國立臺灣大學獸醫專業學院臨床動物醫學研究所 碩士論文
Graduate Institute of Veterinary Clinical Science School of Veterinary Medicine
National Taiwan University Master Thesis
以超音波評估腎上腺功能亢進犬隻心臟及 腎臟功能
Evaluation of Cardiac and Renal Function in Dogs Affected with Hyperadrenocorticism by Ultrasonography
陳虹吟 Hung-Yin Chen
指導教授:黃慧璧 博士
Advisor: Hui-Pi Huang, DVM, Ph.D.
中華民國 101 年 7 月 July 2012
Acknowledgement
回首這三年的研究時光,從懵懂無知到學有專精,從瑟瑟縮縮到獨當一面,
對我來說是改變相當大的三年,除了在學術上的精進外,在待人處事及人生態度 上也有了不小的轉變。其中最感謝的就是我的指導教授黃慧璧博士,老師對於學 術的堅持及專業在這三年中深深影響著我,獸醫不該只是獨善其身的行業,研究 的成果可以對實證醫學提供貢獻才是最重要的。此外,老師樂觀開朗的性格與自 由開放的教學態度,也讓我學習到如何正面思考及自我管理。
本論文的完成另外亦得感謝口試委員吳應寧教授與林荀龍副教授的協助,因 為有您們的幫忙與指教,使得本論文能夠更完整而嚴謹。
與我一起天天待在 402 的同學,悅倫與子綺,感謝妳們的幫助與陪伴,一起 處理不同的病例,一起開會檢討門診的大小事,一起接電話,一起在 402 待到天 亮,一起歡笑一起崩潰,最後,能夠一起順利畢業真是太好了,能與你們共事我 感到非常幸運。
感謝于欣學姊與小向學長,謝謝你們在臨床上的指導與幫助。謝謝阿花與彥 貞學姐,謝謝你們在我們慌亂無助的時候,第一線的提供幫助,也謝謝你們的傳 承讓我們學習到實驗室的技術。謝謝小安學長、佩盈學姐與士琬學姐,雖然相處 的時間不長,但大五時候在你們的門診獲益良多,你們是我進這個實驗室的契機。
唯一的小學妹秉燁,有你真好,非常感謝你總是沒有任何推辭的就幫我們收集及 處理病例,相信你的大方與優秀的外語能力能讓你未來一路順遂。
謝謝台大內科的同仁與助理以及范先生,謝謝你們的幫助讓我病例的收集如 此順利。感謝我最要好的朋友妮妮,雖然你早我一年離開,但研究生生活中與你 一起出外玩耍與互吐苦水是忙亂的研究生活中最快樂的時光。感謝這三年中一直 陪在我身邊的阿杜哥,謝謝你的體諒與包容,你的體貼與陪伴是支持我完成論文 的最大動力。
最後要感謝我的摯愛的家人,謝謝你們當我最大的靠山,讓我在學習的路上 無後顧之憂,這篇論文是獻給你們的。
Abstract
Hyperadrenocorticism (HAC) is a common endocrine disorder in middle-aged and older dogs. Long-term exposure to high levels of glucocorticoids causes several complications, such as hypertension, left ventricular hypertrophy, myocardial fibrosis, glomerulosclerosis and elevated renal resistance. Meanwhile, HAC also contributed both cardiac and renal dysfunction. Left ventricular myocardial function was
investigated using two-dimensional speckle tracking echocardiography (2D-STE).
Resistive index (RI) and pulsatility index (PI) of the renal artery and aorta, as well as the presence of microalbuminuria were also evaluated. In the present study, the prevalence of hypertension, hypertrophic cardiomyopathy (HCM), renal vascular resistance and albuminuria were significantly increased in dogs with HAC compared with age-matched non-HAC group. In dogs with HCM, dogs with adrenal-dependent hyperadrenocorticism had significantly decreased longitudinal systolic and diastolic function despite systolic performance of left ventricular were normal when evaluated using parameters derived from the conventional echocardiography. The presence of albuminuria was positive associated with increased renal RI, suggesting that
albuminuria might be associated with increased vascular resistance within the kidneys.
中文摘要
腎上腺功能亢進為中老年犬隻常見的內分泌疾病,長期暴露於高濃度的醣皮 質醇會導致許多併發症,包括高血壓,左心室壁肥厚,心肌纖維化,絲球體硬化 及血管阻力提高。除了結構改變,腎上腺功能亢進同時也會影響心臟及腎臟的功 能,造成心臟舒張不良,尿液濃縮能力下降及蛋白尿比例提升。此論文包含兩個
部份:(1)以腹腔超音波評估腎上腺功能亢進犬隻腎臟間動脈及後大動脈血管阻
力改變,與蛋白尿與微蛋白尿的發生率(2)以新式的二維斑點追蹤超音波技術 評估腎上腺功能亢進犬隻心肌運動性的改變。整體而言,腎上腺功能亢進犬隻顯 著出現高血壓、心肌增厚、腎臟血管阻力增加與增加蛋白尿的發生率。此外本研 究中,尿蛋白與腎臟阻抗係數成正相關,顯示尿蛋白的增加與腎臟血管阻力增加 有關。在心臟評估方面,儘管傳統超音波用來計算心臟收縮功能的數值在所有犬 隻都是正常且沒有差異的,但心肌厚的犬隻在斑點追蹤超音波結果顯示較正常犬 來的低,其中又以腎上腺型腎上腺功能亢進的犬隻最為顯著。顯示心肌厚會同時 影響舒張其收縮功能,而新式的二維斑點追蹤超音波可做為一敏感性較高的診斷 工具。
Table of Contents
口試委員審定書 i Acknowledgement ii
Abstract iii
中文摘要 iv
Table of Contents v
List of Tables vi
List of Figures vii
Chapter 1 General Introduction 1
References 13
Chapter 2 Vascular Resistance and Albuminuria in Dogs Affected 19 with Chronic Hyperadrenocorticism and Chronic Degenerative
Mitral Valvular Disease
References 32
Chapter 3 Assessment of Hypertrophic Cardiomyopathy in Small Breed 39 Dogs Affected with Hyperadrenocorticism Using 2D
Speckle-Tracking Echocardiography
References 54
Chapter 4 Summarized Discussion 68
References 72
List of Tables Chapter 2
Table 1. Baseline characteristics of healthy controls, dogs 36 affected with chronic degenerative mitral valvular disease
(CDMD group) along and dogs affected with CDMD and concurrent hyperadrenocorticism (HAC group)
Table 2. The resistive index (RI), and pulsatility index (PI) of renal 37 artery and aorta in healthy controls, dogs affected with
