This article was downloaded by: [National Chiao Tung University 國立交通大學] On: 28 April 2014, At: 15:10
Publisher: Routledge
Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
The Service Industries Journal
Publication details, including instructions for authors and subscription information:
http://www.tandfonline.com/loi/fsij20
‘Balanced Scorecard’ as an
operation-level strategic planning tool for service
innovation
Chih-Ming Arthur Luo a , Hung-Fan Chang b & Chi-Hung Su c a
Department of Technology Management , Hsing Kuo University of Management , Tainan , 709 , Taiwan
b
Institute of Management of Technology , National Chiao Tung University , Hsinchu City , Taiwan
c
Department of Information Management , Chihlee Institute of Technology , Taipei County , Taiwan
Published online: 16 May 2011.
To cite this article: Chih-Ming Arthur Luo , Hung-Fan Chang & Chi-Hung Su (2012) ‘Balanced Scorecard’ as an operation-level strategic planning tool for service innovation, The Service Industries Journal, 32:12, 1937-1956, DOI: 10.1080/02642069.2011.574273
To link to this article: http://dx.doi.org/10.1080/02642069.2011.574273
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &
Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
‘Balanced Scorecard’ as an operation-level strategic planning tool for
service innovation
Chih-Ming Arthur Luoa∗, Hung-Fan Changband Chi-Hung Suc
a
Department of Technology Management, Hsing Kuo University of Management, Tainan 709, Taiwan;bInstitute of Management of Technology, National Chiao Tung University, Hsinchu City,
Taiwan;cDepartment of Information Management, Chihlee Institute of Technology, Taipei County, Taiwan
(Received 18 December 2009; final version received 7 February 2011)
This study proposes a model for implementing the balanced scorecard (BSC) as an operation-level strategic planning tool in a medical service department for service innovation. The study involved four major units in a district hospital: the internal medicine ward, surgery ward, gynecology ward, and pediatrics ward. The results indicated that the nursing department not only had its own unique goals and tasks, but also that it was obligated to a comprehensive service system in addition to its specific caring subjects. The study is the first to shed light on the role of department-level strategic planning tool for service innovation. The results also indicated that the operation-level should design its own BSC as a strategic planning for service innovation.
Keywords:service innovation; balanced scorecard; medical service
Introduction
Hospital performance assessment is becoming increasingly important for different stake-holders such as health care providers, decision makers, and purchasers of health care. With hospitals consuming more than half of overall health care budget (McKee, Healy, Edwards, & Harrison, 2002), recent hospital reforms are highlighting a quest for achieving more efficient and effective hospital care. This can be achieved through generalizable, standardized interpretable, and useable information for clinicians or health service managers (Willis, Stoelwinder, & Cameron, 2008).
Conceptualization of hospital functioning is a diverse and complex phenomenon. WHO strategic orientations are encompassed into six interrelated dimensions: clinical effectiveness, safety, patient centeredness, responsive governance, staff orientation, and efficiency (Veillard et al., 2005).
The most important goals in hospital management are to reduce health care costs and provide the best medical care to patients. For this reason, the supervisor of a nursing department (ND) needs a tool to balance the care cost with labor quality, and minimize the gap between the operational and business levels of strategic planning. Moreover, how does a hospital administrator achieve the equally important goals of cost management and labor quality assurance in multiple nursing care units? How can a hospital administra-tor balance the interests of the individual staff members and the hospital? Hospitals are complex service systems. The ND that represents almost 50% of the hospital’s human resources has more interdepartmental contact than any other department in hospital
ISSN 0264-2069 print/ISSN 1743-9507 online # 2012 Taylor & Francis
http://dx.doi.org/10.1080/02642069.2011.574273 http://www.tandfonline.com
∗Corresponding author. Email: [email protected]
The Service Industries Journal
Vol. 32, No. 12, September 2012, 1937 – 1956
administration affairs. The ND is the most productive department in a hospital. Increasing demands have been placed on nursing administrators to be cost-efficient and strategy-effective.
The operation-level strategic planning tool for service innovation strategy proposed in this study is an effective administrative tool that is suitable for both internal management and external reporting of ND service performance.
The advantage that the balanced scorecard (BSC) has over other performance measurement tools is that it is less of a diagnostic control system for highlighting abnormal activities and more of an interactive system for providing signals to the organization about management objectives, stimulating debate, improving quality, and achieving organiz-ational learning. The BSC has evolved to fulfill two control roles within hospital at a stra-tegic and operational level. At the strastra-tegic level, the focus is on trying to determine what the hospital is aiming to achieve, while at the operational level the focus is on trying to determine the salient processes to be monitored. The operation-level strategic planning tool for service innovation strategy proposed in this study is an effective administrative tool that can be used for both internal management and external reporting of ND service performance. This study uses the four major perspectives of the BSC to establish specific measurable indicators and innovation strategy within the ND. Therefore, this study proposes a model designed for implementing a BSC as an operation-level strategic planning for service innovation.
This study uses the four major perspectives of the BSC to establish specific measurable indicators and innovation strategies within the ND. This study proposes a model designed for implementing a BSC as an operation-level strategic planning for service innovation.
The remainder of the article is organized as follows: the second section presents the literature review. The third section presents the methodology used in the requirement analysis and the planning and design of the research framework for implementing the BSC as an operation-level strategic planning tool for service innovation. In the fourth section, we present the results. The fifth section discusses the presented results. Con-clusions, limitations, and suggestions for future work are all reported in the last section.
The next section details the literature review of service innovation and BSC.
Literature review
Due to radical changes in the medical services industry in Taiwan (i.e. the formation of a competitive open-market environment), hospital performance management needs new keys and directions, and its development should be strategy-oriented. Williams, D’Souza, Rosenfeldt, and Kassaee (1995) investigated the relationship between manufac-turing strategy, business strategy, and firm performance in a mature industry. His results show a significant relationship between a firm’s business strategy and manufacturing strat-egy. Though many companies must use the resources and energy for continuous inno-vation, existing literature does not provide a clear idea of how to achieve this.
