中 文 摘 要 : 高血壓為最重要的心血管危險因子,會造成心血管、腦血管、腎臟 病以及死亡。高血壓也會引起無症狀的器官傷害,包括腦部、心臟 、腎臟、以及血管系統。 亮點追蹤超音波可以用來測量心臟的形變,最近也被用來測量頸動 脈的血管應變。我們最近的研究發現頸動脈的血管環狀應變與應變 率可以由亮點追蹤超音波測得。而頸動脈的血管環狀應變與應變率 比起傳統的動脈硬度參數,更準確地與腦中風有相關。我們認為頸 動脈的血管環狀應變與應變率是很好用來評估高血壓對血管影響的 參數,而且也應具有對高血壓併發症預後的預測價值。 這個四年期的研究計畫想要利用頸動脈的血管環狀應變與應變率來 研究高血壓病人。第一年雖未獲通過補助,我們仍利用有限的人力 經費下,取得部分成果。我們分析了120個高血壓受試者的頸動脈血 管超音波影像,發現頸動脈的血管環狀應變與應變率為預測預後的 獨立因子。此重要發現顯示本研究的前瞻性與重要性。有幸第二年 計畫獲得通過,亦獲得重要成果,我們發現脂聯素 (adiponectine)與頸動脈應變與應變率相關,可能藉由改變間質重 組來影響。第三年計畫亦獲得通過、我們進一步發現動脈硬度影響 對運動引起的心臟舒張功能障礙,進一步確立心臟血管應合 (cardio-vascular coupling)的重要性。第四年、我們完成研究頸 動脈血管應變與運動中心臟改變的分析,並研究其對心血管預後的 影響。 中 文 關 鍵 詞 : 高血壓, 頸動脈血管應變, 亮點追蹤心臟超音波
英 文 摘 要 : Hypertension is a well-known major risk factor for cerebral and cardiovascular diseases, and is known to be
significantly associated with increased all-cause and cardiovascular mortality. Hypertension causes symptomatic and asymptomatic organ damage of the brain, heart, kidney and vascular system.
Speckle tracking echocardiography is a technique used to assess myocardial deformation, and has been recently used to assess vascular wall deformation such as for the
abdominal aorta and carotid artery. In our recent study, we have demonstrated that carotid strain and strain rate could be measured from speckle tracking echocardiography. These parameters were better indices for local arterial
properties and that they were associated with previous stroke in the elderly but not regional or systemic
parameters of arterial stiffness. We believe that carotid vascular strain can be a useful tool for evaluation
vascular remodeling under the effects of hypertension and also can have prognostic value for patients with
hypertension.
despite of no funding support in the first year. We have analyzed carotid strain of 120 hypertensive patients. We have found that circumferential strain and strain rate were independent prognostic predictors in these hypertensive patients. Our findings indicate that this proposal is worth to be carried on and supported. Our second year proposal has been approved. We have found serum adiponectin was associated with carotid vascular strain and strain rate. Adiponectin probably affected vascular strain through the effects on matrix remodeling. We also have completed the third year plan. We found peripheral vascular stiffness could affect diastolic dysfunction induced by exercise. This result indicates the importance of cardio-vascular coupling. In this year, we have completed the carotid vascular strain analysis and cardiac changes during
exercise, and also analyzed the effects of these changes on cardiovascular events.
