well established by many large-scale studies from atomic bomb survivors [5]. The lens-es of the eylens-es are the organs most sensitive to radiation injury because of their superfi-cial location and direct contact with the x-ray beam. The relationship of cataract for-mation after cumulative doses of ionizing radiation is also documented in epidemio-logic studies from atomic bomb survivors [6]. The International Commission on Radi-ologic Protection has published threshold values for detectable lens opacities of 5 Sv for fractionated or protracted exposure and 0.5–2.0 Sv for single brief exposures [7, 8]. In recent years, many articles have discussed radiation-induced cataract among work-ers in radiologic departments or among pa-tients who have undergone repeated CT [9, 10]. On the basis of current data, the Interna-tional Commission on Radiologic Protection (ICRP 2011) has provided updated informa-tion regarding the lower threshold radiainforma-tion
The Risk of Cataract Associated
With Repeated Head and Neck
CT Studies: A Nationwide
Population-Based Study
Mei-Kang Yuan
1,2Der-Chong Tsai
3Shih-Chieh Chang
2,4Mei-Chun Yuan
5Shu-Ju Chang
6Huan-Wu Chen
7,8Hsin-Bang Leu
2,9,10,11 Yuan MK, Tsai DC, Chang SC, et al.1Department of Radiology, National Yang-Ming
University Hospital, Yi-Lan, Taiwan.
2Faculty of Medicine, School of Medicine, National
Yang-Ming University, Taipei, Taiwan.
3Department of Ophthalmology, National Yang-Ming
University Hospital, Yi-Lan, Taiwan.
4Department of Internal Medicine, National Yang-Ming
University Hospital, Yi-Lan, Taiwan.
5Department of Nursing, Meiho University, Pingtung,
Taiwan.
6Department of Industrial Management and Enterprise
Information, Aletheia University, Taipei, Taiwan.
7Department of Medical Imaging and Intervention, Chang
Gung Memorial Hospital, TaoYuan, Taiwan.
8Chang Gung University College of Medicine, TaoYuan,
Taiwan.
9Division of Cardiology, Department of Medicine, Taipei
Veterans General Hospital, Taipei, Taiwan.
10Healthcare and Management Center, Taipei
Veterans General Hospital, No. 201, Section 2, Shih-Pai Rd, Taipei 112, Taiwan. Address correspondence to H. B. Leu ([email protected]).
11Cardiovascular Research Center, School of Medicine,
National Yang-Ming University, Taipei, Taiwan.
AJR 2013; 201:626–630
0361–803X/13/2013–626 © American Roentgen Ray Society
T
he increasing use of diagnostic CT has been a worldwide trend in the past decades [1]. In the United States, about 65 million adult and 5 million pediatric CT examinations are per-formed each year [2]. The United Nations Sci-entific Committee on the Effects of Atomic Radiation has announced that 20% of the global annual radiation dose for the period 1997–2007 comes from diagnostic medical and dental radiation [3]. In Taiwan, the most updated official information reveals that there are nearly 400 CT scanners and that more than 90% of these operating CT scanners are MDCT scanners. Although CT studies ac-count for only 10% of x-ray examinations, they take up to 50% of the total medical radia-tion dose [4]. Thus, as the volume of CT in-creases, the adverse effects of their radiation elicit serious concern.Radiation hazards to the human body, in-cluding increased risk of cancer, have been Keywords: cataract, CT, radiation
DOI:10.2214/AJR.12.9652
M. K. Yuan and S. C. Chang contributed equally to this work. Received July 23, 2012; accepted after revision November 20, 2012.
OBJECTIVE. Medical radiation–induced cataracts, especially those resulting from head
and neck CT studies, are an issue of concern. The current study aimed to determine the risk of cataract associated with repeated radiation exposure from head and neck CT.
MATERIALS AND METHODS. This study used information from a random sample
of 2 million persons enrolled in the nationally representative Taiwan National Health Insur-ance Research Database. Exposed cases consisted of patients with head and neck tumor 10– 50 years old who underwent at least one CT between 2000 and 2009. The nonexposed con-trol group was composed of subjects who were never exposed to CT studies but who were matched by time of enrollment, age, sex, history of coronary artery disease, hypertension, and diabetes.
