Gender Differences in Health-related Quality of Life among the Elderly in Taiwan
HUI-CHUAN HSU*
Department of Healthcare Administration, Asia University, Taiwan
ABSTRACT
Purpose: This study examines the gender disparity in the elderly’s health-related quality of life in Taiwan. Method: Data came from the National Health Interview Survey, a series of nation-representative face-to-face interviews held in Taiwan in 2001. The samples were chosen from those aged 65 or over, including populations drawn from the Taiwan area (with a number n=1845), remote mountain areas (n=169), and offshore islands (n=179). Health-related quality of life (HQOL) was measured by SF-36, including the dimensions of physical functioning, role limitation due to physical problems, bodily pain, general health, vitality, social functioning, role limitation due to emotional problems, and mental health. Two-stage linear regression models were used for analysis.
Results: Elderly women showed lower HQOL in almost every dimension in the Taiwan area and offshore islands. After controlling for age, education, marital status, activities of daily living, and numbers of chronic diseases, women elderly showed a lower score in HQOL than men, and the difference was the most prominent in bodily pain which had a 23.6% lower score. The elderly in offshore islands and mountain areas had a lower HQOL than that in the Taiwan area. Other effects were greater than gender for the elderly in remote mountain areas. Discussion: Gender difference appeared across different dimensions of health-related quality of life. More effort to improve equal gender opportunities for health-related quality of life is necessary.
Key words: health inequality, elderly health, health-related quality of life, gender difference.
1. INTRODUCTION
Health inequality is the focus of recent health policy issues (Berkman &
Kawachi, 2000; Braveman, 2006; Curtis & Jones, 1998; Gakidou, Murray & Frenk, 2000; Gwatkin, 2002; Kawachi & Kennedy 2002; Marmot & Wilkinson 1999;
Pradhan, Sahn, & Younger, 2003). The differences of gender, socioeconomic status, geographic area, and other groups are examined for their effects on health and health care. The underlying advantages and disadvantages of social groups are explored, and thus implications are provided for social and health policy. Usually, the measure of health inequality has often been limited to mortality, with a lack of consideration for health-related quality of life. Even where there have been studies about health differences in health-related quality of life in Taiwan, the elderly’s health inequality were less discussed. In this study I would like to examine the gender disparity of health-related quality of life for the elderly in Taiwan.
The most widely cited definition of health inequality is that defined by Whitehead (2000) in The Concepts and Principles of Equity and Heath. In this WHO document Whitehead states that “Equity in health implies that ideally everyone should have a fair opportunity to attain their full potential and, more pragmatically, that no one should be disadvantaged from achieving this potential, if it can be avoided,” and “Equity is therefore concerned with creating equal
* E-mail: [email protected]
H. C. Hsu / Asian Journal of Health and Information Sciences, Vol. 1, No. 4, pp. 366-376, 2007
367
opportunities for health and with bringing health differentials down to the lowest level possible.” Bravemen (2006) commented that this definition is intuitive, clear and accessible, but unjust, unfair, and avoidable: it is open to interpretation, and does not provide guidance on measurement. Other researchers have discussed thoroughly the concept and measures of health inequality (Braveman, 2004, 2006;
Gakidou et al., 2000; Mackenbach & Kunst, 1997; Murray, Gakidou, & Frenk, 1999; Regidor, 2004a, b; Wagstaff, Pact, & Doorslaer, 1991). They agreed that equity in health should minimize the avoidable differences in health and its determinants. They also tried to explicitly define the inequality in terms of systematic and potential disadvantages across social groups, such as those defined by gender, geography, socioeconomics, race/ethnicity/religion, and age, and therefore provide policy implications.
Elderly women have many disadvantages in societies across the world.
Economic (income, food and nutrition, work environment, water and sanitation), social (literacy, education, caregiving, widowhood), political (enfranchisement, advocacy participation), and cultural (attitude to aging, attitudes to women’s self-esteem) factors have made elderly women experience cumulative economic barriers since youth, making them short of resources and contributing to a deterioration in health (Bonita, 1998).