中、英文摘要及關鍵詞 (keywords) 中文摘要 高血壓為最重要的心血管危險因子,會造成心血管、腦血管、腎臟病以及死 亡。高血壓也會引起無症狀的器官傷害,包括腦部、心臟、腎臟、以及血管系 統。 亮點追蹤超音波可以用來測量心臟的形變,最近也被用來測量頸動脈的血 管應變。我們最近的研究發現頸動脈的血管環狀應變與應變率可以由亮點追蹤 超音波測得。而頸動脈的血管環狀應變與應變率比起傳統的動脈硬度參數,更 準確地與腦中風有相關。我們認為頸動脈的血管環狀應變與應變率是很好用來 評估高血壓對血管影響的參數,而且也應具有對高血壓併發症預後的預測價 值。 這個四年期的研究計畫想要利用頸動脈的血管環狀應變與應變率來研究高 血壓病人。第一年雖未獲通過補助,我們仍利用有限的人力經費下,取得部分 成果。我們分析了 120 個高血壓受試者的頸動脈血管超音波影像,發現頸動脈 的血管環狀應變與應變率為預測預後的獨立因子。此重要發現顯示本研究的前 瞻性與重要性。有幸第二年計畫獲得通過,亦獲得重要成果,我們發現脂聯素 (adiponectine)與頸動脈應變與應變率相關,可能藉由改變間質重組來影響。 第三年計畫亦獲得通過、我們進一步發現動脈硬度影響對運動引起的心臟舒張 功能障礙,進一步確立心臟血管應合(cardio-vascular coupling)的重要性。 第四年、我們完成研究頸動脈血管應變與運動中心臟改變的分析,並研究其對 心血管預後的影響。 關鍵字: 高血壓, 頸動脈血管應變, 亮點追蹤心臟超音波 Abstract
Hypertension is a well-known major risk factor for cerebral and cardiovascular diseases, and is known to be significantly associated with increased all-cause and cardiovascular mortality. Hypertension causes symptomatic and asymptomatic organ damage of the brain, heart, kidney and vascular system.
Speckle tracking echocardiography is a technique used to assess myocardial deformation, and has been recently used to assess vascular wall deformation such as for the abdominal aorta and carotid artery. In our recent study, we have demonstrated that carotid strain and strain rate could be measured from speckle tracking
In this 4-year study proposal, we plan to use carotid vascular strain for studying vascular remodeling in hypertension. Unfortunately we did not have the grant in the first year. However, we still have some study results despite of no funding support in the first year. We have analyzed carotid strain of 120 hypertensive patients. We have found that circumferential strain and strain rate were independent prognostic
predictors in these hypertensive patients. Our findings indicate that this proposal is worth to be carried on and supported. Our second year proposal has been approved. We have found serum adiponectin was associated with carotid vascular strain and strain rate. Adiponectin probably affected vascular strain through the effects on matrix remodeling. We also have completed the third year plan. We found peripheral vascular stiffness could affect diastolic dysfunction induced by exercise. This result indicates the importance of cardio-vascular coupling. In this year, we have completed the carotid vascular strain analysis and cardiac changes during exercise, and also analyzed the effects of these changes on cardiovascular events.
Background
Hypertension is a well-known major risk factor for cerebral and cardiovascular diseases, and is known to be significantly associated with increased all-cause and cardiovascular mortality [1,2]. It has been reported that by 2025 hypertensive cardiovascular diseases will affect an estimated population of 1.56 billion [3,4]. Despite advances in antihypertensive therapy, the residual cerebral and cardiovascular risk in patients treated for hypertension remains a serious problem. Hypertension causes symptomatic and asymptomatic organ damage of the brain, heart, kidney and vascular system [5,6].
Arterial stiffness is a functional change of atherosclerosis that can be measured in regional arterial systems and in local arteries such as the carotid artery [7]. Speckle tracking echocardiography is a technique used to assess myocardial deformation, and has been recently used to assess vascular wall deformation such as for the abdominal aorta and carotid artery [8-11]. A recent study using speckle tracking
echocardiography measuring the circumferential strain (CS) and circumferential strain rate (CSR) of the common carotid artery confirmed that this technique is a sensitive method to assess arterial elastic properties [11]. Carotid vascular strain measured by speckle tracking echocardiography has also been validated in animal studies [12,13].
In our recent study, we have demonstrated that carotid CS and CSR could be measured from speckle tracking echocardiography. These parameters were better indices for local arterial properties and they were associated with previous stroke in the elderly but not regional or systemic parameters of arterial stiffness [14]. We believe that carotid vascular strain can be a useful tool for evaluation vascular remodeling under the effects of hypertension and also can have prognostic value for patients with hypertension.
