Original Article
Magnesium status and association with diabetes in the
Taiwanese elderly
Jui-Line Wang
PhD,1,2Ning-Sing Shaw
PhD,2Hsiang-Yu Yeh
PhD1and
Mei-Ding Kao
MS3
1 Department of Food and Nutrition, Hung-Kuang University, Taichung,Taiwan
2 Institute of Microbiology and Biochemistry, National Taiwan University, Taipei,Taiwan
3 Department of Food and Nutrition, Providence University, Taichung, Taiwan
The average dietary intake of magnesium is below recommended dietary allowances in many affluent Western countries. Prolonged low magnesium intake tends to result in hypomagnesaemia which might increase the risk of chronic diseases in elderly people. A national population-based cross-sectional nutrition survey, the Elderly Nutrition and Health Survey in Taiwan (1999-2000), was used to investigate the magnesium status and association with diabetes in the Taiwanese elderly. Dietary magnesium intake was based on 24-hour dietary recalls. Blood biochemical parameters including plasma magnesium and blood glucose were also measured. Average magnesium intake was 250mg in men and 216mg in women, which is equivalent to 68-70% of relevant Taiwanese Dietary Reference Intakes. The mean plasma magnesium concentration was 0.903 mmol/L in men and 0.906 mmol/L in women. The prevalence of a plasma magnesium level of <0.7 mmol/L was 0.7 - 0.9% in the elderly, and that of <0.8 mmol/L was 8.0-9.1%. Elderly vegans had a significantly lower magnesium intake than ovo-lacto vegetarians and non-vegetarians. Diabetic men and women had significantly higher blood glucose levels than non-diabetics. The risk of diabetes was elevated 3.25 times at plasma magnesium levels <0.863mmol/L. There was an inverse association between plasma magnesium concentration and the prevalence of diabetes. However, no association was found between diabetes and low dietary magnesium. Taiwanese elderly persons had suboptimal levels of dietary magnesium intake, which although may be sufficient to avoid overt magnesium deficiency, may not be sufficient to reduce the risk of diabetes in the elderly. Further prospective study is required to help explain the differential results between dietary and plasma magnesium levels.
Key words: magnesium intake, plasma magnesium, the elderly, diabetes mellitus, nutrition survey, Taiwan, Elderly Nutrition and Health Survey in Taiwan (1999-2000)
Introduction
Magnesium is the second most abundant intracellular cation in the body, and is a cofactor in more than 300 enzy-matic reactions involved in energy metabolism, protein and nucleic acid synthesis, transport of potassium and calcium ions, signal transduction and cell proliferation.1-3 The net absorption rate of magnesium from a typical diet is appro-ximately fifty percent and can be inhibited by high levels of dietary fiber, phosphorus, oxalic acid and phytic acid.4-8 The plasma level of magnesium is maintained remarkably constant in healthy individuals by a poorly understood ho-meostatic mechanism.9 Although magnesium is found in a variety of foods and beverages, magnesium depletion is not uncommon among the general population.9,10
Inadequate magnesium intake has been found to be associated with chronic diseases including diabetes, hyper-tension, and atherosclerosis.11-14 Epidemiological and expe-rimental studies support a role for magnesium deficiency in the pathogenesis of hypertension, with reports demonstra-ting an inverse correlation between magnesium levels and blood pressure involving a hypotensive action of dietary magnesium supplementation and a hypertensive effect of magnesium deficiency.14-18 Epidemiological studies also
indicate a direct relationship between atherosclerosis and serum magnesium, which in turn depends on dietary in-take.15 Oral magnesium supplementation has beneficial effects on plasma lipids19 and an inverse association be-tween serum magnesium concentration and mortality from ischemic heart disease has been documented.20,21 Further-more, hypomagnesaemia has been demonstrated in 25-38% of patients with type 2 diabetes, especially in those without good metabolic control.22,23 Low magnesium intake may re-duce glucose tolerance and increase insulin resistance.23-27 The American Diabetes Association has already endorsed magnesium supplementation for diabetics who are at high risk of magnesium deficiency.28
Some short-term metabolic studies suggest that magne-sium supplementation has a beneficial effect on insulin action and glucose metabolism.26-29 Several large obser-vational studies have demonstrated a strong cross-sectional
Correspondence address: Professor Mei-Ding Kao, Dept of Food and Nutrition, Providence University, Taiwan.
Tel: 886-4-26328001-15310 Fax: 886-4-26530027 Email: mdkao@pu.edu.tw Accepted 30 June 2005
association between the incidence of type 2 diabetes and serum Mg as well as dietary Mg.12,15 Recently, results
from prospective studies have also supported a protective role for higher magnesium intake in reducing the risk of developing type 2 diabetes.30-32
Diabetes, hypertension and cardiovascular disease are
among the ten leading causes of death in Taiwan and in-adequate magnesium intake has been linked to these ad-verse health outcomes. As a result, we assessed dietary intake of magnesium, plasma magnesium levels and the population distribution of magnesium status and com-pared these with associated health effects in the Tai-wanese elderly.