Gender difference in the health of the elderly has usually been found in health services’ research (Chavers, Gilbert, & Shelton, 2002; Degl'Innocenti et al., 2002;
Friedman, 2003; Hsu, 2005; Koch et al., 2004; van Mil et al., 2000; Wijnhoven, Kriegsman, Snoek, Hesselink, & de Haan, 2003), but many studies have only focused on the specific diseases of patients, while a gender sensitive analysis was lacking.
Although some evidence of health inequality has been found in Taiwan, most studies have emphasized the differences in disease patterns and causes of death.
Health inequality research by more comprehensive and continuous measures of health could be measured with relatively ease, but only a small amount of this kind of research has been done. Actually, many scales of health-related quality of life have been developed, validated, and widely applied, such as MOS (Tarlove et al., 1989); MOS 36-item Short-Form Health Survey (SF-36) (McHorney, Ware &
Raczek, 1993); WHOQOL (The WHOQOL group, 1995); HRQoL (Bowling, 1997), General Health Questionnaire (GHQ)(Goldberg & Hiller, 1979), etc. The Taiwanese version of SF-36 (Lu, Ho, Lee, & Yen, 2003) has also been developed and validated. However, research on the inequality in elderly health has been uncommon. Only one study has used SF-36 to compare elderly health in urban, rural, and remote islands (Tsai, Chi, Lee, & Chou, 2004). Significant differences were found, but the samples were selected from three specific communities rather than nation-representative samples.
In this study, “health equality” is used according to Whitehead’s definition.
Therefore, a health equality measure should represent not only the same level of health, but also reflect the equal opportunities in health, such as the demands of different roles and the various social functions. So health-related quality of life as measured by Short-Form 36 was chosen as the measure of health. The health
inequality in gender in this study is explained from the viewpoint of there being equal opportunities for health. The purpose of this study is to examine the gender difference in health-related quality of life among the elderly in Taiwan, from remote mountain areas and offshore islands, by nation-representative samples. This paper will examine the gender inequality of health-related quality of life for the elderly and therefore offer implications for health policy.
2. METHODS
2.1 Data and samples
The data was from “The 2001 National Health Interview Survey,” a Taiwan population representative data. This survey included demographics, health status, health behavior, medical utilization, and other health-related variables. The adult participants were drawn by probability-proportional-to-size (PPS) sampling respectively from the Taiwan area (sampling from seven life circles), remote mountain areas (sampling from 30 districts in mountain area), and offshore islands (sampling from offshore islands in four counties). Taiwan is a mountainous island which is surrounded by small islands. People’s health in the mountain areas and the island areas is, on average, lower than that of the general Taiwan area. The health resources in remote mountain and island areas are also much fewer. Most of the aboriginal groups live in mountain areas but some live on the offshore islands.
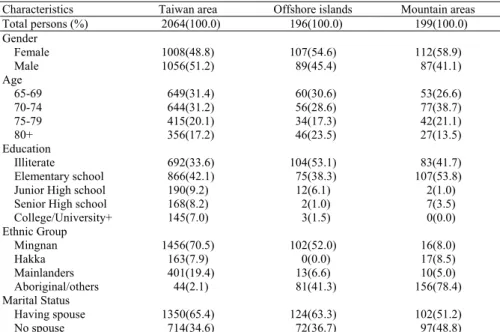
In this study, we used adult questionnaire data (aged 12 or over) and chose only elderly samples aged 65 or over. The sample sizes were 2,064 for the Taiwan area, 199 for mountain areas, and 196 for offshore islands. The sampling from the three areas was independent, so these three sets of samples were not pooled together for analysis in this study. Sample description is as shown in Table 1.
2.2 Measures
Health-related quality of life was measured by the Short-Form 36 (SF-36) Taiwan version (Lu, et al., 2003), which included eight dimensions of physical function, role limitations due to physical problems, bodily pain, general health, vitality, social functioning, role limitation due to emotional problems, and mental health. Some items were score reversed before calculation. After transformation, a higher score indicates a better health-related quality of life. In this study none of the scores were weighted.
