Original Article
Association of B vitamins status and homocysteine levels
in elderly Taiwanese
Kuan-Ju Chen
MS,1,2Wen-Harn Pan
PhD,1Feili-Lo Yang
PhD,3Ien-Lan Wei
PhD,4Ning-Sing Shaw
PhD1and Bi-Fong Lin
PhD11Institute of Microbiology and Biochemistry, National Taiwan University, Taipei, Taiwan, 2Department of Food Nutrition, Chung-Hwa College of Medical Technology, Tainan, Taiwan 3Department of Nutrition and Food Sciences, Fu-Jen University, Hsin-Chuang, Taipei, Taiwan 4School of Nursing, National Yang-Ming University, Taipei, Taiwan
To investigate the relationship between homocysteine (Hcy) and B vitamins status in the Taiwanese elderly population, an analysis was made of the plasma Hcy levels in elderly persons. The study sample was taken from the Elderly Nutrition and Health Survey in Taiwan (1999-2000) (Elderly NAHSIT) and included 1094 males and 1135 females aged 65-90 years. The results showed that average plasma Hcy was 13.3 ± 0.6 µmol/L for males and 10.6 ± 0.7 µmol/L for females. The average plasma Hcy levels of males from all age groups were significantly higher than those of females, and significantly increased with age (P trend <0.0001). The overall prevalence of hyperhomocysteinemia (Hcy >15 µmol/L) was 23.4% for elderly males and 11.2% for elderly females, and this also increased with age (P trend <0.0001). In subjects with normal renal function, folate, vitamin B2, B6, and B12 status were significantly lower in males with hyperhomocysteinemia, while only folate and vitamin B12 were significantly lower in females with hyperhomocysteinemia. Further analysis suggested that folate, vitamin B6 or B12 insufficiency were associated with hyperhomocysteinemia in both sexes, while vitamin B2 insufficiency was significantly associated only in males. In elderly persons with adequate folate, vitamin B6, and B12 status, there was no significant association between vitamin B2 and hyperhomocysteinemia. This association occurred only in those who had concurrent poor folate, vitamin B6, or B12 status. The strength of the association between vitamin B12 insufficiency and hyperhomocysteinemia was not affected by simultaneous vitamin B2 or B6 insufficiency, but increased about 3-fold when combined with folate. This suggests that poor folate and vitamin B12 status has a synergistic effect on the risk of hyperhomocysteinema in the elderly, as did a poor folate and vitamin B6 status. Therefore, maintaining adequate vitamin B12 status and avoiding multiple B vitamin insufficiency, especially that of folate and vitamin B12 or B6, should be emphasized as an important measure for reducing plasma Hcy levels among elderly Taiwanese.
Key Words: folate, vitamin B2, vitamin B6, vitamin B12, homocysteine, elderly, Elderly Nutrition and Health Survey in
Taiwan (1999-2000)
Introduction
Homocysteine (Hcy) is a sulphur-containing amino acid derived from the metabolism of methionine, which is the only dietary precursor of Hcy. Several B vitamins are involved in Hcy metabolism. Vitamin B6 is the coenzyme for cystathionine β-synthase, which irreversibly converts Hcy to cystathionine. Vitamin B12 is the coenzyme for 5-methyltetrahydrofolatehomocysteine S-methyltransferase, which remethylates Hcy to methionine. The 5-methyl-tetrahydrofolate form of folate donates the methyl group in this reaction. Afterwards, 5-methyltetrahydrofolate is re-formed through the enzyme methylenetetrahydrofolate reductase (MTHFR), for which riboflavin (vitamin B2) is required as the coenzyme.1,2 Therefore, Hcy metabolism may be affected by the status of these B vitamins.
Several studies have shown that hyperhomocysteinemia has been associated with CVD and other age-related diseases in elderly people.3-5 Such findings have led to
increased attention to Hcy concentrations in the elderly population. Studies have shown that blood Hcy con-centration exhibits an inverse association with concen-trations of vitamin B2, B6 and B12 and in particular blood folate, in subjects in the lower quartile of blood B vitamin levels.10,11 Prior investigations have found that elderly persons are at higher risk than younger persons for de-ficiencies of B vitamins, leading to elevated plasma Hcy concentrations.7,12 As a result, maintaining good B vitamin status is important for elderly persons.
Correspondence address:. Dr Bi-Fong Lin, Department of Biochemical Science and Technology, Institute of Microbiology and Biochemistry, National Taiwan University.
