ISSN: 1524-4628
Copyright © 2002 American Heart Association. All rights reserved. Print ISSN: 0039-2499. Online Stroke is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX 72514
DOI: 10.1161/hs0102.101626
2002;33;39-44
Stroke
Yuan-Teh Lee
Kuo-Liong Chien, Fung-Chang Sung, Hsiu-Ching Hsu, Ta-Chen Su, Ruey-S. Lin and
Taiwan: Report of the Chin-Shan Community Cardiovascular Study
Apolipoprotein A-I and B and Stroke Events in a Community-Based Cohort in
http://stroke.ahajournals.org/cgi/content/full/33/1/39
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://www.lww.com/reprints
Reprints: Information about reprints can be found online at
[email protected] 410-528-8550. E-mail:
Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Fax: Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters
http://stroke.ahajournals.org/subscriptions/
Community-Based Cohort in Taiwan
Report of the Chin-Shan Community Cardiovascular Study
Kuo-Liong Chien, MD, PhD; Fung-Chang Sung, PhD; Hsiu-Ching Hsu, PhD; Ta-Chen Su, MD;
Ruey-S. Lin, PhD; Yuan-Teh Lee, MD, PhD
Background and Purpose—There are limited prospective cohort studies of the well-known association between stroke events and serum lipids for the Taiwanese population, in whom stroke is the second most common cause of death. Methods—This report describes the effect of dyslipidemia on the risk of stroke in a community-based cohort consisting
of 3602 adults agedⱖ35 years, established in 1990 in the Chin-Shan community in Taipei County, Taiwan.
Results—As of the end of 1998, 97 stroke incidence cases were identified from medical records and death certificates (53 in men and 44 in women). The female-to-male stroke event rates increased from 0.42 in the youngest group (aged 35 to 44 years) to 1.38 in the oldest (agedⱖ75 years). Multiple Cox proportional hazard regression models controlling for age and sex revealed that individuals with serum apolipoprotein A-I (apoA-I) at the highest quartile were more likely to have a stroke event than those at the lowest quartile level (relative risk [RR]⫽2.02, P for trend⫽0.010). The corresponding risk of stroke predicted by apolipoprotein B (apoB) was also significant (RR⫽1.88, P for trend⫽0.020). After adjustment for age, sex, hypertension, and diabetes status, the interaction between hypertension and apoA-I level remained significant in predicting stroke events in men but not in women (RR⫽1.71, P⫽0.033 in men; RR⫽2.29, P⫽0.071 in women).
Conclusions—We conclude that apoA-I but not apoB levels may serve as an effect modifier of hypertension for the risk of stroke events. (Stroke. 2002;33:39-44.)
Key Words: apolipoproteins 䡲 epidemiology 䡲 risk factors 䡲 stroke 䡲 Taiwan
D
yslipidemia, including high serum cholesterol, triglyc-eride, and LDL-cholesterol (LDL-C) levels and low HDL-cholesterol (HDL-C) levels, has been widely accepted as a risk factor for deaths from cardiovascular diseases in white populations. Apolipoprotein A-I (apoA-I) and apoli-poprotein B (apoB) are also identified as risk factors for cardiovascular and possibly cerebrovascular diseases.1,2 Inthe past decades, dyslipidemia has been prevalent in the Taiwanese populations, and the trend toward increasing incidence seems to continue.3However, the impact of
dys-lipidemia on stroke events remains to be determined for Chinese populations.
Cerebrovascular disease was the most lethal disease in Taiwan before 1982 and since then has remained the second most lethal disease. The prevalence of stroke in Taiwan was as high as 1642/100 000 for the population agedⱖ36 years and was composed of the following: cerebral infarction, 67%; cerebral hemorrhage, 14%; subarachnoid hemorrhage, 4%; and unclassified events, 15%.4 Hu et al5 followed up 8562
stroke-free persons in northern Taiwan beginning in 1986 for
4 years; 61 men and 43 women developed first-ever strokes, with an average annual incidence rate of 330/100 000, con-sisting of the following: cerebral infarction, 71%; cerebral hemorrhage, 22%; subarachnoid hemorrhage, 1%; and un-classified, 6%. Hypertension and high sodium content in food were found as risk factors.
The association of hypertension, diabetes, and serum total cholesterol levels with the risk of stroke has been well established.6,7 It is not clear whether the lipid association
pertains to apoA-I and apoB.1,8 Hu et al5 have shown that
hypertension is the major risk factor for stroke in Taiwanese. They did not observe a relationship between serum lipids and stroke.