chronic degenerative mitral valvular disease (CDMD group) along and dogs affected with CDMD and concurrent
hyperadrenocorticism (HAC group) Chapter 3
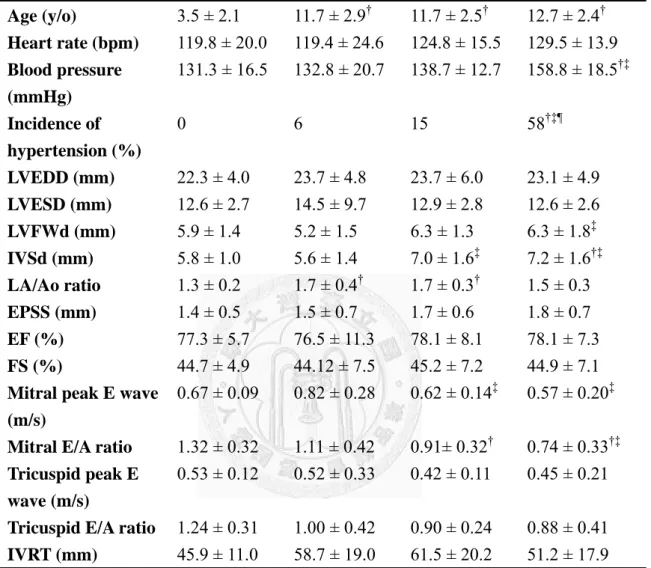
Table 1. Baseline characteristics of groups of the healthy controls, 58 age-matched non-hyperadrenocorticism (non-HAC),
pituitary-dependent hyperadrenocorticism (PDH) and adrenal-dependent hyperadrenocorticism (ADH)
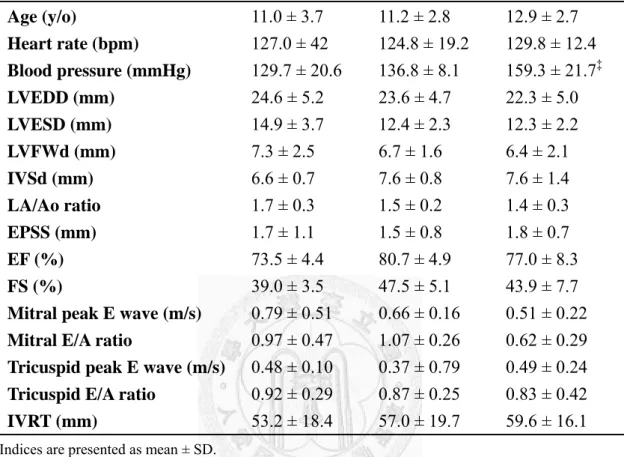
Table 2. Baseline characteristics of dogs affected with hypertrophic 59 cardiomyopathy in age-matched non-hyperadrenocorticism
(non-HAC), pituitary-dependent hyperadrenocorticism (PDH) and adrenal-dependent hyperadrenocorticism (ADH)
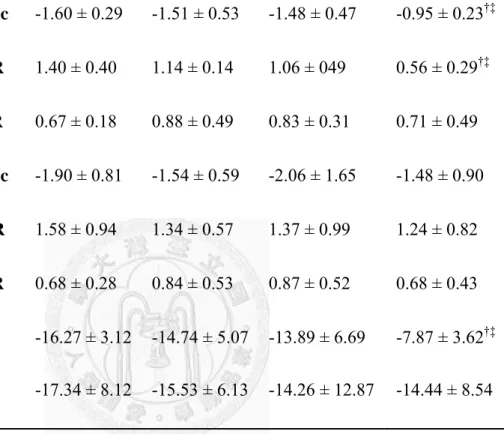
Table 3. Global strains and strain rates derived from two-dimensional 60 speckle-tracking echocardiography in healthy controls and
dogs affected with hypertrophic cardiomyopathy in age-matched non-hyperadrenocorticism (non-HAC), pituitary-dependent hyperadrenocorticism (PDH) and adrenal-dependent hyperadrenocorticism (ADH)
Table 4. Indices of left ventricle longitudinal tissue velocities (LTV) 61 derived from two-dimensional speckle-tracking
echocardiography in healthy controls and dogs affected with hypertrophic cardiomyopathy in age-matched
non-hyperadrenocorticism (non-HAC), pituitary-dependent hyperadrenocorticism (PDH) and adrenal-dependent hyperadrenocorticism (ADH)
Table 5. Indices of left ventricle radial tissue velocities (RTV) derived 62 from two-dimensional speckle-tracking echocardiography in healthy controls and dogs affected with hypertrophic cardio- myopathy in age-matched non-hyperadrenocorticism (non-HAC), pituitary-dependent hyperadrenocorticism (PDH)
and adrenal-dependent hyperadrenocorticism (ADH)
Table 6. Indices of left ventricle longitudinal strain rates (LSR) derived 63 from two-dimensional speckle-tracking echocardiography in healthy controls and dogs affected with hypertrophic cardio- myopathy in age-matched non-hyperadrenocorticism (non-HAC), pituitary-dependent hyperadrenocorticism (PDH)
and adrenal-dependent hyperadrenocorticism (ADH)
Table 7. Indices of left ventricle circumferential strain rates (CSR) 64 derived from two-dimensional speckle-tracking
echocardiography in healthy controls and dogs affected with hypertrophic cardiomyopathy in age-matched
non-hyperadrenocorticism (non-HAC), pituitary-dependent hyperadrenocorticism (PDH) and adrenal-dependent hyperadrenocorticism (ADH)
Table 8. Indices of left ventricular longitudinal (LS) and circumferential 65 (CS) peak strain derived from two-dimensional speckle-tracking echocardiography in healthy controls and dogs affected with hypertrophic cardiomyopathy in age-matched
non-hyperadrenocorticism (non-HAC), pituitary-dependent hyperadrenocorticism (PDH) and adrenal-dependent hyperadrenocorticism (ADH)
Table 9. The intra-obsever coefficient of variance (CV) of 2D-STE 66 variables
List of Figures Chapter 2
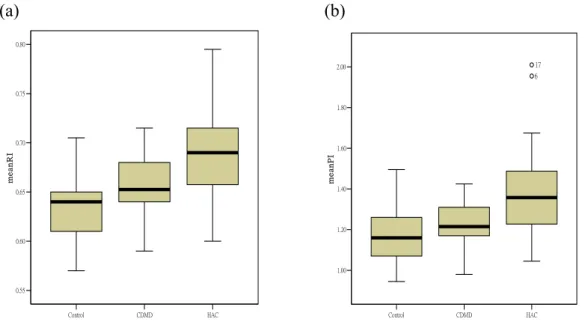
Figure 1. Box-and-whiskers plot of the (a) mean renal resistive index 38 (RI) and (b) mean renal pulsatility index (PI) in clinical healthy control, dogs affected with chronic degenerative mitral valvular disease (CDMD group) along and dogs affected with CDMD and concurrent hyperadrenocorticism (HAC group). For each plot, the box represents the inter quartile range (IQR), the horizontal line in the middle of the box represents the median, and the whiskers denote the range. Outliers between 1.5 and 3 times the IQR are indicated by a circle
Chapter 3
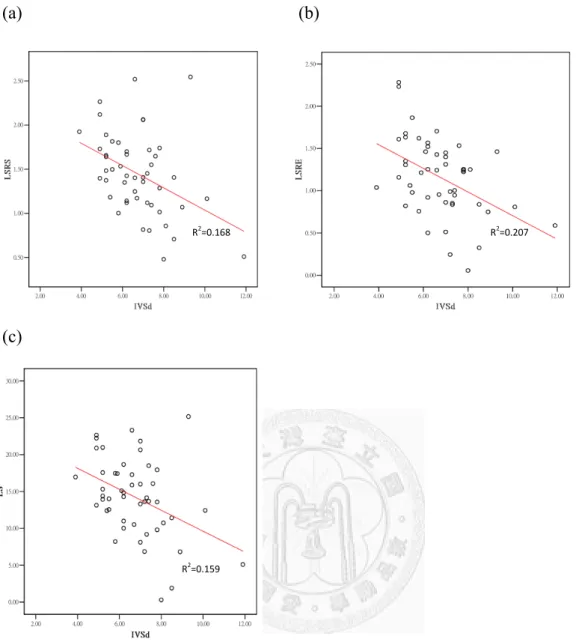
Figure 1. Variables correlated to interventricular septal thickness: 67 (a) systolic longitudinal strain rate, (b) peak early diastolic
longitudinal strain rate, and (c) peak systolic longitudinal strain.
