個案報告
鋼琴活動應用於職能治療之質性研究—個案報告
Qualitative Research into a Piano Activity in Occupational Therapy: A Case Study
……… 施以諾 蘇怡如 吳佳慧 1
紅斑性狼瘡成人併發肺炎雙球菌敗血症引起的腦膜炎續發細菌性迷路炎—病例報告 Meningogenic Labyrinthitis Complicated by Streptococcus Pneumoniae Septicemia in a Systemic Lupus Erythematosus Adult: A Case Report
……… 王維吟 黃奭毓 許晉榮 黃永堅 王拔群 9
Gemcitabine 及 Carboplatin 的複合性化學治療治療單純前列腺小細胞癌
Gemcitabine/Carboplatin Chemotherapy for Pure Small Cell Carcinoma of the Prostate:
A Case Report……… 陳冠州 邱文祥 江漢聲 朱娟秀 鄭建睿 17
綜 論
痛風與高尿酸血症的認知與管理
Recognition and Management of Gout and Hyperuricemia …… 黃麗玲 林川雄 黃建財 25
原 著
非侵入性正壓呼吸器對拔管失敗之影響
Effect of Noninvasive Positive-Pressure Ventilation on Extubation Failure
……… 林恆毅 蘇千玲 楊式興 陳群互 陳建文 吳清平 33 每天使用20 毫克 Simvastatin 於合併有混合型高脂血症的腎功能異常病人之效果評估
Efficacy and Safety of 20 mg/day Simvastatin in Patients with Renal Impairment and
Combined Hyperlipidemia……… 呂至剛 黃美美 白榮貴 江蔚文 43
投稿簡則
作者投稿聲明書
●
●
●
●
●
●
輔仁醫學期刊
中華民國九十四年三月 第三卷 第一期
目 錄
個案報告
人文氣息,使病患較有動機參與活動[7]。本文即 是以個案研究的方式,去探討如何以彈鋼琴的活 動去幫助一位因腦部外傷而造成手功能障礙的病 人,做為其手部功能復健的媒介,並分析此類運 用模式的理論基礎,以及用彈鋼琴來做為復健活
動對其職能領域 (日常生活功能、工作、休閒)
的幫助。
一、彈鋼琴運用於手功能復健之理論基礎 以動作分析的角度來看,彈鋼琴的活動需要 一定的手指動作功能,手指協調度,手指靈巧
度,雙手協調度,不同邊的身體承重 (weight
bearing),以及上肢近端的穩定度,此類的功能 都可能因腦部外傷而造成缺失。以「神經發展」
(neurodevelopmental treatment) 的角度來看,復 健 過 程 中 針 對 病 人 喪 失 的 能 力 (ability and capability) 以簡易的彈鋼琴活動 (如:單手彈音 階、單手彈簡普曲子) 的動作來訓練,恰可符合 緒 論
音樂治療是一項新興的治療技術,它的定義 是"有技巧地使用音樂媒介來恢復、維持、改善 病人的生理、心理與情緒問題[1],此論述也符合 職能治療「利用有目的的活動來增加病人的心 理、生理、社會功能」[2]的定義。近年來,職能 治療師與護理師陸續在學術期刊中發表文章建議 應用音樂活動於醫療領域,並對其療效提出研究 數據或經驗分享[3,4,5]。然而,一般人對於音樂治 療的印象仍停留在給病人用聆聽音樂的方式來舒 緩其疼痛與心情,然而,音樂治療中,聽音樂只 是其中一種運用的方式,其他如音樂性舞蹈及樂 器活動等都是音樂治療可被運用的模式,也都具 有療效[6]。
以樂器活動而言,其在復健照護上有其特殊 的價值,包括可訓練病人手部的靈巧度、注意 力、協調度等,且可同時為漫長的復健過程增添
輔仁大學醫學院職能治療學系1 台北市立萬芳醫院精神科2 育達商業技術學院幼兒保育系3
投搞日期:2004 年 9 月 13 日;接受日期:2005 年 3 月 21 日
* 通訊聯絡作者:電子郵件:[email protected]
鋼琴活動應用於職能治療之質性研究—個案報告
施以諾
1,2, *
蘇怡如2
吳佳慧3
本文敘述臨床職能治療師如何以神經發展理論及人類職能參考架構為治療理論,
將具治療性目的的鋼琴活動運用在一位重鬱症且合併有腦部外傷及頸椎椎間盤凸出的 病人身上。透過質性研究的訪談方式,研究者歸納出職能治療鋼琴活動對病人工作、
休閒、日常生活三方面的職能領域的幫助,文中並討論鋼琴活動應用於腦傷病人時應 注意的原則,可作為日後職能復健在臨床運用上的參考。
(輔仁醫學期刊
2005;3 (1) :1-7 )
關鍵詞:職能治療,音樂治療,鋼琴活動,復健
施以諾 蘇怡如 吳佳慧
2 Fu Jen Journal of Medicine Vol.3 No.1 2005
病人手功能復健之所需,協助病人在協同肌與拮 抗肌的相互協調、穩定度 (stability)、動作度 (mobility) 與動作計畫 (motor planning) 的能力
[8]。
此類的音樂治療活動可讓病人覺得較溫暖且 提升參與的動機[7],若以「人類職能參考架構」
(Model Of Human Occupation) 所闡述的理論來 看彈鋼琴對腦傷病人手功能的幫助,可以發現:
當病 人參 與復 健活 動 的意 志次 系統 (volition subsystem) 提 昇 時,其 表 現 (mind-brain-body performance) 也提升,而提升其功能表現,正是 復健的目的[2,9]。
二、樂器活動運用於手功能復健之相關研究 許多文獻均指出,樂器活動也可用以改善腦 部病變患者的動作功能 (motor function),包括 粗動作與精細動作[7,10]。
復健過程中" 主動式關節活動" (AROM,
active range of motion) 是不可或缺的,然而病人 們卻常因疼痛、恐懼、意願低而不參加療程,此 時若能將這些復健動作設計、融入操作樂器的動 作中,病人的參與意願就會有所提高[6,7]。以粗 動作差的腦部病變患者為例,在病房裡,常有護
理師或治療師將AROM 的動作給設計成讓患者
運用患肢去敲打樂器的活動,如操作沙鈴、木
鳥、鈴鼓,讓整個AROM 的療程充滿樂趣,增
加病人的興趣與參與度,達到復健的作用。此方
式往往比傳統的肢體復健(如:病人需直接執行
動作) 有更好的效果[10]。
一般復健鼓勵病人多從事精細動作,以誘發 肌力,或藉由一些動作以抑制手部的不正常張 力。音樂治療在這方面也有相當的價值。如:許 多樂器在操作時都需要出現"對掌"的復健動作,
能安排病人使用樂器以訓練之,則會是相當有益 的復健活動[10,11]。
在 一 份 以 TMS (transcranial magic stimulation) 為工具的研究中,研究者發現彈鋼 琴的活動可讓人大腦中掌管屈指長肌(long finger flexor) 與伸指長肌 (long finger extensor) 的部位 獲得活化[12],更說明了鋼琴活動對於手部復健 所具有的潛力。
方 法
一、個案