RESULTS. There were 2776 patients in the exposed group and 27,761 matched subjects in
the nonexposed group. The exposed group had higher overall incidence of cataracts (0.97% vs 0.72%; adjusted hazard ratio [HR], 1.76; 95% CI, 1.18–2.63). Further stratifying the num-ber of CT studies in the exposed group into one or two, three or four, and five or more revealed that cataract incidence increased gradually with increasing frequency of CT studies (0.79%, 0.93%, and 1.45%, respectively) (p = 0.001, adjusted for trend). Radiation exposure due to repeated head and neck CT studies was independently associated with an increased risk of developing cataracts when the cumulative CT exposure frequency involved more than four studies (adjusted HR, 2.12; 95% CI, 1.09–4.14).
CONCLUSION. Repeated exposure to head and neck CT is significantly associated
with increased risk of cataract. Yuan et al.
CT-Associated Risk of Developing Cataract Neuroradiology/Head and Neck Imaging Original Research
dose for the lens of the eye. For the induction of deleterious lens opacities, the absorbed dose is about 0.5 Gy. In the recommenda-tions for occupational exposure, the equiva-lent dose limit for the lens of the eye should be 20 mSv in a year, averaged over a defined period of 5 years, with exposure not exceed-ing 50 mSv in any sexceed-ingle year [11].
Because of the boom in radiologic exami-nations, medical radiation–induced cataract, especially that resulting from head and neck CT, is an issue that warrants further assess-ment. This population-based case-control study was conducted using the Taiwan Na-tional Health Insurance Research Database (NHIRD) to investigate the association be-tween cataract development and radiation exposure from head and neck CT.
Materials and Methods
Database
The National Health Insurance program in Tai-wan, operating since 1995, enrolls nearly all in-habitants of Taiwan (21,869,478 of 22,520,776 population by the end of 2002). The NHIRD at the National Health Research Institutes in Miaoli, Taiwan, is in charge of the entire National Health Insurance claims database and has published nu-merous extracted datasets for researchers. For in-stance, the National Health Research Institutes has released cohort datasets comprising 1,000,000 randomly sampled people who were alive in 2000 and collected all of their records from 1995 on-ward. The database is confirmed by the National Health Research Institutes as representative of the Taiwanese population. It is also one of the larg-est nationwide population-based databases in the world, with more than 270 scientific articles pub-lished using its data [12].
In this cohort dataset, each patient’s origi-nal identification number has been encrypted for confidentiality. Of note, the encrypting proce-dure is consistent such that the linkage of claims belonging to the same patient is feasible within the NHIRD datasets. These materials consist of secondary data without identification and re-leased to the public for research. Thus, this study is exempt from full review by the institutional re-view board.
Subjects
The exposed group (n = 2776) was composed of patients with newly diagnosed head, neck, or brain tumors (based on the International Classification of Diseases, Ninth Revision, Clinical Modifica-tion [ICD-9-CM] codes 140–1499 and 191–1949) who had undergone CT studies. The patients were identified from two longitudinal health insurance
databases from NHIRD. The two data subsets are composed of 2,000,000 randomly sampled bene-ficiaries and encompass the period 2000–2009 by linkage of these two datasets without overlapping data [13]. Among the CT examination codes regis-tered on the NHIRD, the CT studies performed in the patients with tumors were assumed to have fo-cused on the head and neck region. The scattered radiation doses to the eye lens from head and neck CT were much higher than those from CT stud-ies of other body parts. The exposed group might have undergone repeated CT during the diagnostic, therapeutic, and follow-up period. The nonexposed control group was composed of age- and sex-matched subjects in the National Health Insurance database who never underwent CT, on enrollment or after. Hence, there were no crossover subjects.
Variables included to balance demograph-ic characteristdemograph-ics and to control the confounding risk factor of diabetes mellitus across groups were history of coronary artery disease (ICD-9-CM codes 411.xx–414.xx), diabetes mellitus (ICD-9-CM codes 250.xx), and hypertension (ICD-9-(ICD-9-CM codes 401.xx–405.xx). In both groups, subjects who underwent intraocular surgery via procedure coding, preexisting congenital, or trauma-related cataract (ICD-9-CM codes 3660, 3662, 36620, 36621, 36622, and 36623) before enrollment were excluded. Because cataracts were not rare compli-cations in patients with ocular tumors after radio-therapy, those with ocular and orbital region tu-mors (ICD-9-CM codes 190; 1900–1909) were also excluded to reduce the confounding factor of radiotherapy. Finally, only subjects 10–50 years old were included to minimize the effect of senile cataracts. All patients were followed up until the study endpoint or December 31, 2009.