All correlations were significant at P < .05
Chapter 1
General Introduction
Key to Abbreviations
2D-STE Two-dimensional speckle-tracking echocardiography A wave Maximal late diastolic mitral flow velocity
ACTH Adrenocorticotropic hormone
ADH Adrenal-dependent hyperadrenocorticism E wave Maximal early diastolic mitral flow velocity FS Fractional shortening
GFR Glomerular filtration rate
HAC Hyperadrenocorticism HCM Hypertrophic cardiomyopathy
PDH Pituitary- dependent hyperadrenocorticism PI Pulsatility index
RI Resistive index
TDI Tissue Doppler imaging
HYPERADRENOCORTICISM
Hyperadrenocorticism (HAC) is often called Cushing's syndrome, after Harvey Cushing, the neurosurgeon who first described the syndrome in humans in 1932.1 This disorder is characterized by physical and biochemical changes resulting from chronic exposure to elevated circulating glucocorticoid concentrations.2 The most common clinical signs of HAC are polydipsia, polyuria, polyphagia, lethargy, abdominal enlargement or potbelly, panting, obesity, muscle weakness, and recurrent urinary tract infections. The mean age at diagnosis is 11 years, and almost all dogs with HAC are older than 9 years of age.3 The main three types of HAC are pituitary-dependent hyperadrenocorticism (PDH), adrenal-dependent hyperadrenocorticism (ADH) and iatrogenic causes. Fifty-five percent to 60% of dogs affected with PDH and 60% to 65% of dogs affected with ADH are female.3
Pathophysiology
PDH is a common endocrine disease in dogs that accounts for 80–85% of spontaneous HAC2,4 and is associated with excessive adrenocorticotropin hormone (ACTH) secretion which induces bilateral adrenocortical hyperplasia and excess production of cortisol. ACTH is secreted by a microscopic tumor (microadenoma) of the pars distalis or the pars intermedia in most dogs with PDH.5,6 Grossly visible pituitary tumors (macroadenomas) account for only 10–30% of cases of PDH in dogs.7,8 In one study of 33 dogs, approximately 60% has noninvasive adenomas, whereas 35% had invasive adenomas and about 5% had pituitary adenocarcinoma.9
The remaining 15% to 20% of dogs of spontaneous hypercortisolism are ACTH-independent and result from autonomous hypersecretion of cortisol by an adrenocortical adenoma or adenocarcinoma (ADH).2 Cortisol production by the adrenal gland tumor lowers corticotropin-releasing hormone and ACTH secretion via
a negative feedback mechanism, resulting in atrophy of the unaffected adrenal gland and the normal cells of the involved adrenal gland.10 Most dogs of ADH are unilateral adrenal gland involved, the two glands being affected about equally. Bilateral adrenal tumors occur in about 10% of cases.11-14 Differentiation between adrenocortical adenoma and carcinomas on clinical is often difficult, but dogs with an adrenal diameter greater than 2 cm are more likely to have an adrenalcortical carcinoma.15
The effect on blood pressure
Hypertension is one of the most distinguishing features of spontaneous HAC, as it is present in 45-85% of adult patients16-18 and in 47% of children and adolescents patients.19,20 Likewise, systemic hypertension occurs in 32-70% of dogs with HAC.21-23 The pathophysiologic mechanism of hypertension in Cushing’s disease is complex and multifactioral affect, is characterized by: (1) activation of the
mineralocorticoid receptor (2) activation of the renin-angiotensin system (3) enhanced activity of vasoactive substances (vasopressin and angiotensin II) and reduced activity of depressor systems (nitric oxide synthase, prostacyclin, and kinin-kallikrein systems) (4) enhanced pressor responses to catecholamines.24-28
The effect on cardiovascular system
In patient with activate Cushing’s syndrome cardiovascular complications cause a mortality rate 4-fold higher than the age- and gender-matched general population.29 It also contributes to cardiac structural changes which were characterized by left
ventricular hypertrophy and concentric remodeling.30-35 All the human patients with HAC had evidence of asymmetric septal hypertrophy.32 In addition to cardiac structural change, cardiac diastolic dysfunction (e.g. reduced E/A ratio, prolonged E
conventional echocardiography.30,31,33-35 But using tissue Doppler imaging could detect myocardial dysfunction in early stage.33 The study of Pereira et al., which evaluate cardiac structural and functional changes in HAC patient with
two-dimensional speckle tracking (2D-STE) image, demonstrated that left ventricular shortening in the circumferential and longitudinal directions was significantly
impaired in Cushing patients compared to controls at short-term follow-up after transsphenoidal adenomectomy, indicated 2D-STE enabled an earlier detection of subtle changes in left ventricular systolic performance.34
The reasons why left ventricular hypertrophy in HAC is remain unknown.
Hypertension was thought to be the major factor in previous studies.36,37 But the increased blood pressure seems not to be essential for the development of initial structural changes in left ventricular wall, because an increase in left ventricular wall thickness could also be demonstrated in normotensive patients compared with controls.33,35 However, hypertensive patients with Cushing’s syndrome presented a more severe alteration of cardiac mass parameters compared with both normotensive patients and hypertensive controls, and proven to worsen cardiac parameters in patients with Cushing’s syndrome, even after remission of HAC. This finding suggests that hypertension is one of the main determinants of cardiac hypertrophy.31 Long-lasting exposure to excess circulating cortisol maybe another factor contribute to left ventricular hypertrophy in patients with Cushing’s syndrome. Several
ventricular structural changes occurred also in normotensive patients with Cushing’s syndrome, upon remission of HAC, most abnormalities in left ventricular mass measurements reversed, and the prevalence of abnormal measurements was markedly reduced, suggesting a direct role of cortisol on myocardial tissue.31 Tissue effect of cortisol could also include potentiation of cardiac angiotensin II and noradrenaline responsiveness or stimulation of the local renin–angiotensin system.38-40 Hypokalemia,
diabetes mellitus, and increased serum cortisol levels are important factors in the development of cardiac dysfunction in patients with adrenal Cushing’s syndrome.18
The effect on kidney
Glucocorticoids influence glomerular and tubular function in kidneys. Excess of glucocorticoids can cause alterations in renal parameters such as glomerular filtration rate (GFR) and urinary protein excretion. Otherwise, renal parenchyma is may influenced by excess glucocorticoids, too.
(1) Glomerular filtration rate
Short term administration of ACTH or Glucocorticoids increases GFR in humans, rats and dogs.41-43 Glucocorticoid-induced rise in GFR by several mechanisms, including plasma volume expansion due to sodium retention, increased plasma level of atrial natriuretic peptide and amino acid ,as well as increased glomerular
ultrafiltration coefficient.41,44,45 Long-term effects of Cushing’s syndrome in humans may decrease GFR, and the researcher also indicated that disease duration was the strongest predictor for a worse GFR.46 The same situation was noted on dogs, which decrease post-treatment GFR, urinary protein-to-creatinine ratio, urinary albumin to-creatinine ratio, urinary immunoglobulin G to-creatinine ratio, and urinary retinol-binding protein to-creatinine ratio.47
(2) Proteinuria/ microalbuminuria
The value of proteinuria as a marker of clinically important events in the kidney arises because it can occur and subsequently vary in magnitude because of altered vascular permeability of glomerular capillary walls (possibly marking the presence of immune complexes, vascular inflammation, or intra-glomerular hypertension) or impaired tubular handling of filtered proteins (possibly marking the presence of
excretion was associated with several machines, including elevated blood pressure and plasma glucose levels, and abnormalities in lipid metabolism which result of excessive free fatty acids binding to the protein.49,50 With a reported incidence of 44 to75%, pathological proteinuria is common in dogs affected with HAC.22,51,52
Presence of microalbuminuria and albuminuria in clinically healthy dogs and dogs affected with HAC was significantly different. The incidences of albuminuria was highest in dogs with ADH, followed by dogs with PDH, with the lowest levels in clinically healthy dogs; but microalbuminuria showed a different pattern which highest incidence in clinically healthy dogs, and lowest level in dogs with ADH.22 In human patients with HAC, urinary albumin excretion also increased before treatment but it was almost completely reversed after successful treatment of HAC.49 This finding was corroborated in a second report, which mainly involved cured subjects without an increase in microalbuminuria.46
(3) Renal parenchyma
In human patient, kidney biopsy was performed in three ADH patients with microalbuminuria showed normal glomeruli and mild, nonspecific tubular atrophy.49 Other renal histopathological findings in humans with Cushing’s syndrome included focal segmental glomerulosclerosis and membranoproliferative
glomerulonephritis.53,54 Glomerulonephritis and amyloidosis have been described in dogs with HAC.52,55 But a cause-effect relationship between Cushing’s syndrome and these renal lesions remains uncertain.
SPECKLE TRACKING ECHOCARDIOGRAPHY
Speckle tracking echocardiography (STE) is a new, non-invasive method for the assessment of left ventricular global and regional function. Similar to tissue Doppler
imaging (TDI), it permits offline calculation of myocardial velocities and deformation parameters such as strain and strain rate. However, in comparison to TDI, STE is insonation angle independent and does not require such high frame rates, and is not influenced by passive traction of scar tissue by adjacent vital myocardium. Speckle tracking is an echocardiographic method based on tracking of characteristic speckle patterns created by interference of ultrasound beams in the myocardium.56
The image-processing algorithm tracks user-defined regions of interest which are comprised of blocks of approximately 20 to 40 pixels containing stable patterns that are described as ‘‘speckles’’. Single speckles are merged in functional units (kernels) and each kernel constitutes a sort of ultrasound fingerprint that can be tracked by software during the entire cardiac cycle. Through analysis of the motion of each kernel that composes a routine two dimensional gray scale image, the system can calculate displacement, the rate of displacement (velocity), deformation (strain), and the rate of deformation (strain rate) of the selected myocardial segments and left ventricle rotation.57 Strain is a dimensionless quantity of myocardial deformation. The so-called Langrangian strain is mathematically defined as the change of myocardial fiber length during stress at end-systole compared to its original length in a relaxed state at end-diastole (L-L0)/L0.58 It is expressed as a percentage (%). The change of strain per unit of time is referred to as strain rate. The strain rate represents the myocardial deformation rate. It is expressed as seconds–1(1/s). As strain rate (1/s) is the spatial derivative of tissue velocity (cm/s), and strain (%) is the temporal integral of strain rate, all of these three parameters are mathematically linked to each other.
Otherwise, speckle analysis is the ability to examine several components or planes in a single data set. Three different components of contraction have been defined:
longitudinal, radial, and circumferential.59
(2) Radial deformation in the short axis is perpendicular to both long axis and epicardium. Thus, radial strain represents myocardial thickening and thinning.
(3) Circumferential strain is defined as the change of the radius in the short axis, perpendicular to the radial and long axes.
