壹、緒 論
主動脈 (aorta) 和大動脈在心血管系統中扮演著重要的角色,其不僅是作
為輸送血液到組織的導管(傳導功能),同時也可緩衝心室唧出間歇性血流時的
壓力變化(緩衝功能)(Kawano, Tanaka, & Miyachi, 2006)。動脈硬化 (arterial stiffness) 與動脈順應性 (arterial compliance) 呈負相關,其乃是反映動脈緩衝心 臟搏動輸出的能力 (Poelkens 等, 2007)。動脈順應性降低或動脈硬化程度增加 將會損害動脈的緩衝功能,進而導致收縮壓和脈壓 (pulse pressure) 的增加、左 心室肥大 (left ventricular hypertrophy)、冠狀動脈缺血性疾病 (coronary ischemic disease),以及降低動脈壓覺反射敏感性 (arterial baroreflex sensitivity) (O'Rourke, 1990)。因此,動脈硬化程度增加不僅是預測心血管危險之重要且獨立的指標, 同時其在心血管疾病 (cardiovascular disease, CVD) 發展的病理生理學上也扮 演著重要的角色 (Blacher, Asmar, Djane, London, & Safar, 1999; McEniery, 2006)。
議的綜合性健康計畫之訓練量 (Cortez-Cooper 等; Okamoto 等; Miyachi 等, 2004),而高強度的阻力訓練期間將導致血壓大幅度的上升,進而可能對血管結 構 和 功 能 產 生 負 面 的 影 響 (Okamoto, Masuhara, & Ikuta, 2006) 。 Haslam, McCartney, McKelvie, 與 MacDougall (1998) 發現,中低強度的阻力訓練期間 所增加的血壓,通常會落在可接受的臨床範圍內,證實為一種安全且可行的運 動訓練模式。因此,針對一般健康成年人所建議的阻力訓練指南,亦即中低強 度及負荷量的阻力訓練,是否也同樣會導致動脈硬化程度的增加,則有待進一 步的觀察。 除了單獨從事有氧運動和阻力訓練外,結合有氧和阻力訓練(即交叉訓練) 因較具樂趣化,可避免因為長期從事單一訓練時而產生的厭倦感,且可獲得各 別訓練模式所特有的益處,進而達到互補作用 (Tanaka & Swensen, 1998),因此 也廣獲一般大眾所喜愛。Cook 等 (2006) 之研究顯示,交叉訓練型態的運動員 (例如划船選手)之動脈順應性顯著高於坐式生活者。Kawano 等 (2006) 則發 現,交叉訓練對健康年輕男性之動脈順應性似乎沒有顯著的改變,證實阻力訓 練對於動脈所造成的負面效果可因從事有氧運動而抵銷或改善。由於此方面的 文獻資料有限,因此有必要更進一步加以探究,以作為個體在開立預防和治療 CVD 或動脈硬化之運動處方時的參考依據。
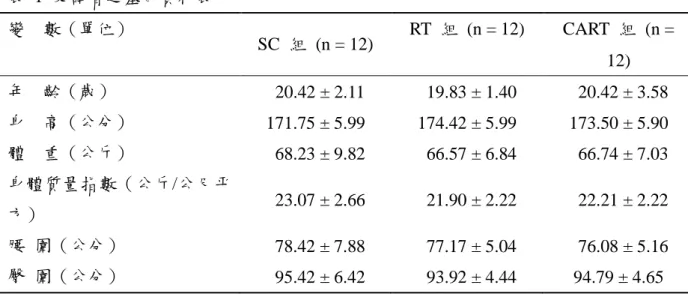
表 1 受試者之基本資料表 變 數(單位) SC 組 (n = 12) RT 組 (n = 12) CART 組 (n = 12) 年 齡(歲) 20.42 ± 2.11 19.83 ± 1.40 20.42 ± 3.58 身 高(公分) 171.75 ± 5.99 174.42 ± 5.99 173.50 ± 5.90 體 重(公斤) 68.23 ± 9.82 66.57 ± 6.84 66.74 ± 7.03 身體質量指數(公斤/公尺平 方) 23.07 ± 2.66 21.90 ± 2.22 22.21 ± 2.22 腰 圍(公分) 78.42 ± 7.88 77.17 ± 5.04 76.08 ± 5.16 臀 圍(公分) 95.42 ± 6.42 93.92 ± 4.44 94.79 ± 4.65 二、實驗設計與訓練計畫 RT 組和 CART 組之受試者每週接受 3 天,持續 12 週的運動訓練,在 每次訓練前後皆需進行 5-10 分鐘的熱身運動和緩和運動。