國立臺灣大學醫學院暨工學院醫學工程學研究所 博士論文
Institute of Biomedical Engineering College of Medicine and Engineering
National Taiwan University Doctoral Dissertation
定量評估表面註冊法於導航系統之準確度–
應用於真人內視鏡鼻竇手術
Quantitative Evaluation of the Surface Registration Accuracy of Navigation Systems –
in Live Endoscopic Sinus Surgery
張智銘
Chih-Ming Chang
指導教授﹕趙福杉 博士 Advisor: Fu-Shan Jaw, Ph. D.
中華民國 106年7月 July 2017
doi:10.6342/NTU201701967
I
誌謝
在此論文完成之際,首先要感謝指導老師趙福杉教授,在這四年的求學過 程中,給我許多寶貴的建議,解答許多研究上遇到的難題;您的悉心關懷,讓 我受益良多,在此表示深摯的謝忱。
謝謝我的啟蒙老師楊怡和教授,在我還是資淺住院醫師時,就開始指導我 做研究的態度和方法,建立我對研究工作的信心;老師在學術上的熱忱和成就,
是我學習的最佳典範。
感謝亞東醫院耳鼻喉科主任鄭博文教授,主任是我工作上的良師,生活中 的益友,這幾年遇到的困難都有主任的相挺;能有這樣的良師益友,我覺得非 常幸運。
謝謝召集委員黃基礎教授、口試委員柯政郁教授,及各位師長細心審查本 論文,你們的耐心指導和寶貴建議,讓本篇研究論文更臻完善。
最後要感謝我最愛的家人們,尤其是我的父母和太太,謝謝你們一直以來 的鼓勵和支持。我能無後顧之憂,順利完成學業,都要歸功你們的無私付出。
張智銘 謹誌於
台灣大學醫學工程學研究所
中華民國 106 年 7 月 15 日
中文摘要
自 1980 年代起,功能性內視鏡鼻竇手術已廣泛應用於鼻竇疾患之治療。90 年代開始,電腦輔助手術日益進展;在內視鏡手術合併即時影像導引之下,幫 助醫師更清楚定位術中解剖構造,預防術中併發症發生。進行電腦輔助手術時,
導航系統須對已儲存之術前影像及術中特定解剖位置進行連結,完成註冊步驟 後,方能進行定位。而使用表面註冊法的導航效能,以及光學導航和電磁導航 之比較,無論在活體手術或大體手術的研究則付之闕如。因此,本研究利用表 面註冊法進行真人內視鏡鼻竇導航手術,探討導航系統的設置及手術時間,分 析光學及電磁導航系統的導航準確度,分享我們臨床進行電腦輔助手術的經驗。
40 名雙側慢性全鼻竇炎之患者納入本研究,接受內視鏡鼻竇手術,使用表 面註冊法後,以電磁導航系統輔助進行手術。術中測量包含設備設置時間、表 面註冊時間、手術時間,以及三個軸向的導航誤差。結果顯示:設備設置時間、
表面註冊時間、手術時間分別為 179 ± 23 秒、39 ± 4.8 秒及 114 ± 36 分鐘。三 個軸向的導航誤差顯示左右軸向的誤差顯著小於前後軸向誤差及頭尾軸向誤 差。第二部分的研究納入 30 名雙側慢性全鼻竇炎之患者,手術醫師隨機於一側 鼻腔進行光學導航內視鏡鼻竇手術,另一側鼻腔則進行電磁導航內視鏡鼻竇手 術。術中測量包含表面註冊時間、手術時間,以及各軸向的導航誤差。結果顯 示:光學導航系統之表面註冊時間顯著大於電磁導航系統,手術時間兩者則無 明顯差異。無論在光學導航下或電磁導航下,各軸向的導航誤差皆顯示左右軸 向的誤差顯著小於前後軸向誤差及頭尾軸向誤差。除此之外,比較光學導航與 電磁導航,同一個解剖定位點測得之兩組導航誤差,相較之下皆無顯著差異。
總結來說,電磁導航系統的設備設置,和使用表面註冊法來進行光學及電
磁導航,經研究顯示均為高效、便利且易於操作的。在臨床應用上,兩種導航
系統的準確度差距不多,且誤差皆在可容許範圍內。除此之外,相較於前後軸
向及頭尾軸向,左右軸向可測得最佳的準確度,光學導航如此,電磁導航亦同。
doi:10.6342/NTU201701967
III
關鍵詞:表面註冊;光學導航系統;電磁導航系統;內視鏡鼻竇手術;電腦輔
助手術;導航誤差;導航準確度
Abstract
Introduction
Functional endoscopic sinus surgery has gained wide application in the management of sinus disease since the 1980s. The use of computer-aided surgery (CAS) technology was developed to assist surgeons in identifying anatomic landmarks during sinus surgery since the 1990s. In CAS, a correlation between a stored preoperative image data set and specific landmarks in the surgical area is required. However, studies on the performance of surface registration and
comparisons between optic and electromagnetic navigation systems were lacking.
Hence, the purpose of our study is to investigate time efficiency of system preparation and operation as well as the precision of optic and electromagnetic navigation systems using the surface registration in live endoscopic sinus surgery.
Forty patients with bilateral chronic paranasal pansinusitis underwent
endoscopic sinus surgery. The surgeries were performed under electromagnetic
navigation guidance after the surface registration had been carried out on all of the
patients. The intraoperative measurements indicate the time taken for equipment
set-up, surface registration and surgical procedure, as well as the degree of
navigation error along the 3 axes. The result revealed that the deviation in the
medial-lateral direction was significantly less than that in the anterior-posterior and
cranial-caudal directions. In the second part of our study, thirty patients with bilateral
chronic paranasal pansinusitis underwent surgery on one side using optic navigation
guidance and on the other side using electromagnetic navigation guidance. The
doi:10.6342/NTU201701967
V
intraoperative measurements performed included the time taken for the surface registration and surgical procedure on each side, as well as the navigation errors at the different locations. The result showed that the time for surface registration was significantly longer in the optic navigation group than the electromagnetic group.
However, the time for surgical procedure has no significant difference between these 2 groups. A comparison of the navigation errors along the 3 axes showed that the deviation in the medial-lateral direction was significantly less than that in the
anterior-posterior and cranial-caudal directions in the optic navigation group as well as the electromagnetic group. Furthermore, in comparison to the navigation error in each specific location, there was no significant difference between the optical and electromagnetic navigation groups.
In conclusion, the procedures of equipment set-up in electromagnetic navigation system, surface registration in both optic and electromagnetic navigation tracking are efficient, convenient and easy to manipulate. The accuracy of both navigation
systems is comparable and within acceptable ranges for clinical use. In addition, the
best accuracy was measured in the medial-lateral direction compared with the other
two axes, either in optic or electromagnetic navigation system.
