The Efficacy of Hyperbaric Oxygen Therapy in
Improving the Quality of Life in Patients
With Problem Wounds
Li-Chen Lin · Grace Yau* · Teng-Fu Lin** · Tsung-Kun Lin*** Yu-Ying Tang**** · Kwua-Yun Wang*****
ABSTRACT: The unpredictable course followed by severe, chronic, non-healing wounds not only restricts the daily activities of affected patients, but also impairs their quality of life (QOL). Hyperbaric oxygen therapy (HBOT) treatment for such wounds elevates tissue oxygen content, increases cellular repair functions and the probability of wound healing, and improves the patient’s QOL. This was a longitudinal, prospective study, and used a purposive sampling method. A total of 15 patients receiving HBOT at a medical center were enrolled. Data were collected by questionnaire before and after HBOT. The questionnaire included basic patient characteristics, self-perceived wound severity, wound physiological indices, and a QOL scale. The overall QOL score of the subjects after HBOT was higher than before HBOT. After HBOT, there was a positive correlation between the QOL of patients with problem wounds and the scoring of the Strauss wound classification system. After HBOT, there was a negative correlation between the QOL of patients with problem wounds and their self-perceived severity of the wound. The results were then used to provide suggestions for nursing care and additional research directions in order to effectively assist patients with problem wounds receiving HBOT, with the goal of achieving an optimal QOL.
Key Words: hyperbaric oxygen therapy (HBOT), problem wounds, quality of life (QOL).
Introduction
Hyperbaric oxygen therapy (HBOT) is a relatively new addition to the medical treatment armamentarium in Taiwan (Niu, 1998; Wang, Chen, & Guo, 1998). With high doses of oxygen, numerous biochemical, cellular, and phy-siologic effects can be achieved (Petzold, Feindt, Carl, & Gams, 1999). Clinically, HBOT is used as the primary ther-apy for decompression sickness, arterial gas embolism, carbon monoxide poisoning, and as an adjunctive therapy for gas gangrene, skin and flap transplants, and chronic, non-healing wounds (Leach, Rees, & Wilmshurst, 1998; Phillips, 2005). In conditions such as edema,
vasculo-pathies, hypovolemia, or local and systemic infections, there is tissue hypoperfusion and hypoxia which reduces cellular metabolism, decreases the efficacy of body de-fense mechanisms, impedes repair of injured cells, and attenuates white blood count, bactericidal function and wound healing, resulting in the formation of a chronic, non-healing wound (Leach et al., 1998; Strauss, 2000). Clinically, the treatment for the most problematic wounds consists of antibiotics, debridement, and skin transplanta-tion, but the effects are limited; patient recovery is delayed, the hospital stay is increased in length, and the number of related tests and treatments is greater. Ultimately, the prob-lem wound becomes a chronic medical condition (Butcher,
RN, MSN, Assistant Head Nurse, Department of Nursing, Tri-Service General Hospital; *PhD, Associate Professor, Department and Graduate Institute of Psychology, National Taiwan University; **PhD, Associate Professor, Institute of Undersea and Hyperbaric, National Defense Medical Center; ***RPh, MS, Chief Pharmacist, Department of Pharmacy Practice, Tri-Service General Hospital; ****RN, PhD, Assistant Professor, School of Nursing, National Defense Medical Center; *****RN, MSN, Professor and Dean, School of Nursing & Doctoral Student, Department of Health Education, National Taiwan Normal University.
Received: January 4, 2006 Revised: June 8, 2006 Accepted: July 4, 2006
Address correspondence to: Kwua-Yun Wang, No. 161, Min-Chuan East Rd. Sec. 6, Neihu, Taipei 11490, Taiwan, ROC.
1999). With HBOT, rapid healing was observed, the wound was closed and was completely epithelialized (Petzold et al., 1999). Taking into account the differences of individ-ual patient characteristics and physiological wound indi-ces, there are many occult variables of importance in the process of wound healing, resulting in changes in lifestyle, combined with social and environmental problems. These issues, in turn, directly impact on the patient’s quality of life (QOL) (Teare & Barrett, 2002; Walshe, 1995).