RT 組的訓練計畫 內容為:70% 最大反覆 (one-repetition maximum, 1-RM),實施 3 組, 8-12 次 反覆,且在執行每個反覆動作時,向心階段和離心階段皆以 3 秒的時間來完成 (ACSM, 2006),組間休息時間為 2 分鐘。阻力訓練的部位包括:蝴蝶式擴胸 (pectoral fly)、三角肌後拉 (rear deltoid fly)、坐姿肱二頭肌捲曲 (seated biceps curl) 、 引 體向 上 (chin-up) 、 肱 三 頭肌 臂屈伸 (dip assist) 、 腿 部伸 展 (leg extensions)、腿部捲曲 (leg curl)、立姿舉踵 (standing calf raise) 等 8 個動作部 位。CART 組除了接受上述之阻力訓練課程外,在每次阻力訓練課程結束後, 額外增加 30 分鐘,運動強度為 70-80% 最大心跳率(以 220-年齡進行預估) 之固定式腳踏車訓練。而為了確保受試者在騎乘腳踏車期間皆能夠達到所規定
之運動強度,受試者必須佩帶手錶型心跳率測定器 (Cardiosport GT5 Heart
Rate Monitor, Healthcare Technology, Taiwan),以記錄運動訓練時的心跳率,且 在運動過程中由研究者或研究助理全程監控和調整。SC 組的受試者並不參與 任何型式的運動訓練計畫,在整個研究過程中,均維持其正常之生活作息。
三、測驗項目及方法
(一)身體組成:以體箱式全人體身體成分測試系統 (BOD POD Body
量來測定身體密度,因此在實施檢測時,受試者必須除去身上的首飾、眼鏡及 鞋襪等物件,而僅穿著泳褲,並攜帶泳帽進行測驗,以降低其對體積測量的影 響。受試者在艙室內應保持放鬆、正常呼吸的狀態,並限制其動作。本儀器所 測得的數據包括:體重、脂肪量和體脂肪百分比 (percent body fat, %BF)、去脂 體重 (fat-free mass, FFM) 和 %FFM。
(二)最大肌力:RT 組與 CART 組必須在運動訓練開始前 (week 0)、訓練 後的第 4 週 (week 4) 和第 8 週 (week 8),以及運動訓練結束後 (week12), 進行 1-RM 的預估測試,以作為訂定 (week 0)、調整運動訓練量 (week 4, 8) 及 檢測訓練效果 (week 12) 之依據;SC 組則只在實驗前和實驗後進行兩次測 試。進行測試之前,由受試者先預估該測驗動作的最大負荷,隨後執行該測驗 動作至疲勞,依據受試者所試舉的負荷以及反覆次數來找出受試者預估的 1-RM,每位受試者嘗試的次數控制在 5-6 次內,每次間隔休息 90 秒。測試 的部位包括:蝴蝶式擴胸、三角肌後拉、坐姿肱二頭肌捲曲、引體向上、肱三 頭肌臂屈伸、腿部伸展、腿部捲曲、立姿舉踵等 8 個動作部位。 (三)動脈硬化:本研究中所指的動脈硬化是以非侵入性的 Cardio Vision
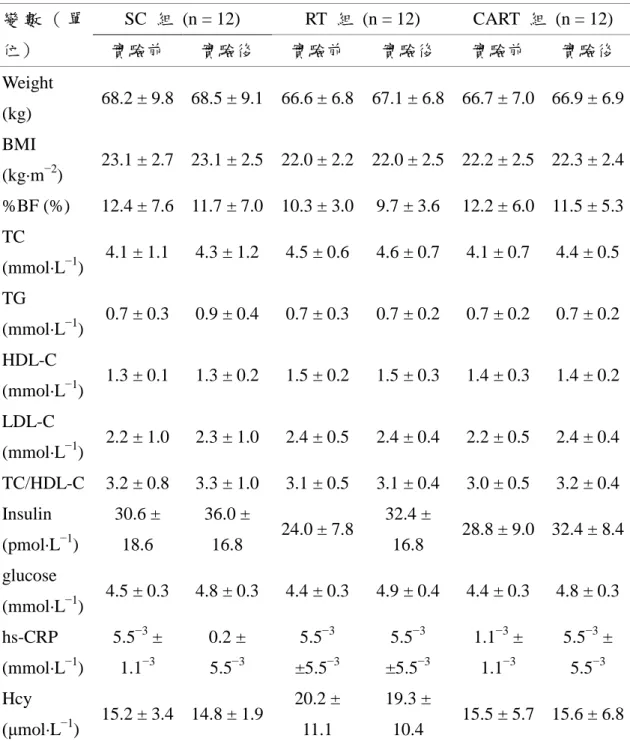