Cataract Occurrence
The endpoint of the study was the first occur-rence of cataract. In this database, the ICD-9-CM codes for cataract (ICD-9-CM codes 366.xx) did not change throughout the whole follow-up period (2000–2009), ensuring the consistency of the dis-ease registry. Subjects who met any of the following two criteria were identified as having cataract: pa-tients who underwent cataract extraction surgery, as identified by procedure codes in the National Health Insurance database; or patients who had at least two clinical visits coded as ICD-9-CM 366.xx combined with therapeutic prescription for cataracts. Statistical Analysis
An SQL server (2008, Microsoft) was used for data management and computing, and SPSS soft-ware (version 15.0, SPSS) was used for statistical analysis. All data were expressed as frequency (per-centage) or mean (± SD). Parametric continuous
data between the exposed and nonexposed groups were compared by unpaired Student t test, whereas categoric data were compared with the chi-square test and Yates correction or Fisher exact test, as ap-propriate. Freedom from cataract was assessed us-ing the Kaplan-Meier analysis, with significance based on the log-rank test. The disease-free time was calculated from the date of enrollment to the date of first diagnosis of cataract. Multivariate re-gression analysis was conducted using Cox propor-tional hazard regression analysis to evaluate wheth-er CT radiation exposure was an independent factor associated with increased risk of cataract.
Results
A sample size of 30,537 subjects, including 2776 subjects with head, neck, or brain tumor who underwent at least one CT study during the study period (exposed group), and 27,761 matched subjects who never underwent CT (nonexposed group), was obtained. There were no significant differences in age, sex, history of hypertension, diabetes mellitus, and coronary artery diseases between these two groups (Table 1).
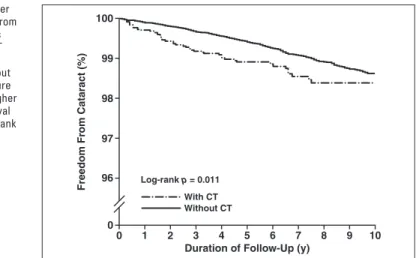
During an average follow-up period of 10 years, 27 (0.97%) patients in the exposed group and 201 (0.72%) subjects in the non-exposed group developed cataracts. Patients in the exposed group had a higher risk of de-veloping cataracts (crude hazard ratio [HR], 1.67; 95% CI, 1.12–2.50). After consider-ing variables such as age, sex, hyperten-sion, diabetes mellitus, and history of coro-nary artery disease, CT exposure remained significantly associated with a higher risk of cataract development (adjusted HR, 1.76; 95% CI, 1.18–2.63). During follow-up, the nonexposed control group had significantly higher cataract-free survival by log-rank test and Kaplan-Meier survival analyses of cata-ract incidence (Fig. 1).
For elucidating the relationship between CT exposure and cataract risk, the num-ber of CT studies was further stratified into one or two, three or four, and five or more to compare the associated risk of cataract ac-cordingly. The cataract occurrence rate in-creased gradually with the increasing num-ber of CT studies (0.79%, 0.93%, and 1.45%, respectively) (crude p for trend, 0.0483). Af-ter adjusting for these variables, the trend of increased risk of cataract associated with in-creasing CT frequency was statistically sig-nificant (adjusted p for trend, 0.001), indi-cating that radiation exposure from CT was independently associated with increased risk of cataract (Table 2).
To observe the confounding effect of radio-therapy on cataract formation, we further di-vided the radiation exposure subjects into two groups: subjects exposed to CT radiation only and subjects exposed to both CT radiation and radiotherapy. We respectively compared the cataract incidence of these two groups with nonexposed matched control subjects. The ra-diation exposure from CT only was indepen-dently associated with increased risk of cataract (adjusted HR, 2.20; 95% CI, 1.32–3.66). The cataractogenic effect in this study was mainly derived from CT in the CT radiation exposure without radiotherapy group (Table 3).
Discussion
The current study shows that patients who undergo CT have a significantly higher risk of developing cataract compared with nonex-posed subjects. Subsequent analysis shows that the frequency of CT exposure is strong-ly associated with increased risk of cataract, further suggesting the positive association be-tween CT exposure and cataract risk.
