行政院國家科學委員會補助專題研究計畫成果報告
利用 ELISPOT 以及細胞內細胞激素染色法來分析慢性 B 型肝炎病
患之 B 型肝炎病毒特異性 CD8 陽性與 CD4 陽性的 T 細胞反應
Analysis of Hepatitis B Virus-specific CD8
+and CD4
+T Cell
Responses in Patients Chronically Infected with Hepatitis B Virus
Using ELISPOT assay and Intracellular Cytokine Staining
計畫類別:▓個別型計畫
□整合型計畫
計畫編號:NSC89-2315-B-002-037
執行期間:
89
年
8
月
1
日至
90
年
7
月
31
日
計畫主持人:陳健弘
共同主持人:
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
執行單位:國立台灣大學附設醫院內科部
中
華
民
國
90
年
10
月
31
日
行政院國家科學委員會專題研究計畫成果報告
計畫編號:NSC89-2315-B-002-037
執行期限:89 年 8 月 1 日至 90 年 7 月 31 日
主持人:陳健弘 執行機構及單位名稱:台大醫院內科部
計畫參與人員:于位元
,鄭光淳 執行機構及單位名稱:台大醫院內科部
一、中文摘要 B 型 肝炎在台灣是個非常嚴重的問 題,大約 15-20﹪的成年人是 B 型肝炎帶原 者。B 型肝炎病毒的感染更是台灣地區慢 性肝炎、肝硬化,肝細胞癌的主要原因。 不少的研究顯示,B 型肝炎病毒本身並不 會造成細胞毒性,而是經由引發宿主免疫 系統而導致肝炎。另一方面,宿主對 B 型 肝炎病毒免疫系統反應的強弱,也與 B 型 肝炎病毒的清除有關。從文獻的回顧顯 示,在急性 B 型肝炎的病人,其體內的 B 型肝炎病毒特異性 T 細胞反應較強。相反 的,在慢性 B 型肝炎的病人,其體內的 T 細胞反應較為微弱。T 細胞反應的強弱似 乎與 B 型肝炎病毒在體內的清除有關。 然而,以往的研究所使用的免疫學分 析方式仍有一些缺點,那些方法比較耗 時,敏感度也較低,所以有可能低估了體 內 B 型肝炎病毒特異性的 T 細胞反應。最 近有二種免疫學分析方法可以用來分析抗 原特異性 T 細胞反應:ELISPOT 與細胞內 細胞激素染色。這兩種方法其敏感度可以 比以往的方法提高 100 倍以上,也不須要 冗長的體外抗原再刺激。已有數個研究成 功的利用這些方法來研究 CMV 病毒,愛滋 病毒,或皮膚黑色素癌腫瘤抗原特異性的 T 細胞反應。 因此,本研究利用 ELISPOT 與細胞內 細胞激素染色法的方式,來分析慢性 B 型 肝炎病人 B 型肝炎病毒特異性的 T 細胞反 應。我們成功的建立了 ELISPOT 與細胞內 細胞泌素染色法的分析方式,我們發現在 慢性 B 型肝炎的病人,其體內的 B 型肝炎 病毒特異性 T 細胞反應相當微弱,甚至偵 徹不出來。 我們的結果意味著,微弱的 B 型肝炎 病毒特異性 T 細胞反應,可能與慢性 B 型 肝炎病毒帶原的致病機轉有關。所以,強 化 B 型肝炎病毒特異性 T 細胞反應,可能 是未來治療慢性 B 型肝炎的方向之一。 關鍵詞:B 型肝炎, T 細胞反應, ELISPOT, 細胞內細胞激素染色法 Abstr actTaiwan is a hyperendemic area of hepatitis B virus (HBV) infection. Around 15-20% adults in Taiwan are chronically infected with HBV. Previous studies demonstrated vigorous T cell responses to HBV-encoded antigens developed in patients with self-limited acute hepatitis B. In contrast, weak or no T cell responses could be detected in chronic hepatitis B patients.
The immunological assays used in these previous studies are T cell proliferating assay or cytokine ELISA assay in bulk cultures of peripheral blood mononuclear cell (PBMC) for CD4+ T cell responses, and chromium release assays for CD8+ T cell responses. These techniques suffer from the drawback that they do not enable analysis of single cell responses in the context of unselected cellular background and need prolonged in vitro restimulation. These methods may underestimate the antigen-specific T cell responses in chronic hepatitis B patients..
In contrast, ELISPOT assay and intracellular cytokine staining are exquisitely sensitive and can detect low frequency T cells. They can detect the cytokine release from an activated T cell and can be used for enumeration of single cytokine-secreting cells. These assays are believed to be at least 30-100 times more sensitive than the
chromium release assay, and is efficient and fast because it does not require any in vitro cellular proliferation.