Key words: Surface registration; optic navigation system; electromagnetic navigation system; endoscopic sinus surgery; computer-aided surgery; navigation error;
navigation accuracy
doi:10.6342/NTU201701967
VII
縮寫對照表
AER/AE Anterior ethmoid roof AP Anterior-posterior
CAS Computer-aided surgery CC Cranial-caudal
CT Computed tomography ESS Endoscopic sinus surgery LP Lamina papyracea
ML Medial-lateral
MRI Magnetic Resonance Imaging NE Navigation error
NP Nasopharynx
OS Opening of the sphenoid sinus PER/PE Posterior ethmoid roof
ST Superior turbinate
UC Upper border of choana
目 錄
誌謝……….. I 中文摘要………...………. .II 英文摘要………...……….……….... IV 縮寫對照表……….…….….VII
Chapter 1 Introduction………..…1
Chapter 2 Materials and Methods……….…6
2.1 The performance of electromagnetic navigation system using surface registration………6
2.1.1 Patients……….6
2.1.2 Equipment set-up………..6
2.1.3 Surface registration……….8
2.1.4 Navigation error………..…8
2.2 The comparisons of optic and electromagnetic navigation system using surface registration………...12
2.2.1 Patients………...12
2.2.2 Equipment set-up………12
2.2.3 Surface registration………....13
2.2.4 Navigation error………...13
2.3 Statistical methods……….………...17
2.4 Ethical consideration…………..……….18
Chapter 3 Results……..………..19
3.1 The performance of electromagnetic navigation system using surface
registration………..19
doi:10.6342/NTU201701967
3.2 The comparisons of optic and electromagnetic navigation system using
surface registration………..21
Chapter 4 Discussion………..………25
Chapter 5 Conclusions………32
References……….………..………33
Appendix……….38
圖 目 錄
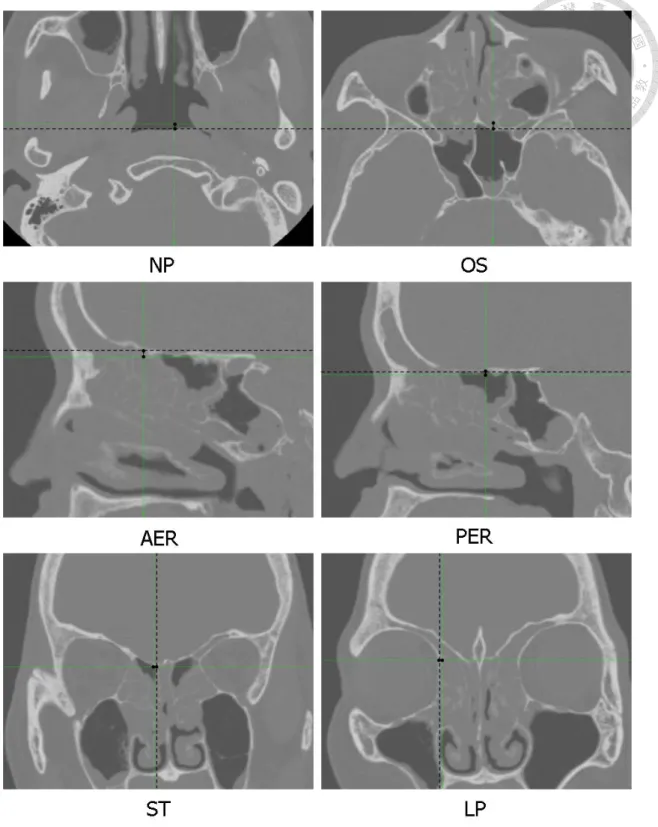
Figure 1 The set-up of the electromagnetic navigation system in endoscopic sinus surgery.………....7 Figure 2 The measurements of the navigation errors at the nasopharynx (NP), the
opening of the sphenoid sinus (OS), the central points of the anterior and posterior ethmoidal roofs (AER, PER, respectively), the insertion point of the superior turbinate (ST) and the most medial point of the lamina
papyracea (LP). Dotted lines indicate imaginary lines passing the
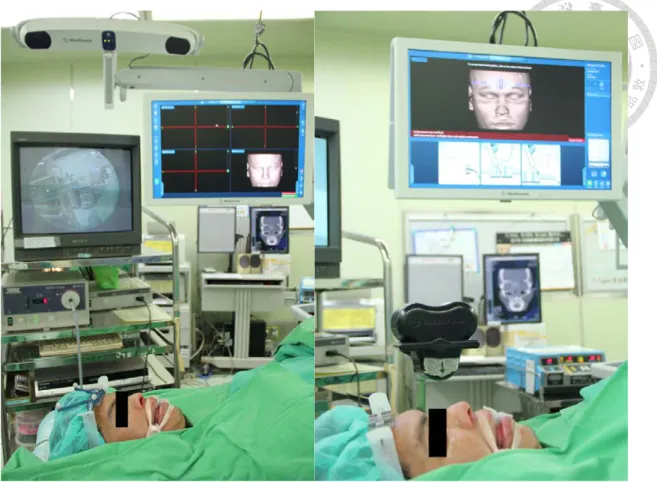
predetermined CT landmarks and perpendicular to the measuring axes..…10 Figure 3 The set-up of (a) the optic navigation system (b) the electromagnetic
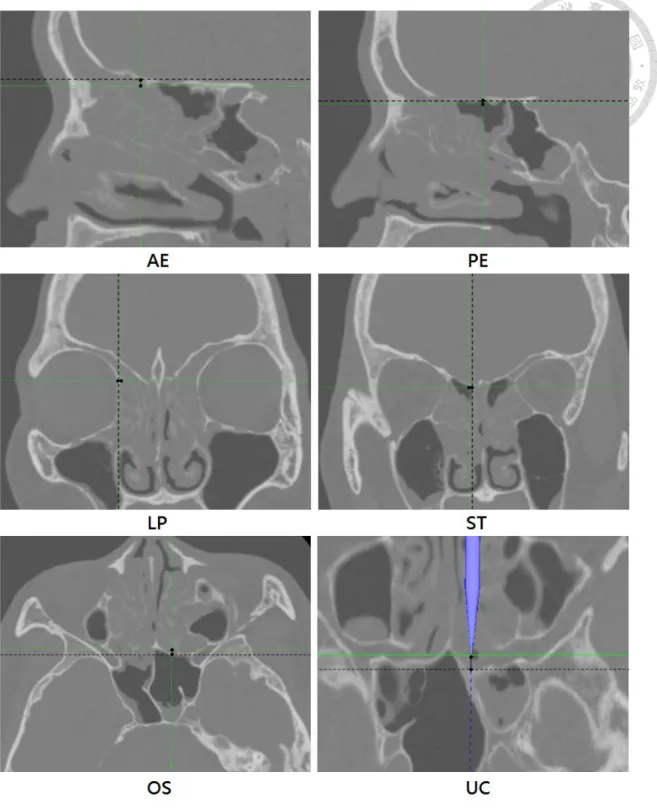
navigation system in endoscopic sinus surgery…..………..…14 Figure 4 The measurements of the navigation errors at the central points of the
anterior and posterior ethmoid roofs (AE, PE, respectively), the most medial point of the lamina papyracea (LP), the insertion point of the superior
turbinate (ST), the opening of the sphenoid sinus (OS) and the upper border of choana (UC). Dotted lines indicate imaginary lines passing the
predetermined CT landmarks and perpendicular to the measuring
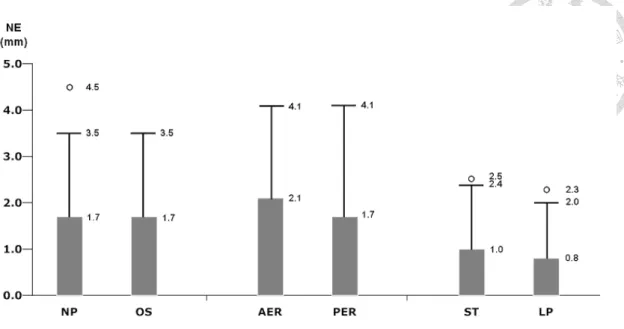
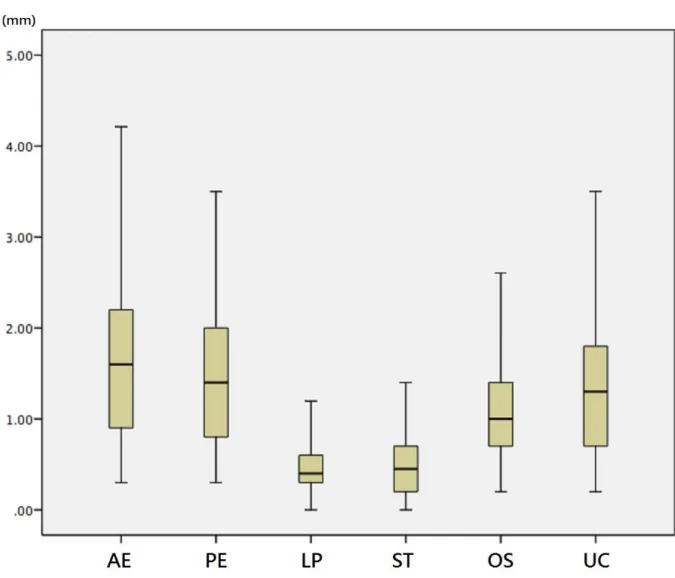
axes.………...………..………..16 Figure 5 The navigation error (NE) in the 6 location groups. The NE in ST and LP
groups (medial-lateral axis) was significantly less than that in the other 4 location groups (cranial-caudal and anterior-posterior axes). Open circles and bars represent the maximum values and upper limits of 95% confidence intervals calculated by mean and standard deviation, respectively. Top edges of the boxes indicate mean values………...…20 Figure 6 The navigation error (NE) of the optic navigation system in the 6 location
groups. The NE in LP and ST groups (medial-lateral axis) was significantly less than that in the other 4 location groups (cranial-caudal and
anterior-posterior axes). The bottom and top of the box are the first and third
doi:10.6342/NTU201701967
quartiles, and the band inside the box is the median. The ends of the
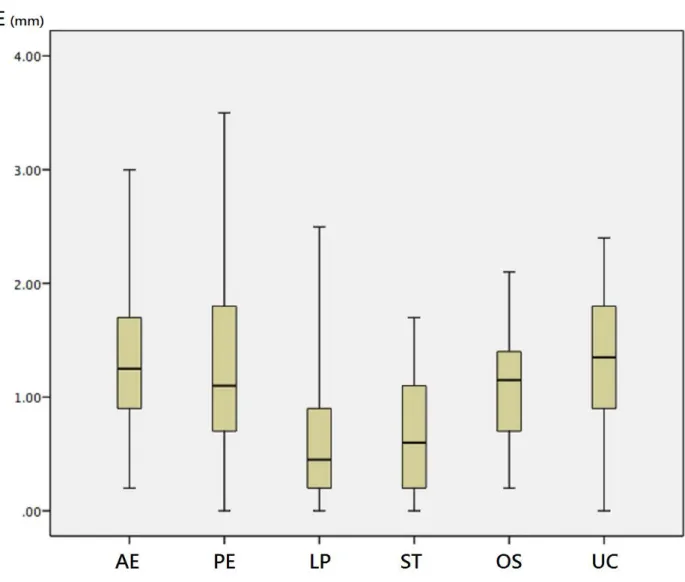
whiskers represent the minimum and maximum of all of the data……...…23 Figure 7 The navigation error (NE) of the electromagnetic navigation system in the 6
location groups. The NE in LP and ST groups (medial-lateral axis) was significantly less than that in the other 4 location groups (cranial-caudal and anterior-posterior axes). The bottom and top of the box are the first and third quartiles, and the band inside the box is the median. The ends of the
whiskers represent the minimum and maximum of all of the data.……..…24
Chapter 1. Introduction
Paranasal sinusitis is one of the most common diseases in otorhinolaryngology field. The symptoms include nasal discomforts, such as nasal obstruction, purulent rhinorrhea, post-nasal drip, hypernasal voice, foul odor in nose, hyposmia and anosmia, and non-nasal symptoms, such as headache, facial fullness sensation, sore throat, otalgia, teethache and chronic cough. It comprises a spectrum of medical conditions that are characterized by inflammation in paranasal sinuses. According to the disease duration, they are divided into acute (< 4 weeks), subacute (4 to 12 weeks) and chronic paranasal sinusitis (>12 weeks). In the acute stage of sinusitis, most patients recover after adequate medical treatment, such as administration of antibiotics, anti-inflammatory agents and mucolytic agents. However, if the symptoms of paranasal sinusitis persist more than 12 weeks, chronic inflammatory process leads to irreversible structural changes of paranasal sinuses, such as polyp formation, blockage of sinus ostium. With multiple potential inflammatory triggers acting through various physiologic pathways, it appears that chronic paranasal sinusitis may be a syndrome with multiple etiologies and a common endpoint for a variety of nose and sinus diseases. In this chronic stage of disease, surgical management instead of medical treatment becomes a mainstream of treatment modalities.
