Contents lists available at ScienceDirect
Resuscitation
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . c o m / l o c a t e / r e s u s c i t a t i o n
Clinical paper
Survey of outcome of CPR in pediatric in-hospital cardiac arrest in a medical center in Taiwan 夽
En-Ting Wu a , Meng-Ju Li a , Shu-Chien Huang b , Ching-Chia Wang a , Yueh-Ping Liu a , Frank Leigh Lu a , Wen-Je Ko b , Ming-Jiuh Wang c , Jou-Kou Wang a , Mei-Hwan Wu a,∗
a
Department of Pediatrics, National Taiwan University Hospital and College of Medicine, National Taiwan University, Taipei, Taiwan
b
Department of Surgery, National Taiwan University Hospital and College of Medicine, National Taiwan University, Taipei, Taiwan
c
Department of Anesthesiology, National Taiwan University Hospital and College of Medicine, National Taiwan University, Taipei, Taiwan
a r t i c l e i n f o
Article history:
Received 27 June 2008
Received in revised form 8 January 2009 Accepted 12 January 2009
Keywords:
Pediatric
Cardiopulmonary resuscitation Cardiac arrest
a b s t r a c t
Purpose of the study: While the outcomes of cardiopulmonary resuscitation (CPR) for pediatric in-hospital cardiac arrest (IHCA) are reported for many regions, none is reported for Asian countries. We report the outcomes of CPR for pediatric IHCA in a tertiary medical center in Taiwan and also identify prognostic factors associated with poor outcome.
Methods: Data were retrieved retrospectively from 2000 to 2003 and prospectively from 2004 to 2006 from our web-based registry system. We evaluated patients younger than 18 years of age who had IHCA and received CPR. The primary outcome was survival to hospital discharge, and the secondary outcomes were sustained return of spontaneous circulation (ROSC), and favorable neurological outcomes as assessed by pediatric cerebral performance categories (PCPC).
Results: We identified 316 patients and the overall hospital survival was 20.9% and 16.1% had favorable neurological outcomes. Sixty-four patients ever supported with ECMO. We further analyzed 252 patients who underwent conventional CPR only and most had cardiac disease (133/252, 52.8%). The second most common preexisting condition was hematologic or oncologic disease (43/252, 17.1%). Of the 252 patients, 153 (60.7%) achieved sustained ROSC, 50 (19.8%) survived to discharge, and 39 patients (15.5%) had favor- able neurological outcomes. CPR during off-work hours resulted in inferior chances of reaching sustained ROSC. Multivariate analysis showed that long CPR duration, hematology/oncology patients, and pre-arrest vasoactive drug infusion were significantly associated with decreased hospital survival (p < 0.05).
Conclusions: Outcomes of CPR for pediatric patients with IHCA in Taiwan were comparable to corre- sponding reports in Western countries, but more hematology/oncology patients were included. Long CPR duration, hematologic or oncologic underlying diseases, and vasoactive agent infusion prior IHCA were associated with poor outcomes. The concept of palliative care should be proposed to families of termi- nally ill cancer patients in order to avoid unnecessary patient suffering. Also, establishing a balanced duty system in the future might increase chances of sustained ROSC.
© 2009 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Although cardiopulmonary resuscitation (CPR) has been avail- able for children for more than 50 years,
1the results remain far from satisfactory. As the Utstein template is suggested as the stan- dard for reporting the outcomes of CPR,
2there are several studies of in-hospital cardiac arrests (IHCA) in children, such as national reg- istry of cardiopulmonary resuscitation (NRCPR) in United States,
3,4夽 A Spanish translated version of the summary of this article appears as Appendix in the final online version at doi:10.1016/j.resuscitation.2009.01.006.
∗ Corresponding author at: 7th, Chung-Shan South Road, Taipei, Taiwan.
Tel.: +886 2 23123456x65126.
E-mail address: [email protected] (M.-H. Wu).
Canada,
5,6South America,
7Australia,
8and European countries.