Therefore, in this current project, we applied the ELISPOT assays and intracellular cytokine staining to assess the HBV antigen-specific CD4+ and CD8+ T cell responses in patients infected with HBV. We successfully establish the ELISPOT and intracellular cytokine staining assays. However, only weak or no T cell responses was detected in patients with chronic HBV infection. This implied that T cell hypo-responsiveness may play an important role in the pathogenesis of chronic hepatitis B. Thus, enhancing the HBV-specific T cell responses would be one of the therapeutic targeting for chronic hepatitis B.
Keywor ds: hepatitis B virus, antigen-specific
T cell responses, ELISPOT, intracellular cytokine staining, CD4+, CD8+
二、緣由與目的
Taiwan is a hyperendemic area of hepatitis B virus (HBV) infection. Around 15-20% adults in Taiwan are chronically infected with HBV (1), which is the major cause of chronic hepatitis, liver cirrhosis and hepatocellular carcinoma in Taiwan (2). Both CD4+ T helper (Th) cell and CD8+ cytotoxic T lymphocyte (CTL) play important role in the control of HBV infection.
CD4+ T cells have been shown to be associated with HBV clearance. June et al. (3) demonstrated that activation of CD4+ T lymphocytes by HBcAg/HBeAg is a prerequisite for viral elimination. Spontaneous clearance of HBV DNA and HBeAg is generally preceded by an acute exacerbation of hepatitis activity and accompanied by increased CD4+ T cell proliferation to HBV (3, 4). Further, the HBV core-specific CD4+ Th cell responses appeared to support efficient CTL induction in patients with viral clearance (5). Several lines of evidences showed that the CD8+ CTL responses to HBV-encoded antigens is
remarkably polyclonal and multispecific in most patients with acute hepatitis. The CD8+ CTL activity can lasts for decades following recovery and is thought to keep the HBV under control (6). The HBV virions can be cleared from the blood, by a series of antiviral signals initially delivered by MHC-I-restricted HBsAg-specific CTL (7).
Most of the immunological assays used in these previous studies are T cell proliferating assay or cytokine ELISA assay in bulk cultures of peripheral blood mononuclear cell (PBMC) for CD4+ T cell responses, and chromium release assays for CD8+ T cell responses. These techniques suffer from the drawback that they do not enable analysis of single cell responses in the context of unselected cellular background (8). In contrast, ELISPOT assay and intracellular cytokine staining have several advantages compared with the above traditional immunological assays. The ELISPOT (9-12) assay can detect the cytokine release from an activated T cell and can be used for enumeration of single cytokine-secreting cells. The ELISPOT is thought to be at least 30-100 times more sensitive than the chromium release assay, and is efficient and fast because it does not require any in vitro cellular proliferation (13). Another immunological assay that can detect cytokines at single cell level is intracellular cytokine staining (8, 14). The intracellular cytokine staining is exquisitely sensitive and can detect low frequency T cells, such as HBV antigen-specific T cells in chronic hepatitis B. It also allows rapid analysis of large numbers of cells.
Therefore, in this current project, we will apply the ELISPOT assays and intracellular cytokine staining to assess the HBV antigen-specific CD4+ and CD8+ T cell responses in patients infected with HBV.
三、結果與討論
Set up the systems of ELISPOT assays
used PBMC stimulated with PMA (50 ng/ml) and calcium ionophore A23187 (500 ng/ml) as positive control. The 96-well filtration plates were coated with anti-human IFN-γ antibody and incubated at 4°C overnight. The stimulated PBMCs were added and incubated at 37°C overnight. After culture, the plate was washed and then followed by incubation with biotinylated IFN-γ antibody at 4°C overnight. After washing, 1.25 µg/ml avidin-alkaline phosphatase, were added and incubated for 2 hours at room temperature. After washing, spots were developed by adding 50 µl BCIP/NBT solution and incubated at room temperature for 1 hr. The spots number were counted with NIH image 1.6 after the image captured by a CCD camera.
As shown in figure 1, no spot was detected if no cell was put into the wells. Unstimulated PBMCs generated 6-10 background spots. In contrast, stimulated PBMCs generated numerous IFN-γ positive spots. No cells 1x105 PBMC without PMA 1x105 PBMC with PMA+ionophore Figure 1.
Set up the systems of intr acellular cytokine staining
To set up the condition of intracellular cytokine staining, we used PBMCs stimulated with PMA (50 ng/ml) and calcium ionophore A23187 (500 ng/ml) as positive control.