As a direct organ impact by blood flow after ventricular ejection, carotid artery remodeling would be affected by high blood pressure in hypertension. Several
parameters for carotid vascular function including pulse wave velocity, carotid intima-medial thickness, carotid beta-index were associated with stroke in hypertension [15,16].Carotid strain by speckle tracking echocardiography do not need to use blood pressure in measurements [17]. It is an ideal tool for evaluation of carotid remodeling under the effects of hypertension.
References
1. Gu Q, Dillon CF, Burt VL, Gillum RF. Association of hypertension treatment and control with all-cause and cardiovascular disease mortality among US adults with hypertension. Am J Hypertens 2010; 23:38-45.
2. James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC Jr, Svetkey LP, Taler SJ, Townsend RR, Wright JT Jr, Narva AS, Ortiz E. 2014 evidence-based
guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; 311:507-520.
3. Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet 2005; 365:217–223. 4. Chiang CE, Chen CH. Hypertension in the Asia-Pacific region. J Hum Hypertens 2008; 22:441–443.
5. Strate M, Thygesen K, Ringsted C, Hansen L, Harvald B. Prognosis in treated hypertension. Acta Med Scand 1986; 219:153-159.
6. Leonetti G, Cuspidi C. The heart and vascular changes in hypertension. J Hypertens Suppl 1995; 13:S29-S34.
7. Araki T, Masanori E, Yokoyama H, Maeno T, Hatsuda S, Mori K, Koyama H, Shoji T, Inaba M, Nishizawa Y. The association of plasma adiponectin level with carotid arterial stiffness. Meta Clin Exp 2006; 55:587-592.
8. Oishi Y, Mizuguchi Y, Miyoshi H, Iuchi A, Nahase N, Oki T. A novel approach to assess aortic stiffness related to changes in aging using two-dimensional strain
imaging. Echocardiography 2008; 25:941-945.
9. Bjallmark A, Lind B, Peolsson M, Shahgaldi K, Brodin LA, Nowak J.
Ultrasonographic strain imaging is superior to conventional non-invasive measures of vascular stiffness in the detection of age-dependent differences in the mechanical properties of the common carotid artery. Eur J Echocardiogr 2010; 11:630-636. 10. Cho IJ, Shim CY, Yang WI, Kim SA, Chang HJ, Jang Y, Chung N, Ho JW. Assessment of mechanical properties of common carotid artery in Takayasu’s arteritis using velocity vector imaging. Circ J 2010; 74:1465-1470.
11. Catalano M, Lamberti-Castronuovo A, Catalano A, Filocamo D, Zimbalatti C. Two-dimensional speckle-tracking strain imaging in the assessment of mechanical properties of carotid arteries: feasibility and comparison with conventional markers of subclinical atherosclerosis. Eur J Echocardiogr 2011; 12:528-535.
12. Widman E, Caidahl K, Heyde B, D’hooge J, Larsson M. Ultrasound speckle tracking strain estimation of in vivo carotid artery plaque with in vitro
2015;60:1107-1123.
13. Larsson M, Verbrugghe P, Smoljkic M, Verhoeven J, Heyde B, Famae N, Herijers P, D’hooge J. Strain assessment in the carotid artery wall using ultrasound speckle tracking: validation in a sheep model.
14. Tsai WC, Sun YT, Liu YW, Ho CS, Chen JY, Wang MC, Tsai LM. Usefulness of vascular wall deformation for assessment of carotid arterial stiffness and associated with previous stroke in elderly. Am J Hypertens 2013; 26:770-777.
15. Laurent S, Katsahian S, Fassot C, Tropeano AI, Gautier I, Laloux B, Boutouyrie P. Aortic stiffness is an independent predictor of fatal stroke in essential hypertension. Stroke 2003; 34:1203-1206.
16. Sugioka K, Hozumi T, Sciacca RR, Miyake Y, Titova I, Gaspard G, Sacco RL, Homma S, Di Tullio MR. Impact of aortic stiffness in ischemic stroke in elderly patients. Stroke 2002; 33:2077-2081.
