Prevalence of hypercholesterolemia and its related factors in middle-aged Taiwanese adults—a hospital-based study
6
0
0
全文
(2) 86. Hypercholesterolemia in Middle-aged Adults. Table 1. Comparison of clinical characteristics between subjects with and without hypercholesterolemia by the t test p Variable Normal Hypercholesterolemia. Age (yr) 2 BMI (kg/m ) Systolic pressure (mmHg) Diastolic pressure (mmHg) Fasting glucose (mmol/L) Total cholesterol (mmol/L) Triglyceride (mmol/L) Uric acid (µmol/L). 49.5 23.9 124.0 80.8 5.4 4.4 1.3 335.8. 6.9 3.5 17.6 11.2 1.3 0.5 1.6 82.4. Hospital for preventive services from April to September, 2002. MATERIALS AND METHODS. This was a cross-sectional hospital-based study. We analyzed the health status of adults who voluntarily visited the China Medical College Hospital in Taichung for preventive services from April to September 2000. All individuals aged 40 to 64 were candidates. In total, 2745 people were included in this study (39% were men and 61% were women). The mean age was 50.2 6.9 years. The items of preventive services included a self-administrated questionnaire, history taking, physical examination, and measurement of fasting blood biochemistry. Subjects who had never smoked or had quit smoking before the time of preventive services were defined as nonsmokers. Subjects who smoked at the time of preventive services were defined as smokers. Subjects who did not drink alcohol or drank alcohol occasionally were classified as nondrinkers. Subjects who habitually drank alcohol were classified as drinkers. Blood pressure was measured in the sitting position by a mercury sphygmomanometer. Blood samples were obtained in the morning after a 12hour overnight fast. A number of biochemical markers, such as total serum cholesterol, triglyceride, fasting glucose, and uric acid were analyzed by a biochemical autoanalyser within 4 hours after collecting the samples (Hitachi 73615, Tokyo, Japan) at the Department of Clinical Laboratory of the China Medical College Hospital.. 51.2 24.5 127.8 83.7 5.7 6.0 1.8 359.0. 6.9 3.4 18.3 11.9 1.8 0.7 2.1 86.2. 0.0001 0.0001 0.0001 0.0001 0.0005 0.0001 0.0001 0.0001. Body mass index (BMI) was measured as follows: weight (kg) height (m)2. BMI ≥ 27 was defined as obese [5]. Hypercholesterolemia was defined as a total serum cholesterol level ≥ 5.18 mmol/L and hypertriglyceridemia was defined as a triglyceride level ≥ 1.70 mmol/L [6]. Hyperglycemia was defined as a fasting glucose level ≥ 6.05 mmol/L or when subjects had a history of diabetes [7]. Subjects were considered hypertensive if the blood pressure reading exceeded 140 mmHg systolically and/or 90 mmHg diastolically or subjects had a history of hypertension [8]. Hyperuricemia was defined as a serum uric acid level ≥ 416.5 µmol/L in men and ≥ 386.8 µmol/L in women [9]. Statistical analyses were performed by the SAS package (version 6.12, SAS Institute Inc., Cary, North Carolina) and included the t test, the chi-square test and logistic regression. A p value < 0.05 was considered statistically significant. RESULTS. The mean level of total serum cholesterol was 5.04 0.95 mmol/L in men and 5.03 0.98 mmol/L in women (p > 0.05). The prevalence of hypercholesterolemia was 40.3% in men and 39.6% in women (p > 0.05). There were significant differences in the mean age, body mass index, systolic blood pressure, diastolic blood pressure, fasting glucose, triglyceride and uric acid levels between the normal and hypercholesterolemia groups (p < 0.001) (Table 1). The clinical characteristics of hypercholesterolemia in middle-aged adults analyzed by the.