Golgistop (Pharmingen) was added 6 hours before harvesting the cells from the culture. Cells were stained with PE-conjugated anti-CD8 or -CD4 and FITC-conjugated anti-IFN-γ (Pharmingen). Cells were subjected to intracellular cytokine staining using the Cytofix/Cytoperm kit according to the manufacturer’s instructions (Pharmingen). Analysis was done on a
Becton-Dickenson FACScan with
CELLQuest software.
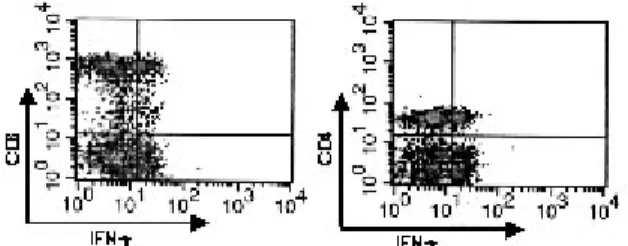
As shown in figure 2, CD8/IFN-γ or CD4/IFN-γ double positive cells can be detected in stimulated PBMCs.
Figure 2. Flow cytometry analysis of IFN-γ secreting CD8+ or CD4+ cells in stimulated PBMCs
HLA typing
A total of 61 patients were screened for the expression of HLA-A2 using RT-PCR or flow cytometry with anti-HLA-A2 MAb. Twenty-eight (51%) of the 55 HBV carriers were HLA-A2(+), while 3 (50%) of the 6 non-HBV carriers were HLA-A2(+).
HBV-specific CD4+ T cell r esponses in patients chr onically infected with HBV
Our initial design was to study both the CD4+ and CD8+ T cell responses. However, we found that core proteins we used can induce similar ELISPOT numbers in both HBV carriers and non-carriers. Because the core protein we used was derived from E coli. Our observation implied that the core protein may contain some lipopolysaccharide, leading to the non-specific T cell activation. Because we had a hard time in getting rid of the lipopolysaccharide, we did not proceed the HBV-specific CD4+ T cell responses after the first 10 cases.
HBV-specific CD8+ T cell r esponses in patients chr onically infected with HBV
We used the ELISPOT assay and intracellular cytokine staining to investigate the HBV-specific CD8+ T cell responses in the 31 HLA-A2(+) patients. The PBMCs were first incubated with HBcAg 18-27 peptides for 3 days before being added to the wells. PMA plus ionophore stimulated PBMCs were used as the positive control in every round of ELISPOT assays. Though there were some spots visible, no
HBV-specific spots can be detected after subtracting the spots numbers of the control (without adding HBV peptides).
The intracellular cytokine staining may be more sensitive than the ELISPOT assay, thus, we also use intracellular cytokine staining to investigate the HBV-specific T cell responses. The PBMCs were incubated with HBcAg 18-27 peptides for 3 days before subjected to flow cytometry. The frequency of HBV-specific CD8+ T cells varied from case to case. We found that 0%-3% of the CD8+ T cells were also IFN-γ(+) (Figure 3). In the non-carrier cases, we can not detected HBV-specific CD8+ T cells. Though the intracellular cytokine staining can detect the HBV-specific CD8+ T cell responses in some patients chronically infected with HBV, the frequency of HBV-specific T cells is still very low.
Figure 3. Flow cytometry analysis of IFN-γ secreting HBV-specific CD8+ cells in patients with chronic hepatitis B. The number in the right upper quadrant indicated the percentage of CD8/IFN-γ double cells in total CD8 T cells
In conclusion, we found that weak or no T cell responses could be detected in chronic hepatitis B patients using ELISPOT and intracellular cytokine staining assays. Our study is consistent with the previous observations using chromium release assay to investigate the T cell responses in chronic hepatitis B patients(15-17). This implied that T cell hypo-responsiveness may play an important role in the pathogenesis of chronic hepatitis B. Thus, enhancing the HBV-specific T cell responses would be one of the therapeutic targeting for chronic hepatitis B. Currently, we are trying to set up the tetramer staining method, a more sensitive method, to investigate the HBV-specific CD8+ T cell responses.
