Elevated lactate dehydrogenase activity and increased cardiovascular mortality in arsenic-endemic areas in southwestern Taiwan
Ya-Tang Liaoa, b, c, Chien-Jen Chenb,c, Wan-Fen Lia, Ling-Yi Hsuc, Li-Yu Tsaid, Yeou-Lih Huangd, Chien-Wen Suna, Wei J. Chenb,e*, Shu-Li Wanga, f*
a Division of Environmental Health and Occupational Medicine, National Health Research Institutes, Taiwan, b Graduate Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University, Taiwan, c Genomics Research Center, Academia Sinica, Taiwan, d Department of Medical Laboratory Science and Biotechnology, Kaohsiung Medical University, Taiwan, e Genetic Epidemiology Core Laboratory, National Taiwan University Center for Genomic Medicine, Taiwan,f Department of Public Health, College of Public Health, China Medical University, Taichung, Taiwan
Addresses for correspondence:
Dr. Wei J. Chen, Graduate Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University, 17 Xu-Zhou Road, Taipei 100, Taiwan; TEL. +886 (0)2-33668010; Fax: +886 (0)2-33668004; E-mail:
Dr. Shu-Li Wang , Division of Environmental Health and Occupational Medicine, National Health Research Institutes, 35, Keyan Road, Zhunan Town, Miaoli County 350, Taiwan, Tel.: +886 (0)37-246166 ext. 36509; Fax: +886 (0)37-587406; E-mail: [email protected]
Abstract
Arsenic ingestion has been linked to increasing global prevalence of and mortality from cardiovascular disease (CVD); arsenic can be removed from drinking water to reducte related health effects. Lactate dehydrogenase (LDH) is used for the evaluation of acute arsenic toxicity in vivo and in vitro, but it is not
validated for the evaluation of long-term, chronic arsenic exposure. The present study
examined the long-term effect of chronic arsenic exposure on CVD and serum LDH
levels, after consideration of genetic susceptibility and arsenic metabolism capacity. A
total of 380 subjects from an arseniasis-endemic area and 303 from a non-endemic
area of southwestern Taiwan were recruited in 2002. Eight functional polymorphisms
in PON1, PON2, AS3MT, GSTO1, and GSTO2 were assessed for genetic susceptibility
in relation to the arsenic-related LDH elevation. Various urinary arsenic species were
analyzed using high-performance liquid chromatography (HPLC) and hydride
generation systems. Fasting plasma was used for quantitative determination of the
total LDH activity. A significant dose-response relationship was observed between
arsenic exposure and LDH elevation, independent of genetic polymorphisms and
urinary arsenic profiles (P < 0.001). Furthermore, abnormal LDH elevation was
associated with CVD mortality after adjustment for Framingham risk scores for
1.39–31.07). LDH was elevated in subjects with arsenic exposure in a dose-dependent manner. LDH is a marker of arsenic toxicity associated with CVD mortality. Results
of this study have important implications for use in ascertaining long-term arsenic
exposure risk of CVD.
Keywords
Arsenic exposure, Lactate dehydrogenase, Cardiovascular mortality, Paraoxonase,
Arsenic methyltransferase, Glutathione S-transferases omega
Introduction
Arsenic is a potent but modifiable environmental pollutant that has been linked to the
increasing prevalence of cardiovascular disease (CVD), a major cause of excess
mortality worldwide (Navas-Acien et al., 2005); arsenic can be removed from
drinking water to reduce related health effects.Nonetheless, little was known
about the excess mortality from arsenic when genetic factors were considered,
notwithstanding individual susceptibility to arsenic toxicity (NRC, 1999) due to
differences in age, sex, and arsenic metabolism (Vahter, 2000; Watanabe et al., 2001).
Inter-individual differences in the speciation and amounts of arsenic metabolites are
reported among subjects chronically exposed to arsenic (Loffredo et al., 2003) and
significant genetic determinants of arsenic metabolism are supported by
格式化: 行距: 2 倍行高
epidemiologic evidence (Chung et al., 2002). Arsenic-induced CVD may result from
the inter-correlations among genetic, environmental, and toxicological mechanisms.
The total level of plasma lactate dehydrogenase (LDH), which measures all five isoforms (LDH1 to LDH5) present in the blood, is usually used in the diagnosis and treatment of acute tissue damage, cardiac diseases such as acute myocardial infarction (Galen et al., 1975), tumors of the lung (Turan et al., 2007), and liver diseases such as acute viral hepatitis, cirrhosis, and metastatic carcinoma of the liver or kidneys (Chu et al., 2002). In addition, LDH has also been shown to predict in-hospital mortality among subjects with severe underlying physical illnesses*{when used in addition to assessment of functional status} (Davis et al., 1995). [Dear Author: *I do not understand why you have the phrase in brackets as it does not seem to have anything to do with the rest of the sentence. Is the revision of
the phrase in brackets accurate according to your meaning?] Furthermore, LDH has
also been widely used for the evaluation of acute arsenic toxicity in vivo and in vitro
(Petrick et al., 2000; Peraza et al., 2003; Saad et al., 2006; Tajima et al., 2010); but the
association between chronic arsenic exposure and the level of serum LDH remains
unclear. One recent cross-sectional study showed that the total LDH level in the
plasma correlated positively with the concentration of arsenic in drinking water
evaluation, we suggest a link between arsenic-related LDH elevation and the mortality
of CVD.
Not until recently have genes encoding enzymes responsible for arsenic metabolism
been cloned and characterized (Whitbread et al., 2003; Wood et al., 2006). They
include AS3MT and GSTO. The AS3MT gene directly encodes a cytosolic enzyme,
arsenic methyltransferase, which catalyzes a multi-step process to convert inorganic
arsenic to monomethyl arsenical (MMA) and dimethyl arsenical (DMA) (Lin et al.,
2002). The polymorphism M287T (rs17885947) in AS3MT is considered to be
related to inter-individual variation in arsenic metabolism (Drobna et al., 2004). Glutathione S-transferases (GSTs) are phase II detoxification enzymes that catalyze
the conjugation of reduced glutathione to a wide variety of endogenous and
exogenous electrophilic compounds (Townsend and Tew, 2003). The GST omega
class is a subfamily of GSTs shown to be identical with human monomethylarsonic
acid (MMA) reductase, the rate-limiting enzyme for biotransformation of inorganic
arsenic. Polymorphisms of the GST omega genes are associated with intracellular
thiol status and the arsenic biotransformation efficiency in liver cells (Tanaka-Kagawa
et al., 2003). A140D (rs4925) in GSTO1 and N142D (rs156697) in GSTO2 have
been identified as common polymorphisms in different ethnic populations (Mukherjee et al., 2006; Polimanti et al., 2011). A140D has also been shown to
reduce enzyme activity and *inhibit inorganic arsenic biotransforming capacity (Tanaka-Kagawa et al., 2003).[Dear Author: *Is this what you mean?]
