※※※※※※※※※※※※※※※※※※※※※※※※※※
※ ※
※ 腳的長度對於人工全髖關節的影響 ※
※ ※
※※※※※※※※※※※※※※※※※※※※※※※※※※
計畫類別:個別型計畫
計畫編號:NSC 90-2314-B-006-087-
執行期間:90 年 08 月 01 日至 91 年 07 月 31 日
計畫主持人:賴國安
共同主持人:蘇芳慶
計畫參與人員:陳俊祥 林啟禎
執行單位:國立成功大學醫學院
中 華 民 國 91 年 10 月 30 日
Leg length difference after total hip arthroplasty
Kuo-An Lai, Chiun-Hsiang Chen, Chii-Jeng Lin, Fong-Chin Su
National Cheng Kung University Medical Center, Tainan, Taiwan
NSC: 90-2314-B-006-087
Corresponding: Kuo-An Lai No.138 Shen Li Road, Tainan Orthopaedic Department
Abstract:
Leg length inequality is very common after total hip arthroplasty. Its significance, however, is still controversial and unclear.
A total of 113 unilateral primary total hip arthroplasty(THA) were studied at an average follow up of 4 years. The study includes a questionnaire about the awareness of leg length difference(LLD) after THA, the shorter side and satisfaction on walking. Preoperative and postoperative LLD’s were measured from roentgenograms and correlated(Pearson’s correlation). Harris hip score was applied for evaluation of the clinical results. Comprehensive gait studies were performed in 34 patients of them for biomechanic evidence of influence of LLD.
LLD itself is not correlated with clinical results (p>0.05) or satisfaction(P>0.05). Awareness of LLD is the most important factor to be related with clinical result, satisfaction and walking. Thirty-one patients(27.4 %) are aware of LLD after THA. The awareness of LLD is associated with limping(p<0.01) and satisfaction of walking(p<0.01) and Harris hip score(p<0.05). Gait study observed more asymmetric gait in patients who are aware of LLD. Positive LLD(the affected side is longer) is associated with higher percentage of awareness of LLD(21 /28 ) than negative LLD(the affected side is shorter 10/37 )(p<0.01).
Leg lengths should be equalized to a reasonable range during total hip surgery. However, overlengthening is more poorly tolerated than underlengthening.
Introduction:
Leg length difference is very common after total hip arthroplasty. Some patients may blame their dissatisfaction to leg length inequality. Leg length inequality up to 2.5 cm is acceptable
for a usual person. However, the significance of leg length inequality for the patients with hip problems after total hip arthroplasty is still controversial. There were reports about preoperative planning and intraoperative measurement for leg length equalization during total hip arthroplasty. There are papers warning leg length inequlity after total hip arthroplasty as a potential risk for malpractice suit. A recent study, however, find that there is no statistical correlation between patients’ satisfaction and leg length equality. Our study on the gait of patients with congenital high dislocation of the hip found that bilateral asymmetry of gait in the unilateral patient could be due to leg length discrepancy. Our another study of unilateral congenital high dislocation of the hip after total hip arthroplasty found great improvement of gait symmetry by leg length equalization in these patients. Since total hip arthroplasties are done for patients with hip disorders, the leg length effect on the results may be different from that of other population. To our knowledge, there are no other existing reports on comprehensive gait analysis to dress the effect of leg length difference on the biomechanics of walking in patients after total hip arthroplasty. This study includes a measurement of the leg length difference, patient’s satisfaction through an inquiry and a comprehensive gait analysis for patients after total hip arthroplasties in order to understand the influence of leg length difference on the result and biomechanics of THA.
Patients and Methods.