9–12These data are lacking for Asian countries. The goal of this study was to report the outcomes of IHCA among pediatric patients in our institute and compare them to those of Western countries.
2. Materials and methods 2.1. Hospital setting
NTUH is a university-affiliated tertiary teaching hospital, with a 120-bed pediatric department. The hospital has a 13-bed pedi- atric intensive care unit (PICU). According to hospital policy, there are always manpower and monitoring devices within the PICU or emergency department in the hospital so that there is no need to call for a CPR team when IHCA occurs in these locations. Other- 0300-9572/$ – see front matter © 2009 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.resuscitation.2009.01.006
wise, the pediatric CPR team helps manage any cardiorespiratory arrest outside the aforementioned areas, such as the general ward or public area in the hospital. The pediatric CPR team consists of a senior pediatric resident, a head nurse, and several registered nurses. Each member of the CPR team is certified to perform pedi- atric advanced life support (PALS). The CPR team responds to each emergency call and provides basic life support and PALS for patients who suffered IHCA. All patients who received CPR outside the PICU are admitted to the PICU for further post-resuscitation care and evaluation.
The study group was retrospectively identified from our pedi- atric database from January 2000 to December 2003. Since January 2004, patients were enrolled prospectively from a web-based reg- istry system in the Quality Management Center in our hospital.
13The hospital’s ethical committee approved this research protocol.
2.2. Inclusion and exclusion criteria
Patients aged from 7 days to 18 years who experienced car- diac arrests in our hospital between January 2000 and December 2006 were eligible to be included in this study. Cardiac arrest was defined as any condition requiring external chest compressions or internal cardiac massage for >60 s because of profoundly low out- put state. For patients with multiple arrest events, only the initial index arrest/event and resuscitation were described and analyzed.
We excluded premature or term neonates treated in the delivery room or neonatal ward. Furthermore, we excluded patients who only received resuscitation drugs or positive pressure ventilation without need of chest compression or defibrillation, and patients who were subject to palliative treatment or to a “do not resusci- tate (DNR)” order. Patients arriving at the emergency department in cardiac arrest were not included in this study. Hypothermia was not routinely induced after resuscitation.
2.3. Outcome measures
We applied Utstein-style data reporting guidelines for cardiac arrests and CPR to describe the outcomes. The primary outcome measure was survival to hospital discharge. Secondary outcome measures included sustained return of spontaneous circulation (ROSC) of >20 min, 24-h survival, neurological outcomes at hospi- tal discharge of the survivors and the 1-year survival. Neurological outcome was determined using pediatric cerebral performance categories (PCPC), in which category (1) represents a normal neu- rological state, (2) mild disability, (3) moderate disability, (4) severe disability, (5) coma or vegetative state, and (6) death. A good neu- rological outcome was defined by a PCPC score of 1, 2 or 3, or no changes from the baseline PCPC score. Because there are increasing reports that imply superior outcomes for extracorporeal membrane oxygenation (ECMO) support during CPR than for conventional CPR,
14–16patients treated with ECMO during CPR or in the post- resuscitative period were considered separately and not included in the further analysis of outcomes.
2.4. Data analysis and statistical methods
Patient age, sex, condition before arrest (presence of intra- arterial blood pressure monitoring, endotracheal intubation, and continuous infusion of vasoactive drugs), location of arrest, first recorded ECG rhythm, use of cardioversion, injection of epinephrine (adrenalin), calcium compounds, and bicarbonate during CPR, and total duration of CPR were collected. The predisposing conditions before arrest were categorized as cardiac, respiratory, neurologi- cal, hematologic/oncologic, hepatic/gastrointestinal, infectious and metabolic/genetic disorders. The age of patients was categorized into newborns (<1 month), infants (1–12 months), young children
(1 year to <8 years) and older children (8–18 years) in order to com- pare the CPR outcome. We then divided the CPR duration into five categories: <10 min, 11–20 min, 21–30 min, 31–60 min and >60 min.