Gender and geographic area were the main independent variables in the models. Samples in the Taiwan area were further stratified to seven living circles to analyze the heterogeneity within Taiwan. The other controlling factors to health-related quality of life were demographics (age, educational level, ethnic groups, and marital status) and health variables (disability and morbidity).
Disability was measured by activities of daily living (ADL), including eating, dressing, transferring, walking indoors, taking a bath, and using the toilet. If the participants had difficulty performing any one of the ADL items and the difficulty lasted for more than three months, then he/she was judged to be ADL disabled.
H. C. Hsu / Asian Journal of Health and Information Sciences, Vol. 1, No. 4, pp. 366-376, 2007
369
Morbidity was measured by the numbers of subjects currently having chronic diseases, which included heart disease, respiratory disease, hypertension, diabetes, high cholesterol, stroke, ulcer, nasosinusitis, liver disease, kidney disease, and prostate or ovary/uterus disease.
Table 1. Sample description
Characteristics Taiwan area Offshore islands Mountain areas Total persons (%) 2064(100.0) 196(100.0) 199(100.0)
Gender
Female 1008(48.8) 107(54.6) 112(58.9)
Male 1056(51.2) 89(45.4) 87(41.1)
Age
65-69 649(31.4) 60(30.6) 53(26.6)
70-74 644(31.2) 56(28.6) 77(38.7)
75-79 415(20.1) 34(17.3) 42(21.1)
80+ 356(17.2) 46(23.5) 27(13.5)
Education
Illiterate 692(33.6) 104(53.1) 83(41.7)
Elementary school 866(42.1) 75(38.3) 107(53.8)
Junior High school 190(9.2) 12(6.1) 2(1.0)
Senior High school 168(8.2) 2(1.0) 7(3.5)
College/University+ 145(7.0) 3(1.5) 0(0.0)
Ethnic Group
Mingnan 1456(70.5) 102(52.0) 16(8.0)
Hakka 163(7.9) 0(0.0) 17(8.5)
Mainlanders 401(19.4) 13(6.6) 10(5.0)
Aboriginal/others 44(2.1) 81(41.3) 156(78.4)
Marital Status
Having spouse 1350(65.4) 124(63.3) 102(51.2)
No spouse 714(34.6) 72(36.7) 97(48.8)
Note. 1. Samples who were literate but have not received formal education were categorized to elementary school.
2. Having spouse includes married and living together. No spouse includes being widowed, divorced, single, and others.
2.3 Analysis
The gender difference stratified by geographic areas was analyzed by the t-test. A two-stage linear regression was used to analyze the gender difference within three geographic areas. Dependent variables were the scores of eight health dimensions of SF-36. Gender was the main independent variable in the first stage, while age, education, marital status, ADL disability, and chronic disease numbers were second stage independent variables. Because there are heterogeneities in Taiwan (remote mountains and offshore islands), the three samples were not pooled but separated for analysis of the gender effect.
3. RESULTS
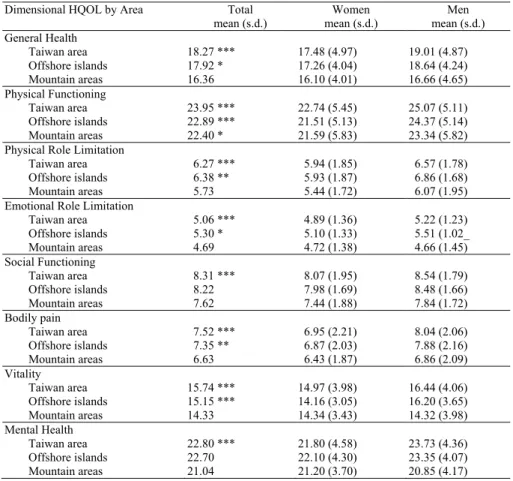
Table 2 examines the gender difference for each SF-36 dimension by geographic stratification of the Taiwan area, mountain areas and offshore islands.