17. Tsai WC, Sun YT, Liu YW, Ho CS, Chen JY, Wang MC, Tsai LM. Response to “vascular mechanics and stroke-a critical appraisal: Study the arteries but do not forget the flow” Am J Hypertens 2013;26:947.
Methods
1. Carotid artery ultrasound: The method for carotid ultrasound has been described clearly in our previous study [14]. Carotid B-mode images will be acquired by using a multi-frequency 7.5-10 MHz high resolution vascular probe equipped on an
echocardiographic system (E9, GE-VingMed, Horton, Norway). The probe is kept perpendicular to the far wall of carotid artery. Bilateral long-axis views of the common carotid arteries up to the carotid bulb are acquired for 3 cardiac cycles to optimize the best visualization of the intima-media complex. Cross sectional images of bilateral common carotid arteries at the level of 1 cm below carotid bulb are also acquired for 3 cardiac cycles with a frame rate of 50-70 frames per second. All of the images are stored digitally in RawDICOM format. All ultrasonographic images are acquired by the same operator who is blinded to the clinical characteristics of each subject.
software. The software selects stable speckles within the arterial wall and tracks these speckles frame by frame throughout the entire cardiac cycle. The software then divides the entire carotid arterial circumference into 6 conventional segments and provides a tracking quality (green=good, red=bad) for each segment. If the tracking is poor, the operator can readjust the region of interest by moving the endothelial lining or by changing its width to achieve a better tracking. After this adjustment, the software will recheck tracking quality. All of the 6 segments with good tracking quality are considered to be satisfactory images. Time-strain and time-strain rate plots are produced automatically by the software. Peak CS and CSR are identified from the global strain or strain rate curve. An average of 3 measurements is taken for analysis. The reproducibility of speckle tracking for carotid artery in our laboratory has been tested from 10 random samples. For CS, the intra-observer concordance correlation coefficient (ρ) was 0.96 and rater agreement statistic (K) was 0.79, and the inter-observer ρ was 0.95 and K was 0.72. For CSR, the intra-inter-observer ρ was 0.95 and K was 0.75, and the inter-observer ρ was 0.94 and K was 0.77. For TCS, the intra-observer ρ was 0.75 and K was 0.51, and the inter-intra-observer ρ was 0.82 and K was 0.64. For TCSR, the intra-observer ρ was 0.90 and K was 0.82, and the inter-observer ρ was 0.86 and K was 0.75 [14].
3. Measurements of intima-medial thickness (IMT), beta-index (BI), and distensibility (DI): The longitudinal images are analyzed to calculate IMT, define as thickness of the vascular intima-media complex obtained 1 cm below the carotid bulb. IMT is measured at the far wall by using automated border detection software in the workstation (EchoPac 2011, GE-VingMed, Horten, Norway). IMT is measured including the inner edge and excluding the outer edge of the double line pattern of the intimal and medial thickness along the carotid artery for 1 cm in length. Average values of IMT along this 1 cm segment are used for analysis. Plaque was defined if IMT >1.1 mm at one or more sites [18]. Diameter of the carotid artery is measured by M-mode across the center of this longitudinal image, and maximal diameter is
measured in systolic phase and minimal diameter in diastolic phase. An average of 3 measurements is used for calculation. BI is calculated as ln(systolic blood
pressure/diastolic blood pressure)/(maximal diameter - minimal diameter); DI as 2(changes in carotid diameter)/(minimal diameter)(pulse pressure) [19].
4. Measurement of pulse wave velocity and peripheral arterial stiffness: For
finger and right second toe simultaneously, and also measure the time difference (i.e., transit time) between the two roots of the digital volume pulses. The finger-to-toe distance was the difference from the sternal notch to the right second toe and from the sternal notch to the right index finger. The values of pulse wave velocity (m/s) were obtained automatically from software calculation of the finger-to-toe distance divided by the transit time, which has been validated and shown to have a good correlation with carotid-to-femoral PWV measured by applanation tonometry in our previous work [20]. We also have developed a new index “compliance index (CI)” for
measurement of peripheral arterial stiffness [26]. The CI was derived from area under curve of digital volume pulse divided by pulse pressure.