Furthermore, to compare the outcome of CPR during working hour and non-working hours, the arrest time was categorized into work- ing hours if it happened from 8 a.m. to 6 p.m., Monday to Friday, or non-working hours (hours outside working hours). The above vari- ables were analyzed to see if these factors affected the outcomes of CPR.
Pearson’s chi-squared test was used for qualitative variable anal- ysis, and Fisher’s exact test was used when n was less than 20 or when any value was less than 5. Student’s t-test was used to compare quantitative variables between independent groups and the Mann–Whitney U-test was used for variables without nor- mal distribution. Multivariate logistic regression was performed to assess the influence of each one of the factors on the primary and secondary outcomes. All the individual factors with statis- tical significance in the univariate analysis were included in the multivariate analysis. Results are expressed as mean ± standard deviation (S.D.). p-Values were considered significant when they were less than 0.05 (two-sided).
3. Results
During the study period, 316 cardiac arrests occurred that resulted in CPR; the incidence was 0.9% out of 35,497 pediatric admissions and 5.7% out of 5514 PICU admissions, which was higher than the report from Australia (0.1 and 2.4%, respectively)
8and Canada (0.94% for PICU admissions),
6but lower than in Finland (0.7 and 7.5%)
12and Brazil (2.14 and 19%).
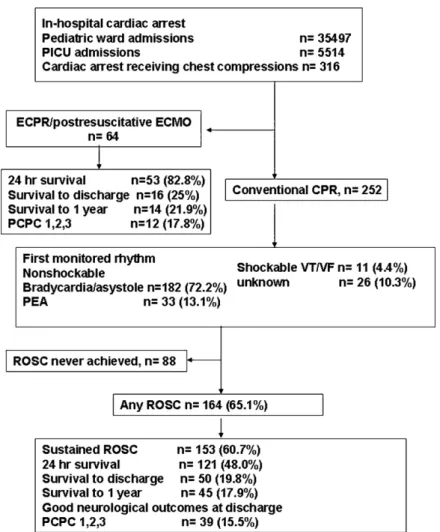
7In this cohort, 228 patients (72.2%) ever achieved ROSC, 174 patients (55.1%) had 24-h sur- vival, 66 patients (20.9%) survived to discharge and 51 patients (16.1%) had good neurological outcomes (PCPC = 1, 2, or 3). Sixty- four patients underwent ECMO during active chest compression (ECPR) or underwent ECMO within 24 h of CPR. In the ECMO group, 25% survived to hospital discharge and 17.8% had good neurological outcomes. We studied 252 children (142 boys and 110 girls) who received conventional CPR. Their mean age was 44.9 ± 58.4 months (median: 15.5 months, range: 0–205 months). The mean CPR dura- tion was 39.5 ± 50.9 min (median: 20.5 min, range: 5–124 min). The outcome of CPR was recorded using the Utstein template (Fig. 1).
Of the 252 patients analyzed, 164 achieved ROSC (65.1%), which was temporary in 11 patients. Therefore, 153 patients achieved sus- tained ROSC (60.7%) and 121 patients (48.0%) survived 24 h after CPR. Thereafter, 71 (28.1%) died 19 ± 32 days (median: 8 days) after CPR, and only 50 (19.8%) survived to hospital discharge. Only 39 patients (15.5%) had good neurological outcomes at discharge. Five patients died 195 ± 86 days (median: 230 days) after discharge and the causes of death included uncontrolled underlying disease (n = 2) and septic shock (n = 3). Therefore, only 45 patients (17.9%) survived to 1 year after the IHCA event.
3.1. The first-monitored rhythm
In this cohort, the most common first-monitored rhythm was bradycardia or asystole (n = 182, 72.2%), followed by pulseless elec- trical activity (n = 33, 13.1%). Shockable ventricular tachycardia or ventricular fibrillation (VT/VF) was seen in only 11 patients (4.4%), and 26 ECG rhythms were missing (no data). The first monitored rhythm did not affect the outcome (p = 0.91).