113 patients with primary unilateral total hip arthroplasty performed during the year of 1998 in our institute were reviewed with their preoperative and post operative roentgenograms. There are 62men and 51women. Age at surgery ranged from 31to 72years(average57.6 years). Diagnosis for total hip arthroplasty include avascular necrosis of the femoral heads in 59(including 3 systemic lupus erythromatosus), primary osteoarthritis in 22 , rheumatoid arthritis in 7, dysplastic hip with secondary osteoarthritis in 14(2 are neglected high
dislocations), sequel after trauma in 7, ankylosing spondylosis in 3 and sequel of septic hip in 1 patient. Harris hip score was applied for evaluation of clinical results. The leg length inequality was measured as the bilateral difference of the distance of horizontal lines passing the tip of the lesser trochanter to the tear drop(Fig. 1). When the affected limb was longer than the sound side, the leg length difference was shown as positive(+) and when the affected limb was shorter than the sound side the leg length difference was shown as negative(-). Lengthening or shortening of the leg with surgery and the final leg length differences were recorded for every patients. These patients were inquired with a inquiry designed to find their self-awareness of the leg length inequality and satisfaction of the results(Table. 1). A total of 98 patients completed the inquiry. The following factors were analysed for satisfaction of the THA: preoperative LLD, operative change of the leg length, final leg length, awareness of LLD. Thirty-four patients were randomly selected for gait analysis to study the relation among the satisfaction, LLD and the biomechanics.
Results:
Clinical evaluation:
Preoperative Harris hip score averaged 47.5(33-72) and improved to 81.5(68-100) after surgery.
Leg length inequality
Preoperative leg length difference averaged –1.8cm (-5 to +4.5cm). Postoperatively, the LLD averaged –0.56cm(-2.5 to +3.5cm). The average lengthening by surgery was +1.24cm(-1.0 to + 3)cm. The distribution of LLD before and after surgery was shown in the Fig. 2. Preoperative LLD is correlated to postoperative LLD(r=0.647, p<0.001, Fig 2). Leg length
was equal in 45 patients, LLD<-1.5cm in 4, -1cm in 12, -0.5 cm in 21, +0.5 cm in 18, +1cm in 5 and > 1.5 cm in 5 patients.
Awareness of LLD and satisfaction
