for interaction 0.04
Green tea drinking
Yes Low 24 96 1.00
No Low 34 65 2.04 (1.11–3.78)
Yes High 40 70 2.20 (1.20–4.03)
No High 59 83 2.47 (1.40–4.38)
p for interaction 0.02
Physical inactivity
No Low 15 74 1.00
Yes Low 43 87 2.58 (1.32–5.05)
No High 24 50 2.30 (1.08–4.88)
Yes High 75 103 3.36 (1.77–6.36)
p for interaction 0.00
Fried/stir-fried foods
Low Low 23 92 1.00
High Low 32 72 1.76 (0.94–3.28)
Low High 35 75 1.78 (0.96–3.32)
High High 67 75 3.18 (1.79–5.63)
p for interaction 0.00
Meat/seafood
Low Low 29 98 1.00
High Low 30 61 1.63 (0.89–3.00)
Low High 44 70 2.06 (1.16–3.66)
High High 54 85 1.89 (1.09–3.27)
p for interaction 0.07
Vegetables/fruits
High Low 33 89 1.00
Low Low 38 70 1.46 (0.83–2.58)
High High 40 83 1.22 (0.70–2.15)
Low High 46 72 1.52 (0.87–2.65)
p for interaction 0.45
DISCUSSION
This study explored the relationships of lifestyle behaviors and the percep- tion of stress in women with breast cancer compared to women without breast cancer. Researchers found that women who reported high levels of
perceived stress had increased odds of breast cancer. These findings are con- sistent with previous epidemiological studies (Helgesson et al., 2003; Lillberg et al., 2003; Kruk & Aboul-Enein, 2004). They also found that low physical activity and high fried/stir-fried foods intake were associated with signifi- cantly increased odds of breast cancer. Moreover, the combination of higher perceived stress and most lifestyle factors examined (e.g., alcohol, habitual smoking, physical activity, and high fried/stir-fried food consumption) was associated with elevated odds of breast cancer in the Taiwanese women in this study. Previous studies have indicated that persons with high stress levels were more likely to smoke (Rod et al., 2009), drink alcohol (Mulia et al., 2008), engage in less physical activity (Jönsson et al., 2003), lead a sedentary lifestyle (Rod et al., 2009), and have a higher intake of high fat food and sugar than those who report less stress (Habhab, Sheldon, &
Loeb, 2009). Unhealthy behaviors coupled with stress-related processes may affect pathways implicated in cancer progression, including immunoregu- lation, angiogenesis, and invasion (Chida et al., 2008; Lutgendorf, Sood,
& Antoni, 2010). A previous study related social isolation to up-regulated mammary gland expression of murine orthologues of several key metabolic genes implicated in human tumor genesis and increased tumor growth in a murine breast cancer model (Williams et al., 2009). In the current study, researchers found that stress was associated with unhealthy behaviors, and together these behaviors and high perceived stress had increased odds of breast cancer.
The mechanism of stress as related to increased risk of breast can- cer is complex and not completely understood. When the human body endures stress or stressful events, the production of the stress hormone cor- tisol may be enhanced. This stress hormone can influence the signals of the hypothalamic-pituitary-adrenal (HPA) axis which in turn can inhibit the func- tion of the hypothalamic-pituitary-gonadal axis by decreasing the synthesis of estrogen (Young & Altemus, 2004; Horst et al., 2011). Although results in some studies have differed in whether stress correlated with increased can- cer risk (Schernhammer et al., 2004; Nielsen et al., 2005), these differences may have been due to different methods of measuring stress. Stress was associated in these studies with dysregulation or alterations in various neu- roendocrine hormones, particularly cortisol and catecholamines, which may be associated with an increased risk of breast cancer, whether by stimulating cell proliferation, increasing levels of oxidative stress, or workings by some other mechanism (Lutgendorf et al., 2010).