個案現離婚,與母親、一對兒女同住,本次 住院的診斷為因跳樓造成腦外傷(head injury) 與 頸椎椎間盤凸(C-HIVD) 出,九十三年五月二十 日起,同時在台北某醫學中心的復健科與精神科 接受職能治療療程。個案民國七十七年間曾開始 使用安非他命、大痲、海洛英等毒品,至民國九 十年間,曾進入勒戒所兩次,並住過台北市某家 精神專科醫院三次,在醫院的診斷為重鬱病 (major depression) 與物質濫用 (alcohol abuse),
民國九十三年二月十九日酒後從家中五樓跳下,
造成右腦傷及頸椎椎間盤凸。個案自今年五月初 開始轉介至復健科職能治療,五月二十日開始轉 介至精神科職能治療日間病房,目前同時於復健 科及精神科兩個科部的職能治療室接受職能治療 的療程。個案目前情緒穩定,可規則服藥,常抱 怨雙手手痲,動作不靈活,又以左手的情況較嚴 重。個案仍有低張力,因不正常低張力的關係,
所以無法施測手功能測驗;褚氏注意力測驗的分
數為78 分,第三級分。個案目前對出院後的期
待是希望能做一些簡單的文書工作。
二、職能治療鋼琴活動進行方式:
(一) 活動名稱:職能治療鋼琴活動 (二) 活動設備:電子鋼琴鍵盤一台。
(三) 活動劑量:週一至週五下午四點至四點半,
鋼琴活動與職能治療
每次活動半個小時,共六週,合計27 次,
地點在某醫學中心精神科日間病房,個案回 家後並未再從事任何鋼琴活動。
(四) 活動目的
1. 增加個案對治療的意志次系統 (volition subsystem)
2. 訓練姿勢控制 (postural control) 3. 訓練動作控制 (motor control) 4. 訓練動作計畫 (motor planning) 能力 5. 五指間的協調度 (coordination) 6. 改善手眼協調 (eye-hand coordination) 7. 訓練對時間點 (timing) 的掌控能力 8. 維持手部的關節活動度 (range of motion) (五) 活動方式與步驟
活動一:單手分別彈音階。
1. 個案在琴前採坐姿,離桌緣約 10 到 15 公 分的距離。
2. 要求個案分別以左、右手來回彈四個八度 的音階,左、右手來回各彈兩次,要求個 案不能同時按到兩個琴鍵,且要求個案在 彈音階時保持固定的速度。
活動二:單手彈簡譜。
1. 個案在琴前採坐姿,離桌緣約 10 到 15 公 分的距離。
2. 讓個案挑自己喜歡的流行歌曲或電影主題 曲的簡譜,左、右手分別以單手的方式來 彈奏。
(六) 活動參考架構與治療理論基礎
1. MOHO (Model of Human Occupation):
增 進 病 人 的 意 志 次 系 統 (volition subsystem),進而連帶提升其表現次系統 (mind-brain-body performance),達 到 增 進復健成效的目的。
2. NDT (neurodevelopmental treatment):
讓病人經由活動學習如何正確地使
用肢體,產生正確的姿勢和動作。
3. Rood approach:
藉由鋼琴活動增進病人上肢近端的 穩定度(stability),來使上肢遠端能從事 有目的性的活動,進而發展出正確的動作 模式。
三、資料收集方法:
民國九十三年六月中旬至八月初,職能治療 師在日間病房開始以具治療性目的的鋼琴活動介 入之。本篇採個案研究法,由研究者擔任個案個 別鋼琴活動治療的主要治療師,研究者並運用身 體評估、觀察,以及與個案的會談來收集資料,
共會談三次,分別為六月中旬、七月中、八月
初,每次約20 分鐘,收集的資料依職能領域分
為日常生活功能、工作、休閒三個方面來呈現 之。
結 果
一、鋼琴活動與一般手功能復健的不同:
研究者發現,相較於一般的手功能復健,用 單手彈鋼琴的活動來做手功能訓練有幾點特別之 處,分述如下:
(一) 可提高個案參與動機
相較於其他的職能治療活動,個案對 此活動的參與度與主動性頗高。個案在訪談 中表示:「這樣的活動比在治療室裡撿綠 豆,或是拿小積木要來得有趣多了!我知道 治療師是要我藉以達到訓練手指活動度的目 的,但這樣的活動不會讓我覺得煩,不但如 此,我 每天來 醫院最期 待的就 是鋼琴 活 動。」
(二) 可顧及個案自尊心
個案曾多次向治療師表示鋼琴活動對
施以諾 蘇怡如 吳佳慧
4 Fu Jen Journal of Medicine Vol.3 No.1 2005
其很有意義,指此活動提升了他的自信與自 尊,個案在訪談的過程中說:「我在做一般 的手功能訓練活動時,會很怕讓認識的人來 看,甚至不太喜歡讓一般人看到,感覺好像 我在做一些很基本的動作,但卻又都做得不 太好,覺得自己很丟臉,會害怕別人異樣的 眼光。但這種用彈鋼琴來訓練手功能的方式 不會讓我有這種困擾,我也比較不會怕被熟 人看到,因為我就算彈不好也不必怕別人會 笑我,反正就算是一般的健康人也不見得就 會彈,所以,雖然只是簡單的單手彈琴,但 只要彈得稍微還可以,我就會很有成就感,
且別人也會給予稱讚,所以我很喜歡這種復 健的方式。」
(三) 鋼琴活動是一種要求節拍的活動
病人必需跟著曲子的快慢而改變手指 的速度,可訓練其對時間點(timing) 的掌控 能力,本研究的個案表示:「一般復健科的 動作練習只要求我做出某些精細動作來,如 撿豆子或拿小積木,但沒有要求我做這些動 作時的速度,因著手部動作還不靈活,我在 做這些復健動作時常會不自覺地忽快忽慢,
但仍可以完成那些復健的活動。可是彈鋼琴 時不能這樣,因為我除了要手指做出動作 外,還需要跟得上曲子的節拍去做那些手指 的動作,是一種更高階的復健與挑戰。」
二、鋼琴活動對患者職能領域的影響
當人在做彈鋼琴的活動時,需做出許 多複雜的動作,如彈連續音階時需不斷做出 對掌的動作,且治療師會要求其控制在一定 的節拍、速度。研究發現這些活動基本要素 對其在「職能領域」(occupational area) 上 有很大的幫助、補強,底下分別以日常生活 功能、工作、休閒三方面陳述之。
(一) 日常生活功能
在訪談中,病人覺得需在一定節拍的 要求下做出敲琴鍵的動作,對其日常生活功 能有以下助益:「我覺得自己在練習鋼琴之 後,在穿衣服扣釦子的動作上順很多,在綁 鞋帶時也覺得打節容易且快得多!以前在布 鞋上打個節得花很多功夫,且在穿線時總是 對不準,在練習鋼琴之後,我覺得這樣的動 作再做起來就快多了,因為其實很多動作都
很像(鋼琴與扣釦子、綁鞋帶),且我每天練
習(鋼琴) 半個小時。」
(二) 工作
個案表示期待未來能夠繼續從事文書 的相關工作,而彈鋼琴的活動對這方面亦有 助益,個案表示:「鋼琴需不斷做出許多複 雜的動作,如手掌的翻轉 (指"對掌"的動 作),各指頭間的動作也需很靈巧,我覺得 這對以後我想在從事操作文具的工作很有幫 助,而且也更有信心了!如果我連這個我沒
學過的東西(指彈鋼琴) 都可以做了,我生
病前本來會做的(指操作文具) 又有什麼問
題呢?」
(三) 休閒
個案過去是一個較喜歡戶外休閒的青 年人,但腦傷後左半邊肢體動作受影響,使 他較無法從事戶外休閒,對於治療師為他所 安排的鋼琴這個活動,個案表示:「我覺得 很有意思,也很開心,我沒有讀過什麼書,
雖然喜歡聽聽音樂,但從來沒想到有一天我 竟可以用自己的手來敲出音符,雖然現在的 能力只能用單手分別敲琴鍵,但我真的覺得 很開心,我喜歡挑一些自己喜歡聽的歌曲的 簡譜來練習,這對我來說不只是一種復健活 動,更是一個很重要的休閒活動,一方面可 以訓練我的手,二方面也可以讓我的日子不
