Key factors affecting healthcare professionals to adopt knowledge management:
The case of infection control departments of Taiwanese hospitals
Yu-Hui Chen
a, Chung-Feng Liu
b,*, Hsin-Ginn Hwang
c aInfection Control Committee, Chi-Mei Medical Center, Taiwan, ROC b
Department of Information Management, Chia-Nan University of Pharmacy and Science, Taiwan, ROC c
Institute of Information Management, National Chiao-Tung University, Taiwan, ROC
a r t i c l e
i n f o
Keywords: Healthcare
Infection control professionals Knowledge management Key factors
a b s t r a c t
Facing new infectious diseases that are result of continuous mutation of virus and bacteria and ever advancing communication and medical technologies, infection control professionals (ICPs) in the health-care industry must be able to obtain instantly the needed knowledge in order to increase efficiency and effectiveness in their practice. The purpose of this study is, after an exhaustive literature review and nec-essary interviews with specialists in this field, to propose a research framework that explores the factors that affect the ICPs’ willingness to adopt knowledge management (KM) into their tasks and to validate the usefulness of this research framework through a survey study. The research framework includes four con-structs that affect infection control professionals’ decision and willingness to introduce and to adopt infection control KM, and they are namely: hospital characteristics, infection control department, exter-nal environment, and project planning. The study conducted a survey among ICPs from 425 hospitals in Taiwan. A total of 227 valid questionnaire responses were returned from the ICPs from 90 hospitals. Among these responses, 55.00% are from medical centers and 47.83% are from regional hospitals. After analyzing the responses through the discriminant analysis method, the study found that ‘‘Hospital Resource Support,” ‘‘Colleagues’ Attitude,” and ‘‘Users’ Participation” are the three factors that signifi-cantly impact the professionals’ willingness for adopting KM in infection control departments. This study not only provides the healthcare industry an understanding about introduction and impact of KM, which can assist in their decision making, but also emphasizes the importance of use of actual data in the study of research framework for introduction of KM in healthcare industry. Therefore, this study presents important results in both practical and academic aspects.
Ó 2010 Elsevier Ltd. All rights reserved.
1. Introduction
In 1997, a new-type and extremely virulent H5N1 influenza virus, a.k.a. the bird flu, was found in Hong Kong, causing 18 infec-tion cases and leading 6 of them to death (WHO, 2005). After that, Severe Acute Respiratory Syndrome (SARS) was first noticed in Vietnam in the February of 2003, and, by the end of that year, 29 countries were under the threat of SARS with a total amount of 8096 suspected cases and 774 deaths (cumulated from 1 Novem-ber 2002 to 31 July 2003) (WHO, 2009a). Unfortunately, a new influenza virus, H1N1 (referred to as ‘‘swine flu” early on), is now spreading all over the world. Up to 23 May 2009, 43 countries have officially reported 12,022 cases of H1N1 infection. Mexico has
re-ported 3892 cases of infection, including 75 deaths (WHO, 2009b). Within few years, human beings faced three new kinds of highly-infectious and lethal diseases, which made the whole world pay more attention to disease prevention and infection con-trol. Infection control is deemed as one of the important tasks which should be fulfilled in the 21st century (Hsueh & Yang’s re-port, 2003).
From the perspective of public health and epidemiology, infec-tion control is a long-term disease preveninfec-tion program. The Tai-wanese government pays much attention on the effects of infection control. For example, it is known from the Medical Care Act that Taiwan’s government has stipulated that hospitals should take the responsibility for infection control, and the performance of which weighs heavily in the hospital accreditation. In practices, hospitals are asked to offer a lot of disease prevention measure, keep an eye on the epidemiological study, and establish an infec-tious disease reporting system. And the infection control depart-ment is deservedly taken as the communicating channel with the stakeholders; the department, hence, covers the disease preven-0957-4174/$ - see front matter Ó 2010 Elsevier Ltd. All rights reserved.
doi:10.1016/j.eswa.2010.06.085
*Corresponding author. Address: Department of Information Management, Chia-Nan University of Pharmacy and Science, 60 Erh-Jen RD., Sec. 1, 717 Jen-Te, Tainan, Taiwan, ROC. Tel.: +886 6 2664911x5303; fax: +886 6 3660607.
E-mail addresses: [email protected] (Y.-H. Chen), fredliu@mail. chna.edu.tw(C.-F. Liu),[email protected](H.-G. Hwang).
Contents lists available atScienceDirect
Expert Systems with Applications
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . c o m / l o c a t e / e s w ation at not only the hospital, but also its neighboring community. But, this trend has caused an increase in workload for infection control department.
Due to the unfamiliarity with professional knowledge pertain-ing to the medical care and infection control, a knowledge gap among the practitioners is formed. The gap is even more obvious when it comes to problems related to infection control or disease spread/prevention. In the face of emerging infectious diseases brought by ever-evolving bacteria or viruses, ICPs must keep on absorbing relevant knowledge – both contributed from literature and experienced predecessors. In fact, managing critical data and information is a key element of infection control and epidemiology in healthcare organizations.
KM in healthcare can be regarded as the confluence of formal methodologies and techniques to facilitate the creation, identifica-tion, acquisiidentifica-tion, development, preservaidentifica-tion, dissemination and final-ly the utilization of the various facets of a healthcare enterprise’s knowledge assets (Abidi, 2001). Knowledge management in infection control involves any systematic process that acquires, conserves, organizes, retrieves, displays, and distributes known infection-con-trol related information. As a result, ICPs often find themselves ‘‘swimming in an ocean of information” (Olmsted, 2000).
Many researchers have proposed various kinds of knowledge management frameworks or applications in healthcare settings (Abidi, 2001; Delesie & Croes, 2000; Lee, Wong, & Zhang, 1999; Liebowitz, 2010; Torralba-Rodriguez et al., 2003), but few have explored the critical factors in implementing KM system (KMS) from users (practitioners)’ view (Hwang, Chang, Chen, & Wu, 2008; Koumpouros, Nicolosi, & Martinez-Selles, 2006). Whether to set up a KM system (KMS) might be influenced by both internal and exter-nal factors. Thus, academically and practically speaking, exploration of factors affecting the adoption of KM in the infection control department from users’ sides is meaningful and worthwhile.