In the present study, researchers found that alcohol consumption alone was not associated with increased odds of breast cancer. This may be due to the fact that most women do not usually drink in Taiwan so that there may have been inadequate statistical power to detect a meaningful association of alcohol with breast cancer as statistically significant, particularly because the magnitude of the associations that some studies have found have been
fairly small (Li et al., 2006; Allen et al., 2009; Chen et al., 2011). Nevertheless, current researchers found that high levels of stress in women, combined with drinking alcohol, were associated with an increased odds of breast cancer. Previous studies have demonstrated that moderate consumption of alcohol was associated with an increased odds of breast cancer (Zhang et al., 2007), due to alcohol increasing estrogen levels in the blood. Alcohol could increase the concentration of estrogen (Deandrea et al., 2008; Lew et al., 2009); estrogen might in turn have a carcinogenic effect on breast tissue through estrogen receptors or a direct effect (Suzuki et al., 2005; Seitz et al., 2012). Women with high levels of stress may already have high levels of estrogen existing in their bodies (Figueiredo, Dolgas, & Herman, 2002). Thus, the excess of endogenous estrogen from alcohol could increase a women’s probability of contracting breast cancer over women who have lower stress or who are stress-free.
Tobacco contains carcinogens, such as polycyclic aromatic hydrocar- bons, that are transported into mammary tissues through blood plasma lipoproteins (Rundle et al., 2000), thereby potentially increasing the risk of breast cancer in mammary epithelial cells (Zhang et al., 2011; Keller et al., 2012). Cigarette smoke may also increase breast cancer risk by raising levels of oxidative DNA damage, although a number of studies (Lin et al., 2008;
Ahern et al., 2009) have found no association of smoking with breast cancer risk. In this study, researchers found no significant correlation between habit- ual smoking and breast cancer. This result might be due to the small number of smokers in the study, which reduced the statistical power to detect a meaningful association as statistically significant. However, the results were similar to those of some previous studies (Brown et al., 2010; Deroo et al., 2011). The current researchers found that higher levels of perceived stress in women who smoked was associated with an increased odds of breast cancer. Generally speaking, people who smoke have higher levels of stress in their daily lives (Rod et al., 2009; Childs & De Wit, 2010). Those who are habitual smokers with high levels of stress could increase their potential for developing breast cancer.
In Taiwan, green tea intake is nearly equivalent to coffee intake in the West, particularly at social functions. Green tea contains polyphenols, which are strong antioxidants that help to inhibit the formation of tumors (Chen & Dou, 2008). In previous epidemiological studies, findings have been inconsistent regarding the relationship between green tea and odds of breast cancer (Wu et al., 2003; Shrubsole et al., 2009; Iwasaki et al., 2010). In this study, researchers found that green tea consumption had no association with breast cancer. However, they found that the joint effects of higher perceived stress without drinking green tea were associated with a higher odds of breast cancer. Green tea intake has been associated with lower psychologi- cal stress (Hozawa et al., 2009), because green tea contains L-theanine and ascorbic acid, which can reduce the heart rate, blood pressure, and cortisol
levels as well as attenuate stress (Brody et al., 2002; Kimura et al., 2007).
Green tea consumption may help individuals to cope with stressful events in everyday life.
In this study, researchers found increased physical activity was associ- ated with a reduced odds breast cancer. This finding is similar to the results of some previous studies (Lahmann et al., 2007; Leitzmann et al., 2008). Physical activity may reduce the odds of breast cancer by its effect on weight and estrone among postmenopausal women (Neilson et al., 2009) that depends on the type, dose, and timing of the activity among lean, normal, and over- weight women (Friedenreich, 2010), but the literature is inconsistent in the findings with some studies showing no protective effect (Gammon et al., 1998; Smith et al., 2011). Premenopausal and postmenopausal women differ in the relation of developing breast cancer to physical activity. For example, one 20-year prospective investigation indicated that total physical activity was not associated with estrogen and progesterone receptor-positive and breast cancer but suggested that moderate physical activity might reduce the risk of postmenopausal breast cancer risk (Eliassen et al., 2010). Usually, women with higher stress levels have lower amounts of physical activity (Jönsson et al., 2003), which could increase the odds of breast cancer. Physical activity may reduce the accumulation of ovarian estrogen and increases energy con- sumption, thereby reducing obesity and lipids, which can delay menarche but enhance menstrual cycle changes, augmenting the binding of the sex hormones and enhancing immune function (McTiernan et al., 2006). One previous study identified daily physical activity as being associated with a lower risk of psychological distress (Hamer, Stamatakis, & Steptoe, 2009).
