112422 Atopic dermatitis and non-atopic hand eczema have similar negative impacts on life quality: Implications on clinical significance
Yin-Chun Chen1,2, Ching-Shuang Wu3, Yi-Wei Lu1, Wan-Chen Li1, Ying-Chin Ko4, Hsin-Su Yu1Gwo-Shing Chen1, Cheng-Che E. Lan1,2
1. Department of Dermatology, Kaohsiung Medical University Hospital. Department of Dermatology, College of Medicine, and Center of Excellence of Environmental Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
2. Department of Dermatology, Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung, Taiwan
3. Department of Medical Laboratory Science and Biotechnology, Kaohsiung Medical University, Kaohsiung, Taiwan
4. Graduate Institute of Clinical Medical Science, College of Medicine, China Medical University, Taichung, Taiwan
Running head: Impact of non-atopic hand eczema on life quality
Corresponding author: Dr. Cheng-Che Lan, 100 Shih-Chuan 1st Rd, Kaohsiung, Taiwan, Fax:+8867 3216580, e-mail: laneric@gmail.com
Word count: 1258 Table: 2
Funding source: This study is supported by National Health Research Institute, Taiwan (NHRI-CN-PD9611P)
Chronic hand eczema has serious consequences including prolonged sick leave, increased health costs, and hindered life quality . This condition has significant clinical impacts since hand eczema represents more than 90% of occupational skin diseases . Wet work, in particular, is an important occupational risk factor for development of hand eczema . Nursing staff of the hospital are prone to develop hand eczema due to the nature of their jobs that entails repetitive hand hygiene . Atopic dermatitis (AD) has been recognized as the most important risk factor for development of hand eczema among nursing staff . However, a population-based twin study has suggested that genetic factor other than AD contributed to development of hand eczema , and it has been shown that hand eczema with onset at young age portends unfavorable prognosis regardless of atopic status . Therefore, AD and non-atopic hand eczema represent distinct disorders. Clinically, since the lesions of AD are recognized to scatter over the entire body, one is likely to presume that AD is a more serious disease than non-atopic hand eczema and that patients are likely to receive more attention from physicians when presenting with AD as compared to hand eczema. In parallel, one is also likely to assume that AD has a more negative effect on life quality as compared to chronic hand eczema. This belief has important implications as previous studies demonstrated that impairment of life quality is a strong predictor of prolonged sick leave in patients with occupational dermatitis . Intriguingly, life quality scores do not always correlate with the clinical severity of skin conditions including hand eczema, acne, and ichthyosis . Therefore, life quality scores, rather than clinical signs, may be a better predictor for disease burden in certain skin diseases such as hand eczema. Although both AD and non-atopic hand eczema are commonly encountered skin conditions, a vis-à-vis comparison between AD and non-atopic hand eczema has rarely been performed from the patients’ perspective. The objective of this study is to determine the potential differences between AD and non-atopic hand eczema in terms of life quality scores among a university hospital nursing population in Taiwan.
MATERIAL AND METHODS Study population
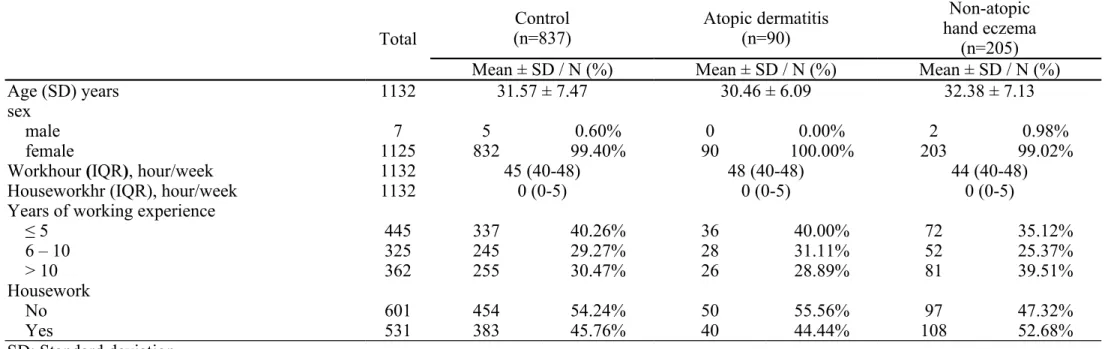
1218 nursing staff from Kaohsiung Medical University Hospital was invited to participate in this cross-sectional study. Of the invited participants, 1132 completed the study. Diagnosis of AD was made by dermatologists according to Hanifin and Rajka criteria . For identification of hand eczema, a validated questionnaire was used. This questionnaire comprised of 13 questions was developed to evaluate the signs and symptoms, locations of affected skin areas, duration of symptoms, and differential diagnoses of hand eczema . The phenotypes of the participants were categorized into three groups: 1) AD (n=90), 2) non-atopic hand eczema (n=205), and 3) control group with no aforementioned skin conditions (n=837). The demographic information of the participants is shown in Table 1.