Subjects and Methods
Subjects and data source
The Elderly Nutrition and Health Survey in Taiwan (1999-2000) (Elderly NAHSIT) was a government-sponsored survey that included 24-h dietary recall and health status assessment by interviewer-administered questionnaires. The complex sampling scheme used in this survey is reported in detail in another publication in this issue33 as is the assessment of dietary intake.34
Esti-mates of dietary magnesium intake were taken from 1911 subjects aged 65 years and older who had completed the dietary assessment. Estimates of the population distri-bution of plasma magnesium concentrations were cal-culated from 2225 subjects aged 65 years and older who had participated in the physical examination which in-cluded measurement of anthropometric and blood bio-chemical parameters. A subgroup of subjects who pro-vided complete data for both dietary recall and blood parameters were used in the analysis of the association between magnesium parameters and the prevalence of diabetes.
Blood an alyses
Venous blood samples were collected into vacuum tubes
from fasting subjects. Plasma samples were frozen and shipped to the laboratory for biochemical analysis after the sample collection was completed. Plasma magnesium concentration was measured using a colorimetric assay in-volving the reaction of xylidylblue to form a complex with absorption at 520 nm. The measurement was carried out with the Olympus System Reagent using an Olympus Autoanalyzer.
Statistical analyses
All variables were weighted to represent the population in Taiwan.23 Values were expressed as mean ± standard
error and differences between groups were tested using the t-test. Trends across quartiles were evaluated by li-near regression. Logistic regression analysis was per-formed to evaluate the association between low plasma magnesium and diabetes mellitus. Statistical analysis was performed using SAS version 8.235 and SUDAAN version
9.0.36 The level for statistical significance was set at P <0.05.
Results
Dietary intake of magnesium by gender and age is listed in Table 1. Daily magnesium intake averaged 250 ± 13mg in men and 216 ± 11mg in women, which is equivalent to 69.4% and 68.6% of the DRIs (Dietary Reference In-takes) for men and women, respectively. Daily calorie intake averaged 1833 ± 72 kcal in men and 1477 ± 63 kcal in women, which is equivalent to 108 % and 100 % of the DRIs for men and women, respectively.34 Mg
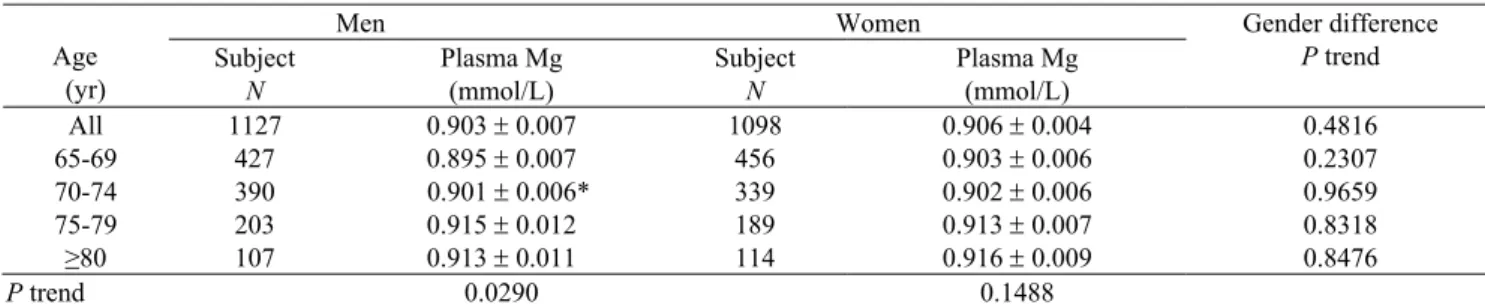
density was 142.7 mg/1000 kcal in men and 153.5 mg/ 1000 kcal in women. Men had a significantly higher in-take than women at every age interval from 65 to 79 years old, but there was no difference in the over 79 age range. Plasma magnesium concentrations by gender and age are listed in Table 2. The mean concentration was 0.903± 0.007 mmol/L in men and 0.906 ± 0.004 mmol/L in wo-men; it increased with age and the trend was significant for men but not for women. Plasma magnesium concen-trations did not differ among vegans, ovo-lacto vegeta-rians and non-vegetavegeta-rians, but dietary magnesium intake was significantly lower in vegans versus non-vegetarians (Table 3).
Table 1. Daily dietary intake of magnesium by gender and age in the Taiwanese elderly *
Men Women Age (yr) Subject N Mg intake mg/day Subject N Mg intake mg/day Gender difference P trend All 955 250 ± 13 956 216 ± 11 <0.0001 65-69 356 253 ± 8 392 222 ± 10 0.0042 70-74 326 246 ± 15 302 216 ± 12 0.0490 75-79 185 256 ± 22 154 222 ± 25 0.0203 ≥80 88 246 ± 31 108 197 ± 19 0.1347
P trend for age 0.8909 0.3559
*Values are expressed as mean ± SE and weighted. Gender difference was tested using the Student’s t test and significance was set at P <0.05.
