BIOMEDICAL
ENGINEERING-APPLICATIONS, BASIS & COMMUNICATIONS 31
SAFETY AND USEFULNESS OF COLONFIBROSCOPY
IN THE VERY ELDERLY
SHU-CHEN WEI, JAU-MIN WONG, MING-JIUM SHIEH, CHENG-YI WANG
Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
ft esmfaotkm de&tf not be
chatge or aneMia. mtd who havt , .. .,
;
, . W&*ti$&&Lu-3£.
Ai.ArBt..
1. INTRODUCTION
As the world population continues to age, the need for colonfibroscopy in the very elderly will in crease. Many authors have stressed the safety and fea sibility of colonfibroscopy for elderly patients with ailments related to the digestive tract [1-5]. Many pre vious reports have discussed the results of upper gas trointestinal tract panendoscopy and sigmoidoscopy in Received: November 7,2001; accepted: February 3,2002. Correspondence: Cheng-Yi Wang, Professor
Department of Internal Medicine, National Taiwan University Hospital, No. 7 Chung-Shan South Road, Taipei, Taiwan.
elderly patients. However, there are still no reports which have restricted their study of colonfibroscopy to the very elderly patients (aged 80 years or above). The aim of this study was to explore the safety and useful ness of colonfibroscopy in the very elderly.
2. METHODS
This retrospective study was conducted to explore the diagnostic role and safety of colonfibroscopy for the very elder patients (aged 80 years or above). We reviewed the medical charts and endoscopic records of all very elderly patients who had received colonfibro-scopic studies at National Taiwan University Hospital from January 1992 to December 1997. The indications
31
-ABSTRACT
The population of elderly people has increased in recent years. The importance of endoscopy as a diagnostic tool is indisputable. The feasibility and safety of upper gastrointestinal tract panendo-scopy and sigmoidopanendo-scopy in elderly patients has been reported previously. However, there are still no reports about colonfibroscopy in the elderly, especially for the very elder patients (aged 80 years or above). This retrospective study reviewed the chart and endoscopic records of patients aged 80 or more who underwent colonfibroscopy examination at our hospital from January 1992 to December 1997. The basic clinical information, indications of endoscopy, the diagnostic results, and the follow-up conditions were all recorded and analyzed. A total of 240 colonfibroscopy examinations were per-formed in 189 patients. All the patients tolerated the procedure well. No complications were noted
during and after the colonfibroscopy studies. The most frequent indication of colonfibroscopy was bloody stool and/or positive stool occult blood test. In considering the final diagnosis, adenoma and/or polyp, hemorrhoids, and colorectal cancer were the three most frequent etiologies in these pa-tients. Only 17 examinations could not be properly completed due to poor colon preparation. Colonfibroscopy was a safe and useful diagnostic tool for the very elder patients. These very elderly patients had a high incidence of colorectal cancer, especially for those who had a past history of
co-lorectal cancer (metachronous cancer). Those who had bloody stool and/or positive stool occult blood test, bowel habit change or anemia, and who have a history of colorectal cancer should un-dergo the colonfibroscopy.
Biomed Eng Appl. Basis Comm, 2002 (February); 14: 31-34. Key words: colonfibroscopy, very elderly.
32 Vol. 14 No. 1 February 2002
for colonfibroscopy, diagnostic results, endoscopic findings, histology results, follow-up periods and pa tients' survival status, and demographic information were recorded and analyzed. Patients were prepared with a low fiber diet for 3 days as possible. Bowel cleaning was then performed with magnesium citrate oral solution and bisacodyl one night before the ex amination. Intramuscular meperidine hydroxy chloride was used for sedation and hyoscine butylbromide for anti-spasmodic effect of the bowel were routinely given before the procedure, except for patients' whose clinical condition could not tolerate the medications.
3. RESULTS
From January 1992 to December 1997, a total of 240 colonfibroscopy examinations were performed in 189 patients aged 80 or above at National Taiwan University Hospital. The National Taiwan University Hospital is a tertiary care center at Taipei in Taiwan. There were 72 women and 117 men with a mean age of 81.6 years (range, 80.0 to 87.6). The post-examination follow-up period ranged from one month to 6.5 years (mean 2.2 years). Among these 240 ex aminations, 140 (58.3%) were done in the out-patient-department, 89 (37.1%) in the general ward, three (1.3%) in the emergency room, four (1.7%) in the in tensive care unit, and four (1.7%) in the general check up unit. Preparative medications for colonfibroscopy included meperidine hydroxychloride 92.1% (221/240), and hyoscine butylbromide 97.1% (233/240). All pa tients tolerated the procedure well. No complications
were noted during and after the colonfibroscopy stud ies. Thirty-eight patients died during the follow-up pe riod. One died of gastrointestinal tract bleeding, 22 died of infection (pneumonia and/or urinary tract in fection), 11 died of heart failure and arrhythmia, two died of colon cancer with complications and two died of sarcoma with complications.