A community-based prospective cohort study was estab-lished in the Chin-Shan community in Taipei County, Tai-wan, in 1990 to investigate cardiovascular events and related risk factors for the Chinese population.9 –11 This study
em-phasized the effect of lipids on cardiovascular events.9,12The
present report focuses on the impact of apoA-I and apoB on stroke events, including morbidity and mortality in the
Received January 3, 2001; final revision received July 14, 2001;accepted September 1, 2001.
From the Department of Internal Medicine, National Taiwan University Hospital (K-L.C.; H-C.H., T-C.S., Y-T.L.); Institute of Environmental Health (F-C.S.); and Institute of Preventive Medicine, National Taiwan University College of Public Health (R-S.L.), Taipei, Taiwan.
Correspondence to Yuan-Teh Lee, MD, PhD, Department of Internal Medicine, National Taiwan University Hospital, 7 Chung-Shan S Rd, Taipei, Taiwan 100. E-mail [email protected]
© 2002 American Heart Association, Inc. Stroke is available at http://www.strokeaha.org
follow-up period. We measured the sex- and age-specific stroke events in a 9-year follow-up and the relative risk (RR) of dyslipidemia associated with the stroke events in a novel Asian population.
Subjects and Methods
Study Design and Population
The design of this study cohort has been described elsewhere.9
Briefly, a study cohort consisting of 1703 men and 1899 women agedⱖ35 years, homogeneous in Chinese ethnicity, was established in 1990 in Chin-Shan township, 30 km north of metropolitan Taipei, Taiwan. A clinic was set up at the Chin-Shan Community Health Center, and cardiologists from National Taiwan University Hospital conducted the medical examinations with the approval of the hospital institutional review committee. All people who were eligible (n⫽4349) in all households were invited to participate in this study. Persons with previous myocardial infarction and stroke were not excluded from this cohort, but we did not include their survival time if the study outcome was coronary heart disease or stroke. The nonrespondents included 95 persons who refused and 652 individu-als working outside of the local community (respondent rate, 82.8%). At the baseline survey, all study participants were individually interviewed with the use of a structured questionnaire. Trained medical students canvassed door-to-door with the assistance of community leaders to extend invitations for the baseline survey to collect information, including sociodemographic characteristics, life-style, dietary characteristics, and personal and family histories of diseases and hospitalizations. With the consent of participants, physicians and students conducted physical examinations and labo-ratory tests for those participants invited to the clinic. A 12-lead ECG was also performed for each participant, and 2 cardiologists evalu-ated the results in a blinded manner.
Blood Sampling and Analytical Methods
All venous blood samples drawn after a 12-hour overnight fast were immediately refrigerated and transported within 6 hours to National Taiwan University Hospital. Serum samples were then stored at ⫺70°C before the batch assay for levels of total cholesterol, triglyceride, LDL-C, HDL-C, apoA-I, apoB, and lipoprotein(a) [Lp(a)]. Standard enzymatic tests for serum cholesterol and triglyc-eride were used (Merck 14354 and 14366, respectively). HDL-C levels were measured in supernatants after the precipitation of specimens with magnesium chloride phosphotungstate reagents (Merck 14993). LDL-C concentrations were calculated as total cholesterol minus cholesterol in the supernatant by the precipitation method (Merck 14992). ApoA-I and apoB concentrations were measured by turbidimetric immunoassay with the use of commercial kits (Sigma). Lp(a) was determined by enzyme-linked immunosor-bent assay (Organon) regardless of isoforms.
Cohort Follow-Up and Data Verification
The study team conducted biennial follow-up household visits with the study participants, and death certificates were reviewed monthly at the local vital statistics office. The cardiologists conducted conferences and discussions to clarify causes of events and deaths, without knowledge of the status of subjects. When there was disagreement about the diagnosis, a neurologist was consulted. The diagnosis was categorized as unclassified if it was controversial. The consistency of diagnoses was maintained by regular discussion among the same committee members and by hospital document verification.
Data analyses were limited to those who were free of stroke at the baseline study (n⫽3514); 88 persons with a history of stroke events before the baseline survey were excluded in the initial cohort. The incidence of stroke was defined as a sudden neurological deficit of vascular origin that lasted⬎24 hours. Transient ischemic attacks were not included in this study.
To ensure the quality of diagnosis of stroke, a committee was established to review cases of stroke. All preliminary diagnoses,
medical records, death certificates, and interviews with patients’ relatives for related events were presented to this committee. The cases were confirmed by internists.
Hypertension was defined according to the criteria established by the sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.13
Persons with systolic blood pressure⬎140 mm Hg and/or diastolic blood pressure⬎90 mm Hg and/or receiving antihypertensive med-ication were considered hypertensive. Diabetes mellitus was defined as fasting blood sugar levels⬎126 mg/dL or use of oral hypogly-cemic agents or insulin injections.14Obesity was defined as body
mass index⬎26.4 kg/m2.