Longitudinal deformation is assessed from the apical 4-chamber views while circumferential and radial deformations are assessed from short axis views of the left ventricle. The description of these three aforementioned ‘normal strains’- which can be measure using current STE technology- allows a good approximation of active cardiac motion. However, they still represent a simplification. When considering myocardial deformation during contraction in three dimensional space, six more
‘shear strains’ can be defined in addition to the normal strains.60
Clinical applications on left ventricular hypertrophy
In hypertrophic cardiomyopathy (HCM), malfunctioning sarcomeric protein, myocyte hypertrophy, fiber disarray, and interstitial fibrosis which result in left ventricular systolic and diastolic dysfunction.61,62 STE has been used in distinguishing the different causes of left ventricular hypertrophy. Investigations with tissue
Doppler–derived strains previously reported that longitudinal myocardial deformation is markedly attenuated in HCM, and the extent and pattern of regional abnormalities show wide regional heterogeneity63 which helps distinguish HCM from athlete’s left ventricular hypertrophy.64 The ability of strain rate imaging derived from TDI to discriminate HCM from hypertensive left ventricular hypertrophy. The mean values of systolic strain cutoff value of -10.6% was associated with a sensitivity of 85.0%, specificity of 100%, and predictive accuracy of 91.2% for discrimination between these 2 conditions.65 Subclinical myocardial changes in left ventricular hypertrophy also could detect by STE. Despite an apparently normal left ventricular systolic
function based on conventional echocardiography, all strain, longitudinal, radial and circumferential components were significantly reduced in patients with HCM.66 The amount and location of left ventricular fibrosis and end-diastolic wall thickness are independent predictors of end-systolic longitudinal strain.67 Similarly, patients with active Cushing’s syndrome showed impaired left ventricular shortening in the circumferential and longitudinal directions. After normalization of corticosteroid excess, left ventricular circumferential and longitudinal shortening occurred, suggest STE is a valuable tool to detect subtle left ventricular dysfunction.34 The prospective study which evaluates longitudinal myocardial strain to assess systolic function in healthy cats and in various stages of feline HCM demonstrate that systolic myocardial strain is already decreased in mild forms of HCM and decreases more in more severe HCM stages. Hence, strain analysis appears to be a more sensitive index of
myocardial function than standard left ventricular function assessment.68
RESISTIVE INDEX AND PULSATILITY INDEX
Doppler ultrasound can be used to record the velocity profile non-invasively from most peripheral vessels. During ultrasound examination, the wave is sent from a stationary transducer and the moving red blood cells reflected wave towards the transducer, which result in the frequency shift (Δf) could indirectly measure the red blood cell velocity (V). The relationship between Δf and V is:
Δf 2f VCosθ c
Where Δf is the frequency shift, f0 is the transmitted frequency, V is the blood velocity, Cosθ is the insonation angle, between the ultrasound beam and the direction of motion (blood flow vector) and c is the sound velocity in tissue.
Flow measurements providing indirect information of peripheral vascular resistance can be obtained from this spectral display. Some indices have been developed to estimate vascular resistance and to evaluate and compare Doppler waveforms. These indices can be calculated from ratios including peak systolic velocity, end diastolic velocity, and mean velocity through the cardiac cycle.69
The two primary indexes used clinically are resistive index (RI) and pulsatility index (PI). RI and PI were calculated by the following equation:
RI peak systolic velocity peak end diastolic velocity peak systolic velocity
PI peak systolic velocity peak end diastolic velocity mean velocity through the cardiac cycle
These indices are advanced as a useful parameter for quantifying the changes in vascular resistance from many diseases. For instance, alteration in hepatic RI have been identified with hepatic disorders,70 higher splanchnic vascular resistance detected on acute pancreatitis,71 and higher RI and PI on metastatic lymphoma nodes.72 Several studies have also evaluated the benefit of using renal RI and PI in renal and urinary abnormalities.73
The kidney is a well- vascularized organ which receiving on average
approximately 20– 25% of the total cardiac output. Many renal diseases have an important vascular component and some systemic diseases, such as hypertension, are mediated by the vascular control system of the juxtaglomerular apparatus. This fact makes the kidney a suitable organ to be evaluated by Doppler.
Renal RI and PI are measured on the blood velocity waveform obtained by placing the sample on the renal interlobar arteries or arcuate arteries. Waveforms should be optimized for measurement using the highest frequency probe, the lowest pulse repetition frequency without aliasing, the highest gain without obscuring background noise, and the lowest wall filter.74 Several factors can produce increased renal RI and
PI, not only dependent on renal vascular resistance but also affected by other confounding factors, including patient characteristics (age, renal disease, arterial disease),73,75 central hemodynamics (heart rate, pulse pressure),76,77 intra-abdominal pressure,78 and renal vascular compliance.77,79 In clinical application, measurement of renal RI and PI are widely used in the evaluation of renal parenchymal and vascular damage, renal failure, and transplantation.73,80 Furthermore, RI of intrarenal arteries has been shown to be associated with the severity of target organ damage in patients with hypertension81 and diabetes mellitus,82 as well as in dogs with hepatic
disorders,83 HAC, diabetes mellitus,21 and degenerative mitral valve disease.84 In summary, renal RI and PI is useful for the evaluation of renal parenchymal injury and other systemic disease which with renal hemodynamics changes.
Reference:
1. Cushing H. The basophil adenomas of the pituitary body and their clinical manifestations (Pituitary Basophilism). Bull Johns Hopkins Hosp 1932;50:137-195.
2. Feldman EC, Nelson RW. Hyperadrenocorticism (Cushing's syndrome). In:
Feldman EC, Nelson RW, eds. Canine and Feline Endocrinology and Reproduction.
Philadelphia: WB Saunders; 2004:252-357.
3. Reusch CE, Feldman EC. Canine hyperadrenocorticism due to adrenocortical neoplasia. Pretreatment evaluation of 41 dogs. J Vet Intern Med 1991;5:3-10.
4. Feldman EC. Distinguishing dogs with functioning adrenocortical tumors from dogs with pituitary-dependent hyperadrenocorticism. J Am Vet Med Assoc
1983;183:195-200.
5. Feldman EC, Nelson RW. Neoplasms in the adenohypophysis of dogs. A clinical and pathologic study. Vet Pathol 1967;4:301-325.
6. Peterson ME, Krieger DT, Drucker WD, et al. Immunocytochemical study of the hypophysis in 25 dogs with pituitary-dependent hyperadrenocorticism. Acta
Endocrinol 1982;101:15-24.
7. Pollard RE, Reilly CM, Uerling MR, et al. Neurologic, endocrinologic, and pathologic findings associated with large pituitary tumors in dogs: eight cases. J Am Vet Med Assoc 2010;24:160-165.
8. Nelson RW, Ihle SL, Feldman EC. Pituitary macroadenomas and
macroadenocarcinomas in dogs treated with mitotane for pituitary-dependent hyperadrenocorticism: 13 cases (1981-1986). J Am Vet Med Assoc
1989;194:1612-1617.
9. Pollard RE, Reilly CM, Uerling MR, et al. Cross-Sectional Imaging
Characteristics of Pituitary Adenomas, Invasive Adenomas and Adenocarcinomas in Dogs: 33 Cases (1988 –2006). J Vet Intern Med 2010;24:160-165.
10. Ettinger SJ, Feldman EC. Textbook of veterinary internal medicine : diseases of the dog and the cat. St. Louis, Mo.: Elsevier Saunders; 2010.
11. Hoerauf A, Reusch C. Ultrasonographic characteristics of both adrenal glands in 15 dogs with functional adrenocortical tumors. J Am Anim Hosp Assoc
1999;35:193-199.
12. Anderson CR, Birchard SJ, Powers BE, et al. Surgical treatment of
adrenocortical tumors: 21 cases (1990-1996). J Am Anim Hosp Assoc 2001;37:93-97.
13. Ford SL, Feldman EC, Nelson RW. Hyperadrenocorticism caused by bilateral adrenocortical neoplasia in dogs: four cases (1983-1988). J Am Vet Med Assoc 1993;202:789-792.
14. Kyles AE, Feldman EC, De Cock HE, et al. Surgical management of adrenal gland tumors with and without associated tumor thrombi in dogs: 40 cases
(1994-2001). J Am Vet Med Assoc 2003;223:654-662.
15. Labelle P, Kyles AE, Farver TB, et al. Indicators of malignancy of canine adrenocortical tumors: histopathology and proliferation index. Vet Pathol 2004;41:490-497.
16. Colao A, Pivonello R, Spiezia S, et al. Persistence of increased cardiovascular risk in patients with Cushing's disease after five years of successful cure. J Clin Endocrinol Metab 1999;84:2664-2672.
17. Mancini T, Kola B, Mantero F, et al. High cardiovascular risk in patients with Cushing's syndrome according to 1999 WHO/ISH guidelines. Clin Endocrinol (Oxf) 2004;61:768-777.