5. Exercise test: Supine bicycle exercise test will be conducted in the second year. After baseline carotid ultrasound in rest, carotid artery images will be acquired in each stage during exercise test. A supine ergometer is used with ability to adjust body position to supine position. Heart rate and blood pressure are monitoring during exercise. Bicycle exercise is started as 25W with cycle rate of 60/min. Each stage is 3 minutes with 25W increment. Carotid images will be recorded in baseline, 25W, and 50W stages.
Reference
18. Hirano M, Nakamura T, Obata J, Fujioka D, Saito Y, Kawabata K, Watanabe K, Watanabe Y, Kugiyama K. Early improvement in carotid plaque echohenicity by acarbose in patients with acute coronary syndrome. Circ J 2012; 76:1452-1469. 19. Chen JY, Tsai WC, Lin CC, Huang YY, Hsu CH, Liu PY, Chen JH. Stiffness index derived from digital volume pulse as a marker in target organ damage of untreated hypertension. Blood Pressure 2005; 14:233-237.
20. Tsai WC, Chen JY, Wang MC, Wu HT, Chi CK, Chen YK, Chen JH, Lin LJ. Association of risk factors with increased pulse wave velocity detected by a novel method using dual-channel photoplethysmography. Am J Hypertens 2005; 18:1118-1122.
21. Tsai WC, Lin CC, Chen JY, Huang YY, Lee CH, Li WT, Weng CM, Chen JH. Association of adiponectin with procollagen type I carboxyterminal propepetide in non-diabetic essential hypertension. Blood Pressure 2008; 17:233-238.
22. Liu P, Sun M, Sader S. Matrix metalloproteinases in cardiovascular disease. Can J Cardiol 2006; 22 (Suppl B): 26B-30B.
23. Back M, Ketelhuth DFJ, Agewall S. Matrix metalloproteinases in atherothrombosis. Prog Cardiovasc Dis 2010; 52:410-428.
transposition of the great arteries. Am J Cardiol 2014;113:713-718.
25. Wang J, Fang F, Yip GWK, Sanderson JE, Feng W, Xie JM, Luo XX, Yu CM, Lam YY. Quantification of left ventricular performance in different heart failure phenotypes by comprehensive ergometry stress echocardiography. Int J Cardiol 2013;169:311-315.
Results
1. Effects of carotid strain on prognosis in treated hypertension patients (full paper under submission)
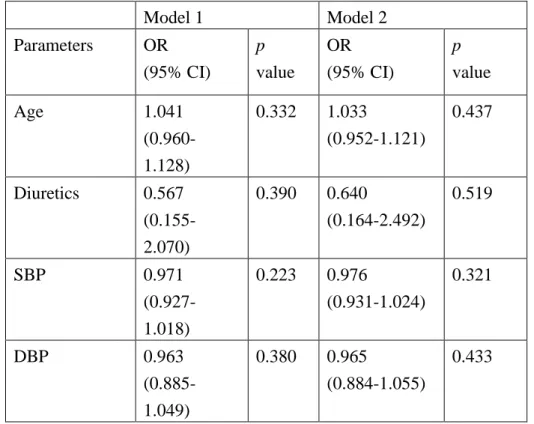
We have prospectively recruited 120 patients being treated for hypertension (65.8 ± 11.8 years, 58% male) in this observational study. Carotid deformation indices including peak circumferential strain (CS) and peak strain rate (CSR) after ejection were identified using two-dimensional speckle tracking echocardiography. The average of bilateral CS and CSR of the carotid arteries