Table 2. Plasma magnesium concentrations by gender and age in the Taiwanese elderly*
Men Women Age (yr) Subject N Plasma Mg (mmol/L) Subject N Plasma Mg (mmol/L) Gender difference P trend All 1127 0.903 ± 0.007 1098 0.906 ± 0.004 0.4816 65-69 427 0.895 ± 0.007 456 0.903 ± 0.006 0.2307 70-74 390 0.901 ± 0.006* 339 0.902 ± 0.006 0.9659 75-79 203 0.915 ± 0.012 189 0.913 ± 0.007 0.8318 ≥80 107 0.913 ± 0.011 114 0.916 ± 0.009 0.8476 P trend 0.0290 0.1488
The distribution of plasma magnesium concentrations in the elderly is shown in Figure 1. The median value of plasma magnesium was 0.905 mmol/L for both men and women. The prevalence of magnesium deficiency defined as serum Mg values <0.7mmol/L was 0.9% in men and 0.7% in women (Table 4). The prevalence of low plasma magnesium defined as values <0.8 mmol/L was 9.1% in men and 8.0% in women (Table 4).
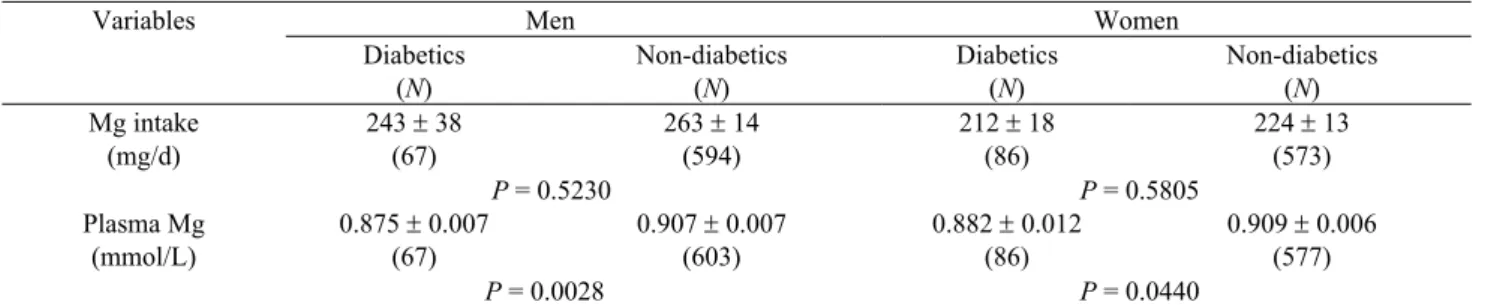
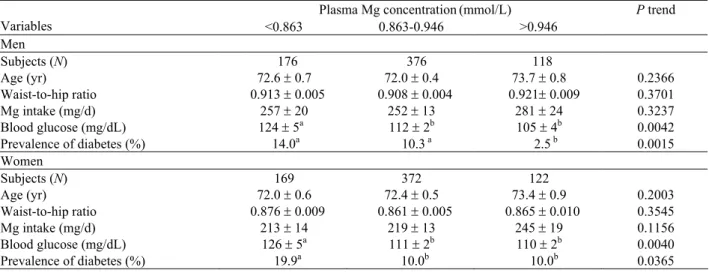
Table 5 compares the magnesium intake and plasma magnesium concentrations in diabetic and non-diabetic subjects, which were identified according to a physician’s diagnosis. In both men and women, dietary intake of magnesium did not differ between diabetic and non-diabetic subjects, but plasma magnesium concentrations were significantly lower in diabetic subjects than in non-diabetics. The prevalence risks for diabetes by quartile of plasma magnesium concentration according to logistic regression analysis are listed in Table 6. Compared to the highest quartile of plasma magnesium concentration, the odds ratios of diabetes prevalence in elderly men and women were 5.27 and 2.66, respectively, for the lowest quartile with a plasma magnesium level lower than 0.863 mmol/L. Table 7 compares several predictors of diabetes across three different plasma magnesium ranges. There
was no difference in age, waist-to-hip ratio or magnesium intake, but low plasma magnesium levels were associated with higher fasting blood glucose concentrations (P = 0.0042 and 0.0040) and a higher prevalence of diabetes (P = 0.0015 and 0.0365) in both men and women.