18. Tsuiki M, Tanabe A, Takagi S, et al. Cardiovascular risks and their long-term clinical outcome in patients with subclinical Cushing's syndrome. Endocr J
2008;55:737-745.
19. Magiakou MA, Mastorakos G, Oldfield EH, et al. Cushing's syndrome in children and adolescents. Presentation, diagnosis, and therapy. N Engl J Med 1994;331:629-636.
20. Magiakou MA, Mastorakos G, Zachman K, et al. Blood pressure in children and adolescents with Cushing's syndrome before and after surgical care. J Clin Endocrinol Metab 1997;82:1734-1738.
21. Novellas R, de Gopegui RR, Espada Y. Determination of renal vascular resistance in dogs with diabetes mellitus and hyperadrenocorticism. Vet Rec 2008;163:592-596.
22. Lien YH, Hsiang TY, Huang HP. Associations among systemic blood pressure, microalbuminuria and albuminuria in dogs affected with pituitary- and
adrenal-dependent hyperadrenocorticism. Acta Vet Scand 2010;52:61.
23. Goy-Thollot I, Péchereau D, Kéroack S, et al. Investigation of the role of aldosterone in hypertension associated with spontaneous pituitary-dependent hyperadrenocorticism in dogs. J Small Anim Pract 2002;43:489-492.
24. Ulick S, Wang JZ, Blumenfeld JD, et al. Cortisol inactivation overload: a mechanism of mineralocorticoid hypertension in the ectopic adrenocorticotropin syndrome. J Clin Endocrinol Metab 1992;74:963-967.
25. Saruta T, Suzuki H, Handa M, et al. Multiple factors contribute to the pathogenesis of hypertension in Cushing's syndrome. J Clin Endocrinol Metab 1986;62:275-279.
26. Saruta T. Mechanism of glucocorticoid-induced hypertension. Hypertens Res 1996;19:1-8.
27. Kirilov G, Tomova A, Dakovska L, et al. Elevated plasma endothelin as an additional cardiovascular risk factor in patients with Cushing's syndrome. Eur J
Endocrinol 2003;149:549-553.
28. Sakaue M, Hoffman BB. Glucocorticoids induce transcription and expression of the alpha 1B adrenergic receptor gene in DTT1 MF-2 smooth muscle cells. J Clin Invest 1991;88:385-389.
29. Boscaro M, Barzon L, Fallo F, et al. Cushing's syndrome. Lancet 2001;357:783-791.
30. Baykan M, Erem C, Gedikli O, et al. Assessment of left ventricular diastolic function and Tei index by tissue Doppler imaging in patients with Cushing's Syndrome. Echocardiography 2008;25:182-190.
31. Toja PM, Branzi G, Ciambellotti F, et al. Clinical relevance of cardiac structure and function abnormalities in patients with Cushing's syndrome before and after cure.
Clin Endocrinol (Oxf) 2012;76:332-338.
32. Sugihara N, Shimizu M, Kita Y, et al. Cardiac characteristics and postoperative courses in Cushing's syndrome. Am J Cardiol 1992;69:1475-1480.
33. Bayram NA, Ersoy R, Aydin C, et al. Assessment of left ventricular functions by tissue Doppler echocardiography in patients with Cushing's disease. J Endocrinol Invest 2009;32:248-252.
34. Pereira AM, Delgado V, Romijn JA, et al. Cardiac dysfunction is reversed upon successful treatment of Cushing's syndrome. Eur J Endocrinol 2010;162:331-340.
35. Muiesan ML, Lupia M, Salvetti M, et al. Left ventricular structural and functional characteristics in Cushing's syndrome. J Am Coll Cardiol
2003;41:2275-2279.
36. Cushing H. The basophil adenomas of the pituitary body and their clinical manifestations. Bull Johns Hopkins Hasp 1932;50:137-195.
37. Scholz DA, Sprague RG, Kernohan JW. Cardiovascular and renal complications of Cushing's syndrome. N Engl J Med 1957;256:833-837.
38. Sudhir K, Jennings GL, Esler MD, et al. Hydrocortisone-induced hypertension in humans: pressor responsiveness and sympathetic function. Hypertension
1989;13:416-421.
39. Dzau VJ. Cardiac renin-angiotensin system. Molecular and functional aspects.
Am J Med 1988;84:22-27.
40. Ritchie CM, Sheridan B, Fraser R, et al. Studies on the pathogenesis of hypertension in Cushing's disease and acromegaly. Q J Med 1990;76:855-867.
41. Connell JM, Whitworth JA, Davies DL, et al. Effects of ACTH and cortisol administration on blood pressure, electrolyte metabolism, atrial natriuretic peptide and renal function in normal man. J Hypertens 1987;5:425-433.
42. Davis JO, Howell DS. Comparative effect of ACTH, cortisone and DCA on renal function, electrolyte excretion and water exchange in normal dogs.
Endocrinology 1953;52:245-255.
43. Wen C, Fraser T, Li M, et al. Hemodynamic profile of corticotropin-induced hypertension in the rat. J Hypertens 1998;16:187-194.
44. Hall JE, Morse CL, Smith MJ, Jr., et al. Control of arterial pressure and renal function during glucocorticoid excess in dogs. Hypertension 1980;2:139-148.
45. Manning RD, Jr. Renal hemodynamic, fluid volume, and arterial pressure changes during hyperproteinemia. Am J Physiol 1987;252:F403-411.
46. Haentjens P, De Meirleir L, Abs R, et al. Glomerular filtration rate in patients with Cushing's disease: a matched case-control study. Eur J Endocrinol
2005;153:819-829.
47. Smets PM, Lefebvre HP, Meij BP, et al. Long-Term Follow-Up of Renal Function in Dogs after Treatment for ACTH-Dependent Hyperadrenocorticism. J Vet Intern Med 2012;26:565-574.
48. Lees GE, Brown SA, Elliott J, et al. Assessment and management of proteinuria in dogs and cats: 2004 ACVIM Forum Consensus Statement (small animal). J Vet Intern Med 2005;19:377-385.
49. Koh JM, Kim JY, Chung YE, et al. Increased urinary albumin excretion in Cushing's syndrome: remission after correction of hypercortisolaemia. Clin Endocrinol (Oxf) 2000;52:349-353.
50. Hayashi Y, Morikawa A, Makino M. Heterogeneity of urinary albumin from diabetic patients. Clin Chim Acta 1990;190:93-103.
51. Hurley KJ, Vaden SL. Evaluation of urine protein content in dogs withpituitary-dependent hyperadrenocorticism. J Am Vet Med Assoc 1998;212:369-373.
52. Ortega TM, Feldman EC, Nelson RW, et al. Systemic arterial blood pressure and urine protein/creatinine ratio in dogs with hyperadrenocorticism. Journal of the
American Veterinary Medical Association 1996;209:1724-1729.
53. Hsieh Ck Fau - Hsieh YP, Hsieh Yp Fau - Wen YK, Wen Yk Fau - Chen ML, et al. Focal segmental glomerulosclerosis in association with Cushing's disease. 2007.
54. Tatsumi T, Morishima T, Watarai T, et al. Recurrent Cushing's disease associated with nephrotic syndrome. Intern Med 1995;34:10-14.
55. Center SA, Smith CA, Wilkinson E, et al. Clinicopathologic, renal
immunofluorescent, and light microscopic features of glomerulonephritis in the dog:
41 cases (1975-1985). J Am Vet Med Assoc 1987;190:81-90.
56. Bohs LN, Trahey GE. A novel method for angle independent ultrasonic imaging of blood flow and tissue motion. IEEE Trans Biomed Eng 1991;38:280-286.
57. Perk G, Tunick PA, Kronzon I. Non-Doppler two-dimensional strain imaging by echocardiography--from technical considerations to clinical applications. J Am Soc
Echocardiogr 2007;20:234-243.
58. Urheim S, Edvardsen T, Torp H, et al. Myocardial strain by Doppler echocardiography. Validation of a new method to quantify regional myocardial function. Circulation 2000;102:1158-1164.
59. Blessberger H, Binder T. Two dimensional speckle tracking echocardiography:
clinical applications. Heart 2010;96:2032-2040.
60. Pavlopoulos H, Nihoyannopoulos P. Strain and strain rate deformation parameters: from tissue Doppler to 2D speckle tracking. Int J Cardiovasc Imaging 2008;24:479-491.
61. Unverferth DV, Baker PB, Pearce LI, et al. Regional myocyte hypertrophy and increased interstitial myocardial fibrosis in hypertrophic cardiomyopathy. Am J Cardiol 1987;59:932-936.
62. Varnava AM, Elliott PM, Sharma S, et al. Hypertrophic cardiomyopathy: the interrelation of disarray, fibrosis, and small vessel disease. Heart 2000;84:476-482.