Cataracts, defined as lens opacity, are the most frequent cause of visual impairment worldwide [14]. Major risk factors include ocular trauma, intraocular surgery, diabetes mellitus, corticosteroid use, and radiation ex-posure. In the past decades, excessive doses of ionizing radiation have been documented to induce opacities in eye lenses [15]. Recent studies from atomic bomb survivors,
Cher-nobyl clean-up workers, and residents of ra-diation-contaminated buildings show that the threshold radiation dose for inducing lens opacity is lower than previously reported [16–18]. Dose estimation due to inadequate data in such populations is difficult, where-as subsequent calculated risks in these epide-miologic studies may have limitations in va-lidity. Aside from epidemiologic researches, several smaller studies that examined cata-ract in relation to self-reported exposure to CT revealed either no association or an as-sociation for posterior subcapsular cataracts at relatively low doses (0.1–0.3 Gy) [19]. However, the potential bias of self-reported questionnaires should be considered.
Experi-mental animal studies using molecular analy-sis showed that the pathogeneanaly-sis of radiation-induced cataract involves genomic damage to lens epithelium cells [20]. Theoretically, one genetically damaged cell with prolifera-tive potential can be divided into a number of abnormal lens cells. As such, the incidence of cataract increases with radiation dose, and no threshold for induction should be further evaluated (stochastic effect).
Currently, epidemiologic studies also raise the concept of a linear no-threshold model of radiation cataractogenesis [21]. Probably be-cause of the limited numbers of CT proce-dures and the lack of potential patients with radiation-induced cataract in individual
insti-TABLE 1: Demographic Data of Study Population
Demographic Characteristic Not Exposed to CT Radiation (n = 27,761) Exposed to CT Radiation (n = 2776) p
Age (y), mean ± SD 40.00 ± 8.98 40.27 ± 8.38 0.113
Male 20,108 (72.43) 2012 (72.48) 0.959
Hypertensiona 3139 (11.31) 312 (11.24) 0.914
Diabetes mellitusb 1658 (5.97) 165 (5.91) 0.891
Coronary artery diseasec 961 (3.46) 93 (3.35) 0.759
Note—Except for age and p values, data are no. (%) of patients. The p values for comparisons between the two categoric groups were determined by chi-square test with Yates correction. Continuous data were compared by unpaired Student t test. All chronic conditions were defined by administrative claims using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes.
aHypertension: ICD-9-CM codes 401.xx–405.xx. bDiabetes mellitus: ICD-9-CM codes 250.xx.
cCoronary artery disease: ICD-9-CM codes 411.xx–414.xx.
100 99 98 97 96 0 0 1 Log-rank p = 0.011 With CT 2 3 4 5
Duration of Follow-Up (y)
Freedom Fr
om Cataract (%)
6 7 8 9 10
Without CT
Fig. 1—Kaplan-Meier curves of freedom from cataract in subjects with and without CT radiation exposure. Control group without CT radiation exposure had significantly higher cataract-free survival rate (p = 0.011, log-rank test).
TABLE 2: Association Between Radiation Exposure From CT and Cataract Incidence
No. of CT Studies Cataract Incidence, No. (%) Crude Hazard Ratio (95% CI) Adjusted Hazard Ratio (95% CI)a
0 (n = 27,761) 201 (0.72) 1 (referent) 1 (referent)
1–2 (n = 1512) 12 (0.79) 1.40 (0.78–2.50) 1.61 (0.90–2.88)
3–4 (n = 645) 6 (0.93) 1.71 (0.76–3.85) 1.64 (0.73–3.69)
≥ 5 (n = 619) 9 (1.45) 2.23 (1.14–4.35) 2.12 (1.09–4.14)
Note—p for trend =0.001.
aAdjusted for age, sex, history of hypertension, diabetes mellitus, and coronary artery disease.
tutions, few studies discuss the association be-tween repeated head and neck CT and cataract formation [22]. In Taiwan, a large number of CT procedures was performed (1,268,921 CT procedures in 2008) and contributed 50.8% of the annual collective and average effective doses from medical radiation exposure [23]. The current study used two data subsets, com-posed of 2,000,000 randomly sampled benefi-ciaries, which provided thousands of CT ex-aminations with the corresponding clinical information. We retrospectively compared these data with an age-, sex-, and comorbidi-ty-matched nonexposed control group. The re-sults reveal a possible linear trend of increas-ing cataract incidence rate with increasincreas-ing number of CT studies (i.e., 1–2, 3–4, and ≥ 5 studies, with cataract incidence rate of 0.79%, 0.93%, and 1.45%, respectively, with adjusted p for trend of 0.001). Cox proportional hazard regression model analysis shows that radiation exposure from CT is independently associat-ed with an increasassociat-ed risk of developing cata-racts when cumulative CT exposure frequency is five or more (adjusted HR, 2.12; 95% CI, 1.09–4.14).