鋼琴活動與職能治療
會過得這麼無聊,因為我至少在短時間內不 太可能再從事太劇烈的運動。」
討 論
以治療者的角度觀之,這個用彈鋼琴來達成 手功能復健的音樂治療模式,非常符合「全人」
治療的原則,除了顧及「病人」的「病」之外,
亦考量到他的「人」;是一種非常特別的復健活 動。
一、鋼琴活動對於本研究之病人的幫助
此類活動除了注重其手功能的復健外,更可 同時兼顧其自尊心、參與意願、興趣,依照「人 類 職 能 參 考 架 構」 (Model Of Human Occupation) 觀之,當病人參與復健活動的意願 (volition) 提高時,其表現 (performance) 也會跟
著提高[2,9],在訪談的過程中,研究者發現此一
鋼琴活動顯然提高了病人的參與意願、動機,依 上述理論,本活動對於病人功能的提升有正面的 幫助。
而 除 此 之 外,依「神 經 發 展」 (NDT, neurodevelopmental treatment) 理論觀之,本研 究的個案在彈鋼琴時,其手眼協調 (eye-hand coordination)、手指間的協調度,以及動作控制 (motor control)、姿勢控制 (postural control) 等 功能也會得到訓練,這些基本的生理功能得到改 善後,對其許多日常生活中的細部動作都有幫助
[8]。
綜合以上兩點,以及歸納與本研究的個案的 訪談後,我們可以說:在病人不排斥的前提下,
將諸如此類操作樂器的音樂治療活動運用在復健 過程中,可對其日常生活功能、工作、休閒這三 個職能領域有正面的幫助。
二、鋼琴活動用於腦傷病人的注意事項
在利用諸如鋼琴活動等音樂治療活動來介入 患者時,醫護人員需有以下幾點認知:
(一) 此類音樂活動不能完全取代正式的手功能復 健療程
諸如單手彈鋼琴等樂器活動雖可對病 人的手功能有幫助,但並不可以取代正式的 復健療程,如:物理治療、一般的職能治 療、藥物治療。但此類活動可在醫護人員的 醫囑下讓病人從事之,可有輔助的功效。
(二) 此類音樂活動必需是符合病人興趣的活動 依 MOHO 的 理 論,意 願 (volition subsystems) 次系 統中 包含了 興趣、價 值 觀、個人因果三個成份。雖然此單手彈鋼琴 的活動對本研究的個案很有幫助,但不是每 個病患都會對這種活動有興趣,如果病患本 身對音樂甚排斥,則如此「用操作樂器來做 復健」的模式只會降低其意願次系統中的興 趣成份(interest components),進而使其表 現(mind-brain-body performance) 也跟著降 低,反而會有反效果。
(三) 注意此類音樂活動所可能帶給病人的挫折感 即便病人很有興致,但仍有可能因其 動作功能的缺失,而使其在樂器活動中的表 現受到限制,進而受到挫折感。醫護人員需 依其當下的功能而針對其表現給予適當的鼓 勵,才不會徒增病人在療程中的失落感與自 棄。
三、本研究的限制與未來建議
本前趨研究的資料收集方式僅只於會談,資 料呈現方式也僅只於書面文字,且為個案報告,
未來研究者可收集更多的個案樣本,並以量化的 方式來探討鋼琴活動對腦外傷、腦中風等腦部病 變患者的手功能、注意力、協調度、手臂近端穩
施以諾 蘇怡如 吳佳慧
6 Fu Jen Journal of Medicine Vol.3 No.1 2005
定度等功能的幫助,甚至可研究鋼琴活動對改善 偏癱患者在復健過程中憂鬱程度的助益,將可對 鋼琴活動對於腦部病變患者的成效以量化的方式 更具體的呈現出來。
復健科有許多此類的手功能受損之病人,但 通常在復健科並沒有鋼琴或鍵盤的設備,就算在 醫院的其他地點也難以一見,然而,鋼琴或鍵盤 在精神科的職能治療室,或是護理之家裡卻是常 見的設備之一。各醫療院所若能妥善地結合院內 各科室的復健、護理、職能治療資源,將可對病 人有更多元的幫助。
參考文獻
1. Canadian Association for Music Therapy. Music Therapy: A Health Care Profession. Sarnia, ON, Canada: Canadian Association for Music Therapy;
1992.
2. Neistadt ME, Crepeau EB. Willard & Spackman's OccupationalTherapy.Washington,DC: Lippincott- Raven Publishers; 1998.
3. Biley F. Use of music in therapeutic care. Br J Nurs 1992;1:178-179.
4. Chlan L, Tracy MF. Music therapy in critical care:
indications and guidelines for intervention. Crit Care Nurse 1999;19:35-41.
5. 施以諾。音樂治療與健康照護。長庚護理2004;
14(1): 72-79。
6. Shih YN, Chiang HS, Hwang MT, et al. Music, nerve, and occupational therapy. Fu-Jen J Med 2004;1:13-20.
7. 施以諾、江漢聲。運用音樂治療於腦傷復健。
慈濟護理2003;2:7-12.
8. Sabari JS. Motor learning concepts applied to activity-based intervention with adults with hemiplegia. Am J Occup Ther 1991;45:523-530.
9. Haglund L, Kjellberg AA. Critical analysis of the Model of Human Occupation. Can J Occup Ther 1999;66:102-108.
10. Johnson G, Otto D, Clair AA. The effect of instrumental and vocal music on adherence to a physical rehabilitation exercise program with persons who are elderly. J Music Ther2001;38:82-96.
11. Hilliard RE. The effects of music therapy-based bereavement groups on mood and behavior of grieving children: a pilot study. J Music Ther 2001;
38:291-306.
12. Pascual LA, Nguyet D, Cohen LG, et al. Modulation of muscle responses evoked by transcranialmagnetic stimulation during the acquisition of new fine motor skills. J Neurophysiol 1995;74:1037-1045.