3 of the 4 patients with <1.5cm LLD are aware of that the affected side is shorter than the sound side. 3 of the 12 patients with –1cm LLD are aware of that the affected side is shorter. However, 2 of the –0.5cm LLD are aware of that the affected side is shorter while 1 was aware of the affected side was longer. Among the 45 patients with equal leg length, 4 are aware of the affected side is longer while 2 are aware of that the affected side is shorter. 7 out of 18 +0.5cmLLD, 4 of the 5 +1cm LLD and all 5 of the LLD>1.5cm are all aware of that the affected side is longer. Although there are 37 patients with negative LLD there are only 10 patients aware of negative LLD in contrast to 21 patients aware of positive LLD in 28 patients who had positive LLD(p<0.01).(Fig. 3).
Limping is correlated to awareness of LLD. 25/33( 75%) of the patients with limping are aware of LLD while only %(6/80 ) without limping are aware of LLD(p<0.01). Harris hip score is related with limping(p<0.01) and awareness of LLD(p<0.05).
Gait study
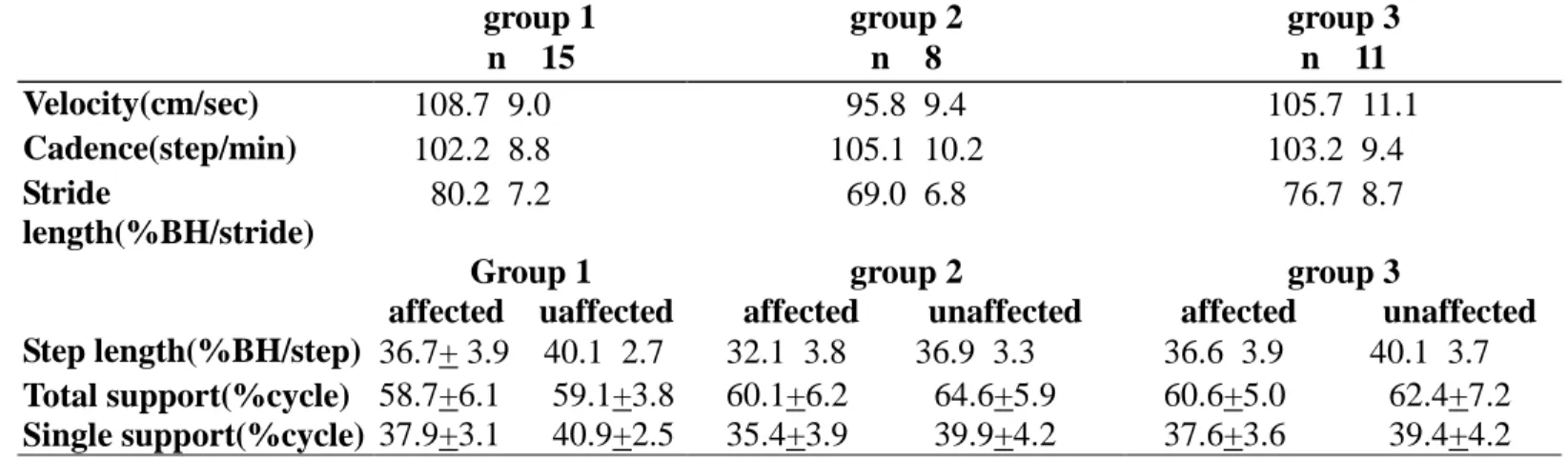
Temporospatial : The speed and cadence are faster in the patients without awareness of
LLD(Group 1) than patients who are aware of LLD(Group2: aware of negative LLD and Group 3: aware of positive LLD)(Table 2). Group 1 patients had more symmetric gait than the groups 2 and 3.
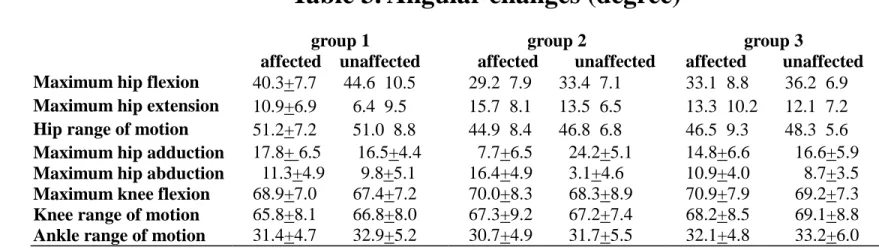
Kinematics:
The group 1 patients has more bilateral symmetric kinematics than both groups 2 and 3(Table 3).
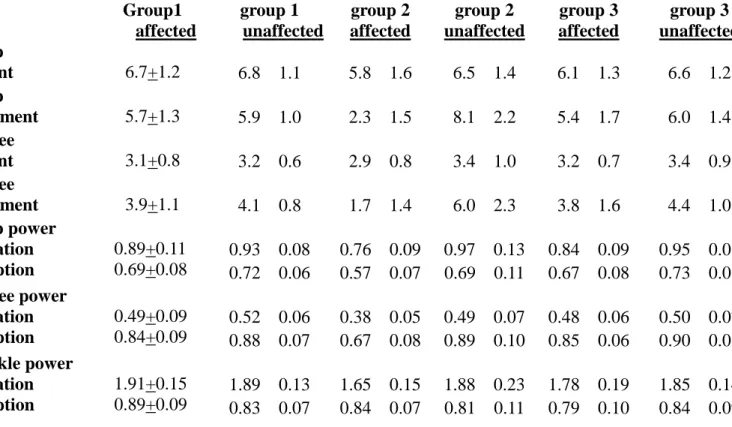
Kinetics: The Group 1 patients had more bilateral symmetric kinetics than both Group 2 and 3.
The joint moments, power generation and absorption are less in the awared shorter limbs inboth Group 2 and 3(Table 4).
Discussion:
Leg length problem after total hip arthroplasty has long been debated. The leg length measured during or after surgery are not the same as the functional leg length or the leg length patient himself/herself perceives.
Edeen et al(1995) reported that 32% of total hip patients were aware of leg length difference(LLD) and the measured LLD averaged 9.7mm. In those patients who were aware of LLD had more measure LLD(14.9) than average(9.7mm). More than half of the patients who were aware of LLD were also had disturbed gait. Jasty et al(1996) also reported 16% of THA patients with LLD. 4 patients used shoe lifts on the affected side and 2 patients used shoe lifts on the sound side for compensation of the LLD. Ranawat and Rodriguez(1997) assessed functional leg length inequality in a series of 100 consecutive primary THA’s and found that 14 % had FLLI 1 months after surgery and all resolutes 6 months after surgery. Nine patients had persistent FLLI 15 years after surgery which can be related to spine deformities. White and Dougall(2002), however, found that there are not any statistical association between LLD after THA and functional outcome or patient satisfaction.