In a review of the medical literature, Wunderlich, Peters, and Lavery (2000) analyzed patients with diabetes, gas gangrene, chronic osteomyelitis, necrotizing fascilitis, burns, or traumatic wounds. They found 76 publications which included patients undergoing HBOT, 49 of which involved human research, literature reviews, or case re-ports; the remainder of the publications were largely animal-based experimental studies. Most HBOT was conducted at a 2-2.8 atmosphere absolute (ATA), with an average treat-ment time of 90-120 minutes, and an average number of treatment sessions of 12-50. Collectively, the results de-monstrated that HBOT promotes wound healing in 68-95.2% of cases, clearly consistent with significant clinical efficacy. It was surmised that HBOT reduced tissue hy-poxemia, decreased the severity of the patient’s wound, augmented wound healing in problem cases, and restored health (Petzold et al., 1999).
In step with social transitions, there has been an in-creasing demand among patients for healthcare services and the quality of services provided. This has resulted in a corresponding change in the provision of medical services, not only focusing on prolongation of life, but also the QOL (Ni, 1998). Healthcare providers have recognized that they not only need to help patients survive, but they must also help patients maintain or return to an acceptable level of QOL (Belcher, 1990; Petzold et al., 1999), and moreover, enjoy a high quality standard of life (Wu & Lin, 1997). In QOL studies derived from a MEDLINE search of the ex-tant literature related to challenging wounds, whether the wounds were caused by diabetic ulcers or vascular insuffi-ciency-induced ulcers, there were no studies comparing the QOL of patients before and after HBOT. Also, as Scully (1999), Teare and Barrett (2002), and Walshe (1995), pointed out, for most patients, ulcers involving the lower extremities are not an acute, but rather a chronic condition. Lower extremity ulcers often recur and disrupt skin integ-rity, and affect patients physically and psychologically. This motivated us to evaluate the efficacy of HBOT in
improving the overall QOL of patients with problem wounds, using a QOL scale as an evaluation reference in assessing patient treatment efficacy. We have also suggested possi-ble areas of improvement for medical personnel who pro-vide continuing care (Belcher, 1990; William, 2000) so as to deliver the most suitable health education and protocols for patients at different stages of wound healing in order to elevate the patient’s overall QOL.
Methods
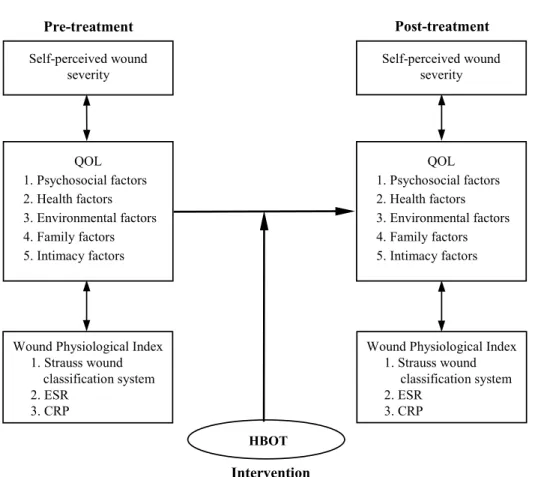
In light of the literature review, the conceptual model of this research is as follows (Figure 1). This study was a longitudinal, prospective study involving one group of subjects who were administered structured questionnaires before and after the treatment under evaluation. The sub-jects were patients with problem wounds receiving HBOT at a medical center. Hyperbaric oxygen therapy treatment is a form of therapy in which patients are placed in a sealed chamber, and 100% oxygen is supplied intermittently at pressures above 1 ATA. Oxygen pressure must be above 1.4 ATA to be of therapeutic value (Hampson, 1999; Yildiz et al., 2004). In this study, patients were placed in multi-compartmental chambers at a pressure of 2.5 ATA and a treatment time of 105-120 minutes. Selection criteria in-cluded: (1) a diagnosis of chronic and/or non-healing wounds, (2) requirement for HBOT as determined by a HBOT specialist, (3) 18 years of age or older, (4) clear consciousness and the ability to communicate, and (5) willingness to participate in the study and to complete the treatment.