鋼琴活動與職能治療
Qualitative Research into a Piano Activity in Occupational Therapy: A Case Study
Yi-Nuo Shih 1,2 Yi-Ju Su 2 Chia-Hui Wu 3
In this research, we explored how occupational therapists used a therapeutic piano activity to cure a patient with a head injury and cervical-HIVD (Herniated Intervertebral Disc) with major depression. The approach was based on theories of neurodevelopmental treatment and the Model of Human Occupation. We used an in-depth interview methodology of qualitative research to sum up the helpfulness of a piano activity for patients at work, at leisure, and in activities of daily living, 3 aspects of occupational areas. We discuss our findings of using a piano activity to treat patients with head injuries, which may offer references for clinical use for related staff in the area of rehabilitative care. (
FJJM 2005; 3 (1): 1-7 )
Key words: occupational therapy, music therapy, piano activity, rehabilitation care
School of Occupational Therapy, College of Medicine, Fu Jen Catholic University1 Department of Psychology, Municipal Wan Fang Hospital2 Department of Child Care and Education, Yu-Da College of Business3
Submitted September, 13, 2004; final version accepted March, 21, 2005.
* Correspondence author:[email protected]
Case Report
INTRODUCTION
The most-common bacterial pathogen of meningitis is Streptococcus pneumoniae (47%), followed by Neisseria meningitidis (25%) and group B Streptococcus (12%)[1]. The incidence of bacterial meningitis has been steadily decreasing since the introduction of hemophilus influenzae type B vaccine (HIB) in 1990. Most victims are in the pediatric age group, and the incidence of hearing
impairment after bacterial meningitis may range from 10.3% to 21% [2]. In adults, the incidence of bacterial meningitis is relatively low, and the hearing impairment after meningitis seems to be even lower;
however, the definite prevalence of hearing loss in adults is unknown. In this report, we present an immunocompromised adult who developed unusual meningogenic bacterial labyrinthitis. Related articles are also reviewed.
Meningogenic Labyrinthitis Complicated by Streptococcus Pneumoniae Septicemia in a Systemic
Lupus Erythematosus Adult: A Case Report
Wei-Yin Wang 1 Shih-Yu Huang 2 Chin-Jung Hsu 2 Yung-Chien Huang 3 Pa-Chun Wang 1,4, *
Sensorineural hearing loss can be a complication of bacterial meningitis. Most victims are in the pediatric age group. In adults, the incidence of meningitis is low, and the hearing impairment after meningitis seems to be even lower. Sensorineural hearing loss in meningitis may be attributable to cochlear involvement of infection through various routes including the internal auditory canal, hematogenous spread, or through the cochlear aqueduct. Imaging findings may include a slight reduction in the fluid signal within the cochlea on T2-weighted magnetic resonance (MR) images and cochlear enhancement on gadolinium-enhanced T1-weighted images, or ossification of the cochlear with computed tomography (CT) later in the recovery stage.
Patients who have no response to the auditory brainstem evoked potential response initially may never recover the hearing loss. Antibiotics combined with dexamethasone may offer some benefit for certain cases. In this report, we present a systemic lupus erythematosus adult who was on continuous ambulatory peritoneal dialysis and who developed meningogenic bacterial labyrinthitis. Important related articles are also reviewed. (
FJJM 2005; 3 (1): 9-15 )
Key words: sensorineural hearing loss, bacterial meningitis, bacterial labyrinthitis
Department of Otolaryngology1 Division of Nephrology, Department of Radiology2 Department of Internal Medicine3 Cathay General Hospital, Taipei, Taiwan School of Medicine, Fu-Jen Catholic University, Hsinchuang, Taipei, Taiwan4
Submitted December, 21, 2004; final version accepted March, 15 , 2005
* Correspondence author: [email protected]
Wei-Yin Wang Shih-Yu Huang Chin-Jung Hsu Yung-Chien Huang Pa-Chun Wang
10 Fu Jen Journal of Medicine Vol.3 No.1 2005
CASE REPORT
The patient was a 31-year-old woman with a history of systemic lupus erythematosus (SLE) and chronic renal failure who was on continuous ambulatory peritoneal dialysis. A hypertension crisis, fever, and consciousness change (Glasgow coma scale: E4M6V2) developed immediately before admission; neck rigidity was found during the physical examination. The Gram stain of blood smear showed gram (+) diplococci and the blood culture later yielded S. pneumoniae. Bacterial peritonitis was the initial impression and was later confirmed by identifying S. pneumoniae in the turbid dianeal. Meningitis was also confirmed by positivefindingsof S. pneumoniae in thecerebrospinal fluid (CSF). There was no evidence of SLE flare- up; the follow-up laboratory tests revealed no active change of C3, C4, C1q, CH50, anti-double stranded DNA, or anti-cardiolipin antibody levels as compared with previous data.
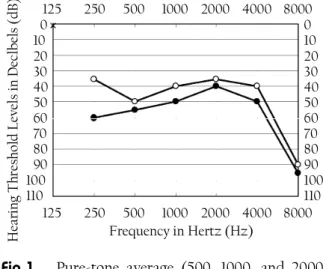
Twodaysafteradmissionwhenherconsciousness had gradually recovered, the patient began to complain of bilateral hearing impairment, tinnitus (especially on the left side), and vertigo. She denied anypreviousotologicalsymptoms.Anotolaryngological physical examination revealed normal eardrums and a right-beating horizontal nystagmus. Pure- tone audiometry (PTA) performed 7 days after symptom onset revealed bilateral sensorineural hearing loss (SNHL). The pure tone average in the left ear was above 110 dB and in right ear was 48 dB. (Fig. 1) The vestibular nystagmographic (VNG) examination suggested a left peripheral lesion by showing right-beating nystagmus superimposed on a right-wards saccade and an upward nystagmus on positional and positioning tests. The auditory brainstem evoked potential response (ABR) revealed no response on the left side, which was suggestive of cochlear pathology. There was no ossification
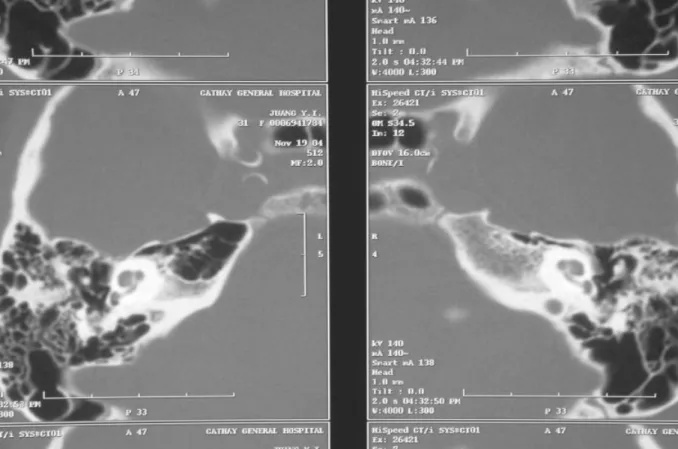
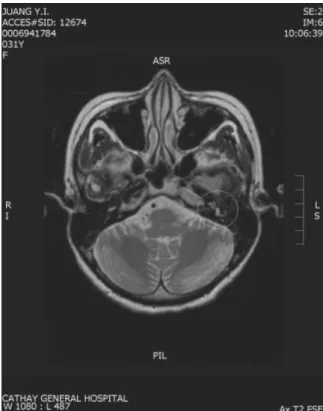
of the bilateral cochlea or vestibular organ, nor was there any middle ear lesion as shown on high- resolution temporal bone computed tomography (CT) scan on day 26 (Fig. 2). Magnetic resonance imaging (MRI) performed on day 30 showed abnormal enhancement of the bilateral cochlea (gadolinium-enhanced T1-weightedimages, especially on the left side, Fig. 3) and a reduction in the fluid signal intensity within the cochlea (T2-weighted MR images, Fig. 4). The imaging study findings confirmed the existence of meningogenic bacterial labyrinthitis.