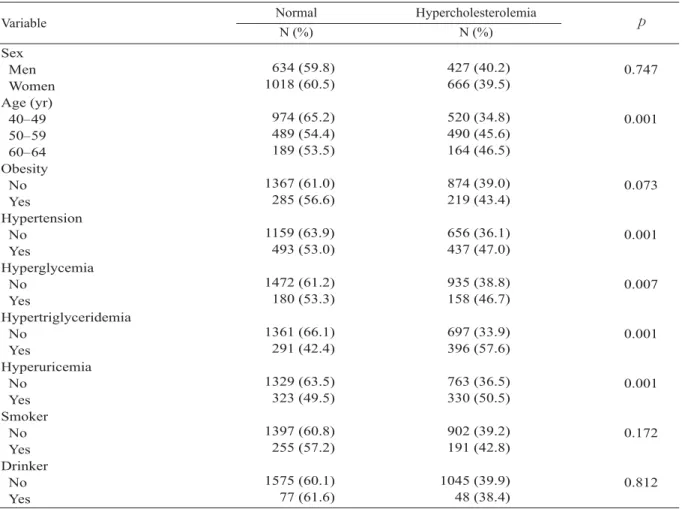
(3) Chih-Hsueh Lin, et al.. 87. Table 2. Comparison of clinical characteristics between subjects with and without hypercholesterolemia by the chi-square test. Variable Sex Men Women Age (yr) 40–49 50–59 60–64 Obesity No Yes Hypertension No Yes Hyperglycemia No Yes Hypertriglyceridemia No Yes Hyperuricemia No Yes Smoker No Yes Drinker No Yes. Normal N (%). Hypercholesterolemia N (%). 634 (59.8) 1018 (60.5). 427 (40.2) 666 (39.5). 0.747. 974 (65.2) 489 (54.4) 189 (53.5). 520 (34.8) 490 (45.6) 164 (46.5). 0.001. 1367 (61.0) 285 (56.6). 874 (39.0) 219 (43.4). 0.073. 1159 (63.9) 493 (53.0). 656 (36.1) 437 (47.0). 0.001. 1472 (61.2) 180 (53.3). 935 (38.8) 158 (46.7). 0.007. 1361 (66.1) 291 (42.4). 697 (33.9) 396 (57.6). 0.001. 1329 (63.5) 323 (49.5). 763 (36.5) 330 (50.5). 0.001. 1397 (60.8) 255 (57.2). 902 (39.2) 191 (42.8). 0.172. 1575 (60.1) 77 (61.6). 1045 (39.9) 48 (38.4). 0.812. Table 3. The related factors of hypercholesterolemia in middle-aged adults by logistic regression analysis 95% CI Variable OR. Age 1.03 1.02 1.04** Hypertension 1.22 1.02 1.44* Hyperglycemia 1.00 0.78 1.27 Hypertriglyceridemia 2.33 1.94 2.81** Hyperuricemia 1.38 1.15 1.67** *p < 0.05, **p < 0.001. OR = odds ratio; CI = confidence interval.. chi-square test are shown in Table 2. The prevalence of hypercholesterolemia increased with age (p < 0.01). The statistically significant related factors of hypercholesterolemia were age, hypertension, hyperglycemia, hypertriglyceridemia and hyperuricemia. The results of logistic regression analysis for hypercholesterolemia are displayed in Table 3. Five independent variables were analyzed. p. according to the results of the t test and the chisquare test. After controlling for the covariables, the significantly related factors of hypercholesterolemia were age (odds ratio [OR] = 1.03, 95% confidence interval [CI] = 1.02 – 1.04, p < 0.001), hypertension (OR = 1.22, 95% CI = 1.02 – 1.44, p < 0.05), hypertriglyceridemia (OR = 2.33, 95% CI = 1.94 – 2.81, p < 0.001) and hyperuricemia (OR = 1.38, 95% CI = 1.15 – 1.67, p < 0.001). No significant association was found between hypercholesterolemia and hyperglycemia. DISCUSSION. Although the volunteers were not representative of Taiwanese adults and the sample size was small, we hoped that this study could still provide basic information for further studies on the epidemiology of hypercholesterolemia in Taiwanese adults..
(4) 88. Hypercholesterolemia in Middle-aged Adults. In Chou's community-based study, the prevalence of hypercholesterolemia (≥ 6.22 mmol/L) was 33.5% in men and 31.5% in women [10]. In this hospital-based study, the prevalence of hypercholesterolemia (≥ 5.18 mmol/L) was 40.3% in men and 39.6% in women (p > 0.05). The prevalence in our study was higher than that in Chou's study becasue the cholesterol level used for the definition of hypercholesterolemia in our study was lower than that used in Chou's study. Other factors related to the differences in results include the different populations studied and the different detection methods used. This study also found that the prevalence of hypercholesterolemia increases with age, which is consistent with the study by Chou et al [11]. Hypercholesterolemia, hypertriglyceridemia, obesity, essential hypertension, and hyperuricemia are common in people with insulin resistance [9,12-17]. Therefore, this notable association suggests the same pathogenesis for hypercholesterolemia, hypertriglyceridemia, glucose intolerance/diabetes mellitus, essential hypertension, and hyperuricemia [9,12-20]. In this study, hypercholesterolemia was significantly associated with hypertension, hypertriglyceridemia, and hyperuricemia. These findings further indicate that multiple metabolic disorders can often cluster within the same individual [9,12-20]. Undoubtedly, it is particularly important to determine other metabolic disorders if one metabolic disorder is detected. In conclusion, hypercholesterolemia is very common in middle-aged adults and is significantly associated with age, hypertension, hypertriglyceridemia and hyperuricemia. We suggest measuring total serum cholesterol levels when older individuals present with hypertension, hypertriglyceridemia, or hyperuricemia. REFERENCES. 1. Soons KR, Little DN, Harvey J. Cholesterol screening in the elderly: changing attitudes. Gerontology 1995;41:57-62. 