High-density lipoprotein (HDL) is postulated to prevent the development of
atherosclerosis by inhibiting the oxidation of low-density lipoprotein (LDL). Human
paraoxonase (PON1) is a serum esterase/lactonase transported on HDL particles and
the major determinant of the antioxidant action of HDL (Aviram et al., 1998). Both in
in vitro and animal studies using PON1-knockout mice showed that PON1 prevented LDL oxidation and is, therefore, a protective enzyme against the development of
atherosclerosis (Mackness et al., 1991; Watson et al., 1995; Shih et al., 1998; Li et al.,
2009). The PON1 gene has two common polymorphisms, L55M (rs854560) and
Q192R (rs662), within the coding region resulting in amino acid substitutions, and one common polymorphism, C-108T (rs705379), in the promoter region, *{which have all} have been associated with PON1 levels (Adkins et al., 1993; Leviev and James, 2000; Furlong et al., 2005). [Dear Author: *Is the phrase in
brackets accurate?] A148G (rs12026) and C311S (rs6954345) in PON2 have also
been identified and are considered to be associated with lipid profiles including levels of total cholesterol, low-density lipoprotein, and apolipoprotein A1 and B (Boright et al., 1998; Hegele, 1999). Animal study has demonstrated that
atherosclerosis is induced by arsenic in drinking water through alteration of lipid
metabolism (Cheng et al., 2011). Additionally, our previous studies showed significant genetic variation in the PON gene cluster, as well as in PON1 activity,
electrocardiographic abnormalities, and increased intima medium thickness of the
carotid artery in subjects who had long-term arsenic exposure (Li et al., 2009; Liao et
al., 2009). The present study examined the long-term effect of chronic arsenic
exposure and serum LDH levels on CVD after consideration of individual genetic
susceptibility ???*{to arsenic and CVD, and urinary arsenic metabolism.} [Dear
Author: The previous sentence is not clear and I could not guess what you meant, *especially the words in brackets. What is “urinary arsenic metabolism”? Do you
mean “urinary arsenic metabolites”?] Our results are beneficial to the identification of
a biomarker for long-term arsenic exposure risk assessment.
Materials and methods Study areas
The study included a community-based cohort comparing the population from a
previously arseniasis-endemic area in southwestern Taiwan to a non-exposed
population recruited from a documented non-endemic area in the same county. The
subjects shared similar ages, genders, and ecological statuses at the time of data
collection. The arseniasis-endemic area of Homei, Fusin, and Hsinming villages in
Putai Township on the southwestern coast of Taiwan were described previously (Chen
et al., 1985; Chen et al., 1995; Tseng et al., 2003). In short, residents in the study area
consumed contaminated artesian well water for decades since the 1910s, and the
arsenic concentration in the water as measured in the early 60s ranged from 0.035 to
1.14 ppm, with a median of 0.78 ppm (Chen et al., 1962; Kuo, 1964). The total daily
intake of arsenic by the locals was estimated as high as 1 mg (Blackwell, 1961), until
a municipal water supply system was installed and commonly functional in the early
1970s. The arsenic concentration of tap water supplied in the study area was then
reduced to less than 0.01 ppm (Chen and Chen, 1975). The non-endemic area was
Chiali Township where the arsenic concentration of well water was under the
detection limits according to surveys conducted in 1960s and 1970s (Kuo, 1964; Lo et
al., 1977). The climate, ethnic background (Han Chinese), degree of urbanization and
socioeconomic status were similar between Putai and Chiali.
Study subjects
In January 2002, approximately 490 subjects who still resided in the study area were invited to participate in this study. Frequency matching of the age and gender distributions (from 35- to 85- years old, in 5-year age groups) was
and 303 residents were enrolled for the present study respectively. Among these subjects, 380 and 296 from the endemic and non-endemic areas, respectively, who had complete biochemical measurements were included in the final analysis of mean baseline characteristics (Table 1) and baseline characteristics stratified by LDH levels (Table 2). Urinary arsenic species (Table 3) and DNA (Table 4) were analyzed in 343 and 291 subjects with these data from endemic and non-endemic areas, respectively. Multivariable association of abnormal LDH elevation was conducted in 316 and 275 subjects from endemic and non-endemic areas who had complete data (Table 5). Only subjects from endemic areas were included in the final analysis of association of abnormal LDH elevation with causes of death (Table 6).
Data collection
Physical measurements, including blood pressure, electrocardiograms and carotid artery imaging were collected. In addition, standardized personal interviews were conducted by public health nurses using a structured questionnaire to acquire baseline and socioeconomic characteristics, artesian well water usage, residential history, lifestyle variables, and personal and family histories of hypertension, diabetes, and CVD. Cumulative arsenic exposure (in
ppm-years) was calculated from the arsenic concentration in artesian well water (ppm)
and the duration of water consumption (years). The cause of death for a deceased
subject, as classified according to the 9th revision of International Classification of Diseases (ICD-9), was retrieved from the database of the National Death Certification
System referenced to the subject’s national identification number, with the approval
from the Department of Health in Taiwan. All deaths that occurred during the time of
study (from January 1, 2002 to December 31, 2009) were counted. The study protocol
was approved by the Human Ethical Committee of the National Health Research
Institutes in Taiwan and informed consent was obtained from each participant before
starting the study.
Biochemical analysis
Fasting venous blood samples were collected for quantifying the serum total LDH
levels using a Beckman SYNCHRON LX20 System (Beckman Coulter, Fullerton, CA,
USA) according to the manufacture’s protocol. The detection limit for the LDH assay
was 5 IU/L. Plasma glucose, serum levels of glycated hemoglobin A1c (HbA1c),
lipid profiles (high density lipoprotein, low density lipoprotein, cholesterol, and triglycerides), liver function enzymes (aspartate aminotransferase and alanine aminotransferase), *microalbumin, uric acid and creatinine were also analyzed
when the subjects participated in a health examination in 2002.[Dear Author: Do you mean “albumin” here? “Microalbumin” is usually measured in the urine.]
Urinary samples were collected from each subject for arsenic species analyses.
Subjects were asked not to consume seafood three days before urine collection.
Arsenite (As(III)), arsenate (As(V)), MMA, and DMA were quantified using
high-performance liquid chromatography (HPLC) coupled with flow injection atomic
absorption spectrometry. The HPLC system consisted of a solvent delivery pump
(PU-1580, Jasco, Tokyo, Japan) and a silica-based anion-exchange column (Nucleosil
10 SB, 250 mm×4.6 mm; Phenomenex, CA, USA) with a guard column packed with
the same material. A flow injection analysis system (FIAS-400, PerkinElmer, CT,
USA) was designed as the on-line interface to the continuous hydride generation
system (Analyst 100, PerkinElmer) used in this study. With this method, the within-
and between-day precision (coefficient of variation, CV%) for As(III), As(V), MMA,
and DMA range from 1.0% to 3.7%. Furthermore, the recoveries for As(III), As(V),
MMA, and DMA were 99.0, 98.9, 99.0, and 99.0%, while the detection limits were
0.75, 1.47, 1.19, and 0.76 μg/L, respectively. The primary methylation index was
defined as the ratio between MMA and iAs (As(III) + As(V)) levels, and the
secondary methylation index was defined as the ratio between DMA and MMA.
格式化: 字型: 非粗體
SNP selection and genotyping
DNA was collected in 2002 and analyzed in 2005 in both the endemic and non-endemic areas . Eight functional polymorphisms for genotyping analysis were selected from the National Center for Biotechnology Information single nucleotide polymorphism (SNP) database based on their implications in arsenic metabolism, cardiovascular disease and minor allele frequency. These SNPs included C-108T (rs705379), L55M (rs854560) and Q192R (rs662) of PON1; A148G (rs12026) and C311S (rs6954345/rs7493) of PON2; M287T (rs17885947) of AS3MT; A140D (rs4925) of GSTO1; and N142D (rs156697) of GSTO2. Genomic DNA was extracted from buffy coat using commercial kit (PUREGENE®,
Gentra, Minneapolis, MN, USA). The AS3MT M287T polymorphism was determined
using a commercially designed TaqMan SNP Genotyping Assay (Applied Biosystems,
Foster City, CA, USA). All other genotypes were determined by polymerase chain
reaction amplification followed by polymorphism-specific restriction enzyme
digestion analysis (RFLP-PCR). For the A140D in GSTO1, N142D in GSTO2, and
M287T in AS3MT, all specimens were repeated by RFLP-PCR. The kappa statistics were about 0.88 and the samples with discordant results were sent for DNA sequencing for genotype validation. For other SNPs, 20% of the samples were run in duplicate and all of the kappa statistics were > 0.94. All the samples
were relabeled for the experiments and the researchers were blinded to individual identities and results.
Statistical analysis
Differences between the study subjects in endemic (Putai) and non-endemic (Chiali)
areas were assessed for the association between demographic characteristics and
cardiovascular risk factors. Continuous variables were expressed as means with
standard deviations and evaluated using Student’s t-test or the Wilcoxon rank-sum test.
