1 Title page
Full title: Pilot Scheme of Health Policy in Stroke Adjuvant Acupuncture Therapy
(HPSAAT) for Acute and Subacute Ischemic Stroke in Taiwan Word count for text: 2512
Number of table: 2
Number of figure: 2
Key words: ischemic stroke, acute, subacute, acupuncture, national health programs,
complementary therapies Authors and affiliation:
Yi-Chia Wei, MD
Department of Neurology, Chang Gung Memorial Hospital at Keelung, Taiwan [email protected]
Mao-Feng Sun, MD, PhD
Department of Acupuncture, China Medical University Hospital, Taichung, Taiwan
School of Chinese Medicine, China Medical University, Taichung, Taiwan [email protected]
Ku-Chou Chang, MD
2
Center, Chang Gung University College of Medicine, Kaohsiung, Taiwan [email protected]
Chee-Jen Chang, PhD
Graduate Institute of Clinical Medical Sciences, Chang Gung University, Taoyuan, Taiwan
Clinical Informatics and Medical Statistics Research Center, Chang Gung University, Taoyuan, Taiwan
[email protected] Yu-Chiang Hung, MD, PhD
Department of Traditional Chinese Medicine, Chang Gung Memorial Hospital - Kaohsiung Medical Center, Chang Gung University College of Medicine, Kaohsiung, Taiwan
[email protected] Yu-Jr Lin, MSc
Resource Center for Clinical Research, Chang Gung Memorial Hospital at Linkou, Taiwan
[email protected] Hsien-Hsueh Elley Chiu, MD
3
Kaohsiung Medical Center, Chang Gung University College of Medicine, Kaohsiung, Taiwan
[email protected] Correspondence:
Corresponding author: Hsien-Hsueh Elley Chiu
Address: No.123, Dapi Rd., Niaosong Township, Kaohsiung County 83301, Taiwan
Fax number: +886-7-7317123 ext 2332
Phone number: (O)+886-7-7317123 ext 2332 (M)+886-968376593 E-mail address: [email protected]
4 Abstract
To reduce the health care burden of strokes, the Taiwan Department of Health launched the Pilot Scheme of the Health Policy in Stroke Adjuvant Acupuncture Therapy (HPSAAT) in 2006. This cross-sectional, hospital-based, match-controlled study at Chang Gung Memorial Hospital-Kaohsiung Medical Center during 2006~2008 retrospectively evaluated the clinical characteristics of acute and subacute ischemic stroke patients who electively joined the HPSAAT. The study also evaluated the safety and clinical benefits of adjuvant acupuncture in treating acute and subacute ischemic stroke patients.
Twenty-six HPSAAT participants and 52 age-sex matched random controls were enrolled. The stroke baseline of the HPSAAT participants was more severe than the non-HPSAAT controls. Although the stroke severity closely correlates to mortality and comorbidity, this study noted no significant complications in the HPSAAT participants during the acupuncture treatment course. Adjuvant acupuncture was considered safe at the acute and subacute stages of ischemic stroke. Due to uneven baseline severity, the clinical benefits in reducing neurological deficits and functional recovery were not concluded in this study.
5 Introduction
As one of the leading causes of death, strokes contribute to a worldwide health care burden (1, 2). Acupuncture has long been applied in treating stroke patients and has thus been recommended by the World Health Organization (4). The National Health Insurance (NHI) is the social insurance that has covered the medical expenses of over 99 % of 23.0 million Taiwanese citizens since 1995 (5–7). In Taiwan, acupuncture prevailed in one-fifth of NHI beneficiaries (3). Aiming to improve the health care of stroke patients, the Department of Health launched an NHI-sponsored national project in 2006, namely the Pilot Scheme of the Health Policy in Stroke Adjuvant Acupuncture Therapy (HPSAAT). The HPSAAT promotes integration of traditional Chinese medicine (TCM) in conventional stroke care. In 2010, the HPSAAT has been conducting in 27 medical centers and local hospitals under an annual budget of 2.7 million US dollars. Patients with newly onset stroke (during the past year) receive support and elective acupuncture. Both inpatient treatment and outpatient clinic visits are covered.
Along the clinical course of ischemic stroke, the most important period of recovery is at the acute and subacute stage (8). In this study, we sought to identify the characteristics of acute and subacute stroke patients who electively chose to participate in the HPSAAT. We also aimed to evaluate the safety of adjuvant
6 acupuncture in stroke inpatient care.