In the Taiwan area, women elderly were significantly lower than men elderly in all HQOL dimensions. In the offshore islands, women had lower HQOL in general
health, physical function, physical role limitation, emotional role limitation, bodily pain, and vitality. In the mountain area, most of the HQOL dimensions were similar in women and men, except the physical function; women was lower than men in this aspect. However, the mean scores in these three areas were also different. The scores in the Taiwan area were the highest in almost every dimension, except that the offshore islands showed a higher score in physical role limitation and emotional role limitation. Mountain areas showed the lowest score in every dimension of SF-36.
Table 2. Gender difference of elderly’s health-related quality of life by SF-36 score, stratified by geographic area
Dimensional HQOL by Area Total mean (s.d.)
Women mean (s.d.)
Men mean (s.d.) General Health
Taiwan area 18.27 *** 17.48 (4.97) 19.01 (4.87) Offshore islands 17.92 * 17.26 (4.04) 18.64 (4.24) Mountain areas 16.36 16.10 (4.01) 16.66 (4.65) Physical Functioning
Taiwan area 23.95 *** 22.74 (5.45) 25.07 (5.11) Offshore islands 22.89 *** 21.51 (5.13) 24.37 (5.14) Mountain areas 22.40 * 21.59 (5.83) 23.34 (5.82) Physical Role Limitation
Taiwan area 6.27 *** 5.94 (1.85) 6.57 (1.78) Offshore islands 6.38 ** 5.93 (1.87) 6.86 (1.68)
Mountain areas 5.73 5.44 (1.72) 6.07 (1.95)
Emotional Role Limitation
Taiwan area 5.06 *** 4.89 (1.36) 5.22 (1.23) Offshore islands 5.30 * 5.10 (1.33) 5.51 (1.02_
Mountain areas 4.69 4.72 (1.38) 4.66 (1.45)
Social Functioning
Taiwan area 8.31 *** 8.07 (1.95) 8.54 (1.79) Offshore islands 8.22 7.98 (1.69) 8.48 (1.66)
Mountain areas 7.62 7.44 (1.88) 7.84 (1.72)
Bodily pain
Taiwan area 7.52 *** 6.95 (2.21) 8.04 (2.06) Offshore islands 7.35 ** 6.87 (2.03) 7.88 (2.16)
Mountain areas 6.63 6.43 (1.87) 6.86 (2.09)
Vitality
Taiwan area 15.74 *** 14.97 (3.98) 16.44 (4.06) Offshore islands 15.15 *** 14.16 (3.05) 16.20 (3.65) Mountain areas 14.33 14.34 (3.43) 14.32 (3.98) Mental Health
Taiwan area 22.80 *** 21.80 (4.58) 23.73 (4.36) Offshore islands 22.70 22.10 (4.30) 23.35 (4.07) Mountain areas 21.04 21.20 (3.70) 20.85 (4.17) Note. Examined by t-test. *p<0.05, **p<0.01, ***p<0.001.