Categorical variables were expressed as proportions and compared using the
chi-square test or Fisher’s exact test. Histograms were used to present LDH
distributions for the endemic and non-endemic areas. Since no clinical threshold is currently set for abnormal serum LDH level, we defined an abnormal LDH level as
an elevation of two standard deviations above the mean LDH level of the subjects in
the non-endemic area. Characteristics among subjects including urinary arsenic
species were compared between groups with normal and abnormal LDH levels stratified by arsenic-endemic and non-endemic populations.Univariate analyses
of LDH elevation in relation to genetic polymorphisms were performed based on
logistic regression. A multiple regression model was then utilized to evaluate the
Arsenic exposure in the endemic area was stratified into two categories by the median
level in reference to the subjects in non-endemic area. All-cause and CVD-caused
deaths including cardiovascular disease (ICD-9: 390-429) and cerebrovascular disease (ICD-9: 430-438) were identified as mortalities of interest. Multivariate Cox regression analysis was used to determine the hazard ratios for abnormal
elevation of LDH levels and mortality of interest after adjustment for conventional
risk factors, including age, gender, cigarette smoking, hypertension, and diabetes
mellitus (D’Agostino et al., 2008), using the Framingham risk score for 10-year
cardiovascular disease as a covariate. P-values less than 0.05 were considered
statistically significant. All statistical analyses were conducted using SAS 9.2 (SAS,
Inc., Cary, NC).
Results
Descriptive statistics of study participants
The average characteristics of the study populations are summarized in Table 1. The
numbers of study subjects in endemic area and non-endemic area were 380 and 296,
respectively. Demographic data showed that there was no significant difference in the
age and gender profiles between the two areas. However, the percentage of subjects
LDH levels for the non-endemic and endemic areas were 295.06 (IU/L) and 408.43 (IU/L), respectively.Additionally, the subjects in the endemic area had higher
aspartate aminotransferase, alanine aminotransferase, LDL levels, and body mass
index; their diastolic blood pressure, HDL, and uric acid levels were significantly
lower, when compared to the subjects from the non-endemic area.
[Table 1 here]
The Figure shows the histograms of the LDH levels among the study subjects. A great majority of the subjects (n=296; 77.8%) from the endemic area had LDH levels greater than 300 (IU/L). On the other hand, only 38.6% of subjects (n=117) from the non-endemic area had elevated LDH levels (>300 IU/L), while most of the subjects had LDH levels that ranged from 200 to 300 IU/L.
[Figure here]
Univariate and multivariate associations with LDH elevation
The association of characteristics of study subjects and abnormal LDH elevation stratified by endemic and non-endemic areas is shown in Table 2. As mentioned
格式化: 行距: 2 倍行高
above, the critical threshold for abnormal LDH elevation in this study was calculated as the mean LDH level of subjects in the non-endemic plus two standard deviations, or 450 (IU/L). Based on this criterion, 12 out of 296 subjects from the non-endemic area and 97 out of 380 subjects from the endemic area were identified as having abnormal LDH elevation. Subjects with abnormal LDH elevation were significantally older than those with without LDH elevation in both the endemic and non-endemic areas. In addition, significantly elevated systolic blood pressure (SBP), aspartate aminotransferase (AST), alanine aminotransferase (ALT), and body mass index (BMI) and *{significanlty more microalbuminuria} were also seen in subjects with abnormal LDH levels in the endemic area but not in non-endemic area. [Dear Author: *Is this phrase in brackets correct? Is the previous sentence edited correctly?]
[Table 2 here]
Table 3 shows a comparison of urinary arsenic species between subjects with normal and abnormal LDH levels stratified by arsenic-endemic and
non-endemic areas. In subjects from the endemic area, urinary arsenic species of As(III), iAs, the sum of iAs and MMA, and the sum of iAs, MMA, and DMA were significantly higher in subjects with abnormal LDH elevation compared
with that of subjects with normal LDH levels.
[Table 3 here]
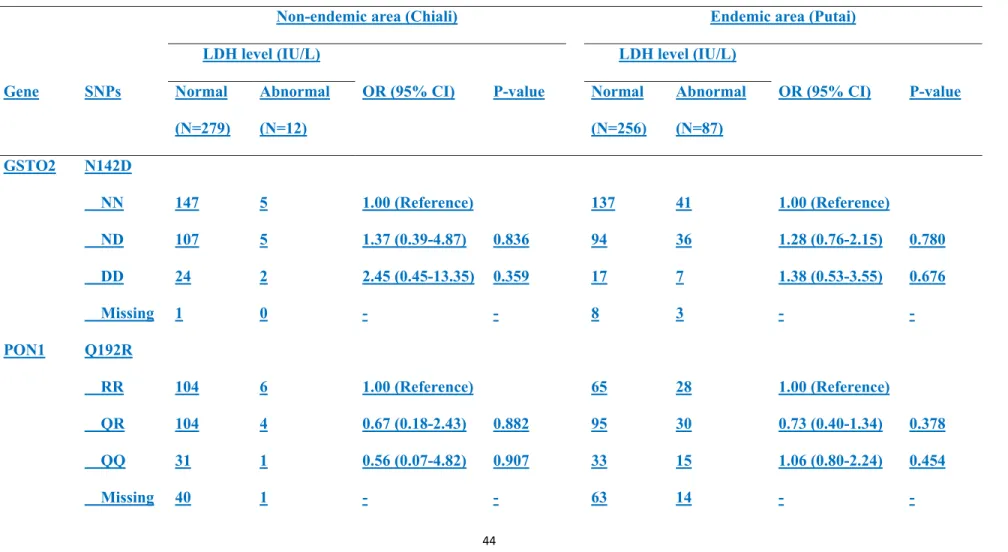
Eight functional polymorphisms, i.e., C-108T, L55M and Q192R in PON1, A148G
and C311S in PON2, M287T in AS3MT, A140D in GSTO1, and N142D in GSTO2,
were screened for their association with abnormal LDH elevation. The
Hardy-Weinberg equilibrium was calculated for the subjects with normal LDH levels
in both endemic and non-endemic areas. The A140D and C-108T polymorphisms
showed a significant departure from equilibrium; M287T and L55M had a minor allele frequency less than 5% and were thus removed from further analysis. Genotypic frequencies of C311S showed a significant association with abnormal LDH
elevation in the endemic area, but not in the non-endemic area. Compared with the SS
genotype, the CC genotype of C311S had a 5.91-time increased risk (95% CI:
1.70–20.55, p=0.005) of abnormal LDH elevation in the endemic area (Table 4).