3.2. Age category and outcome of CPR
Most patients were 1–8 years of age (n = 81, 32.1%), followed by
infants (n = 78, 31.0%). In this study, infants (1 month to 1 year of
age) showed a trend toward increased survival to discharge (n = 23,
Fig. 1. Pediatric Utstein template for recording outcomes of in-hospital CPR. PICU: pediatric intensive care unit, ECMO: extracorporeal membrane oxygenation, PEA: pulseless electrical activity, ROSC: return of spontaneous circulation and PCPC: pediatric cerebral performance category.
29.5%, p = 0.07) and had more favorable neurological outcomes (n = 20, 25.6%, p = 0.03) than any other age category (Table 1).
3.3. Locations of arrest
In this study, 218 (86.5%) patients arrested in the PICU, 22 (8.7%) in the general wards, and 12 (4.8%) in other areas such as diagnos- tic rooms (cath lab, computer tomography room) and outpatient clinics. The outcomes of CPR in this study were not influenced by locations of IHCA (Table 2).
3.4. Preexisting disease
Most patients who underwent IHCA had cardiac disease (133/252, 52.8%). The second most common preexisting condition was hematologic or oncologic disease (43/252, 17.1%). Among the
Table 2
Locations and outcomes.
ICU Ward others p
Number (%) 218 (86.5%) 22 (8.7%) 12 (4.8%)
Primary outcome 0.40
Survival to discharge 44 (20.2%) 3 (13.6%) 3 (25.0%) Secondary outcomes
Sustained ROSC 130 (59.6%) 13 (59.1%) 10 (83.3%) 0.45
24 h survival 107 (49.1%) 6 (27.3%) 8 (66.7%) 0.09
Good neurological outcome 33 (15.1%) 3 (13.6%) 3 (25.0%) 0.29
patients with hematologic or oncologic disease, only two survived to hospital discharge (4.7%) and only one had good neurologi- cal function (2.3%). This group had the worst among all patients (p < 0.05) (Table 3).
Table 1
Age category and outcomes.
<1 month 1–12 months 1–8 years 9–18 years p
Number (%) 44 (17.5%) 78 (31.0%) 80 (31.7%) 50 (19.8%)
Primary outcome
Survival to discharge 6 (13.6%) 23 (29.5%) 14 (17.5%) 7 (14.0%) 0.07
Secondary outcome
Sustained ROSC 27 (61.4%) 47 (60.3%) 52 (65.0%) 27 (54.0%) 0.67
24 h survival 20 (45.5%) 42 (53.8%) 42 (52.5%) 17 (34.0%) 0.13
Good neurological outcome 5 (11.4%) 20 (25.6%) 9 (11.3%) 5 (10.0%) 0.03
Table 3
Preexisting condition and outcomes.
Cardiac Hematology/oncology Neurology GI/hepatic Infection Respiratory Metabolic/genetic disorder p
Number (%) 133 (52.8%) 43 (17.1%) 19 (7.5%) 18 (7.1%) 14 (5.6%) 4 (1.6%) 21 (8.3%)
Primary outcome
Survival to discharge 29 (21.8%) 2 (4.7%) 6 (31.6%) 4 (22.2%) 2 (14.3%) 1(25%) 6 (28.6%) 0.01
Secondary outcome
Sustained ROSC 79 (59.4%) 27 (62.8%) 13 (68.4%) 12 (66.7%) 5 (35.7%) 3(75%) 14 (66.7%) 0.51
24 h survival 69 (51.9%) 14 (32.6%) 11 (57.9%) 9(50%) 4 (28.6%) 3(75%) 11 (52.4%) 0.16
Good neurological outcome 24 (18.0%) 1 (2.3%) 4 (21.1%) 4 (22.2%) 1 (7.1%) 1(25%) 4 (19.0%) 0.01
3.5. Condition before CPR and CPR management
Before IHCA, 174 of the 252 (69.0%) patients had already under- gone intra-arterial blood pressure monitoring, 202 (80.2%) had been intubated for assisted ventilation, and 165 (65.5%) had con- tinuous intravenous infusions of vasoactive drugs. Cardiac patients had a greater percentage of the latter two pre-CPR measures than other groups (117/134, 87.3%, and 99/134, 73.9%, respectively, both p < 0.05). During CPR, 171 of 252 patients (67.9%) received calcium compound injections and 168 (66.7%) had bicarbonate injections.
