IntroductIons
Population aging is an important issue in many countries around the world. In the United States, for example, the percentage of people 65 years of age and older increased dramatically from 8.1% in 1950 to 12.4% in 2000, and is projected to reach 20.6% by 2050[1]. This growth in the elderly portion of the population
Physical functioning and health care costs in an older population
in Taiwan
Tzuo-Yun Lan1,*, Hsing-Yi CHang2, CHing-Yu CHen1
Objectives: Past research involving functional problems and medical utilization has been
limited to earlier surveys, local people, women, or use of Activities of Daily Living (ADLs) as the only measure of functional status, and is rarely investigated in non-US countries. We sought to re-examine the effect of functional status on health care utilization in the elderly, using a recent health survey conducted in Taiwan. Methods: 2,243 community-dwelling residents 60 years of age and older in the 2001 National Health Interview Survey (NHIS) in Taiwan were analyzed. Physical function was assessed using six ADLs questions and nine questions involving mobility tasks. The NHIS data were merged with the National Health Insurance claim data. Multiple linear regression was used to model the relationship between functional status and health care costs.
Results: A clear gradient relationship between functional status and expenses was observed,
with a small proportion of people with declining function responsible for a large proportion of the expenses. Functional status was independently associated with health care expenditures in the multiple regression model. Conclusions: Results from this more recent, non-US, nationwide research support the notion that functional status has an independent contribution to total health care expenditures in the elderly across countries. (Taiwan J Public Health. 2007;26(6):482-490)
Key Words: functional status, health care costs, elderly
1 Division of Gerontology Research, National Health Research Institutes, No. 35, Keyan Road, Zhunan, Maoli,
Taiwan, R.O.C.
2 Center for Health Policy Research and Development, National Health Research Institutes, Maoli, Taiwan, R.O.C. * Correspondence author. E-mail: tylan@nhri.org.tw
Received: Aug 9, 2007 Accepted: Nov 26, 2007
is particularly rapid in newly developed or developing countries. In Taiwan, the proportion of elderly people in the population rose from 2.4% in 1950 to 8.6% in 2000 and is expected to increase exponentially to 35.3% by 2050[2].
Population aging inevitably increases health care costs because older people use more health care services than younger people. In the United States, total and average health care
costs increased markedly from 1992 to 2001[1]. This substantial financial burden has raised the importance of identifying and analyzing the health factors affecting health care utilization in the elderly population. In addition to chronic diseases, functional status is also a core component of the health status of the elderly. In the past decade, researchers have found that older people experiencing functional problems [3–5] or a decline in health status[6–9] are more likely to have higher subsequent medical utilization than independent older people.
However, these studies are limited to earlier surveys[3,4,6,9], local people[7], women[5], or use of Activities of Daily Living (ADLs) as the only measure of functional status[8]. The average health care expenditure may also vary across countries with different health care systems[10]. Therefore, it is unclear whether the influence of functional status on medical care costs remains the same in countries other than the United States. Using recent national survey data from Taiwan, we sought to re-examine the extent of the influence of physical function on the use of health care services in the older population.
MAterIAl And Methods study Participants
Data were based on the 2001 National Health Interview Survey (NHIS) in Taiwan. Similar to surveys conducted in other countries, the NHIS in Taiwan is a nationwide survey aimed at understanding the general health of the non-institutionalized population, with a representative sample of approximately 6,592 households selected by a multi-stage, stratified systematic sampling strategy. All family members in the selected household were interviewed with self-reported questionnaires in 2001. The methods and study design used in the NHIS have been described in
detail elsewhere[11]. For this study, all of the 2,955 survey participants who were 60 years of age and older were included. Self-reported information regarding gender, age, years of education, marital status, self-rated health status, chronic conditions diagnosed by physicians, mental health, and physical function were all obtained from the NHIS questionnaire designed for those 12 years of age and older. Self-rated health status was determined by asking participants to rate their health as excellent, very good, good, fair, and poor, and was categorized as positive (excellent, very good, or good), neutral (fair), and negative (poor). Chronic conditions were determined by the presence of seven common chronic conditions covering heart disease, lung disease (including chronic bronchitis, emphysema, asthma, and COPD), hypertension, diabetes, stroke, liver disease, and renal disease. The total number of these chronic conditions was categorized as 0, 1, and 2 or more for use in the analysis. Mental health was evaluated by five questions adopted from the mental health domain in the Taiwan version, SF-36[12,13]. Mental health scores were grouped as low (0-64), middle (65-80), and high (81-100), with a lower score representing a greater probability of mental disorder.