Assessment of life quality
Short Form-36 (SF-36), a validated self-questionnaire, was used for evaluation of life quality. SF-36 is a generic quality of life index evaluating the quality of life and giving scores for eight specific domains: physical functioning (PF: limitations in performing physical activities such as dressing), role physical (RP: limitations with work and other daily activities as a result of physical health), role emotional (RE, limitations with work and other daily activities as a result of emotional problems), bodily pain (BP: how severe and limiting is pain), social functioning (SF: interference with normal social activities due to physical or emotional problems), vitality (VT: feeling tired and worn out versus feeling full of energy), mental health (MH: feeling nervous and depressed versus peaceful, happy, and calm), and general health (GH: how general personal health is evaluated by the patient) . The scores for each domain range from 0 to 100, with higher scores indicating a better life quality. This questionnaire was used for current study since Wallenhammer et al. has shown that SF-36 is a suitable tool for measurement of life quality affected by hand eczema.
Statistical Analysis
Statistical analysis was performed with SAS version 9.2 for Windows (SAS Institute Inc, Cary, North Carolina, USA). An alpha level of 0.05 was accepted as significant for all statistical procedures.
Characteristics of study participants are presented as means with their standard deviation (SD) values for normally distributed variables, medians with 25th to 75th percentile for non-normally distributed variables, and frequencies for categorical variables. For comparison of life quality scores, One-way Anova analyses were performed followed by post-hoc Tukey for direct comparison between specific groups
RESULTS
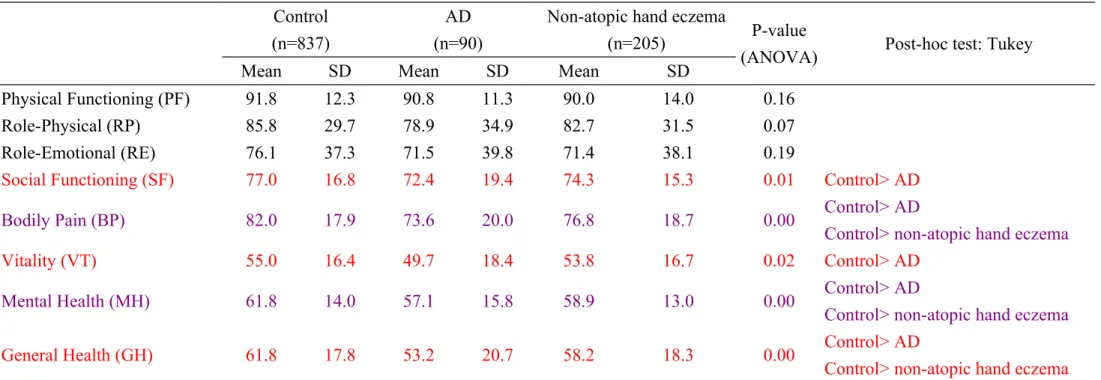
The demographic information of the study participants was shown in Table 1. Table 2 demonstrated the analyses of the SF-36 scores between different groups. The quality of life was significantly lower for AD patients as compared to controls in 5 out of 8 domains including SF, BP, VT, MH, and GH. Similarly, the
life quality of non-atopic hand eczema group was significantly lower than control in 3 out of 8 domains including BP, MH, and GH. No significant difference was found between AD and non-atopic hand eczema group in all domains of life quality investigated.