This study used a two-stage purposive sampling met-hod. The first stage was a preliminary experiment, admin-istering the questionnaire to five patients with problem wounds. This stage was intended to test the reliability and validity of the questionnaire, to evaluate whether experi-mental tools were suitable for the task, to estimate the time needed to collect data from each individual, and to modify the questionnaire and study protocol to facilitate the collec-tion of data. The second stage was the formal experiment. Researchers explained the purpose of the research and the methods to be utilized to the patients, obtained written con-sent, and then collected pre-experimental data, all of which took a total of 30-40 minutes. Questionnaires were pro-vided after patients completed their treatment. A total of 15 valid questionnaires were collected. Since the sample size in this study was rather small, the central limit theorem was
applied and we confirmed to the sample recruiter was nor-mally distributed.
The basic patient characteristics collected included: sex, age, marital status, education level, religious beliefs, primary diagnosis, and the date of wound occurrence. The information collected was collated and analyzed using a minimum number of categories while still preserving sig-nificant differences.
Self-perceived wound severity was a linear scale, with values from 1-10, with 1 being ‘not serious at all’ and 10 being ‘extremely serious’. In 1980, Zederfeldt suggested that problem wounds are defined as soft tissue damage which does not achieve satisfactory healing under standard therapeutic treatments (citations from Oriani, 1998). Alternatively, a problem wound can occur second-ary to an interruption of the wound healing process, re-sulting in prolonged wound healing time. In the current study, a problem wound was considered to be soft tissue damage which did not heal after one month, with a score of less than 8 according to the Strauss wound classifica-tion system (Table 1). A distincclassifica-tion was made between
healthy and problem wounds by the differences in scoring, with a higher score corresponding to a healthier wound. The validity of this wound scoring system was 4.60 (range = 1-5), as determined by expert validity. The Cronbach’s a is used to assess the reliability of wound scoring in this study. The purpose was to understand the internal consis-tency of this scale. The value ofa is between 0 and 1. A large value means a more reliable result. In this studya is 0.83. Which means the results obtained by using the wound scoring was reliable.
The erythrocytes sedimentation rate (ESR) and C-reactive protein (CRP) level of the patients were measured both before and after receiving hyperbaric oxygen. The ESR is a measure of the acute phase response, with a nor-mal range of 10-20 mm/hr (He, 1992). The nornor-mal range for CRP is less than 0.8 mg/dL, with a value above the nor-mal range consistent with an inflammatory reaction (Qi & Lee, 1998).
The current study relied upon the version of QOL in-dicators as developed by Ferrans and Powers (1985), and then translated into Chinese by Liu (1993). This QOL was Self-perceived wound severity QOL 1. Psychosocial factors 2. Health factors 3. Environmental factors 4. Family factors 5. Intimacy factors
Wound Physiological Index 1. Strauss wound classification system 2. ESR 3. CRP Self-perceived wound severity QOL 1. Psychosocial factors 2. Health factors 3. Environmental factors 4. Family factors 5. Intimacy factors
Wound Physiological Index 1. Strauss wound classification system 2. ESR 3. CRP HBOT Pre-treatment Post-treatment Intervention
Figure 1. Conceptual Model: Comparison of data before and after hyperbaric oxygen therapy. Note. QOL = quality of life; ESR = erythrocytes sedimentation rate; CRP = C-reactive protein; HBOT = hyperbaric oxygen therapy.
developed to measure the quality of life of healthy individ-uals, as well as those who are experiencing an illness. It includes an individual’s satisfaction with various aspects of life and the perceived importance of those features (Ferrans & Powers, 1992). In the current study, QOL was considered to be the state of contentment in a conscious individual due to their satisfaction in physiological, psy-chological, social, and spiritual aspects of life. After input from experts and subsequent modifications, a total of 37 questions were selected and divided into five dimensions: (1) social psychology, which probed an individual’s psy-chological response to life and social interactions, (2) he-alth, which was comprised of the hehe-alth, life expectancy, stress, and healthcare conditions of the patient and the patient’s family, (3) environment, consisting of the pa-tient’s personal living conditions and the general environ-mental conditions of Taiwan, (4) intimacy, including the relationship and intimacy between the patient and their spouse, and overall family happiness, and (5) family, in-volving the relationships between the patient and his/her siblings and the patient’s satisfaction with their children. It is a six-point scale (i.e., zero to six), ranging from ‘not applicable’ (assigned a value of zero) to ‘very important’ or ‘very satisfied’ (assigned a value of six). The QOL score was represented by the weighted values of responses of the patients’ satisfaction of life and their perceived relative importance. The lowest possible score, therefore, was zero and the highest possible score was 30. The higher the score, the higher the QOL. The reliability of this score was calcu-lated by Cronbach’sa coefficient, which indicated the internal consistency. The overalla coefficient was .96, and thea coefficient of the five questionnaire dimensions had
values of .67-.93. Validity was determined by expert valid-ity, and the expert validity of this scoring system was 4.60.