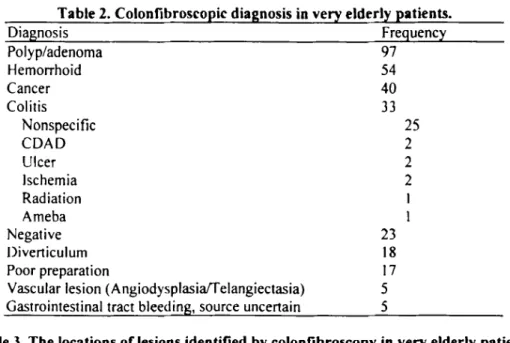
The indications for colonfibroscopy in these pa tients are listed in Table 1. The most frequent indica tions were bloody stool and/or positive stool occult blood test, adenoma and/or polyp follow-up, and bowel habit change, respectively. The three most fre quent etiologies in these patients were adenoma and/or polyp, hemorrhoids, and colorectal cancer. The diag nostic results are summarized in Table 2. Thirteen pa tients had colorectal cancer as well as adenoma and/or polyp. Only 17 examinations could not be completed due to poor colon preparation. The locations of the le sions identified by colonfibroscopy are shown in Table 3. The most frequent indication for colonfibroscopy was bloody stool and/or positive stool occult blood test. The final diagnoses of these patients are summarized in Table 4. Adenoma and/or polyp were the most common diagnosis. The indications for performing colonfibroscopy in patients with a final diagnosis of colorectal cancer are shown in Table 5.
4. DISCUSSION
As a diagnostic procedure, colonfibroscopy is relatively more difficult than other type of endoscopy and might carry a higher complication rate also. The Table 1. The Indications for colonfibroscopy in very elderly patients.
Indication Frequency Percent
Bloody stool and/or Positive stool occult blood test Adenoma and/or polyp, F/U
Bowel habit change
Suspicious lesion by abdominal sonography or barium enema Colon cancer s/p operation, Follow-up
Anemia
Abdominal pain Physical examination
Increase of carcinoembryonic antigen (CEA) Searching for primary site of metastatic cancer Carcinoid tumor, Follow-up
Ileus 66 61 35 27 23 9 7 4 4 2 1 1 27.5 25.4 14.6 11.3 9.6 3.8 2.9 1.7 1.7 0.8 0.4 0.4 Total 240 100 3 2
-BI0MED1CAL
ENGINEERING-APPLICATIONS, BASIS & COMMUNICATIONS 33
Table 2. Colonfibroscopic diagnosis in very elderly patients.
Diagnosis Frequency Polyp/adenoma Hemorrhoid Cancer Colitis Nonspecific CDAD Ulcer Ischemia Radiation Ameba Negative Diverticulum Poor preparation
Vascular lesion (Angiodysplasia/Telangiectasia) Gastrointestinal tract bleeding, source uncertain
97 54 40 33 25 2 2 2 1 1 23 18 17 5 5
Table 3. The locations of lesions identified by colonfibroscopy in very elderly patients. Locations Frequency Percent
Anus/Rectum Sigmoid colon Descending colon Transverse colon Ascending colon Cecum
Multiple, distal colon Multiple, proximal colon
Multiple, distal and proximal colon
57 35 9 7 16 5 28 10 27 29.2 17.9 4.6 3.6 8.2 2.6 14.4 5.1 14.4 Total 195 100
safety of colonfibroscopy and the colonic disease pat terns in the very elderly remain unclear. In this study, there were no complications during and after 240 colonfibroscopy procedures. A l l of the 198 patients tolerated the procedure well. Thus, colonfibroscopy seems to be a safe procedure for the very elderly.
Flexible sigmoidoscopy is superior to rigid sig-moidoscopy, as it allows examination o f longer lengths of bowel and has a five- to sixfold greater diagnostic yield than rigid sigmoidoscopy [3]. The relative supe riority between flexible sigmoidoscopy and colonfi broscopy is less clear. According to the locations of the identified lesions by colonfibroscopy in our pa tients, 33.9% would have been missed i f we had only performed the sigmoidoscopy. By using the same bowel preparation and pre-procedure medications, we suggest that colonfibroscopy is a better diagnostic tool than sigmoidoscopy which has a similar complication rate but obtains a higher diagnostic yield.
Double-contrast enema is another option for studying the colon. In a previous study, the rate o f suc cessful completion was 94.9% (113/119) in patients in
the eighth decade, and 90% (81/90) in those 80 and over. Most unsuccessful double contrast enemas were due to the patient's inability to retain barium or the en ema tip itself, and occurred mostly in the non-ambulatory patients [6]. In our colonfibroscopic stud ies, 7 . 1 % (17/240) o f failures were due to poor prepa ration and 2 . 1 % (5/240) were due to bleeding from a source which could not be clearly identified on colon fibroscopy. Overall, the success rate was still higher than that reported for double contrast enema. In this study, poor bowel preparation was also mostly seen in patients with disability. Endoscopy can identify minor lesions such as vascular lesions and inflammatory change and allows for biopsy for histology studies. We recommend colonfibroscopy for elderly patients in stead of sigmoidoscopy or double contrast enema.