Only 39 patients (15.5%) underwent cardioversion. Furthermore, calcium or bicarbonate injections were associated with longer CPR durations (p = 0.001 and 0.0009, respectively). Comparing the sur- vivors and non-survivors, non-survivors had longer CPR durations, more pre-CPR intra-arterial monitoring (p = 0.022), endotracheal intubation (p = 0.052), and continuous infusion of vasoactive drug (p < 0.001) (Table 4).
3.6. CPR duration
Survivors had significantly shorter CPR duration than non- survivors (15.1 ± 12.7 min vs. 44.3 ± 53.2 min, p = 0.001) ( Table 4).
Longer CPR duration is associated with the worse outcomes (for both survival to discharge and good neurological survival), espe- cially when CPR lasted for more than 20 min (p = 0.000). Forty-nine patients received CPR for more than 60 min and none survived (Fig. 2).
3.7. Cardiac arrest during nights and weekends
Only 75 indexed events happened during nights and weekends.
Among patients who had CPR during nights and weekends, fewer achieved sustained ROSC compared to those who had CPR dur- ing working hours (45.3% vs. 67.2%, respectively, p = 0.001), but the chances of survival to discharge (14.7% vs. 22.0%, respectively) and good neurological outcomes (10.7% vs. 17.5%, respectively)
Table 4
Comparisons between survivors and non-survivors.
Survivor (n = 50)
Non-survivor (n = 202)
p
Sex (M/F) 28/22 114/88 0.956
Age (months) 30.4± 47.3 48.6 ± 60.4 0.048
CPR duration (minutes) 15.1 ± 12.7 44.3 ± 53.2 0.002 Pre-CPR condition
Intraarterial BP monitoring 28 (56.0%) 146 (72.3%) 0.026 Endotracheal intubation 35 (70.0%) 167 (82.7%) 0.037 Continuous infusion of vasoactive drugs 21 (42.0%) 144 (71.3%) 0.000 CPR management
Epinephrine > 0.02 mg/kg 18 (36.0%) 123 (60.9%) 0.002
Calcium injection 28 (56.0%) 143 (70.8%) 0.031
Bicarbonate injection 29 (58.0%) 139 (68.8%) 0.147
Cardioversion 7 (14.0%) 32 (15.8%) 0.747
Fig. 2. CPR duration and outcome. ROSC: return of spontaneous circulation.
did not differ significantly between patients who had CPR on nights/weekends and working hours (Fig. 3).
3.8. Factors associated with poor outcome
Multivariate analysis showed that patients who had vasoactive drug infusions before CPR, hematologic or oncologic diseases, and longer CPR durations had decreased chances of surviving to hospital discharge (p < 0.05).
4. Discussion
We describe the outcomes of CPR for pediatric IHCA at National Taiwan University Hospital, based on Utstein template. The overall hospital survival was 20.9% and 16.1% of the patients had favorable good neurological outcomes. Of the 252 patients who received con-
Fig. 3. The CPR timing and outcome. ROSC: return of spontaneous circulation. (*)
Means statistical significance (p < 0.05).
ventional CPR, 60.7% had sustained ROSC, 48.0% had 24 h survival, 19.8% survival to discharge, 17.9% survived 1 year and only 15.5%
had good neurological outcomes. We also identified the risk factors that were associated with poor outcomes, including hematologic or oncologic disease, prolonged CPR duration, and pre-CPR vasoactive drug requirements.
According to the NRCPR,
352% of pediatric patients who under- went CPR had sustained ROSC, 36% had 24-h survival, 27% survived to discharge, and 15.4% had good neurological outcomes. Further- more, the NRCPR reported that the most common first-documented pulseless cardiac arrest rhythm was asystole (40%) followed by pulseless electrical activity (24%), then VT/VF (13.6%). Also, survival rates were highest among patients in whom VT/VF was present initially than among those in whom it developed subsequently.