2. Factors influencing the ICPs’ adoption of KM
The factors affecting the adoption of innovative technology can be explored in diversity of dimensions. For example,Wixom and Watson (2001)posit that organizational factors (management sup-port, resources, user participation, etc.), project-related factors (re-source, user participation, team skills, etc.) and technical factors (high-quality source systems, better development technology, etc.) are important for implementing data warehouse technologies. According to an empirical research conducted byAlavi and Leidner (1999), the success/failure of adopting KM can be seen from three aspects of management, knowledge and information content, and technology. Holsapple and Joshi compiled past studies pertaining to KM and also believe that management, resources, and the indus-trial environment are the three key factors which decide whether KM is utilized (Holsapple & Joshi, 2000).
The healthcare industry is knowledge-intensive; it has a great amount of intangible assets and intellectual capital, and it is also different from other industries in many aspects. Based on the liter-ature review and experts’ viewpoints we conduct that factors influ-encing the introduction of infection control knowledge management (ICKM) can be explored from four constructs: the hospital characteristics, the infection control department, the external environment, and the project planning.
2.1. The construct of hospital characteristics 2.1.1. Hospital culture
The organizational culture is an aggregation of all members’ specific values and organization’s regulations, which pose influ-ences on the interaction method between external interested
par-ties and organizational members. According toDavenport, DeLong, and Beers (1998), knowledge-oriented culture is one of the most crucial factors for effectively enforcing KM. As well, it is pointed out by Glasser (1999) that the organizational culture is one of the key factors which determine the success/failure of enforcing KM. Organizational culture in general greatly influences how an organization handles knowledge (Maier, 2004). When a hospital can provide an effective way to encourage infection control col-leagues to cooperate and share knowledge with each other, the development of KM will be smoother.
2.1.2. Hospital scale
It is mentioned by many studies that the larger the organization scale (size) is, the more abundant resources and capital there will be for introducing new information technology (Dewar & Dutton, 1986; Kannebley, Porto, & Pazello, 2005; Levin, Levin, & Meisel, 1987). In terms of the healthcare industry, hospitals with different scales hold dissimilar attitudes to the investment in and applica-tion of the informaapplica-tion system. For instance, Furukawa, Raghu, Spaulding, and Vinze (2008) indicate that hospital scale is an important factor associated with health IT adoption for medication safety.
Ein-Dor and Segev (1978)argue that resource shortage is less seen in organizations with a larger scale, and it is more likely for such organizations to successfully establish an information system. In the eyes ofRaymond (1990), the introduction of IT is affected by the organization scale. Also, it is believed by Grover and Goslar (1993)that larger organizations stand on a solider foundation with more resources and better capability in tackling risks. After grow-ing into a certain scale, an organization will be able to adopt inno-vative technology. The most used indicator to represent the scale of a hospital is the number of beds.
2.1.3. Hospital resource support
Haley (1997) states that enterprise resources refer to those which can be made use of in a system development, such as the capital, the developing time and the manpower. Whether an orga-nization can offer sufficient capital, manpower, and time is said to be crucial for enterprise systems development (Grover & Goslar, 1993; Tait & Vessey, 1998). That is, top management support of re-sources allocation for systems development is very important. It can be seen in terms of the following indicators: executives’ under-standing in an information system’s advantages, executives’ assis-tance and related resources allocation, executives’ encouragement to colleagues for IT use, executives’ efforts in overcoming any resis-tance, executives’ involvement in decision-making of the project and their degree of satisfaction to users’ participation (Haley, 1997; Premkumar & Robert, 1999; Yap, Thong, & Raman, 1994). Meanwhile,Ein-Dor and Segev (1978)note that the development and implementation of the system will be constrained not only by internal factors (e.g. time and capital) but by external ones (e.g. manpower training and software/hardware).
2.1.4. Hospital internal needs
Premkumar and Ramamurthy (1995)point out that the organi-zational need is a key factor influencing the introduction of IT. They argue that internal needs can be emphasized on the average bene-fit for the organization. It refers to how the innovative technology can decrease cost and increase the service quality, work efficiency and competitive advantage. Many scholars believe that the organi-zational need is an important factor which triggers the willingness to utilize the information technology (Premkumar & Ramamurthy, 1995; Zmud, 1984). Whether an investment should be made is pondered over only when the decision makers are in need of and willing to adopt the innovative technology. This leads to our first hypothesis:
Hypothesis 1. Hospital characteristics poses a significant influence on the ICP’s willingness to adopt ICKM.
Hypothesis 1.1: The hospital culture poses a significant influence on the ICP’s willingness to adopt ICKM.
Hypothesis 1.2: The hospital scale poses a significant influence on the ICP’s willingness to adopt ICKM.
Hypothesis 1.3: The hospital resource support poses a significant influence on the ICP’s willingness to adopt ICKM. Hypothesis 1.4: The hospital internal needs poses a significant influence on the ICP’s willingness to adopt ICKM. 2.2. The construct of infection control department
2.2.1. Executives’ leadership style
Generally, leadership is described as a process of influencing others and creating an environment for achieving the goal of the group (or the organization). In the eyes ofStogdill (1974), the lead-ership style refers to a leader’s behaviors in pushing a team to accomplish their goal.Gardner (1999)also indicates that leading is a process of lobbying or exemplifying, from which the group members will be invigorated to pursue the goal set by the leader or shared by them all.
Gatignon and Robertson (1989)examined factors affecting an organization to adopt new IT and found that the way decision-makers deal with the information is one of the main factors. Lead-ers push their followLead-ers by pLead-ersuasion and power, and they create an environment for followers to work more efficiently. Through executives’ leading, colleagues’ latent capabilities are triggered, their work efficiency are raised, personal needs of every member are satisfied, the hospital’s effectiveness is enhanced, and the hos-pital’s goal is accomplished.