Ittner and Larcke (1998) suggested that performance management was a systematic management process for setting up the objectives of the organization and individuals and a methodology for reaching agreement on the objectives. According to this; effective employee management methods are to be used to increase the possibility of achieving those objectives. Gruca and Nath (1994) held that hospital performance conceptually has several perspectives, with no single indicator providing a complete overall view. Therefore, this study applies the four-dimensional BSC to evaluate ND. Moreover, it should be noted that if there are connections between the department and the strategic
1938 C.A. Luo et al.
objectives of the hospital it is more effective to carry out a performance evaluation of the department that relates to the strategy objectives of the hospital. The BSC provided an opportunity to capture indicators in four aspects of hospital performance: (i) labeled learn-ing and growth (staff orientation and satisfaction), (ii) internal processes (clinical out-comes and management of health services), (iii) customer (patient) satisfaction, and (iv) financial efficiency/performance. BSC serves as a dashboard for meaningful decision making and quality improvement and relates results to external references while promot-ing internal comparisons overtime (Veillard et al., 2005).
Kaplan and Norton (1993) emphasized that the BSC should be used to drive the measurement of future performance, and make up for the deficiencies of financial measures, which have traditionally been the only performance assessment measure. The BSC not only emphasizes financial performance. It also indicates the importance of non-financial performance for the evaluation of enterprise performance. Meliones, Ballard, Liekweg, and Burton (2001) argued that the importance of the BSC lay in the establishment of a performance evaluation system, and that it might affect different strat-egy positions and tasks in various organizations. There are many studies on the application of the BSC on different organizations. Phillips (2007) applied the BSC to discuss strategic control in hotel study. Afghanistan has adopted the BSC as a tool to measure and manage performance in delivery of a Basic Package of Health Services (Hansen et al., 2008). Wu, Tsai, Shih, and Fu (2010) applied the BSC to evaluate government performance. BSC is also utilized as a framework to develop evaluation indicators for banking performance (Davis & Albright, 2004). Lee, Chen, and Chang (2008) proposed applied BSC for eval-uating an information technology department in the Taiwan manufacturing industry. Result of study to shown information technology departments in the Taiwan manufactur-ing industry regardmanufactur-ing strategies for improvmanufactur-ing department performance. There have been numerous studies in the literature dealing with organization strategic, finance or operation performance on BSC. Thakkar, Deshmukh, Gupta, and Shankar (2007) presented in con-sidering the basis for integrating organization’s strategic intent issues, the first questions that arise concerns the identification of performance measures and at large development of BSC. Although present work demonstrates the use of an innovative approach to the development of performance measurement system, no clear direction has emerged to suggest how such considerations translate into service innovation practice. As was men-tioned above, there has been relatively little research conducted on ND’s strategic plan-ning of operation-level. The study we present in the present paper is an attempt to supplement the finding of these earlier studies. It is similar to the previous studies dis-cussed above, in that the focus is on applied of the four major perspectives of the BSC. It differs from previous studies, however, in the way understanding of how strategic plan-ning drives service innovation in ND.
The most effective motivation for BSC performance evaluation is the link between assessment and remuneration. However, previous researchers have not related the advan-tages of BSC performance evaluation to strategic planning for departments unit. This study proposes that the most important function of the BSC is to convert strategy into action, and establish an overall labor evaluation system. The ND is the largest human resource unit in a hospital. Therefore, this study proposes a model designed for implement-ing a BSC as an operation-level strategic plannimplement-ing tool in this department. This study uses the BSC to develop a management system that can translate a hospital’s innovation strat-egy into an actual action plan in the ND.
The next section details the theoretical background of our research, construct develop-ment, and result.
The Service Industries Journal 1939
Methodology
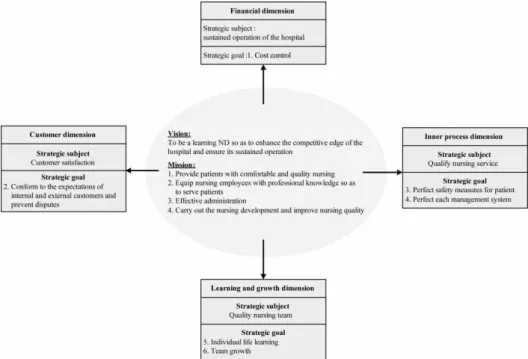
Four hospital wards in St Joseph’s hospital in Taiwan were investigated: internal medicine, surgery, gynecology, and pediatrics. Seven experts helped design the strategic planning tool in the ND. Six experts were from the ND, including the director of nursing, one super-visor, and four head nurses. The other participant was the director of the administration department. This study proposes that the most important function of the BSC is to convert strategy into action, and establish an overall labor evaluation system. The convert strategy of BSC into action must through strategy maps. The strategy map made director of nursing, supervisor, and head nurses speed up their decision on oper-ation-level strategic planning. The cause-and-effect logic to construct the strategy map helped them balance the four major perspectives of the BSC for the ND. A BSC strategy map of performance indicators was created based on the professional goals of the nurses’ mission (see Figure 1).
The paper in Kaplan and Norton (1993) provide extensive discussions of the applications of the BSC measures that drive performance. And, Kaplan and Norton offered a sounder theoretical basis for strategic management. Therefore, this study applied the four major perspectives of the BSC based on Kaplan and Norton (1993). The seven experts identified four dimensions. In order of priority from greatest to least, these include financial, customer, inner process, and learning and growth dimensions. The following discussion presents the strategy and tactical goals for each of these four dimensions.
First, the strategy and tactical goals of the financial dimension were cost control and continuity of hospital management (item 1, Figure 1). Second, the strategy and tactical goals of the customer dimension were customer satisfaction and meeting the expectations of both internal and external customers (items 2 and 3, Figure 1). Third, the strategy of the inner process dimension was to provide excellent service quality, while its tactical goal
Figure 1. Translating the nursing department strategy into action.
1940 C.A. Luo et al.
was completely implementing patient safety standards and perfecting every aspect of the regulations and guidelines in the administrative system (items 4 and 5, Figure 1). Fourth, the strategy of the learning and growth dimension was to certify nursing care team, while its tactical goal was to foster individual life learning and group growth (item 6, Figure 1).
The construction of these four dimensions was, in a way, from bottom to top (e.g. learning and growth dimension, inner process dimension, customer dimension, financial dimension), while the determination of the six strategies and tactical goals occurred in the opposite direction, starting from first dimension (financial) (see Figure 1).
The four dimensions of the BSC were developed according to vision of the ND that was to be a learning ND, to enhance the competitive edge of the hospital, and to ensure its sustained operation. The nursing mission statement included the following goals: (1) providing patients with comfortable and quality nursing, (2) equipping nursing employees with professional knowledge to serve patients well, (3) having an effective administration, and (4) carrying out nursing development and improving nursing quality (see Figure 1).
