Complete Recovery from Dasatinib-induced Pulmonary Arterial Hypertension after Successful
Discontinuation of Tyrosine Kinase Inhibitor in A Case of Chronic Myeloid Leukemia
En-Jie Shih
1,2, Shih-Hsien Sung
1,3, and Jyh-Pyng Gau
1,41
Faculty of Medicine, National Yang-Ming University, Taipei, Taiwan;
2
Department of Medical Education,
3Division of Cardiology,
4Division of Hematology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
Abstract
Chronic myeloid leukemia could be treated by tyrosine kinase inhibitor successfully. However, a few rare but lethal adverse reactions have been reported. In cases of dasatinib-induced pulmonary arterial hyperten- sion (PAH), the majority generally recovers incompletely and needs alternative TKIs for CML treatment. A 34-year-old woman diagnosed with chronic myeloid leukemia (CML) had taken dasatinib for more than two years. Before dasatinib, she had been under nilotinib treatment for two years, achieving complete molecular response at sixth months, but with persistent hyperbilirubinemia and epigastric discomfort. Twenty months after shifting to dasatinib, she began to experience shortness of breath. Severe pulmonary arterial hyperten- sion was subsequently diagnosed. After withdrawal of dasatinib, the PAH thoroughly resolved. Moreover, complete molecular response was maintained for more than two years without additional tyrosine kinase inhibitor (TKIs) administration. The strength of our case is that the patient fully recovered from the dasatinib- induced severe PAH and kept complete molecular response without taking other TKIs. Early detection of the adverse effect of dasatinib is important for better outcomes. (J Intern Med Taiwan 2019; 30: 161-165)
Key Words: Chronic myeloid leukemia, Dasatinib, Pulmonary arterial hypertension, Tyrosine kinase inhibitor
Reprint requests and correspondence:Dr. Jyh-Pyng Gau
Address:Division of Hematology, Department of Medicine, Taipei Veterans General Hospital, No. 201, Sec 2, Shih-Pai Road, Taipei 112, Taiwan
Introduction
Patients with chronic myeloid leukemia (CML) are administered with tyrosine kinase inhibitors (TKIs) to extend their life expectancy as to that of the general population
1,2,3. Subsequently, reducing the side effects of TKI also becomes equally impor- tant. The second-generation TKIs, such as nilotinib
and dasatinib, are treatment options with better out-
comes comparing to first-generation TKI, imatinib
1.
Several studies have reported the hematologic and
non-hematologic adverse effects of these TKIs
1,4,5.
Pulmonary arterial hypertension (PAH) is one of
the uncommon but severe cardiovascular compli-
cations related to dasatinib
6-12. Understanding the
possibility of occurrence and signs of PAH is neces-
sary for early diagnosis and management. In addi- tion, most of the cases of dasatinib-induced PAH could only recover partially and another TKI for further CML treatment is usually necessary. Here, we report a case of CML developing critical PAH after dasatinib therapy, and the patient achieved complete recovery after drug discontinuation.
Case report
A 34-year-old woman presenting with marked leukocytosis of 465,000/µL and a differential of blast less than 10% was diagnosed with chronic myeloid leukemia in June 2011. Philadelphia chro- mosome, t(9;22) (q43;q11.2), and BCR-ABL fusion gene with a subtype of p210 b3a2 were noted. She was then prescribed with nilotinib 300 mg twice daily. Because of the adverse effects of hyperbili- rubinemia and persistent epigastric discomfort, she was switched to dasatinib therapy and her total bili- rubin level decreased from 2.24 mg/dl to a normal level thereafter. In addition, the patient achieved the hematologic goal within three months with TKI therapy, the molecular response was up to 4.5 log reduction in BCR-ABL transcript level at 6 months.