2. The Lipids Research Clinics Coronary Primary Prevention Trial results. I. Reduction in incidence of. coronary heart disease. JAMA 1984;251:351-64. 3. Chen TJ, Yu BT. Report on survey of serum glucose, cholesterol, uric acid and creatinine values in adults of Taipei city. J Nephrology ROC 1995;9:109-18. 4. M a n o l i o TA , F u r b e r g C D , Wa h l PW, et al. Eligibility for cholesterol referral in communitydwelling older adults. The Cardiovascular Health Study. Ann Intern Med 1992;116:641-9. 5. Department of Health, Taiwan. http://www. doh.gov.tw/newverprog/proclaim/content.asp?class_no =25&doc_no=32 6. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001;285:2486-97. 7. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2000;23(Suppl 1):4-19. 8. Summary of 1993 World Health OrganisationInternational Society of Hypertension guidelines for the management of mild hypertension. Subcommittee of WHO/ISH Mild Hypertension Liaison committee. BMJ 1993;307:1541-6. 9. Saggiani F, Pilati S, Targher G, et al. Serum uric acid and related factors in 500 hospitalized subjects. Metabolism 1996;45:1557-61. 10. Chou P, Hsiao KJ, Lin JW, et al. Community-based survey on blood pressure, blood biochemistry and dietary habits in Pu-Li, Taiwan. Zhonghua Yi Xue Za Zhi (Taipei) 1992;50:279-87. 11. Chou P, Shaw CK, Lai MY. Community-based study on the relationship between serum cholesterol/triglyceride and dietary habits/life styles in Pu-Li, Taiwan. Zhonghua Yi Xue Za Zhi (Taipei) 1993;52:155-60. 12. Woo J, Swaminathan R, Cockram C, et al. Association between serum uric acid and some cardiovascular risk factors in a Chinese population. Postgrad Med J 1994;70:486-91. 13. Agamah ES, Srinivasan SR, Webber LS, et al. Serum uric acid and its relation to cardiovascular disease risk factors in children and young adults from a biracial community: the Bogalusa Heart Study. J Lab Clin Med 1991;118:241-9. 14. Lin CC, Li TC, Lai SW, et al. Hypertriglyceridemia and the Related Factors in Middle-Aged Adults in Taiwan. Mid Taiwan J Med 2001;6:1-6. 15. Ng KC, Lin CC, Lai SW, et al. Obesity and the Related Factors in Middle-Aged Adults in ChungHsing Village in Taiwan. Mid Taiwan J Med.
(5) Chih-Hsueh Lin, et al.. 2001;6:35-9. 16.Collantes Estevez E, Pineda Priego M, Anon Barbudo J, et al. Hyperuricemia-hyperlipidemia association in the absence of obesity and alcohol abuse. Clin Rheumatol 1990;9:28-31. 17. Vuorinen MH, Yki JH. Hyperuricemia and insulin resistance. J Clin Endocrinol Meta 1994;78:25-9. 18. Bonora E, Kiechl S, Willeit J, et al. Prevalence of. 89. insulin resistance in metabolic disorders: the Bruneck Study. Diabetes 1998;47:1643-9. 19. Tan CC, Ng KC, Lai SW, et al. The results of preventive services for adults at a medical center in Taichung. Mid Taiwan J Med 2001;6:233-7 20.Lai SW, Tan CC, Ng KC. Hepatic effects in hyperlipidemic patients. Mid Taiwan J Med 2002; 7:160-4..
(6) 90. 2000 2745 38.7%. 40. 61.3%. 4. 9. 64. 50.2. t. 6.9. 5.04. 0.95 mmol/L. 0.98 mmol/L. 40.3% (. p<0.001). 1.03. (. p<0.05). 1.22. p<0.001). 1.67. p<0.001). 95% 2.33. (. 1.38. 39.6% 1.02. 95%. (. 2.81. 5.03. 1.02 95% 95%. 1.04 1.44 1.94 1.15. 2003;8:85-90. 404. 2. 2002. 11. 8. 2003. 2. 26. 2002. 12. 18.
(7)
數據
相關文件
In the 2010/2011 academic year, there were 10 institutions of higher education with courses offered; a total of 106 schools a were providing pre-primary, primary and secondary
Analyzed by occupation, 26 774 were engaged in positions that are directly related to betting services, such as hard and soft count clerks, cage cashiers, pit bosses, casino
Analyzed by occupation, 22 669 were engaged in positions that are directly related to betting services, such as hard and soft count clerks, cage cashiers, pit bosses, casino
Analyzed by occupation, 15 213 were engaged in positions that are directly related to betting services, such as hard and soft count clerks, cage cashiers, pit bosses,
Each course at the Institute is assigned a number of units corresponding to the total number of hours per week devoted to that subject, including classwork, laboratory, and the
Income is generated from wages and salaries, interest, rent and profits. In a labour-intensive industry such as tourism, a large part of income comes from wages and salaries earned
Type case as pattern matching on values Type safe dynamic value (existential types).. How can we
y In the 2012/2013 academic year, number of higher education institutions remained at 10; a total of 71 institution were providing pre-primary, primary and secondary education, there