The mission-expectations map was derived and translated in a sequence of steps from nursing mission statement, core value, vision, and BSC, through to strategy (see Figure 2). The performance management model was based on the following six questions:
Question 1: Does the hospital have an accurate model that for assessing the perform-ance of its administrative system? What is the standard operating procedure? Question 2: How well does it work for the objective management system currently
used by the administrative system in the ND?
Question 3: What are the key performance indicators for evaluating the ND? Question 4: Should any indicator be added to the four dimensions of the BSC? Question 5: What are the benefits of applying the BSC for achieving the vision and
objectives of the ND? What are the potential difficulties? Are there any challenges to improving BSC evaluation?
Question 6: The hospital has not yet implemented the BSC in the ND. If implemented, how would BSC evaluation apply to, or affect, the financial performance of the hospital?
Three main methods have been used in the health field: the Delphi, the Nominal Group Technique, and the Consensus Development Conference. The comparative advantage of the Delphi technique over other strategies is the enhanced opportunity for all participants to contribute greater number of ideas than other group processes, minimizing domination of the process by more confident or outspoken individuals, the ease of interpreting the results, and minimal resource requirements with efficient use of time (Murphy, Black, & Lamping, 1998).
This study analyzes data using the Delphi method that was designed using a theoretical framework based on Yin’s (1994) designing cases. The main indicators and questionnaires were discussed and created in two meetings in the ND. Two general meetings and four ward meetings were held to identify the indicators. Table 1 shows the results of weighing, discussing, reweighing, and reaching agreement on these indicators.
This study appointed seven experts, according to the roles as decision makers within the hospital, to a Delphi team. These seven experts were members of the Steering Com-mittee for the indications of each measure and driver in ward unit and the ND with BSC. This study performed the Delphi method in two rounds. In the first Delphi round, each expert evaluated each of the 23 outcome measures and 28 performance drivers from the four dimensions of the BSC. Each expert could indicate more than one choice The Service Industries Journal 1941
among the list of answers. Anyone uncertain about the final decision had the option of an open field for the answers. In the second round, the experts considered the same outcome measures and performance drivers, but informed of the other experts’ answers for each outcome measured and the performance drivers from the first poll. If they then changed previous judgments, they included an explanation for the changes. The process was terminated after the second round.
The two-stage process identified 13 indicators of each measure and driver, and the scoring of the each indicator was set according to four criteria: that strategy-related, Figure 2. The map of mission-expectation translation.
1942 C.A. Luo et al.
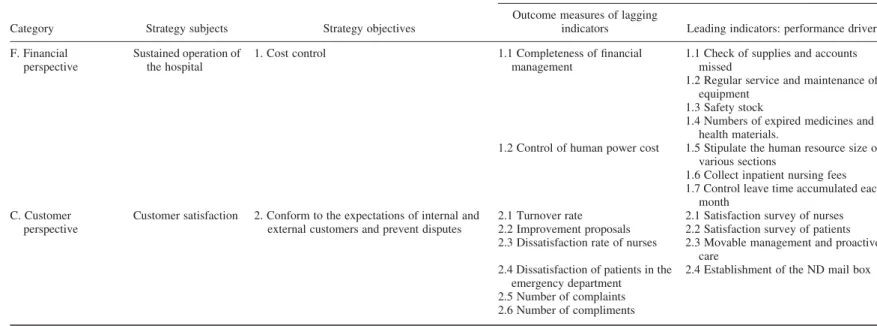
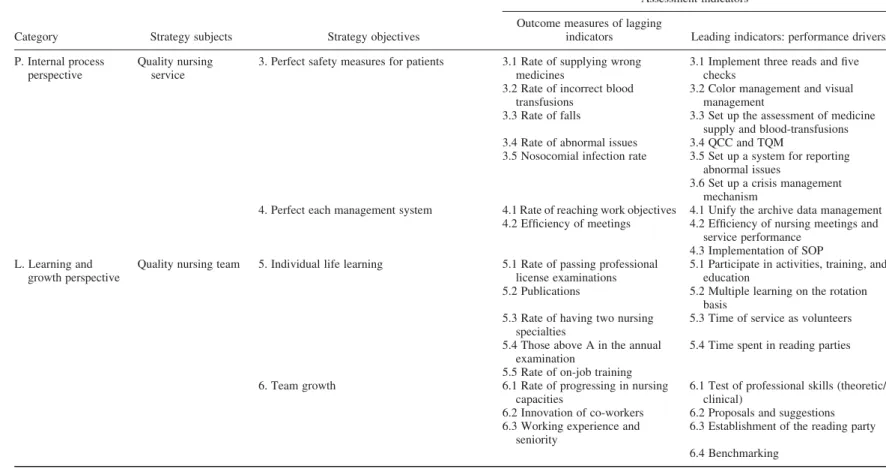
Table 1. Lagging and Leading indicators in the ND BSC.
Category Strategy subjects Strategy objectives
Assessment indicators Outcome measures of lagging
indicators Leading indicators: performance drivers F. Financial
perspective
Sustained operation of the hospital
1. Cost control 1.1 Completeness of financial management
1.1 Check of supplies and accounts missed
1.2 Regular service and maintenance of equipment
1.3 Safety stock
1.4 Numbers of expired medicines and health materials.
1.2 Control of human power cost 1.5 Stipulate the human resource size of various sections
1.6 Collect inpatient nursing fees 1.7 Control leave time accumulated each
month C. Customer
perspective
Customer satisfaction 2. Conform to the expectations of internal and external customers and prevent disputes
2.1 Turnover rate 2.1 Satisfaction survey of nurses 2.2 Improvement proposals 2.2 Satisfaction survey of patients 2.3 Dissatisfaction rate of nurses 2.3 Movable management and proactive
care 2.4 Dissatisfaction of patients in the
emergency department
2.4 Establishment of the ND mail box
2.5 Number of complaints 2.6 Number of compliments (Continued ) The Service Industr ies Journal 1943
Table 1. Continued.