After numerically labeling the data, descriptive and inferential statistical analyses were performed with SPSS/ PC10.0 software. Inferential analyses used were the paired
t-test to analyze the self-perceived wound severity, Strauss
classification system score, ESR, CRP, QOL data before and after HBOT and the Pearson product-moment correlation to correlate self-perceived wound severity, Strauss classification system score, ESR, and CRP data with QOL. The value of p was set to be less than .05 for the significance level of the test.
Results
Some significant trends were noted amongst the 15 research subjects. There were 11 males (73.33%), nine were under the age of 68 years (60%), seven had completed a primary or junior high school education (46.67%), 13 were married (86.67%), 12 practiced a specific religious belief (80%), 11 had a primary diagnosis of diabetic foot ulcers (73.33%), seven had a wound duration of 3-6 mon-ths (46.67%), and 13 had wound surgery in conjunction with HBOT (86.67%).
The self-perceived wound severity in patients after HBOT was statistically lower than before HBOT (1.93± 1.33 vs 8.57± 2.21; p < .001). In accordance with the St-rauss wound classification system, appearance, size, depth, presence or absence of infection, and perfusion status were used as a basis for evaluation. The wound score in patients after HBOT was higher than that before HBOT (8.80± 1.01 vs 5.33± 1.58), with a statistically significant differ-ence before and after treatment (p < .001).
Table 1.
Strauss Wound Classification Scoring System
Scoring*
Criteria 2 points* 1 point* 0 point*
Appearance (wound base) Red Yellow or white Black
Size Thumb tip or smaller Between thumb tip and fist Larger than fist Depth (deepest tissue exposed) Skin or subcutaneous Muscle or tendon Bone or joint Infection None or superficial
contamination
Cellulitis Septic+
Perfusion Warm, pink, rapid capillary refill, palpable pulse
Cool, pale, sluggish capillary refill, and/or Doppler-detectable pulse
Cold, cyanotic, no capillary refill, and/or no pulse Note. *Half points may be used when findings are intermediate between two scores or mixed (a wound appearance that is partially vascularized and partially covered with a fibrinous exudate).+Findings associated with sepsis include fever, chills, leukocytosis, and/or uncontrolled blood glucose level.
The ESR in patients before receiving HBOT (39.25± 21.90 mm/hr) was higher than that after HBOT (34.67± 16.20 mm/hr), but the difference was not statistically sig-nificant (p > .05). The CRP level before HBOT (3.76± 5.87 mg/dL) was significantly higher than that after HBOT (0.38± 0.37 mg/dL; p < .05).
Before HBOT, the average score for overall QOL was 17.57± 5.95, indicating a moderate level of QOL among the patients. Of the five main QOL dimensions, ‘intimacy’ had the highest score (24.93 ± 6.27), and ‘health’ had the lowest score (13.61± 6.74). Of the 37 minor categories, the five highest-scoring categories, in descending order, were ‘family happiness’, ‘children’, ‘health of the family members’, ‘emotional support’, and ‘home’. In contrast, the five lowest-scoring categories, in descending order, were ‘health’, ‘free from pain or physi-cal discomfort’, ‘having control over what happens in life’, ‘having the ability to do something or being able to walk around’, and ‘able to travel during the holidays’. After HBOT, the average score for overall QOL was 21.92± 4.48, indicating an upper-middle level of QOL among the patients. Of the five main QOL dimensions, ‘intimacy’ had the highest score (25.36± 5.52) and ‘psy-chosocial’ ranked the lowest (20.40± 7.25). Of the 37 minor categories, the five highest-scoring categories, in descending order, were ‘medical care’, ‘family happi-ness’, ‘health’, ‘children’, and ‘free from pain or physical discomfort’. The five lowest-scoring categories, in des-cending order, were ‘influence over local or central gov-ernments’, ‘having a job’, ‘work’, ‘pressure and stress’, and ‘overall situation in Taiwan’. There was a statistically significant difference in overall QOL before and after HBOT, as based on differences in the psychosocial and health dimensions (Table 2).