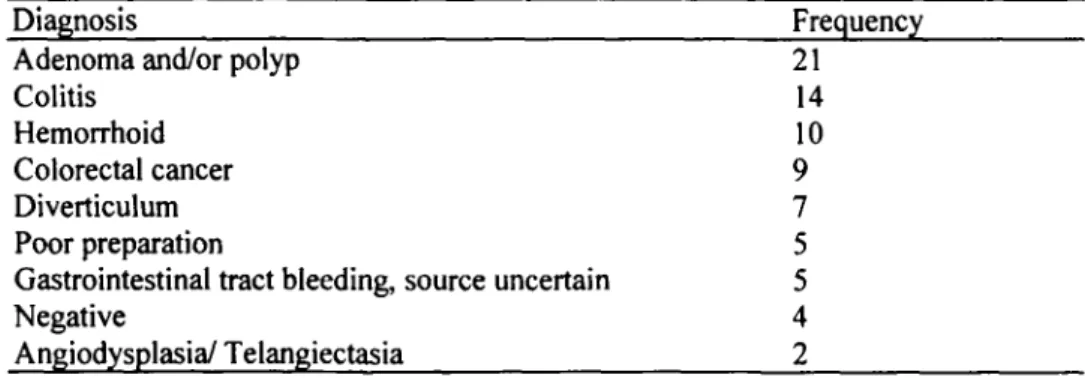
In this series, the most frequent indication for colonfibroscopy was bloody stool and/or positive stool occult blood test. The most prevalent diagnoses were adenoma and/or polyp followed by colitis, hemorrhoid, colorectal cancer for patients with this indication (Ta ble 4). A relatively high incidence 16.7% (40/240) of
34 Vol. 14 No. 1 February 2002
Table 4. The final diagnosis among very elderly patients with the colonfibroscopic indication of bloody stool and/or positive stool occult blood test
Diagnosis
Adenoma and/or polyp Colitis
Hemorrhoid Colorectal cancer Diverticulum Poor preparation
Gastrointestinal tract bleeding, source uncertain Negative Angiodysplasia/ Telangiectasia Frequency 21 14 10 9 7 5 5 4 2
Table 5. Indications for coionfibroscopy in very elderly patients with a final diagnosis of colorectal cancer
Indication Frequency Percent (%)
Bloody stool and/or positive stool occult blood test
Suspicious lesion by abdominal sonography or barium enema Colorectal cancer s/p operation
Bowel habit change Anemia Adenoma/polyp Abdominal pain Ileus 9 9 8 6 4 2 1 1 22.5 22.5 20 15 10 5 2.5 2.5 Total 40 100
colorectal cancer was found in this series. It is gener ally agreed that the incidence of cancer increases with age [7,8]. In this series, the three most frequent presen tations of colorectal cancer were bloody stool and/or positive stool occult blood test, bowel habit change and anemia (Table 5). Therefore, the occurrence of these symptoms in the very elderly should lead to sus picion of colorectal cancer and prompt coionfibro scopy is highly recommended. Among the follow-up patients with a history of colorectal cancer, a very high percentage (34.7%, 8/23) of metachronous colorectal cancer was found on coionfibroscopy. The necessity of regular colonfibroscopic follow-up for patients with colorectal cancer should not be overlooked.
In summary, in this series, coionfibroscopy was a safe and useful diagnostic tool for very elderly patients. Bloody stool and/or positive stool occult blood test was the most frequent indication for coionfibroscopy, and adenoma and/or polyp was the most common di agnosis. These very elderly patients had a high inci dence of colorectal cancer. Therefore, we conclude that very elderly patients with bloody stool and/or positive stool occult blood test, bowel habit change or anemia, and those with a history of colorectal cancer should undergo the coionfibroscopy examination.
REFERENCES
1. Jacobson WZ, Levy A. Endoscopy of upper gastro intestinal tract is feasible and safe in elderly pa tients. Geriatrics. 1977; 1: 80-83.
2. Lee YC, Tarn HC. Upper gastrointestinal endo scopy for Chinese elderly in an acute geriatric unit: a review. Age Ageing. 1984; 13:285-290.
3. Helzberg JH, Mccallum RW. Flexible sigmoido-scopy: safety and usefulness in the geriatric patient.
Geriatrics. 1985; 40: 105-108.
4. Brussaard CC, Vandewoude MFJ. A prospective analysis of elective upper gastro- intestinal endo scopy in the elderly. Gastrointest Endosc. 1988; 34:118-121.
5. Holt RW, Wherry DC. Why flexible fiberoptic sigmoidoscopy is important in the geriatric patient. Geriatrics. 1979;5:85-88.
6. Wolf EL, Frager D, Beneventano TC. Feasibility of double-contrast barium enema in the elderly. AJR
Am J Roentgenol. 1985; 145:47-8.
7. Bolin S, Nilsson E, Sjodahl R. Carcinoma of colon and rectum. Growth rate. Ann Surg. 1983; 198:151. 8. Minaker K, Rowe J. Gastrointestinal system. In:
Health and Disease in old age. Rowe J., Besdine R. eds. Boston: Little Brown and Company; 1982.