Gender difference by controlling other variables and stratified by geographic area is shown in Table 3. Elderly women in the Taiwan area and the offshore islands showed worse health in most of the health-related quality of life dimensions after controlling other variables. However, gender difference was not found in the mountain areas. In the eight dimensions of health-related quality of life, the greatest
Table 3. Gender difference of Health-related quality of life by geographic area stratification
Taiwan area General Health Physical
Functioning Physical Role
Limitation Emotional Role
Limitation Social
Functioning Bodily Pain Vitality Mental Health Gender (Female) -0.154*** -0.198*** -0.170*** -0.118*** -0.125*** -0.236*** -0.171*** -0.197***
Age -0.014 -0.225*** -0.141*** -0.099*** -0.103** -0.079*** -0.060** 0.042
Education 0.007 0.015 0.011 0.021 -0.017 0.049* 0.006 0.005
Marital status -0.001 0.019 0.012 -0.014 0.042 0.004 -0.004 -0.021
ADL disability -0.285*** -0.468*** -0.243*** -0.207*** -0.372*** -0.306*** -0.296*** -0.263***
Chronic disease
no. -0.302 -0.179*** -0.214*** -0.196*** -0.144*** -0.210 -0.207*** -0.171***
Adjusted R2 0.219 0.413 0.180 0.125 0.213 0.234 0.189 0.151
Offshore Islands General Health Physical
Functioning Physical Role
Limitation Emotional Role
Limitation Social
Functioning Bodily Pain Vitality Mental Health Gender (Female) -0.143 -0.229** -0.320*** -0.173* -0.155 -0.216* -0.190* -0.080
Age 0.001 -0.168* -0.139 0.068 -0.081 -0.026 -0.009 0.018
Education 0.086 0.092 -0.086 0.042 -0.005 0.088 0.163 0.117
Marital status 0.048 0.075 -0.024 -0.011 0.026 -0.018 0.124 0.051 ADL disability -0.042 -0.276*** -0.170* -0.074 -0.184* -0.148* -0.004 -0.028 Chronic disease
no. -0.347 -0.231** -0.299*** -0.282*** -0.198* -0.338*** -0.241** -0.125
Adjusted R2 0.128 0.260 0.182 0.099 0.082 0.183 0.139 0.014
Mountain Area General Health Physical
Functioning Physical Role
Limitation Emotional Role
Limitation Social
Functioning Bodily Pain Vitality Mental Health Gender (Female) 0.015 -0.053 -0.103 0.095 -0.045 -0.015 0.103 0.106
Age -0.150* -0.139* -0.089 -0.086 -0.125 -0.010 -0.014 -0.032
Education 0.118 0.111 -0.009 0.203* 0.010 0.063 0.152* 0.136
Marital status 0.037 0.008 0.089 -0.009 0.016 0.054 0.039 -0.024
ADL disability -0.251** -0.542*** -0.303*** 0.264** -0.431*** -0.405*** -0.341*** -0.264**
Chronic disease
no. -0.337*** -0.246*** -0.139 -0.130 -0.163* -0.250*** -0.268*** -0.211**
Adjusted R2 0.204 0.419 0.135 0.122 0.028 0.223 0.192 0.105
Note 1: A two-stage linear regression is used for analysis; gender is put in the first stage. The standardized coefficients are listed in the table. A constant is omitted. The score is not weighted; a higher score means better health. The coefficients are standardized.
Note 2: Education is counted by educational year. Marital status (1=married or living together, 0=single, divorce, widowed, others). ADL disability means if there is any difficulty of any one item from eating, dressing, transferring, walking indoors, bathing, and using the toilet, and the difficulty has lasted for more than three months (1=difficulties in any one item, 0=none). Chronic diseases include hearing disease, respiratory disease, hypertension, diabetes, high cholesterol, stroke, ulcer, nasosinusitis, liver disease, kidney disease, and prostate or ovary/uterus disease.
Note 3: Reference group of independent variables: Gender (male), age (continuous), educational year (continuous), marital status (no spouse), ADL disability (none), and number of chronic diseases (continuous).
H. C. Hsu / Asian Journal of Health andInformation Sciences, Vol.1, No.4, pp. 366-376, 2007
371
disparity between men and women for the Taiwan area was bodily pain (r =
−0.236). Next were mental health (r = −0.197) and physical functioning (r =
−0.170). As for the offshore islands, the greatest disparities between the two genders were physical role limitation (r = −0.320), physical functioning (r =
−0.229), and bodily pain (r = −0.216).
Being older appeared to be worse in six health dimensions for the Taiwan elderly, except for general health and mental health. The elderly of the offshore islands’ were only worse in physical functioning, while the elderly from the mountains were only worse in general health and physical functioning. Having any ADL disability and more chronic diseases showed a worse health-related quality of life across three areas. Educational level and marital status were not significant at all. The variance across the models were quite different (R square ranged from 0.01 to 0.42), with the physical functioning model giving the best explanation and the mental health model giving the least probable explanation.
4. DISCUSSION
In this study, SF-36 was used as the measure of health-related quality of life, and found gender differences in the elderly in Taiwan. Elderly women showed a lower health-related quality of life, while the elderly in offshore islands and mountain areas had a lower HQOL than those in the Taiwan area.