were used for analysis. The end-points of this study were cardiovascular events including any admission for stroke, acute coronary syndrome, and heart failure. After a mean follow-up period of 63.6 ± 14.5 months, 14 (12%) patients reached the end-points. Age (75.3 ± 9.2 vs. 64.6 ± 11.6 years; p = 0.001), systolic blood pressure (131.8 ± 15.5 vs. 143.1 ± 16.6 mmHg; p = 0.021), diastolic blood pressure (74.6 ±11.4 vs. 82.1 ± 12.2 mmHg; p = 0.039), use of diuretics (71 vs. 92 %; p = 0.014), carotid CS (2.17 ± 1.02 vs. 3.28 ± 1.14 %; p = 0.001), and CSR (0.28 ± 0.17 vs. 0.51 ± 0.18 1/s; p <0.001) were
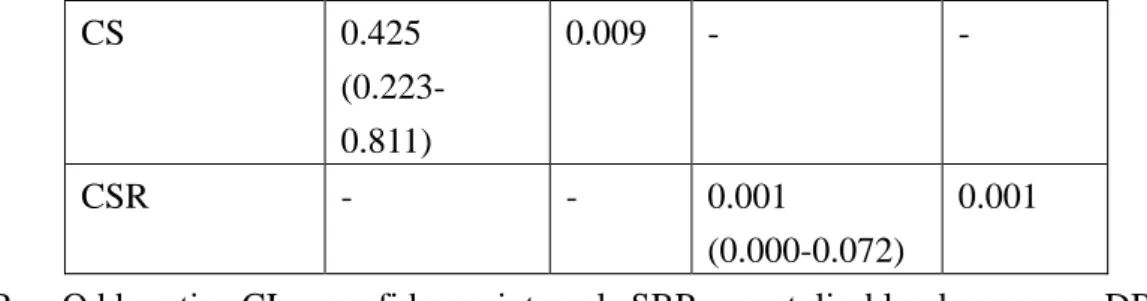
significantly different between the patients who did and did not reach the end-points. Multivariate Cox regression analysis controlling for age, systolic blood pressure, diastolic blood pressure, and use of diuretics showed that CS (OR 0.425, 95%CI 0.223-0.811, p = 0.009) and CSR (OR 0.001, 95%CI 0.000-0.072, p = 0.001) were independent predictors for cardiovascular events (Table 1). In conclusions, decreased carotid strain and strain rate were associated with cardiovascular events in
hypertension.
Table 1. Multivariate Cox regression analysis for independent factors for outcomes
CS 0.425 (0.223-0.811) 0.009 - - CSR - - 0.001 (0.000-0.072) 0.001
OR = Odds ratio; CI = confidence interval; SBP = systolic blood pressure; DBP = diastolic blood pressure; CS = carotid circumferential strain; CSR = carotid circumferential strain rate; : not enrolled.
2. Factors affect carotid strain (full paper under submission)
In order to study factors contributed to the carotid strain, we have recruited 89 consecutive elder patients (mean age 72 ± 6 years, 31 men) from a community health survey program. We found that serum adiponectin was significantly correlated with carotid CS (r = 0.362, p = 0.001) and CSR (r = 0.313, p = 0.003) but not intima-medium thickness (IMT) and Beta-index. After multivariate analysis controlling age, blood pressure, body mass index, and serum glucose level, adiponectin was still significantly correlated with CS (Beta = 0.313, p = 0.001) and CSR (Beta = 0.272, p = 0.010) (Table 2). Adiponectin was significantly correlated with procollage type I carboxyterminal propeptide, pro-matrix metalloproteinases I, and tissue inhibitor of metalloproteinases I (Table 3). These results indicated that adiponectin was correlated with CS and CSR of carotid artery independently. This association was probably through the effects on matrix remodeling of carotid artery.