As shown in Table 3, the less severe patients per-ceived their wounds to be after HBOT, the higher their
QOL. Moreover, patients who had a higher Strauss clas-sification system score after HBOT had a higher QOL (Table 4).
Table 3.
Correlation Analysis Between Self-Perceived Wound Severity and QOL in Patients With Problem Wounds Before and After HBOT (r) (N = 15)
QOL
Item Pre-treatment Post-treatment
Self-Perceived Wound Severity
Pre-treatment -0.45
-Post-treatment - -0.80**
Note. QOL = quality of life; HBOT = hyperbaric oxygen therapy. **p < .01.
Table 4.
Correlation Analysis Between Wound Physiological Index (Strauss Wound Classification System) and QOL in Patients With Problem Wounds Before and After HBOT (r) (N = 15)
QOL
Item Pre-treatment Post-treatment
Strauss Wound Classification System Pre-treatment -0.48 -Post-treatment - -000.82** ESR Pre-treatment -0.39 -Post-treatment - -0.11 CRP Pre-treatment -0.39 -Post-treatment - -0.42
Note. QOL = quality of life; HBOT = hyperbaric oxygen therapy; ESR = erythrocytes sedimentation rate; CRP = C-reactive protein. **p < .01.
Table 2.
Differences in Overall Patient QOL Before and After HBOT
Hyperbaric Oxygen Therapy (HBOT)
Categories Pre-treatment Post-treatment t p
Overall 17.56 20.75 -5.74 .000 Social psychology 15.85 19.63 -3.60 .003 Environment 19.99 20.41 -0.72 .484 Health 13.61 23.90 -6.81 .000 Family 22.54 22.69 -1.68 .116 Intimacy 24.93 25.36 -1.47 .165
Discussion
The overall QOL of patients was 17.56 points before HBOT. Of the five dimensions, ‘intimacy’ had the highest score and ‘health’ had the lowest. After HBOT, the overall QOL of patients was 20.75 points; the ‘intimacy’ dimen-sion had the highest score and ‘psychosocial’ had the low-est score. In patients with problem wounds after HBOT, there was a significant negative correlation between QOL and self-perceived wound severity, and there was a positive correlation between QOL and the Strauss wound classifi-cation system score.
Within the five dimensions measuring patient QOL before and after HBOT, the ‘intimacy’ dimension pertained to family happiness, and the relationship and intimacy with the spouse. When not requiring HBOT, patients with prob-lem wounds tended not to appreciate the care provided by the spouse and family members. However, when the wound did not heal and interfered with daily activities, and further medical treatment was needed, they appreciated the love and care they received from their family members. This is likely to be because HBOT is neither a well known nor widely accepted treatment in the medical field (Wang et al., 1998). Also, a course of HBOT requires continuous treat-ment for two weeks or longer. Because of the difficulties in traveling to and from hospital and also the enormous time consumed in the treatment process, family and spousal as-sistance and their psychological support were needed to encourage the patients to persevere with the treatment for an extended period of time. Therefore, the ‘intimacy’ di-mension had the highest score. In this study, the ‘health’ dimension was related to aspects such as patient health, medical care, and freedom from pain or physical discom-fort. Scully (1999) and Walshe (1995) pointed out that due to delayed wound healing, compounded by complications (e.g., infection or septicemia) aggravating the underlying condition, longer treatment time was required, which re-sulted in patients losing confidence in medical care or wound healing. If unbearable pain was also present, it di-rectly threatened the patient, and therefore this dimension had the lowest score in patients before receiving HBOT. In this study, the ‘psychosocial’ dimension mainly disclosed the psychological reaction of patients with regard to their living conditions and social interactions. This dimension scored the lowest in patients after HBOT, because patients would like to walk around after their foot wounds had healed, but since the healing was fresh, most patients
indi-cated a need for further rest before they could walk confi-dently. There was a partial loss of control, so that compared with other dimensions, this dimension received the lowest score.