Consistent with past studies (Friedman, 2003; Koch et al., 2004; Wjinhoven et al., 2003), we have shown that older women have a lower health-related quality of life in general, or in some dimensions. In another Taiwan study, elderly women also had less successful aging than elderly men and this may possibly be related to cumulative disadvantages (Hsu, 2005). In this study the gender difference in HQOL was significant, but with a varying pattern in geographic areas. In the Taiwan area, women had lower HQOL in every dimension, especially in bodily pain, physical functioning, and mental health, which is consistent with other studies (Friedman, 2003; Koch et al., 2004; Wjinhoven et al., 2003). Women’s lower HQOL might be related to poorer recovery from illness in physical function (Friedman, 2003), or a high level of depression and anxiety related to the disease severity (Wjinhoven et al., 2003). But in the offshore islands elderly women felt in poorer health in their roles, physical function, pain, or vitality. These dimensions all reflected some kinds of demands from their roles or functions, which may be related to gender. It is possible that elderly women need to carry more responsibilities, perform more physical activity or have taxing family roles. The opportunities for health-related quality of life were not equally gender-distributed.
Gender difference was not found in remote mountain areas. However, the health in mountain areas was the lowest in every dimension compared to the Taiwan area and offshore islands. It implies that the geographic inequality is greater than gender differences for mountain areas, especially for the aboriginal groups. In the past, the aboriginal group had less opportunity for education, a lower socio-economic status, and less health care resource than in the Taiwan area. They
H. C. Hsu / Asian Journal of Health and Information Sciences, Vol. 1, No. 4, pp. 366-376, 2007
373
also have higher social isolation and lack of cultural stimulation in these rural areas.
Some behavior related to poor health was also more prevalent in the mountain areas (Hurng et al., 2000; Lu, Tseng & Tsai, 2003). Public health effort is still needed and social infrastructure for the remote mountain areas is necessary to improve the situation.
Geographic health inequality is also an important field in health inequality issues. Curtis & Jones (1998) explain the geographic differences by compositional (individual) and contextual effects. The contextual effects are interpreted by the spatial patterning and diffusion of physical and biological risk factors, the role of space and place in social relations important for health; and a sense of place helps to understand the significance of health. Geographic effect is often related to different exposures to health risks, inequity in access to health care, or income inequality (Krieger, 1999; Marmot & Wilkinson, 1999). The geographic difference in the elderly’s health-related quality of life may be related to the unfair opportunity for the same level of quality of health. The life for farmers is usually labor-intensive, and reduced access to health care may influence their health. These elderly are also more likely to have a low income, or worry about economic security after retirement (Ministry of Interior, 2002).
This study has some limitations. First, the samples of the offshore islands and remote mountain areas were limited. The samples were drawn from the 2001 National Health Interview Survey. Although the sampling was over-weighted for selecting more from the offshore islands and mountain area samples, the available samples were still limited. Secondly, multi-level analysis was not applied in this study, and personal characteristics were only used for control in the models. The main reasons include that the offshore islands and mountain areas samples were limited and the sampling method in the survey was without city/county representation. Thus this study only compared the differences in the Taiwan area, offshore islands, and mountain areas by stratification. In addition, this study analyzed the absolute difference rather than a single index of distribution, and therefore the dissimilarity or distribution of health inequality was not represented (Regidor, 2004 a, b). Third, for many cases the income variable was missing or unavailable for analysis. Additionally, most of the elderly do not have work.
Educational level was the only socio-economic status variable to be controlled in the analysis.
Gender difference of the elderly’s health-related quality of life exists in geographic area in Taiwan. Although National Health Insurance is implemented to remove the financial access risk, and public health efforts were made for health care distribution equity, there seems to be health inequality for the elderly. The unfair opportunity that impedes the health-related quality of life for women needs to be examined, and gender sensitivity analysis should be applied to health policy to create equal opportunities for health and quality of life for both genders. In addition, further studies are suggested to examine the geographic difference in health inequality within Taiwan, to examine the underlying factors of geographic and individual levels by multi-level analysis, and to explore the relations between health and geography with intensive qualitative research.