Discussion
Recent dietary surveys have shown that the average mag-nesium intake is slightly below the appropriate RDAs in Western countries.10 The dietary magnesium intake for
US men and women aged 71 years and older from the NHANES III was 314 mg/d and 230 mg/d, which is equi-valent to 90% and 84% of the RDAs, respectively.9,15,37
The average magnesium intake in the Dutch elderly was 311mg/d.38 The true intake of magnesium in a German
diet has been found to be about 200mg for women and 260mg for men.39 The mean magnesium intakes in adult
men and women based on the results of the SU.VI.MAX cohort in France were 369 and 280mg, respectively.40 In
Belgium, a mean magnesium intake of 271mg/day was found.41 In Switzerland, an estimate based on
disappear-ance data from 1994/1995 was 406 mg/d for subjects aged 15 years and above,42 and the mean intake in Swiss
elderly was 421 mg/d in men and 383 mg/d in women.43
The Taiwanese DRI of magnesium is 360 and 315 mg/d for adult men and women, respectively.44 According to
this study, the average magnesium intake of 250 and 216 mg/d in elderly Taiwanese men and women, respectively, is suboptimal and is comparatively lower than that found in Western countries. Our study agrees with others with respect to a gender-related difference, with men having a higher magnesium intake than women.
Magnesium intake may vary with different types of diets. Compared to the data from the US, Swiss elderly had higher magnesium intake because of their higher con-sumption of cereal products, which contribute 23% of magnesium intake in the Swiss diet in contrast to only 17- 18% in the US diet.43 A population of Mexicans eating a
more plant-based diet had magnesium intakes of 301 mg/d in women and 318 mg/d in men.39 In Germany,
magnesium intake for lacto-ovo vegetarians was 376 mg/d
Table 3. Comparison of magnesium intake and plasma magnesium concentrations among vegans, ovo-lacto vegetarians
and non-vegetarians*
Men Women
Dietary types
N
Plasma Mg
(mmol/L) N Mg Intake (mg/d) N Plasma Mg (mmol/L) N Mg Intake (mg/d) Vegan 17 0.915 ± 0.012 18 196 ± 17a 92 0.906 ± 0.011 102 193 ± 17a Ovo-lacto vegetarian 42 0.918 ± 0.015 44 244 ± 16ab 192 0.911 ± 0.008 211 225 ± 14ab Non-vegetarian 611 0.902 ± 0.007 680 263 ± 15b 379 0.903 ± 0.007 403 233 ± 21b
*The vegan diet excluded all animal products; the ovo-lacto vegetarian diet excluded all animal flesh but included dairy products and eggs. Values are expressed as mean ± SE. Groups not sharing the same superscript letters “a, b” are significantly different based on the t-test significant at P <0.05.
Table 4. Prevalence of magnesium deficiency by age and gender in the Taiwanese elderly
Proportion (%) by plasma Mg concentration* Gender Subjects (N) < 0.7 (mmol/L) 0.7 - < 0.8 (mmol/L) 0.8 - <0.9 (mmol/L) 0.9 - <1.0 (mmol/L) > 1.0 (mmol/L) Men 1127 0.9 9.1 31.7 50.8 8.3 Women 1098 0.7 8.0 31.6 50.3 10.1
Figure 1. Distribution of plasma magnesium concentrations in the Taiwanese elderly. Frequency (%) 0 10 20 30 40 < 0. 7 0.7 - <0.7 5 0.7 5 - <0. 8 0.8 - <0.8 5 0.8 5 - < 0.9 0. 9 - < 0.95 0. 95 < 1 .0 1. 0 < 1. 05 1. 05 < 1. 1 >= 1. 1 Male Female
in women and 474 mg/d in men, which was significantly higher than the intake of 205 mg/d and 266 mg/d in omni-vorous women and men, respectively.39 However,
fin-dings in Taiwan are contrary to those of Western coun-tries.39,43 Elderly vegans in Taiwan had a lower
magne-sium intake than non-vegetarians, and the differences in magnesium intake between ovo-lacto vegetarians and non-vegetarians was not significant (Table 3). This dis-agreement is most likely related to food choices as Chi-nese vegetarians tend to use more soy products made of processed soy proteins rather than whole legumes and whole grains. This supports the idea that a beneficial ve-getarian diet requires an appropriate combination of a range of plants as food. 34
The inadequate magnesium intakes observed in vari-ous countries including Taiwan may reflect similar trends in dietary patterns. The “Western diet” is considered rela-tively deficient in magnesium, while the “Oriental diet” is traditionally characterized by a greater intake of fruits and vegetables and therefore is richer in magnesium.34
How-ever, dietary patterns in Taiwan have been gradually westernized as the nation has become more affluent. We have noted that the analyzed magnesium content in meals prepared by some registered Taiwanese dieticians was only 258 mg/d,45 which is below the Taiwanese DRI of
magnesium for adults.44 The top-ranked source of
mag-nesium was rice/rice products (14.5% of total intake) for males and green vegetables for females (15.8% of total intake).34 The consumption of magnesium-rich foods such
as whole grains, legumes and nuts is below the recom-mended quantities.