In this study, we found that the leg length difference measured by the x-ray was not correlated with the satisfaction of the patients. However, awareness of the LLD is the most important factor that correlates with clinical results and satisfaction. Limping gait is an
asymmetric gait and is also correlated with aware ness of LLD. Patients who are aware of LLD walk slower and bear less weight on the shorter legs. This may imply that the patients use less the shorter leg to bear weight during walking.
Leg lengthening during THA may cause problems to the sciatic or femoral nerves. Over-lengthening of the leg may also cause aseptic loosening of the prosthesis. However, there is not any report on problems caused by a slightly shorter leg on the THA side.
The higher percentage of awareness of positive LLD than negative LLD in this study suggests that under-lengthening of the affected limb is better tolerated than over-lengthening during total hip arthroplasty.
Reference:
1. Bhave A, Paley D, Herzenberg JE: Improvement in gait parameters after lengthening for treatment of limb-length discrepancy. J Bone Joint Surg[Am] 81-A:529-34. 1999. 2. Kaufman KR, Miller LS, Sutherland DH: Gait asymmetry in patients with limb length
inequality. J Pediatr Orthop 16:144-50, 1996.
3. Hofmann AA, Skrzynski MC: Leg length inequality and nerve palsy in total hip arthroplasty: a lawyer awaits! Orthopaedics.23(9):943-4, 2000.
4. Cameron HU: Managing length: the too long leg. Orthopaedics 20(9):791-2, 1997. 5. Huddleston HD: An accurate method for measuring leg length and hip offset in hip
arthroplasty. Orthopaedics 20(4):331-2, 1997
6. Ranawat CS, Rodriguez JA: Functional leg length inequality following total hip arthroplasty. J Arthroplasty 12(4):359-64, 1997.
7. Jasty M, Webster W, Harris W: Management of limb length inequality during total hip replacement. Clin Orthop 333:165-71, 1996.
8. Bal BS: A technique for comparison of leg lengths during total hip replacement. American J of Orthopaedics 25(1):61-2, 1996.
9. Edeen J, Sharkey PF, Alexander AH: Clinical significance of leg length inequality after total hip arthroplasty. AM J Orthopaedics 24(4):347-51, 1995.
10. Nercessian OA, Piccoluga F, Eftekhar NS: Postoperative sciatic and femoral nerve palsy with referenceto leg lengthening and medialization/lateralization of the hip joint following total hip arthroplasty. Clin Orthop 304:165-71 1994.
11. Visuri T, Lindholm TS, Antti-Poika I, Koskenvuo M: The role of overlength of the leg in aseptic loosening after total hip arthroplasty. Italian J Orhop and Traumatology
19(1):107-11, 1993.
North Am 23(2):201-9, 1992.
13. Hoikka V, Vankka E, Tallroth K, Paavilainen T, Lindholm TS: Leg length inequality in total hip replacement, Annales Chirurgiae et Gynaecologiae 80(4):396-401, 1991.
14. Hoikka V, Santavirta S, Eskola A, PaavilainenT, Wirta J, Lindholm TS: Methodology for restoring functional leg length in revision total hip arthroplasty. J Arthroplasty 6(3):189-93, 1991.
15. Lai KA, Lin CJ, Su FC: Gait analysis of adult patients with untreated congenital complete dislocation of the hip. J Formossan Medical Association 96:740-4, 1997.
16. Lai KA, Lin CJ, Jou IM, Su FC: Gait analysis after total hip arthroplasty with leg length equalization in women with unilateral congenital complete dislocation of the hip. J Orthop Research 19:1147-1151, 2001.
17. White TO, Dougall TW: Arthroplasty of the hip-leg length is not important. J Bone Joint Surg 84-B:335-338 2002.
Table 1 Inquiry about LLD
1. Do you walk with limp? Yes.
No.
2. Are you aware of leg length difference? Yes.
No.