ACKNOWLEDGEMENTS
This research was supported by grants from the National Science Council, Taiwan, R.O.C., under the project “Elderly women’s health problems and improving strategies” (NSC 93-2621-Z-468-001). This study is based on data from the National Health Interview Survey Original Database provided by the Bureau of Health Promotion, Department of Health and National Health Research Institutes.
The interpretation and conclusions contained herein do not represent those of Bureau of Health Promotion, Department of Health or National Health Research Institutes. The author also thanks the anonymous reviewers’ for their comments, and Mr. Gerald Irby’s help in English editing.
REFERENCES
Berkman, L. F., & Kawachi, I. (Eds.). (2000). Social Epidemiology. New York, USA: Oxford Express.
Bonita, R. (1998). Women, Aging, and Health: Achieving health across the life span. Under the guidance of Ageing and Health Programme. Geneva, Switzerland: World Health Organization.
Bowling, A. (1997). Measuring Health: A Review of Quality of Life Measurement Scales, Vol. 2. Milton Keynes, UK: Open University Press.
Bravemen, P. (2004). Defining equity in Health. Health Policy and Development, 2(3), 180-185.
Braveman, P. (2006). Health disparities and health equity: concepts and measurement. Annual Review of Public Health, 27, 167-194.
Chavers, L. S., Gilbert, G. H., & Shelton, B. J. (2002). Racial and socioeconomic disparities in oral disadvantage, a measure of oral health-related quality of life:
24-month incidence. Journal of Public Health Dentistry, 62(3), 140-147.
Curtis, S., & Jones, I. R. (1998). Is there a place for geography in the analysis of health inequality? Sociology of Health & Illness, 20(5), 645-672.
Degl'Innocenti, A., Elmfeldt, D., Hansson, L., Breteler, M., James, O., Lithell, H., Olofsson, B., Skoog, I., Trenkwalder, P., Zanchetti, A., & Wiklund, I. (2002).
Cognitive function and health-related quality of life in elderly patients with hypertension - baseline data from the study on cognition and prognosis in the elderly (SCOPE). Blood Pressure, 11(3), 157-65.
Friedman, M. M. (2003). Gender differences in the health related quality of life of older adults with heart failure. Heart & Lung, 32(5), 320-327.
Gakidou, E. E., Murray, C. J. L., & Frenk, J. (2000). Defining and measuring health inequality: an approach based on the distribution of health expectancy. Bulletin of the World Health Organization, 78(1), 42-54.
Gwatkin, D. R. (2002). Reducing health inequalities in developing countries. In R.
Detels, J. Mcewen, R. Beaglehole, & H. Tanaka (Eds.), Oxford Textbook of Public Health (4th ed.). New York, USA: Oxford University Press.
H. C. Hsu / Asian Journal of Health and Information Sciences, Vol. 1, No. 4, pp. 366-376, 2007
375
Goldberg, D. P., & Hillier, V. F. (1979). A scaled version of the General Health Questionnaire. Psychological Medicine, 9(1), 139-145.
Hurng, B. S., Chang, Y. C., Lo, S. Y., Lu, M. L., Chen, J. R., Huang, L. Y., &
Hung, M. W. (2000). Health care demands and needs for offshore islands in Taiwan Province. Public Health, 26(4), 283-302. [in Chinese]
Hsu, H. C. (2005). Gender disparity of successful aging in Taiwan. Women &
Health, 42(1), 1-21.
Kawachi, I., & Kennedy, B. P. (2002) The health of nations: why inequality is harmful to your health. New York, USA: New Press.
Koch, C. G., Khandwala, F., Cywinski, J. B., Ishwaran, H., Estafanous, F. G., Loop, F. D., & Blackstone, E. H. (2004). Health-related quality of life after coronary artery bypass grafting: a gender analysis using the Duke Activity Status Index.
Journal of Thoracic & Cardiovascular Surgery, 128(2), 284-95.