No.1, Section 4, Roosevelt Road. Taipei 10617, Taiwan, ROC. Tel/Fax: +886 2-23621301;
Email: bifong@ntu.edu.tw Accepted 30 June 2005
A previous survey, the Nutrition and Health Survey in Taiwan 1993-1996 (NAHSIT 1993-1996), indicated that elderly people had a high prevalence of folate insuffi-ciency.13 This has led to increased attention to Hcy levels in the Taiwanese elderly population. Therefore, the aim of this study was to determine plasma Hcy concentrations in the Taiwanese elderly population, and to assess the associated status of B vitamins such as B2, B6, B12 and folate.
Subjects and Methods Subjects
The subjects in this study were sampled from the Tai-wanese elderly population as part of the Elderly NAHSIT project by a multistage, stratified sampling method. A detailed description of sampling design can be found in Pan et al’s report.14 The sample consisted of 2229 subjects aged 65 to 90 years, including 1094 males and 1135 females. In order to determine the relationship between plasma Hcy levels and various B vitamins, subjects with serum creatinine ≥1.5 mg/dL were excluded to eliminate the effect of renal function on Hcy clearance. This re-sulted in 1350 subjects, including 656 males and 694 fe-males, who had complete data from physical examina-tions and interviewer-administered questionnaires. Biochemical analyses, data collection and definition of vitamin B insufficiency
Plasma was separated immediately after sampling and frozen at -80oC until analysis. Plasma Hcy was measured by automated analyzer (IMMULITE 2000 analyzer and IMMULITE Hcy Kit, Diagnostic Products Corporation, LA, USA). A series of quality control tests were per-formed to evaluate the precision of this assay. These tests +confirmed both the between- and within-run consistency of this method. The Coefficient of Variation (CV) for the Hcy assay was 7.1 %.
Data collection included physical examinations, bio-chemical measurements of blood and interviewer-administered questionnaires. The data items included height, weight, systolic blood pressure, diastolic blood pressure, sex, age, smoking history, alcohol intake, plas-ma folate, erythrocyte glutathione reductase activity co-efficient (EGRAC), pyridoxal phosphate (PLP) and serum vitamin B12. Height and weight were used to calculate body mass index (weight in kg/height2 in meters). Although there is considerable debate about the defi-nition of hyperhomocysteinemia, with suggested cut-offs ranging from 9 to over 20 µmol/L, hyperhomocysteine-mia was defined as a Hcy plasma level >15 µmol/L in our study as this is the cut-off used most fre-quently.7,15,16 Insufficient vitamin B2 status was defined as an EGRAC value of ≥1.2, a functional test for vitamin B2.17 In-sufficient folate was defined as a plasma folate ≤14 nmol/L (6 ng/ml).18,19 Insufficient vitamin B
6 status was defined as a plasma pyridoxal phosphate <30nmol/L,20 and insufficient vitamin B12 status was defined as a serum cobalamin ≤ 258 pmol/L.21
Statistical analyses
Statistical analysis was carried out using the SAS pro-gram (SAS/STAT Version 8.0, SAS Institute, Cary, NC). As the Elderly NAHSIT was conducted in a stratified, multistage probability design, sample weighting by SUDAAN, SAS-callable version 8.0 was used to account for the complex survey design in the variance estimates. The data was analyzed by gender, and age was grouped into the age groups 65-69, 70-74, 75-79, and 80 and older. The Student’s t test was used for analysis of differences in continuous variables between the groups with and without hyperhomocysteinemia. Differences were considered sig-nificant if P <0.05. Multiple logistic regression was used to obtain adjusted odds ratios (AOR) and 95 percent confidence intervals (95% CIs). Further analyses were done in which the data were stratified to investigate the AOR and 95% CIs of insufficiency in one or two B vita-mins in relation to hyperhomocysteinemia. All estimates were adjusted for potential confounders including age, systolic blood pressure, diastolic blood pressure, smoking and alcohol intake.