Endoscopic sinus surgery (ESS) for the treatment of sinus disease has been a common otolaryngological surgical procedure since the mid-1980s, with an expanding role in the management of orbital, facial bone and skull base diseases (1,2). Computer-aided surgery (CAS) technology has been developed to assist surgeons in achieving better anatomical localization since the 1990s (3,4), and may help prevent potential sinus complications such as orbital damage, cerebrospinal fluid leakage and carotid artery injury (5). Based on real-time image guidance in association with
doi:10.6342/NTU201701967
2
endoscopy, CAS systems may help to improve the intraoperative precision of orientation
(6,7) using either computed tomography (CT) or Magnetic Resonance Imaging (MRI) (8). Among the commercially available CAS systems, both optical and electromagnetic tracking systems have become popular, as they are more accurate and convenient than electromechanical (9) or sonic tracking systems (10). The optical tracking system was developed earlier than the electromagnetic system and was the first to be widely adopted in the clinical setting because of its high degree of accuracy (1). Numerous studies (4,11-16) have analyzed its performance under both clinical and laboratory conditions. Claes et al.
(11) conducted a cadaveric study for comparisons of navigation errors of conventional fiducial marker registration and anatomical landmark registration using an active optic navigation system (OptoTrak 3020®). The results showed matching with external fiducials on the face results in smaller navigation error than matching with anatomical landmarks. The accuracy was comparable and acceptable in the fiducial marker group (mean=2.13 ± 1.42 mm). Eliashar et al. (12) demonstrated accurate anatomical localization with less than 2 mm localization error. (1.1~2.0 mm, mean =1.6mm) in 94% (32/34) live sinus surgeries using an active optic navigation system (LandmarX®).
In 2 out of 34 surgeries, the localization errors were more than 2 mm (2.2 and 2.3 mm).
They were still considered as acceptable errors because there is general consensus that 3-mm navigation error is clinical acceptable and applicable (13). The same optic navigation system (LandmarX®) was used in Metson’s clinical study (14). The navigation errors of 754 sinonasal surgeries performed by 34 physicians were analyzed, and the mean accuracy of anatomical localization at the start of surgery was 1.69 ± 0.38 mm. Snyderman et al. (15) used a passive optic navigation system (Stryker®) in 50 endoscopic, anterior cranial base procedures, and the accuracy was evaluated after fiducial marker registration. The results revealed that the mean error of initial
registration was 2.8 mm (1.4~7.1 mm). Anon (4) used an active optic navigation system (OptoTrak 3020®) in 24 endoscopic sinus surgeries. Accuracy measurements were recorded after fiducial marker registration and the overall accuracy was 1.88 ± 1.04 mm.
Klimek et al. (16) recorded the accuracy of laboratory condition and that of live surgery using a passive optic navigation system. Laboratory accuracy measurements were obtained on a Plexiglas model with known coordinates of fiducial markers, before and after predefined table movement. Intraoperative accuracy measurements were recorded from 24 patients undergoing endoscopic sinus surgery with fiducial marker referencing technique. The result demonstrated laboratory accuracy to 0.86 ± 0.94 mm. After table movements, the accuracy decreased to 1.12 ± 0.99 mm, 1.05 ± 0.96 mm, 1.15 ± 1.04 mm and 1.54 ± 1.25 mm, respectively, in four different positions. Intraoperative accuracy was 1.14 ± 0.57 mm. Briefly, the accuracies of optic navigation systems under laboratory conditions, in cadaveric studies and live surgeries are good and acceptable, either using fiducial marker registration or using anatomical registration.
The development of electromagnetic tracking systems for surgical use was limited by ferromagnetic distortion that adversely affected system accuracy until certain hardware and software advances were recently reported (4,17-19). Using fiducial marker registration, Anon (4) reported the electromagnetic navigation (InstaTrak®) accuracy were within 0.96 ± 0.86 mm after localization measurement of 10 dry skull bases. Fried et al. (19) presented a multicenter clinical study (n=55) that evaluated the electromagnetic navigation (InstaTrak®) systems’s capability for localizing anatomical structure in critical surgical sites when performing endoscopic sinus surgery. The results showed mean accuracies in autoheadset registration group and fiducial registration group were 2.28 mm and 1.97mm, respectively. Although optic navigation systems were widely adopted before; currently, the electromagnetic systems are much more popular in North
doi:10.6342/NTU201701967
4
America due to advanced accuracy. There are only few studies concerning the navigation accuracy of newly-developed electromagnetic systems at present; therefore, one purpose of this study is to further analyze the performance of new electromagnetic navigation system (Medtronic S7®).