Among patients with stroke, the major cause of death is from medical complications (9) that mostlydevelop within the first 6 weeks after stroke onset (10). The incident rate of medical complications increases with the baseline severity of stroke. A higher score of the National Institution of Health Stroke Scale (NIHSS) (11, 12) or a higher dependency at stroke onset (10) is correlated to an increase of medical complications. Among all medical complications during acute and subacute stroke, infection is the most common medical complication (13) and is an independent predictor of mortality and poor functional outcome (9, 14, 15). The high prevalence of post-stroke infections, as well as other post-CNS (central nervous system) injury infections, has been supposed to be the consequence of CNS immunodepression with imbalanced subsets of helper T cells (16, 17). In acupuncture theory, correcting imbalances is the ultimate goal of needling. Both pro-inflammatory and inflammatory effects have been observed in acupuncture studies (18). The post-acupuncture sequential change of peripheral blood leukocyte subpopulation and cytokines reveals immune-boosting effects (19, 20). Based on the previous findings, we hypothesize that acupuncture has the potential to correct CNS injury-induced immunodepression and reduce the infectious complications of stroke patients. In this study, we attempted to use age-sex matched control to evaluate the clinical benefits of adjuvant
7
acupuncture in reducing medical complications in HPSAAT participants.
The other major burden in stroke care involves neurological deficits and functional impairment. The acute and subacute stages account for the golden time of stroke recovery (8). The plasticity of the brain significantly affects stroke recovery (21). In recent systematic reviews of acupuncture in acute ischemic stroke, potential therapeutic effects have been noticed (22, 23). Acupuncture increases regional cerebral blood flow in the hypoperfusion area surrounding the ischemic core and in the sensorimotor area of the affected and unaffected hemisphere of the brain in ischemic stroke patients (24). A functional MRI study confirmed that acupuncture elicits higher signals in the somatosensory area of post-stroke brains (25). In this study, we compared the neurological improvement between the HPSAAT participants and age-sex matched controls.
8 Method
Study design and patients
This research involved a cross-sectional, hospital-based, matched-control study conducted at Chang Gung Memorial Hospital-Kaohsiung Medical Center (KCGMH). The study was approved by the institutional review board of KCGMH. Acute and subacute stroke patients admitted to the neurology ward and neurology intensive care unit (NICU) from 1 July 2006 to 30 Jun 2008 were assessed for eligibility. Ischemic stroke is defined by ICD-9 code 434. Only admissions for initial management of acute and subacute ischemic stroke were included. Re-admissions of a single patient during the investigation period were excluded. Among ischemic stroke patients, some patients electively joined the HPSAAT to receive adjuvant acupuncture. Occasionally, families of patients with cognitive impairment made the decision regarding HPSAAT participation. After patients began participating in the HPSAAT, TCM doctors received a consultation sheet, visited the HPSAAT participants, and began the treatment course.
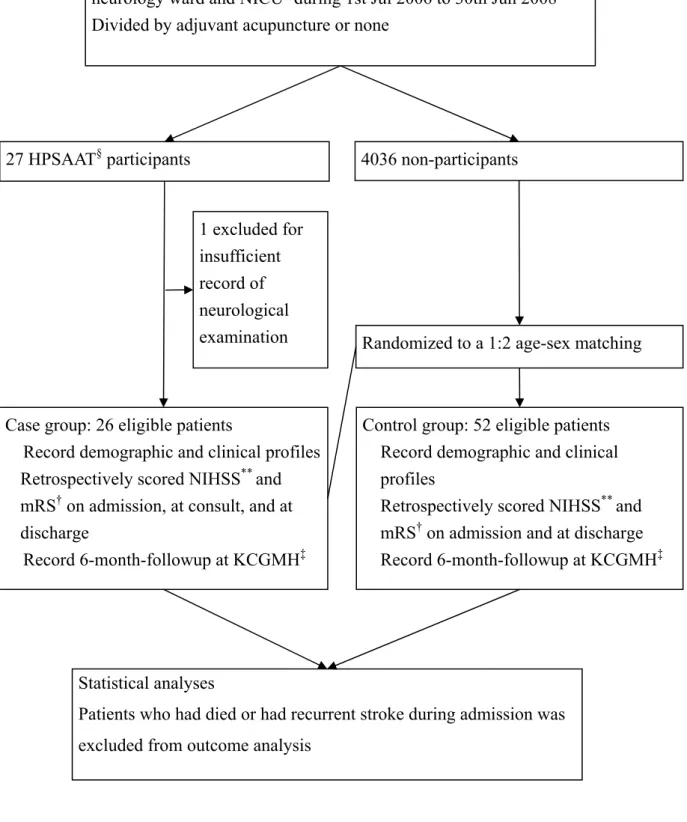
In this study, HPSAAT participants were allocated to case groups. Matched control group members were randomly selected among the non-HPSAAT participants by 1:2 age-sex matching (26). Those cases whose medical records did not present sufficient neurological descriptions for NIHSS scoring were excluded. The enrolled cases were retrieved for full chart review of the admission course and 6-month period of post-stroke follow-up at KCGMH (Figure 1).
9 Procedures
All patients received concomitant stroke care in the neurology ward and/or in NICU. In addition, experienced TCM doctors visited the HPSAAT participants three times per week and performed acupuncture treatment. The acupuncture point selection was determined by doctor clinical evaluation in accordance with TCM principles. After manual acupuncture, the disposable stainless needles were retained for 15 minutes. When clinical conditions deteriorated or infectious conditions occurred, doctors of both neurology and TCM could evaluate the patients and decide if acupuncture should be administered.