[Table 4 here]
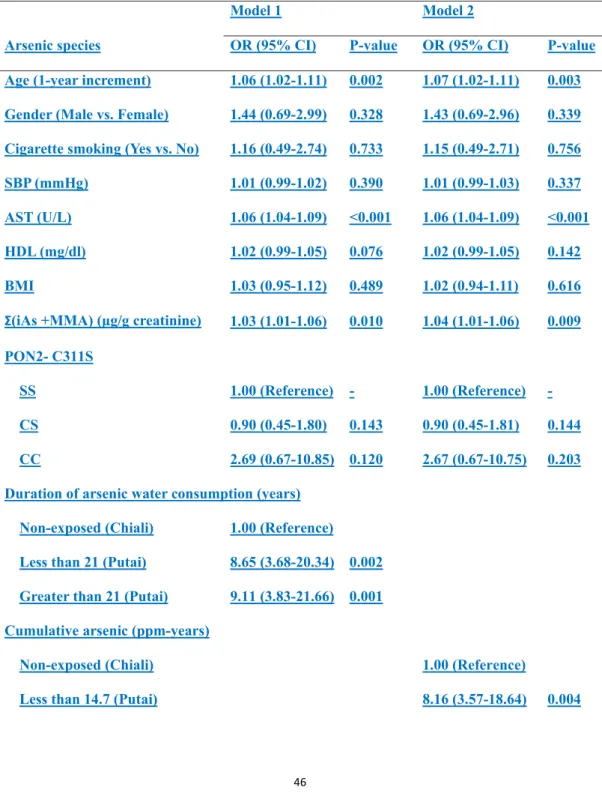
Multivariable analyses of the association between chronic arsenic exposure and abnormal LDH elevation are shown in Table 5. Arsenic exposure was evaluated by duration of arsenic water consumption (Model 1) and cumulative arsenic
(Model 2). Compared t with subjects from the non-endemic area, subjects in the endemic area with short durations (less than 21 years) and long durations ( more than 21 years) of arsenic exposure had significantly increased odds ratios of abnormal LDH elevation, OR= 8.65 (95% CI: 3.68–20.34, p=0.002) and 9.11 (95% CI: 3.83–21.66, p=0.001), respectively. Similar results were also observed when cumulative arsenic exposure was considered. The odds ratios for abnormal LDH elevation for short (<14.7 ppm-years) and long cumulative exposures (>14.7 ppm-years) were 8.16 (95% CI: 3.57–18.64, p=0.004), and 9.59 (95% CI:
3.75–24.53, p=0.002), respectively. Moreover, variables including age, AST, and urinary levels of iAs and MMA were also associated with increased odds ratios of abnormal LDH elevation independent of other covariates in both models. In addition, gender, cigarette smoking, SBP, HDL, BMI and CC genotype of C311S polymorphism in PON2 showed increased risks for abnormal LDH elevation but were not statistically significant.
[Table 5 here]
Association between abnormal LDH elevation and mortality
During the 7-year follow-up, 45 subjects died from all-cause mortality including 43 subjects from physical illness- related deaths: 17 from neoplasms (ICD-9:
140–239), 10 from CVD, including cardiovascular disease (ICD-9: 390–429) and cerebrovascular disease (ICD-9: 430–438), 6 from respiratory disease (ICD-9: 460–519), 5 from endocrine disease (ICD-9: 240–279), and 4 from other systemic diseases including 1 from infectious disease, 1 from genitourinary disease, and 2 from external causes. One subject died from an accident and one from a
homicide.[Dear Author: Is the previous sentence accurate according to your meaning?]Eight subjects from the non-endemic area died from physical illness- related deaths including 4 from neoplasms, 2 from CVD, 1 from respiratory disease and 1 from infection. Because of the diversity and limited number of deaths, the non-endemic area was not included in the final analysis of mortality.
[Dear Author: Is the previous sentence accurate according to your meaning?] Only
the associations of abnormal LDH elevation with all-cause mortality, excluding the accidental death and homicide, which are not conventional natural causes, and CVD-caused mortality in subjects in the arsenic-endemic area are
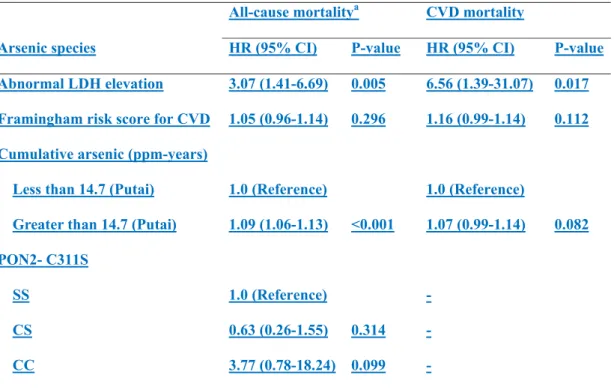
summarized in Table 6. After adjustment for cumulative arsenic exposure and conventional risk factors for CVD by the Framingham risk score for 10-year CVD, abnormal LDH elevation was associated with increased risks of all-cause mortality (HR=3.07, 95% CI: 1.41–6.69) and CVD mortality (HR=6.56, 95% CI: 1.39–31.07). Furthermore, a longer cumulative exposure to arsenic (>14.7
ppm-years) was also associated with increased risk of all-cause (HR=1.09, 95% CI: 1.06–1.13) and CVD mortality (HR=1.07, 95% CI: 0.99-1.14). In addition, patients with the CC genotype of C311S polymorphism in PON2 showed an increased risk for all-cause mortality with marginal statistical significance (HR=3.77, 95% CI: 0.78-18.24), but this was not analyzed in CVD mortality because of the small sample size (all subjects with CVD mortality carried SS genotypes).
[Table 6 here]
Discussion
The present study examined the association between chronic arsenic exposure and
LDH elevation. Previously, Brancaccio et al. (Brancaccio et al., 2008) reported that
factors associated with LDH levels included age, gender, race, muscle mass, physical
activity, and climatic conditions. Our study further demonstrated that urinary arsenic
species were associated with LDH elevation, especially As(III) and MMA, after
adjustment for the reported conventional risk factors. We also examined the sum of
iAs and MMA, both of which are indicators of inorganic arsenic exposure
(Navas-Acien et al., 2008; Longnecker, 2009). Multiple logistic regression analysis
showed a link between urinary arsenic consisting of iAs and MMA and abnormal
LDH elevation, independent of chronic arsenic exposure as well as underlying health status including the SBP, AST, HDL and BMI.
Additionally, we observed an increased risk of elevated LDH from PON2 C311S
genotypes in the arsenic-exposed subjects, suggesting that PON2 genotype could
affect arsenic toxicity as reflected in LDH activity. In addition, subjects with
missing genotyping were evaluated and showed no significant association with abnormal LDH levels, assuring the independent extent of missing data on genotyping. [Dear Author: Is the previous sentence accurate according to your
meaning? It is not very clear.] The 311C allele in PON2 is associated with increased
risks of coronary artery disease, myocardial infarction, and also diabetic
nephropathy (Pinizzotto et al., 2001; Martinelli et al., 2004; Jalilian et al., 2008); it is also reported to be associated with lower PON activity (Stoltz et al., 2009). Recent studies have demonstrated that low PON1 activity is associated with increased risks of arsenic-induced atherosclerosis (Li et al., 2009) and is a
successful predictor of cardiovascular diseases such as myocardial infarction and stroke (Mackness et al., 2003; Bhattacharyya et al., 2008). Our data indicate the significance of the PON2 C311S polymorphism during the pathogenesis of CVD,
especially after chronic arsenic exposure, and therefore, suggest that cardiovascular
Furthermore, we found that the risk of LDH elevation occurred in a dose-response
relationship. The highest risk for abnormal LDH elevation was found among subjects
with markedly long arsenic exposure, while a low risk was found among those never
exposed. The elevation of LDH in the study areas also showed a statistically
significant association with CVD mortality. The same was found after adjustment by
the Framingham risk score for 10-year CVD risk factors, including age, gender,
cigarette smoking, hypertension, and diabetes. While this finding could support for an
underlying causal relationship between CVD and arsenic poisoning irrespective of
other conventional risk factors, it is essential to note that LDH should be routinely
monitored for clinical examinations, particularly in arsenic endemic areas in many
parts of the world. Previous epidemiologic studies have demonstrated liver toxicity
and *{elevated liver function enzymes in the serum} in a dose-response relationship with arsenic exposure (Mazumder, 2005; Islam et al., 2011). [Dear Author: *If you mean “AST and ALT” here, please use these enzyme names instead of
this phrase in brackets.] In the current study, AST and ALT levels were
significantly higher among arsenic exposed subjects compared with those from the non-endemic area. AST levels were also associated with abnormal LDH elevation, especially among subjects in the arsenic-endemic area. These findings might be helpful for the early detection of arsenic-related liver disease.
格式化: 字型: 非粗體
We note several limitations, which should be considered when interpreting the results.
First, the data were collected decades after the cessation of arsenic exposure.