Navigation accuracy is highly dependent on the registration process, which establishes the correlation between specific landmarks and stored image data. Various registration methods have been proposed, based on external fiducial markers (20), anatomical landmarks (21) and contour-based registration (10,22), respectively. Anatomical landmark registration has been commonly used with an acceptable precision in a variety of practical situations, as it utilizes natural markers and is non-invasive (21). The surface registration procedure that aligns the unique facial contours eliminates the long preparation time of the usual registration technique and is thus clinically convenient
(23,24). Thus far, the accuracy of surface registration for optical tracking systems has been shown to be satisfactory in a variety of studies (22-25). Ledderose et al. (25) assessed the accuracy of surface laser registration using a passive optic navigation system (VectorVisionCompact®) on two cadaver heads. Repeated measurements were performed for 10 times and averaged. The resulting overall accuracy was 1.13 ± 0.53 mm, ranging from 0.77 to 1.76 mm, and thus proved to be clinically sufficient (13). Raabe et al. (22) evaluated the accuracy of another passive optic navigation system (Polaris®) using laser registration in live surgeries. The mean accuracy was 2.4 ± 1.7 mm. Stelter et al. (24) present their experience with a passive optic navigation system (VectorVisionCompact®) using laser registration for endoscopic sinus surgery on 368 patients. The clinical plausibility test produced an average deviation of 1.3 mm. Schlaier et al. (23) evaluate the registration accuracy and practicability of the passive optic navigation system (VectorVisionCompact®) with a laser registration technique in
comparison to marker registration. Thirty-five patients were registered by paired-point registration. In 16 patients, a second registration was carried out using a special laser pointer. The marker registration proved to be more accurate than the surface registration with regard to localization of anatomical landmarks and target fiducials (1.31 ± 0.87 mm vs. 2.77 ± 1.64 mm; p < .01). Nevertheless, the data for electromagnetic systems using surface registration is lacking for both live surgery and cases of cadaveric dissection. Accordingly, the precision of the surface registration used in electromagnetic tracking systems needs to be further evaluated. To our knowledge, this study presents the first investigation of the efficiency of system preparation and the three-dimensional accuracy of the surface registration used in electromagnetic tracking systems in live endoscopic sinus surgery.
In addition, comparisons of optic and electromagnetic systems using fiducial marker-matching registration or anatomical landmark registration were conducted in previous studies (1,26). Optic navigation systems were proved to be more accurate than electromagnetic navigation systems under laboratory condition (1) and in cadaveric study (mean error = 0.12 vs. 0.37mm, p < .05) (26). How about the performance of these two navigation systems using newly-developed surface registration technique? Is the optic navigation system still more accurate than the newly-developed electromagnetic navigation system under clinical condition? So far, comparisons between optic and electromagnetic systems using surface registration have not been reported, either in live surgery or cadaveric dissection. In the second part of our study, we investigate the anatomical precision of the two different navigation systems using surface registration in the course of live endoscopic sinus surgery on the same patients, and to share our experience with their use in clinical practice.
doi:10.6342/NTU201701967
6
Chapter 2. Materials and Methods
2.1 The performance of electromagnetic navigation system using surface registration
2.1.1Patients
Forty patients (20 men and 20 women) with chronic paranasal pansinusitis were enrolled in this study. The severity of disease was classified according to the
Lund-Mackay endoscopic grade and CT scan classification systems of chronic
rhinosinusitis. All patients were scored as Grade III-IV nasal polyposis according to the endoscopic grade system proposed by Meltzer et al. (27). The total score was more than 15 in the Lund-Mackay CT scan classification system. We excluded patients younger than 18 years, patients with concomitant external sinus surgery, unusual soft tissue sensitivity or damaged tissue at the intended mounting area. We also excluded those with any circulatory disease of the skin that might make it prone to damage by pressure from the silicone contact pad of the head frame used as the navigation reference. Prior to surgery, physicians performed CT scans of the sinus area to obtain images at a 0.75 mm slice thickness. The image data were then transferred to the navigation unit using a compact disc. The same medical team performed bilateral ESS using the Medtronic S7 navigation system (Medtronic Navigation, Minneapolis, MN, USA) on all patients. The intraoperative measurements in this study indicate the time taken for equipment set-up, surface registration, and surgical procedure, as well as the navigation errors (NEs) along the 3 axes.
2.1.2 Equipment set-up
After the induction of general anesthesia, a head frame was attached to the patient’s forehead using an elastic strap. The head frame was equipped with a headset patient tracker to provide a continuous point of reference for the navigation system (Figure 1).
Figure 1. The set-up of the electromagnetic navigation system in endoscopic sinus surgery.
doi:10.6342/NTU201701967
8
The head frame was placed at the center of the forehead (20-50 mm above the supraorbital foramen nerve), and was manipulated gently to ensure that it was attached securely and that its position relative to the head would be maintained throughout the course of the surgical procedure. A low-energy electromagnetic field emitter was fixed on a holder and attached to the operating table bed frame. The emitter holder was positioned at least 20 cm above the operating table and pointed directly at the patient’s nose from a distance of 20 cm. No part of the holder was extended into the emitter’s electromagnetic field. All of the instrument tracker cables for intraoperative navigation were connected to the navigation unit ports. The time for equipment set-up was recorded for all of the steps.
2.1.3 Surface registration
Synergy Cranial Software (Medtronic, Minneapolis, MN, USA) was employed for both registration and measurement. Surface registration method was used in this study.
The points that were used for the surface scanning were distributed at various locations along the nose, forehead and orbital rim. After collecting a sufficient number of points on the scanned area for computer calculation, the three-dimensional location information was automatically matched with the CT image. After completing the registration procedure, the correlation between the position of the instrument in the surgical field and the corresponding location on the CT images was established to allow real-time orientation during surgery. No additional registration processes were needed during the operation to adjust for anatomical drift. The time taken for surface registration was recorded.
2.1.4 Navigation error
During the operation, the patient’s head as well as the operating table may sometimes be moved or tilted, and bulb press testing was performed to check the
integrity of the lamina papyracea. However, the reference position of the head-tracking system on the forehead must remain unchanged in order to ensure an accurate navigational reading. We cleared the abnormal sinonasal tissue on both sides to achieve adequate exposure of the skull base, lamina papyracea and sphenoid sinus. A navigational probe was then used to determine the NE. The probe was used to touch a predetermined landmark in the patient. The NE was measured as the vertical distance from the navigated tip of the probe (i.e. the crosshairs) to an imaginary line passing the predetermined CT landmark and perpendicular to the measuring axis (Figure 2)
(11,25,28-29). The NE in the anterior-posterior (AP) direction was measured on the axial plane of the CT scan relative to the nasopharynx (NP) and opening of the sphenoid sinus (OS) reference points, whereas the NE in the cranial-caudal (CC) direction was measured on the sagittal plane using the central points of the anterior and posterior ethmoid roofs (AER, PER, respectively). The NE in the medial-lateral (ML) direction was measured on the coronal plane with the insertion point of the superior turbinate (ST) and the most medial point of the lamina papyracea (LP). The reason why predetermined landmarks were chosen is because these landmarks are easy to be identified on the specific planes of the CT images. For example, the referred points of AE and PE are easier to be located on the sagittal plane than the coronal or the axial plane. However, even when we measure the navigation error being zero in one axis, it only means that the navigated point is equal to the predetermined virtual point in that axis, but the error may still exist in other axes. For all patients, the measurements of the distance were performed 3 times without repeating the registration process. The mean of these values was considered the NE for specific locations. All the NE results were expressed as absolute values, and those on both sides were averaged for the purposes of statistical analysis.