4Outcomes of CPR and first-documented rhythms in this Asian cohort are comparable to those reported by the NRCPR. Nonethe- less, we could not proceed with further analysis of VT/VF due to incomplete data recording.
We found that infants (1 month to 1 year of age) showed a trend toward better survival (p = 0.07) and had better neurologi- cal outcomes (p = 0.03) in comparison to other age groups (Table 1).
This phenomenon has been mentioned in NRCPR.
17Besides, the NRCPR identified that improved 24-h survival for children receiv- ing CPR was associated with the presence of pediatric residents and fellows.
18Most of our patient’s cardiac arrests occurred in the PICU (86.2%) where pediatric residents or fellows, even attending physi- cians were always present. Survival outcomes did not differ by CPR location in our study (Table 2).
In this series, before IHCA, 174 patients (69.0%) already had received intra-arterial blood pressure monitoring, 202 (80.2%) had been intubated for assisted ventilation, and 165 (65.5%) had intra- venous continuous infusion of vasoactive drugs. The percentages of the above interventions were higher in our study than those in previous reports, and most cardiac arrests were due to progres- sive deterioration of the underlying disease, rather than sudden arrest.
4,9,10In the report by the Spanish Study Group for Cardiopul- monary Arrest in Children, 68.1% of the patients were supported with mechanical ventilation and 59.4% with vasoactive drugs, and the risk of mortality was significantly higher in these patients, which is consistent with our findings.
10The NRCPR data showed that 29.5% (295/855) of patients had arterial catheters, while 39.3%
(336/855) had vasoactive infusions before cardiac arrest; the use of vasoactive infusion was associated with increased mortality, which was also observed in our study.
4We noticed that injection of calcium compounds was associ- ated with inferior outcomes, which was also observed in other studies.
6,19In the NRCPR study, calcium was more likely to be used in the settings of pediatric facilities, ICUs, cardiac surgery, CPR dura- tion of ≥15 min, asystole, and concurrently with other advanced life support medications. We also observed increased calcium use with prolonged CPR (p = 0.001). Although the AHA has published guidelines limiting the recommended use of calcium to selected resuscitation circumstances, physicians in our hospital tended to inject calcium more liberally to try all possible therapies during CPR. This could have reflected the medical futility of the situation.
We found that patients with preexisting hematologic and onco- logic diseases had inferior outcomes, with only 2 (4.6%) surviving to discharge and one (2.3%) good neurological outcome. These patients comprised the second majority (43/252, 17.1%) of this study group, only outnumbered by cardiac patients. In the NRCPR study, cancer patients comprised only 4.7% (40/855) of the patient population, and their outcomes were also poor.
4This is a unique phenomenon, which is the result of cultural differences. In another report from Taiwan mentioning these circumstances among 101 pediatric patients with cancer, 35 (34%) patients underwent CPR and they all died.
20Taiwanese parents tended to insist on ‘resus-
citating until the last second’. Furthermore, no patient had ‘do not resuscitate’ orders, even as teenagers. This reflects how Taiwanese patients are often overprotected and precluded from knowing the reality of their terminal illness. The idea of palliative care should be proposed in such circumstances.
We found that longer CPR durations were associated with poor outcomes. Among 94 patients who were resuscitated for more than 30 min, 7 (7.4%) survived to discharge and only 3 (3.2%) had good neurological outcomes. None of the patients who were resuscitated for more than 60 min survived. Similar findings are also reported in the literatures.
7,9,10,12Lopez-Herce et al. reported that a life-support time period of more than 20 min predicted a final mortality of 78%, and more than 60 min predicted 100% mortality.
9Rodriguez-Nunez et al. also mentioned the mortality rate was 72.7% if the CPR dura- tion was 10–19 min and approached 100% if CPR lasted >20 min.
10