The normal range of plasma magnesium concentration is 0.75-1.00 mmol/L.10 The prevalence of magnesium
deficiency in developing countries such as India has been found to be as high as 11.8%.46 The prevalence of low
serum magnesium concentration (<0.8 mmol/L) was esti-mated to be 23% in U.S. adults aged 25-74 years.21 In
Germany, low serum magnesium concentrations were found in about 5-8% of the overall population of various ages,47 and plasma magnesium concentrations below 0.76
mmol/L were observed in 14.5% of an unselected popu-lation.48 According to the results of this study, overt
mag-nesium deficiency (0.7-0.9%) and low serum magmag-nesium (8.0-9.1%) in the elderly were both less prevalent in Taiwan than in some developing and developed countries. Low serum magnesium levels in patients with type 2 diabetes and an inverse association between magnesium status and risk of type 2 diabetes have been reported in Caucasian populations.15,22,43 The association has been
further supported by cross-sectional studies that have ob-served an inverse association between plasma or erythro-cyte magnesium levels and fasting insulin levels in dia-betic patients and apparently healthy individuals.15,23,49,50
Strong support also comes from several prospective die-tary studies, including the Atherosclerosis Risk in Communities Study,30 the Women’s Study,31 the Nurses’
Health Study,32 and the Health Professionals Follow-up
Study.32 This study of Taiwanese elderly persons is the
first to demonstrate an inverse association between serum magnesium concentration and the prevalence of diabetes in a non-Caucasian population. The findings are con-sistent with the results found for Western countries, but
Table 5. Comparison of magnesium intake and plasma magnesium concentration between diabetic and non-diabetic
elderly in Taiwan Men Women Variables Diabetics (N) Non-diabetics (N) Diabetics (N) Non-diabetics (N) 243 ± 38 (67) 263 ± 14 (594) 212 ± 18 (86) 224 ± 13 (573) Mg intake (mg/d) P = 0.5230 P = 0.5805 0.875 ± 0.007 (67) 0.907 ± 0.007 (603) 0.882 ± 0.012 (86) 0.909 ± 0.006 (577) Plasma Mg (mmol/L) P = 0.0028 P = 0.0440
*The diabetic subjects were diagnosed clinically by physicians. The difference between diabetic and non-diabetic groups was tested using a t-test, significant level set at P <0.05.
Table 6. Odds ratio of diabetes mellitus by quartile of plasma magnesium in the Taiwanese elderly
Odds ratio by quartile of plasma Mg concentration* Gender I < 0.863 mmol/L II, III 0.863 - 0.946 mmol/L IV > 0.946 mmol/L All 3.25 (1.67 - 6.34) 1.94 (0.91 - 4.12) 1 Men 5.27 (1.69 - 16.47) 4.06 (1.01 - 16.39) 1 Women 2.66 (1.24 - 5.67) 1.30 (0.68 - 2.4) 1
*Logistic regression analysis was used. Numbers in parentheses indicate 95% confidence intervals adjusted for age, waist-hip ratio, blood pressure, BMI, and supplements for both men and women. In men, drinking and smoking were also adjusted for. Interval classes for adjustment were: age (65 - 69, 70 - 74, 75 - 79, 80+), waist-hip ratio ( ≥ 0.9 or < 0.9 for men, ≥ 0.85 or < 0.85 for women), SBP (≥140, <140 mmHg), DBP (≥ 90, <90 mmHg), drinking (≥ 1 time/wk, N), smoking (Y,N), supplements (regular intake, N), BMI (<19.8, ≥19.8).
the causal relationship is not clear as magnesium deple-tion might induce insulin resistance, alternatively hyper-insulinemia and glucosuria might also contribute to mag-nesium depletion.12 Taken together, our data seem to
indi-cate a plasma magnesium concentration at the lower end of the reference range might not be sufficient to reduce the risk or ameliorate the symptoms of diabetes in the elderly. However, a prospective study is required to con-firm the temporal nature of this relationship.
The elderly are probably susceptible to magnesium de-pletion due to several reasons. Firstly, aging is associa-ted with increased intracellular calcium and decreased intracellular magnesium levels.51 Secondly, magnesium
intake from dietary sources would seem to be suboptimal throughout life. In addition, the elderly might not be able to benefit from magnesium-rich foods due to their hard texture and inappropriate physical properties. An im-provement of glucose metabolism and/or insulin sensi-tivity by magnesium supplements has been demonstrated in diabetic and apparently healthy elderly persons.26,52,53
Therefore, increased everyday consumption of whole grains, legumes, and vegetables rich in magnesium and the use of supplements may help to improve the magne-sium status of the elderly.
