Research Express@NCKU - Articles Digest
Research Express@NCKU Volume 10 Issue 10 - October 9, 2009 [ http://research.ncku.edu.tw/re/articles/e/20091009/4.html ]
Sustained hepatitis B e antigen
seroconversion in patients with chronic
hepatitis B after adefovir dipivoxil treatment:
analysis of precore and basal core promoter mutants
I-Chin Wu
*, Ting-Tsung Chang
Department of Internal Medicine, College of Medicine, National Cheng Kung University
Clinical Infectious Disease 2008 Nov;47:1305-1311
C
hronic hepatitis B patients are at risk for development ofcirrhosis and hepatocellular carcinoma, and 15% to 40% will develop cirrhosis, liver failure, or hepatocellular carcinoma during their lifetime. Several nucleoside or nucleotide analogues could be used as antiviral therapy. However, long-term therapy is necessary because recurrence develops after discontinuation of antiviral therapy.
Hepatitis B e antigen (HBeAg) seroconversion (loss of HBeAg and appearance of antibody to HBeAg) is considered to be an important therapeutic endpoint. Current treatment guidelines for HBeAg positive chronic hepatitis B recommend that nucleoside or
nucleotide analogue treatment should be continued until the patient
has achieved HBeAg seroconversion with undetectable serum hepatitis B virus (HBV) DNA and completed at least 6 months of additional treatment (consolidation therapy). HBV precore mutant abolishes synthesis of HBeAg, and basal core promoter mutant reduces synthesis of HBeAg. Previous studies found that these mutants were associated with HBeAg-negative hepatitis B, hepatocellular carcinoma, and advanced liver disease, but little is known regarding the role of these mutants in antiviral therapy. Adefovir dipivoxil, a nucleotide analog of adenosine monophosphate, is used to treat chronic hepatitis B. The objective of this study was to investigate the durability of HBeAg seroconversion after discontinuation of therapy in patients who had experienced HBeAg seroconversion in a previous clinical trial of adefovir dipivoxil therapy. Precore and basal core promoter mutants before initiation of antiviral therapy and at the last visit were also analyzed.
Forty-five patients with confirmed HBeAg seroconversion and serum HBV DNA < 105 copies/mL while receiving adefovir dipivoxil in a prior clinical trial were enrolled in the present study. All patients tested HBeAg positive before adefovir dipivoxil therapy, had HBeAg seroconversion during antiviral therapy, and received regular follow-up after discontinuation of adefovir dipivoxil therapy. The lower limit of quantification for serum HBV DNA assay was 1000 copies/mL. Values from the HBV DNA assay that were less than 1000 copies/mL were set to 999 copies/mL for calculating summary statistics. At the time of the last dose of adefovir dipivoxil (baseline), the median age was 35 years, 64% were male, 73% were Asian, 27% were white, the median alanine aminotransferase was 25 IU/L, and the median serum HBV DNA were 3.0 log copies/mL. The median follow-up time was 150 weeks (range, 13–252 weeks). Forty-
1 of 3
Research Express@NCKU - Articles Digest
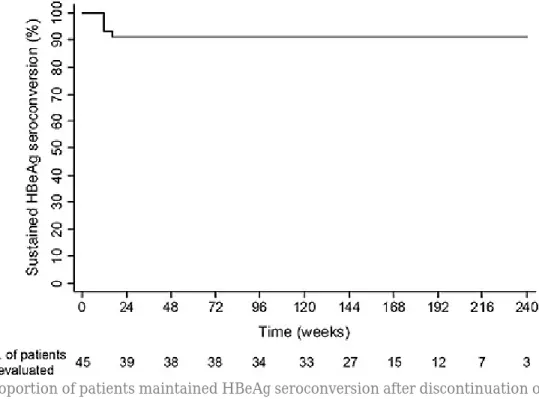
one patients maintained sustained seroconversion at the last 2 assessments, and four patients
experienced seroreversion (reappearance of HBeAg) at week 12 (3 patients) and week 16 (1 patient) of follow-up (Figure 1).
Figure 1. Proportion of patients maintained HBeAg seroconversion after discontinuation of adefovir dipivoxil. The survival curve was plotted by the Kaplan-Meier method.
Forty-nine percent (20/41) of patients with sustained HBeAg seroconversion had serum HBV DNA >
1000 copies/mL at the last visit. Among 13 patients who were viremic with available samples at the last visit, 11 had precore or basal core promoter mutants. Notably, 8 of these 11 patients had precore or basal core promoter mutants prior to adefovir dipivoxil therapy (Figure 2). The median duration of adefovir dipivoxil treatment was shorter before seroconversion (48 vs. 108 weeks; P = 0.03) and longer following seroconversion (41 vs. 22 weeks; P = 0.02) for patients with sustained seroconversion, compared with patients with seroreversion.
2 of 3
Research Express@NCKU - Articles Digest
Figure 2. Analysis for precore and core promoter mutants.
In conclusion, the majority of patients had sustained HBeAg seroconversion after discontinuation of adefovir dipivoxil over a median follow-up of 3 years. Prolonged antiviral therapy after HBeAg seroconversion appeared to increase sustained HBeAg seroconversion, and longer duration of
consolidation therapy might be needed in patients who experience seroconversion late after initiation of therapy. However, one-half of patients with sustained HBeAg seroconversion had viremia and most of them had precore or basal core promoter mutants, which usually existed prior to adefovir dipivoxil therapy. The clinical significance of these mutants in patients receiving antiviral therapy needs to be illustrated in large clinical trials.
References:
1. Nguyen MH, Keeffe EB. Are Hepatitis B e Antigen (HBeAg)-Positive Chronic Hepatitis B and HBeAg-Negative Chronic Hepatitis B Distinct Diseases? Clin Infect Dis 2008;47:1312-4.
2. Lok ASF, McMahon BJ. Chronic hepatitis B. Hepatology 2007;45:507-39.
3. Liaw YF, Leung N, Kao JH, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int 2008;2:263-83.
3 of 3