Data Collection
The demographic profiles recorded age, sex, and body mass index. The clinical profile regarding strokes recorded stroke types, lesion sites, previous strokes, and risk factors. The population profile recorded patient sources, dispositions, and timescale of treatment. The medical resource profile recorded thrombolytic therapy (r-tPA), NICU stay, craniectomy or shunt implantation, mechanical ventilation, bedside physical therapy, and length of stay. Confounding factors of outcome were assessed by a baseline NIHSS (27) and a baseline modified Rankin Scale (mRS) (28). We retrospectively scored the NIHSS (29, 30) and mRS by an independent clinical investigator certified by the American Heart Association professional education center (31).
10
stroke-in-evolution (32). Medical complications during admission were evaluated by urinary tract infection, pneumonia, and cellulitis (13). Also the stress events represented by gastrointestinal (GI) bleeding episodes, hemodynamic stability evaluated by vital sign at 09:00 a.m. of the day next to admission day and of the day before discharge day. Significant adverse events of acupuncture were reviewed (33). We also traced patient admission records and outpatient visits at KCGMH for a 6-month period. Patients who had died or had a recurrent stroke during admission were separated from outcome analysis.
Statistical analysis
Categorical data was expressed by frequency (percentage) and was examined by a chi-squared test. Continuous data were expressed by mean (standard deviation) and were examined by an independent t-test. A p-value <0.05 in a 2-tailed test was considered to be statistically significant. Data were analyzed using a commercial software program, SPSS version 17.0 for Windows; SPSS Inc.
Funding
This study was supported by the Chung Gung Research Project, CMRPG880551. The funding source had no role in the study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author and the first author had full access to all data in the study and had final responsibility for the decision to submit the paper for publication.
11 Results
This study involved 273 HPSAAT participants, most of them were in the stroke recovery stage and admitted in rehabilitation wards. Only 27 participants with acute and subacute ischemic stroke were eligible for the case group. One case was further excluded due to insufficient neurological examination records for retrospective NIHSS scoring, leaving 26 participants in the case group. Fifty-two age-sex matched controls were randomly selected from 4,036 acute and subacute ischemic stroke patients who did not participate in the HPSAAT but received conventional treatment indiscriminately (Figure 1).
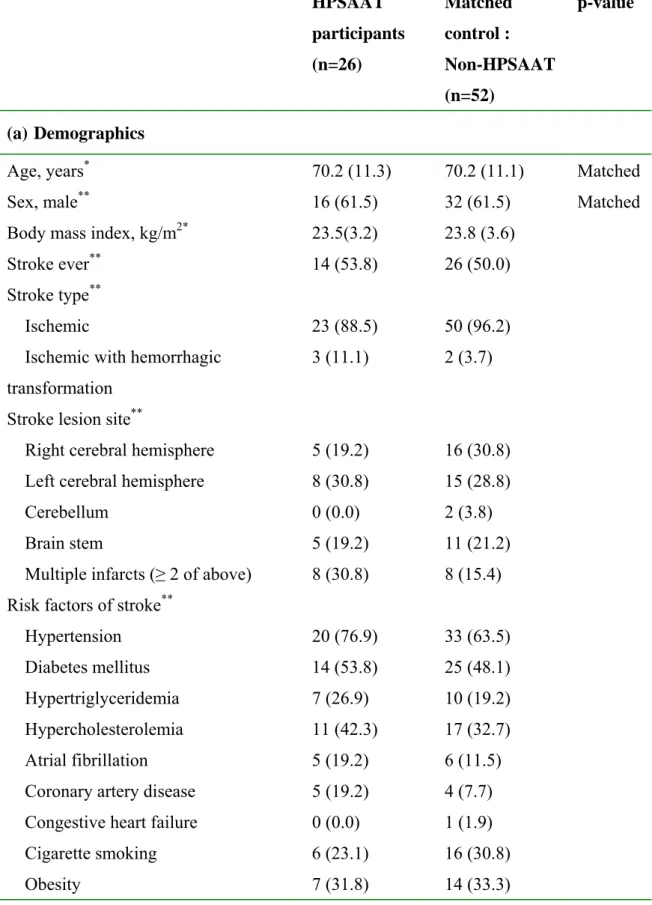
The characteristic profile of the HPSAAT participants and age-sex matched non-HPSAAT controls showed no difference in demographics, stroke type (Table 1a), or patient source (Table 1b). However, the HPSAAT participants seemed to have longer treatment courses, including length of stay in NICU, in the neurology ward, and in total (32.9±21.9:13.8±16.1 days, p<0.001). Compared to the non-HPSAAT controls, the HPSAAT participants tended to stay in health care institutions after discharge from the neurology ward and/or NICU, including the rehabilitation ward, TCM ward, and long-term care units (Table 1b). Bedside physical therapy was more prevalently applied to the HPSAAT participants (92.3 %:53.8 %, p=0.001; Table 1c).