Intravenousantibiotics(cefazolinandgentamicin on days 1 and 2, cefotaxime on days 3~17, penicillin G sodium on days 5~17, metronidazole on days 8~17, and ceftriaxone on days 18~28) and prednisolone (20 mg IV on days 2~17) were given. The vertigo symptom gradually subsided following anti- vertiginous treatment with vestibular suppressants and minor tranquilizers. Her hearing remained impaired on both sides (Fig. 1).
0 10 20 30 40 50 60 70 80 90 100 110
125 250 500 1000 2000 4000 8000 0 10 20 30 40 50 60 70 80 90 100 110 125 250 500 1000 2000 4000 8000
Frequency in Hertz (Hz)
H ea rin g T hr es ho ld Le ve ls in D ec lb el s (d B)
Fig 1.
Pure-tone average (500, 1000, and 2000 Hz) of the right side of 48 dB (black circles) at the first evaluation and of 42 dB (white circles) before discharge. The left side hearing was off the scale (not shown in the figure).Miningogenic Labyrinthitis in Systemic Lupus Erythmatosus
DISCUSSION
SNHL is a complication of bacterial meningitis that may occur unilaterally, bilaterally, partially, or completely. Nearly 1/3 of children with S.
pneumoniae meningitis and approximately 10% of those with N. meningitidis may develop SNHL[2]. Bacterial meningitis is uncommon in the adult group.Inthepresentcase,duetoherimmunocompromised condition (SLE under prednisolone treatment), the patientsimultaneously developedbacterial peritonitis, bacteremia, and bacterial meningitis; this was confirmed by the identical pathogen being isolated from various specimens.
SNHL in meningitis is attributable to cochlear
involvement through various routes of infection including the internal auditory canal, hematogenous spread, or the cochlear aqueduct. The cochlear aqueduct is a bony canal that connects the subarachnoid space with the perilymphatic space of the inner ear at the basal turn of the scala tympani and is thought to be the main source of cochlear infection[3,4].
Animal models of bacterial meningitis have clearly shown bacterial involvement in the cochlear aqueduct with spread to the perilymphatic space of the scala tympani [3]. Examination of temporal bones from human cadavers with SNHL secondary to bacterial meningitis also disclosed cochlear aqueduct and perilymphatic invasion[4].
Fig 2.
High-resolution CT of the temporal bone. No cochlear ossification or abnormality in the middle ears is evident.Wei-Yin Wang Shih-Yu Huang Chin-Jung Hsu Yung-Chien Huang Pa-Chun Wang
12 Fu Jen Journal of Medicine Vol.3 No.1 2005
Extension of bacterial infection from the subarachnoid space to the perilymphatic space may lead to variable extents of inner ear inflammation.
The sequence of events typically follows 3 stages.
In the acute stage, bacteria, leukocytes, and a serofibrinous exudate appear in the perilymphatic space. In the fibrous stage, granulation tissue consistingofhypertrophicfibroblastsandneovascularity results in fibrosis [5]. The ossification stage is characterized by metaplastic or osteoplastic bone formation which may occur as early as 3 days after the infection[6-8].
Imaging studies are often done later in the
disease stage when cochlear implantation is planned.
The findings may include ossification of the cochlea on high-resolution temporal bone CT, a slight reduction in the fluid signal within the cochlea on T2-weighted MR, and cochlear enhancement on gadolinium-enhanced T1-weighted images. Abnormal findings are observed in the cochlear basal turn and semicircular canals more often than in the middle and apical turns[9]. Labyrinthine enhancement on gadolinium-enhanced MR images is ascribable to the breakdown of the basal membrane of the labyrinthine vasculature, resulting in leakage of the paramagneticcontrast materials into the inflamed labyrinth soft tissue [10]. A correlation between clinical manifestations and MRI findings was established by Dichgans[11]; the stronger left cochlear
Fig 3.
Gadolinium-enhanced T1-weighted image.Abnormal enhancement in the bilateral cochlea, especially on the left side (yellow circle), can be seen.
Fig 4.
T2-weighted MR image. Reduction in fluid signal within the left side cochlea (yellow circle) is apparent.Miningogenic Labyrinthitis in Systemic Lupus Erythmatosus
enhancement in this patient (on gadolinium- enhanced T1-weighted images) may explain her more-severe audiological symptoms on this side.
The intense enhancement on T1-weighted images may predict future cochlear fibrosis and ossification;
earlyimplantationmightaccordingly berecommended
[6].
Dichgans reported that hearing impairment can be noticed clinically between the 2nd and 45th hospitalizationdays.Patientswithothercomplications, such as subdural effusion, convulsions, brain edema, and paralysis, were found to have a higher incidence of hearing loss[12]. However, diagnosis of hearing impairment can be delayed until after cerebral or systemic complications are controlled.
Early identification of SNHL secondary to meningitis is imperative because the success rate of cochlear implantation may drop over time following maturation of the cochlear ossification
[13]. There is an ideal window of opportunity during which implantation can be executed. Afterwards, thecochlearductmaybeobliteratedbyosteoneogenesis, often within a few months of the occurrence of meningitis[14].
The use of short-period dexamethasone as an adjunct to antibiotic therapy remains controversial in the treatment of bacterial meningitis. Although evidence has shown that the incidence of SNHL can be reduced in H. influenzae meningitis when dexamethasone is in use [15], no clear evidence exists to support the usefulness of dexamethasone in reducing the SNHL rate after pneumococcal meningitis. In addition, there are some concerns that use of dexamethasone may decrease the penetration of antibiotics (such as vancomycin) into the CSF[16]. Ismail and Kulahli concluded that severe SNHL is less-often seen in groups receiving both dexamethasone and antibiotic as compared to groups treated by antibiotics alone. The body temperature, CSF cell count, protein concentration,
and glucose level also returned to normal levels more quickly in the dexamethasone plus antibiotics group[12].
Recovery of hearing impairment may be observed during the convalescent stage. Smyth reported the amelioration of SNHL in 2/3 of acute- phase patients. Brookhouser reported that patients with mild or moderate hearing impairment may eventually completely recover; but hearing may never return for those who had no initial reaction of the ABR[12].
CONCLUSION
Bacterial labyrinthitis is a well-known, but easily overlooked complication of meningitis, especially when it occurs in adult patients. Due to the severity of labyrinthitis, subsequent ossification and possible treatment are closely related to the early MRI findings. MR imaging studies should be arranged as early as possible once a diagnosis of meningitisisestablishedandauralsymptomsarepresented.