2.2.2. Colleagues’ attitudes to ICKM
KM collects knowledge, experiences, and technologies within an organization and turns them into resources that are accessible to all colleagues. KM is an activity of gathering knowledge from everyone; it achieves the organizational task through deliberate estimation (Wiig, 1997), and it betters the organizational effective-ness through creating, acquiring, and making use of knowledge (Laurie, 1997). With higher satisfaction degree of self-awareness in KM, colleagues tend to hold greater identification with the KM system of their hospital in every dimension (Su, 2003).
The application of KM penetrates the functional areas of all industries, and the healthcare industry is no exception. Therefore, hospitals with different types and different scales hold dissimilar attitudes to ICKM, and their willingness to adopt ICKM also differs. 2.2.3. Colleagues’ computer literacy
The degree of prevalence of IT-related knowledge is a crucial factor for determining the success/failure of the digitalization of the medical information (Marion, 1999). According toMontazemi, Cameron, and Gupta (1996), the evaluation on the system software will be influenced by users’ experience in using a computer and whether they feel uneasy about it. Such experience is in terms of some basic IT concepts, such as: knowing fundamental compo-nents of a computer system (including PC, the terminating ma-chine, the internet, the computer software, programming languages, and peripheral equipment of a computer), basic under-standing of the internet and the communication technology, and the establishment and application of the database (Hwang, Chang, & Liu, 2006; Saranto & Leino-Kilpi, 1997; Staggers, Gassert, & Cur-ran, 2002; Verhey, 1999).
Today, computer literacy does not talk about what a person accomplished in the past, but cares about what a person will
achieve in the future. It is not about a person’s basic skills (e.g. starting a computer, formatting a disk, or using specific software) but represents a person’s awareness in completing a task by using a computer (e.g. using software package, writing a mail by a word processor, and analyzing data) (Compeau & Higgins, 1995). There-fore, we propose the second hypothesis:
Hypothesis 2. Infection control department poses a significant influence on the ICP’s willingness to adopt ICKM.
Hypothesis 2.1: Executives’ leadership style poses a significant influence on the ICP’s willingness to adopt ICKM. Hypothesis 2.2: Colleagues’ attitudes to ICKM pose a significant influence on the ICP’s willingness to adopt ICKM. Hypothesis 2.3: Colleagues’ computer literacy poses a significant influence on the ICP’s willingness to adopt ICKM. 2.3. The construct of external environment
Medical systems and regulations vary and thus causing the healthcare environment to be unstable. So, it is brought forth by some researchers that the environment of a target industry is one of the key factors affecting the willingness and motivation for introducing a new system (Gatignon & Robertson, 1989; Grover & Goslar, 1993).
2.3.1. Medical acts and regulations
Medical service determines life/death of a patient, so it is strictly regulated by the government. That is, the operational suc-cess of a medical organization relies on whether it can effectively cope with the variation of government’s medical policies and the competition from the external environment (Kaluzny & Shorter, 2005). Hence, hospitals in all kinds of scales are influenced by political factors, including the new policy promulgation, legal reg-ulations, the implementation of the National Health Insurance (NHI), and strategies of development of the electronic medical re-cord (EMR).
In the mean time, as emerging infectious diseases increase, ‘‘Communicable Disease Control Acts and Regulations” and per-taining articles are constantly amended by the Center for Disease Control of Taiwan, which stipulates the violation penalties (on medical institutions, physicians, medical technologists, etc.). Under such circumstances, all hospitals have to adapt themselves to gov-ernmental regulations, NHI policy variation, and competition against other hospitals.
Sher, Hsueh, and Hwang (2005)indicate that the adoption of IT in a hospital is influenced by the government’s guidance policies. Similarly, it can be noticed fromInamura et al.’s (2003)study that regulations and guidance measures done by the government will pose an impact on the introduction of PACS (picture archiving and communication system) in a hospital.
2.3.2. Support from the technology supplier
Undoubtedly, IT service suppliers will import innovative tech-nology and service for adopting a new IT service. While imple-menting complex or cross-disciplinary systems, it shows more important. Many researchers indicate that technical support and training from and interactions with IT service suppliers are impor-tant indicators for evaluating technology supplier support ( Gati-gnon & Robertson, 1989; Yap et al., 1994). In the eyes of
Premkumar and Robert (1999), such indicators include effective application, encouragement to adoption, whether training is pro-vided, and active marketing. Finally,Sher et al. (2005)point out that, if we want to take into account technology suppliers, we should first assess their reputation, quotation, company scale,
and other hospitals’ feedbacks. Hence, we propose the third hypothesis:
Hypothesis 3. The external environment poses a significant influ-ence on the ICP’s willingness to adopt ICKM.
Hypothesis 3.1: Medical Acts and Regulations pose a significant influence on the ICP’s willingness to adopt ICKM. Hypothesis 3.2: Support from the technology supplier poses a sig-nificant influence on the ICP’s willingness to adopt ICKM.
2.4. The construct of project planning
Project planning is a key factor for the adoption of the informa-tion system. A highly skilled project team is much better equipped to manage and solve technical problems (Wixom & Watson, 2001). During project planning, it is hard to estimate users’ needs, and the data management design is also difficult to meet what every unit wants.
2.4.1. Task force skills
Task force members of a large IT project play an important role in planning (Inmon, 1997). A task force should possess experience in establishing information system and interacting with others. Moreover, the task force should be composed of colleagues who are familiar with the operation of all units, so that the introduction of KM can be facilitated (Haley, 1997).
2.4.2. Assistance from the information consultant
Because KMS is quite different from general transaction-based systems and requires a great amount of time and capital, professionals who are experienced in large IT imple-mentation projects will play a very crucial role in the introduction of KM. With the assistance from the information consultant, the lack of specific experience in IT can be over-come. Based upon professional experiences, the information consultant can offer useful suggestions for the large IT project (Haley, 1997).