Results
The frequency distribution of various plasma Hcy levels in the Taiwanese elderly population is shown in Fig 1. The average plasma Hcy levels and prevalence of hyper-homocysteinemia are shown in Table 1. The average plasma Hcy level was 13.3 ± 0.6 µmol/L for males and 10.6 ± 0.7 µmol/L for females aged 65-90 years. The age-specific total plasma Hcy concentrations were signi-ficantly higher in males than in females for each age group, and significantly increased with age (P trend <0.0001). Furthermore, using the cut-off of 15µmol/L for hyper-homocysteinemia,15,16 our results showed that the prevalence of hyperhomocysteinemia was 23.4% for males and 11.2% for females. A higher percentage of hyperhomocysteinemia in males compared to females was noted in all age groups. In addition, a significant age
Males Age group N Homocysteine 1 (µmol/L) Hyperhomocysteinemia2 % (N) 65-69 421 12.6 ± 0.5* 17.6 (74) 70-74 377 13.1 ± 0.6* 21.8 (82) 75-80 203 14.1 ± 0.6* 32.0 (65) 80~ 93 15.6 ± 1.5* 37.7 (35) Total 1094 13.3 ± 0.6* 23.4 (256) P trend <0.0001 <0.0001 Females Age group N Homocysteine 1 (µmol/L) Hyperhomocysteinemia2 % (N) 65-69 467 9.7 ± 0.6 6.2 (29) 70-74 350 10.8 ± 0.6 10.0 (35) 75-80 198 11.3 ± 0.6 14.7 (29) 80~ 120 12.7 ± 1.0 28.3 (34) Total 1135 10.6 ± 0.7 11.2 (127) P trend <0.0001 <0.0001
1All valuesare shown as mean±SE or number of participants. 2Hyperhomocysteinemia: plasma homocysteine levels >15 µmol/L. *Significantly different from the female values (P<0.0001).
Table1. Plasma homocysteine levels and prevalence of hyperhomocysteinemia in the Taiwanese elderly, by age
trend (P trend<0.0001) in the prevalence of hyperhomo-cysteinemia was noted in both males and females.
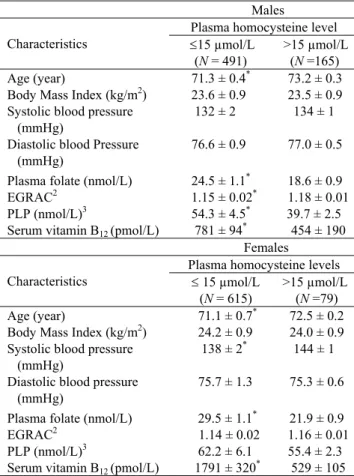
Epidemiological studies have shown that the level of Hcy is increased in chronic renal insufficiency.22 De-creased renal function with reduced clearance of Hcy results in elevated plasma Hcy levels which are inversely related to serum creatinine levels.23 Therefore, to in-vestigate the association between B vitamin status and Hcy levels, subjects with a serum creatinine ≥ 1.5 mg/dL were excluded. The clinical characteristics of the elderly subjects with normal renal function by plasma Hcy level are shown in Table 2. Folate, vitamin B2, B6, and B12 status were significantly better in males with normal Hcy levels as compared to those with hyperhomocysteinemia. Female subjects with normal Hcy levels, also had signi-ficantly better folate and vitamin B12 status, and lower systolic blood pressure, suggesting that folate and vitamin B12 status might have a more important impact on Hcy levels in the elderly population.
Table 3 shows the association between folate, vitamin B2, B6 or B12 insufficiency and hyperhomocysteinemia and confirms the importance of adequate vitamin B status in maintaining a normal Hcy level in the elderly. After adjustment for age, systolic pressure, diastolic pressure,
smoking and alcohol intake, the status of vitamin B6 (AOR =1.7, 95% CI 1.14-2.38 for males, AOR =2.1, 95% CI 1.28-3.47 for females), folate (AOR =3.0, 95% CI 1.94-4.60 for males, AOR =4.1, 95% CI 2.25-7.33 for females) and vitamin B12 (AOR =3.4, 95% CI 2.23-5.32 for males, AOR =3.3, 95% CI 1.72-6.32 for females) were significantly associated with hyperhomocysteinemia in both sexes. Vitamin B2 insufficiency was only signi-ficantly associated with hyperhomocysteinemia in males (AOR =1.7, 95% CI 1.19-2.51). We investigated whether the relationship between vitamin B2 and plasma Hcy in elderly Taiwanese was influenced by the status of other B vitamins. The association between insufficiency in one or two B vitamins and hyperhomocysteinemia is illustrated in Table 4, with subjects stratified on the basis of their B vitamin status. After adjustment for age, systolic pressure, diastolic pressure, smoking and alcohol intake, vitamin B2 insufficiency was not significantly associated with hyper-homocysteinemia in elderly persons with adequate folate, vitamin B6 and B12 status. However, vitamin B2 insuffi-ciency combined with poor vitamin B6 status (AOR=3.5 for B2 plus B6 vs. AOR=2.1 for B6 only), or poor vitamin B2 combined with poor folate status (AOR=4.5 for B2 plus folate vs. AOR=2.1 for folate only), were signi-ficantly associated with hyperhomocysteinemia. Insuffi-ciency in both vitamin B2 and B12 was not associated with hyperhomocysteinemia (AOR =6.4 for B2 plus B12 vs AOR =6.3, 6.5 for B12 only). These results suggest that the association between vitamin B2 insufficiency and hyperhomocysteinemia is influenced by folate and vita-min B6 status.