Statistical Analysis
Mean and SD values for continuous variables and contingency tables for binary data are presented. Student’s t test and2test were initially
used to test the difference between stroke and nonstroke groups. Sex-and age-specific incidence rates of stroke were calculated with the use of person-years on the basis of the follow-up periods of individuals eligible for this study.15Female-to-male rate ratios were
calculated for age groups stratified by 1 decade (35 to 44, 45 to 54, 55 to 64, 65 to 74, andⱖ75 years). RRs of stroke events and 95% CIs were estimated by fitting a Poisson regression model.16A Cox
proportional hazards model17was also applied to estimate the RRs
and 95% CIs for various covariates. One-way ANCOVA with adjustment for age was used to compare the mean values of continuous variables by stroke status. Logarithmic transformation was performed because of skewed distribution in triglyceride and Lp(a) values. All continuous variables were standardized to a mean of 0 and SD of 1 to compare the relative effects on stroke events. Multiple linear regression by the Cox proportional hazards model, with adjustment for age and sex, was fitted to estimate risk ratios of highest to lowest quartiles of various lipid and apolipoprotein values. Hypertension and diabetes mellitus were also included in the models for the estimation of RRs of apoA-I and apoB for stroke. Interaction items between hypertension and apoA-I and apoB were estimated in the model. Because of the negative interaction of age and sex on stroke rates, the interaction of age and sex was also included. Age was input as a continuous variable in the model, and smoking, hypertension, and diabetes status were stratified as binary variables. Data analysis was performed with SAS/STAT software (SAS Insti-tute Inc, version 6.11).18
Results
Basic Characteristics
As of the end of 1998, with a follow-up rate of 89.7% in a 9-year period (mean, 7.0 years; median, 7.5 years), 46 persons died as a result of stroke events and another 51 persons suffered stroke events for the first time. These 97 persons were considered to have experienced stroke events (53 in men, 44 in women). The estimated rates from stroke events were 4.67/1000 person-years for men and 3.32/1000 person-years for women.
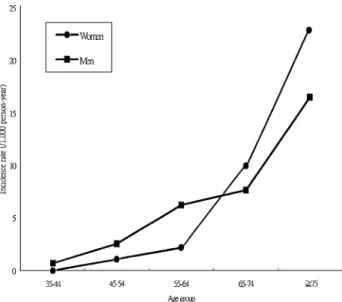
The age-specific stroke rates during the follow-up period increased exponentially from 0.71/1000 person-years in the group aged 35 to 44 years to 16.49/1000 person-years for the group agedⱖ75 years for men and from 0.00 to 22.83/1000 person-years for women with corresponding ages (Figure). The age-specific female to-male rate ratio increased as age increased from 0.42 in the group aged 45 to 54 years to 1.38 in the oldest age group (ⱖ75 years). A crossover change in the age-specific ratio appeared between the group aged 55 to 64 years (rate ratio⫽0.35) and the group aged 65 to 74 years (rate ratio⫽1.31).
Comparison of Lipids, Blood Pressure, and Body Mass Index Between Persons With and Without Stroke Events
Compared with persons free of stroke, those with stroke events were significantly older and had higher systolic and/or diastolic blood pressure. They also had higher cholesterol and LDL-C values at borderline significant levels and were more likely hypertensive and diabetic (Table 1). Triglyceride,
HDL-C, Lp(a), apoA-I, and apoB levels were higher in the stroke group, but this was not statistically significant. After adjustment for age, differences between the stroke and nonstroke groups were significant only for systolic and diabolic blood pressure (data not shown).
Distribution of Selected Lipids and Lipoprotein Values and RRs of Stroke Events
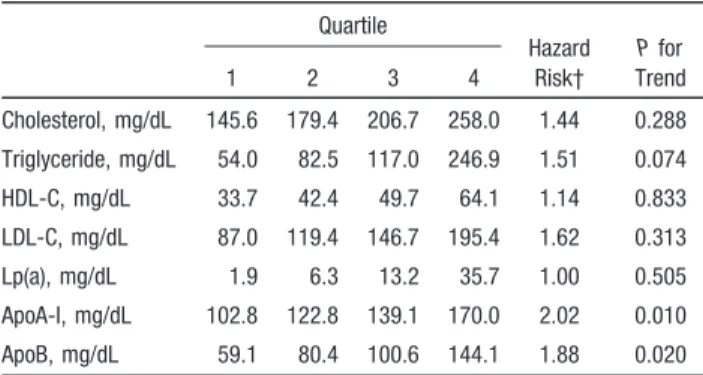
The quartile values of various lipids and lipoproteins and RRs of highest versus lowest quartiles are described in Table 2. After adjustment for age and sex, the RRs were significant only for apoA-I (RR⫽1.99; 95% CI, 1.18 to 3.35) and apoB levels (RR⫽2.13; 95% CI, 1.08 to 4.20). Other lipids and lipoproteins were not significant risk factors for stroke.