2.4.3. User participation
It is pointed out by many studies that there is a positive corre-lation between users’ participation and the successful adoption of IT.Olson and Ives (1981)think that user participation should be defined as the act of taking part in the process of development, and this act is done by a member or a group of people who share the same goal.Tait and Vessey (1998) suggest that user system, technical system, and development process variables should also be taken into account in assessing the effect of user involvement on system success. Similarly,Lawrence and Low (1993)argue that the group formed by users should guarantee that they should ac-tively join the process of developing the system, understanding the system objectives, receiving enough training, and providing sufficient technology documents. According toHartwick and Barki (1994), the most important evaluation indicators for user partici-pation are: taking the responsibility throughout the development, the correlation between users and the information system, and personally joining the activity design. This leads to our last hypothesis:
Hypothesis 4. Project planning poses a significant influence on the ICP’s willingness to adopt ICKM.
Hypothesis 4.1: Task force skills pose a significant influence on the ICP’s willingness to adopt ICKM.
Hypothesis 4.2: Assistance from the information consultant poses a significant influence on the ICP’s willingness to adopt ICKM.
Hypothesis 4.3: User participation poses a significant influence on the ICP’s willingness to adopt ICKM.
3. Research methodology
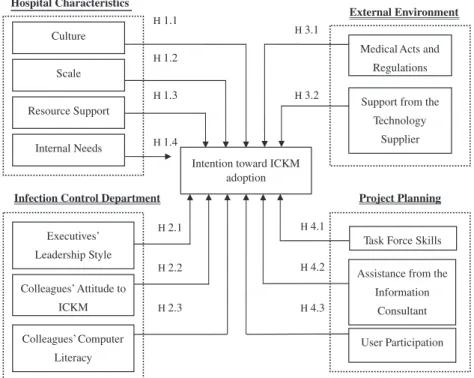
Based upon the reviewed literature and experts’ opinions, this survey study developed a research framework for ‘‘factors influ-encing a hospital’s willingness to adopt ICKM,” which includes four constructs: ‘‘hospital characteristics,” ‘‘infection control depart-ment,” ‘‘external environdepart-ment,” and ‘‘project planning” (see
Fig. 1). Questionnaire survey was used in this study with infection control department colleagues as respondents. After responses were collected, the discriminant analysis method was adopted to examine the hypotheses and relevant discussions.
This survey adopted a 5-point Likert scale, the content of which was based on questionnaire samples and pertinent theories pro-posed and verified by earlier researchers (Ein-Dor & Segev, 1978; Gardner, 1999; Gatignon & Robertson, 1989; Grover, 1998; Grover & Goslar, 1993; Haley, 1997; Inamura et al., 2003; Laurie, 1997; Premkumar & Robert, 1999; Premkumar & Ramamurthy, 1995; Raymond, 1990; Saranto & Leino-Kilpi, 1997; Sher et al., 2005; Staggers et al., 2002; Verhey, 1999; Wiig, 1997; Yap et al., 1994).
Furthermore, a group of experts, which includes a professor in medical information management and an executive of a hospital’s infection control department, were invited to review and modify the questionnaire. Then, an in-depth interview and a pretest were conducted on three experienced ICPs, whose opinions were com-piled as the modification reference for the final draft of the ques-tionnaire. Likert five-point scale was adopted, in which 1 means ‘‘strongly disagree” and 5 ‘‘strongly agree.”
4. Results
4.1. Description statistics
In this study, infection control department colleagues from 425 hospitals in Taiwan (covering medical centers, regional hospitals, and community hospitals) were recruited as subjects, who consist of doctors, infection control nurses, and medical technologists. Fi-nally, 227 valid responses were collected from 90 hospitals, which account for 21.18% of total hospitals in Taiwan. In terms of re-sponses from different hospital scales, the response rate of medical centers is 55.00%, while that of regional hospitals is 47.83%, which reveal that the survey outcome is representative.
When it comes to the basic information of respondents, most of them are female, who account for 79.30% of the total respondents; many of the infection control colleagues are nurses (63.44%), fol-lowed by doctors (22.47%), and medical technologists (14.10%); middle- and higher-level executives account for 22.03% of the total respondents; as for the years of work experience in infection con-trol, those working for 5–20 years account for the biggest propor-tion (40.53%).
Basic descriptive statistics of each construct’s evaluation indica-tors can be seen inTable 1below. All in all, in the eyes of infection control colleagues, the most important factor influencing the intro-duction of KM is ‘‘Support from the Technology Supplier,” followed by ‘‘Executives’ leadership Style,” and ‘‘Colleagues’ Computer Liter-acy.” On the other hand, the least important factor is ‘‘Hospital Cul-ture,” followed by ‘‘Hospital Resource Support,” and ‘‘Assistance from the Information Consultant.”
Generally, respondents agreed that KM is important to the development of infection control (87.67%). As for the willingness
to promote ICKM, 73.13% of the respondents showed high willing-ness, while low willingness was noticed in 3.08% of them, and the rest of the respondents held a moderate attitude toward it.
4.2. Validity and reliability
A questionnaire was carefully devised in order to gather data from the variables in the research framework based on related lit-erature review. Two-expert reviews were invited to validate the re-search framework and associated variables prior to the investigation being launched. Three-ICP pre-tests were completed in order to ensure that the items in the questionnaire were well ex-pressed to procure the required information for analysis. As a re-sult, the content validity and face validity of the instruments in the study could be guaranteed acceptably.
Cronbach’s
a
was used to examine the reliability of the variables in the research framework. Except for ‘‘hospital cultural” whicha
value is 0.681,a
values of the other variables range between 0.764 and 0.964. It indicates that the reliability of this study is acceptable (Nunnally, 1978).4.3. Hypotheses testing
In this study, the degree of user’s willingness to adopt ICKM was taken into consideration to examine the importance (the discrim-inating power) of each construct variable. In terms of the willing-ness to adopt ICKM, those answering ‘‘1. very low willingwilling-ness,” ‘‘2. low willingness,” and ‘‘3. moderate willingness” were catego-rized into the group of ‘‘Low Willingness,” which included 61 respondents. On the other hand, those answering ‘‘4. high willing-ness,” and ‘‘5. very high willingness” were categorized into the group of ‘‘High Willingness,” which included 166 respondents. The average and standard deviation of variables in each group can be seen inTable 2.