Functional status
In the NHIS questionnaire designed for those 12 years of age and older, functional status was mainly measured by 6 basic ADLs questions (with 4 response categories of difficulty or inability in taking a bath, dressing, eating, getting in and out of bed, walking across a room, and toileting) together with 9 mobility questions (with 3 response categories of limitation in doing vigorous activities, moderate activities, lifting or carrying groceries, climbing several flights, climbing 1 flight, bending and
kneeling, walking a mile, walking several blocks, and walking 1 block) adapted from the physical functioning domain in the Taiwan version, SF-36 [12,13]. The level of physical function was categorized, based on the ability to perform these 15 tasks, into dependency, difficulty, much limitation, some limitation, and normal. “Dependency” was defined as being unable to perform at least one of the six ADLs tasks. “Difficulty” was defined as having some or much difficulty to perform at least 1 of the 6 ADLs tasks. “Much limitation” was defined as having much limitation in performing at least 1 of the 9 mobility tasks. “Some limitation” was defined as having some limitation in performing at least 1 of the 9 mobility tasks. “Normal” was defined as having no difficulty or limitation in any of the 15 tasks.
health care expenses
The survey data were further linked to the health care data in order to obtain an understanding on the 1-year health care costs that occurred in the same year of the NHIS interviews. In Taiwan, comprehensive health and medical care for residents has been provided by the government through the National Health Insurance (NHI) program since 1995. Medical and health services covered in the NHI program include inpatient, outpatient, traditional Chinese medicine, dentistry, prenatal care and delivery, rehabilitation and home care, and preventive medicine. For this study, all claims made to the NHI program between 1 January 2001 and 31 December 2001 were retrieved by the Bureau of National Health Insurance for 2,420 (81.9%) of the NHIS participants who completed the informed consent of data linkage to the NHI program. The remaining 535 participants did not differ from those who consented in age, number of chronic conditions, self-rated health, and functional status, but they were more likely
to be females, widowed, depressed, and had a lower educational level. Of the participants who agreed to link their medical data, 84 failed to provide the needed data about final expenses because of deaths, unmatched ID numbers, or other unspecified reasons; 93 participants had missing information regarding physical function and 2,243 participants remained for the final analysis.
Analysis
The basic characteristics of the samples, including sociodemographics (gender, age, education level, and marital status), health status (self-rated health, total number of chronic diseases, and mental health), functional status, and health care expenditures were analyzed. The association between physical function and health care costs was first examined with direct comparison of the average costs and relative proportion of health care utilization across groups of elderly people with different levels of physical function. The independent effect of physical function on total health care expenses was further estimated using multivariate linear regression analysis. To satisfy the assumption of a normal distribution for the dependent variable in the linear regression, total health care expenses were logarithmic-transformed. All statistical analyses were carried out using SPSS-PC, version 12 (SPSS Inc., Chicago, IL, USA).