Before undergoing HBOT, regardless of the QOL score, every patient perceived their wound as very serious. Although the relationship between self-perceived wound severity and QOL before HBOT was not statistically sig-nificant, there was a widespread belief in wound improve-ment after HBOT. When the wound was no longer perce-ived to be severe, there was a statistically significant nega-tive correlation between self-perceived wound severity and QOL after treatment. This finding affirmed the conclusion of Chen (2000) on 17 diabetic patients with early foot ul-cers, in which there was an improvement in symptoms after HBOT according to the patients. It is known from the med-ical literature pertaining to patients with foot ulcers or os-teomyelitis receiving HBOT that patients are distressed by their condition, and that if they can increase their ability to control their condition or reduce pain, there will be an increase in the degree of life satisfaction (Blixen & Kippes, 1999). As stated by Bertero and Ek (1993), QOL is a per-sonal measurement, and different disease severity impacts on the QOL of different individuals in different ways.
Problem wound sickness in accepts before the HBOT, no matter the QOL scores points the height, each problem wound on the Strauss wound classification scoring system, all belongs to the difficult wound or the non-hope wound. The serum test of ESR and CRP, mean value all indicated has serious or the slight infection existence, The result were not reveal the correlation existence with the life qual-ity. It is because problem wound sickness in the physiologi-cal data obviously all indicated has the infection existence, but each person’s aware degree is different. Some people thought extremely affects the life, but others not. Therefore was no correlation with the life quality.
There was a positive correlation between the Strauss wound classification score and QOL, indicating that HBOT has the advantage of reducing wound size and decreasing amputation rates after therapy (Simmons, 1999; Wu, Li, & Lin, 2000). Wang (1994) pointed out that in problematic wounds, such as chronic ulcers, diabetic foot ulcers, and ischemic skin flaps, the vascular supply of the wound is in adequate, so HBOT is needed to enhance wound healing. In discussing clinical applications of HBOT, Wang et al. (1998) suggested that in managing tissue hypoperfusion, non-healing or problem wounds, HBOT was of significant
therapeutic value. Dong and Guo (1995) summarized the application of HBOT in plastic surgery, showing that they aided wound healing, especially in cases of delayed heal-ing. This line of research indicated that in such patients, their wounds not only healed subjectively, but pathophy-siological examination results also showed that infection was under control, and the wound condition improved sig-nificantly. Patients felt their lives were no longer affected by their wounds. Evidently, the healthier the wound, the higher the patient’s QOL.
Suggestions and Limitations
From the results of this study, in practical nursing care, ‘health’ and ‘psychosocial’ had the lowest points of the five QOL dimensions before and after HBOT. These are the areas to be strengthened for nursing personnel in educating patients with difficult wounds receiving HBOT in the future. Due to restrictions in time and manpower, we only examined the differences which existed before HBOT and immediately after therapy. We found significant differ-ences in QOL before and after HBOT, and we suggest that future research should continue to follow up patients’ QOL six months and one year after HBOT. Also, due to payment issues in the National Health Insurance system, we only collected data pre-experimentally using a single-group, pretest-posttest method from patients with problem wounds in one hospital in northern Taiwan. The number of subjects was small and may not be representative of the general population. There were many independent variables which we wished to examine. The subjects themselves were spe-cial cases, so the statistical significance of results was pro-bably affected. Future related research should cover the entire northern, central, and southern areas, and compare the QOL in patients with problem wounds of different cha-racteristics before and after HBOT. During the study, it was determined that factors such as extent of social support of the patient, degree of distress caused by the disease, changes in self-image of patients with problem wounds, and the stresses and coping behaviors resulting from the disease all affected the QOL of patients undergoing HBOT. Future research should include the above-mentioned vari-ables in their analyses.
Acknowledgments
We are grateful to Professors Liu and Farrans and Dr. Strauss for providing the relevant scales used in this study.
References
Belcher, A. E. (1990). Nurses: Workhorses or wondawork-ers? Journal of Pediatric Oncology Nursing, 7(2), 65-66.
Bertero, C., & Ek, A. (1993). Quality of life of adults with acute leukemia. Journal of Advanced Nursing, 18(9), 1346-1353.
Blixen, C. E., & Kippes, C. (1999). Depression, social sup-port, and quality of life in older adults with osteoarth-ritis. Image: Journal of Nursing Scholarship, 31(3), 221-226.
Butcher, M. (1999). A systematic approach to complex wounds.
Nursing Standard, 13(29), 58, 61-62, 64.
Chen, S. B. (2000). The clinical role of hyperbaric oxygen in
treating early diabetic feet. Unpublished master’s thesis,
National Defense Medical Center Undersea and Hyper-baric Medicine Research Institute, Taipei.