3. If you feel leg length difference, The affected(THA) side is longer. The affected(THA) side is shorter. 4. How do you walk?
Very well.
Well at level walking, difficult at stairs Occasional difficult at level walking Difficult at level walking
Table 2. Temporospatial parameters group 1 n=15 group 2 n=8 group 3 n=11 Velocity(cm/sec) 108.7±9.0 95.8±9.4 105.7±11.1 Cadence(step/min) 102.2±8.8 105.1±10.2 103.2±9.4 Stride length(%BH/stride) 80.2±7.2 69.0±6.8 76.7±8.7 Group 1 affected uaffected group 2 affected unaffected group 3 affected unaffected Step length(%BH/step) 36.7+ 3.9 40.1±2.7 32.1±3.8 36.9±3.3 36.6±3.9 40.1±3.7 Total support(%cycle) 58.7+6.1 59.1+3.8 60.1+6.2 64.6+5.9 60.6+5.0 62.4+7.2 Single support(%cycle) 37.9+3.1 40.9+2.5 35.4+3.9 39.9+4.2 37.6+3.6 39.4+4.2 BH: body height,
Table 3. Angular changes (degree)
group 1 affected unaffected group 2 affected unaffected group 3 affected unaffected Maximum hip flexion 40.3+7.7 44.6±10.5 29.2±7.9 33.4±7.1 33.1±8.8 36.2±6.9Maximum hip extension 10.9+6.9 6.4±9.5 15.7±8.1 13.5±6.5 13.3±10.2 12.1±7.2
Hip range of motion 51.2+7.2 51.0±8.8 44.9±8.4 46.8±6.8 46.5±9.3 48.3±5.6
Maximum hip adduction 17.8+ 6.5 16.5+4.4 7.7+6.5 24.2+5.1 14.8+6.6 16.6+5.9
Maximum hip abduction 11.3+4.9 9.8+5.1 16.4+4.9 3.1+4.6 10.9+4.0 8.7+3.5
Maximum knee flexion 68.9+7.0 67.4+7.2 70.0+8.3 68.3+8.9 70.9+7.9 69.2+7.3
Knee range of motion 65.8+8.1 66.8+8.0 67.3+9.2 67.2+7.4 68.2+8.5 69.1+8.8
Table 4. Joint moment and power
( unit of moment : % of body weight×body height , unit of power : watt/body weight )
Group1 group 1 group 2 group 2 group 3 group 3 affected unaffected affected unaffected affected unaffected Maximum hip flexion moment 6.7+1.2 6.8 ±1.1 5.8 ±1.6 6.5 ±1.4 6.1 ±1.3 6.6 ±1.2 Maximum hip adduction moment 5.7+1.3 5.9 ±1.0 2.3 ±1.5 8.1 ±2.2 5.4 ±1.7 6.0 ±1.4 Maximum knee flexion moment 3.1+0.8 3.2 ±0.6 2.9 ±0.8 3.4 ±1.0 3.2 ±0.7 3.4 ±0.9 Maximum knee adduction moment 3.9+1.1 4.1 ±0.8 1.7 ±1.4 6.0 ±2.3 3.8 ±1.6 4.4 ±1.0
Maximum hip power generation absorption 0.89+0.11 0.69+0.08 0.93 ±0.08 0.72 ±0.06 0.76 ±0.09 0.57 ±0.07 0.97 ±0.13 0.69 ±0.11 0.84 ±0.09 0.67 ±0.08 0.95 ±0.08 0.73 ±0.08
Maximum knee power generation absorption 0.49+0.09 0.84+0.09 0.52 ±0.06 0.88 ±0.07 0.38 ±0.05 0.67 ±0.08 0.49 ±0.07 0.89 ±0.10 0.48 ±0.06 0.85 ±0.06 0.50 ±0.07 0.90 ±0.08
Maximum ankle power generation absorption 1.91+0.15 0.89+0.09 1.89 ±0.13 0.83 ±0.07 1.65 ±0.15 0.84 ±0.07 1.88 ±0.23 0.81 ±0.11 1.78 ±0.19 0.79 ±0.10 1.85 ±0.14 0.84 ±0.09