研究所測量的血液生化項目包括:總膽固醇 (total cholesterol, TC)、三酸甘油酯 (triglycerides, TG)、高密度脂蛋白膽固醇 (high-density lipoprotein cholesterol, HDL-C)、低密度脂蛋白膽固醇 (low-density lipoprotein cholesterol, LDL-C)、胰 島素 (insulin)、葡萄糖 (glucose)、高敏感性 C-反應蛋白 (high-sensitivity C-reactive proteins, hs-CRP) 和同半胱胺酸 (homocysteine) 等。
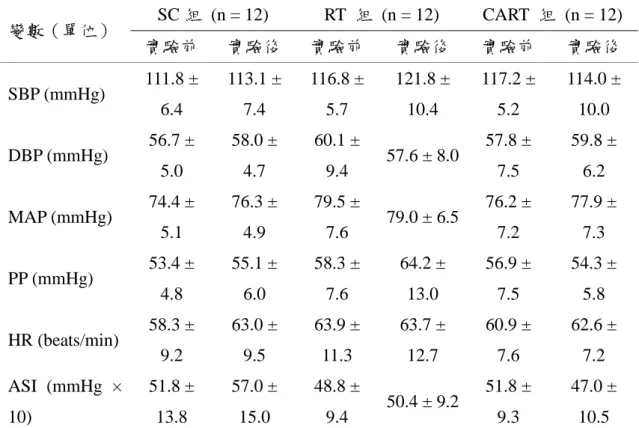
綜合以上的討論可得到以下結論,短時間的阻力訓練及結合有氧和阻力訓 練對大學男生動脈硬化程度沒有影響,證實以健康機構所建議的阻力訓練指導 方針來從事運動訓練,並不會增加動脈硬化程度或損害血管功能。而在健康、 年輕的大學生之中,舒張壓和平均動脈壓為決定動脈硬化程度的主要因素。而 未來之研究可針對罹患心血管疾病之高危險族群,進行長期不同運動強度之介 入,以觀察其對動脈硬化之影響。
引用文獻
Altunkan, S., Oztas, K., & Seref, B. (2005). Arterial stiffness index as a screening test for cardiovascular risk: a comparative study between coronary artery calcifica- tion determined by electron tomography and arterial stiffness index determined by a VitalVision device in asymptomatic subjects. European
Journal of Internal Medicine, 16, 580-584.
American College of Sports Medicine. (1998). Position Stand: The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness in healthy adults. Medicine and
Science in Sports and Exercise, 30, 975-991.
American College of Sports Medicine. (2006). ACSM’s guidelines for exercise
testing and prescription (7th ed.). Baltimore: Lippincott Williams & Wilkins.
Bertovic, D. A., Waddell, T. K., Gatzka, C. D., Cameron, J. D., Dart, A. M., & Kingwell, B. A. (1999). Muscular strength training is associated with low arterial compliance and high pulse pressure. Hypertension, 33, 1385-1391. Blacher, J., Asmar, R., Djane, S., London, G. M., & Safar, M. E. (1999). Aortic pulse
wave velocity as a marker of cardiovascular risk in hypertensive patients.
Hypertension, 33, 1111-1117.