Table 2 Multivariate linear regression analysis for correlation between
adiponectin and carotid deformation
Factors affect carotid
deformation*
Circumferential strain Circumferential strain
rate
Adiponectin β = 0.313, p = 0.001 β = 0.272, p = 0.010
Age β = -0.321, p = 0.001 β = -0.229, p = 0.029
Systolic blood pressure β = 0.076, p = 0.581 β = -0.060, p = 0.692
Body mass index β = -0.094, p = 0.305 β = 0.014, p = 0.886
Glucose β = -0.187, p = 0.048 β = 0.027, p = 0.790
*Including significant factors in correlation test and body mass index
Table 3 Correlation between adiponectin and matrix metalloproteinases
Matrix
metallopreteinases
Correlation analysis Multivariate analysis
controlling systolic blood
pressure and body mass
index PICP r = -0.219, p = 0.039 β = -0.185, p = 0.085 pMMP1 r = -0.354, p = 0.001 β = -0.385, p = 0.001 MMP3 r = 0.122, p = 0.256 MMP9 r = 0.063, p = 0.555 TIMP1 r = 0.387, p <0.001 β = 0.370, p <0.001 pMMP1/TIMP1 r = 0.345, p = 0.001 β = -0.315, p = 0.003 MMP9/TIMP1 r = -0.148, p = 0.165
PICP = procollage type I carboxyterminal propeptide pMMP1 = pro-matrix metalloproteinases I
MMP3 = matrix metalloproteinases III MMP9 = matrix metalloproteinases IX
3. Effects of arterial compliance on exercise (abstract in EUROECHO 2017 conference)
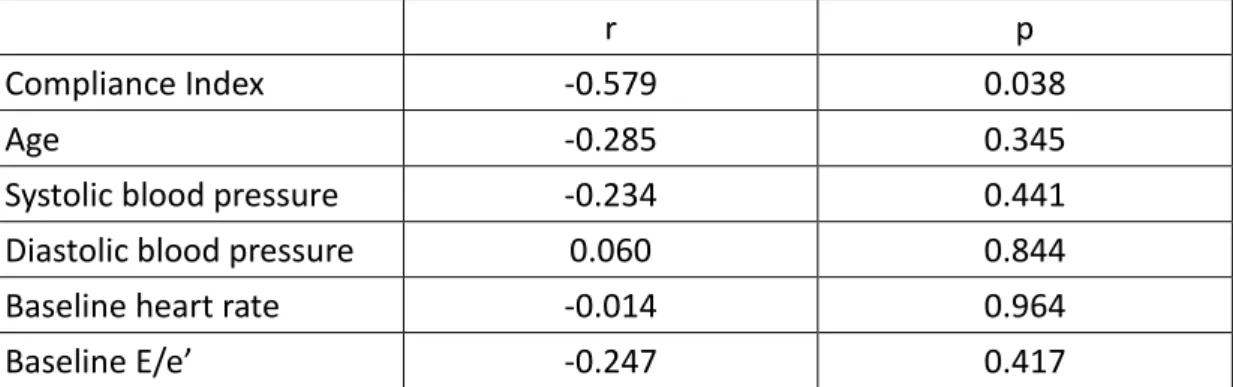
We recruited 23 patients (mean age 54 ± 11 years, 2 women) with regularly treated hypertension in this study. All patients were all uncomplicated and free of structural heart diseases. All patients were without left ventricular hypertrophy and diastolic heart failure and with normal ejection fraction. Peripheral arterial Compliance Index (CI) was measured by self-development photoplethysmography system immediately before stress test. This system could record digital volume pulse (DVP) from the index finger. The area under the curve of each DVP was measured automatically using the system. A novel CI was derived by dividing the average area under the curve of the DVP in 5 s by the brachial pulse pressure.CI has been proved to be an index for peripheral arterial stiffness. Stress echocardiography was performed by supine ergometer with fixed work-load (50-75W). Diastolic function was assessed by early filling velocity to average annular velocity ration (E/e’) before and during exercise. We found that (1) Differences of E/e’ (DEe) between maximal stress and rest were regarded as changes of diastolic function during exercise. DEe was significantly correlated with CI (r = -0.579, p = 0.038). There were no correlation between DEe with age, blood pressure, and resting E/e’ (Table 4). (2) After multivariate analysis controlling age and baseline E/e’, CI was still an independent factor for DEe (beta = -0.664, p = 0.028). These results indicated that decreased peripheral arterial
compliance was associated with exercise related diastolic dysfunction in hypertension.
Table 4 Correlation of DEe with other factors
r p
Compliance Index -0.579 0.038
Age -0.285 0.345
Systolic blood pressure -0.234 0.441 Diastolic blood pressure 0.060 0.844 Baseline heart rate -0.014 0.964 Baseline E/e’ -0.247 0.417
4. Effects of carotid strain and cardiac exercise changes on prognosis (data under analysis)