results
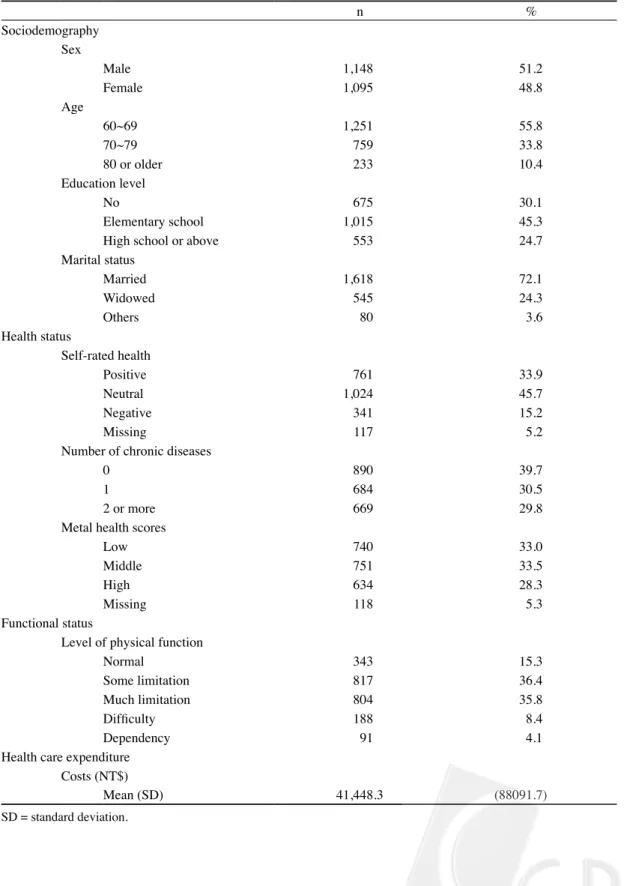
Descriptive details of the studied samples are given in Table 1. Of the 2,243 participants analyzed, 48.8% were females. The respondents aged 60-69, 70-79, and 80 years or older accounted for 55.8, 33.8, and 10.4% of the number of the analyzed study participants, respectively. Only 24.7% of the participants had completed high school or higher. Most of
Table 1. Characteristics of Study Participants on Demography, Health and Functional Status, and Health Care Use
n % Sociodemography Sex Male 1,148 51.2 Female 1,095 48.8 Age 60~69 1,251 55.8 70~79 759 33.8 80 or older 233 10.4 Education level No 675 30.1 Elementary school 1,015 45.3
High school or above 553 24.7
Marital status Married 1,618 72.1 Widowed 545 24.3 Others 80 3.6 Health status Self-rated health Positive 761 33.9 Neutral 1,024 45.7 Negative 341 15.2 Missing 117 5.2
Number of chronic diseases
0 890 39.7
1 684 30.5
2 or more 669 29.8
Metal health scores
Low 740 33.0
Middle 751 33.5
High 634 28.3
Missing 118 5.3
Functional status
Level of physical function
Normal 343 15.3
Some limitation 817 36.4
Much limitation 804 35.8
Difficulty 188 8.4
Dependency 91 4.1
Health care expenditure Costs (NT$)
Mean (SD) 41,448.3 (88091.7)
the participants (72.1 %) were married, 15.2 % of the participants rated their health status negatively, and 39.7% of the participants had no chronic disease. The mean score of mental health was 71.5 (SD=18.2). For the level of physical function, most of the participants had some (36.4%) or much (35.8 %) limitation; only 15.3, 8.4, and 4.1 % were classified as normal, with difficulty, or with dependency
respectively. The average health care cost was NT$41,448 (SD = NT$88,092).
Figure 1 depicts the distribution of average health costs (A) and the relative proportion of total participants and total expenses (B) among different functional categories. A clear gradient reverse relationship was observed between functional status and average health care costs. Individuals having functional problems used
Figure 1. Diagram showing the relationship between functional status and use of health care service (A. Average Health Care Costs among Older People with Different Level of Function. B. Rate Ratio and Relative Proportion Accounted for Total Participants and Total Health Care Expenses among Older People with Different Level of Function.)
The bars in Figure 1A indicate 95% confidence interval of average health care costs. * Rate ratio = % of total health care expenses / % of total participants.
higher health care costs. Furthermore, the increase of health care utilization in individuals with a decline in physical functioning reflects not only on the absolute means of total expenses, but also on the relative percentage of total expenses. In general, while accounting for a smaller proportion of the total population, individuals with functional problems consumed relatively larger proportions of the total health care expenses.