One and a half years after dasatinib therapy, the patient experienced progressively exertional dyspnea. Because of the New York Heart Associa- tion (NYHA) functional class III symptoms, jugular
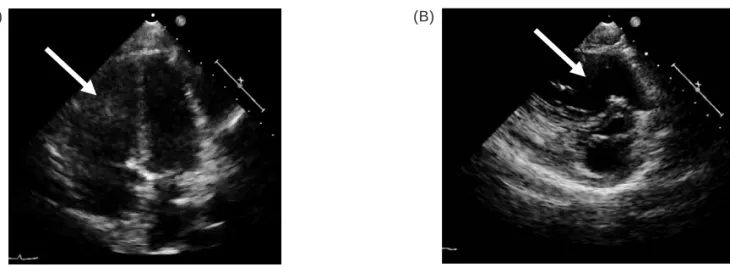
vein engorgement, and accentuated P2 on ausculta- tion, she underwent echocardiogram, revealing an estimated right ventricular systolic pressure (RVSP) of 111 mmHg, dilated right ventricle and right atrium, and normal left ventricular systolic func- tion (Figure 1A and B). Right heart catheteriza- tion illustrated pulmonary arterial wedge pressure of 11 mmHg, mean pulmonary arterial pressure of 30 mmHg, cardiac index of 2.72 L/min/m
2, and negative vasoreactivity test. Further examinations, including pulmonary function test, arterial blood gas analysis, and chest computed tomography scan confirmed the diagnosis of PAH. The serologic studies did not show evidence of human immunode- ficiency virus infection, viral hepatitis, or connec- tive tissue disease.
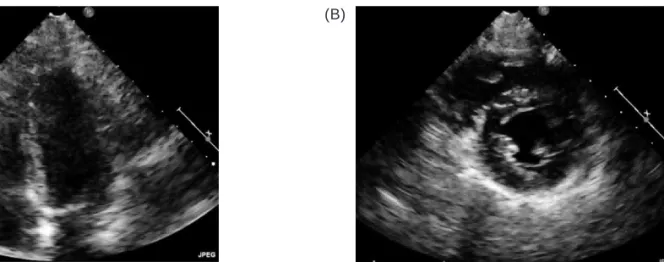
Dasatinib was withdrawn, and the patient was put on sildenafil therapy under the impression of drug-related PAH. The patient’s symptoms signifi- cantly improved to NYHA functional class I, and her follow-up echocardiogram at the fourth month showed normal RVSP, and normalized right ventric- ular size and function (Figures 2A and B). Sildenafil was then tapered, and further echocardiography up to 2 years all showed normal RVSP and normal right ventricular performance. In addition, her CML remained in complete molecular response without additional TKIs.
(A) (B)
Figure 1. (A) Four-chamber view of the patient’s echocardiogram. (B) Short-axis view of the patient’s echocardio-
gram. Echocardiograms of (A) and (B) revealed normal LV function, dilated RV (arrows) and RA, and pre-
served RV function. LV= left ventricle, RV= right ventricle, RA= right atrium.
Discussion
Before the invention of TKIs, interferon-α (IFNα) and stem cell transplantation (SCT) were two major options to cure CML patients
1. However, IFNα had many unfavorable side effects, such as pancytopenia, flu-like syndromes, and hair loss. On the other side, despite its high cure rate with a 3-year survival rate of more than 80%, SCT has formidable potential complications of graft-versus-host disease.
Without any curative attempt, patients on palliative medications of hydroxyurea will have acute leuke- mia with a median duration of approximately 4.5 years.
Prior to 2001, more than 2 in 3 CML patients died 5 years after they have been diagnosed.
Because of TKI administration, the overall survival rate of CML patients now is 89%, and the rate of survival of CML-related death is about 95% within 3 years
12,13. Thus, identifying the adverse effects of this agent should be important to improve CML patients’ quality of life. Imatinib is the first-genera- tion TKI for CML patients from 2000 to 2005. Since then, second-generation TKIs, such as dasatinib, nilotinib, were introduced with more effective com- plete cytogenetic response (CCyR), major molecular response (MMR), and favorable event-free survival (EFS)
1. Hence, the current trend of CML treatment is to use second-generation TKIs as a frontline
therapy for certain population for MMR or complete molecular response (CMR)
14.
The adverse effects of TKIs could be classified as hematologic and non-hematologic events. PAH is a rare cardiovascular complication, while the first case of dasatinib-related PAH has been reported in 2009
10. Montani et al. have presented 9 cases of dasatinib-related PAH, and two of them died of cardiac failure
7. The other patients remained symp- tomatic persistently after being switched to other TKI drugs. It is suggested that dasatinib has a caus- ative relationship with PAH, which may be fatal and irreversible even after withdrawing dasatinib
7-12.