doi:10.6342/NTU201701967
10
Figure 2. The measurements of the navigation errors at the nasopharynx (NP), the opening of the sphenoid sinus (OS), the central points of the anterior and posterior ethmoidal roofs (AER, PER, respectively), the insertion point of the superior turbinate (ST) and the most medial point of the lamina papyracea (LP). Dotted lines indicate
imaginary lines passing the predetermined CT landmarks and perpendicular to the measuring axes.
doi:10.6342/NTU201701967
12
2.2 The comparisons of optic and electromagnetic navigation system using surface registration
2.2.1 Patients
Thirty patients (24 men and 6 women) with chronic paranasal pansinusitis were enrolled in this study. The severity of the disease was classified according to the
Lund-Mackay CT scan classification systems of chronic rhinosinusitis. All patients were scored as Grade III-IV nasal polyposis according to the endoscopic grade system
proposed by Meltzer et al. (27). The total score for each case was greater than 15 in the Lund-Mackay CT scan classification system. Exclusion criteria were the same as section 2.1. Preoperative sinus CT was done and the image data were then transferred to the navigation unit using a compact disc. The same medical team performed bilateral endoscopic sinus surgery using the Medtronic S7 navigation system on all patients. The S7 system has both optic and electromagnetic tracking devices in one machine to facilitate the operation. We used the optic navigation system when performing one side endoscopic sinus surgery and the electromagnetic navigation system to assist the other side endoscopic sinus surgery in a random allocation through the use of a random number table. The test statistics measured intraoperatively in this study indicate the times taken for surface registration and the surgical procedure, as well as the navigation errors (NEs) along the 3 axes.
2.2.2 Equipment set-up
After the induction of general anesthesia, a head reference frame was attached to the patient’s forehead using an elastic strap. The head frame was equipped with a headset patient tracker to provide a continuous point of reference for the navigation system. The head frame was placed at the center of the forehead and manipulated gently to ensure that it was attached securely, and that its position relative to the head would be
maintained during the registration process and subsequent procedure.
The localizer (i.e. the optic system camera or the electromagnetic field emitter) was set up before the surgery on each side. For optical tracking, the system camera
triangulates the spatial coordinates of the optical markers on the tracked devices. The position the camera head is approximately 1.75 m from the patient reference, and the camera must have a clear line of sight to the optical markers (Figure 3). For
electromagnetic tracking, a low-energy electromagnetic field emitter was fixed on a holder and attached to the operating table bed frame. The emitter holder was positioned at least 20 cm above the operating table and pointed directly at the patient’s nose from a distance of 20 cm. No part of the holder was extended into the emitter’s electromagnetic field (Figure 3). All of the instrument tracker cables for intraoperative electromagnetic navigation were connected to the navigation unit ports.
2.2.3 Surface registration
A surface registration technique was used in both the optic and electromagnetic systems. Synergy Cranial Software was employed for the registration and measurement in both systems. The points that were used for the surface matching computer algorithm were distributed along various locations at the nose, forehead and orbital rim. After collecting a sufficient number of points on the scanned area for computer calculation, the three-dimensional location information was automatically matched with the CT image. After completing the registration procedure, the correlation between the position of the instrument in the surgical field and the corresponding location on the CT images was established to allow real-time orientation during surgery. No additional registration processes were needed during the operation to adjust for anatomical drift. The time required for surface registration in both systems was recorded.
2.2.4 Navigation error
doi:10.6342/NTU201701967
14
(a) (b)
Figure 3. The set-up of (a) the optic navigation system (b) the electromagnetic navigation system in endoscopic sinus surgery.
During the operation, a best effort was made to avoid moving or tilting the
patient’s head or the operating table. The bulb press testing was sometimes performed to check the integrity of the lamina papyracea. However, the head reference frame must remain attached and stable until navigation is complete to ensure an accurate
navigational reading. We cleared the abnormal sinonasal tissue on both sides to achieve adequate exposure of the skull base, lamina papyracea and sphenoid sinus. A
navigational probe was then used to determine the NE. The probe was used to touch a predetermined anatomic landmark in the patient. The NE was measured as the vertical distance from the navigated tip of the probe to an imaginary plane passing the
predetermined CT landmark and perpendicular to the measuring axis (Figure 4). The NE in the cranial-caudal (CC) direction was measured on the sagittal plane using the central points of the anterior and posterior ethmoid roofs (AE, PE, respectively) as the
predetermined CT landmarks, whereas the NE in the medial-lateral (ML) direction was measured on the coronal plane with the most medial point of the lamina papyracea (LP) and the insertion point of the superior turbinate (ST) as the CT landmarks. The NE in the anterior-posterior (AP) direction was measured on the axial plane of the CT scan relative to the opening of the sphenoid sinus (OS) reference points and the upper border of choana (UC). For all patients, the distance measurements were performed 3 times without repeating the registration process. The mean of these values was considered the NE for specific locations. All the NE results were expressed as absolute values for the purpose of statistical analysis.
doi:10.6342/NTU201701967
16
Figure 4. The measurements of the navigation errors at the central points of the anterior and posterior ethmoid roofs (AE, PE, respectively), the most medial point of the lamina papyracea (LP), the insertion point of the superior turbinate (ST), the opening of the sphenoid sinus (OS) and the upper border of choana (UC). Dotted lines indicate imaginary lines passing the predetermined CT landmarks and perpendicular to the measuring axes.
2.3 Statistical methods
The time of equipment set-up, surface registration, surgical procedure, as well as the NE in the AP, CC and ML directions, are expressed as mean values ± standard deviations. One-way ANOVA followed by the Bonferroni test was employed for multiple comparison tests. In part II study, the times used for the registration and surgery, as well as NEs in the specific anatomic locations of optic and electromagnetic navigation groups were compared by independent t-test. In addition, one-way ANOVA followed by the Bonferroni test was employed for multiple comparisons of NEs among the 6 anatomic locations in the optic or electromagnetic navigation system. The level of significance was set at p <.05. The statistical package SPSS 16.0 for Windows was used for all statistical analyses.
doi:10.6342/NTU201701967
18
2.4 Ethical considerations
The institutional review board of Far Eastern Memorial Hospital approved this study, and written informed consent was obtained from all of the patients.
Chapter 3. Results
3.1 The performance of electromagnetic navigation system using surface registration
Forty patients aged between 24 and 75 years (mean 51.3 years) underwent bilateral endoscopic sinus surgery. The surgery was primary for 34 patients (85 %) and a
revisionary procedure for 6 (15 %). The mean score on the Lund-Mackay CT scan classification system for all of the patients was 19.5 points. The time for the equipment set-up, surface registration and surgical procedure ranged between 141 and 212 s (mean
± standard deviation: 179 ± 23), 30 and 50 s (39 ± 4.8), and 60 and 190 min (114 ± 36), respectively. In other words, the equipment set-up and surface registration, respectively, took 2.6 % and 0.6 % of the entire procedure time. There were no cases of operative complications. The NE of the NP, OS, AER, PER, ST and LP was 1.7 ± 0.9, 1.7 ± 0.9, 2.1 ± 1.0, 1.7 ± 1.2, 1.0 ± 0.7 and 0.8 ± 0.6 mm, respectively, with a significant
difference for these 6 groups (p < .05, one-way ANOVA test, Figure 5). In comparison to the NE for the 6 location groups, the distance deviation in the ST and LP groups was significantly less than that in the other groups (p < .05, Bonferroni test, Figure 5). No significant differences were observed in any paired comparison between the NP, OS, AER and PER groups (p > .05, Bonferroni test, Figure 5). Furthermore, there was also no significant difference between the NE in the ST and LP groups (p > .05, Bonferroni test, Figure 5).
doi:10.6342/NTU201701967
20
Figure 5. The navigation error (NE) in the 6 location groups. The NE in ST and LP groups (medial-lateral axis) was significantly less than that in the other 4 location groups (cranial-caudal and anterior-posterior axes). Open circles and bars represent the maximum values and upper limits of 95% confidence intervals calculated by mean and standard deviation, respectively. Top edges of the boxes indicate mean values.