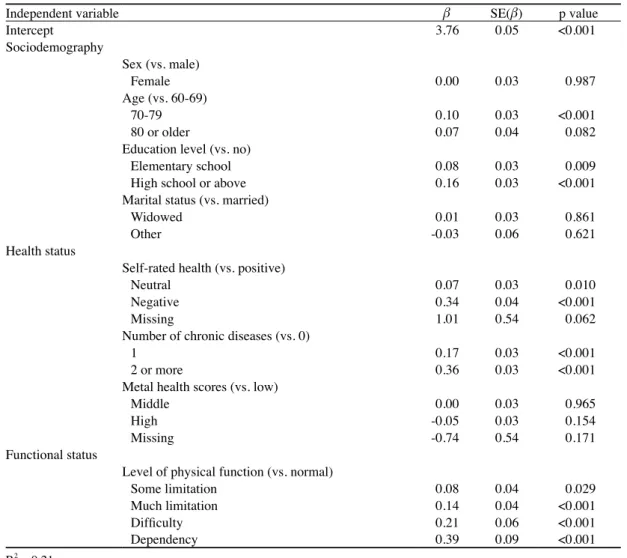
Table 2 presents the results of the multiple linear regression model used to estimate the effect of functional status on total health care expenditures, with adjustment for covariates, including age, gender, education level, marital status, self-rated health, number of selected medical conditions, and mental health. A gradient increase of regression coefficients was observed in the categories of functional status, and the level of physical function was, in general, independently associated with the use of health care. Older people who were classified as “dependent,” “difficulty,” or “much limitation” in their physical functioning incurred significantly higher health care costs than their counterparts who were classified as “normal” or “with some limitation.” Overall, the results from the model showed that health care costs increased with older age, higher education level, poorer self-rated health, more chronic conditions, and worse physical function.
dIscussIons
Our findings, although consistent with those of past studies on functional limitations and health care costs for the elderly[8,9], are unique in providing up-to-date evidence testifying to the significant association between the level of physical functioning and health care utilization from a non-US, nationwide representative survey data of a
non-institutionalized elderly population. Clearly, functional status is an important determinant of health care utilization in the elderly population across countries.
This is the first study evaluating the effect of functional status on medical care costs in the elderly population in Taiwan. In addition to the results, our study has several methodologic strengths that may be of help to researchers interested in pursuing similar studies in the future. For example, we employed not only ADLs, but advanced-skill items, to measure physical function and took into consideration the level of inability, difficulty, or limitation in differentiating the level of severity. Our results further identified a clear gradient relationship between the level of physical functioning and health care costs. This suggests that using domains of physical functioning and levels of severity in measuring and classifying the level of physical functioning can be expected to provide more complete information on functional status. Moreover, the source of information on health and functional status was from the NHIS, a routine nationwide survey that is commonly conducted in many countries and aimed at collecting health-related information.
Certain limitations of this research need to be considered. First, while most participants allowed us to access their NHI claims data, some declined the request. Those who did not consent reported obvious differences from the consenters with respect to several variables. The potential influence from the bias on the results cannot be excluded. Second, our study was limited by the cross-sectional design, and the dynamic effect of functional change, especially functional decline, on health care costs could not be measured. Third, some factors that could affect health care utilization, such as cognitive function and living arrangement, were not included in the regression, and the results need
Table 2. Multiple Linear Regression Model Assessing the Adjusted Relationship between Functional Status and Health Care Utilization
Independent variable β SE(β) p value
Intercept 3.76 0.05 <0.001 Sociodemography Sex (vs. male) Female 0.00 0.03 0.987 Age (vs. 60-69) 70-79 0.10 0.03 <0.001 80 or older 0.07 0.04 0.082
Education level (vs. no)
Elementary school 0.08 0.03 0.009
High school or above 0.16 0.03 <0.001
Marital status (vs. married)
Widowed 0.01 0.03 0.861
Other -0.03 0.06 0.621
Health status
Self-rated health (vs. positive)
Neutral 0.07 0.03 0.010
Negative 0.34 0.04 <0.001
Missing 1.01 0.54 0.062
Number of chronic diseases (vs. 0)
1 0.17 0.03 <0.001
2 or more 0.36 0.03 <0.001
Metal health scores (vs. low)
Middle 0.00 0.03 0.965
High -0.05 0.03 0.154
Missing -0.74 0.54 0.171
Functional status
Level of physical function (vs. normal)
Some limitation 0.08 0.04 0.029 Much limitation 0.14 0.04 <0.001 Difficulty 0.21 0.06 <0.001 Dependency 0.39 0.09 <0.001 R2 = 0.21 β = regression coefficient. SE = standard error.
to be explained with caution. Fourth, health care costs covering medical and home care spending were used in the study to represent health care utilization. Our data did not include information on the use of other formal (such as long-term care services) and informal services in the health care system. It is therefore not known whether the relationship between functional status and the overall health care utilization was the same as that in our study. Finally, only
total medical care costs were analyzed in this study. In addition to the effect on medical care costs, the relationship of functional status and other health care utilization indicators, such as outpatient visits and days of inpatients, needs to be examined in future studies.