DISCUSSION
Although AD is the major risk factor for development of hand eczema in nursing population, we had previously shown that non-atopic hand eczema made up the majority of the nursing population with hand eczema . Intriguingly, while the impacts of AD and chronic hand eczema on life quality has been extensively studied , a vis-à-vis comparison has not been performed. As clearly demonstrated in this study, while both AD and non-atopic hand eczema impart significant negative impacts on life quality of those affected, no significant difference was found between the AD and non-atopic hand eczema groups. The significance of life quality alterations was demonstrated in many studies previously. In patients with different cancers, pretreatment life quality scores can predict survival independent of the extent of the disease and other clinical prognostic factors . For patients with psoriasis, those who reported poor life quality scores showed poor compliance to treatment . Since the impact on life quality significantly affects disease course and prognosis, the clinical significance of non-atopic hand eczema may deserve more attention than it is currently receiving as this condition may be as incapacitating as AD, a condition that is currently recognized as a chronic relapsing disease associated with serious negative impact on life quality and many research projects are currently focused on elucidating its pathogenesis and establishing better therapeutic strategies. It should be noted that since the lesions of AD tend to have a more generalized distribution, the effect of AD on overall physical appearance probably contributed to the lower scores in SF and VT domains as compared to control. Nevertheless, no significant differences was found between AD and non-atopic hand eczema groups in any life quality domains and both conditions imposed significant negative impact on BP, MH, and GH as compared to control. It is worthy to mention that the difference in life quality scores was also not found among AD patients with (n=43) or without (n=47) hand eczema (data not shown), although the number after subclassification is rather small. In this study, the majority of the participants were female. How gender may affect our result is an intriguing tissue that requires further investigation. In summary, AD and non-atopic hand eczema imposed similar negative impact on affected individuals in terms of life quality. As non-atopic hand eczema is the most commonly encountered occupational skin disease, more attention should be focused on this condition in order to provide more efficient preventive/therapeutic strategies.
ACKNOWLEDGEMENT
This study is supported by National Health Research Institute, Taiwan (NHRI-CN-PD9611P) REFERENCES
1. Skoet R, Olsen J, Mathiesen B, Iversen L, Johansen JD, Agner T. A survey of occupational hand eczema in Denmark. Contact Dermatitis 2004; 51: 159-166.
2. Cvetkovski RS, Rothman KJ, Olsen J, Mathiesen B, Iversen L, Johansen JD, et al. Relation between diagnoses on severity, sick leave and loss of job among patients with occupational hand eczema. Br J Dermatol 2005; 152: 93-98.
3. Lan CC, Feng WW, Lu YW, Wu CS, Hung ST, Hsu HY, et al. Hand eczema among University Hospital nursing staff: identification of high-risk sector and impact on quality of life. Contact Dermatitis 2008; 59: 301-306.
4. Flyvholm MA, Bach B, Rose M, Jepsen KF. Self-reported hand eczema in a hospital population. Contact Dermatitis 2007; 57: 110-115.
5. Lan CC, Tu HP, Lee CH, Wu CS, Ko YC, Yu HS, et al. Hand dermatitis among university hospital nursing staff with or without atopic eczema: assessment of risk factors. Contact Dermatitis 2011; 64: 73-79.
6. Bryld LE, Hindsberger C, Kyvik KO, Agner T, Menne T. Risk factors influencing the development of hand eczema in a population-based twin sample. Br J Dermatol 2003; 149: 1214-1220.
7. Meding B, Wrangsjo K, Jarvholm B. Fifteen-year follow-up of hand eczema: predictive factors. J Invest Dermatol 2005; 124: 893-897.
8. Cvetkovski RS, Zachariae R, Jensen H, Olsen J, Johansen JD, Agner T. Prognosis of occupational hand eczema: a follow-up study. Arch Dermatol 2006; 142: 305-311.
9. Demircay Z, Seckin D, Senol A, Demir F. Patient's perspective: an important issue not to be overlooked in assessing acne severity. Eur J Dermatol 2008; 18: 181-184.