REFERENCES
1. Schuchat A, Robinson K, Wenger JD, et al. Bacterial meningitis in the United States in 1995: active surveillance team. N Engl J Med 1997;337:970-976.
2. Dodge PR, Davis H, Feigin RD, et al. Prospective evaluation of hearing impairment as a sequela of acute bacterial meningitis. N Engl J Med 1984;
311:869-874.
3. Blank AL, Davis GL, VanDeWater TR, et al. Acute Streptococcuspneumoniaemeningogeniclabyrinthitis:
an experimental guinea pig model and literature review. Arch Otolaryngol Head Neck Surg 1994;
120:1342-1346.
4. Merchant SN, Gopen Q. A human temporal bone study of acute bacterial meningogenic labyrinthitis.
Am J Otol 1996;17:375-385.
Wei-Yin Wang Shih-Yu Huang Chin-Jung Hsu Yung-Chien Huang Pa-Chun Wang
14 Fu Jen Journal of Medicine Vol.3 No.1 2005
5. Paparella MM, Sugiura S. The pathology of suppurative labyrinthitis. Ann Otol RhinolLaryngol 1967;76:554-586.
6. Hegarty JL, Patel S, Fischbein N, et al. The value of enhanced magnetic resonance imaging in the evaluation of endocochlear disease. Laryngoscope 2002;112:8-17.
7. Tinling SP, Colton J, Brodie HA. Location and timing of initialosteoiddepositionin postmeningitic labyrinthitis ossificans determined by multiple fluorescent labels. Laryngoscope 2004;114:675-680.
8. Nabili V, Brodie HA, Neverov NI, et al. Chronology of labyrinthitis ossificans induced by Streptococcus pneumoniameningitis.Laryngoscope1999;109:931-935.
9. Himi T, Akiba H, Yamaguchi T. Topographic analysis of inner ear lesions in profoundly deafened patients with tympanogenic and meningogenic labyrinthitis using three-dimensional magnetic resonance imaging. Am J Otol 1999;20:581-586.
10. Mafee MF. MR Imaging of intralabyrinthine schwannoma, labyrinthitis, and other labyrinthine
pathologies. Otolaryngol Clin North Am 1995;28:
407-430.
11. Dichgans M, Jager L, Mayer T, et al. Bacterial meningitis in adults: demonstration of inner ear involvement using high-resolution MRI. Neurology 1999;52:1003-1009.
12. Kulahi I, Ozturk M, Bilen C, et al. Evaluation of hearing loss with auditory brainstem responses in the early and late period of bacterial meningitis in children. J Laryngol Otol 1997;111:223-227.
13. WellmanMB,SommerDD,McKennaJ.Sensorineural hearing loss in postmeningitic children. Otol Neurotol 2003;24:907-912.
14. Drake R, Dravitski J, Voss L. Hearing in children after meningococcal meningitis. J Pediatr Child Health 2000;36:240-242.
15. Lebel MH, Freij B, Syrogiannopoulos GA, et al.
Dexamethasone therapy for bacterial meningitis.
N Engl J Med 1988;319:964-971.
16. Roos K. Acute bacterial meningitis. Semin Neurol 2000;20:293-306.
Miningogenic Labyrinthitis in Systemic Lupus Erythmatosus
紅斑性狼瘡成人併發肺炎雙球菌敗血症引起的 腦膜炎續發細菌性迷路炎—病例報告
王維吟
1
黃奭毓2
許晉榮2
黃永堅3
王拔群1,4, *
神經性聽力喪失是細菌性腦膜炎之併發症。大部分的病人為兒童。成年人的腦膜 炎發生機率並不高而之後又併發感覺神經性聽力喪失的比率一般也認為遠低於兒童。
細菌性腦膜炎後之感覺神經性聽力喪失為耳蝸受到侵犯所致。其路徑有三:從內聽道,
經由血液來源,及耳蝸導水管。影像方面可能的發現有:在電腦斷層上可見耳蝸之鈣
化,在核磁共振造影T2 影像上,耳蝸之水信號減弱以及在核磁共振造影 T1 影像加顯
影劑上,耳蝸會有異常的顯影。 病人早期接受聽性腦幹反射檢查如果無反應,聽力一 般不會恢復。抗生素加上類固醇治療對於聽力的改善或許會有幫助。本文報告一接受 腹膜透析之紅斑性狼瘡病人在細菌性腦膜炎後併發不常遇見的兩側感覺神經性聽力喪 失。我們同時瀏覽相關文獻並加以討論。(輔仁醫學期刊
2005;3 (1) :9-15 )
關鍵詞:細菌性腦膜炎,神經性聽力喪失,細菌性迷路炎
國泰綜合醫院耳鼻喉科1 國泰綜合醫院腎臟內科2 國泰綜合醫院放射線科3 輔仁大學醫學系4
投搞日期:2004 年 12 月 21 日;接受日期:2005 年 03 月 15 日
* 通訊聯絡作者:電子郵件:[email protected]
Case Report
INTRODUCTION
Small cell carcinoma (SCC) of the prostate is rare and is thought to behave clinically as a highly aggressive neoplasm [1]. Early diagnosis of SCC is quite difficult, because of early dissemination, rapid growth, and lack of a concordant elevation in serum PSA levels as with a usual acinar adenocarcinoma of the prostate. These cases usually present at a high stage with multiple bone, lymph node, and visceral organ metastases. Because of the rarity of the condition, no standard therapeutic regimen has been developed.
Gemcitabine,afluorine-substituteddeoxycytidine analog, produced a 27% overall response rate in
previously untreated patients of SCC of the lung
[2]. The combination of carboplatin and gemcitabine has recently emerged as a relatively new standard regimen for SCC of the lung [3]. A phase III trial of patients with SCC of the lung and a poor prognosis revealed comparable overall response and median survival rates using the combination of carboplatin and gemcitabine with those of etoposide and cisplatin, but less non-hematologic toxicity was seen[3].
We present the clinical and pathologic pictures of 1 case of small cell carcinoma of the prostate.
The metastatic bone lesions showed a partial responsetothecombinationofgemcitabineandcarboplatin.
Gemcitabine/Carboplatin Chemotherapy for Pure Small Cell Carcinoma of the Prostate: A Case Report
Kuan Chou Chen 1 Allen W. Chiu 1,2 Han-Sun Chiang 1,3 Jan-Show Chu 4 Chien-Jui Cheng 4, *
Small cell carcinoma of the prostate is rare and is thought to behave clinically as a highly aggressive neoplasm. We report on a patient with pure small cell carcinoma of the prostate presenting as multiple organ metastases. Immunohistochemical studies of the tumor cells revealed positive reactions to chromogranin A, synaptophysin, and cytokeratin stains, and a negative reaction to PSA stain. This patient received 5 courses of gemcitabine/carboplatin chemotherapy after transurethral resection of the prostate, and the previous metastatic bone lesions showed partial resolution. (
FJJM 2005; 3 (1): 17-23 )
Key words: chemotherapy, prostate, small cell carcinoma, neuroendocrine, immunohistochemical studies
Department of Urology, Taipei Medical University Hospital, Taipei, Taiwan1 Taipei Municipal Chung Hsiao Hospital, Taipei, Taiwan2 College of Medicine, Fu Jen Catholic University, Taipei, Taiwan3 Department of Pathology, Taipei Medical University Hospital, Taipei, Taiwan4
Submitted February, 10, 2004; final version accepted March, 2 , 2005
* Correspondence author: [email protected]
Kuan Chou Chen Allen W. Chiu Han-Sun Chiang Jan-Show Chu Chien-Jui Cheng
18 Fu Jen Journal of Medicine Vol.3 No.1 2005
CASE REPORT
A 79-year-old man underwent transurethral resection of the prostate (TURP) due to repeated urinary retention. The pathological report revealed pure small cell carcinoma (SCC) of the prostate.