Furthermore, the Wilks’ Lambda value from the discriminant analysis is 0.730, and the p value is 0.000, which reaches the level of significance and reveals that the whole model is sufficiently dis-criminated. Besides, it is held byHair, Anderson, Tatham, and Black (1998)that the discriminant ability can be assessed by discrimi-nant loading and standardized discrimidiscrimi-nant coefficient. A variable possesses a strictly significant discriminant-ability if both indica-Infection Control Department Project Planning
Assistance from the Information
Consultant Task Force Skills
User Participation H 4.2 H 4.1 H 4.3 H 3.1 H 3.2 External Environment
Medical Acts and Regulations
Support from the Technology Supplier Hospital Characteristics Culture Scale Resource Support Internal Needs H 1.4 H 1.1 H 1.2 H 1.3
Intention toward ICKM adoption H 2.2 H 2.1 H 2.3 Executives’ Leadership Style Colleagues’ Attitude to ICKM Colleagues’ Computer Literacy
Fig. 1. Research framework.
Table 1
Descriptive statistics of variables.
Construct Variable Average Standard deviation Rank of average
Hospital characteristics Hospital Culture 3.37 0.69 11
Hospital Resource Support 3.47 0.77 10
Hospital Internal Needs 3.88 0.53 7
Infection control department Executives’ Leadership Style 4.03 0.69 2
Colleagues’ Attitudes to ICKM 3.98 0.50 4
Colleagues’ Computer Literacy 4.01 0.53 3
The external environment Medical Acts and Regulations 3.92 0.65 5
Support from the Technology Supplier 4.17 0.55 1
Project planning Task Force Skills 3.87 0.75 8
Assistance from the Information Consultant 3.71 0.83 9
tors are equal to or greater than 0.3 (absolute value). It could be shown from the analysis results that the discriminant ability is found in three variables (seeTable 3): ‘‘Colleagues’ Attitudes to ICKM,” ‘‘Hospital Resource Support,” and ‘‘User Participation.” That is to say, Hypothesis 1.3, Hypothesis 2.2 and Hypothesis 4.3 were significantly supported.
5. Discussion
This study aims to investigate factors influencing ICPs’ willing-ness to adopt ICKM, and it could be noticed from the results that infection control colleagues generally held high willingness on this issue. Nevertheless, influencing factors differ in accordance with the level of willingness. This situation will be discussed in the fol-lowing sections.
5.1. The construct of hospital characteristics
Eeekin, Helms, and Haynes (1990)argue that colleagues’ trust in the project or technology that executives promote is conducive to
smooth implementation. As well, it is mentioned byHaley (1997)
that full resource integration helps prevent unnecessary obstacles. The introduction of sufficient manpower and capital into the pro-ject will make it run more smoothly. Contrast to general comput-erization activities, however, the adoption of KM system covers the establishment of an innovative management mechanism and the implementation of advanced software/hardware—similar to so-called ‘‘Technology and support infrastructure” component of
Guptill (2005)’s framework for applying knowledge management to healthcare. That is to say, for a hospital to make a success IT, it has to not only invest considerable capital and time, but also hold top-management’s attitudes toward the promotion of the project. Therefore, compared to Hospital Culture and Hospital Scale, ‘‘Hospital Resource Support” is seen as a more significant fac-tor influencing infection control department personnel’ willingness to adopt KM. In other words, the success in adopting ICKM lies in hospital managerial personnel’s willingness to invest sufficient re-sources; this argument is supported by this study.
Additionally, it is held byPremkumar, Ramamurthy, and Nilak-anta (1994)that whether IT is adopted relies much on the organi-zation’s internal needs. So far, KM is less applied in hospitals (Hwang et al., 2006), and it is a new concept to infection control staff. The study result still cannot prove if hospital’s internal needs will influence the willingness to adopt ICKM.
5.2. The construct of infection control department
Undoubtedly, the introduction of ICKM is directly affected by infection control colleagues’ understanding on it such as: profes-sional infection control knowledge, the awareness in document categorization, the awareness in knowledge- or skill-sharing, the awareness in retaining relevant colleagues’ experiences and knowledge, and the needs in market competition. Besides, it is sup-ported by the research result that the willingness to adopt ICKM is significantly influenced by ‘‘Colleagues’ Attitudes to ICKM.”
According toStogdill (1974), the leadership style refers to an executive’s behaviors in pushing a team to accomplish their goal. However in practice, the infection control in a hospital requires pro-fessional services, and is usually in charge by a physician with rel-evant knowledge as a part-time job. As result, it is shown from the study that infection control colleagues’ willingness to adopt ICKM is not significantly influenced by ‘‘Executives’ Leadership Style.”
On the other hand, computer literacy refers to a person’s aware-ness in completing a task by using a computer. In the field of healthcare, it is pointed out by many studies that whether the computer system is easy to use will not influence the benefits brought by it (Chau & Hu, 2002; Liu & Ma, 2005; Yi, Jackson, Park, & Probst, 2006). The study still cannot tell us whether ‘‘Colleagues’ Computer Literacy” will influence the ICP’s willingness to adopt ICKM or not.
5.3. The construct of the external environment
It is shown from the research result that the infection control colleagues’ willingness to adopt ICKM is not significantly influ-enced by ‘‘Medical Acts and Regulations” and ‘‘Support from the Technology Supplier.” Even though the infection control is stan-dardized in the accreditation system, KM is still a new concept to infection control and famous cases of successful implementation are seldom seen, i.e. the supply source is rather limited. That is, the ICPs may have no clear idea for adopting ICKM, let alone con-sidering support from outside KM supplier. Hence, these two fac-tors are agreed to be important though, they are not taken as key factors affecting the adoption of ICKM.