Alongside population aging, there will be an increase in people with chronic diseases and functional problems. This will impose a huge financial burden on health care services[14].
Evidence from this cross-sectional analysis indicates that the utilization of health care among the elderly population in a health care system different from the one in the United States is also partly affected by functional status. It is clear that delaying or preventing the occurrence of functional decline for elderly adults is as important as preventing chronic diseases[15] to achieve effective reduction in health care expenditures.
AcknowledgMents
The 2001 National Health Interview Survey (NHIS), Taiwan was funded by the National Health Research Institutes (Project numbers: HP-090-PP-01, HP-091-PP-01, BS-090-PP-04, BS-091-PP-04), Taiwan.
reFerences
1. U.S. Federal Interagency Forum on Aging-Related Statistics. Older Americans 2004: Key Indicators of Well-Being. Washington, DC: U.S. Government Printing Office, 2004; 2, 44.
2. Manpower Planning Department. Projections of the Population of Taiwan Area, Republic of China, 2004-2051. Taipei: Council for Economic Planning and Development, 2004. [In Chinese]
3. Wan TT, Odell BG. Factors affecting the use of social and health services among the elderly. Aging Soc 1981;1:95-115.
4. Gruenberg L, Kaganova E, Hornbrook MC. Improving the AAPCC (adjusted average per capita cost) with health-status measures from the MCBS (Medicare Current Beneficiary Survey). Health Care Financ Rev 1996;17:59-75.
5. Weiner M, Fan MY, Johnson BA, Kasper JD, Anderson GF, Fried LP. Predictors of health resource
use by disabled older female Medicare beneficiaries l i v i n g i n t h e c o m m u n i t y. J A m G e r i a t r S o c 2003;51:371-9.
6. Mor V, Wilcox V, Rakowski W, Hiris J. Functional transitions among the elderly: patterns, predictors, and related hospital use. Am J Public Health 1994;84:1274-80.
7. Ferrucci L, Guralnik JM, Pahor M, Corti MC, Havlik RJ. Hospital diagnoses, medicare charges, and nursing home admissions in the year when older persons become severely disabled. JAMA 1997;277:728-34. 8. Fried TR, Bradley EH, Williams CS, Tinetti ME.
Functional disability and health care expenditures for older persons. Arch Intern Med 2001;161:2602-7. 9. Guralnik JM, Alecxih L, Branch LG, Wiener JM.
Medical and long-term care costs when older persons become more dependent. Am J Public Health 2002;92:1244-5.
10. Anderson G, Hussey PS. Comparing health system performance in OECD countries. Organization for Economic Cooperation and Development. Health Aff (Millwood) 2001;20:219-32.
11. Shih YT, Hung YT, Chang HY, et al. The design, contents, operation and the characteristics of the respondents of the 2001 National Health Interview Survey in Taiwan. Taiwan J Public Health 2003;22:419-30. [In Chinese: English abstract] 12. McHorney CA, Ware JE, Raczek AE. The MOS
36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care 1993;31:247-63.
13. Tseng HM, Lu JFR, Tsai YJ. Assessment of health-related quality of life in Taiwan (II): norming and validation of SF-36 Taiwan version. Taiwan J Public Health 2003;22:512-8. [In Chinese: English abstract] 14. Lan TY. Population aging in Taiwan: future health
implications. Taiwan J Public Health 2003;22:237-44. 15. Fried LP, Bush TL. Morbidity as a focus of
preventive health care in the elderly. Epidemiol Rev 1988;10:48-64.
1 國家衛生研究院老年醫學研究組 2 國家衛生研究院衛生政策研發中心 * 通訊作者:藍祚運 聯絡地址:苗栗縣竹南鎮科研路35號 E-mail: tylan@nhri.org.tw 投稿日期:96年8月9日 接受日期:96年11月26日