The HPSAAT participants in the neurology ward and NICU started adjuvant acupuncture an average of 17.7±14.4 days after stroke onset and continued the treatment
12
course for 17.4±16.2 days with 6.7±6.4 acupuncture sessions (Table 1b). The safety of acupuncture was evaluated in a detailed chart review. No vital sign instability was noted among the HPSAAT participants during acupuncture. The baseline vital sign on admission was not significantly different between groups; whereas, the HPSAAT participants presented lower diastolic blood pressure (76.8±8.5:82.1±9.7 mmHg, p<0.05), lower mean arterial pressure (95.6±8.9:100.7±10.7 mmHg, p<0.05), and faster heart rate (79.1±8.1:73.7±7.2 beat per minute, p<0.01) than the non-HPSAAT controls. The adverse event survey revealed no needle sickness. In one participant, left-arm cellulitis developed 8 days after acupuncture initiation (cause undetermined). An intravenous antibiotic was administered and the acupuncture treatment was uninterrupted and completed until the patient was discharged home. Regarding another participant who had begun acupuncture treatment in the neurology ward, the acupuncture treatment was interrupted after two sessions (7 days) of treatment because of sudden collapse and admission to NICU. The other 24 HPSAAT participants completed the acupuncture treatment course smoothly during the stay in the neurology ward and/or NICU.
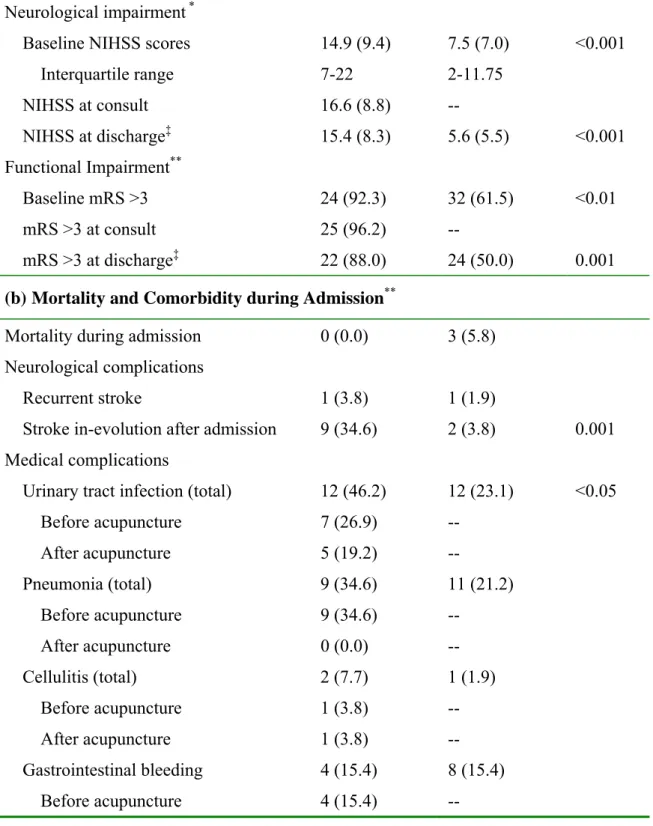
The mortality and comorbidity analysis began from a baseline comparison. The baseline NIHSS was higher on average (14.9±9.4:7.5±7.0, p<0.001; Table 2a) and was skewed more to the left in distribution (Figure 2a) among the HPSAAT participants than that of the non-HPSAAT controls. The baseline mRS of the HPSAAT participants
13
was also more severe than that of the non-HPSAAT controls (dependent as mRS>3 in 92.3 %: 61.5 %, p<0.01), but was distributed similarly (Figure 2b). Three enrolled cases expired during admission. All mortalities occurred in the control group and were caused by severe infection with septic shock. A comparison of neurological and medical complications discovered more stroke-in-evolution (34.6 %:3.8 %, p=0.001) and urinary tract infection (46.2 %:23.1 %, p<0.05) in the HPSAAT participants than in the non-HPSAAT controls during stays in the neurology ward and/or NICU. However, more urinary tract infections occurred before initiating acupuncture (Table 2b). No difference was noted in the occurrences of recurrent stroke, pneumonia, cellulitis, or GI bleeding. In the 6-month follow up period, the HPSAAT participants tended to maintain regular outpatient visits to the rehabilitation department (20.0 %:2.1 %, p<0.05) and acupuncture department (32.0 %:0.0 %, p<0.001). Approximately seventy percent of cases in both groups continued following up in the neurology department for at least 6 months after stroke onset.
14 Discussion
In this study, the major finding, but also the major limitation, was the uneven baseline severity between the HPSAAT participants and the age-sex matched non-HPSAAT controls. The acute and subacute ischemic stroke patient with severe neurological impairment and significantly functional limitations was prone to join the HPSAAT for adjuvant acupuncture in addition to conventional treatment. This finding indicated the desire for major ischemic stroke patients and their families to pursue satisfying treatment modalities or a combination of treatment modalities. This finding also indicated that the developmental principal of acupuncture in treating ischemic stroke should be emphasized on moderate to severe patients.