Table 2
Average and standard deviation of variables in each group.
Group Variable Average SD
Low willingness
Hospital Culture 3.05 0.71
Hospital Resource Support 2.97 0.66
Hospital Internal Needs 3.61 0.51
Executives’ Leadership Style 3.72 0.76 Colleagues’ Attitudes to ICKM 3.60 0.48 Colleagues’ Computer Literacy 3.89 0.55 Medical Acts and Regulations 3.63 0.67 Support from the Technology Supplier 3.95 0.58
Task Force Skills 3.75 0.78
Assistance from the Information Consultant 3.47 0.82 User Participation 3.69 0.62 High willingness Hospital Culture 3.48 0.65
Hospital Resource Support 3.66 0.72
Hospital Internal Needs 3.98 0.51
Executives’ Leadership Style 4.14 0.63 Colleagues’ Attitudes to ICKM 4.11 0.42 Colleagues’ Computer Literacy 4.06 0.52 Medical Acts and Regulations 4.03 0.60 Support from the Technology Supplier 4.25 0.51
Task Force Skills 3.92 0.74
Assistance from the Information Consultant
3.80 0.81
User Participation 4.00 0.66
Table 3
Discriminant loadings and standardized discriminant coefficients of variables.
Variable Discriminant
loading
Standardized discriminant coefficient Colleagues’ attitudes to ICKM 0.86 0.68
Hospital resource support 0.72 0.47
Hospital internal needs 0.53 0.07
Hospital culture 0.48 0.04
Medical acts and regulations 0.47 0.12 Executives’ leadership style 0.46 0.03 Support from the technology
supplier
0.42 0.05
User participation 0.36 0.30
Hospital scale 0.32 0.06
Assistance from the information consultant
0.30 0.15
Colleagues’ computer literacy 0.23 0.04
5.4. The construct of project planning
KM is a set of intricate organizational strategy mechanisms, which should be promoted officially by a cross-sector task force in an organization. This task force should involve ICPs, information systems personnel, personnel from other medical departments, and/or external professional suppliers and consultants. It is found byHaley (1997)that it is extremely important for a task force to possess experiences in implementing a large-scale information system. Without such experiences, the organization can turn to the information consultant for assistance. It is also mentioned by
Grover (1998) that the establishment of a steering committee can help the task force in facilitating the development of the pro-ject. The committee should not only be a coordinator between the stakeholders, but also establish the priority for the develop-ment procedures and lead resource integration.
Furthermore, the establishment of IT calls for not only technol-ogists’ relevant skills, but also users’ domain knowledge. Without either of them, the establishment task would fail (Haley, 1997), i.e. ‘‘User Participation” is a key for the success in adopting the information system (Lawrence & Low, 1993; Hartwick & Barki, 1994). Infection control is a professional and important job. A suc-cessful implementation of ICKM counts on users’ participation; that is, the promotion of ICKM will run less smoothly if the task force fails to recruit ideal users to join the project or if users do not actively take part in project planning. In this situation, the ICP’s willingness to adopt ICKM will also be influenced, and this view-point is supported by the study result.
As analyzed above, ‘‘Support from the Technology Supplier” poses an insignificant influence on the ICP’s willingness to adopt ICKM. So, advanced factors, like task force skills and external infor-mation consultant’s capability, would also be less concerned by the ICP. The study result cannot let us know if ‘‘Task Force Skills” and ‘‘Assistance from the Information Consultant” will influence the ICP’s willingness to adopt ICKM.
6. Conclusion
Knowledge-based economy is the mainstream in today’s society and KM has been aware of a trend for improving personal and orga-nizational efficiency and effectiveness. So far, the application of IT in industries has reached maturity and produced many achieve-ments. KM has been promoted with great efforts by many Taiwan-ese organizations thTaiwan-ese years, and government also set up numerous guiding mechanisms for it. But, the development and introduction of KM in the healthcare industry is not visible, espe-cially in the field of infection control.
6.1. Implications
Academically, this study brought forth a model investigating the healthcare practitioners’ willingness to adopt KM and sup-ported the empirical research results of the application of IT in this industry. This is a valuable reference for studies on KM application in specific fields. Nevertheless, a significant influence could not found in many constructs and variables, so future researchers are suggested to explore more influencing factors from other theories or practical fields in an effort to conduct further investigations to strengthen the explanatory power of this study. In addition, since KM has been promoted in the business circle for a period of time and produced some successes, it is suggested that research com-parisons be made by taking into account pertinent studies from other industries, like the financial industry or the electronics industry, so that the research results can be taken as the founda-tion for studies related to the establishment of KM.
Practically, because the introduction of IT calls for a great amount of capital and time and brings unpredictable profits, hospi-tals, during the introduction process, are suggested to take into consideration influencing factors and care more about user partic-ipation so that unnecessary loss or waste in manpower or re-sources can be reduced or prevented. In addition, hospitals of different levels possess different amount of available resources, and a hospital and its infection control department may hold dif-ferent attitudes to the introduction of ICKM. Therefore, it is sug-gested that hospitals make early planning, properly allocate available resources, and encourage and nurture staff who are expe-rienced in ICKM. Meanwhile, as a trend, despite having long been applied by other industries, KM per se and its combination with IT are still new concepts in the healthcare industry, and medical colleagues’ understanding in them is limited. Hence, it is suggested that more ICKM-related instruction and on-the-spot visits should be provided, and executives and ICPs should be encouraged to take part in these activities in an attempt to enrich their knowledge in ICKM. As consequence, executives’ and colleagues’ willingness to adopt ICKM will be raised, and they would actively join the project planning, too. Additionally, if we want to retain and spread col-leagues’ ICKM-related experiences and knowledge, the incorpora-tion of IT is inevitable. Thus, it is suggested that hospitals integrate current resources, make more effective use of existing knowledge, and classify and preserve the existing knowledge in an effort to set up an adequate KM mechanism. In the future, appli-cation software can be adopted to Improve KM per se.