Compared with less physical activity, higher amounts of physical activity tended to decrease serum sex hormone concentrations (Monninkhof et al., 2009; Van Gils et al., 2009) and increase sex hormone binding globulin con- centrations (Friedenreich et al., 2010), which should be associated with a decrease breast cancer risk. However, under stress women who engaged in less physical activity (Jönsson et al., 2003) would have higher levels of estrone, estradiol, and free estradiol, and lower levels of sex hormone- binding globulin (McTiernan et al., 2006), potentially increasing the odds of breast cancer.
Researchers found that high intake of fried and stir-fried foods was associated with an increased odds of breast cancer. Foods cooked at high temperatures, such as those that are fried or stir-fried, produce carcinogens and heterocyclic amines, especially amino-1-methyl-6-phenylimidazo [4,5-b]
pyridine (PhIP) (Sinha et al., 2000). Increased PhIP intake had been cor- related with the increased risk of breast cancer in one study (Snyderwine, Venugopal, & Yu, 2002). Current researchers also found that the joint relation of perceived stress and high intake of fried and stir-fried foods was associ- ated with an increased odds of breast cancer. Although there is no direct evidence that people under stress ingest more fried and stir-fried foods,
Taiwanese dietary habits have been influenced by Western-style food, and fried and stir-fried foods have gradually become part of the Taiwanese diet.
Researchers also found that women who reported high perceived stress lev- els and high meat and seafood intake had increased odds of breast cancer.
It is possible that monounsaturated trans fats may drive the associations between different types of fat and breast cancer (Wang et al., 2008). Obesity and uneven energy intake could affect the secretion and balance of estrogen and thus potentially explain the increased odds of breast cancer (Meyskens et al., 2000; McTiernan et al., 2006). Women with high stress are also often obese (Vicennati et al., 2009). In the current study, researchers did not find a correlation between high perceived stress levels and high vegetable and fruit intake or an increase in the odds of breast cancer. High stress levels have been negatively associated with vegetable and fruit intake (Roohafza et al., 2007). Vegetables and fruits contain antioxidant vitamins, fiber, and folic acid, all of which can help to enhance immune response, inhibit tumor cell proliferation, and reduce DNA oxidative damage to cells (Rock, Lampe,
& Patterson, 2000; Li et al., 2009). However, they did not identify any rela- tionship of breast cancer to vegetable and fruit intake in conjunction with high perceived stress.
A number of individual studies have described specific risk factors acting together to produce an increase or decrease in the risk of breast cancer that is greater than a single risk factor acting alone (Suzuki et al., 2005; Li et al., 2009; Sánchez-Zamorano et al., 2011). Few of these interactions have led to more than a moderate change in risk. The current study has established the interactions between multiple lifestyle risk factors and perceived stress in relation to breast cancer.
However, the current study had a number of limitations that must be considered when interpreting the results. First, the main limitation was the potential for recall bias. Patients with breast cancer may have differentially recalled lifestyle behaviors compared to controls and may have been influ- enced by their disease when reporting perceived stress in the interviews.
If breast cancer patients objectively recalled their perceived stress prior to their breast cancer diagnosis, then the bias in this group on this variable would be similar to the bias in the control group on this variable so that no differential misclassification would occur. Interviewers in this study encour- aged respondents to remember the exposure to risk factors and stress prior to their illness (for cases) to decrease recall bias, but they cannot be certain that respondents’ illness did not influence responses in the cases. A sec- ond limitation was that although they had criteria for recruiting cases and controls into this study, the lack of use of a standard instrument to screen the participants for eligibility was a limitation which could have resulted in erroneously including or excluding eligible participants. Third, the lack of inclusion of factors that have been associated with breast cancer in the literature might have resulted residual uncontrolled confounding for such
factors as marital status (Kruk & Aboul-Enein, 2004), BMI (McTiernan et al., 2006), age at menopause (Chavez-MacGregor et al., 2005), and family history (Nemesure et al., 2009). Fourth, participants in the case and control groups were from a single Taiwanese medical center, which was not designed to serve a specific group but rather had very similar patient population to other Taiwanese hospitals, thus potentially enhancing the representativeness of the study groups. Taiwanese residents visiting this hospital were not from one specific background (i.e., they came from the general population, not from any one specific group). Because most of participants came from Taichung neighborhood attending a single hospital, local dietary traditions, religious practices, or even genetics of isolated, relatively non-mobile populations could have affected the results such that they would not be representative of women in other Taiwanese areas. Fifth, selection and participation biases may have played a role in this hospital-based study, which included clinic- based participants and thus might not be representative of all women in Taiwan. Finally, participants may have exhibited social acceptability biases when responding to certain questions on the survey (particularly, drinking and smoking habits). However, it was unlikely that the breast cancer patients differed in this regard compared to the controls.