Individual assessment of arsenic exposure at the time when exposure was *on-going was not conducted. [Dear Author: *Is this what you mean?] Instead, the exposure assessment in this study was performed in an ecological manner. Prior epidemiologic studies have demonstrated a positive correlation of cumulative arsenic exposure and the body burden of inorganic arsenic in Taiwan, even after residents had not consumed arsenic contaminated water for decades (Hsueh et al., 1998; Huang et al., 2007). Urinary arsenic data were presented as an indicator for accumulation of body burden as individual exposure data, however, the specific mechanism awaits further investigation.
Second, LDH is a general marker for cell toxicity and organ damage. An elevation of
the LDH level may indicate the overall health condition caused by arsenic toxicity, but may not be specific enough to pinpoint the target tissue(s). This study investigated the association between arsenic-related LDH elevation and all-cause mortality coded as physical illness-related deaths, an inherently heterogeneous category.The total LDH level could only be used as a preclinical
indicator in this study because the LDH isoform subtype was not specified. Clinical
heterogeneity could result in dismissing this finding when different pathological
格式化: 行距: 2 倍行高
conditions are considered. Recently, other cardiac markers such as creatine kinase
MB (CK-MB), B-type natriuretic peptide (BNP) and troponins have been favored over LDH because of its low specificity.[Dear Author: Is the previous sentence accurate according to your meaning?]
Nonetheless, if we restricted the mortality to cardiovascular disease only, the findings remained similar and the adjusted hazard ratio reached 6.56 (95% CI: 1.39–31.07). One particular study of 11,746 subjects in Bangladesh with current exposure to arsenic-contaminated drinking water showed a significantly increased risk of CVD mortality during an average of 6.6 years of follow-up (Chen et al., 2011). In addition, a synergistic effect between cigarette smoking and arsenic exposure was identified in CVD mortality, especially from heart disease. However, we could not evalutate this synergistic association in the current study because of the limited sample size.
Third, the Framingham risk score was applied to handle multiple comparison issues
when a number of conventional risk factors were to be considered simultaneously.
Although the 95% confidence interval for CVD mortality still falls into a significant
range, the strength of this association requires further modification based on the
effective number of subjects. Overall, a long-term follow-up study of subjects at the
current level of exposure would improve the strength our results.
Some other factors that might have influenced the arsenic methylation profiles were not considered in this study. It is very difficult to control for the influence of nutritional status and dietary intake. In addition, the distribution of certain rare alleles, including C-108T and L55M in PON1, A140D in GSTO1, and M287T in AS3MT, could not be reliably determined in our sample. The possibility of individual variability in arsenic methylation and its impact on the pathogenesis of CVD cannot be ruled out. Therefore, a further study with a larger sample size with sufficient control for other confounders that may be directly related to arsenic risks is warranted for the evaluation of the relations of genetic variants to abnormal LDH elevation.
In conclusion, this study provides a new perspective of the factors associated with
abnormal LDH elevation among subjects with chronic arsenic exposure. LDH is an
arsenic toxicity marker associated with ??*an increased incidence of all-cause and CVD death. [Dear Author: *Is this what you mean?] Our findings emphasize the long-term effects of arsenic exposure, which may lead to excessive CVD and physical illness- related deaths.
Acknowledgements
This work was supported by the National Health Research Institute (grants
格式化: 行距: 2 倍行高
EO-094-PP-11, EO-095-PP-07, and EO-096-PP-07) and National Taiwan University
(grant 100R0001). We thank the clinicians and nurses at Hsin-Ying Branch Hospital,
Beimen, Tainan, for their support with the health examinations of the study subjects.
We are also deeply indebted to all members of the Blackfoot Disease Team for their
assistance in data collection and management.
Conflict of interest
References
[Dear Author: You need to use journal abbreviations in your new references.]
Adkins, S., Gan, K. N., Mody, M., and La Du, B. N., 1993. Molecular basis for the polymorphic forms of human serum paraoxonase/arylesterase: glutamine or arginine at position 191, for the respective A or B allozymes. American journal of human genetics 52, 598-608.
Aviram, M., Rosenblat, M., Bisgaier, C. L., Newton, R. S., Primo-Parmo, S. L., La Du,
B. N., 1998. Paraoxonase inhibits high-density lipoprotein oxidation and
preserves its functions. A possible peroxidative role for paraoxonase. J Clin
Invest 101, 1581-1590.
Bhattacharyya, T., Nicholls, S. J., Topol, E. J., Zhang, R., Yang, X., Schmitt, D., Fu, X., Shao, M., Brennan, D. M., Ellis, S. G., Brennan, M. L., Allayee, H., Lusis, A. J., and Hazen, S. L.,2008. Relationship of paraoxonase 1 (PON1) gene polymorphisms and functional activity with systemic oxidative stress and cardiovascular risk. JAMA : the journal of the American Medical Association 299, 1265-1276.
Blackwell, R. Q.,1961. Estimation total arsenic ingested by residents in the endemic
blackfoot area. J Formosan Med. Assoc. 60, 1143-1144.
格式化: 字型: 非粗體 格式化: 字型: 非粗體
Boright, A. P., Connelly, P. W., Brunt, J. H., Morgan, K., and Hegele, R. A., 1998. Association and linkage of LDLR gene variation with variation in plasma low density lipoprotein cholesterol. Journal of human genetics 43, 153-159. Brancaccio, P., Maffulli, N., Buonauro, R., and Limongelli, F. M., 2008. Serum
enzyme monitoring in sports medicine. Clinics in Sports Medicine 27, 1-18, vii.
Chen, C. J., Chuang, Y. C., Lin, T. M., Wu, H. Y., 1985. Malignant neoplasms among
residents of a blackfoot disease-endemic area in Taiwan: high-arsenic artesian
well water and cancers. Cancer Res 45, 5895-5899.
Chen, C. J., Hsueh, Y. M., Lai, M. S., Shyu, M. P., Chen, S. Y., Wu, M. M., Kuo, T. L.,
Tai, T. Y., 1995. Increased prevalence of hypertension and long-term arsenic
exposure. Hypertension 25, 53-60.
Chen, K. P., Wu, T. C., Wu, T. C., 1962. Epidemiologic studies on blackfoot disease in
Taiwan. 3. Physicochemical characteristics of drinking water in endemic
blackfoot disease areas. Memoirs of College of Medicine (National Taiwan
University) 8, 115-129.
Chen, W. Y., Chen, K. P., 1975. Study on arsenic artesian well water and blackfoot
disease progress. In Taichung, Taiwan: Taiwan Provincial Institute of
Environmental Sanitation.
Chen, Y., Graziano, J. H., Parvez, F., Liu, M., Slavkovich, V., Kalra, T., Argos, M., Islam, T., Ahmed, A., Rakibuz-Zaman, M., Hasan, R., Sarwar, G., Levy, D., van Geen, A., and Ahsan, H., 2011. Arsenic exposure from drinking water and mortality from cardiovascular disease in Bangladesh: prospective cohort study. BMJ 342, d2431.
Cheng, T. J., Chuu, J. J., Chang, C. Y., Tsai, W. C., Chen, K. J., and Guo, H. R., 2011. Atherosclerosis induced by arsenic in drinking water in rats through altering lipid metabolism. Toxicology and applied pharmacology 256, 146-153.
Chu, W. W., Dieter, R. S., Stone, C. K., 2002. A review of clinically relevant cardiac
biochemical markers. WMJ 101, 40-48.
Chung, J. S., Kalman, D. A., Moore, L. E., Kosnett, M. J., Arroyo, A. P., Beeris, M.,
Mazumder, D. N., Hernandez, A. L., Smith, A. H., 2002. Family correlations of
arsenic methylation patterns in children and parents exposed to high
concentrations of arsenic in drinking water. Environ Health Perspect 110,
729-733.
D'Agostino, R. B., Sr., Vasan, R. S., Pencina, M. J., Wolf, P. A., Cobain, M., Massaro,
care: the Framingham Heart Study. Circulation 117, 743-753.
Davis, R. B., Iezzoni, L. I., Phillips, R. S., Reiley, P., Coffman, G. A., and Safran, C., 1995. Predicting in-hospital mortality. The importance of functional status information. Medical care 33, 906-921.