When the interaction items hypertension and apoA-I or apoB were included together with the interaction of age and sex in Cox proportional hazards regression models, apoA-I and apoB had minor positive effects on stroke events in both sexes (Table 3). The interaction of hypertension and apoA-I level had a significant positive effect on stroke risk in men (RR⫽1.71; P⫽0.033) but a moderate effect in women (RR⫽2.29; P⫽0.071). We also found, in an additional analysis separating hypertensive from normotensive subjects, that apoA-I was a significant risk factor in the hypertensive group (RR⫽1.81; P⬍0.001) but not in the normotensive group (RR⫽1.09; P⫽0.542) (data not shown). ApoB was not a significant risk factor for either the normotensive or hypertensive group (RR⫽1.07 and RR⫽1.34; P⫽0.647 and
P⫽0.160, respectively).
Incidence rates of stroke events in the study population by sex and age groups in the Chin-Shan community.
TABLE 1. Baseline Data of Study Population in Chin-Shan Community Cohort, Stratified by Status of Stroke Events
Stroke Events (n⫽96) No Stroke Events (n⫽3417) P RR* 95% CI Mean SD Mean SD Age, y 73.6 9.4 61.8 12.0 0.0001 3.06 2.43–3.85 SBP, mm Hg 144.8 25.8 124.6 19.8 0.0001 2.07 1.80–2.39 DBP, mm Hg 83.7 11.2 76.8 11.0 0.0001 1.77 1.48–2.11 BMI, kg/m2 23.8 3.7 23.5 3.4 0.381 1.07 0.87–1.30 Cholesterol, mg/dL 210.0 47.4 197.5 45.2 0.008 1.19 0.98–1.43 Triglyceride, mg/dL 129.7 77.6 125.3 96.1 0.590 1.15† 0.94–1.40 HDL-C, mg/dL 48.6 16.1 47.6 12.4 0.529 1.06 0.87–1.29 LDL-C, mg/dL 149.3 45.2 137.2 43.9 0.009 1.18 0.97–1.43 Lp(a), mg/dL 17.1 17.9 14.0 15.2 0.096 1.03† 0.84–1.28 ApoA-I, mg/dL 135.7 32.8 133.7 36.0 0.606 1.08 0.98–1.19 ApoB, mg/dL 101.5 35.6 95.6 49.6 0.124 1.10 0.97–1.24 Sex, % female 45.4 53.1 0.131 1.44 0.97–2.15 Smoking, % 43.3 36.2 0.150 1.45 0.97–2.16 Hypertension, % 60.8 26.5 0.001 4.48 2.98–6.74 Diabetes, % 30.9 12.0 0.001 2.98 1.94–4.58 Obesity, % 24.0 17.9 0.130 1.43 0.89–2.28 SBP indicates systolic blood pressure; DBP, diastolic blood pressure; and BMI, body mass index. *Univariate Cox proportional hazards model results. The continuous variables were standardized, with variables minus means, divided by SD as independent covariate.
Discussion
This study was the first report of stroke events in a community-based prospective cohort of the Chinese popula-tion in Taiwan. The unique and novel aspects of this study were the population examined and the interaction factors associated with stroke events in a longitudinal follow-up.
Our study did not specify stroke type as infarction or hemorrhage and included several types of vascular disorders of the brain with different etiologies. Because no local hospital was available for this community, only a conserva-tive diagnosis was noted. The diagnoses of definite cerebral hemorrhage and cerebral infarction decreased after late 1986 in Taiwan.19Imaging studies, such as CT, were not available
in this suburban area. The diagnosis of stroke is not very reliable in population studies because of the limited use of imaging and insufficient participation by qualified neurolo-gists. Completely accurate ascertainment by type of stroke is
not possible in epidemiological studies, even in well-developed countries. Therefore, stroke defined by clinical observation has proved to be reliable for total case definition and collection.20 Some epidemiological studies of stroke,
such as the Goteborg and Copenhagen studies, also include a few hemorrhagic strokes and unspecified strokes.21,22In our
study all types of stroke event were included as outcome, although there was heterogeneity in the subtypes of stroke.