6.2. Limitations and future research
Due to the time and manpower constraint, responses were col-lected from 90 hospitals. Although both the response rate of med-ical centers and that of regional hospitals nearly reached 50%, island-wide hospital data, all in all, were unable to obtain.
So far, there have been few studies on the application of ICKM in the healthcare industry. It is hoped that the research results can help hospitals know key factors influencing the willingness to adopt ICKM and be taken as a reference for subsequent studies in the academic circle and the practical one. Due to great resource dif-ferences between medical centers, regional hospitals, and commu-nity hospitals, a questionnaire survey might neglect the real needs, limitation, and dissimilar influencing factors in hospitals of differ-ent levels, which, in fact, may adopt ICKM for differdiffer-ent consider-ation. Future researchers can further examine factors influencing same-level hospitals’ willingness to adopt ICKM. In addition to probing into the ICP’s willingness to adopt ICKM, future research-ers can also analyze other factors from the presearch-erspective of an orga-nization in an effort to establish a model with greater explanatory power. Besides, from the results in this study, respondents with low/high willingness can be invited for an in-depth interview in an attempt to gain advanced and deeper results and conclusions.
When it comes to subsequent research directions, it is sug-gested that future researchers test the model of this study with subjects from different information-intensive industries, such as the financial industry or the electronics one. Furthermore, research results in different industries can be compared and analyzed to raise the reliability, validity, and value of the model in this study. Besides, the investigation can be conducted from other variables, such as the degree of introduction, the introduction benefits, etc. so that a more comprehensive and deep result would be gained. As for whether the promotion or introduction of ICKM will be influ-enced by a disease outbreak or some special situations, it can be examined in influencing constructs. Meanwhile, after the IT devel-opment in the healthcare industry has reached maturity, research-ers can try to conduct longitudinal empirical research on more
precisely comparing factors posing influences in the beginning and in the maturing of adopting ICKM.
References
Abidi, S. S. R. (2001). Knowledge management in healthcare: Towards knowledge-driven decision-support services. International Journal of Medical Informatics, 63(1–2), 5–18.
Alavi, M., & Leidner, D. E. (1999). Knowledge management systems: Issues, challenges and benefit. Communications of the AIS, 1, 1–37.
Chau, Y. K., & Hu, J. H. (2002). Investigating healthcare professionals’ decisions to accept telemedicine technology: An empirical test of competing theories. Information & Management, 39, 297–311.
Compeau, D. R., & Higgins, C. A. (1995). Computer self-efficacy: Development of a measure and initial test. MIS Quarterly, 21(2), 189–211.
Davenport, T. H., DeLong, D. W., & Beers, M. C. (1998). Successful knowledge management projects. Sloan Management Review, 39(2), 43–57.
Delesie, L., & Croes, L. (2000). Operations research and knowledge discovery: A data mining method applied to health care management. International Transactions in Operational Research, 7, 159–170.
Dewar, R. D., & Dutton, J. E. (1986). The adoption of radical and incremental innovations: An empirical analysis. Management Science, 32, 1422–1433. Eeekin, L. P., Helms, M. M., & Haynes, P. J. (1990). People: A critical element of new
technology implementation. Industrial Management, 32(5), 27–29.
Ein-Dor, P., & Segev, E. (1978). Organizational context and the success of management information system. Management Science, 24(10), 1064–1077. Furukawa, M. F., Raghu, T. S., Spaulding, T. J., & Vinze, A. (2008). Adoption of health
information technology for medication safety In U.S. hospitals 2006. Health Affairs, 27(3), 865–875.
Gardner, H. (1999). The disciplined mind; what all students should understand. NY: Simon & Schuster.
Gatignon, H., & Robertson, T. S. (1989). Technology diffusion an empirical test of competitive effects. Journal of Marketing, 53(1), 35–49.
Glasser, P. (1999). The knowledge factor. CIO Magazine.http://www.cio.com.au/ article/107326/knowledge_factor.
Grover, G. (1998). Identification of factors affecting the implementation of data warehousing. Unpublished PhD Dissertation. Auburn University at Montgomery.
Grover, V., & Goslar, M. D. (1993). The initiation, adoption, and implementation of telecommunications technologies in US organizations. Journal of Management Information Systems, 10(1), 141–163.
Guptill, J. (2005). Knowledge management in health care. Journal of Health Care Finance, 31(3), 10–14.
Hair, J. F., Anderson, R. E., Tatham, R. L., & Black, W. C. (1998). Multivariate data analysis (5th ed.). New Jersey: Prentice-Hall.
Haley, B. J. (1997). Implementing the decision support infrastructure: Key success factors in data warehousing. Unpublished PhD Dissertation. University of Georgia.
Hartwick, J., & Barki, H. (1994). Explaining the role of user participation in information system use. Management Science, 40(4), 440–465.
Holsapple, C. W., & Joshi, K. D. (2000). An investigation of factors that influence the management in organizations. Journal of Strategic Information Systems, 9(2–3), 235–261.
Hsueh, P. R., & Yang, P. C. (2003). Severe Acute Respiration Syndrome (SARS) – An emerging infection of the 21st century. Journal of the Formosan Medical Association, 102(12), 825–839.
Hwang, H. G., Chang, I. C., Chen, F. J., & Wu, S. Y. (2008). Investigation of the application of KMS for diseases classifications: A study in a Taiwanese hospital. Expert Systems with Applications, 34(1), 725–733.
Hwang, H. G., Chang, I. C., & Liu, C. F. (2006). Current states of development of electronic medical record in health care – 2005 annual report. Taiwan: Department of Health.
Inamura, K., Kousaka, S., Yamamoto, Y., Sukenobu, Y., Okura, Y., Matsumura, y., et al. (2003). PACS development in Asia. Computerized Medical Imaging and Graphics(27), 121–128.
Inmon, W. H. (1997). Managing the data warehouse. John Wiley & Sons.