10. Ganemo A, Lindholm C, Lindberg M, Sjoden PO, Vahlquist A. Quality of life in adults with congenital ichthyosis. J Adv Nurs 2003; 44: 412-419.
11. Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol 1980; Suppl 92:44-47.
12. Ware JE, Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992; 30: 473-483.
13. Wallenhammar LM, Nyfjall M, Lindberg M, Meding B. Health-related quality of life and hand eczema--a comparison of two instruments, including factor analysis. J Invest Dermatol 2004; 122: 1381-1389.
14. Cvetkovski RS, Zachariae R, Jensen H, Olsen J, Johansen JD, Agner T. Quality of life and depression in a population of occupational hand eczema patients. Contact Dermatitis 2006; 54: 106-111.
15. Hald M, Agner T, Blands J, Veien NK, Laurberg G, Avnstorp C, et al. Clinical severity and prognosis of hand eczema. Br J Dermatol 2009; 160: 1229-1236.
16. Moberg C, Alderling M, Meding B. Hand eczema and quality of life: a population-based study. Br J Dermatol 2009; 161: 397-403.
17. Linnet J, Jemec GB. An assessment of anxiety and dermatology life quality in patients with atopic dermatitis. Br J Dermatol 1999; 140: 268-272.
18. Braun DP, Gupta D, Grutsch JF, Staren ED. Can changes in health related quality of life scores predict survival in stages III and IV colorectal cancer? Health Qual Life Outcomes 2011; 9: 62. 19. Zaghloul SS, Goodfield MJ. Objective assessment of compliance with psoriasis treatment. Arch
Table 1. Demographic profile of participating nurses in this study
Total (n=837)Control Atopic dermatitis(n=90)
Non-atopic hand eczema
(n=205) Mean ± SD / N (%) Mean ± SD / N (%) Mean ± SD / N (%)
Age (SD) years 1132 31.57 ± 7.47 30.46 ± 6.09 32.38 ± 7.13
sex
male 7 5 0.60% 0 0.00% 2 0.98%
female 1125 832 99.40% 90 100.00% 203 99.02%
Workhour (IQR), hour/week 1132 45 (40-48) 48 (40-48) 44 (40-48)
Houseworkhr (IQR), hour/week 1132 0 (0-5) 0 (0-5) 0 (0-5)
Years of working experience
≤ 5 445 337 40.26% 36 40.00% 72 35.12% 6 – 10 325 245 29.27% 28 31.11% 52 25.37% > 10 362 255 30.47% 26 28.89% 81 39.51% Housework No 601 454 54.24% 50 55.56% 97 47.32% Yes 531 383 45.76% 40 44.44% 108 52.68% SD: Standard deviation IQR: Inter-quartile range
Table 2. Differences in the short form (SF)-36 domain scores between control, atopic dermatitis (AD) and non-atopic hand eczema groups Control
(n=837)
AD (n=90)
Non-atopic hand eczema
(n=205) P-value
(ANOVA) Post-hoc test: Tukey
Mean SD Mean SD Mean SD
Physical Functioning (PF) 91.8 12.3 90.8 11.3 90.0 14.0 0.16
Role-Physical (RP) 85.8 29.7 78.9 34.9 82.7 31.5 0.07
Role-Emotional (RE) 76.1 37.3 71.5 39.8 71.4 38.1 0.19
Social Functioning (SF) 77.0 16.8 72.4 19.4 74.3 15.3 0.01 Control> AD
Bodily Pain (BP) 82.0 17.9 73.6 20.0 76.8 18.7 0.00 Control> AD
Control> non-atopic hand eczema
Vitality (VT) 55.0 16.4 49.7 18.4 53.8 16.7 0.02 Control> AD
Mental Health (MH) 61.8 14.0 57.1 15.8 58.9 13.0 0.00 Control> AD
Control> non-atopic hand eczema
General Health (GH) 61.8 17.8 53.2 20.7 58.2 18.3 0.00 Control> AD
Control> non-atopic hand eczema
One-way analysis of variance (ANOVA) was used to compare mean between the groups. When ANOVA showed a significant difference (p- value<0.05) , Tukey's test was used for post-hoc multiple comparisons among different group means.