Category Strategy subjects Strategy objectives
Assessment indicators Outcome measures of lagging
indicators Leading indicators: performance drivers P. Internal process
perspective
Quality nursing service
3. Perfect safety measures for patients 3.1 Rate of supplying wrong medicines
3.1 Implement three reads and five checks
3.2 Rate of incorrect blood transfusions
3.2 Color management and visual management
3.3 Rate of falls 3.3 Set up the assessment of medicine supply and blood-transfusions 3.4 Rate of abnormal issues 3.4 QCC and TQM
3.5 Nosocomial infection rate 3.5 Set up a system for reporting abnormal issues
3.6 Set up a crisis management mechanism
4. Perfect each management system 4.1 Rate of reaching work objectives 4.1 Unify the archive data management 4.2 Efficiency of meetings 4.2 Efficiency of nursing meetings and
service performance 4.3 Implementation of SOP L. Learning and
growth perspective
Quality nursing team 5. Individual life learning 5.1 Rate of passing professional license examinations
5.1 Participate in activities, training, and education
5.2 Publications 5.2 Multiple learning on the rotation basis
5.3 Rate of having two nursing specialties
5.3 Time of service as volunteers
5.4 Those above A in the annual examination
5.4 Time spent in reading parties
5.5 Rate of on-job training 6. Team growth 6.1 Rate of progressing in nursing
capacities
6.1 Test of professional skills (theoretic/ clinical)
6.2 Innovation of co-workers 6.2 Proposals and suggestions 6.3 Working experience and
seniority
6.3 Establishment of the reading party
6.4 Benchmarking 1944 C.A. Luo et al.
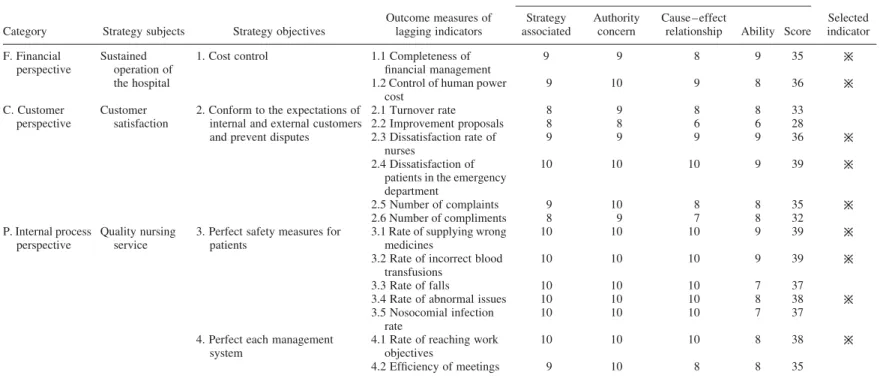
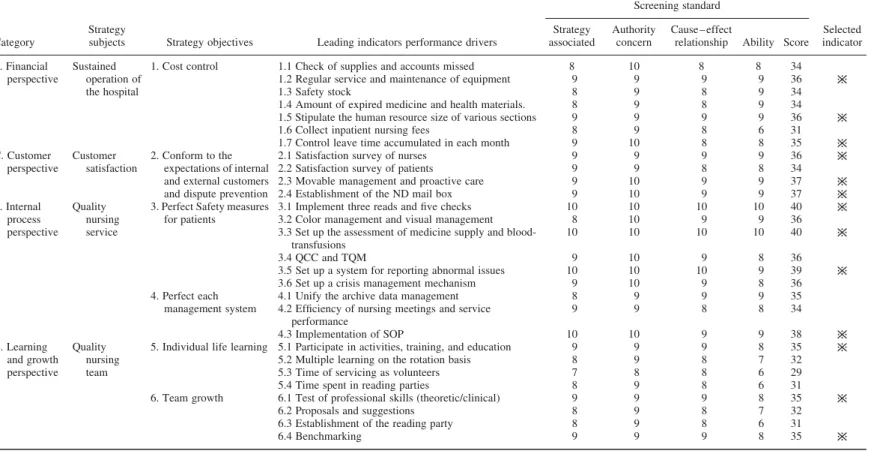
authority-related, and cause – effect-related. The scores for a particular indicator were calculated and selected when the mean was greater than the average. This process selected 13 of the 23 outcome measures (see Table 2), and 13 of the 28 performance drivers (see Table 3) to match the objectives of the nursing unit and the department.
This process resolved the problems of ill-defined department objectives and ambiguity in department strategy. The implementation steps for planning the BSC in the ND adopted the framework proposed by Kaplan and Norton (2001). The process started from the vision and strategy of the top management level of the hospital and the mission of the ND. Then, through interviews and communication with the ND leaders (director, supervisor, and nursing chief), related data collection, each perspective of the BSC was created for the department.
Planned implementation steps of the BSC for the ND
A meeting was held after the interview and communication with the director of the ND to brief the leaders (supervisor and head nurse) on BSC policy and methods, explain the intended future direction for implementation, review the collection of related written data, and identify possible applications for this data. The experts then reached consensus through open-ended questionnaires, interviews, and discussions with each other. This led to the creation of a BSC for the ND. This study adopted the Delphi method to reach an agreement regarding the BSC of the ND through anonymous written discussions, staff experience, expert suggestions, and meetings.
Steps of selecting experts and implementation
As was pointed out at the beginning, we started this research with the nursing mission and goals on the BSC. For the strategic planning of operation-level in the BSC, and the purpose of this study discussed service innovation issues in the ND. Therefore, the experts have to be equipped for knowledge of ND on the four major perspectives of the BSC. The primary criterion for selecting subjects was that they vary in the management echelon/department at which they in hospital of Taiwan. To ensure some homogeneity of expert background, all subjects were selected from the managers at a regional teaching hospital in Taiwan. This study was reviewed and approved by a panel of specialists consisting of head nurses, the nursing director, and supervisors from the internal medicine, surgery, gyneco-logy, and pediatrics departments. Expert sample was drawn from a list of all ND managers who have been making in the medical industry management for seven or more years. The seven participants involved in this study can be further categorized by their working experience, one being classified as middle manager (head nurses) and six as senior managers (the director of nursing and supervisor) according to work level by a regional teaching hospital.
The first round of meetings focused on the research process and subjects. An open-ended question format was adopted for the questionnaire, and respondents included directors, supervisors, and head nurses of the ND, for seven experts. All of the questionnaires distributed to these experts were completed and returned. This study sorted the answers, analyzed the results, and compiled the ideas with some minor modifications. Based on this pilot study, the results of the first round, this study constructed the second questionnaire. The second round focused on the mission, vision, and strategic objectives of each perspec-tive as a basis for data collection. This produced a draft of the perspecperspec-tives, with 23 defined result measurements and 28 performance drivers. The second questionnaire was created by The Service Industries Journal 1945
Table 2. Screening the lagging indicators in the ND BSC.