This study is the first to demonstrate an inverse asso-ciation between plasma magnesium concentration and the prevalence of diabetes in a non-Caucasian population. In addition, this report describes the magnesium status of the elderly in Taiwan. The average daily intake of dietary magnesium in both men and women was below the Tai-wanese DRIs for adults. A vegetarian diet did not increase magnesium intake and had no significant effect on plasma magnesium concentrations. Overt magnesium deficiency rarely occurred, and the prevalence of low serum magne-sium levels was comparatively lower than that found in other developed countries. However, diabetic subjects had significantly lower plasma magnesium and higher blood glucose concentrations than non-diabetic subjects. An increased prevalence of diabetes was significantly asso-ciated with plasma magnesium concentrations less than 0.863mmol/L. Both dietary modification and magnesium
supplementation may need to be considered for the elderly
when this relationship is confirmed.
Acknowledgements
This study was supported by a grant (DOH93-FS-6-2) from the Department of Health in Taiwan. The authors thank Dr. Tsan-Zon Liu, Department of Medical Biotechnology and Laboratory Science, Chang Gung University, Tao-Yuan, and staff of the Laboratory Medicine Department, Yuan’s General Hospital, Kaohsiung, for their excellent technical assistance in hematological analyses. Appreciation also goes to Dr. Wen-Harn Pan, Director of the research project "Nutrition and Health Survey in Taiwan (NAHSIT)" (DOH-88-FS, DOH89-88shu717, DOH90-FS-5-4, DOH91-FS-5-4) for collection of the blood specimens and disease data. The views expressed herein are solely those of the authors.
References
1. Wacker WE, Parisi AF. Magnesium Metabolism. N Eng J Med 1968; 45: 658-663.
2. Wester PO. Magnesium. Am J Clin Nutr 1987; 45: 1305-1312.
3. Saris NE, Mervaala E, Karppance H, Khawaja JA, Lewenstam A. Magnesium an update on physiological, clinical and analytical aspects. Clin Chem Acta 2000; 294: 1-26.
4. Kelsay JL, Behall KM, Prather ES. Effect of fiber from fruits and vegetables on metabolic responses of human subjects. II Calcium, magnesium, iron, and silicon balances. Am J Clin Nutr 1979; 32: 1876-1880.
5. Wisker E, Nagel R, Tanudjaja TK, Feldheim W. Calcium, magnesium, zinc, and iron balances in young women: Effects of a low-phytate barley-fiber concentrate. Am J Clin Nutr 1991; 54: 553-559.
6. Siener R, Hesse A. Influence of a mixed and vegetarian diet on urinary magnesium excretion and concentration. Br J Nutr 1995; 73: 783-790.
7. Hardwick LL, Jones MR, Brautbar N, Lee DB. Magnesium absorption: Mechanisms and the influence of vitamin D, calcium and phosphate. J Nutr 1991; 121: 13-23.
8. Bohn T, Davidsson L, Walczyk T, Hurrell RF. Phytic acid added to white-wheat bread inhibits fractional apparent magnesium absorption in humans. Am J Clin Nutr 2004; 79:418-23.
Table 7. Comparison of blood glucose and selected predictors for diabetes mellitus by quartile of plasma magnesium
concentration*
Plasma Mg concentration(mmol/L)
Variables <0.863 0.863-0.946 >0.946 P trend Men Subjects (N) 176 376 118 Age (yr) 72.6 ± 0.7 72.0 ± 0.4 73.7 ± 0.8 0.2366 Waist-to-hip ratio 0.913 ± 0.005 0.908 ± 0.004 0.921± 0.009 0.3701 Mg intake (mg/d) 257 ± 20 252 ± 13 281 ± 24 0.3237 Blood glucose (mg/dL) 124 ± 5a 112 ± 2b 105 ± 4b 0.0042 Prevalence of diabetes (%) 14.0a 10.3 a 2.5 b 0.0015 Women Subjects (N) 169 372 122 Age (yr) 72.0 ± 0.6 72.4 ± 0.5 73.4 ± 0.9 0.2003 Waist-to-hip ratio 0.876 ± 0.009 0.861 ± 0.005 0.865 ± 0.010 0.3545 Mg intake (mg/d) 213 ± 14 219 ± 13 245 ± 19 0.1156 Blood glucose (mg/dL) 126 ± 5a 111 ± 2b 110 ± 2b 0.0040 Prevalence of diabetes (%) 19.9a 10.0b 10.0b 0.0365
*Values are mean ± SE. Differences between groups were evaluated using the t-test. A different superscript letter indicates significant difference at P<0.05.
9. Institute of Medicine. Dietary Reference Intakes for Calcium, Phosphorous, Magnesium, Vitamin D, and Fluoride. Washington DC: National Academy Press, 1997. 10. Vormann J. Magnesium: nutrition and metabolism. Mol
Aspects Med 2003; 24: 27-37.
11. Maier JAM. Low magnesium and atherosclerosis: an evidence-based link. Mol Aspects Med 2003; 24: 137-146. 12. Barbagallo M, Dominguez LJ, Galioto A, Ferlisi A, Cani
C, Malfa L, Pineo A, Busardo' A, Paolisso G. Role of magnesium in insulin action, diabetes and cardio-metabolic syndrome X. Mol Aspects Med 2003; 24:39-52.