The tumor was composed of small- to medium- sized tumor cells with scanty cytoplasm and inconspicuousnucleoli(Fig.1A).Immunohistochemical studies revealed positive reactions to chromogranin A stain (Fig.1B), synaptophysin stain, and cytokeratin stain, and a negative reaction to PSA stain. No
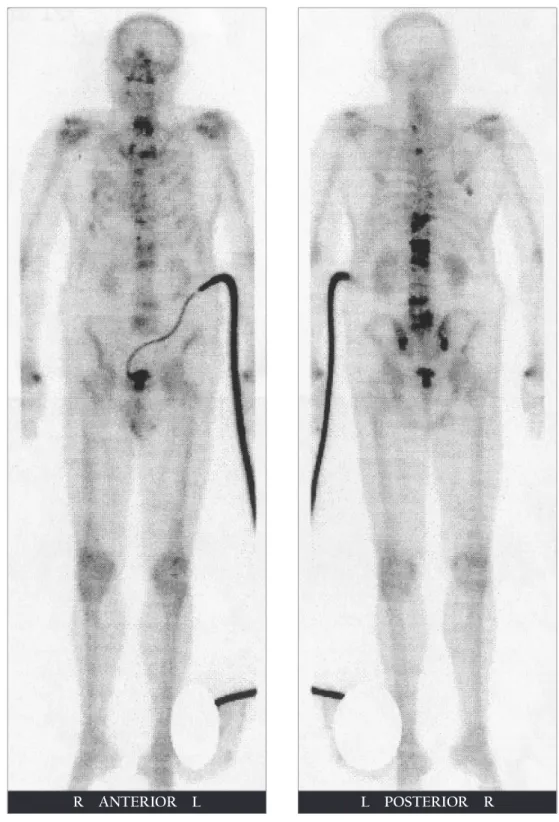
usual acinar adenocarcinoma was seen after all tissues were submitted for a diagnosis. Computed tomography (CT) revealed multiple metastases, including to the liver, spleen, pelvic lymph nodes, and bones. A bone scan demonstrated multiple bone metastases to the ribs, all thoracic and lumbar vertebrae, the sacrum, and bilateral sacroiliac joints (Fig. 2A). After 5 courses of gemcitabine/carboplatin chemotherapy, the previous metastatic bone lesions in the T11, T12, L1, L2, L4, and L5 vertebrae showed partial resolution (Fig. 2B), but the other metastatic lesions remained unchanged. During the 5 courses of chemotherapy, the most-common side effects were a poor appetite, nausea, and vomiting, and these could be well controlled by administration of corticosteroids. Pancytopenia was also noted after every course of chemotherapy, but it was always reversible within 2 weeks. A check of the PSA value was omitted before the TURP, but the PSA value after the final course of chemotherapy was 0.06 ng/ml. He died shortly after the final course of chemotherapy due to sudden cardiac arrest with a survival duration of 7.4 months.
DISCUSSION
Primary SCC is well known in the lung, but SCC of the prostate is a very rare condition, comprising 0.5%~2% of prostate cancers[4]. These extrapulmonary SCCs are indistinguishable from SCC of the lung by light microscopic, ultrastructural, and immunohistochemical examinations.
Neuroendocrine differentiation of prostate cancer includes pure SCC, carcinoid and carcinoid- liketumors,andaconventionalprostateadenocarcinoma with focal neuroendocrine differentiation[5]. Pure SCC has a more-aggressive clinical course with a dismal prognosis.
SCC of the prostate was proposed to arise from amine precursor uptake decarboxylation
(A)
(B)
Fig. 1
(A) Small- to medium-sized tumor cells with scanty cytoplasm and inconspicuous nucleoli (H&E stain, 400x). (B) Tumor cells reactive to chromogranin A. (ABC stain, 400x).Gemcitabine/Carboplatin Chemotherapy for Pure Small Cell Carcinoma of the Prostate
Fig. 2
(A) Bone scan showing skeletal metastases in the ribs, T1-L5 spine, sacrum, and both sacroiliac joints.R ANTERIOR L L POSTERIOR R
Kuan Chou Chen Allen W. Chiu Han-Sun Chiang Jan-Show Chu Chien-Jui Cheng
20 Fu Jen Journal of Medicine Vol.3 No.1 2005
Fig. 2
(B) Follow-up bone scan revealing partial resolution of the previous metastatic lesions in the T11, T12, L1, L2, L4, and L5.R ANTERIOR L L POSTERIOR R
Gemcitabine/Carboplatin Chemotherapy for Pure Small Cell Carcinoma of the Prostate
(APUD) cells of local endodermal origin[6]or from dedifferentiation of prostatic adenocarcinomas[7]. But the most-widely accepted view is that prostatic SCC, similar to lung cancer, arises from totipotential stem cells of the prostate, which have the ability to differentiate intoeither epithelial orneuroendocrine type carcinomas[8,9]. This concept is supported by the similarity of the histopathologic pictures and immunohistochemical studies, and by the presence ofsomeparaneoplasticsyndromes.Immunohistochemical studies often show multidirectional differentiation along epithelial,neuroendocrine, and/ormesenchymal lines of these poorly differentiated prostate cancers
[10,11].
In contrast to a prostatic adenocarcinoma, PSA is an unreliable tumor marker for SCC and is usually normal, even when there is metastatic disease.Onestudysuggestedthatthecarcinoembryonic antigen is a more-reliable marker, because increases and decreases in antigen levels are found with disease progression and regression,respectively[9].
SCC of the prostate has a propensity to metastasize to visceral organs, including the liver, bones,lungs, central nervoussystem, and pericardium, and regionally to pelvic lymph nodes, the rectum, and bladder[9].
The small cell lung cancer (SCLC) of prostate cancer has the same unfavorable outcome as other SCC counterparts [12]. SCC of the prostate has a highly aggressive course and a poor prognosis, with no successful treatment to the present. SCC of the prostate, as distinct from an adenocarcinoma, has been found to be unresponsive to hormone therapy.
Despite chemotherapy with different combinations of reagents, the prognosis of SCC is extremely poor, and the median survival is 7 months[13].
The combinationof carboplatin and gemcitabine has emerged as a standard regimen for SCC lung cancer[3]. By combining gemcitabine and carboplatin, we achieved a partial response to the metastatic
bone lesions, but adjustments and modifications of the regimens and dosages are still necessary to achieve a more-effective response.
REFERENCES
1. Bolton DM, Chiu ST, Clarke S, et al. Primary small cell carcinoma of the prostate: unusual modes of presentation. Aust NZ Surg 1994;64:91-94.