Category Strategy subjects Strategy objectives
Outcome measures of lagging indicators Screening standard Selected indicator Strategy associated Authority concern Cause – effect
relationship Ability Score F. Financial
perspective
Sustained operation of the hospital
1. Cost control 1.1 Completeness of financial management
9 9 8 9 35
1.2 Control of human power cost 9 10 9 8 36 C. Customer perspective Customer satisfaction
2. Conform to the expectations of internal and external customers and prevent disputes
2.1 Turnover rate 8 9 8 8 33 2.2 Improvement proposals 8 8 6 6 28 2.3 Dissatisfaction rate of nurses 9 9 9 9 36 2.4 Dissatisfaction of patients in the emergency department 10 10 10 9 39 2.5 Number of complaints 9 10 8 8 35 2.6 Number of compliments 8 9 7 8 32 P. Internal process perspective Quality nursing service
3. Perfect safety measures for patients
3.1 Rate of supplying wrong medicines
10 10 10 9 39
3.2 Rate of incorrect blood transfusions
10 10 10 9 39
3.3 Rate of falls 10 10 10 7 37
3.4 Rate of abnormal issues 10 10 10 8 38
3.5 Nosocomial infection rate
10 10 10 7 37
4. Perfect each management system
4.1 Rate of reaching work objectives 10 10 10 8 38 4.2 Efficiency of meetings 9 10 8 8 35 1946 C.A. Luo et al.
L. Learning and growth perspective
Quality nursing team
5. Individual life learning 5.1 Rate of passing professional license examinations
9 9 9 9 36
5.2 Publications 9 10 10 7 36
5.3 Rate of having two nursing specialties
9 9 6 7 33
5.4 Those above A in the annual examination
8 9 8 8 33
5.5 Rate of on-job training 10 9 10 8 37
6. Team growth 6.1 Rate of progressing in nursing capacities
9 10 10 8 37
6.2 Innovation of co-workers
9 9 8 7 33
6.3 Working experience and seniority 9 8 8 7 32 The Service Industr ies Journal 1947
Table 3. Screening the leading indicators in the ND BSC.
Category
Strategy
subjects Strategy objectives Leading indicators performance drivers
Screening standard Selected indicator Strategy associated Authority concern Cause – effect
relationship Ability Score F. Financial
perspective
Sustained operation of the hospital
1. Cost control 1.1 Check of supplies and accounts missed 8 10 8 8 34
1.2 Regular service and maintenance of equipment 9 9 9 9 36
1.3 Safety stock 8 9 8 9 34
1.4 Amount of expired medicine and health materials. 8 9 8 9 34 1.5 Stipulate the human resource size of various sections 9 9 9 9 36
1.6 Collect inpatient nursing fees 8 9 8 6 31
1.7 Control leave time accumulated in each month 9 10 8 8 35 C. Customer perspective Customer satisfaction 2. Conform to the expectations of internal and external customers and dispute prevention
2.1 Satisfaction survey of nurses 9 9 9 9 36
2.2 Satisfaction survey of patients 9 9 8 8 34
2.3 Movable management and proactive care 9 10 9 9 37
2.4 Establishment of the ND mail box 9 10 9 9 37
P. Internal process perspective Quality nursing service
3. Perfect Safety measures for patients
3.1 Implement three reads and five checks 10 10 10 10 40
3.2 Color management and visual management 8 10 9 9 36
3.3 Set up the assessment of medicine supply and blood-transfusions
10 10 10 10 40
3.4 QCC and TQM 9 10 9 8 36
3.5 Set up a system for reporting abnormal issues 10 10 10 9 39
3.6 Set up a crisis management mechanism 9 10 9 8 36
4. Perfect each management system
4.1 Unify the archive data management 8 9 9 9 35
4.2 Efficiency of nursing meetings and service performance 9 9 8 8 34 4.3 Implementation of SOP 10 10 9 9 38 L. Learning and growth perspective Quality nursing team
5. Individual life learning 5.1 Participate in activities, training, and education 9 9 9 8 35
5.2 Multiple learning on the rotation basis 8 9 8 7 32
5.3 Time of servicing as volunteers 7 8 8 6 29
5.4 Time spent in reading parties 8 9 8 6 31
6. Team growth 6.1 Test of professional skills (theoretic/clinical) 9 9 9 8 35
6.2 Proposals and suggestions 8 9 8 7 32
6.3 Establishment of the reading party 8 9 8 6 31
6.4 Benchmarking 9 9 9 8 35 1948 C.A. Luo et al.
sorting the opinions of the first questionnaire. This second draft was screened by the director of the ND, and assessed by the department BSC that served as the assessment indicator.
After the assessment scores were collected, the averages of each perspective were calculated and compiled. The indicators were assessed by dividing the total scores of perspectives by the number of options for each perspective. For example, the total score of 334 was divided by 9, resulting in an average of 37. Hence, any indicator above 37 would be selected. When an average indicator could not be selected, the department director would hold a meeting to select the final assessment indicator.
Results
Definition of indicators in the ND BSC
The ND carried assessed the 23 initial achievements (lagging indicators) and selected 13 indicators for the department’s BSC using the Delphi method. Ward units screened 13 assessment indicators for the ward BSC based on the 28 performance drivers (leading indicators) (see Table 1). These items, including descriptions of indicators, formula calculations, expected objectives, assessment frequency, and data resources, were the basis for carrying out the performance evaluation with the BSC.
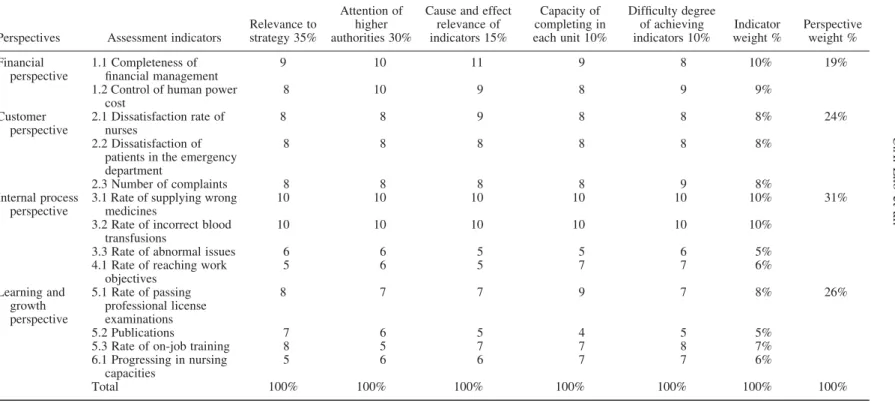
Weights of assessment indicators for each perspective
To help each ward realize the importance of each perspective, a weight score was added to each assessment pointer. The weights of indicators and perspectives in the ND were determined using the Delphi method, and the BSC was constructed to fit the needs of the hospital. The weights of the perspectives were as follows: financial perspective 19%, customer perspective 24%, learning and growth perspective 26%, and internal process perspective 31% (see Table 4).