The typical effective dose of head CT is estimated to be 1–2 mSv for diagnostic sin-gle-detector CT and MDCT. The lens of the eye receives considerably high absorbed dos-es, up to 50 mGy, during head CT examina-tions [24]. According to this estimated aver-age dose for each head CT, our study results imply that the effective and absorbed radia-tion threshold doses of head and neck CT to induce cataracts may be as low as 10 mSv and 0.25 Gy. The eye lens is under direct ra-diation exposure during CT examinations. Most patients undergo head and neck CT without eye shields, because artifacts caused by eye protective shields may affect the qual-ity of images. The current study’s results in-dicate that the risk of radiation-induced cata-racts during head and neck CT examination is higher than may be previously expected, and radiology authorities should not ignore this problem. Suggestions such as low-dose head CT using iterative reconstruction and the use of protective shielding materials with mini-mal artifacts should be encouraged.
The current study has limitations. First, the case group consists of patients with head and neck tumor, and radiotherapy is one of the therapeutic options for these patients. Second-ary data from the NHIRD can only provide in-formation about the frequency of radiotherapy. The target area varies with different radiother-apy protocols, and the scattered radiation dose cannot be exactly determined in our study. The modified protocols of imaging-guided or intensity-modulated radiotherapy has sub-stantially reduced scattered radiation dose and complications over nontarget areas. Recent re-ports of radiotherapy-induced cataracts main-ly discuss radiosensitive orbital main-lymphoma or retinoblastoma [25–27]. Therefore, patients with ocular and orbital tumors are excluded in the case group. Although head and neck radio-therapy may play a role in cataract formation, the percentage of cataracts caused by scattered dose of radiotherapy is expected to be small in the current study. Second, risk factors for cataract such as previous ocular trauma and surgery were excluded, whereas diabetes mellitus was included as a matched charac-teristic in both the case and control groups. Corticosteroid use was also not assessed in this study because miscellaneous corticoste-roid prescriptions in Taiwan are difficult to extract in the NHIRD.
Despite these limitations, the current study is one of the largest population-based studies to focus on the association between cataract and repeated head and neck CT studies. The results will be valuable evidence of the medical radiation hazards to lenses of the human eyes.
In conclusion, in spite of the rapid progress in high-technology CT machines, the radia-tion dose generated by CT still contributes more than half the medical radiation to human subjects. This 10-year retrospective popula-tion-based study using the NHIRD in Taiwan shows the possible dose-dependent relationship between CT examinations and cataract occur-rence, because repeated exposure to head and neck CT is significantly associated with in-creased risk of cataract incidence. Such con-cerns suggest the need for more efforts to low-er the incidence of radiation-induced cataract.
References
1. [No authors listed]. The imaging boom. Health Aff (Millwood) 2008; 27:1466
2. Brenner DJ. Should we be concerned about the rapid increase in CT usage? Rev Environ Health 2010; 25:63–68
3. Charles M. UNSCEAR report 2000: sources and effects of ionizing radiation. United Nations Scien-tific Committee on the Effects of Atomic Radia-tion. J Radiol Prot 2001; 21:83–86
4. United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR). Effects of ionizing radiation: UNSCEAR 2006 Report to the General As-sembly, with Scientific Annexes. UNSCEAR website. www.unscear.org/docs/reports/2006/07-82087_ Report_2006_Web.pdf. Published 2006. Accessed May 10, 2013
5. Thompson DE, Mabuchi K, Ron E, et al. Cancer incidence in atomic bomb survivors. Part II. Solid tumors, 1958-1987. Radiat Res 1994; 137:S17–S67 6. Otake M, Schull WJ. A review of forty-five years
study of Hiroshima and Nagasaki atomic bomb survivors: radiation cataract. J Radiat Res (To-kyo) 1991; 32(suppl):283–293