13. Delva P. Magnesium and coronary heart disease. Mol Aspects Med 2003; 24: 63-78.
14. Touyz RM. Role of magnesium in the pathogenesis of hypertension. Mol Aspects Med 2003; 24: 107-136. 15. Ma J, Folsom AR, Melnick SL. Associations of serum and
dietary magnesium with cardiovascular disease, hypertension, diabetes, insulin, and carotid arterial wall thickness: The ARIC study. Atherosclerosis Risk in Community Study. J Clin Epidemiol 1995; 48: 927-940. 16. Joffres MR, Reed DM, Yano K. Relationship of
magnesium intake and other dietary factors to blood pressure: The Honolulu heart study. Am J Clin Nutr, 1987; 45: 469-475.
17. Sacks FM, Obarzanek E, Windhauser MM, Svetkey LP, Vollmer WM, McCullough M, Karanja N, Lin PH, Steele P, Proschan MA, Evans MA, Appel LJ, Bray GA, Vogt TM, Moore TJ. Rationale and design of the dietary approaches to stop hypertension trial (DASH). A multicenter controlled-feeding study of dietary pattern to lower blood pressure. Ann Epidemiol 1995; 5: 108-118. 18. Peacock JM, Folsom AR, Arnett DK, Eckfeldt JH, Szklo
M. Relationship of serum and dietary magnesium to incident hypertension: the Atherosclerosis Risk in Communities (ARIC) Study. Ann Epidemiol 1999; 9: 159-165.
19. Rasmussen HS, Aurup P, Goldstein K, McNair P, Mortensem PB, Larsen OG, Lawaetz H. Influence of magnesium substitution therapy on blood lipid composition in patients with ischemic heart disease. A double-blind, placebo controlled study Arch Int Med 1989; 149: 1050-1053.
20. Rubenowitz E, Axelsson G, Rylander R. Magnesium in drinking water and death from myocardial infarction. Am J Epidemiol 1996; 143: 456-462.
21. Ford ES. Serum magnesium and ischaemic heart disease: findings from a national sample of US adults. Int J Epidemiol 1999; 28: 645–651.
22. Sjogren A, Floren CH, Nilszon A. Magnesium, potassium and zinc deficiency in subjects with type diabetes mellitus. Acta Med Scand 1988; 224: 461-465.
23. Nadler JL, Bunchanan T, Natarajan R, Antonipillai I, Bergman R, Rude RK. Magnesium deficiency produces insulin resistance and increased thromboxane synthesis. Hypertension 1993; 21: 1024-1029.
24. Paolisso G, Scheen A, D'Onofrio F, Lefebvre P. Magne-sium and glucose homeostasis. Diabetologia 1990; 33: 511-514.
25. Schmidt LE, Arfken CL, Heins JM. Evaluation of nutrient intake in subjects with non-insulin-dependent diabetes mellitus. J Am Diet Assoc 1994; 94: 773-774.
26. Paolisso G, Sgambato S, Gambardella A, Pizza G, Tesauro P, Varricchio M, D'Onofrio F. Daily magnesium supple-ments improve glucose handling in elderly subjects. Am J Clin Nutr 1992; 55: 1161-1167.
27. Paolisso G, Passariello N, Pizza G, Marrazzo G, Giunta R, Sgambato S, Varricchio M, D'Onofrio F. Dietary magnesium supplements improve B-cell response to glucose and arginine in elderly non-insulin-dependent diabetic subjects. Acta Endocrinol Copenh 1989; 121: 16-20.
28. American Diabetes Association. Magnesium supplemen-ation in the treatment of diabetes. Diab Care 1992;15: 1065.
29. Lima Mde L, Cruz T, Pousada JC, Rodrigues LE, Barbosa K, Cangucu V. The effect of magnesium supplementation in increasing doses on the control of type 2 diabetes. Diabetes Care 1998;21: 682-686.
30. Kao WH, Folsom AR, Nieto FJ, Mo JP, Watson RL, Brancati FL. Serum and dietary magnesium and the risk for type 2 diabetes mellitus: the Atherosclerosis Risk in Communities Study. Arch Intern Med 1999; 159:2151-2159.
31. Song Y, Manson JE, Buring J, Liu S. Dietary magnesium intake in relation to plasma insulin levels and risk of type 2 diabetes in women. Diabetes Care 2004; 27: 59-65. 32. Lopez-Ridaura R, Willett WC, Rimm EB, Liu S, Stampfer
MJ, Manson JE, Hu FB. Magnesium intake and risk of type 2 diabetes in men and women. Diabetes Care 2004; 27: 134-40.