Age had different impacts on stroke events in both sexes. The accelerated increase of stroke incidence rates for elderly women may indicate the effects of menopause on stroke events. Other studies also showed that women after meno-pause had risks of cardiovascular events comparable to those of men.23,24
The effect of cholesterol levels on the risk of stroke events remains controversial.25 The Honolulu Heart Program
re-vealed a significant inverse association between cholesterol and cerebral hemorrhage.26 However, the Multiple Risk
Factor Intervention Trial (MRFIT) found insignificant asso-ciations with intracranial hemorrhage, observed from the 6-year follow-up.27Increased lipid levels, such as cholesterol,
triglyceride, and LDL-C, have not predicted cerebral infarc-tion in several populainfarc-tion-based cohort studies.28 –30Increased
serum lipid levels have generally not been associated with an increased risk of stroke, except for men aged⬍60 years.31
No consistent association was found regarding the roles of apoA-I and apoB in the pathogenesis of stroke events. Avogaro et al32 considered apolipoprotein levels more
dis-criminative than lipid and lipoprotein levels in the prediction of cardiovascular disease. Durrington et al33also indicated
that serum apoB is more significant in the development of cardiovascular diseases. ApoA-I may improve HDL-C in reducing the risk of coronary heart disease.34However, the
Physician’s Health Study35 found no significant role for
apoA-I and apoB in the prediction of myocardial infarction. In this study we found that apoA-I was a significant risk factor for a stroke event, in contrast to previous studies. Lamarche et al36 concluded that apoB was an independent
risk factor for ischemic heart disease. ApoB can be consid-ered in terms of number of atherogenic particles in plasma. The study of Pedro-Botet et al1showed that apoA-I levels
were higher in the ischemic stroke group. Woo et al2studied
304 Chinese acute stroke patients and found that HDL-C and apoA-I were protective factors. Unfortunately, when they dissected the data into binary groups, no protective effect of apoA-I was demonstrated.
In this study we could not identify HDL-C as a protective factor for stroke. We have included various types of stroke in this study, and the effects of HDL-C varied in different subtypes of stroke. The sample size might be inadequate as well. The role of HDL-C in stroke deserves further investi-gation in the Taiwanese population.
It has been suggested in a longitudinal study that Lp(a) may be an independent risk factor for stroke.37 However,
Lp(a) concentration in other studies failed to independently predict stroke-related events.38,39 Lp(a) was considered a
weak risk factor for stroke in men and was not considered a significant risk factor for stroke in women in a community-based cohort of 9936 persons in Olmsted County, Minneso-TABLE 2. Quartile Distribution* of Selected Lipids and
Lipoproteins in the Study Population and Age- and Sex-Adjusted Hazard Risk of Highest to Lowest Quartile for Prediction of Stroke Events
Quartile Hazard Risk† P for Trend 1 2 3 4 Cholesterol, mg/dL 145.6 179.4 206.7 258.0 1.44 0.288 Triglyceride, mg/dL 54.0 82.5 117.0 246.9 1.51 0.074 HDL-C, mg/dL 33.7 42.4 49.7 64.1 1.14 0.833 LDL-C, mg/dL 87.0 119.4 146.7 195.4 1.62 0.313 Lp(a), mg/dL 1.9 6.3 13.2 35.7 1.00 0.505 ApoA-I, mg/dL 102.8 122.8 139.1 170.0 2.02 0.010 ApoB, mg/dL 59.1 80.4 100.6 144.1 1.88 0.020
*Means within each quartile are presented.
†RR: highest versus lowest quartile for the prediction of stroke events, age and sex adjusted, considering other 2 quartiles simultaneously in the model.
TABLE 3. Cox Proportional Hazard Regression Model for ApoA-I and ApoB in Predicting Stroke Events in the Chin-Shan Community Cardiovascular Study Population
Women Men Hazard Risk 95% CI P Hazard Risk 95% CI P Analysis 1 Age 1.12 1.08–1.15 0.000 1.07 1.04–1.10 0.000 Diabetes mellitus 2.18 1.13–4.19 0.020 2.33 1.27–4.27 0.006 Hypertension 2.11 1.10–4.05 0.025 2.95 1.67–5.20 0.000 ApoA-I 0.90 0.43–1.86 0.773 1.07 0.83–1.37 0.616 ApoA-I⫻ hypertension 2.29 0.93–5.60 0.071 1.71 1.05–2.80 0.033 Analysis 2 Age 1.11 1.08–1.14 0.000 1.07 1.04–1.10 0.000 Diabetes mellitus 1.85 0.95–3.61 0.073 2.13 1.16–3.89 0.014 Hypertension 2.04 1.04–4.00 0.037 2.78 1.56–4.98 0.001 ApoB 1.05 0.56–1.96 0.890 0.98 0.58–1.64 0.925 ApoB⫻ hypertension 1.12 0.47–2.67 0.793 1.58 0.74–3.36 0.234 42 Stroke January 2002
ta.40We also did not identify Lp(a) as a convincing risk factor
in the pathogenesis of a stroke event.