63. Sengupta PP, Mehta V, Arora R, et al. Quantification of regional nonuniformity and paradoxical intramural mechanics in hypertrophic cardiomyopathy by high frame rate ultrasound myocardial strain mapping. J Am Soc Echocardiogr 2005;18:737-742.
64. Rajiv C, Vinereanu D, Fraser AG. Tissue Doppler imaging for the evaluation of patients with hypertrophic cardiomyopathy. Curr Opin Cardiol 2004;19:430-436.
65. Kato TS, Noda A, Izawa H, et al. Discrimination of nonobstructive hypertrophic cardiomyopathy from hypertensive left ventricular hypertrophy on the basis of strain rate imaging by tissue Doppler ultrasonography. Circulation 2004;110:3808-3814.
66. Serri K, Reant P, Lafitte M, et al. Global and regional myocardial function quantification by two-dimensional strain: application in hypertrophic cardiomyopathy.
J Am Coll Cardiol 2006;47:1175-1181.
67. Popović ZB, Kwon DH, Mishra M, et al. Association between regional
ventricular function and myocardial fibrosis in hypertrophic cardiomyopathy assessed by speckle tracking echocardiography and delayed hyperenhancement magnetic resonance imaging. J Am Soc Echocardiogr 2008;21:1299-1305.
68. Wess G, Sarkar R, Hartmann K. Assessment of left ventricular systolic function by strain imaging echocardiography in various stages of feline hypertrophic
cardiomyopathy. J Vet Intern Med 2010;24:1375-1382.
69. Nelson TR, Pretorius DH. The Doppler signal: where does it come from and what does it mean? AJR Am J Roentgenol 1988;151:439-447.
70. García-Criado A, Gilabert R, Salmerón JM, et al. Significance of and
contributing factors for a high resistive index on Doppler sonography of the hepatic artery immediately after surgery: prognostic implications for liver transplant
recipients. AJR Am J Roentgenol 2003;181:831-838.
71. Topal NB, Kaya E, Ercan I, et al. The role of Doppler sonography in predicting severity of acute pancreatitis. J Clin Ultrasound 2008;36:141-147.
72. Nyman HT, Kristensen AT, Skovgaard IM, et al. Characterization of normal and abnormal canine superficial lymph nodes using gray-scale B-mode, color flow
mapping, power, and spectral Doppler ultrasonography: a multivariate study. Vet Radiol Ultrasound 2005;46:404-410.
73. Rivers BJ, Walter PA, Polzin DJ, et al. Duplex doppler estimation of intrarenal pourcelot resistive index in dogs and cats with renal disease. J Vet Intern Med 1997;11:250-260.
74. Tublin ME, Bude RO, Platt JF. Review. The resistive index in renal Doppler sonography: where do we stand? AJR Am J Roentgenol 2003;180:885-892.
75. Chang YJ, Chan IP, Cheng FP, et al. Relationship between age, plasma renin activity, and renal resistive index in dogs. Vet Radiol Ultrasound 2010;51:335-337.
76. Mostbeck GH, Gossinger HD, Mallek R, et al. Effect of heart rate on Doppler measurements of resistive index in renal arteries. Radiology 1990;175:511-513.
77. Tublin ME, Tessler FN, Murphy ME. Correlation between renal vascular resistance, pulse pressure, and the resistive index in isolated perfused rabbit kidneys.
Radiology 1999;213:258-264.
78. Umgelter A, Reindl W, Franzen M, et al. Renal resistive index and renal
function before and after paracentesis in patients with hepatorenal syndrome and tense ascites. Intensive Care Med 2009;35:152-156.
79. Bude RO, Rubin JM. Relationship between the resistive index and vascular compliance and resistance. Radiology 1999;211:411-417.
80. Novellas R, Ruiz de Gopegui R, Espada Y. Assessment of renal vascular resistance and blood pressure in dogs and cats with renal disease. Vet Rec 2010;166:618-623.
81. Raff U, Schmidt BM, Schwab J, et al. Renal resistive index in addition to low-grade albuminuria complements screening for target organ damage in therapy-resistant hypertension. J Hypertens 2010;28:608-614.
82. Ohta Y, Fujii K, Arima H, et al. Increased renal resistive index in atherosclerosis and diabetic nephropathy assessed by Doppler sonography. J Hypertens
2005;23:1905-1911.
83. Novellas R, de Gopegui RR, Espada Y. Increased renal vascular resistance in dogs with hepatic disease. Vet J 2008;178:257-262.
84. Chetboul V, Daste T, Gouni V, et al. Renal resistive index in 55 dogs with degenerative mitral valve disease. J Vet Intern Med 2012;26:101-108.
Chapter 2
Vascular Resistance and Albuminuria in Dogs Affected with Chronic Hyperadrenocorticism and
Chronic Degenerative Mitral Valvular Disease
Key to Abbreviations ACTH Adrenocorticotropic hormone
ADH Adrenal-dependent hyperadrenocorticism
ALKP Alkaline phosphatase
ALT Alanine transaminase
BUN Blood urea nitrogen
CDMD Chronic degenerative mitral valvular disease CV Coefficients of variations
HAC Hyperadrenocorticism HPF High power of field
ISACHC International Small Animal Cardiac Health Council PDH Pituitary- dependent hyperadrenocorticism
PI Pulsatility index RI Resistive index SD Standard deviation
UACR Urinary albumin:creatinine ratio
Vascular Resistance and Albuminuria in Dogs Affected with Chronic Hyperadrenocorticism and Chronic Degenerative Mitral Valvular Disease
Hung-Yin Chen, Hui-Pi Huang
Department of Veterinary Medicine, National Taiwan University, Taipei, Taiwan.
Background: Hypertension and increased peripheral vascular resistance is associated with hyperadrenocorticism (HAC).
Hypothesis/Objectives: Microalbuminuria is associated with increased systemic blood pressure, resistive index (RI) and pulsatility index (PI) of the renal artery and aorta in dogs affected with chronic degenerative mitral valvular disease (CDMD) with and without HAC in dogs.
Animals: 25 clinical healthy controls, 27 age-matched dogs affected with CDMD, and 20 dogs with spontaneous HAC and concurrent CDMD
Methods: A non-invasive blood pressure measurement, routine blood workups, echocardiography, abdominal Doppler sonography, and urine albumin analysis.
Results: Systolic blood pressure, mean renal RI, and mean renal PI were
significant higher in dogs with spontaneous HAC and concurrent CDMD compared with other 2 groups (P = .002, P < .001, and P < .001, respectively). The prevalence of increased renal vascular resistance and albuminuria were higher in dogs with HAC and concurrent CDMD compared with other 2 groups (P < .001 and P < .001,
respectively). No significant differences in aortal RI (P = .124) or aortal PI (P = .067) were found among all groups. In general, the presence of albuminuria was associated with increased renal RI (r = .421, P < .001). No correlation among blood pressure, renal RI, PI and albuminuria was found.
Conclusion and Clinical Importance: Presence of microalbuminuria and
albuminuria might be associated with increased vascular resistance within the kidneys of dogs with HAC, but was not associated with increased systemic pressure, and concurrent CDMD.
Key words: canine, hyperadrenocorticism, resistive index, pulsatility index, microalbuminuria
Part of the study is going to present as an abstract in the 22nd European College of Veterinary Internal Medicine Congress, Maastricht, the Netherlands. Sep. 6-8, 2012.
Introduction
Hyperadrenocorticism (HAC) is a frequent endocrine disorder in middle-aged and older dogs. Up to 86% of dogs with untreated HAC have systemic hypertension and up to 75% have proteinuria.1,2 Glucocorticoid-induced hypertension results from several pathophysiological mechanisms, including increased cardiac output, total peripheral resistance and renal vascular resistance.3 Systemic hypertension leads to an increased capillary hydrostatic pressure and hyperfiltration, may eventually result in glomerulosclerosis and proteinuria. Proteinuria and systemic hypertension are major complications in development and progression of chronic kidney disease in dogs with chronic renal failure.4,5 Several studies have demonstrated that a correlation between human patients affected with HAC and renal failure. One case-control study reported patients with Cushing’s disease have a decreased glomerular filtration rate.6
Creatinine clearance was lower in patients with active and cured Cushing’s disease compared with controls.7 In addition, a highly significant correlation between endogenous glucocorticoid production and the progression rate of chronic renal failure has been described.8 In dogs, glomerular markers (urinary protein-to-creatinine ratio, urinary albumin and urinary immunoglobulin) and tubular markers (urinary retinol-binding protein and urinary N-acetyl-b-D-glucoseaminidase) were
significantly higher in the dogs with HAC compared with control dogs, which indicated glomerular and tubular dysfunction.9 Research regarding renal vascular resistance of dogs affected with HAC also indicated that the mean values of resistive index (RI) and pulsatility index (PI) in the dogs with HAC were significant higher than health control dogs, suggesting that the dogs with HAC had a higher vascular resistance.10
Renal RI and PI were a useful parameter for quantifying the alterations in renal blood flow that occur with renal or systemic disease. By analysis of the blood flow
velocity waveform these indices are widely accepted as indicators of vascular resistance. In human medicine, the renal RI and PI are widely used to assess renal vascular resistance in diseases involving essential hypertension, acute and chronic renal failure and, diabetes mellitus.11-16 Not only renal vascular, RI and PI also used in different major abdominal blood vessels to predicting the severity of disease in the early stage or organ perfusion changes after transplantation17,18
The aim of the study was to report systemic blood pressure, RI and PI of the renal artery and aorta, as well as the presence of microalbuminuria in dogs affected with HAC and chronic degenerative mitral valvular disease (CDMD).