四、計畫成果自評
This project had two specific aims. We successfully achieve the first specific aim: Set up the systems of ELISPOT assays and intracellular cytokine staining. These two systems can also be applied to investigate other antigen-specific T cell response. Unfortunately, we encountered difficulty in the 2nd specific aim: to investigate the HBV-specific CD4+ T cell responses, because of the impurity of the HBV core protein. Endotoxin-free grade protein is needed for a beautiful study of immune responses. We are currently trying solve this issue. We have finished the 3rd specific aim: to investigate the HBV-specific CD8+ T cell responses. However, only weak or no T cell responses could be detected in chronic hepatitis B patients even using ELISPOT or intracellular cytokine assays. This implied that harnessing the immune responses is important in treating chronic hepatitis B patients. In other aspect, more sensitive immunological method, such as tetramer staining, is still needed since only weak HBV-specific CD8+ T cell responses can be detected.
五、參考文獻
1. Chen DS. Hepatitis B virus infection, its sequelae, and prevention in Taiwan. In: Okuda K, Ishak KG, editors. Neoplasms of the liver. Tokyo: Springer-Verlag; 1987. p. 71-80.
2. Chen DS. From hepatitis to hepatoma: lessons from type B viral hepatitis. Science 1993;262(5132):369-70. 3. Jung MC, Diepolder HM, Spengler U,
Wierenga EA, Zachoval R, Hoffmann RM, et al. Activation of a heterogeneous hepatitis B (HB) core and e antigen-specific CD4+ T-cell population during seroconversion to anti-HBe and
anti-HBs in hepatitis B virus infection. J Virol 1995;69(6):3358-68.
4. Tsai SL, Chen PJ, Lai MY, Yang PM, Sung JL, Huang JH, et al. Acute
exacerbations of chronic type B hepatitis are accompanied by increased T cell responses to hepatitis B core and e antigens. Implications for hepatitis B e
antigen seroconversion. J Clin Invest 1992;89(1):87-96.
5. Lohr HF, Krug S, Herr W, Weyer S, Schlaak J, Wolfel T, et al. Quantitative and functional analysis of core-specific T-helper cell and CTL activities in acute and chronic hepatitis B. Liver
1998;18(6):405-13.
6. Rehermann B, Ferrari C, Pasquinelli C, Chisari FV. The hepatitis B virus persists for decades after patients' recovery from acute viral hepatitis despite active maintenance of a cytotoxic T- lymphocyte response. Nat Med
1996;2(10):1104-8.
7. Guidotti LG, Ishikawa T, Hobbs MV, Matzke B, Schreiber R, Chisari FV. Intracellular inactivation of the hepatitis B virus by cytotoxic T lymphocytes. Immunity 1996;4(1):25-36.
8. Maino VC, Picker LJ. Identification of functional subsets by flow cytometry: intracellular detection of cytokine expression. Cytometry
1998;34(5):207-15.
9. Miyahira Y, Murata K, Rodriguez D, Rodriguez JR, Esteban M, Rodrigues MM, et al. Quantification of antigen specific CD8+ T cells using an ELISPOT assay. J Immunol Methods 1995;181(1):45-54.
10. McCutcheon M, Wehner N, Wensky A, Kushner M, Doan S, Hsiao L, et al. A sensitive ELISPOT assay to detect low-frequency human T lymphocytes. J Immunol Methods 1997;210(2):149-66. 11. Schmittel A, Keilholz U, Scheibenbogen
C. Evaluation of the interferon-gamma ELISPOT-assay for quantification of peptide specific T lymphocytes from peripheral blood. J Immunol Methods 1997;210(2):167-74.
12. Power CA, Grand CL, Ismail N, Peters NC, Yurkowski DP, Bretscher PA. A valid ELISPOT assay for enumeration of ex vivo, antigen-specific,
IFNgamma-producing T cells. J Immunol Methods
1999;227(1-2):99-107.
13. Romero P, Cerottini JC, Waanders GA. Novel methods to monitor
antigen-specific cytotoxic T-cell
responses in cancer immunotherapy. Mol Med Today 1998;4(7):305-12.
14. Carter LL, Swain SL. Single cell analyses of cytokine production. Curr Opin Immunol 1997;9(2):177-82.
15. Ferrari C, Penna A, Bertoletti A, Valli A, Antoni AD, Giuberti T, et al. Cellular immune response to hepatitis B virus-encoded antigens in acute and chronic hepatitis B virus infection. J Immunol 1990;145(10):3442-9.
16. Ferrari C, Bertoletti A, Penna A, Cavalli A, Valli A, Missale G, et al.
Identification of immunodominant T cell epitopes of the hepatitis B virus
nucleocapsid antigen. J Clin Invest 1991;88(1):214-22.
17. Jung MC, Spengler U, Schraut W, Hoffmann R, Zachoval R, Eisenburg J, et al. Hepatitis B virus antigen-specific T-cell activation in patients with acute and chronic hepatitis B. J Hepatol 1991;13(3):310-7.