Using the OR to compare breast cancer cases to controls, the 58% preva- lence of high stress (Nielsen et al., 2005), the 2:1 ratio of cases to controls (Helgesson et al., 2003), with a two-sided alpha= 0.05, and power of 80%, researchers calculated sample size and found they needed 115 participants in the case group and 230 in the control group. They collected more than these required sample sizes in both case and control groups in anticipation of insufficient expected frequencies in some of the cells for interaction. They did not explore frequencies of lifestyle and perceived stress owing to the restricted sample size. For future studies, examination of dose-response as related to lifestyle and perceived stress would be beneficial.
The study also included a degree of subjectivity regarding lifestyle mea- surements. Defining the cut-off point of dichotomous groups was somewhat arbitrary, but the study emphasis was on the comparison of groups that were either “high” or “low” with respect to a certain characteristic, not by strictly defining the groups themselves. On the other hand, lifestyle factors may act synergistically and be reinforced by stress, thereby enhancing the odds of breast cancer. To help prevent breast cancer, it would be beneficial to incorporate stress management in high-risk populations to help offset other risk factors.
REFERENCES
Ahern, T. P., T. L. Lash, K. M. Egan, and J. A. Baron. 2009. Lifetime tobacco smoke exposure and breast cancer incidence. Cancer Cause Control 20:1837–44.
Ainsworth, B. E., W. L. Haskell, M. C. Whitt, M. L. Irwin, A. M. Swartz, S. J. Strath, et al. 2000. Compendium of physical activities: An update of activity codes and MET intensities. Med Sci Sports Exerc 32:S498–504.
Allen, N. E., V. Beral, D. Casabonne, S. W. Kan, G. K. Reeves, A. Brown, and J.
Green. 2009. Moderate alcohol intake and cancer incidence in women. J Natl Cancer Inst 101:296–305.
Bernstein, L., and R. K. Ross. 1993. Endogenous hormones and breast cancer risk.
Epidemiol Rev 15:48–65.
Brody, S., R. Preut, K. Schommer, and T. H. Schürmeyer. 2002. A randomized controlled trial of high dose ascorbic acid for reduction of blood pressure, cortisol, and subjective responses to psychological stress. Psychopharmacology 159:319–24.
Brown, L. M., G. Gridley, A. H. Wu, R. T. Falk, M. Hauptmann, L. N. Kolonel, et al.
2010. Low level alcohol intake, cigarette smoking and risk of breast cancer in Asian-American women. Breast Cancer Res Treat 120:203–10.
Cauley, J. A., F. L. Lucas, L. H. Kuller, K. Stone, W. Browner, and S. R. Cummings.
1999. Elevated serum estradiol and testosterone concentrations are associated with a high risk for breast cancer. Study of Osteoporotic Fractures Research Group. Ann Intern Med 130:270–7.
Chavez-MacGregor, M., S. G. Elias, N. C. Onland-Moret, Y. T. van der Schouw, C. H. Van Gils, E. Monninkhof, et al. 2005. Postmenopausal breast cancer risk and cumulative number of menstrual cycles. Cancer Epidemiol Biomarkers Prev 14:799–804.
Chen, C. H. 1993. Effects of home visits and telephone contacts on breastfeeding compliance in Taiwan. Matern Child Nurs J 21:82–90.
Chen, D., and Q. P. Dou. 2008. Tea polyphenols and their roles in cancer prevention and chemotherapy. Int J Mol Sci 9:1196–206.
Chen, W. Y., B. Rosner, S. E. Hankinson, G. A. Colditz, and W. C. Willett. 2011.
Moderate alcohol consumption during adult life, drinking patterns, and breast cancer risk. J Am Med Assoc 306:1884–90.