Drobna, Z., Waters, S. B., Walton, F. S., LeCluyse, E. L., Thomas, D. J., and Styblo, M., 2004. Interindividual variation in the metabolism of arsenic in cultured primary human hepatocytes. Toxicology and applied pharmacology 201, 166-177.
Furlong, C. E., Cole, T. B., Jarvik, G. P., Pettan-Brewer, C., Geiss, G. K., Richter, R. J., Shih, D. M., Tward, A. D., Lusis, A. J., and Costa, L. G., 2005. Role of paraoxonase (PON1) status in pesticide sensitivity: genetic and temporal determinants. Neurotoxicology 26, 651-659.
Galen, R. S., Reiffel, J. A., Gambino, R., 1975. Diagnosis of acute myocardial
infarction. Relative efficiency of serum enzyme and isoenzyme measurements.
JAMA 232, 145-147.
Hegele, R. A., 1999. Paraoxonase genes and disease. Annals of medicine 31, 217-224.
Hsueh, Y. M., Huang, Y. L., Huang, C. C., Wu, W. L., Chen, H. M., Yang, M. H., Lue, L. C., and Chen, C. J., 1998. Urinary levels of inorganic and organic
arsenic metabolites among residents in an arseniasis-hyperendemic area in Taiwan. Journal of toxicology and environmental health. Part A 54, 431-444. Huang, Y. K., Tseng, C. H., Huang, Y. L., Yang, M. H., Chen, C. J., and Hsueh, Y.
M., 2007. Arsenic methylation capability and hypertension risk in subjects living in arseniasis-hyperendemic areas in southwestern Taiwan. Toxicology and applied pharmacology 218, 135-142.
Islam, K., Haque, A., Karim, R., Fajol, A., Hossain, E., Salam, K. A., Ali, N., Saud, Z. A., Rahman, M., Sultana, P., Hossain, M., Akhand, A. A., Mandal, A., Miyataka, H., Himeno, S., and Hossain, K. ,2011. Dose-response relationship between arsenic exposure and the serum enzymes for liver function tests in the individuals exposed to arsenic: a cross sectional study in Bangladesh. Environ Health 10, 64.
Jalilian, A., Javadi, E., Akrami, M., Fakhrzadeh, H., Heshmat, R., Rahmani, M., Bandarian, F., 2008. Association of cys 311 ser polymorphism of
paraoxonase-2 gene with the risk of coronary artery disease. Arch Iran Med 11, 544-549.
Karim, M. R., Salam, K. A., Hossain, E., Islam, K., Ali, N., Haque, A., Saud, Z. A.,
Yeasmin, T., Hossain, M., Miyataka, H., Himeno, S., Hossain, K., 2010.
lactate dehydrogenase activity. The Science of the total environment 409,
278-283.
Kuo, T. L., 1964. Arsenic Content of Artesian Well Water in Endemic Area of Chronic
Arsenic Poisoning In Institute of Pathology, pp. 7-13. National Taiwan
University.
Leviev, I., and James, R. W., 2000. Promoter polymorphisms of human paraoxonase PON1 gene and serum paraoxonase activities and
concentrations. Arteriosclerosis, thrombosis, and vascular biology 20, 516-521. Li, W. F., Sun, C. W., Cheng, T. J., Chang, K. H., Chen, C. J., Wang, S. L., 2009. Risk
of carotid atherosclerosis is associated with low serum paraoxonase (PON1)
activity among arsenic exposed residents in Southwestern Taiwan. Toxicology
and applied pharmacology 236, 246-253.
Liao, Y. T., Li, W. F., Chen, C. J., Prineas, R. J., Chen, W. J., Zhang, Z. M., Sun, C. W.,
Wang, S. L., 2009. Synergistic effect of polymorphisms of paraoxonase gene
cluster and arsenic exposure on electrocardiogram abnormality. Toxicol Appl
Pharmacol 239, 178-183.
Lin, S., Shi, Q., Nix, F. B., Styblo, M., Beck, M. A., Herbin-Davis, K. M., Hall, L. L.,
Simeonsson, J. B., Thomas, D. J., 2002. A novel S-adenosyl-L-methionine:
10795-10803.
Lo, M. C., Hsen, Y. C., Lin, B. K., 1977. Arsenic content of underground water in
Taiwan: Second report., pp. 1-17. Taiwan Provincial Institute of Environmental
Sanitation, Taichung, Taiwan.
Loffredo, C. A., Aposhian, H. V., Cebrian, M. E., Yamauchi, H., Silbergeld, E. K.,
2003. Variability in human metabolism of arsenic. Environ Res 92, 85-91.
Longnecker, M. P., 2009. On confounded fishy results regarding arsenic and diabetes.
Epidemiology 20, 821-823; discussion e821-822.
Mackness, M. I., Arrol, S., Durrington, P. N., 1991. Paraoxonase prevents
accumulation of lipoperoxides in low-density lipoprotein. FEBS Lett 286,
152-154.
Mackness, B., Durrington, P., McElduff, P., Yarnell, J., Azam, N., Watt, M., and Mackness, M., 2003. Low paraoxonase activity predicts coronary events in the Caerphilly Prospective Study. Circulation 107, 2775-2779.
Martinelli, N., Girelli, D., Olivieri, O., Stranieri, C., Trabetti, E., Pizzolo, F., Friso, S., Tenuti, I., Cheng, S., Grow, M. A., Pignatti, P. F., Corrocher, R., 2004. Interaction between smoking and PON2 Ser311Cys polymorphism as a determinant of the risk of myocardial infarction. Eur J Clin Invest 34, 14-20. Mazumder, D. N. ,2005. Effect of chronic intake of arsenic-contaminated water
on liver. Toxicology and applied pharmacology 206, 169-175.
Mukherjee, B., Salavaggione, O. E., Pelleymounter, L. L., Moon, I., Eckloff, B. W., Schaid, D. J., Wieben, E. D., and Weinshilboum, R. M., 2006.
Glutathione S-transferase omega 1 and omega 2 pharmacogenomics. Drug metabolism and disposition: the biological fate of chemicals 34, 1237-1246. Navas-Acien, A., Sharrett, A. R., Silbergeld, E. K., Schwartz, B. S., Nachman, K. E.,
Burke, T. A., Guallar, E., 2005. Arsenic exposure and cardiovascular disease: a
systematic review of the epidemiologic evidence. Am J Epidemiol 162,
1037-1049.
Navas-Acien, A., Silbergeld, E. K., Pastor-Barriuso, R., Guallar, E., 2008. Arsenic
exposure and prevalence of type 2 diabetes in US adults. JAMA 300, 814-822.
NRC, 1999. Arsenic in drinking water. National Academy Press, Washington, DC.
Peraza, M. A., Carter, D. E., Gandolfi, A. J., 2003. Toxicity and metabolism of
subcytotoxic inorganic arsenic in human renal proximal tubule epithelial cells
(HK-2). Cell Biol Toxicol 19, 253-264.
Petrick, J. S., Ayala-Fierro, F., Cullen, W. R., Carter, D. E., Vasken Aposhian, H., 2000.
Monomethylarsonous acid (MMA(III)) is more toxic than arsenite in Chang
human hepatocytes. Toxicol Appl Pharmacol 163, 203-207.
Paraoxonase2 polymorphisms are associated with nephropathy in Type II diabetes. Diabetologia 44, 104-107.
Polimanti, R., Piacentini, S., De Angelis, F., De Stefano, G. F., and Fuciarelli, M., 2011. Human GST loci as markers of evolutionary forces: GSTO1*E155del and GSTO1*E208K polymorphisms may be under natural selection induced by environmental arsenic. Disease markers 31, 231-239.
Saad, S. Y., Alkharfy, K. M., Arafah, M. M., 2006. Cardiotoxic effects of arsenic
trioxide/imatinib mesilate combination in rats. J Pharm Pharmacol 58, 567-573.