Materials and Methods Animals
Seventy-two client-owned dogs that presented to the National Taiwan University Veterinary Hospital since November 2010 to April 2012 were enrolled in this study.
These dogs were categorized into clinical healthy controls, dogs affected with CDMD, dogs with CDMD and concurrent spontaneous HAC. All dogs underwent physical examination, blood pressure measurements, routine blood work (complete blood counts and biochemical profiles) examinations, conventional echocardiography, renal and aorta ultrasonography and freshly voided urine samples collected.
Dogs that had acute renal failure, hydronephrosis and nephrolithiasis were excluded from the study.
Clinically healthy dogs (control)
Twenty-five were included as healthy controls, 14 were males and 11 were females.
The breeds represented in this groups including 13 miniature Dachshunds, 5 Maltese terriers, 2 each of Chihuahuas, Mongrels and toy Poodles and 1 miniature Schnauzer.
The median age of these dogs was 3.2 ± 1.9 years (range 1 to 7 years) and the mean body weight was 5.5 ± 2.3 kg (range 2.2 to 13 kg).
Dogs affected with CDMD along (CDMD group)
Twenty-seven dogs included in this group, 11 were males and 16 were females.
The mean age was 11.7 ± 2.6 years (range 7 to 17 years) and the mean body weight was 9.3 ± 8.1 kg (range 2.4 to 32 kg). The following breeds were represented: 11 Maltese terriers, 7 Mongrels, 3 miniature Schnauzers, 2 Yorkshire terriers, 1 each of English Cocker Spaniel, Labrador Retriever, Pomeranian, and Shih-Tzu.
Diagnosis of CDMD was based on echocardiographic evidence of degenerative lesions of mitral valves and mitral regurgitation. Dogs with CDMD were classified by International Small Animal Cardiac Health Council (ISACHC) classification system:
13 dogs were into ISACHC class 1, 11 were into class 2, and 3 dogs were into class 3.
Dogs affected with CDMD concurrent with HAC (HAC group)
Twenty dogs affected with HAC were included in this group; 15 dogs affected with pituitary-dependent hyperadrenocorticism (PDH) and 5 dogs affected with
adrenal-dependent hyperadrenocorticism (ADH). The mean age of the 20 dogs with HAC was 12.3 ± 2.5 years (range 8 to 17 years), with a mean body weight of 7.0 ± 4.2 kg (range 3.5 to 15.3 kg), 17 were females and 3 were males. Breeds represented in this group were 6 Maltese terriers, 4 Mongrels, 3 Pomeranians, 2 each of Shih-Tzus and Yorkshire terriers, 1 each of miniature Dachshund, miniature Schnauzer and Whippet.
Diagnosis of CDMD was used the same criteria as described above. Nine was classified as ISACHC class 1, 11 were in the ISACHC class 2, and none in the
polyuria, polyphagia, alopecia, heat intolerance, lethargy, and abdominal enlargement), increased plasma hepatic enzyme activities, and affirmative results of
adrenocorticotropic hormone (ACTH) stimulation test of post-ACTH cortisol concentration > greater than 20 µg/dl one hour after intramuscular administration of 0.25 mg synthetic ACTH (Cortrosyn, Organon, The Netherlands).19 Differentiation of PDH and ADH was based on adrenal morphological assessment.20,21 Bilaterally symmetrical maintenance of the normal adrenal shape and contour, and homogeneous echogenicity were classified as PDH; whereas adrenal glands with an irregular, rounded shape and mixed echogenicity were classified as ADH.20,21
Systemic blood pressure measurement
Systolic blood pressure was evaluated using the indirect method of Doppler flow detector with a 9.5 MHz transducer.a Dogs were considered as hypertensive if the average systemic blood pressure exceeded 160 mmHg.22
Renal Doppler Ultrasonography
Hairs of the ventral abdomen and left flank areas were clipped and cleaned, and then acoustic coupling gel was applied onto the skin surface. The dogs were in right or left lateral recumbency to scan the uppermost kidney and no sedation was required.
Triplex Doppler ultrasonography was performed by a single operator (HYC) using an ultrasound machineb with a high-resolution multi-frequency Convex probe (4-8 MHz).
Using color Doppler to visualize the intrarenal vasculature and then detecting renal blood flow on one of the interlobar or arcuate arteries by pulsed Doppler. The smallest scale that displayed the flow without aliasing was selected. The mean RI and PI for each kidney were determined by averaging a total of nine Doppler waveforms at the arteries at three separate locations.23,24 RI and PI were calculated by the following
equation:
RI peak systolic velocity peak end diastolic velocity peak systolic velocity
PI peak systolic velocity peak end diastolic velocity mean velocity through the cardiac cycle
Aorta Doppler ultrasonography
Aorta Doppler ultrasonography was obtained with the animal in right lateral recumbency. Aorta waveforms were obtained with pulsed Doppler ultrasound and aorta RI and PI were calculated by mean of six Doppler waveforms by the machine software applications.
Microalbuminuria assay and urinary albumin:creatinine ratio
The freshly voided urine samples were collected. Samples of hematuria (≥ 10 RBC/high power of field), pyuria (≥ 5 WBC/HPF), and bacteriuria were excluded from the study. The urine albumin and creatinine concentrations were
semi-quantitatedc and urinary albumin:creatinine ratio (UACR) was calculated accordingly. In this study, no microalbuminuria, microalbuminuria and albuminuria were defined as UACR < 30 mg/g (0.03), 30-300 mg/g (0.03-0.3), and > 300 mg/g (0.3), respectively.
Statistical analysis
The results of data were expressed as mean ± standard deviation (SD). The Kolomogorov-Smirnov test was used for testing normal distribution of all data with commercial computer statistics software.d
One-way ANOVA with Bonferroni correction was used for the normally distributed data to make comparison between groups, while the non-normally distributed data
were analyzed by using Kruskal-Wallis test. Chi-square statistic was used to assess differences of categorical variables between groups. Left and right interlobar RI
values were compared in each class by a paired t-test. The relationship between RI, PI, age and blood pressure was assessed with Pearson’s correlation coefficient. The
relationships between RI, PI and UACR were assessed with Spearman’s correlation coefficient.
The intra-observer coefficients of variations (CV) of the RI and PI were calculated by a variance component analysis. The CV was determined by dividing the SD value by the overall mean. Six clinical healthy dogs were scanned on three nonconsecutive occasions within one day by the same examiner (HYC), who was unaware of values from the first examination.
All tests were two-tailed and the P value < .05 was considered statistically significant.
Results
Baseline characteristics of the study population are shown in Table 1. The age of clinical healthy control was significant younger than CDMD and HAC groups (P
< .001). No significant differences in body weight (P = .055) were found among all groups. The systemic blood pressure and body condition score was significant higher in HAC group compared with control group (P = .002 and P = .018, respectively).
Prevalence of hypertension among control, CDMD and HAC groups were 4% (1/25), 4% (1/27) and 30% (6/20), respectively. The prevalence of hypertension was also significantly different among groups (P = .007). Plasma ALKP concentration was significantly higher in HAC group compared with control and CDMD group (P
= .002). Plasma urea and creatinine concentrations were significantly lower in control group than CDMD group (P = .013 and P = .001, respectively). No significances in
plasma albumin, ALT, glucose and total protein concentrations were found among all groups (P = .172, P = .067, P = .403 and P = .869, respectively). (Table 1)
The RI and PI of right and left kidneys were not different in all dogs (P = .103 and P = .175, respectively). Both right and left renal RI of the HAC group were
significantly higher than the indices of the control and CDMD group (P < .001 and P
< .001, respectively). Similarly, both right and left renal PI were significantly higher than the indices of the control and CDMD group (P < .001 and P < .001, respectively, Table 2). The means of renal RI and PI are also presented graphically in Figure 1. The upper cut-off values for renal RI and PI were calculated as the mean + 2 SD of the indices of the clinical healthy controls and were 0.70 for renal RI and 1.45 for renal PI.