However, the baseline discrepancy limited the effective comparison of neurological and functional outcomes. The alternative solution may come from data mining in the Chang Gung Stroke Registry Database, which includes clinical data of all stroke patients admitted to the four branches of Chang Gung Memorial Hospital since 2008. Searching by the NIHSS on admission could find that the baseline equaled populations in the database.
The varied duration of stroke onset to acupuncture treatment (17.7±14.4 days) and varied duration of acupuncture treatment (17.4±16.2 days) among the HPSAAT participants also limited the comparison of benefits from adjuvant acupuncture in ischemic stroke. For more accurate generalization and more effective comparison, a
15 randomized control trial is required.
Since the 1990s, the efficacy and effectiveness of acupuncture for acute and subacute stroke has been evaluated by many research groups. Although some study designs have been limited by the strength of evidence, systemic reviews revealed the potential benefits of acupuncture to patients with acute and subacute strokes (22, 23). The HPSAAT is the first public health policy-modifying project to include acupuncture in stroke care. Previous evidence has suggested that the worse the baseline is, the worse the outcomes are. Moderate to severe strokes had poorer outcomes (34, 35), greater demand of long-term care (36, 37), and higher expense of medical costs (38). The acute and subacute stages constitute the golden recovery period for ischemic stroke. From this study, we found that major ischemic stroke patients tended to choose adjuvant acupuncture in the acute and subacute stages. Future studies must clarify whether or not the HPSAAT reduced the financial burden. Moreover, the baseline severity also correlated to the increased post-stroke infections (12). In this study, a higher rate of urinary tract infection of the HPSAAT participants, but not of pneumonia or GI bleeding, was noted. The infections that occurred after starting acupuncture treatment did not seem significantly increased. Therefore, in addition to improving neurological impairment or functional recovery, acupuncture may play a role in eliminating medical complications of stroke. The immune-boosting potentials of acupuncture in modulating CNS injury-induced immunodepression of acute and subacute stroke is still worthy of
16 further investigation.
The 6-month follow up period revealed favorable compliance of the HPSAAT participants to continue acupuncture treatment after discharge. The needs of long-term functional recovery and the selection of acupuncture as a treatment modality was noticed in one-third of the HPSAAT participants.
17 Conclusion
This cross-sectional study analyzed data from a single medical center to depict a brief summary of the HPSAAT in Taiwan. Adjuvant acupuncture care is a safe modality in the acute and subacute stages of ischemic stroke. Ischemic stroke patients with a severe baseline tended to participate in the HPSAAT. To validate the clinical benefits of adjuvant acupuncture care in acute and subacute ischemic stroke, a baseline equaled randomized control trial is warranted.
18 Statement of Contribution
We state the contribution of Yi-Chia Wei MD in data acquirement, data analysis, and manuscript drafting, Mao-Feng Sun MD/PhD in HPSAAT project supervision, Ku-Chou Chang MD in data acquiring and study supervision, Chee-Jen Chang PhD in study design, Yu-Chiang Hong MD/PhD in supervision of this study, Yu-Jr Lin MSc in performing statistical analysis, and Hsien-Hsueh Elley Chiu MD in conducting HPSAAT, conceiving and design the research, analyzing and interpreting the data, and making critical revision of the manuscript.
Acknowledgements
The authors give thanks to the Taiwan Traditional Chinese Medicine Association for providing information of HPSAAT. We acknowledge the contribution of Hen-Hong Chang, MD, PhD, and Sheng-Teng Huang, MD, PhD, in the administration support of this study, and Jer-Ming Sheen, MD, Cheng-Nan Lu, MD, Guo-Wei Bi, MD, and Wu-Long Hu, MD, in treating the HPSAAT patients in Kaohsiung Chang Gung Memorial Hospital.
Conflicts of Interest
19 References
1. WHO. Global Burden of Disease: Statistics. In. Geneva, Switzerland:World Health Organization.
2. Department H. Statistics of Cause of Death 2008. In. Taipei, Taiwan (R.O.C.):Department of Health: 2008.
3. Chen FP, Kung YY, Chen TJ, Hwang SJ. Demographics and patterns of acupuncture use in the Chinese population: the Taiwan experience. J Altern
Complement Med 2006;12:379-387.
4. World Health Organization. Acupuncture : review and analysis reports on controlled clinical trials. Geneva: World Health Organization 2002.
5. Liu CT. Health care systems in transition. II. Taiwan, Part I. A general overview of the health care system in Taiwan. J Public Health Med 1998;20:5-10.
6. Department S. Statistical Yearbook of Interior. In. Taipei:Department of Statistics, Ministry of the Interior, Taiwan (R.O.C.): 2009.
7. Bureau NHI. The National Insurance Statistics 2008. In. Taipei:Bureau of National Health Insurance: 2008.
8. Jorgensen HS, Nakayama H, Raaschou HO, Vive-Larsen J, Stoier M, Olsen TS. Outcome and time course of recovery in stroke. Part II: Time course of recovery. The Copenhagen Stroke Study. Arch Phys Med Rehabil 1995;76:406-412.