Casey, D. P., Pierce, G. L., Howe, K. S., Mering, M. C., & Braith, R. W. (2007). Effect of resistance training on arterial wave reflection and brachial artery reactivity in normotensive postmenopausal women. European Journal of
Applied Physiology, 100, 403-408.
Physiology-Heart and Circulatory Physiology, 290, H1596-H1600.
Cortez-Cooper, M. Y., DeVan, A. E., Anton, M. M., Farrar, R. P., Beckwith, K. A., Todd, J. S., et al. (2005). Effects of high intensity resistance training on arterial stiffness and wave reflection in women. American Journal of
Hypertension, 18, 930-934.
Haslam, D. R. S., McCartney, N., McKelvie, R. S., & MacDougall, J. D. (1998). Direct measurements of arterial blood pressure during formal weightlifting in cardiac patients. Journal of Cardiopulmonary Rehabilitation, 8, 213-225. Hayman, L. L., Williams, C. L., Daniels, S. R., Steinberger, J., Paridon, S., Dennison,
B. A., et al. (2004). Cardiovascular health promotion in school: a statement for health and education professionals and child health advocates from the Committee on Atherosclerosis, Hypertension, and Obesity in Youth (AHOY) of the Council on Cardiovascular Disease in the Young, American Heart Association. Circulation, 110, 2266-2275.
Hurley, B. F., & Roth, S. M. (2000). Strength training in the elderly: effects on risk factors for age-related disease. Sports Medicine, 30, 249-268.
Kaibe, M., Ohishi, M., Komai, N., Ito, N., Katsuya, T., Rakugi, H., et al. (2002). Arterial stiffness index: a new evaluation for arterial stiffness in elderly patients with essential hypertension. Geriatrics and Gerontology
International, 2, 199-205.
Kawano, H., Tanaka, H., & Miyachi, M. (2006). Resistance training and arterial compliance: keeping the benefits while minimizing the stiffening. Journal of
Hypertension, 24, 1753-1759.
Kawano, H., Tanimoto, M., Yamamoto, K., Sanada, K., Gando, Y., Tabata, I., et al. (2008). Resistance training in men is associated with increased arterial stiffness and blood pressure but does not adversely affect endothelial function as measured by arterial reactivity to the cold pressor test.
Experimental Physiology, 93, 296-302.
LeMura, L. M., von Duvillard, S. P., Andreacci, J., Klebez, J. M., Chelland, S. A., & Russo, J. (2000). Lipid and lipoprotein profiles, cardiovascular fitness, body composition, and diet during and after resistance, aerobic and combination training in young women. European Journal of Applied Physiology, 82, 451-458.
index as a cardiovascular risk marker in asymptomatic. Taiwan Journal of
Family Medicine, 17,210-221.
McEniery, C. M. (2006). Novel therapeutic strategies for reducing arterial stiffness.
British Journal of Pharmacology, 148, 881-883.
Miyachi, M., Donato, A. J., Yamamoto, K., Takahashi, K., Gates, P. E., Moreau, K. L., et al. (2003). Greater age-related reductions in central arterial compliance in resistance-trained men. Hypertension, 41, 130-135.
Miyachi, M., Kawano, H., Sugawara, J., Takahashi, K., Hayashi, K., Yamazaki, K., et al. (2004). Unfavorable effects of resistance training on central arterial compliance. A randomized intervention study. Circulation, 110, 2858-2863. Nurnberger, J., Dammer, S., Saez, A. O., Philipp, T., & Schafers, R. F. (2003).
Diastolic blood pressure is an important determinant of augmentation index and pulse wave velocity in young, healthy males. Journal of Human
Hypertension, 17, 153-158.
O'Rourke, M. (1990). Arterial stiffness, systolic blood pressure, and logical treatment of arterial hypertension. Hypertension, 15, 339-347.
Okamoto, T., Masuhara, M., & Ikuta, K. (2006). Effects of eccentric and concentric resistance training on arterial stiffness. Journal of Human Hypertension, 20, 348-354.
Okamoto, T., Masuhara, M., & Ikuta, K. (2008). Effects of low-intensity resistance training with slow lifting and lowering on vascular function. Journal of
Human Hypertension, 22, 509-511.