Chida, Y., M. Hamer, J. Wardle, and A. Steptoe. 2008. Do stress-related psychoso- cial factors contribute to cancer incidence and survival? Nat Clin Pract Oncol 5:466–75.
Childs, E., and H. de Wit. 2010. Effects of acute psychosocial stress on cigarette craving and smoking. Nicotine Tob Res 12:449–53.
Cohen, S., T. Kamarck, and R. Mermelstein. 1983. A global measure of perceived stress. J Health Soc Behav 24:385–96.
Deandrea, S., R. Talamini, R. Foschi, M. Montella, L. D. Maso, F. Falcini, et al.
2008. Alcohol and breast cancer risk defined by estrogen and progesterone receptor status: A case-control study. Cancer Epidemiol Biomarkers Prev 17:
2025–8.
Deroo, L. A., P. Cummings, J. R. Daling, and B. Mueller. 2011. Smoking during first pregnancy and breast cancer: A case-control study using Washington state registry data. Ann Epidemiol 21:53–5.
Eliassen, A. H., S. E. Hankinson, B. Rosner, M. D. Holmes, and W. C. Willett. 2010.
Physical activity and risk of breast cancer among postmenopausal women. Arch Intern Med 170:1758–64.
Figueiredo, H. F., C. M. Dolgas, and J. P. Herman. 2002. Stress activation of cor- tex and hippocampus is modulated by sex and stage of estrus. Endocrinology 143:2534–40.
Friedenreich, C. M. 2010. The role of physical activity in breast cancer etiology.
Semin Oncol 37:297–302.
Friedenreich, C. M., C. G. Woolcott, A. McTiernan, R. Ballard-Barbash, R. F. Brant, F. Z. Stanczyk, et al. 2010. Alberta physical activity and breast cancer preven- tion trial: Sex hormone changes in a year-long exercise intervention among postmenopausal women. J Clin Oncol 28:1458–66.
Gammon, M. D., J. B. Schoenberg, J. A. Britton, J. L. Kelsey, R. J. Coates, D. Brogan, et al. 1998. Recreational physical activity and breast cancer risk among women under age 45 years. Am J Epidemiol 147:273–80.
Gram, I. T., T. Braaten, P. D. Terry, A. J. Sasco, H. O. Adami, E. Lund, and E.
Weiderpass. 2005. Breast cancer risk among women who start smoking as teenagers. Cancer Epidemiol Biomarkers Prev 14:61–6.
Gunin, A. G. 1996. Effect of chronic stress on estradiol action in the uterus of ovariectomized rats. Eur J Obstet Gynecol Reprod Biol 66:169–74.
Habhab, S., J. P. Sheldon, and R. C. Loeb. 2009. The relationship between stress, dietary restraint, and food preferences in women. Appetite 52:437–44.
Hamer, M., E. Stamatakis, and A. Steptoe. 2009. Dose-response relationship between physical activity and mental health: The Scottish Health Survey. Br J Sports Med 43:1111–4.
Helgesson, O., C. Cabrera, L. Lapidus, C. Bengtsson, and L. Lissner. 2003. Self- reported stress levels predict subsequent breast cancer in a cohort of Swedish women. Eur J Cancer Prev 12:377–81.
Horst, J. P., E. R. Kloet, H. Schachinger, and M. S. Oitzl. 2011. Relevance of stress and female sex hormones for emotion and cognition. Cell Mol Neurobiol 32(5):725–35. doi:10.1007/s10571-011-9774-2.
Howard, R. A., M. F. Leitzmann, M. S. Linet, and D. M. Freedman. 2009. Physical activity and breast cancer risk among pre- and postmenopausal women in the U.S. Radiologic Technologists cohort. Cancer Causes and Control 20:323–33.
Hozawa, A., S. Kuriyama, N. Nakaya, K. Ohmori-Matsuda, M. Kakizaki, T. Sone, et al. 2009. Green tea consumption is associated with lower psychological distress in a general population: The Ohsaki Cohort 2006 Study. Am J Clin Nutr 90:
1390–6.
Iwasaki, M., M. Inoue, S. Sasazuki, N. Sawada, T. Yamaji, T. Shimazu, W. Cwillett, and S. Tsugane. 2010. Green tea drinking and subsequent risk of breast cancer in a population to based cohort of Japanese women. Breast Cancer Res 12:R88.