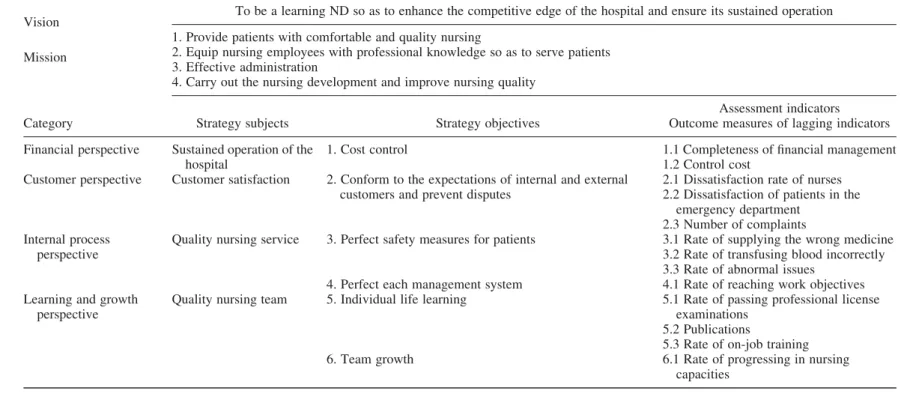
ND BSC
The BSC was derived from the vision and strategy of the ND. The BSC was first screened by the department chiefs using the Delphi method, and then constructed through discus-sions (see Table 5).
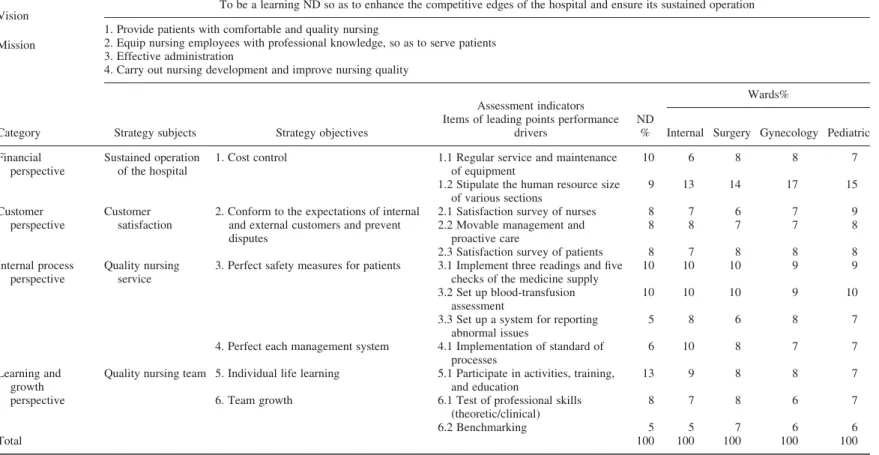
Ward unit BSC
Based on the BSC developed by the ND, promotion included application in four ward units (internal medicine, surgery, gynecology, and pediatrics), as Table 6 shows. To promote the ward BSC effectively, a performance assessment table for each ward was set up to track implementation progress, and served as the management’s assessment tool.
Discussion
The findings of this study suggest that in the medical service industry, the BSC, as a department-level strategic planning tool for service innovation strategy, can be practically implemented and provide adequate results that link excellence strategies between organ-ization and departments. This finding agrees with Williams’s et al. (1995) showed a sig-nificant relationship between the business strategy and manufacturing strategy of a firm. The Service Industries Journal 1949
Table 4. Weights of each perspective and outcome assessment indicators in the ND.
Perspectives Assessment indicators
Relevance to strategy 35%
Attention of higher authorities 30%
Cause and effect relevance of indicators 15% Capacity of completing in each unit 10% Difficulty degree of achieving indicators 10% Indicator weight % Perspective weight % Financial perspective 1.1 Completeness of financial management 9 10 11 9 8 10% 19%
1.2 Control of human power cost 8 10 9 8 9 9% Customer perspective 2.1 Dissatisfaction rate of nurses 8 8 9 8 8 8% 24% 2.2 Dissatisfaction of patients in the emergency department
8 8 8 8 8 8%
2.3 Number of complaints 8 8 8 8 9 8%
Internal process perspective
3.1 Rate of supplying wrong medicines
10 10 10 10 10 10% 31%
3.2 Rate of incorrect blood transfusions
10 10 10 10 10 10%
3.3 Rate of abnormal issues 6 6 5 5 6 5%
4.1 Rate of reaching work objectives 5 6 5 7 7 6% Learning and growth perspective 5.1 Rate of passing professional license examinations 8 7 7 9 7 8% 26% 5.2 Publications 7 6 5 4 5 5%
5.3 Rate of on-job training 8 5 7 7 8 7%
6.1 Progressing in nursing capacities 5 6 6 7 7 6% Total 100% 100% 100% 100% 100% 100% 100% 1950 C.A. Luo et al.
Table 5. ND BSC.
Vision To be a learning ND so as to enhance the competitive edge of the hospital and ensure its sustained operation Mission
1. Provide patients with comfortable and quality nursing
2. Equip nursing employees with professional knowledge so as to serve patients 3. Effective administration
4. Carry out the nursing development and improve nursing quality
Category Strategy subjects Strategy objectives
Assessment indicators Outcome measures of lagging indicators Financial perspective Sustained operation of the
hospital
1. Cost control 1.1 Completeness of financial management
1.2 Control cost Customer perspective Customer satisfaction 2. Conform to the expectations of internal and external
customers and prevent disputes
2.1 Dissatisfaction rate of nurses 2.2 Dissatisfaction of patients in the
emergency department 2.3 Number of complaints Internal process
perspective
Quality nursing service 3. Perfect safety measures for patients 3.1 Rate of supplying the wrong medicine 3.2 Rate of transfusing blood incorrectly 3.3 Rate of abnormal issues
4. Perfect each management system 4.1 Rate of reaching work objectives Learning and growth
perspective
Quality nursing team 5. Individual life learning 5.1 Rate of passing professional license
examinations 5.2 Publications
5.3 Rate of on-job training
6. Team growth 6.1 Rate of progressing in nursing
capacities The Service Industr ies Journal 1951
Table 6. ND and Ward BSC.