Otsuki, T., Maeda, S., Iemitsu, M., Saito, Y., Tanimura, Y., Ajisaka, R., et al. (2007a). Vascular endothelium-derived factors and arterial stiffness in strength- and endurance-trained men. American Journal of Physiology Heart and
Circulatory Physiology, 292, H786-H791.
Otsuki, T., Maeda, S., Iemitsu, M., Saito, Y., Tanimura, Y., Ajisaka, R., et al. (2007b). Relationship between arterial stiffness and athletic training programs in young adult men. American Journal of Hypertension, 20, 967-973.
Left ventricular diastolic function in weight lifters. American Journal of
Cardiology, 58, 1254-1259.
Petersen, S. E., Wiesmann, F., Hudsmith, L. E., Robson, M. D., Francis, J. M., Selvanayagam, J. B. (2006). Functional and structural vascular remodeling in elite rowers assessed by cardiovascular magnetic resonance. Journal of the
American College of Cardiology, 48, 790-797.
Poelkens, F., Rakobowchuk, M., Burgomaster, K. A., Hopman, M. T. E., Philips, S. M., & MacDonload, M. J. (2007). Effect of unilateral resistance training on arterial compliance in elderly men. Applied Physiology, Nutrition, and
Metabolism, 32, 670-676.
Rakobowchuk, M., McGowan, C. L., de Groot, P. C., Bruinsma, D., Hartman, J. W., Phillips, S. M., et al. (2005). Effect of whole body resistance training on arterial compliance in young men. Experimental Physiology, 90, 645-651. Sharma, G. K., Gudapati, S., Waller, J. L., & Prisant, L. M. (2005). Assessment of
test repeatability of arterial stiffness index. Blood Pressure Monitoring, 10, 271-274.
Stehouwer, C. D., & Ferreira, I. (2006). Diabetes, lipids and othe cardiovascular risk factors. In M. E. Safar & M. F. O'Rourke (Eds.), Arterial stiffness in
hypertension-handbook of hypertension (pp. 427-456). Elsevier, Amsterdam.
Tanaka, H., & Safar, M. E. (2005). Influence of lifestyle modification on arterial stiffness and wave reflections. American Journal of Hypertension, 18, 137-144.
Tanaka, H., & Swensen, T. (1998). Impact of resistance training on endurance performance: A new form of cross-training? Sports Medicine, 25, 191-200. Wilkinson, I. B., & McEniery, C. M. (2004). Arterial stiffness, endothelial function
and novel pharmacological approaches. Clinical and Experimental
Effects of Resistance Training and Combined Aerobic and
Resistance Training on Arterial Stiffness in Male College
Students
Chu, Chia-Hua、Pan, Chien-Yu National Kaohsiung Normal University
Abstract
Purpose: The purpose of this study was to investigate the effects of resistance
training (RT) and combined aerobic and resistance training (CART) on arterial stiffness in male college students. Methods: Thirty-six males (20.22 ± 2.47 years) volunteered to participate and were randomly assigned to either RT group (n = 12), CART group (n = 12), or sedentary control (SC) group (n = 12). The RT and CART groups performed RT three times a week for 12 weeks, and the CART group performed a cycle exercise at 70-80% of the maximal heart rate for 30 min immediately after each RT session. Two-way ANOVAs with repeated measures on one factor (Time) were used to examine training effects. For those with interactions, the main effect will be used to further analyze the treatment effect under different conditions. Pearson product-moment correlation coefficients were calculated to evaluate the relationship between arterial stiffness index (ASI) and other CVD risk factors. Results: (1) Both RT and CART groups significantly increased 1RM values on all trained muscle groups, (2) no significant changes in ASI, blood lipid profiles, blood pressure or body composition were observed in the experimental groups, and (3) ASI was negatively correlated to diastolic blood pressure (DBP; r = − 0.382, p < .05) and mean arterial pressure (MAP; r = − 0.334, p < .05); no correlations among ASI and other cardiovascular disease risk factors were found. Conclusions: The 12 weeks of RT and CART dose not alter arterial stiffness, suggesting that RT when performed in accordance with American College of Sports Medicine guidelines does not have deteriorate effects on arterial function. DBP and MAP were important determinants of ASI in healthy male college students.