2. CormierY,EisenhauerE, MuldalA, etal.Gemcitabine is an active new agent in previously untreated extensive small cell lung cancer (SCLC). A study of the National Cancer Institute of Canada Clinical Trials Group. Ann Oncol 1994;5:283-285.
3. Simon M, Argiris A, Murren JR. Progress in the therapy of small cell lung cancer. Crit Rev Oncol Hematol. 2004;49:119-133.
4. Helpap B, Kollermann J, Oehler U. Neuroendocrine differentiation in prostatic carcinomas: histogenesis, biology, clinical relevance, and future therapeutical perspectives. Urol Int 1999;62:133-138.
5. di Sant'Agnese PA. Neuroendocrine differentiation in carcinomaof the prostate. Diagnostic, prognostic, andtherapeuticimplications.Cancer1992;70:254-268.
6. di Sant'Agnese PA, Cockett AT. Neuroendocrine differentiation in prostatic malignancy. Cancer 1996;78:357-361.
7. Schron DS, Gipson T, Mendelsohn G. The histogenesis of small cell carcinoma of the prostate.
An immunohistochemical study. Cancer 1984;53:
2478-2480.
8. Aygun C. Small cell carcinoma of the prostate: a case report and review of the literature. MD Med J 1997;46:353-356.
9. Rubenstein JH, Katin MJ, Mangano MM et al.
Small cell anaplastic carcinoma of the prostate:
seven new cases, review of the literature, and discussion of a therapeutic strategy. Am J Clin Oncol 1997;20:376-380.
10. Helpap B, Kollermann J. Undifferentiatedcarcinoma
Kuan Chou Chen Allen W. Chiu Han-Sun Chiang Jan-Show Chu Chien-Jui Cheng
22 Fu Jen Journal of Medicine Vol.3 No.1 2005
of the prostate with small cell features:
immunohistochemical subtyping and reflections on histogenesis. Virchows Arch 1999;434:385-391.
11. Weaver MG, Abdul-Karim FW, Srigley JR. Paneth cell-like change and small cell carcinoma of the prostate. Two divergent forms of prostatic neuroendocrine differentiation. Am J Surg Pathol 1992;16:1013-1016.
12. Jelbert ME, Russell PJ, Russell P. The biology and managementof smallcellundifferentiated carcinoma of prostate. In: Williams CJ, Krikarian JG, Green MR, Rayhaven D, eds. Textbook of Uncommon Cancer. London: Wiley; 1998:249-262.
13. Patel A, Ball J, Chappell M. Pure primary small cell carcinoma of the prostate. Br J Urol 1993;72:
380-381.
Gemcitabine/Carboplatin Chemotherapy for Pure Small Cell Carcinoma of the Prostate
Gemcitabine 及 Carboplatin 的複合性化學治療
治療單純前列腺小細胞癌陳冠州
1
邱文祥1,2
江漢聲1,3
朱娟秀4
鄭建睿4, *
前列腺小細胞癌為少見的前列腺惡性疾患。我們報告一位病人為單一細胞型態的 單純小細胞癌,診斷時已合併骨骼及多重器官之轉移。病灶病理切片組織免疫特殊染 色呈現chromogranin A, synaptophysin, and cytokeratins 陽性,及陰性的 PSA 染色。病 人在經尿道前列腺切除手術做出診斷後給予gemcitabine 及 carboplatin 的複合性化學治 療,其骨骼轉移病灶得到部分改善。(輔仁醫學期刊
2005;3 (1) :17-23 )
關鍵詞:攝護腺,小細胞癌,神經內分泌,組織免疫染色
臺北醫學大學附設醫院泌尿科1 臺北市立聯合醫院忠孝院區泌尿科2 私立輔仁大學醫學院3 臺北醫學大學附設醫院病理科4
投搞日期:2005 年 2 月 10 日;接受日期:2005 年 3 月 2 日
* 通訊聯絡作者:電子郵件:[email protected]
綜 論
室檢驗和藥物治療等經濟學模式估計痛風的影 響,則美國每年對以1/1000 發生率的新發病 45 歲男性急性痛風患者的直接醫療負擔就超過 2700 萬美元[3]。因此,痛風不僅是一種常見的疾 病,更由於其經常伴隨著短期的失能、職業工作 的限制和醫療資源的使用,所以,痛風也是一個 重要的公共衛生問題。
高尿酸血症(hyperuricemia)可定義為血清尿 酸鹽濃度大於7.0 mg/dl (420 mol/L)。在生理化 學上,高尿酸血症是指血中的尿酸鹽超過單鈉尿 酸鹽在血槳的飽和度。此數值約為7.0 mg/dl[4]。 流行病學上則以健康人的血中尿酸鹽平均值加上 兩個標準差定義為高尿酸血症。隨機測量的結果 緒 論
痛風(gout)是一種由於尿酸合成增加或排出 減少,導致尿酸鹽沈積所引起的疾病[1]。痛風包 含了一群可單獨或共同出現的疾病,這些失調包 括了:(1)高尿酸血症;(2)反覆發作一種特有形 式的急性關節炎,關節滑液內白血球可發現尿酸 鹽晶體;(3)尿酸鹽晶體聚集的痛風石,沉積在 關節內和關節附近;(4)尿酸鹽晶體沉澱在腎臟 的組織間質,使腎臟受損;(5)尿酸腎結石。這
些症狀可單獨出現或一起出現。據估計1979 到
1981 年美國人因痛風而導致活動的限制達 3700 萬人日[2]。而若以包括痛風的初診、確診、實驗
中台醫護技術學院醫務管理系1 國立陽明大學公共衛生研究所2
投搞日期:2004 年 11 月 9 日;接受日期:2004 年 3 月 26 日
* 通訊聯絡作者:電子郵件:[email protected]
痛風與高尿酸血症的認知與管理
黃麗玲
1,2
林川雄1
黃建財1, *
本文的目的在回顧最近流行病學上痛風與高尿酸血症的文章,以對痛風與高尿酸 血症的認知與管理有新的見解,同時也回顧有關痛風與高尿酸血症臨床上關注的文章。
結果發現痛風的自然發展史中,可分作四期:無症狀的高尿酸血症、急性痛風性關節
炎、發作間期及慢性痛風性關節炎。痛風是40 歲以上成年男子最常見的關節炎疾病。
此外,痛風的發生率正在增加中,且發生的年齡愈來愈早;此很可能與飲食習慣的改 變,導致高尿酸血症的發展,進而形成痛風有關。病人在無症狀的高尿酸血症期間,
並不需要治療,但需要鼓勵他們藉由改變飲食或生活型態來降低體內的尿酸鹽濃度。
使用非類固醇抗發炎藥物、秋水仙素、皮質類固醇或鎮痛劑可終止急性痛風關節炎的 發作。而預防急性痛風症狀的復發則可以使用增加腎臟排泄尿酸的藥物及減少尿酸製 造的藥物。此外,肥胖、喝酒和某些特定的食物或藥物可促成高尿酸血症的形成。建 議這些潛在加重疾病的因子也應該被確認和改變。(輔仁醫學期刊