Shih, D. M., Gu, L., Xia, Y. R., Navab, M., Li, W. F., Hama, S., Castellani, L. W.,
Furlong, C. E., Costa, L. G., Fogelman, A. M., Lusis, A. J., 1998. Mice lacking
serum paraoxonase are susceptible to organophosphate toxicity and
atherosclerosis. Nature 394, 284-287.
Stoltz, D. A., Ozer, E. A., Recker, T. J., Estin, M., Yang, X., Shih, D. M., Lusis, A. J., and Zabner, J., 2009. A common mutation in paraoxonase-2 results in impaired lactonase activity. The Journal of biological chemistry 284, 35564-35571.
Tajima, H., Yoshida, T., Ohnuma, A., Fukuyama, T., Hayashi, K., Yamaguchi, S.,
Ohtsuka, R., Sasaki, J., Tomita, M., Kojima, S., Takahashi, N., Kashimoto, Y.,
Pulmonary injury and antioxidant response in mice exposed to arsenate and
hexavalent chromium and their combination. Toxicology 267, 118-124.
Tanaka-Kagawa, T., Jinno, H., Hasegawa, T., Makino, Y., Seko, Y., Hanioka, N., Ando,
M., 2003. Functional characterization of two variant human GSTO 1-1s
(Ala140Asp and Thr217Asn). Biochem Biophys Res Commun 301, 516-520.
Townsend, D., Tew, K., 2003. Cancer drugs, genetic variation and the
glutathione-S-transferase gene family. Am J Pharmacogenomics 3, 157-172.
Tseng, C. H., Chong, C. K., Tseng, C. P., Hsueh, Y. M., Chiou, H. Y., Tseng, C. C.,
Chen, C. J., 2003. Long-term arsenic exposure and ischemic heart disease in
arseniasis-hyperendemic villages in Taiwan. Toxicol Lett 137, 15-21.
Turan, O., Akkoclu, A., Coker, C., 2007. Plasma LDH levels as a Prognostic factor for
evaluating stages and types of local advanced and metastatic NSCLC. Journal of
thoracic oncology 2.
Vahter, M., 2000. Genetic polymorphism in the biotransformation of inorganic arsenic
and its role in toxicity. Toxicol Lett 112-113, 209-217.
Watanabe, C., Inaoka, T., Kadono, T., Nagano, M., Nakamura, S., Ushijima, K.,
Murayama, N., Miyazaki, K., Ohtsuka, R., 2001. Males in rural Bangladeshi
communities are more susceptible to chronic arsenic poisoning than females:
Watson, A. D., Berliner, J. A., Hama, S. Y., La Du, B. N., Faull, K. F., Fogelman, A.
M., Navab, M., 1995. Protective effect of high density lipoprotein associated
paraoxonase. Inhibition of the biological activity of minimally oxidized low
density lipoprotein. J Clin Invest 96, 2882-2891.
Whitbread, A. K., Tetlow, N., Eyre, H. J., Sutherland, G. R., Board, P. G., 2003.
Characterization of the human Omega class glutathione transferase genes and
associated polymorphisms. Pharmacogenetics 13, 131-144.
Wood, T. C., Salavagionne, O. E., Mukherjee, B., Wang, L., Klumpp, A. F., Thomae,
B. A., Eckloff, B. W., Schaid, D. J., Wieben, E. D., Weinshilboum, R. M., 2006.
Human arsenic methyltransferase (AS3MT) pharmacogenetics: gene
Table 1. The average characteristics, including cardiovascular risk factors, of the subjects in the arsenic-endemic and non-endemic areas in southwestern Taiwan.
Factor Non-endemic area
(Chiali) (N=296) Endemic area (Putai) (N=380) P-value Age (years) 61.5 (10.1) 61.2 (8.9) 0.759 Gender (Male, %) 119 (39.3) 164 (43.3) 0.292 Cigarette smoking (%) 38 (12.8) 80 (21.1) 0.005 Alcohol consumption (%) 26 (8.7) 47 (12.4) 0.122 SBP (mmHg) 138.9 (18.3) 136.9 (22.3) 0.207 DBP (mmHg) 83.8 (10.8) 80.2 (13.8) <0.001 LDH (IU/L) 295.1 (73.5) 408.4 (224.8) <0.001 AST (U/L) 22.6 (14.0) 26.4 (16.8) 0.001 ALT (U/L) 15.2 (10.9) 21.7 (21.4) <0.001 Glucose (mg/dl) 110.6 (30.5) 112.0 (49.8) 0.669 HbA1c (%) 5.9 (1.1) 6.3 (4.7) 0.146 Cholesterol (mg/dl) 201.9 (37.9) 203.0 (37.7) 0.723 Triglyceride (mg/dl) 132.2 (89.3) 137.0 (88.4) 0.488 HDL (mg/dl) 44.7 (12.5) 40.5 (12.7) <0.001 LDL (mg/dl) 124.9 (36.1) 139.8 (40.3) <0.001 BMI (kg/m^2) 24.4 (3.2) 25.3 (3.7) <0.001 Microalbumin (mg/dl) 3.0 (11.7) 5.7 (24.0) 0.074 UA (mg/dl) 7.5 (2.3) 6.6 (3.2) <0.001
SBP: systolic blood pressure; DBP: diastolic blood pressure, LDH: lactate dehydrogenase, AST: aspartate aminotransferase; ALT: alanine aminotransferase; HbA1c: glycated hemoglobin A1, HDL: high density lipoprotein; LDL: low density lipoprotein; BMI: Body mass index; UA: uric acid
Table 2. Characteristics of study subjects stratified by LDH levels in arsenic-endemic and non-endemic areas in southwestern Taiwan
Factor
Non-endemic area (Chiali) Endemic-area (Putai)
LDH levels P-value LDH levels P-value Normal (N=284) Abnormal (N=12) Normal (N=283) Abnormal (N=97) Age (years) 61.1 (10.1) 69.9 (6.16) 0.003 60.6 (9.0) 63.1 (8.3) 0.015 Gender (Male, %) 109 (38.4) 7 (58.3) 0.166 124 (43.82) 40 (41.67) 0.713 Cigarette smoking (%) 36 (12.9) 1 (8.3) 1.000 57 (20.14) 23 (23.71) 0.457 Alcohol consumption (%) 24 (8.54) 1 (8.3) 1.000 36 (12.72) 11 (11.34) 0.722 SBP (mmHg) 138.9 (18.2) 142.2 (20.82) 0.538 135.4 (20.1) 141.2 (22.6) 0.018 DBP (mmHg) 83.8 (10.7) 83.8 (13.04) 0.993 79.4 (13.9) 82.2 (13.5) 0.096 AST (U/L) 21.7 (10.7) 43.5 (42.07) 0.100 23.6 (11.0) 34.6 (25.7) <0.001 ALT (U/L) 14.8 (9.4) 24.6 (28.60) 0.260 19.6 (16.5) 28.0 (30.9) 0.012 Glucose (mg/dl) 110.37 (30.3) 18.9 (24.20) 0.834 110.0 (49.9) 117.8 (48.8) 0.179 HbA1c (%) 5.9 (1.1) 6.1 (1.64) 0.726 6.3 (5.4) 6.3 (1.7) 0.929 Cholesterol (mg/dl) 202.0 (38.0) 199.8 (37.47) 0.840 204.0 (37.7) 199.8 (37.6) 0.337 Triglyceride (mg/dl) 132.3 (89.3) 129.3 (94.27) 0.908 140.3 (93.7) 127.2 (69.9) 0.207 HDL (mg/dl) 44.6 (12.6) 47.9 (10.66) 0.364 40.3 (13.0) 41.1 (11.7) 0.613 LDL (mg/dl) 125.2 (36.3) 117.2 (34.10) 0.454 141.8 (41.2) 134.0 (37.1) 0.106 BMI (kg/m^2) 24.5 (3.1) 22.6 (4.97) 0.222 25.0 (3.7) 26.3 (3.9) 0.008 Microalbumin (mg/dl) 3.5 (14.9) 1.7 (3.4) 0.668 4.0 (11.4) 6.5 (20.9) 0.079 UA (mg/dl) 7.4 (2.2) 8.6 (3.27) 0.220 6.6 (3.5) 6.5 (2.0) 0.753