Vision To be a learning ND so as to enhance the competitive edges of the hospital and ensure its sustained operation
Mission
1. Provide patients with comfortable and quality nursing
2. Equip nursing employees with professional knowledge, so as to serve patients 3. Effective administration
4. Carry out nursing development and improve nursing quality
Category Strategy subjects Strategy objectives
Assessment indicators
ND %
Wards% Items of leading points performance
drivers Internal Surgery Gynecology Pediatric Financial
perspective
Sustained operation of the hospital
1. Cost control 1.1 Regular service and maintenance of equipment
10 6 8 8 7
1.2 Stipulate the human resource size of various sections 9 13 14 17 15 Customer perspective Customer satisfaction
2. Conform to the expectations of internal and external customers and prevent disputes
2.1 Satisfaction survey of nurses 8 7 6 7 9
2.2 Movable management and proactive care
8 8 7 7 8
2.3 Satisfaction survey of patients 8 7 8 8 8
Internal process perspective
Quality nursing service
3. Perfect safety measures for patients 3.1 Implement three readings and five checks of the medicine supply
10 10 10 9 9
3.2 Set up blood-transfusion assessment
10 10 10 9 10
3.3 Set up a system for reporting abnormal issues
5 8 6 8 7
4. Perfect each management system 4.1 Implementation of standard of processes
6 10 8 7 7
Learning and growth perspective
Quality nursing team 5. Individual life learning 5.1 Participate in activities, training, and education
13 9 8 8 7
6. Team growth 6.1 Test of professional skills (theoretic/clinical) 8 7 8 6 7 6.2 Benchmarking 5 5 7 6 6 Total 100 100 100 100 100 1952 C.A. Luo et al.
This study proposes a framework linking the strategic planning for service innovation between operation and business levels.
This study shows that several indicators had been already implemented in the ND for a long time, and had become standard assessment requirements in the hospital. Some indicators were assessed regularly, but were not sorted and analyzed for management. All of these indicators were included as performance management indicators in the BSC. The BSC was established after the department directors reached agreement. Among the 13 assessment indicators on the BSC, the ND had only overlooked five (control of leave time accumulated, dissatisfaction rate of nurses, dissatisfaction rate of inpatients, rate of achieving work objectives, and publications). In the business model, the four perspectives would operate in a logical sequence, or priority order, of learning and growth, inner process, customer and service, and finally, financial perspectives. These four main streams are the basis of the BSC. Moreover, each stream can be assigned more weight to match the indicator system. As for the weight percentage of the four perspectives in the BSC for the ND, priority was given to the safety and satisfaction of patients, since the ND’s customers are patients. After the assessment, the rankings of the four dimensions were consistent with the mission priority of the case hospital (see Table 4).
Four perspectives of the BSC for the case department Financial perspective
Since the financial objective does not clearly calculate or reflect nursing fees, this study had to be implemented under the limitation that it could be completed or controlled by the ND. The financial perspective focuses on the prevention of abnormal issues and controlling human resource costs. Avoiding increased financial expenditures is one of the assessment indicators. The Catholic hospital in this case study operates with charity in mind. For example, the hospice ward and detoxification units account for a significant portion of the hospital’s operational budget and human resources. This mission-oriented factor complicated the assessment of the financial indicator. Thus, this factor became an important indicator in the financial dimension, and required more attention and control.
The different evaluations provided by specialty members versus ward staff suggest that, on the aspects of financial dimension, the ND was more concerned about the regular service and maintenance of equipment (10% vs. 6 – 8% for ND and the ward, respectively), while the wards paid more attention to downsizing human resources in various sections (9% vs. 13 – 15% for the ND and the ward, respectively). This implies that the ND was more concerned about patient safety, and was reluctant to cut the maintenance cost of medical equipments (see Table 6).
Although profit is not a major concern for the case hospital investigated in this study, the financial dimension needs to be addressed further from a management point of view. The current results do not show any profit indicator in the end. Since this BSC was devel-oped for the ND, and the focus of the department may be limited to the short term. The resulting health care business model seemed to lack long-term financial indicators, such as new client visiting rate, non-insurance covered nursing services, ward bed occupation rate, operation room use rate, and new patient admission rate. That might assure the hospital a better long-term financial status. However, it would be better if a higher-level hospital financial controller was involved.
The Service Industries Journal 1953
Customer perspective
Customer satisfaction is the top performance assessment indicator of almost every organ-ization. In the past, the ND of the hospital emphasized patient satisfaction, and assessed its performance twice a year. For nurse satisfaction, however, a survey was taken only once a year. This study’s approach is to take patient’s dissatisfaction issues and comments into consideration to improve understanding between nurses and patients. Moreover, the dissa-tisfaction of nurses was an assessment indicator of internal customer sadissa-tisfaction. On the other hand, the dissatisfaction rate of inpatients and complaints represented the satisfaction of external customers, and that served as the key indicator for improving nursing quality and achieving customer satisfaction in the ND. Since the ND and other wards gave similar weights to each indicator in the customer dimension, consistency should help the hospital management to earn customer loyalty (see Table 6, Figure 1). This, in turn, would further increase the revisiting rate and create financial income.
Internal process perspective
This study takes the key facts that have the maximum influence on the customer satisfaction, the prerequisite of service from the perspective of customers, and relates them to the operation flow design of the organization. Hence, in determining the weights of the four perspective of the BSC, the ND used the internal process as the key implementation indicator. However, for the indicator ‘Set up a system for reporting abnormal issues’ (Table 6, 3.3), the scores for every evaluator were low (5 – 8) compared to the other two indicators (9 – 10, Table 6, 3.1 and 3.2). The expert team members from the ND gave an especially low score of 5 compared to those from other wards (6 – 8). The ND actually thought that this indicator was in good running condition, and did not deserve additional attention.
Learning and growth perspective
This study shows that among the disadvantages and challenges faced by the ND, personnel growth was the most pressing indicator. This indicator includes ‘participation in activities, training, and education’ for the nursing team. The team of experts gave an extraordinarily high score of 13 compared to the 7 – 9 given by the head nurses of wards (see Table 6, 5.1). The difference between the ND and ward results might come from the differences in indi-vidual life learning. For the case hospital, the specialty team might regard ‘Rate of passing professional license examinations’ and ‘Publications’ as individual life learning and important for the Learning and Growth Perspective, while the head nurses from the wards might hold different views. It is possible that the incentive for advancing learning and growth was not strong enough in this hospital. Note that in the hospitals of other systems, such as Veterans Affair hospitals, individual life learning might be encouraged and supported by the hospital in other ways, such as offering employees study leave with pay. Thus, if the hospital provided more resources and support for individual learning, individual learning, and group growth would be in a better balance.