Kaluzny, A. D., & Shorter, S. M. (2005). Creating and managing the future. In Shortell & Kaluzny (Eds.), Health care management – Organization design and behavior (5th ed.). NY: Delmar.
Kannebley, S., Porto, G. S., & Pazello, E. T. (2005). Characteristics of Brazilian innovative firms: An empirical analysis based on PINTEC—Industrial research on technological innovation. Research Policy, 34(2005), 872–893.
Koumpouros, Y., Nicolosi, G. L., & Martinez-Selles, M. (2006). Critical success factors for establishing a multidisciplinary health community knowledge management system using internet-based ICTs: The cardiology paradigm. International Journal of Healthcare Technology and Management, 7(3–4), 283–302.
Laurie, J. (1997). Harnessing the power of intellectual capital. Training & Development, 51(12), 25–30.
Lawrence, M., & Low, G. (1993). Exploring individual user satisfaction within user-led development. MIS Quarterly, 17(2), 195–208.
Lee, M. R., Wong, W. Y., & Zhang, D. M. (1999). A knowledge-based framework for clinical incident management. Expert Systems with Applications, 17(4), 315–325. Levin, S. G., Levin, S. L., & Meisel, J. B. (1987). A dynamic analysis of the adoption of a new technology: The case of optical scanner. The Review of Economics and Statistics, 69(1), 12–17.
Liebowitz, J. (Ed.). (2010). Knowledge management in public health. NY: Taylor & Francis.
Liu, L., & Ma, Q. (2005). The impact of service level on the acceptance of application service oriented medical records. Information & Management, 42(8), 1121–1135. Maier, R. (2004). Knowledge management systems: Information and communication
technologies for knowledge management (2nd ed.). Springer.
Marion, G. (1999). Barriers to the adoption of computerized technology in health care systems. Topic in Health Information Management, 19(4), 1–19.
Montazemi, A. R., Cameron, D. A., & Gupta, K. M. (1996). An empirical study of factors affecting software package selection. Journal of Management Information Systems, 13(1), 89–105.
Nunnally, J. C. (1978). Psychometric theory (2nd ed.). NY: McGraw-Hill.
Olmsted, R. N. (2000). Turning information into knowledge to prevent health care-associated infections and other adverse events: The electronic ICP as an agent of change. American Journal of Infection Control, 28(6), 389–391.
Olson, M. H., & Ives, B. (1981). User involvement in system design: An empirical test of alternative approaches. Information & Management, 4(4), 183–195. Premkumar, G., & Ramamurthy, K. (1995). The Role of interorganizational and
organizational factors on the decision mode for adoption of interorganizational systems. Decision Sciences, 26(3), 303–336.
Premkumar, G., Ramamurthy, K., & Nilakanta, S. (1994). Implementation of electric date interchange: An innovation diffusion perspective. Journal of Management Information Systems, 11(2), 157–186.
Premkumar, G., & Robert, M. (1999). Adoption of new information technologies in rural small business. Omega, 27(4), 467–484.
Raymond, L. (1990). Organizational context and information system success: A contingency approach. Journal of Management Information System, 6(4), 5–20. Saranto, K., & Leino-Kilpi, H. (1997). Computer literacy in nursing: Developing the
information technology syllabus in nursing education. Journal of Advanced Nursing, 25(2), 377–385.
Sher, M. L., Hsueh, Y. S., & Hwang, H. G. (2005). An empirical study of key factors affecting the performance evaluation of hospital information systems: Executives’ perspective. Taiwan Journal of Public Health, 24(1), 22–32. Staggers, N., Gassert, C. A., & Curran, C. (2002). A Delphi study to determine
informatics competencies for nurses at four levels of practice. Nursing Research, 51(6), 383–390.
Stogdill, R. M. (1974). Handbook of leadership: A survey of theory and research. NY: Free Press.
Su, C. P. (2003). A study of hospital director’s recognition and attitude about knowledge management (KM) and the Status Quo of Hospital’s Adoption of KM. Unpublished master’s thesis. Institute of Health Care Organization Administration, National Taiwan University.
Tait, P., & Vessey, I. (1998). The effect of user involvement on system success: A contingency approach. MIS Quarterly, 12(1), 91–108.
Torralba-Rodriguez, F. J., Fernandez-Breis, J., Garcia, R. V., Ruiz-Sanchez, J. M., Martinez-Bejar, R., & Gomez-Rubi, J. A. (2003). An ontological framework for representing and exploiting medical knowledge. Expert Systems with Applications, 25(2), 211–230.
Verhey, M. P. (1999). Information literacy in an undergraduate nursing curriculum: Development, implementation, and evaluation. Journal of Nursing Education, 38(5), 252–259.
World Health Organization (2005). The weekly epidemiological record. No. 49/50, 80, 425–432.http://www.who.int/wer/2005/wer8049.pdf.
World Health Organization (2009a). Cumulative number of reported probable cases of SARS. <http://www.who.int/csr/sars/country/table2004_04_21/en/index.html> Retrieved 03.04.09.
World Health Organization (2009b). Situation updates – Influenza A(H1N1).<http:// www.who.int/csr/don/2009_05_23/en/index.html>Retrieved 24.05.09. Wiig, K. M. (1997). Knowledge management: An introduction and perspective.
Journal of Knowledge Management, 1(1), 6–14.
Wixom, B. H., & Watson, H. J. (2001). An empirical investigation of the factors affecting data warehousing success. MIS Quarterly, 25(1), 17–41.
Yap, C. S., Thong, J. Y. L., & Raman, K. S. (1994). Effect of government incentive on computerization in small business. European Journal of Information System, 3(3), 191–206.
Yi, M. Y., Jackson, J. D., Park, J. S., & Probst, J. C. (2006). Understanding information technology acceptance by individual professionals: Toward an integrative view. Information & Management, 43(3), 350–363.
Zmud, R. W. (1984). An examination of push–pull theory applied to process innovation in knowledge work. Management Science, 30(6), 727–738.