Krieger, N. (1999). Embodying inequality: a review of concepts measures and methods for studying health consequences of discrimination. International Journal of Health Services, 29(2), 295-352.
Lu, J. F., Tseng, H. M., & Tsai, Y. J. (2003). Assessment of health-related quality of life in Taiwan (I): development and psychometric testing of SF-36 Taiwan version. Taiwan Journal of Public Health, 22(6), 501-511. [in Chinese]
Lu, T. H., Ho, L. H., Lee, M. C., & Yen, C. H. (2003). Epidemiological transition and trends of inequality in mortality in aboriginal areas in Taiwan, 1974-1998.
Chung Shan Medical Journal, 14, 545-555.
Mackenbach, J. P., & Kunst, A. E. (1997). Measuring the magnitude of socio-economic inequalities in health: an overview of available measures illustrated with two examples from Europe. Social Science & Medicine, 44(6), 757-771.
Marmot, M., & Wilkinson, R. G. (Eds.). (1999). Social Determinants of Health.
(1st ed.). New York, USA: Oxford University Press.
McHorney, C. A., Ware, J. E., & Raczek, A. E. (1993). The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Medical Care, 31(3), 247-263.
Ministry of Interior, R.O.C. (2002). Survey of living conditions of the elderly in Taiwan-Fuchien area, 2002. Taipei, Taiwan: Department of Statistics, Ministry of Interior.
Murray, C. J. L., Gakidou, E. E., & Frenk, J. (1999). Health inequalities and social group differences: what should we measure? Bulletin of World Health Organization, 77(7), 537-543.
Pradhan, M., Sahn, D. E., & Younger, S. D. (2003). Decomposing world health inequality. Journal of Health Economics, 22(2), 271-293.
Regidor, E. (2004a). Measures of health inequalities: part 1. Journal of Epidemiology & Community Health, 58, 858-861.
Regidor, E. (2004b). Measures of health inequalities: part 2. Journal of Epidemiology & Community Health, 58, 900-903.
Tarlove, A. R., Ware, A. E., Greenfield, S., Nelson, E. C., Perrin, E., & Zubkoff, M.
(1989). The Medical Outcomes Study. An application of methods for monitoring the results of medical care. Journal of American Medical Association, 262(7), 925-930.
Tsai, S. Y., Chi, L. Y., Lee, L. S., & Chou, P. (2004). Health-related quality of life among urban, rural, and island community elderly in Taiwan. Journal of the Formosan Medical Association, 103(3), 196-204.
van Mil, A. H., van Klink, R. C., Huntjens, C., Westendorp, R. G., Stiggelbout, A.
M., Meinders, A. E., & Lagaay, A. M. (2000). Cardiopulmonary resuscitation preferences in Dutch community- dwelling and hospitalized elderly people: an interaction between gender and quality of life. Medical Decision Making, 20(4), 423-429.
Wagstaff, A., Pact, P., & Doorslaer, E. V. (1991). On the measurement of inequalities in health. Social Science & Medicine, 33(5), 545-557.
Whitehead, M. (2000). The concepts and principles of equity and health.
Copenhagen, Denmark: WHO, Regional Office for Europe (EUR/ICP/RPD 414 7734r).
WHOQOL Group. (1995). The World Health Organization Quality of Life Assessment (WHOQOL): position paper from the World Health Organization.
Social Science & Medicine, 41(10), 1403-1409.
Wijnhoven, H. A., Kriegsman, D. M., Snoek, F. J., Hesselink, A. E., & de Haan, M.
(2003). Gender differences in health-related quality of life among asthma patients. Journal of Asthma, 40(2), 189-199.
Hui-Chuan Hsu received her Ph.D. in health policy and management from National Taiwan University, Taipei, Taiwan in 2001. She served in Department of Planning, National Taiwan University Hospital in 1998-2000, and National Taipei College of Nursing as a part-time lecturer in 2000-2001. She is currently an Associate Professor in the Department of Department of Healthcare Administration at Asia University, Taiwan. Her current research interests include successful aging, social gerontology, and long-term care policy.