The vision of this study was to be a learning ND so as to enhance the competitive edge of the hospital and ensure its sustained operation. The above-mentioned, we discussed measures with strategic intent in ‘four perspectives of the BSC for the case department’ on the section of discussion. We will begin our discussion by reviewing research findings, and then turn to strategic intent. Finally, the results drawn above should be interpreted in relation to four major perspectives of the BSC in ND.
1954 C.A. Luo et al.
Conclusions
The research proved that although the case hospital did not carry out the BSC, the ND did however design a BSC independently to improve operation-level strategic planning tool for service innovation efficiency, as shown in Table 5. In the BSC developed by the ND, the four perspectives, ranked by importance, were internal process, learning and growth, customer, and financial. This is consistent with the mission goal of the Catholic hospital in this study. Among these four perspectives and the 13 indicators, the customer perspective indicators were given the most consistent weight from the ND and the wards. The financial indicators might need further investigation to maintain the financial balance in the end. As for internal process indicators, the patient safety culture was already well established at the hospital, and did not need additional effort or attention. Under a reasonable financial structure, the resources for individual and group learning should be optimized to improve the learning climate.
The results of this study hold several important management implications. The case study reported in this paper demonstrates that the BSC can be implemented as an oper-ation-level strategic planning tool for service innovation. This study indicates that it might be fruitful to investigate the use of the BSC as an operation-level strategic planning tool for service innovation further. These are not only important for understanding the sources and drivers of strategic planning in ND, but also for the accurate measurement of service innovation. This study will offer ND and hospital 4 contributions: (1) a com-munication tool, (2) a strategic planning tool, (3) a total performance measurement system, and (4) a implementing administration innovation system.
Limitations and suggestions for further study
This study demonstrates the practicality of the proposed methodology using a case study. This study acknowledges that this study is exploratory in nature, and that there are problems with the research scope and limitations on the wards of the NDs involved. In addition, methodological problems in the research design limit our interpretations. Since this study only covers four wards of ND, the results cannot be generalized to other areas. This case study focuses on four ND wards: internal, surgery, gynecology, and pediatrics, but does not discuss other ND wards, such as intensive care unit and the emergency ward. In the future, we suggested adapt to results of this study with cooperation hospital of apply BSC.
Since the study involved only covers four wards of ND, the results cannot be general-ized on health sector in other cases. It is not within the scope of this paper to provide an extended discussion of the ongoing debates. Therefore, future research is obviously required, but this is an exciting first step. As area of future research that should be considered is how BSC has helped health sector in other cases. In the future, we intend to continue pursuing this line of investigation in a series of studies, include: (1) how will you ensure an evolutionary aspect of BSC in other health sector? (2) What is review frequency? (3) On what basis obsolete measures may be dropped or new may be included in future. While this study has its limitations, it is hoped that it can serve as a basis for further study in other health sector.
References
Davis, S., & Albright, T. (2004). An investigation of the effect of the balanced scorecard implemen-tation on financial performance. Management Accounting Research, 15(2), 135–153.
The Service Industries Journal 1955
Gruca, T.S., & Nath, D. (1994). The impact of marketing on hospital performance. Journal of Hospital Marking, 2, 316–351.
Hansen, P.M., Peters, D.H., Niayesh, H., Singh, L.P., Dwievedi, V., & Burnham, G. (2008). Measuring and managing progress in the establishment of basic health services: The Afghanistan Health Sector Balanced Scorecard. International Journal of Health Planning and Management, 23, 107–117.
Ittner, C.D., & Larcke, D.F. (1998). Innovations in performance measurement: Treads and research implications. Journal of Management Accounting Research, 12, 205–238.
Kaplan, R.S., & Norton, D.P. (1993). Putting the balanced scorecard to work. Harvard Business Review, 71, 139–144.
Kaplan, R.S., & Norton, D.P. (2001). Transforming the balanced scorecard from performance measurement to strategic management: Part I. Accounting Horizons, 15, 87–104.
Lee, A.H.I., Chen, W.C., & Chang, C.J. (2008). A fuzzy AHP and BSC approach for evaluating performance of IT department in the manufacturing industry in Taiwan. Expert Systems with Applications, 34, 96–107.
McKee, M., Healy, J., Edwards, N., & Harrison, A. (2002). Pressures for change. In M. McKee & J. Healy (Eds.), Hospitals in changing Europe (pp. 36 – 58). World Health Organization (WHO): European Observatory on Health Care Systems Series. Philadelphia: Open University Press.
Meliones, J.N., Ballard, R., Liekweg, R., & Burton, W. (2001). No mission, no margin. Journal of Health Care Finance, 27, 21–29.
Murphy, M.K., Black, N.A., & Lamping, D.L. (1998). Consensus development methods, and their use in clinical guideline development. Health Technology Assessment, 2(1), 1–8.
Phillips, P.A. (2007). The balanced scorecard and strategic control: A hotel case study analysis. The Service Industries Journal, 27(6), 731–746.
Thakkar, J., Deshmukh, S.G., Gupta, A.D., & Shankar, R. (2007). Development of a balanced scorecard: An integrated approach of Interpretive Structural Modeling (ISM) and Analytic Network Process (ANP). International Journal of Productivity and Performance Management, 56(1), 25–59.
Veillard, J., Champagne, F., Klazinga, N., Kazandjian, V., Arah, O.A., & Guisset, A.L. (2005). A performance assessment framework for hospitals: The WHO regional office for Europe PATH project. International Journal of Quality in Health Care, 17, 74–87.
Williams, F.P., D’Souza, D.E., Rosenfeldt, M.E., & Kassaee, M. (1995). Manufacturing strategy, business strategy and firm performance in a mature industry. Journal of Operations Management, 13, 19–33.
Willis, C.D., Stoelwinder, J.U., & Cameron, P.A. (2008). Interpreting process indicators in trauma care: Construct validity versus confounding by indication. International Journal of Quality in Health Care, 20, 1–8.
Wu, C.T., Tsai, H.T., Shih, M.H., & Fu, H.H. (2010). Government performance evaluation using a balanced scorecard with a fuzzy linguistic scale. The Service Industries Journal, 30(3), 449–462.
Yin, R.K. (1994). Case study research: Design and methods. Thousand Oaks, CA: Sage Publications.
1956 C.A. Luo et al.