Jönsson, D., S. Johansson, A. Rosengren, G. Lappas, and L. Wilhelmsen. 2003. Self- perceived psychological stress in relation to psychosocial factors and work in a random population sample of women. Stress & Health 19:149–62.
Kam, K., Y. Park, M. Cheon, G. H. Son, K. Kim, and K. Ryu. 2000. Effects of immobi- lization stress on estrogen-induced surges of luteinizing hormone and prolactin in ovariectomized rats. Endocrine 12:279–87.
Keller, P. J., L. M. Arendta, A. Skibinski, T. Logvinenko, I. Klebba, S. Dong, et al.
2012. Defining the cellular precursors to human breast cancer. P Natl Acad Sci USA 109:2772–7.
Kimura, K., M. Ozeki, L. R. Juneja, and H. Ohira. 2007. L-Theanine reduces psychological and physiological stress responses. Biol Psychol 74:39–45.
Kruk, J., and H. Y. Aboul-Enein. 2004. Psychological stress and the risk of breast cancer: A case-control study. Cancer Detect Prev 28:399–408.
Kuriyama, S., T. Shimazu, K. Ohmori, N. Kikuchi, N. Nakaya, Y. Nishino, et al. 2006.
Green tea consumption and mortality due to cardiovascular disease, cancer, and all causes in Japan: The Ohsaki study. JAMA 296:1255–65.
Lahmann, P. H., C. Friedenreich, A. J. Schuit, S. Salvini, N. E. Allen, T. J. Key, et al. 2007. Physical activity and breast cancer risk: The European prospec- tive investigation into cancer and nutrition. Cancer Epidemiol Biomarkers Prev 16:36–42.
Leitzmann, M. F., S. C. Moore, T. M. Peters, J. V. Lacey Jr., A. Schatzkin, C. Schairer, et al. 2008. Prospective study of physical activity and risk of postmenopausal breast cancer. Breast Cancer Res 10:R92.
Lew, J. Q., N. D. Freedman, M. F. Leitzmann, L. A. Brinton, R. N. Hoover, A. R.
Hollenbeck, et al. 2009. Alcohol and risk of breast cancer by histologic type and hormone receptor status in postmenopausal women: The NIH-AARP Diet and Health Study. Am J Epidemiol 170:308–17.
Li, Y., C. B. Ambrosone, M. J. McCullough, J. Ahn, V. L. Stevens, M. J. Thun, and C. C. Hong. 2009. Oxidative stress-related genotypes, fruit and vegetable consumption and breast cancer risk. Carcinogenesis 30:777–84.
Li, C. I., J. R. Daling, K. E. Malone, L. Bernstein, P. A. Marchbanks, J. M. Liff, et al. 2006. Relationship between established breast cancer risk factors and risk of seven different histologic types of invasive breast cancer. Cancer Epidemiol Biomarkers Prev 15:946–54.
Lillberg, K., P. K. Verkasalo, J. Kaprio, L. Teppo, H. Helenius, and M. Koskenvuo.
2003. Stressful life events and risk of breast cancer in 10,808 women: A cohort study. Am J Epidemiol 157:415–23.
Lin, Y., S. Kikuchi, K. Tamakosh, K. Wakai, T. Kondo, Y. Niwa, et al. 2008. Active smoking, passive smoking, and breast cancer risk: Findings from the Japan collaborative cohort study for evaluation of cancer risk. J Epidemiol 18:77–83.
Lutgendorf, K. S., A. K. Sood, and M. H. Antoni. 2010. Host factors and cancer progression: Biobehavioral signaling pathways and interventions. J Clin Oncol 28:4094–9.
McTiernan, A., L. Wu, C. Chen, R. Chlebowski, Y. Mossavar-Rahmani, F. Modugno, et al. 2006. Relation of BMI and physical activity to sex hormones in postmenopausal women. Obesity 14:1662–77.
Meyskens, F. L. Jr., W. F. Jungi, M. Gerber, F. de Waard, E. Heidemann, M. E. Heim, et al. 2000. WHO consensus conference on diet and cancer. Members of the breast cancer panel. Eur J Cancer Prev 9:213–6.