Instead of taking TKIs for the rest of CML patients life in the past, physicians began to focus on the time to stop medications
1,2,15. However, the safety criteria for discontinuation of TKIs has not yet been established. Several studies targeting with- drawal of imatinib after more than 32 months of treatment indicated 50% of molecular relapse rate within 12 months. In 2016, one research reported that the cumulative incidences of molecular relapse from dasatinib or nilotinib discontinuation was 35%
by one year after at least a 3-year therapy
2. It seems that long-term discontinuation of TKIs seems pos- sible for patients having achieved deep molecular response for a certain period of time.
The strength of our case report is that the patient recovered completely from the dasatinib-
(A) (B)
Figure 2. (A) Four-chamber view of the patient’s echocardiogram. (B) Short-axis view of the patient’s echocardio-
gram. The images of (A) and (B) show the normal RV size. RV = right ventricle.
induced severe PAH according to the NYHA functional classification and her echocardiogram findings. In addition, she also maintained com- plete molecular response after discontinuation of dasatinib for more than 2 years without additional TKIs. Physicians should be vigilant on the potential complication of dasatinib-induced PAH, and early discontinuation of the agent allows the patient to completely recovery.
References
1. Cortes J, Kantarjian H. How I treat newly diagnosed chronic phase CML. Blood 2012; 120: 1390-7.
2. Saussele S, Richter J, Hochhaus A, et al. The concept of treat- ment-free remission in chronic myeloid. Leukemia 2016; 30:
1638-47.
3. Riou M, Seferian A, Savale L, et al. Deterioration of pulmo- nary hypertension and pleural effusion with bosutinib follow- ing dasatinib lung toxicity. Eur Respir J 2016; 48: 1517-19.
4. Valent P, Hadzijusufovic E, Schernthaner GH, et al. Vascular safety issues in CML patients treated with BCR/ABL1 kinase inhibitors. Blood 2015; 125: 901-6.
5. Pasvolsky O, Leader A, Iakobishvili Z, et al. Tyrosine kinase inhibitor associated vascular toxicity in chronic myeloid leu- kemia. Cardio-Oncology 2015; 1: 5.
6. Galie N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS guide- lines for the diagnosis and treatment of pulmonary hyperten- sion. Rev Esp Cardiol (Engl Ed) 2016; 69: 177.
7. Montani D, Bergot E, Günther S, et al. Pulmonary arterial hypertension in patients treated by dasatinib. Circulation 2012; 125: 2128-37.
8. Seegobin K, Babbar A, Ferreira J, et al. A case of worsen- ing pulmonary arterial hypertension and pleural effusions by bosutinib after prior treatment with dasatinib. Pulm Circ 2017; 7: 808-12.
9. Guignabert C, Phan C, Seferian A, et al. Dasatinib induces lung vascular toxicity and predisposes to pulmonary hyper- tension. J Clin Invest 2016; 126: 3207-18.
10. Moslehi JJ, Deininger M. Tyrosine kinase inhibitor-associated cardiovascular toxicity in chronic myeloid leukemia. J Clin Oncol 2015; 33: 4210-8.
11. Weatherald J, Chaumais MC, Savale L, et al. Long-term out- comes of dasatinib-induced pulmonary arterial hypertension:
a population-based study. Eur Respir J 2017; 50.
12. Yun S, Anwer F, Vincelette ND. Dasatinib-induced pulmonary hypertension in chronic myelogenous leukaemia. BMJ Case Rep 2014; 2014.
13. Rea D, Nicolini FE, Tulliez M, et al. Discontinuation of dasat- inib or nilotinib in chronic myeloid leukemia: interim analysis of the STOP 2G-TKI study. Blood 2017; 129: 846-54.
14. Mario A, Roberto L, Alessandra L, et al. Young CML Patients Treated Frontline with Imatinib or Second Generation TKIs:
Clinical Characteristics and Outcome. Blood 2016; 128:
3078.
15. Cortes JE, Saglio G, Kantarjian, HM, et al. Final 5-year study results of DASISION: the dasatinib versus imatinib study in treatment-naive chronic myeloid leukemia patients trial. J Clin Oncol 2016; 34: 2333-40.
慢性骨髓性白血病患者服用 dasatinib 導致的肺高壓 在停藥後復原,且不需再服用酪胺酸激酶抑制劑:
病例報告
施恩潔1,2 宋思賢1,3 高志平1,4
1國立陽明大學醫學系
臺北榮民總醫院 2教學部 內科部 3心臟科 4血液科
摘 要