The important role of hypertension in the pathogenesis of stroke events, including both cerebral hemorrhage and cere-bral infarction, has been well established. This study also demonstrated a high impact of hypertension on stroke. The RR of hypertension on stroke determined in our study was similar to that suggested by others, at approximately 2.5 to 3.0.25 Further analysis of the interaction between
hyperten-sion and apoA-I level has demonstrated that apoA-I is a risk modifier for the pathogenesis of stroke events in men. Pedro-Botet et al1and Airo et al8demonstrated that apoA-I
levels in stroke patients are similar to those in normal controls. They noted that apoA-I was not always protective for stroke events. Furthermore, complex mechanisms are involved in the apoA-I–regulated HDL-C effect on athero-sclerosis. Certain genetic disorders, such as cholesteryl ester transfer protein deficiency, induce elevated apoA-I levels without definite protection in regard to stroke.41Improvement
of blood pressure control is protective for stroke events. Consistent with other studies, this study also established diabetes as a risk factor for stroke. In community-based studies of various countries, diabetes has been shown to be a risk factor for stroke.42– 45Diabetes results in progression of
the atherosclerotic process, and aggressive control of diabetes is therefore important for the prevention of stroke.
Study Limitations
This study used a community-based cohort established in a suburban area near the largest metropolitan area in Taiwan. The socioeconomic status of the cohort members may be different from that of an urban population. However, on the basis of educational level and age distribution, this cohort is similar to the general population in Taiwan of similar age.
Because the death registry system in Taiwan is well established, we should have recovered all deaths that oc-curred in the cohort. However, the mortality rate may be slightly overestimated because 10.3% of persons who were lost to follow-up were censored in the 9-year mortality calculation. Because of the low incidence of cardiovascular disease events in the Chinese, a longer follow-up period will measure the mortality rate with greater accuracy and will allow estimation of the subtle effects of dyslipidemia on mortality.
Stroke events that are traced from hospital sources, nursing homes, and death certificates may lead to inconsistent results. Consistent diagnoses and verification of events are highly important for case identification. Our study team consistently collected measurements of risk factors. The variation in stroke diagnosis may not affect the estimation of risk to a significant level in this study. The current paradigm suggests that cholesterol has different effects on stroke types.27
How-ever, for those who do not die in the hospital, type of stroke is usually not documented by general community practitio-ners in Taiwan. After extensive inquiry, 30% of stroke cases in this study lack adequate medical documentation regarding the type of stroke. This disadvantage limits the ability of analysis to separate ischemic strokes from hemorrhagic strokes.
Additionally, false inference of multiple comparisons should be taken into consideration. In this study we limited the number of analyses and only focused on lipid profiles to prevent exaggeration of a type I error. In the first analysis, the comparison was conducted with only average values between the stroke and nonstroke groups. This analysis showed that apoA-I was a moderate risk factor. Further analyses in which stratified methods were used revealed that apoA-I was a significant risk factor for stroke only in men.
Conclusions
This study demonstrated that apoA-I is a significant effect modifier of stroke events in a longitudinal cohort study of a Chinese population. Aggressive intervention and treatment of risk factors should emphasize hypertension and diabetes control in decreasing stroke events in the Chinese.
Acknowledgments
This study was supported in part by the Power Development Foundation of Taiwan Power Company and National Science Coun-cil (NSC86-2314-B002-184-M40), Executive Yuan, Taiwan. The authors thank Ya-Li Huang and Yuh-Chen Huang for careful revision of data structure and Ching-Chu Chien for technical assistance.
References
1. Pedro-Botet J, Senti M, Nogues X, Rubies-Prat J, Roquer J, D’Olhaberriague L, Olive J. Lipoprotein and apolipoprotein profile in men with ischemic stroke: role of lipoprotein(a), triglyceride-rich lipoproteins, and apolipoprotein E polymorphism. Stroke. 1992;23: 1556 –1562.
2. Woo J, Lau E, Lam CWK, Kay R, Teoh R, Wong HY, Prall WY, Kreel L, Nicholls MG. Hypertension, lipoprotein(a), and apolipoprotein A-I as risk factors for stroke in the Chinese. Stroke. 1991;22:203–208. 3. Pan WH, Chiang BN. Plasma lipid profiles and epidemiology of
athero-sclerotic diseases in Taiwan: a unique experience. Atherosclerosis. 1995; 118:285–295.