Monninkhof, E. M., M. J. Velthuis, P. H. M. Peeters, J. W. R. Twisk, and A. J. Schuit.
2009. Effect of exercise on postmenopausal sex hormone levels and role of body fat: A randomized controlled trial. J Clin Oncol 27:4492–9.
Mulia, N., L. Schmidt, J. Bond, L. Jacobs, and R. Korcha. 2008. Stress, social support and problem drinking among women in poverty. Addiction 103:1283–93.
National Heart Blood Lung Institute (NHLBI) Expert Panel on the Identification, Evaluation, and Treatment of Overweight, Obesity in Adults. 1998. Clinical
guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: The evidence report. Obes Res 6 (suppl2):51S–209S.
Neilson, H. K., C. M. Friedenreich, N. T. Brockton, and R. C. Millikan. 2009. Physical activity and postmenopausal breast cancer: Proposed biologic mechanisms and areas for future research. Cancer Epidemiol Biomarkers Prev 18:11–27.
Nemesure, B., S. Y. Wu, I. R. Hambleton, M. C. Leske, and A. J. Hennis. 2009. Risk factors for breast cancer in a black population: The Barbados National Cancer Study. Int J Cancer 124:174–9.
Nielsen, N. R., Z. F. Zhang, T. S. Kristensen, B. Netterstrom, P. Schnohr, and M.
Grønbaek. 2005. Self reported stress and risk of breast cancer: Prospective cohort study. BMJ 331:548. doi:10.1136/bmj.38547.638183.06.
Ollonen, P., J. Lehtonen, and M. Eskelinen. 2005. Stressful and adverse life expe- riences in patients with breast symptoms: A prospective case-control study in Kuopio, Finland. Anticancer Res 25:531–6.
Persson, I. 2000. Estrogens in the causation of breast, endometrial and ovarian can- cers: Evidence and hypotheses from epidemiological findings. J Steroid Biochem Mol Biol 74:357–64.
Pitot, H. III, and Y. Dragan, 2001. Chemical carcinogenesis. In Toxicology, the basic science of poisons, ed. C. D. Klaassen, 241–320. New York: McGraw-Hill.
Rock, C. L., J. W. Lampe, and R. E. Patterson. 2000. Nutrition, genetics, and risks of cancer. Annu Rev Public Health 21:47–64.
Rod, N. H., M. Gronbaek, P. Schnohr, E. Prescott, and T. S. Kristensen. 2009.
Perceived stress as a risk factor for changes in health behaviour and cardiac risk profile: A longitudinal study. J Intern Med 266:467–75.
Roohafza, H., M. Sadeghi, N. Sarraf-Zadegan, A. Baghaei, R. Kelishadi, M. Mahvash, et al. 2007. Relation between stress and other lifestyle factors. Stress & Health 23:23–9.
Rundle, A., D. Tang, H. Hibshoosh, A. Estabrook, F. Schnabel, W. Cao, et al.
2000. The relationship between genetic damage from polycyclic aromatic hydrocarbons in breast tissue and breast cancer. Carcinogenesis 21:1281–9.
Sánchez-Zamorano, L. M., L. Flores-Luna, A. Ángeles-Llerenas, I. Romieu, E. Lazcano- Ponce, H. Miranda-Hernández, et al. 2011. Healthy lifestyle on the risk of breast cancer. Cancer Epidemiol Biomarkers Prev 20:912–22.
Schernhammer, E. S., S. E. Hankinson, B. Rosner, C. H. Kroenke, W. C. Willett, G.
A. Colditz, and I. Kawachi. 2004. Job stress and breast cancer risk: The nurses’
health study. Am J Epidemiol 160:1079–86.
Seitz, H. K., C. Pelucchi, V. Bagnardi, and C. L. Vecchia. 2012. Epidemiology and pathophysiology of alcohol and breast cancer: Update 2012. Alcohol Alcoholism 47:204–12.
Shrubsole, M. J., W. Lu, Z. Chen, X. O. Shu, Y. Zheng, Q. Dai, et al. 2009. Drinking green tea modestly reduces breast cancer risk. J Nutr 139:310–6.
Sinha, R., D. R. Gustafson, M. Kulldorff, W. Q. Wen, J. R. Cerhan, and Z. Wei.