3.2 The comparisons of optic and electromagnetic navigation system using surface registration
Thirty patients aged between 20 and 62 years (mean 42 years) underwent bilateral endoscopic sinus surgery. The mean score on the Lund-Mackay CT scan classification system for all of the patients were 19 points. As regards to the severity of disease in both groups, there was no significant difference of unilateral Lund Mackey score between these 2 groups (9.7 ± 1.5 in the optic group vs. 9.3 ± 1.5 in the electromagnetic group).
The times required for surface registration and surgical procedure are 58.9 ± 4.2 seconds and 62 ± 11.5 minutes in the optic navigation group, and 33.2 ± 2.4 seconds and 56.7±
11.1 minutes in the electromagnetic group, respectively. The time for surgical procedure has no significant difference between these 2 groups; however, the time for surface registration was significantly longer in the optic navigation group than electromagnetic group (p < .05, independent t-test). There were no cases of operative complications. In the optic navigation group, the NEs of AE, PE, LP, ST, OS and UC were 1.7 ± 1.0, 1.5
± 0.9, 0.6 ± 0.4, 0.6 ± 0.5, 1.2 ± 0.7 and 1.4 ± 0.8 mm, respectively, with a significant difference among these 6 groups (Figure 6) (p < .05, one-way ANOVA test). In the electromagnetic navigation group, the NEs of AE, PE, LP, ST, OS and UC were 1.3 ± 0.7, 1.2 ± 0.8, 0.6 ± 0.6, 0.7 ± 0.5, 1.1 ± 0.6 and 1.4 ± 0.6 mm, respectively, with a significant difference among these 6 groups (Figure 7) (p < .05, one-way ANOVA test).
Among the 6 anatomic locations, the distance deviations in the ST and LP groups were significantly less than those in the other groups (p < .05, Bonferroni test) in both the optic (Figure 6) and electromagnetic (Figure 7) navigation setting. No significant differences were observed in any paired comparison between the NP, OS, AE and PE groups (p > .05, Bonferroni test). There was also no significant difference between the NE in the ST and LP groups (p > .05, Bonferroni test). Furthermore, in comparison to
doi:10.6342/NTU201701967
22
the NE in each specific location, there was no significant difference between the optical and electromagnetic navigation groups (p > .05, independent t-test).
Figure 6. The navigation error (NE) of the optic navigation system in the 6 location groups. The NE in LP and ST groups (medial-lateral axis) was significantly less than that in the other 4 location groups (cranial-caudal and anterior-posterior axes). The bottom and top of the box are the first and third quartiles, and the band inside the box is the median. The ends of the whiskers represent the minimum and maximum of all of the data.
doi:10.6342/NTU201701967
24
Figure 7. The navigation error (NE) of the electromagnetic navigation system in the 6 location groups. The NE in LP and ST groups (medial-lateral axis) was significantly less than that in the other 4 location groups (cranial-caudal and anterior-posterior axes). The bottom and top of the box are the first and third quartiles, and the band inside the box is the median. The ends of the whiskers represent the minimum and maximum of all of the data.
Chapter 4. Discussion
Over the past decade, image-guided surgical navigation has been welcomed as a technology in both primary and revision sinus surgery. The anatomic aid provided by navigation system is very important for the surgeon. It facilitates better intraoperative orientation and enables more thorough eradication of diseased tissue, especially in cases of extensive polyposis, revision surgery and neoplastic sinonasal disease. Due to the delicate neighboring structures in close proximity to the orbits, vessels and base of the skull, a variety of major surgical complications, including loss of vision, diplopia, injury to the internal carotid artery, cerebrospinal fluid leak and brain damage may occur when the surgeon is unaware of which anatomical areas are dangerous (5,30). The demand for safety can be particularly challenging in cases of anatomical complexity, mostly in patients with extensive sinus disease or requiring revision surgery. With the assist of this modern technology, surgeons may prevent accidental damage to vital structures in proximity to the surgical area by monitoring the real-time position of surgical
instruments, especially in cases in which there is anatomical complexity or intraoperative heavy bleeding (6,14,25,31).
The tracking modalities, registration methods and navigation locations all influence system accuracy. Hence, exact knowledge about the navigation systems under specific conditions is required for a confident use of CAS. Two main types of navigation modalities are in general use in current clinical practice. First modality, optical
navigation systems use active light-emitting diodes or passive reflecting spheres that are mounted on the navigational instruments and the reference headset to detect the
movement of the instruments by triangulation of an infrared camera system. Many studies have shown that optical navigation systems possess a high degree of accuracy for clinical use (11,18,23,26). However, a major drawback of the optic navigation system is that
doi:10.6342/NTU201701967
26
no obstacle can be allowed between the infrared camera system and the navigational instruments (23). Restated, continuous navigation may frequently be disturbed due to a blockage of the direct line of sight. Second modality, electromagnetic navigation systems do not need to keep the direct line of sight between all components because a different tracking technique is employed. While moving, the coil arrays embedded in the trackers can sense the change in the electromagnetic field that is constructed by an emitter. As a result, an electromagnetic tracking system can offer continuous
localization information on the monitor without interruption throughout the operation and is superior to an optic tracking system in a cluttered operating field (27,32). Currently, optical tracking systems are popular because of their availability and relative accuracy
(16,33). Numerous studies have shown that these systems achieve superior spatial
resolution and accuracy compared to electromagnetic tracking systems (1,26,34). However, electromagnetic tracking systems have improved the accuracy by means of advances in technology and have become more popular in clinical use (17). Nowadays, optical and electromagnetic tracking systems have both come to be accepted as suitable for CAS
(1,16,19).
Using the same electromagnetic navigation system (Medtronic S7®) as our study, Kral et al. (26) reported that the mean NE of electromagnetic tracking systems in human cadavers was 0.37 mm, which was more precise than the results in our study (0.8 - 2.1 mm). This may be explained by the use of externally fixed fiducial markers for
paired-point matching registration and immediate measurement following registration in Kral’s study. Furthermore, unlike cadavers, intraoperative stretching of the skin/soft tissue may occur easily and result in a displaced reference frame, which appears to have been the case in our study (16). The fixation of an endotracheal tube on the patient’s face with adhesive tape may also have contributed to the distortion of the facial contours and
caused surface registration discordance in the preoperative CT images. All of these factors influence the navigational accuracy during surgery. In this study, we measured the NE during the course of surgical procedures on patients diagnosed with severe sinus diseases. In contrast to the optimized conditions of laboratory settings, in clinical practice, the conditions tend to reduce system accuracy, especially when long periods have elapsed since surface registration. It may be appropriate to repeat surface
registration in consideration of intraoperative anatomical drift to overcome the increased NE in longer operations (7,32). However, we performed surface registration just once, at the beginning of surgery, and defined the NE value intraoperatively to evaluate whether it remained acceptable at the time the ESS was completed.
Although surface registration has been shown to be less accurate than the other registration methods in cadaveric heads, the errors are still within that which is typically deemed the acceptable ranges for navigation (25,35). To our knowledge, this is the first study to measure the NE of the surface registration obtained with an electromagnetic system in live surgery. The results show that the NEs in the 6 location groups have a maximal mean value of 2.1 mm; such variation may be important to surgeons if they, for example, want to assess the anatomical position in relation to the optic nerve or carotid artery. Although there is general agreement that the navigation system may be used for clinical purposes when the error is less than 3 mm (13,36), the acceptable range of the error may still depend on the location at which the operation is being carried out.
Regarding the additional time (mean 218 s) for equipment set-up and surface registration, only a small proportion (3.2%) of the total operation time was spent on system preparation. That is, the extra procedures of preparation for navigation surgery are not time-consuming.