Dong, H. C., & Guo, N. C. (1995). The application of hy-perbaric oxygen therapy in plastic surgery-wound heal-ing. Veterans General Hospital Nursing, 12(1), 12-18. Ferrans, C. E., & Powers, M. J. (1985). Quality of life index: Development and psychometric properties. Advance in
Nursing Science, 8(1), 15-24.
Ferrans, C. E., & Powers, M. J. (1992). Psychometric assess-ment of the quality of life index. Research in Nursing &
Health, 15(1), 29-38.
Hampson, N. B. (1999). Hyperbaric oxygen therapy: 1999
committee report. Kensington, MD: Undersea and
Hy-perbaric Medical Society.
He, M. F. (1992). Clinical physiology. Taipei: Hochi. Leach, R. M., Rees, P. J., & Wilmshurst, P. (1998). ABC of
oxygen: Hyperbaric oxygen therapy. British Medical
Jour-nal, 317(7166), 1140-1143.
Liu, X. O. (1993). Discussions on the psychometrics of pa-tient family quality of life. Journal of Nursing Research,
1(2), 127-136.
Ni, L. J. (1998). Discussions on the quality of life and related
factors in medical and surgical ward nursing personnel.
Unpublished master’s thesis, National Taiwan Univer-sity Medical School Nursing Research Institute, Taipei. Niu, K. C. (1998). Clinical applications of hyperbaric oxygen
therapy. In X. Z. Wang (Ed.), Clinical medicine and
sur-gery (pp. 1323-1351). Taipei: Hochi.
Oriani, G. (1998). HBO and wound healing: The current “state of the art”. In D. J. Bakker, J. C. Le Pechon, & A. Marroni (Eds.), Hyperbaric oxygen: Wound healing
sa-fety and cost-effectiveness (pp. 83-103). Flagstaff, AZ:
Petzold, T., Feindt, P. R., Carl, U. M., & Gams, E. (1999). Hyperbaric oxygen therapy in deep sternal wound infec-tion after heart transplantainfec-tion. Chest, 115(5), 1455-1458.
Phillips, J. C. (2005). Understanding hyperbaric oxygen the-rapy and its use in the treatment of compromised skin grafts and flaps. Plastic Surgical Nursing, 25(2), 72-80. Qi, W. M., & Lee, W. H. (1998). C-reactive protein. Medical
Digest, 27(4), 211-212.
Scully, C. (1999). Assessing leg ulcers. Nursing Times, 95(27), 59, 62, 65.
Simmons, S. (1999). Help is in the air. Nursing Times, 95(11), 74, 77-78.
Strauss, M. B. (2000). Problem wounds, practical solution.
The Journal of Musculoskeletal Medicine, 17, 267-283.
Teare, J., & Barrett, C. (2002). Using quality of life assess-ment in wound care. Nursing Standard, 17(6), 59-68. Walshe, C. (1995). Living with a venous leg ulcer: A
descrip-tive study of patients’ experiences. Journal of Advanced
Nursing, 22(6), 1092-1100.
Wang, J. H. (1994). Hyperbaric oxygen therapy. Clinical
Me-dicine, 34(1), 1-9.
Wang, J. R., Chen, P. R., & Guo, S. D. (1998). Clinical appli-cations of hyperbaric oxygen therapy. Clinics in Chest
Medicine, 13(4), 249-257.
William, H. P. (2000). Understanding and assessing diabetes-specific quality of life. Diabetes Spectrum, 13(1), 36-41. Wu, J. Z., & Lin, C. J. (1997). Concept analysis of the ‘quality of life’ idea. Journal of Clinical Nursing, 14(1), 102-106. Wu, E. C., Li, C. H., & Lin, T. F. (2000). Use of hyperbaric
oxygen therapy in patient with diabetic food. Medical
Digest, 30(3), 251-253.
Wunderlich, R. P., Peters, E. J. G., & Lavery, L. A. (2000). Systemic hyperbaric oxygen therapy. Diabetes Care,
23(10), 1551-1555.
Yildiz, S., Uluutku, H., Gunay, A., Yildirim, I., Yildirim, S., & Gurbuz, A. K. (2004). The effect of hyperbaric oxy-gen therapy on the adverse effects of octreotide on wound healing. European Journal of Gastroenterology &