33. Pan WH,Hung YT, Shaw NS, Lin W, Lee SD, Chiu CF, Lin MC, Chen SY, Hong CM, Huang TY, Chang HY, Tu SH, Chang YH, Yeh WT, Su SC. Elderly Nutrition and Health Survey in Taiwan (1999-2000): research design, methodology and content. Asia Pac J Clin Nutr 2005; 14 (3): 203-210.
34. Wu SJ, Chang YH, Wei IL, Kao MD, Lin YC, Pan WH. Intake levels and major food sources of energy and nutrients in the Taiwanese elderly. Asia Pac J Clin Nutr 2005; 14:(3): 211-220.
35. SAS Institute Inc. SAS/STAT User's Guide, Version 6, 4th ed., vol. 2 SAS Institute, Cary, NC, 1990.
36. Shah BV, Barnwell BG, Bieler GS. SUDAAN User's Manual. Release 7.5. Research Triangle Park, North Carolina: Research Triangle Institute, 1997.
37. Ford ES, Mokdad AH. Dietary magnesium intake in a national sample of US adults. J Nutr 2003; 133:2879-2882. 38. Geleijnse JM, Witteman JC, den Breeijen JH, Hofman A,
de Jong PT, Pols HA, Grobbee DE. Dietary electrolyte intake and blood pressure in older subjects: the Rotterdam Study. J Hypertens 1996 ;14: 737-741.
39. Vormann J, Anke M. Dietary magnesium: supply, require-ments and recommendations–results from duplicate and balance studies in man. J Clin Basic Cardiol 2002; 5: 49-53.
40. Galan P, Preziosi P, Durlach V, Valeix P, Ribas L, Bouzid D, Favier A, Hercberg S. Dietary magnesium intake in a French adult population. Magnes Res 1997;10: 321 -328. 41. Hendrix P, Van Cauwenbergh R, Robberecht HJ, Deelstra
A. Measurement of the daily dietary calcium and magne-sium intake in Belgium, using duplicate portion sampling. Z Lebensm Unters Forsch 1995; 201: 213-217.
42. Fourth Swiss Nutrition Report (Vierter schweizerischer Erna¨hrungsbericht). Bern: Bundesamt fu¨r Gesundheit. 1998: 18-50.
43. Walti MK, Zimmermann MB, Spinas GA, Jacob S, Hurrell RF. Dietary magnesium intake in type 2 diabetes. Eur J Clin Nutr 2002; 56:409-414.
44. Department of Health. Dietary Reference Intakes. 6 th ed. Taipei, 2003.
45. Liu JF, Lo FL, Wang TY, Cheng CM, Shaw NS, Kao MD, Chung CY, Huang CJ. Analysis of Vitamin E, Selenium, and other nutrition in planned balanced diets in Taiwan. Nutr Sci J 2002; 27: 221-231.
46. Singh RB, Rastogi V, Singh R, Niaz MA, Srivastav S, Aslam M, Singh NK, Moshir M, Postiglione A. Magnesium and antioxidant vitamin status and risk of complications of ageing in an elderly urban population. Magnes Res 1996; 9: 299-306.
47. Kohlmeier M, Thefeld W, Stelte W, Grimm R, Hauber A, Hunchen K, Reuter U, Saupe J, Schek A, Kubler W. Versorgung Erwachsener mit Mineral-stoffen und Spurenelementen in der Bundesrepublik Deutschland. In: K€ubler W, Andersen HJ, Heeschen W(Eds.), Vera-Schriftenreihe Band V Wissen-schaftlicher Fachverlag Dr Fleck, Niederkleen, 1995.
48. Schimatschek HF, Rempis R. Prevalence of hypo-magnesaemia in an unselected German population of 16,000 individuals. Magnes. Res 2001; 14: 283-290. 49. Rosolova H, Mayer O Jr, Reaven GM. Insulin-mediated
glucose disposal is decreased in normal subjects with relatively low plasma magnesium concentrations. Metabol Clin Exp 2000; 49: 418-420.
50. Fung TT, Manson JE, Solomon CG, Liu S, Willett WC, Hu FB. The association between magnesium intake and fasting insulin concentration in healthy middle-aged women. J Am Coll Nutr 2003; 22: 533-538.
51. Barbagallo M, Gupta RK, Dominguez LJ, Resnick LM. Cellular ionic alterations with age: relation to hypertension and diabetes. J Am Geriatrics Soc 2000; 48:1111-1116. 52. Paolisso G, Sgambato S, Pizza G, Passariello N, Varricchio
M, D'Onofrio F. Improved insulin response and action by chronic magnesium administration in aged NIDDM subjects. Diabetes Care 1989; 12:265-269.
53. Paolisso G, Scheen A, Cozzolino D, Di Maro G, Varricchio M, D'Onofrio F, Lefebvre PJ. Changes in glucose turnover parameters and improvement of glucose oxidation after 4-week magnesium administration in elderly non insulin dependent (type II) diabetic patients. J Clin Endocrinol Metab 1994; 78:1510-1514.