Furthermore, our results show that the NE in the ML direction had a significantly
doi:10.6342/NTU201701967
28
higher accuracy than measurements in the AP and CC directions. A possible explanation is that the more dispersed registration points resulted in a more accurate anatomic localization. Because the extent of the divergence in tracing the paths is greater in the ML direction than in the AP and CC directions, the NE data consequently show the reading to be more precise on the ML axis. In addition, there is the possibility that depressed skin/soft tissue during the course of surface registration may shift the surface registration points and subsequently result in erroneous positional information, especially in the AP direction. Most importantly, before CAS may be used with confidence in sinus surgery, the surgeon has to keep in mind that the NEs in any of the axes may affect his or her judgment. As the dissection approaches an important anatomical structure, the users should be aware that the navigational instrument may have touched the critical site, in which case its location may not be correctly displayed on the monitor. Because the navigational accuracy is less reliable in the AP and CC directions than in the ML direction, dissections near the skull base are of greater risk than those closer to the lamina papyracea. In addition, sinus surgeons in training tend to have an excessive level of trust in the navigation system (37); such an excessive reliance on the navigation system can lead to a neglect of personal anatomical knowledge on the part of the surgeon and result in needless surgical complications. Although substantial but acceptable NE levels were confirmed in this study, it emphasized that CAS is only a useful adjunct to surgical experience and anatomical knowledge when it is applied properly (37).
In the second part of our study, the comparisons of the optic and electromagnetic navigation systems were conducted. In order to eliminate the need for the time-consuming application of the landmark and fiducial marker matching registration, a surface contour-based registration technique was proposed many years ago (22,23,25).
Although surface registration was shown to be less accurate as compared to the other registration methods (22,23,35), the NEs using the former registration for both the optic and electromagnetic navigation systems are still within the range that are typically deemed sufficient for clinical purposes (13,35,36). Because of small amount of registration time relative to the entire operation time (1.58% in the optically navigated surgery and 0.98%
in the electromagnetically navigated surgery), surface registration offers a great deal of practical convenience in navigation preparation. Although surface registration costs significantly less time in the electromagnetic navigation group than the optic one, the entire surgical times in both groups were similar.
To the best of our knowledge, this is the first report to measure NEs using both optic and electromagnetic navigation systems on the same patient in live surgery. The results show that the NEs in the 6 measured areas have maximal mean values of 1.7 mm in the optic navigation group and 1.4 mm in the electromagnetic navigation group. This finding can be taken as acceptable accuracy for clinical practice. Using the same navigation system as ours, Kral et al. (26) reported both the optic and electromagnetic navigation systems have excellent sub-millimetric accuracy in the case of anatomical specimens from an experimental setup. However, the optical tracking was reported to be significantly more precise than the electromagnetic tracking. In contrast, the NEs measured in our study demonstrated that the accuracy of electromagnetic tracking is comparable to that of optic tracking for live navigated endoscopic procedures. This may be because recent hardware and software advances in the electromagnetic navigation system have improved the system accuracy, which was initially highly influenced by ferromagnetic distortion (17,18). Furthermore, the advantage of the admirable accuracy of the optic tracking system when used under optimized laboratory conditions is somewhat offset in the course of live surgery, leading to a certain loss of precision. The surface
doi:10.6342/NTU201701967
30
registration method in this study also played a role in a decrease in accuracy, because either a displacement of the reference frame or distortion of the facial contour caused by intraoperative stretching of the skin/soft tissue may result in a discordance between the facial contour and the preoperative image (22,23,25). Consequently, our comparative study of these two systems used in the same patients provides objective evidence that both systems are similar in terms of accuracy, no matter which location of the NEs was measured. Together with previous reports in the existing literature (1,6,22-26,32), our results and experience provide a referential basis that should prove to be informative for a surgeon or institution in the selection of a navigation system.
Furthermore, in terms of both optic navigation and electromagnetic navigation, our results show that the NEs in the ML direction had a significantly higher precision than NEs in the CC and AP directions. The reason for the difference lies mostly in the fact that a more precise correlation between the pre-operative image and intra-operative anatomy depends on the collection of more widely dispersed registration points, regardless of the modality of the navigation system. Because the extent of the
divergence in tracing the points of the facial contour is greater for the ML axis than the CC and AP axes, it is more precise when analyzing the navigational accuracy in the ML direction. In addition, a shift of the patient’s skin/soft tissue, mostly in the AP direction, or changes in the tension in the muscles of expression during the course of surface registration may also play a role in an invalid data set correlation for CAS, especially in the AP direction. Since the measurement has even less precision on the CC and AP axes, the surgeon has to keep in mind that dissection near the skull base presents greater risks than when performed closer to the lamina papyracea. A thorough knowledge of the complex anatomy and surgical techniques, instead of just relying on the navigation system, remains essential for performing safe endoscopic sinus surgery (12,37), even
though this study has confirmed that the NEs in both systems are quite acceptable in terms of providing assistance during the surgery.
doi:10.6342/NTU201701967
32
Chapter 5. Conclusions
Electromagnetic navigation systems using surface registration are a suitable adjuvant tool for ESS. It takes less than 4 minutes to complete the equipment set-up and surface registration, and it offers invaluable real-time information on location with sufficient accuracy. In the three-dimensional analysis of surface registration accuracy, the deviations in the ML direction are significantly less than those for the other two axes.
Regarding comparisons of the optic and electromagnetic navigation systems, the electromagnetic navigation system takes significantly less time to complete the surface registration than the optic navigation system. The time for registration in both systems only accounts for less than 2% of the time taken for the surgery on one side.
Furthermore, the accuracy of the two navigation systems is acceptable and comparable in clinical use. In other words, the electromagnetic navigation system is as accurate as the optic navigation system using the surface registration technique under clinical condition. However, we recommend using the electromagnetic navigation in CAS because of the advantage provided by continuous tracking without interruption, especially in cluttered operation theatres. In the three-dimensional analysis of the two-system accuracy, the best accuracy was also measured in the ML direction compared with the other two axes, either in optic or electromagnetic navigation tracking.
This finding suggests that surgeons should be more cautious when dissecting in the AP or CC direction during the course of navigation for sinus surgery.
References
1. Ecke U, Luebben B, Maurer J, Boor S, Mann WJ. Comparison of Different Computer-Aided Surgery Systems in Skull Base Surgery. Skull Base. 2003; 13:
43-50.
2. Kennedy DW, Zinreich SJ, Rosenbaum AE, Johns ME. Functional endoscopic sinus surgery. Theory and diagnostic evaluation. Arch Otolaryngol. 1985; 111:
576-582.
3. Schloendorff G, Moesges R, Meyer-Ebrecht D, Krybus W, Adams L. CAS (computer assisted surgery). A new procedure in head and neck surgery. HNO.
1989; 37: 187-190.
4. Anon JB. Computer-aided endoscopic sinus surgery. Laryngoscope. 1998; 108:
949-961.
5. Mafee MF, Chow JM, Meyers R. Functional endoscopic sinus surgery: anatomy, CT screening, indications, and complications. AJR Am J Roentgenol. 1993; 160:
735-744.
6. Hepworth EJ, Bucknor M, Patel A, Vaughan WC. Nationwide survey on the use of image-guided functional endoscopic sinus surgery. Otolaryngol Head Neck Surg. 2006; 135: 68-73.
7. Al-Swiahb JN, Al Dousary SH. Computer-aided endoscopic sinus surgery: a retrospective comparative study. Ann Saudi Med 2010; 30: 149-152.
8. Fried MP, Topulos G, Hsu L, et al. Endoscopic sinus surgery with magnetic resonance imaging guidance: initial patient experience. Otolaryngol Head Neck Surg. 1998; 119: 374-380.
9. Mosges R1, Schlondorff G. A new imaging method for intraoperative therapy control in skull-base surgery. Neurosurg Rev. 1988; 11: 245-247.
doi:10.6342/NTU201701967
34
10. Reinhardt HF, Horstmann GA, Gratzl O. Microsurgical removal of deep vascular malformations using sonar-stereometry. Ultraschall Med. 1991; 12: 80-83.