Based on these upper limits, the prevalence of increased renal vascular resistance of the dogs in control group (1/25, 4%), CDMD group (2/27, 7%) and HAC group (10/20, 50%) were significantly different (P < .001). However, no significant
differences in aortal RI and aortal PI values were found between all groups (P = .124 and P = .067, respectively, Table 2).
In control group, 68% (17/25) did not have microalbuminuria, 32% (8/25) had microalbuminuria, and 0% (0/25) had albuminuria. In CDMD group, 44% (12/27) did not have microalbuminuria, 56% (15/27) had microalbuminuria, and 0% (0/27) had albuminuria. In HAC group, 30% (6/20) did not have microalbuminuria, 30% (6/20) had microalbuminuria, and 40% (8/20) had albuminuria. Presence of
microalbuminuria and albuminuria in dogs among three groups were significantly different (P < .001).
In general, the presence of albuminuria was positive associated with increased mean renal RI (r = .421, P < .001). Age was mild but positively correlated with mean renal RI (r = .296, P = .012). No correlation among systemic blood pressure, renal RI
CV (%) of renal RI, renal PI, aorta RI and aorta PI were 2.8%, 4.5%, 7.1% and 9.1%, respectively.
Discussion
The RI and the PI provide information on expression of the resistance to blood flow within an artery by means of a ratio between peak systolic, end diastolic, and mean velocities of spectral Doppler vascular flow waveform. When an increase in vascular resistance occurs, diastolic blood flow is reduced to a greater degree than systolic blood flow. Then, the relatively greater decrease in end diastolic velocity than in peak systolic velocity causes an elevation in RI and PI.25 Increased RI and PI has been reported in dogs with ureteral obstruction,23 acute or chronic kidney disease,15,16 liver disease,26 CDMD,27 diabetes mellitus and HAC.10 In the present study, higher renal RI and PI were recorded in HAC group compared with control and CDMD groups, suggesting that the dogs affected with HAC had a higher vascular resistance.
These findings agreed with the results of previous study.10 However, there was no statistically significant in renal RI and PI values between control and CDMD groups, although both values of CDMD group were higher than control group. Although a positive association between increased interlobar RI and severity of heart failure class has been reported in dogs with CDMD, interlobar RI values in ISACHC class 1 dogs and normal dogs were not different.27 In this study, 48% of dogs in CDMD group was classified as ISACHC class 1, this might explain that the difference of RI of controls and CDMD was not significant.
The renal RI can be affected by age. The renal RI were significantly higher in the young dogs (< 4 months old) and children (< 4 years old).28,29 In elderly patients without renal insufficiency, the normal renal RI can also exceed 0.70. In this study, a positive correlation was found between age and mean renal RI. This finding was
based on a pool of clinically healthy dogs, dogs with CDMD with and without HAC.
However, control group was significant younger than groups of both CDMD and HAC. Most dogs with higher renal RI were affected by diseases. The effect of age on renal arterial resistance in dogs remains unclear.
No significant different was found between aorta RI and PI among all groups.
Some studies in animals suggested that several mechanisms may cause marked alterations in blood flow resistance in more distal arterial branches of the kidney.30 Excess glucocorticoids have many detrimental effects on kidney function. High levels of glucocorticoids accelerate the progression of chronic renal failure.8 The glomerular and tubular dysfunction has also been indicated in dogs with HAC.9 In this study increased RI and PI was detected in renal artery instead of aorta, suggesting that kidney was sensitive to evaluate vascular resistance than aorta.
Microalbuminuria, is an early and sensitive marker which permits timely and effective therapy in the early phase of renal damage, and is independently associated with increased cardiovascular risk factors and cardiovascular morbidity in human patients.31 Microalbuminuria is also associated with various systemic diseases such as neoplasia, infectious diseases, and immune-mediated, or inflammatory disease and urinary disorders.32 Several machines contribute to increased urinary albumin excretion in patient affected with HAC, such as hypertension, elevated plasma glucose levels, and abnormalities in lipid metabolism.33-35 In the present study, the prevalence of microalbuminuria in control group was similar to previous studies which ranged from 19 to 52%.36,37 And the prevalence of microalbuminuria was higher in CDMD group than HAC group, and the prevalence of albuminuria was higher in HAC group than CDMD group. In this study all dogs in HAC group had concurrent CDMD. Presence of albuminuria was positively associated with increased
circulating glucocorticoids might be responsible for a greater degree of albuminuria secretion in HAC group.
Systemic hypertension is commonly found in dogs with HAC.1,2,10,38 Activation of the renin-angiotensin system and mineralocorticoid receptor, enhanced activity of vasoactive substances (catecholamines and/or vasopressin and angiotensin II), and reduced activity of depressor systems (nitric oxide synthase, prostacyclin, and kinin-kallikrein systems) may be involved in glucocorticoid associated
hypertension.39-43 In this study, both the mean systolic blood pressure and the
prevalence of hypertension of HAC group were significantly higher than control and CDMD group. Although hypertension can be a cause and a consequence of renal failure.4,44 Significantly higher systemic blood pressure, increased renal RI, PI and prevalence of albuminuria was found in dogs with HAC, our study failed to demonstrate the correlation between hypertension and albuminuria.
Conclusion
Increased systemic hypertension, renal vascular resistance and prevalence of albuminuria were found in dogs with HAC. The presence of microalbuminuria and albuminuria might be associated with increased vascular resistance within the kidneys, but was not associated with increased systemic pressure or concurrent CDMD.
Footnotes
a. Model 811-B, Parks Medical Electronics Inc., U.S.A.
b. MyLabTM 50 Family, Esaote, Genova, Italy
c. Clinitek Microalbumin Reagent Strips and Clinitek Status Analyser, Bayer Diagnostic Mfg. Ltd., UK
d. SPSS Version 12.0.1, Lead Technologies Inc., Charlotte, North Carolina, U.S.A.
Reference:
1. Hurley KJ, Vaden SL. Evaluation of urine protein content in dogs with
pituitary-dependent hyperadrenocorticism. J Am Vet Med Assoc 1998;212:369-373.
2. Ortega TM, Feldman EC, Nelson RW, et al. Systemic arterial blood pressure and urine protein/creatinine ratio in dogs with hyperadrenocorticism. J Am Vet Med Assoc 1996;209:1724-1729.
3. Magiakou MA, Smyrnaki P, Chrousos GP. Hypertension in Cushing's syndrome.
Best Pract Res Clin Endocrinol Metab 2006;20:467-482.
4. Jacob F, Polzin DJ, Osborne CA, et al. Association between initial systolic blood pressure and risk of developing a uremic crisis or of dying in dogs with chronic renal failure. J Am Vet Med Assoc 2003;222:322-329.
5. Jacob F, Polzin DJ, Osborne CA, et al. Evaluation of the association between initial proteinuria and morbidity rate or death in dogs with naturally occurring chronic renal failure. J Am Vet Med Assoc 2005;226:393-400.
6. Haentjens P, De Meirleir L, Abs R, et al. Glomerular filtration rate in patients with Cushing's disease: a matched case-control study. Eur J Endocrinol
2005;153:819-829.
7. Faggiano A, Pivonello R, Spiezia S, et al. Cardiovascular risk factors and
common carotid artery caliber and stiffness in patients with Cushing's disease during active disease and 1 year after disease remission. J Clin Endocrinol Metab
2003;88:2527-2533.
8. Walser M, Ward L. Progression of chronic renal failure is related to glucocorticoid production. Kidney Int 1988;34:859-866.
9. Smets PM, Lefebvre HP, Meij BP, et al. Long-Term Follow-Up of Renal Function in Dogs after Treatment for ACTH-Dependent Hyperadrenocorticism. J Vet Intern Med 2012;26:565-574.
10. Novellas R, de Gopegui RR, Espada Y. Determination of renal vascular resistance in dogs with diabetes mellitus and hyperadrenocorticism. Vet Rec 2008;163:592-596.
11. Sugiura T, Wada A. Resistive index predicts renal prognosis in chronic kidney disease. Nephrol Dial Transplant 2009;24:2780-2785.
12. Ohta Y, Fujii K, Arima H, et al. Increased renal resistive index in atherosclerosis and diabetic nephropathy assessed by Doppler sonography. J Hypertens
2005;23:1905-1911.
13. Petersen LJ, Petersen JR, Talleruphuus U, et al. The pulsatility index and the resistive index in renal arteries. Associations with long-term progression in chronic renal failure. Nephrol Dial Transplant 1997;12:1376-1380.
14. Stevens PE, Gwyther SJ, Hanson ME, et al. Noninvasive monitoring of renal