4. Hu HH, Chu FL, Chiang BN, Lan CF, Sheng WY, Lo YK, Wong WJ, Luk YO. Prevalence of stroke in Taiwan. Stroke. 1989;20:858 – 863. 5. Hu HH, Sheng WY, Chu FL, Lan CF, Chiang BN. Incidence of stroke in
Taiwan. Stroke. 1992;23:1237–1241.
6. Kagan A, Harris BR, Winkelsteink W, Johnson KG, Kato H, Syme SL, Rhoads GG, Gay ML, Nichaman MZ, Hamilton HB, Tillotson J. Epide-miologic studies of coronary heart disease and stroke in Japanese men living in Japan, Hawaii and California: demographic, physical, dietary and biochemical characteristics. J Chron Dis. 1974;27:345–364. 7. WHO MONICA Project Principal Investigators. The World Health
Orga-nization MONICA Project (Monitoring Trends and Determinants in Car-diovascular Disease): a major international collaboration. J Clin Epi-demiol. 1988;41:105–114.
8. Airo R, Ferrari C. High density lipoproteins and apolipoprotein A in cerebrovascular disease. Atherosclerosis. 1985;54:343–346.
9. Lee YT, Lin RS, Sung FC, Yang CY, Chien KL, Chen WJ, Su TC, Hsu HC, Huang YC. Chin-Shan Community Cardiovascular Cohort in Taiwan: baseline data and five-year follow-up morbidity and mortality. J Clin Epidemiol. 2000;53:836 – 846.
10. Chien KL, Lee YT, Sung FC, Su TC, Hsu HC, Lin RS. Lipoprotein (a) level in the population in Taiwan: relationship to sociodemographic and atherosclerotic risk factors. Arteriosclerosis. 1999;143:267–273. 11. Chien KL, Lee YT, Sung FC, Hsu HC, Su TC, Lin RS. Hyperinsulinemia
and related atherosclerotic risk factors in the population at cardiovascular risk: community-based study. Clin Chem. 1999;45:838 – 846.
12. Torng PL, Su TC, Sung FC, Chien KL, Huang SC, Chow SN, Lee YT. Effects of menopause and obesity on lipid profiles in middle-aged Tai-wanese women: the Chin-Shan Community Cardiovascular Cohort Study. Arteriosclerosis. 2000;153:413– 421.
13. National Heart, Lung, and Blood Institute. National High Blood Pressure Education Program: The Sixth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood
Pressure. Bethesda, Md: US Dept of Health and Human Services, National Institutes of Health; 1997. Publication 98-4080, 1-68. 14. Report of the Expert Committee on the Diagnosis and Classification of
Diabetes Mellitus. Diabetes Care. 1997;20:1183–1197.
15. Chen CJ, Chiou HY, Chiang MH, Lin LJ, Tai TY. Dose-response rela-tionship between ischemic heart disease mortality and long-term arsenic exposure. Arterioscler Thromb Vasc Biol. 1996;16:504 –510.
16. Kahn HA, CT Sempos. Statistical Methods in Epidemiology. New York, NY: Oxford University Press; 1989:1–292.
17. Cox DR. Regression models and life-tables. J R Stat Soc A. 1972;2: 187–220.
18. SAS Institute Inc. SAS/STAT Software: Changes and Enhancements Through Release 6.11. Cary, NC: SAS Institute Inc; 1996:1–1104. 19. Chang CC, Chen CJ. Secular trend of mortality from cerebral infarction
and cerebral hemorrhage in Taiwan, 1974 –1988. Stroke. 1993;24: 212–218.
20. Terent A. Stroke morbidity. In: Whisnant JP, ed. Stroke: Populations, Cohorts and Clinical Trials. Oxford: Butterworth-Heinemann; 1993: 37–58.
21. Harmsen P, Tsipogianni A, Wilhelmsen L. Stroke incidence rates were unchanged, while fatality rates declined, during 1971–1987 in Goteborg, Sweden. Stroke. 1992;23:1410 –1415.
22. Boysen G, Nyboe J, Appleyard M, Sorensen PS, Boas J, Somnier F, Jensen G, Schnohr P. Stroke incidence and risk factors for stroke in Copenhagen, Denmark. Stroke. 1988;19:1345–1353.
23. Bush TL. The epidemiology of cardiovascular disease in postmenopausal women. Ann NY Acad Sci. 1990;592:263–271.
24. Matthews KA, Meilahn E, Kuller LH, Kelsey SF, Caggiula AW, Wing RR. Menopause and risk factors for coronary heart disease. N Engl J Med. 1989;321:641– 646.
25. Ueda K, Omae T. Risk factors for stroke and transient ischemic attack. In: Whisnant JP, ed. Stroke: Populations, Cohorts and Clinical Trials. Oxford: Butterworth-Heinemann; 1993:80 –110.