20
Haley EC, Jr. Medical and neurological complications of ischemic stroke: experience from the RANTTAS trial. RANTTAS Investigators. Stroke 1998;29:447-453.
10. Langhorne P, Stott DJ, Robertson L, MacDonald J, Jones L, McAlpine C, Dick F, Taylor GS, Murray G. Medical complications after stroke: a multicenter study. Stroke 2000;31:1223-1229.
11. Weimar C, Roth MP, Zillessen G, Glahn J, Wimmer ML, Busse O, Haberl RL, Diener HC. Complications following acute ischemic stroke. Eur Neurol 2002;48:133-140.
12. Hong KS, Kang DW, Koo JS, Yu KH, Han MK, Cho YJ, Park JM, Bae HJ, Lee BC. Impact of neurological and medical complications on 3-month outcomes in acute ischaemic stroke. Eur J Neurol 2008;15:1324-1331.
13. Kumar S, Selim MH, Caplan LR. Medical complications after stroke. Lancet
Neurol 2010;9:105-118.
14. Vermeij FH, Scholte op Reimer WJ, de Man P, van Oostenbrugge RJ, Franke CL, de Jong G, de Kort PL, Dippel DW. Stroke-associated infection is an independent risk factor for poor outcome after acute ischemic stroke: data from the Netherlands Stroke Survey. Cerebrovasc Dis 2009;27:465-471.
15. Emsley HC, Hopkins SJ. Acute ischaemic stroke and infection: recent and emerging concepts. Lancet Neurol 2008;7:341-353.
21
injury-induced immune deficiency syndrome. Nat Rev Neurosci 2005;6:775-786.
17. Chamorro A, Urra X, Planas AM. Infection after acute ischemic stroke: a manifestation of brain-induced immunodepression. Stroke 2007;38:1097-1103.
18. Zijlstra FJ, van den Berg-de Lange I, Huygen FJ, Klein J. Anti-inflammatory actions of acupuncture. Mediators Inflamm 2003;12:59-69.
19. Yamaguchi N, Takahashi T, Sakuma M, Sugita T, Uchikawa K, Sakaihara S, Kanda T, Arai M, Kawakita K. Acupuncture Regulates Leukocyte Subpopulations in Human Peripheral Blood. Evid Based Complement Alternat Med 2007;4:447-453.
20. Shiue HS, Lee YS, Tsai CN, Hsueh YM, Sheu JR, Chang HH. DNA microarray analysis of the effect on inflammation in patients treated with acupuncture for allergic rhinitis. J Altern Complement Med 2008;14:689-698.
21. Murphy TH, Corbett D. Plasticity during stroke recovery: from synapse to behaviour. Nat Rev Neurosci 2009;10:861-872.
22. Zhang SH, Liu M, Asplund K, Li L. Acupuncture for acute stroke. Cochrane
Database Syst Rev 2005:CD003317.
23. Zhang T, Zhang L, Zhang HM, Li Q. [Systematic review of acupuncture therapy for acute ischemic stroke]. China Journal of Traditional Chinese Medicine and
Pharmacy 2009;24:101-104.
24. Lee JD, Chon JS, Jeong HK, Kim HJ, Yun M, Kim DY, Kim DI, Park CI, Yoo HS. The cerebrovascular response to traditional acupuncture after stroke. Neuroradiology
22 2003;45:780-784.
25. Li G, Jack CR, Jr., Yang ES. An fMRI study of somatosensory-implicated acupuncture points in stable somatosensory stroke patients. J Magn Reson Imaging 2006;24:1018-1024.
26. Girou E, Schortgen F, Delclaux C, Brun-Buisson C, Blot F, Lefort Y, Lemaire F, Brochard L. Association of noninvasive ventilation with nosocomial infections and survival in critically ill patients. JAMA 2000;284:2361-2367.
27. Brott T, Adams HP, Jr., Olinger CP, Marler JR, Barsan WG, Biller J, Spilker J, Holleran R, Eberle R, Hertzberg V, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke 1989;20:864-870.
28. van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJ, van Gijn J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988;19:604-607. 29. Williams LS, Yilmaz EY, Lopez-Yunez AM. Retrospective assessment of initial stroke severity with the NIH Stroke Scale. Stroke 2000;31:858-862.
30. Kasner SE, Chalela JA, Luciano JM, Cucchiara BL, Raps EC, McGarvey ML, Conroy MB, Localio AR. Reliability and validity of estimating the NIH stroke scale score from medical records. Stroke 1999;30:1534-1537.
31. Lyden P, Raman R, Liu L, Emr M, Warren M, Marler J. National Institutes of Health Stroke Scale certification is reliable across multiple venues. Stroke 2009;40:2507-2511.