7. International Commission on Radiological Pro-tection. 1990 Recommendations of the Interna-tional Commission on Radiological Protection: ICRP Publication 60. Ann ICRP 1991; 21:1–3 8. [No authors listed]. The 2007 Recommendations
of the International Commission on Radiological Protection: ICRP publication 103. Ann ICRP 2007; 37:1–332
9. Zammit-Maempel I, Chadwick CL, Willis SP. Ra-diation dose to the lens of eye and thyroid gland in para-nasal sinus multi-slice CT. Br J Radiol 2003; 76:418–420
10. Chodick G, Bekiroglu N, Hauptmann M, et al. Risk of cataract after exposure to low doses of ionizing radiation: a 20-year prospective cohort study among US radiologic technologists. Am J Epidemiol 2008; 168:620–631
11. Thorne MC. Regulating exposure of the lens of the eye to ionising radiations. J Radiol Prot 2012; 32:147–154
12. National Health Research Institutes. National Health Insurance Research Database: research/publications. National Health Insurance Research Database web-site. w3.nhri.org.tw/nhird/en/Research.html. Up-dated 2010. Accessed April 28, 2012
13. National Health Research Institutes. National Health TABLE 3: Radiation Exposure From CT and Radiotherapy and Association With Cataract
Hazard Ratio Exposed to CT Radiation (n = 2776) Without Radiotherapy (n = 1231)Exposed to CT Radiation Exposed to CT Radiation With Radiotherapy (n = 1545) and Radiotherapy (n = 27,761)Not Exposed to CT Radiation Crude Hazard Ratio (95% CI) 1.67 (1.12–2.50) 1.91 (1.15–3.18) 1.43 (0.78–2.62) 1 (referent) Adjusted Hazard Ratio (95% CI)a 1.76 (1.18–2.63) 2.20 (1.32–3.66) 1.38 (0.75–2.53) 1 (referent)
aAdjusted for age, sex, history of hypertension, diabetes mellitus, and coronary artery disease.
Insurance Research Database: data subsets. Na-tional Health Insurance Research Database web-site. nhird.nhri.org.tw/en/Data_Subsets.html#S3. Accessed May 13, 2013
14. Abraham AG, Condon NG, West Gower E. The new epidemiology of cataract. Ophthalmol Clin North Am 2006; 19:415–425
15. Wilde G, Sjöstrand J. A clinical study of radiation cataract formation in adult life following gamma irradiation of the lens in early childhood. Br J Ophthalmol 1997; 81:261–266
16. Minamoto A, Taniguchi H, Yoshitani N, et al. Cataract in atomic bomb survivors. Int J Radiat Biol 2004; 80:339–345
17. Worgul BV, Kundiyev YI, Sergiyenko NM, et al. Cataracts among Chernobyl clean-up workers: implications regarding permissible eye exposures.
Radiat Res 2007; 167:233–243
18. Chen WL, Hwang JS, Hu TH, Chen MS, Chang WP. Lenticular opacities in populations exposed to chronic low-dose-rate gamma radiation from radio-contaminated buildings in Taiwan. Radiat Res 2001; 156:71–77
19. Klein BE, Klein RE, Moss SE. Exposure to diag-nostic x-rays and incident age-related eye disease. Ophthalmic Epidemiol 2000; 7:61–65
20. Wolf N, Pendergrass W, Singh N, Swisshelm K, Schwartz J. Radiation cataracts: mechanisms in-volved in their long delayed occurrence but then rapid progression. Mol Vis 2008; 14:274–285 21. Ainsbury EA, Bouffler SD, Dörr W, et al.
Radia-tion cataractogenesis: a review of recent studies. Radiat Res 2009; 172:1–9
22. Michel M, Jacob S, Roger G, et al. Eye lens radiation
exposure and repeated head CT scans: a problem to keep in mind. Eur J Radiol 2012; 82:1896–1900 23. Chen TR, Tyan YS, Teng PS, et al. Population
dose from medical exposure in Taiwan for 2008. Med Phys 2011; 38:3139–3148
24. Mattsson S, Söderberg M. Radiation dose man-agement in CT, SPECT/CT and PET/CT tech-niques. Radiat Prot Dosimetry 2011; 147:13–21 25. Ferrufino-Ponce ZK, Henderson BA.
Radiothera-py and cataract formation. Semin Ophthalmol 2006; 21:171–180
26. Chodick G, Kleinerman RA, Stovall M, et al. Risk of cataract extraction among adult retinoblastoma survivors. Arch Ophthalmol 2009; 127:1500–1504 27. De Cicco L, Cella L, Liuzzi R, et al. Radiation thera-py in primary orbital lymphoma: a single institution retrospective analysis. Radiat Oncol 2009; 4:60
F O R Y O U R I N F O R M A T I O N
Unique customized medical search engine service from ARRS! ARRS GoldMiner® is a keyword- and
concept-driven search engine that provides instant access to radiologic images published in peer-reviewed journals. For more information, visit goldminer.arrs.org.