2000. 2-Amino-1-methyl-6-phenylimidazo [4,5-b] pyridine, a carcinogen in high temperature-cooked meat, and breast cancer risk. J Natl Cancer Inst 92:
1352–4.
Smith, A. J., W. R. Phipps, A. Y. Arikawa, M. O’Dougherty, B. Kaufman, W. Thomas, et al. 2011. Effects of aerobic exercise on premenopausal sex hormone levels:
Results of the WISER Study, a randomized clinical trial in healthy, sedentary, eumenorrheic women. Cancer Epidemiol Biomarkers Prev 20:1098–1106.
Snyderwine, E. G., M. Venugopal, and M. Yu. 2002. Mammary gland carcinogenesis by food-derived heterocyclic amines and studies on the mechanisms of carcinogenesis of 2-amino-1-methyl-6-phenylimidazo [4,5-b] pyridine PhIP.
Mutat Res 30:145–52.
Suzuki, R., W. Ye, T. Rylander-Rudqvist, S. Saji, G. A. Colditz, and A. Wolk.
2005. Alcohol and postmenopausal breast cancer risk defined by estrogen and progesterone receptor status: A prospective cohort study. J Natl Cancer Inst 97:1601–8.
Taiwan Health Bureau, Executive Yuan, R.O.C. 2011. Statistics on cancer incidence.
Retrieved December 25, 2011, from http://www.bhp.doh.gov.tw.
Toniolo, P. G., M. Levitz, A. Zeleniuch-Jacquotte, S. Banerjee, K. L. Koenig, R. E.
Shore, et al. 1995. A prospective study of endogenous estrogens and breast cancer in postmenopausal women. J Natl Cancer Inst 87:190–7.
Trichopoulou, A., C. Bamia, P. Lagiou, and D. Trichopoulos. 2010. Conformity to tra- ditional Mediterranean diet and breast cancer risk in the Greek EPIC European Prospective Investigation into Cancer and Nutrition cohort. Am J Clin Nutr 92:620–5.
Van Gils, C. H., P. H. M. Peeters, M. C. J. Schoenmakers, R. M. Nijmeijer, N. C. Onland-Moret, Y. T. van der Schouw, et al. 2009. Physical activity and endogenous sex hormone levels in postmenopausal women: A cross- sectional study in the Prospect-EPIC Cohort. Cancer Epidemiol Biomarkers Prev 18:377–83.
Verkasalo, P. K., H. V. Thomas, P. N. Appleby, G. K. Davey, and T. J. Key. 2001.
Circulating levels of sex hormones and their relation to risk factors for breast cancer: A cross-sectional study in 1,092 pre- and postmenopausal women (United Kingdom). Cancer Causes Control 12:47–59.
Vicennati, V., F. Pasqui, C. Cavazza, U. Pagotto, and R. Pasquali. 2009. Stress-related development of obesity and cortisol in women. Obesity 17:1678–83.
Wang, J., E. M. John, P. L. Horn-Ross, and S. A. Ingles. 2008. Dietary fat, cooking fat, and breast cancer risk in a multiethnic population. Nutr Cancer 60:492–504.
Williams, J. B., D. Pang, B. Delgado, M. Kocherginsky, M. Tretiakova, T. Krausz, et al. 2009. A model of gene-environment interaction reveals altered mammary gland gene expression and increased tumor growth following social isolation.
Cancer Prev Res 2:850–61.
Wu, A. H., M. C. Yu, C. C. Tseng, J. Hankin, and M. C. Pike. 2003. Green tea and risk of breast cancer in Asian Americans. Int J Cancer 106:574–9.
Young, E. A., and M. Altemus. 2004. Puberty, ovarian steroids, and stress. Ann N Y Acad Sci 1021:124–33.
Zhang, S. M., I. M. Lee, J. E. Manson, N. R. Cook, W. C. Willett, and J. E. Buring.
2007. Alcohol consumption and breast cancer risk in the Women’s Health Study.
Am J Epidemiol 165:667–76.
Zhang, H., F. Meng, G. Liu, B. Zhang, J. Zhu, F. Wu, et al. 2011. Transcription factor foxq1 promotes epithelial-mesenchymal transition and breast cancer metastasis.
Cancer Res 71:1292–301.