23
32. Karepov VG, Gur AY, Bova I, Aronovich BD, Bornstein NM. Stroke-in-evolution: infarct-inherent mechanisms versus systemic causes. Cerebrovasc Dis 2006;21:42-46. 33. Witt CM, Pach D, Brinkhaus B, Wruck K, Tag B, Mank S, Willich SN. Safety of acupuncture: results of a prospective observational study with 229,230 patients and introduction of a medical information and consent form. Forsch Komplementmed 2009;16:91-97.
34. Adams HP, Jr., Davis PH, Leira EC, Chang KC, Bendixen BH, Clarke WR, Woolson RF, Hansen MD. Baseline NIH Stroke Scale score strongly predicts outcome after stroke: A report of the Trial of Org 10172 in Acute Stroke Treatment (TOAST).
Neurology 1999;53:126-131.
35. Tseng MC, Chang KC. Stroke severity and early recovery after first-ever ischemic stroke: results of a hospital-based study in Taiwan. Health Policy 2006;79:73-78.
36. Schlegel D, Kolb SJ, Luciano JM, Tovar JM, Cucchiara BL, Liebeskind DS, Kasner SE. Utility of the NIH Stroke Scale as a predictor of hospital disposition. Stroke 2003;34:134-137.
37. Rundek T, Mast H, Hartmann A, Boden-Albala B, Lennihan L, Lin IF, Paik MC, Sacco RL. Predictors of resource use after acute hospitalization: the Northern Manhattan Stroke Study. Neurology 2000;55:1180-1187.
38. Chang KC, Tseng MC. Costs of acute care of first-ever ischemic stroke in Taiwan.
24 Table 1 Clinical Characteristics
HPSAAT participants (n=26) Matched control : Non-HPSAAT (n=52) p-value (a) Demographics
Age, years* 70.2 (11.3) 70.2 (11.1) Matched
Sex, male** 16 (61.5) 32 (61.5) Matched
Body mass index, kg/m2* 23.5(3.2) 23.8 (3.6)
Stroke ever** 14 (53.8) 26 (50.0)
Stroke type**
Ischemic 23 (88.5) 50 (96.2)
Ischemic with hemorrhagic transformation
3 (11.1) 2 (3.7) Stroke lesion site**
Right cerebral hemisphere 5 (19.2) 16 (30.8) Left cerebral hemisphere 8 (30.8) 15 (28.8)
Cerebellum 0 (0.0) 2 (3.8)
Brain stem 5 (19.2) 11 (21.2)
Multiple infarcts (≥ 2 of above) 8 (30.8) 8 (15.4) Risk factors of stroke**
Hypertension 20 (76.9) 33 (63.5)
Diabetes mellitus 14 (53.8) 25 (48.1) Hypertriglyceridemia 7 (26.9) 10 (19.2) Hypercholesterolemia 11 (42.3) 17 (32.7) Atrial fibrillation 5 (19.2) 6 (11.5) Coronary artery disease 5 (19.2) 4 (7.7) Congestive heart failure 0 (0.0) 1 (1.9) Cigarette smoking 6 (23.1) 16 (30.8)
Obesity 7 (31.8) 14 (33.3)
25
*: Data are given as mean (SD). **: Data are given as number (percentage). †: Mortality
was excluded (case=0, control=3). ‡: Mortality (case=0, control=3) and patients with recurrent stroke during admission (case=1, control=1) were excluded. §: Long-term care unit included local hospital and nursing home. Abbreviation: HPSAAT, the Pilot Patient source**
Emergency room 20 (76.9) 39 (75.0) Referred from other hospital 3 (11.5) 4 (7.7)
Outpatients 1 (3.8) 9 (17.3)
Referred from other ward in hospital 2 (7.7) 0 (0.0) Timescale of treatment, days*
Onset to ward 2.9 (4.7) 2.3 (3.1)
Onset to acupuncture 17.7 (14.4) -- Duration of acupuncture† 17.4 (16.2) --
Acupuncture session, times 6.7 (6.4) -- Interval of acupuncture sessions 2.9 (1.5) -- Length of stay, days*,‡
In NICU 11.6 (14.1) 2.2 (4.7) <0.01 In Neurology ward 19.2 (8.6) 11.6 (12.7) <0.01 In RCC 2.0 (5.5) 0.0 (0.0) Total 32.9 (21.9) 13.8 (16.1) <0.001 Disposition**,‡ Home 16 (64.0) 46 (95.8) 0.001 Rehabilitation ward 4 (16.0) 0 (0.0) <0.05 Traditional Chinese medicine ward 1 (4.0) 0 (0.0)
Long-term care unit§ 5 (20.0) 2 (4.2) <0.05 (c) Medical Resource Use**
Received r-tPA 0 (0.0) 0 (0.0)
Ever NICU stay 17 (65.4) 15 (28.8) <0.01
Craniectomy or shunt implantation 2 (7.7) 0 (0.0) Mechanical ventilation 4 (15.4) 2 (3.8)
26
Scheme of the Health Policy in Stroke Adjuvant Acupuncture Therapy. NICU, neurology intensive care unit. RCC, respiratory care center. r-tPA, thrombolytic therapy.