26. Yano K, Reed DM, MacLean CJ. Serum cholesterol and hemorrhagic stroke in the Honolulu Heart Program. Stroke. 1989;20:1460 –1465. 27. Iso H, Jacobs DR Jr, Wentworth D, Neaton JD, Cohen JD. Serum
cholesterol levels and six-year mortality from stroke in 350,977 men screened for the Multiple Risk Factor Intervention Trial. N Engl J Med. 1989;320:904 –910.
28. Harmsen P, Rosengren A, Tsipogianni A, Wilhelmsen L. Risk factors for stroke in middle-aged men in Goteborg, Sweden. Stroke. 1990;21: 223–229.
29. Kannel WB, Dawber TR, Sorlie P, Wolf PA. Components of blood pressure and risk of atherothrombotic brain infarction: the Framingham Study. Stroke. 1976;7:327–331.
30. Kagan A, Popper JS, Rhoads GG, Yano K. Dietary and other risk factors for stroke in Hawaiian Japanese men. Stroke. 1985;16:390 –396.
31. Kannel WB, Gordon T, Dawber TR. Role of lipids in the development of brain infarction: the Framingham Study. Stroke. 1974;5:679 – 685. 32. Avogaro P, Bon GB, Cazzolato G, Quinci GB. Are apolipoproteins better
discriminators than lipids for atherosclerosis? Lancet. 1979;1:901–903. 33. Durrington PN, Hunt L, Ishola M, Kane J, Stephens WP. Serum
apoli-poproteins A1 and B and liapoli-poproteins in middle aged men with and without previous myocardial infarction. Br Heart J. 1986;56:206 –212. 34. Bhatnagar D, Durrington PN. Clinical value of apolipoprotein
mea-surement. Ann Clin Biochem. 1991;28:427– 437.
35. Stampfer MJ, Sacks FM, Salvini S, Willett WC, Hennekens CH. A prospective study of cholesterol, apolipoproteins, and the risk of myo-cardial infarction. N Engl J Med. 1991;325:373–381.
36. Lamarche B, Tchernof A, Mauriege P, Cantin B, Dagenais GR, Lupien PJ, Despres JP. Fasting insulin and apolipoprotein B levels and low-density lipoprotein particle size as risk factors for ischemic heart disease. JAMA. 1998;279:1955–1961.
37. Schreiner PJ, Chambless LE, Brown SA, Watson RL, Toole J, Heiss G. Lipoprotein (a) as a correlate of stroke and transient ischemic attack prevalence in a biracial cohort: the ARIC Study: Atherosclerosis Risk in Communities. Ann Epidemiol. 1994;4:351–359.
38. van Kooten F, van Krimpen J, Dippel DW, Hoogerbrugge N, Koudstaal PJ. Lipoprotein(a) in patients with acute cerebral ischemia. Stroke. 1996; 27:1231–1235.
39. Ridker PM, Stampfer MJ, Hennekens CH. Plasma concentration of lipoprotein(a) and the risk of future stroke. JAMA. 1995;273:1269 –1273. 40. Nguyen TT, Ellefson RD, Hodge DO, Bailey KR, Kottke TE, Abu-Lebdeh HS. Predictive value of electrophoretically detected lipoprotein(a) for coronary heart disease and cerebrovascular disease in a community-based cohort of 9936 men and women. Circulation. 1997;96: 1390 –1397.
41. Koizumi J, Inazu A, Yagi K, Koizumi I, Uno Y, Kajinami K, Miyamoto S, Moulin P, Tall AR, Mabuchi H. Serum lipoprotein lipid concentration and composition in homozygous and heterozygous patients with cho-lesteryl ester transfer protein deficiency. Atherosclerosis. 1991;90: 189 –196.
42. Salonen JT, Puska P, Tuomilehto J, Homan K. Relation of blood pressure, serum lipids, and smoking to the risk of cerebral stroke: a longitudinal study in Eastern Finland. Stroke. 1982;13:327–333.
43. Kagan A, Popper JS, Rhoads GG. Factors related to stroke incidence in Hawaii Japanese men: the Honolulu Heart Study. Stroke. 1980;11:14 –21. 44. Davis PH, Dambrosia JM, Schoenberg BS, Schoenberg DG, Pritchard DA, Lilienfeld AM, Whisnant JP. Risk factors for ischemic stroke: a prospective study in Rochester, Minnesota. Ann Neurol. 1987;22: 319 –327.
45. Barrett-Connor E, Khaw KT. Diabetes mellitus: an independent risk factor for stroke? Am J Epidemiol. 1988;128:116 –123.