Critical threshold for abnormal LDH elevation was defined as an LDH activity greater than 450 (IU/L); SBP: systolic blood pressure; DBP: diastolic blood pressure, LDH: lactate dehydrogenase, AST: aspartate aminotransferase; ALT: alanine aminotransferase; HbA1c: glycated hemoglobin A1c, HDL: high density lipoprotein; LDL: low density lipoprotein; BMI: Body mass index; UA: uric acid
Table 3. Urinary arsenic species of study subjects stratified by LDH levels in arsenic-endemic and non-endemic areas in southwestern Taiwan
Non-endemic area (Chiali) Endemic-area (Putai)
Factor Normal (N=279) Abnormal (N=12) P-value Normal (N=256) Abnormal (N=87) P-value As(III) (μg/g creatinine) 2.07 (2.98) 1.82 (3.21) 0.779 3.89 (6.32) 7.20 (12.01) 0.019 As(V) (μg/g creatinine) 2.73 (3.14) 3.26 (3.43) 0.573 2.65 (3.04) 3.55 (8.31) 0.340
iAs (As(III) + As(V) )(μg/g creatinine) 4.08 (4.62) 5.08 (5.64) 0.834 6.54 (7.58) 10.75 (15.66) 0.022
MMA (μg/g creatinine) 2.96 (3.12) 4.68 (7.87) 0.465 4.09 (4.13) 5.43 (8.00) 0.149
Σ(iAs +MMA) (μg/g creatinine) 7.76 (6.45) 9.77 (10.28) 0.517 10.63 (9.92) 16.18 (19.82) 0.017
DMA (μg/g creatinine) 42.78 (34.78) 40.94 (22.51) 0.856 34.42 (26.35) 44.76 (49.98) 0.078
Σ(iAs + MMA + DMA) (μg/g creatinine) 50.55 (38.10) 50.70 (31.84) 0.989 45.07 (31.58) 60.94 (60.22) 0.025
PMI (MMA/iAs) 0.84 (0.96) 1.13 (1.57) 0.545 0.84 (0.64) 0.85 (0.90) 0.956
SMI (DMA/MMA) 23.80 (23.10) 21.38 (13.54) 0.570 14.31 (21.53) 22.03 (41.24) 0.098
Data are reported as means (S.D); Critical threshold for abnormal LDH elevation was defined as an LDH activity greater than 450 (IU/L); PMI: Primary methylation index; SMI: Secondary methylation index
Table 4. The association of genotypes in GSTO2, PON1 and PON2 polymorphisms and abnormal LDH elevation in the subjects from arsenic-endemic (Putai) and non-endemic (Chiali) areas in southwestern Taiwan
Non-endemic area (Chiali) Endemic area (Putai)
LDH level (IU/L) LDH level (IU/L)
Gene SNPs Normal (N=279)
Abnormal (N=12)
OR (95% CI) P-value Normal (N=256) Abnormal (N=87) OR (95% CI) P-value GSTO2 N142D NN 147 5 1.00 (Reference) 137 41 1.00 (Reference) ND 107 5 1.37 (0.39-4.87) 0.836 94 36 1.28 (0.76-2.15) 0.780 DD 24 2 2.45 (0.45-13.35) 0.359 17 7 1.38 (0.53-3.55) 0.676 Missing 1 0 - - 8 3 - - PON1 Q192R RR 104 6 1.00 (Reference) 65 28 1.00 (Reference) QR 104 4 0.67 (0.18-2.43) 0.882 95 30 0.73 (0.40-1.34) 0.378 QQ 31 1 0.56 (0.07-4.82) 0.907 33 15 1.06 (0.80-2.24) 0.454 Missing 40 1 - - 63 14 - -
PON2 A148G AA 200 9 1.00 (Reference) 121 38 1.00 (Reference) AG 72 3 0.93 (0.24-3.52) 0.952 82 37 1.44 (0.84-2.45) 0.755 GG 4 0 - - 7 5 2.28 (0.68-7.59) 0.240 Missing 3 0 - - 46 7 - - C311S SS 188 9 1.00 (Reference) 136 46 1.00 (Reference) CS 65 3 0.96 (0.25-3.67) 0.956 62 21 1.00 (0.55-1.82) 0.996 CC 10 0 0.94 (0.05-17.36) 0.976 4 8 5.91 (1.70-20.55) 0.005 Missing 16 0 - - 54 12 - -
Table 5. Multivariable association of abnormal LDH elevation among subjects in arsenic-endemic and non-endemic areas in southwestern Taiwan
Model 1 Model 2
Arsenic species OR (95% CI) P-value OR (95% CI) P-value
Age (1-year increment) 1.06 (1.02-1.11) 0.002 1.07 (1.02-1.11) 0.003
Gender (Male vs. Female) 1.44 (0.69-2.99) 0.328 1.43 (0.69-2.96) 0.339
Cigarette smoking (Yes vs. No) 1.16 (0.49-2.74) 0.733 1.15 (0.49-2.71) 0.756
SBP (mmHg) 1.01 (0.99-1.02) 0.390 1.01 (0.99-1.03) 0.337
AST (U/L) 1.06 (1.04-1.09) <0.001 1.06 (1.04-1.09) <0.001
HDL (mg/dl) 1.02 (0.99-1.05) 0.076 1.02 (0.99-1.05) 0.142
BMI 1.03 (0.95-1.12) 0.489 1.02 (0.94-1.11) 0.616
Σ(iAs +MMA) (μg/g creatinine) 1.03 (1.01-1.06) 0.010 1.04 (1.01-1.06) 0.009
PON2- C311S
SS 1.00 (Reference) - 1.00 (Reference) -
CS 0.90 (0.45-1.80) 0.143 0.90 (0.45-1.81) 0.144
CC 2.69 (0.67-10.85) 0.120 2.67 (0.67-10.75) 0.203
Duration of arsenic water consumption (years)
Non-exposed (Chiali) 1.00 (Reference)
Less than 21 (Putai) 8.65 (3.68-20.34) 0.002
Greater than 21 (Putai) 9.11 (3.83-21.66) 0.001
Cumulative arsenic (ppm-years)
Non-exposed (Chiali) 1.00 (Reference)
Greater than 14.7 (Putai) 9.59 (3.75-24.53) 0.002 Critical threshold for abnormal LDH elevation was defined as 450 (IU/L)
1 2
Table 6. The association of abnormal LDH elevation with mortality among subjects in arsenic-endemic area by cox proportional hazards analysis
All-cause mortalitya CVD mortality
Arsenic species HR (95% CI) P-value HR (95% CI) P-value
Abnormal LDH elevation 3.07 (1.41-6.69) 0.005 6.56 (1.39-31.07) 0.017 Framingham risk score for CVD 1.05 (0.96-1.14) 0.296 1.16 (0.99-1.14) 0.112 Cumulative arsenic (ppm-years)
Less than 14.7 (Putai) 1.0 (Reference) 1.0 (Reference)
Greater than 14.7 (Putai) 1.09 (1.06-1.13) <0.001 1.07 (0.99-1.14) 0.082 PON2- C311S
SS 1.0 (Reference) -
CS 0.63 (0.26-1.55) 0.314 -
CC 3.77 (0.78-18.24) 0.099 -
Critical threshold for abnormal LDH elevation was defined as 450 (IU/L);
Mortality data was calculated from the date of study entry in 2002 to year 2009 according to ICD-9
1
Figure 2
Histogram of the LDH levels of subjects from arsenic-endemic and non-endemic 3
areas in southwestern Taiwan 4
[Dear Author: If you have only one figure, you don’t need to number it.]