11. Claes J, Koekelkoren E, Wuyts FL, Claes GM, Van den Hauwe L, Van de Heyning PH. Accuracy of computer navigation in ear, nose, throat surgery: the influence of matching strategy. Arch Otolaryngol Head Neck Surg. 2000; 126:
1462-1466.
12. Eliashar R, Sichel JY, Gross M, et al. Image guided navigation system-a new technology for complex endoscopic endonasal surgery. Postgrad Med J. 2003; 79:
686-690.
13. Metson RB. Image-guided sinus surgery: Lessons learnt from the first 1000 cases. Otolaryngol Head Neck Surg. 2003; 128: 8-13.
14. Metson RB, Cosenza MJ, Cunningham MJ, Randolph GW. Physician experience with an optical image guidance system for sinus surgery. Laryngoscope. 2000;
110: 972-976.
15. Snyderman C1, Zimmer LA, Kassam A. Sources of registration error with image guidance systems during endoscopic anterior cranial base surgery. Otolaryngol Head Neck Surg. 2004; 131: 145-149.
16. Klimek L, Ecke U, Lubben B, Witte J, Mann W. A passive-marker-based optical system for computer-aided surgery in otorhinolaryngology: development and first clinical experiences. Laryngoscope. 1999; 109: 1509-1515.
17. Hummel J, Figl M, Birkfellner W, et al. Evaluation of a new electromagnetic tracking system using a standardized assessment protocol. Phys Med Biol. 2006;
51: N205-210.
18. Yaniv Z, Wilson E, Lindisch D, Cleary K. Electromagnetic tracking in the clinical environment. Med Phys. 2009; 36: 876-892.
19. Fried MP, Kleefield J, Gopal H, Reardon E, Ho BT, Kuhn FA. Image-guided endoscopic surgery: results of accuracy and performance in a multicenter clinical study using an electromagnetic tracking system. Laryngoscope. 1997; 107:
594-601.
20. Maurer CR Jr, Fitzpatrick JM, Wang MY, Galloway RL Jr, Maciunas RJ, Allen GS. Registration of head volume images using implantable fiducial markers.
IEEE Trans Med Imaging. 1997; 16: 447-462.
21. Maurer CR Jr, Maciunas RJ, Fitzpatrick JM. Registration of head CT images to physical space using a weighted combination of points and surfaces. IEEE Trans Med Imaging. 1998; 17: 753-761.
22. Raabe A, Krishnan R, Wolff R, Hermann E, Zimmermann M, Seifert V. Laser surface scanning for patient registration in intracranial image-guided surgery.
Neurosurgery. 2002; 50: 797-803.
23. Schlaier J, Warnat J, Brawanski A. Registration accuracy and practicability of laser-directed surface matching. Comput Aided Surg 2002; 7: 284-290.
24. Stelter K, Andratschke M, Leunig A, Hagedorn H. Computer-assisted surgery of the paranasal sinuses: technical and clinical experience with 368 patients, using the Vector Vision Compact system. J Laryngol Otol. 2006; 120: 1026-32.
25. Ledderose GJ, Stelter K, Leunig A, Hagedorn H. Surface laser registration in ENT-surgery: accuracy in the paranasal sinuses--a cadaveric study. Rhinology.
2007; 45: 281-285.
26. Kral F, Puschban EJ, Riechelmann H, Pedross F, Freysinger W. Optical and electromagnetic tracking for navigated surgery of the sinuses and frontal skull base. Rhinology 2011; 49: 364-368.
27. Meltzer EO, Hamilos DL, Hadley JA, et al. Rhinosinusitis: Developing guidance
doi:10.6342/NTU201701967
36
for clinical trials. Otolaryngol Head Neck Surg. 2006; 135: S31-80.
28. Fitzpatrick JM, West JB, Maurer CR Jr. Predicting error in rigid-body point-based registration. IEEE Trans Med Imaging. 1997; 17: 694-702.
29. Labadie RF, Davis BM, Fitzpatrick JM. Image-guided surgery: what is the accuracy? Curr Opin Otolaryngol Head Neck Surg. 2005; 13: 27-31.
30. May M, Levine HL, Mester SJ, Schaitkin B. Complications of endoscopic sinus surgery: analysis of 2108 patients--incidence and prevention. Laryngoscope.
1994; 104: 1080-1083.
31. Tschopp KP, Thomaser EG. Outcome of functional endonasal sinus surgery with and without CT-navigation. Rhinology. 2008; 46: 116-120.
32. Metson R, Gliklich RE, Cosenza M. A comparison of image guidance systems for sinus surgery. Laryngoscope. 1998; 108: 1164-1170.
33. Grevers G, Menauer F, Leunig A, Caversaccio M, Kastenbauer E. Navigation surgery in diseases of the paranasal sinuses. Laryngorhinootologie. 1999; 78:
41-46.
34. Schmerber S, Chassat F. Accuracy evaluation of a CAS system: laboratory protocol and results with 6D localizers, and clinical experiences in otorhinolaryngology. Comput Aided Surg. 2001; 6: 1-13.
35. Knott PD, Batra PS, Butler RS, Citardi MJ. Contour and paired-point registration in a model for image-guided surgery. Laryngoscope. 2006; 116:
1877-1881.
36. Roth M, Lanza DC, Zinreich J, Yousem D, Scanlan KA, Kennedy DW.
Advantages and disadvantages of three-dimensional computed tomography intraoperative localization for functional endoscopic sinus surgery.
Laryngoscope. 1995; 105: 1279-1286.
37. Stelter K, Ertl-Wagner B, Luz M, et al. Evaluation of an image-guided navigation system in the training of functional endoscopic sinus surgeons. A prospective, randomised clinical study. Rhinology. 2011; 49: 429-437.
doi:10.6342/NTU201701967
38
Appendix
Publication List of Chih-Ming Chang (SCI):
1. Chang CM, Young YH, Jaw FS, Wang CT, Cheng PW (2017). Degeneration of the vestibular nerve in unilateral Meniere’s disease evaluated by galvanic vestibular-evoked myogenic potentials. (In press)
2. Chang CM, Jaw FS, Lo WC, Fang KM, Cheng PW (2016). Three-dimensional analysis of the accuracy of optic and electromagnetic navigation systems using surface
registration in live endoscopic sinus surgery. Rhinology 54: 88-94.
3. Lo WC, Chang CM, Liao LJ, Wang CT, Young YH, Chang YL, Cheng PW (2015).
Assessment of d-methionine protecting cisplatin-induced otolith toxicity by
vestibular-evoked myogenic potential tests, ATPase activities and oxidative state in guinea pigs. Neurotoxicol Teratol 51: 12-20.
4. Sung PH, Chang CM, Young YH, Jaw FS, Cheng PW (2014). Optimal stimulation mode for obtaining galvanic ocular vestibular-evoked myogenic potentials. Clin Otolaryngol. 39: 240-245.
5. Chang CM, Young YH, Cheng PW (2013). Feasibility of simultaneous recording of cervical and ocular vestibular-evoked myogenic potentials via galvanic vestibular stimulation. Acta Otolaryngol. 133: 1278-1284.
6. Chang CM, Fang KM, Huang TW, Wang CT, Cheng PW (2013). Three-dimensional analysis of the surface registration accuracy of electromagnetic navigation systems in live endoscopic sinus surgery. Rhinology 51: 343-348.
7. Chang CM, Young YH, Cheng PW (2012). Age-related Changes in Ocular Vestibular-Evoked Myogenic Potentials via Galvanic Vestibular Stimulation and Bone-conducted Vibration Modes. Acta Otolaryngol 132: 1295-1300.
8. Chang CM, Cheng PW, Wang SJ, Young YH (2010). Effects of repetition rate of bone-conducted vibration on ocular and cervical vestibular-evoked myogenic potentials.
Clin Neurophysiol 121: 2121-2127.
9. Chang CM, Cheng PW, Young YH (2010). Aging effect on galvanic vestibular-evoked myogenic potentials. Otolaryngol Head Neck Surg 143: 418-421.