27
Table 2 Mortality and Comorbidity during Admission and in Six-Month-Followup
HPSAAT participants (n=26) Matched control : Non-HPSAAT (n=52) p-value
(a) Baseline Comparison: Factors Affecting Mortality and Comorbidity Neurological impairment *
Baseline NIHSS scores 14.9 (9.4) 7.5 (7.0) <0.001
Interquartile range 7-22 2-11.75 NIHSS at consult 16.6 (8.8) -- NIHSS at discharge‡ 15.4 (8.3) 5.6 (5.5) <0.001 Functional Impairment** Baseline mRS >3 24 (92.3) 32 (61.5) <0.01 mRS >3 at consult 25 (96.2) -- mRS >3 at discharge‡ 22 (88.0) 24 (50.0) 0.001
(b) Mortality and Comorbidity during Admission**
Mortality during admission 0 (0.0) 3 (5.8) Neurological complications
Recurrent stroke 1 (3.8) 1 (1.9)
Stroke in-evolution after admission 9 (34.6) 2 (3.8) 0.001 Medical complications
Urinary tract infection (total) 12 (46.2) 12 (23.1) <0.05
Before acupuncture 7 (26.9) -- After acupuncture 5 (19.2) -- Pneumonia (total) 9 (34.6) 11 (21.2) Before acupuncture 9 (34.6) -- After acupuncture 0 (0.0) -- Cellulitis (total) 2 (7.7) 1 (1.9) Before acupuncture 1 (3.8) -- After acupuncture 1 (3.8) -- Gastrointestinal bleeding 4 (15.4) 8 (15.4) Before acupuncture 4 (15.4) --
28
*: Data are given as mean (SD). **: Data are given as number (percentage). †: Mortality
was excluded (case=0, control=3). ‡: Mortality (case=0, control=3) and patients with
recurrent stroke (case=1, control=1) during admission were excluded. Abbreviation: HPSAAT, the Pilot Scheme of the Health Policy in Stroke Adjuvant Acupuncture Therapy. NIHSS, National Institutes of Health Stroke Scale. mRS, modified Rankin Scale. mRS >3 was defined as dependent status. KCGMH, the Kaohsiung Chang Gung Memorial Hospital.
After acupuncture 0 (0.0) --
(c) Six-Month Follow Up in KCGMH**,‡
Ever readmission due to acute disorders 2 (8.0) 7 (14.6) Recurrent stroke within 6 months 0 (0.0) 1 (2.1) Expire within 6 months 0 (0.0) 2 (4.2) Outpatient follow up**,‡ In Neurology Department First 3 months 19 (76.0) 37 (77.1) 6 months 17 (68.0) 37 (77.1) In Rehabilitation Department First 3 months 5 (20.0) 2 (4.2) <0.05 6 months 5 (20.0) 1 (2.1) <0.05 In Acupuncture Department First 3 months 9 (36.0) 0 (0.0) <0.001 6 months 8 (32.0) 0 (0.0) <0.001
29 Figure Legends
Figure 1
*: NICU, neurology intensive care unit. **: NIHSS, National Institutes of Health Stroke
Scale. Scored by one independent physician with certification of American Heart Association Professional Education Center website. †: mRS, modified Rankin Scale. ‡:
KCGMH, the Kaohsiung Chang Gung Memorial Hospital. §: HPSAAT, the Pilot Scheme of the Health Policy in Stroke Adjuvant Acupuncture Therapy. HPSAAT provides stroke patients elective acupuncture at outpatients and inpatients departments during the first year after stroke onset.
Figure 2
The histogram of baseline NIHSS showed the different distribution of severity between groups. There were more moderate to severe strokes among the HPSAAT participants with acute and subacute ischemic stroke than the age-sex matched non-HPSAAT controls (a). The number and percentage of baseline mRS showed that the HPSAAT participants were more dependent than the random controls (b).
30 Figure 1 Participant Flowsheet
4036 non-participants 27 HPSAAT§ participants 1 excluded for insufficient record of neurological examination
Case group: 26 eligible patients
Record demographic and clinical profiles Retrospectively scored NIHSS** and
mRS† on admission, at consult, and at
discharge
Record 6-month-followup at KCGMH‡
Control group: 52 eligible patients Record demographic and clinical profiles
Retrospectively scored NIHSS** and
mRS† on admission and at discharge
Record 6-month-followup at KCGMH‡
Randomized to a 1:2 age-sex matching
Statistical analyses
Patients who had died or had recurrent stroke during admission was excluded from outcome analysis
4064 acute ischemic stroke patients (ICD-9 code 434) admitted to neurology ward and NICU* during 1st Jul 2006 to 30th Jun 2008 Divided by adjuvant acupuncture or none
31
Figure 2 Baseline Discrepancies between HPSAAT Participants and Age-Sex
Matched Non-Participants
(a) Histogram of Baseline NIHSS
(b) Baseline mRS (Case Numbers and Percentages)