Table 2. Clinical characteristics of elderly persons with a serum creatinine below 1.5 mg/dL by plasma homocysteine level1
Males
Plasma homocysteine level Characteristics ≤15 µmol/L
(N = 491)
>15 µmol/L (N =165) Age (year) 71.3 ± 0.4* 73.2 ± 0.3 Body Mass Index (kg/m2) 23.6 ± 0.9 23.5 ± 0.9 Systolic blood pressure
(mmHg)
132 ± 2 134 ± 1 Diastolic blood Pressure
(mmHg)
76.6 ± 0.9 77.0 ± 0.5 Plasma folate (nmol/L) 24.5 ± 1.1* 18.6 ± 0.9 EGRAC2 1.15 ± 0.02* 1.18 ± 0.01 PLP (nmol/L)3 54.3 ± 4.5* 39.7 ± 2.5 Serum vitamin B12 (pmol/L) 781 ± 94* 454 ± 190
Females
Plasma homocysteine levels Characteristics ≤ 15 µmol/L
(N = 615)
>15 µmol/L (N =79) Age (year) 71.1 ± 0.7* 72.5 ± 0.2 Body Mass Index (kg/m2) 24.2 ± 0.9 24.0 ± 0.9 Systolic blood pressure
(mmHg)
138 ± 2* 144 ± 1 Diastolic blood pressure
(mmHg)
75.7 ± 1.3 75.3 ± 0.6 Plasma folate (nmol/L) 29.5 ± 1.1* 21.9 ± 0.9 EGRAC2 1.14 ± 0.02 1.16 ± 0.01 PLP (nmol/L)3 62.2 ± 6.1 55.4 ± 2.3 Serum vitamin B12 (pmol/L) 1791 ± 320* 529 ± 105
1All data excludes subjects with serum creatinine ≥1.5 mg/dL, and are
shown as mean±SE. 2Erythrocyte glutathione reductase activity
(EGRAC) was an indicator of vitB2 status. 3Plasma pyridoxal
phos-phate (PLP) was an indicator of vitB6 status. *Significantly different
between subjects with normal plasma homocysteine concentration and hyperhomocysteinemia (P<0.05).
Table 3. Adjusted Odds ratio (AOR) of hyperhomo-cysteinemia in elderly persons with a serum creatinine below 1.5 mg/dL1,2
Males
(N = 656) (N = 694) Females B vitamins
status3 Case/ normal (N) AOR4 95 % CIs Case/ normal (N) AOR4 95 % CIs Adequacy 96/344 1.0 55/458 1.0 Vit B2 Insufficiency 69/147 1.7 (1.19-2.51) 24/157 1.1 (0.64-1.84) Adequacy 84/316 1.0 43/462 1.0 Vit B6 Insufficiency 81/175 1.7 (1.14-2.38) 36/153 2.1 (1.28-3.47) Adequacy 112/432 1.0 63/571 1.0 Vit B12 Insufficiency 53/59 3.4 (2.23-5.32) 16/44 3.3 (1.72-6.32) Adequacy 113/424 1.0 57/565 1.0 Folate Insufficiency 52/67 3.0 (1.94-4.60) 22/50 4.1 (2.25-7.33) 1All data excludes subjects with a serum creatinine ≥1.5 mg/dL. 2Hyperhomocysteinemia: plasma homocysteine levels > 15 µmol/L. 3
The criteria for various B vitamins status was defined as following: insufficient vitamin B2 status was defined as EGRAC value ≥1.2, insufficient folate was defined as plasma folate ≤ 14 nmol/L (6
ng/ml), insufficient vitamin B6 status was defined as plasma
pyridoxal phosphate <30 nmol/L, and insufficient vitamin B12 status
was defined as serum cobalamin ≤ 258 pmol/L.
4
Adjusted for age (65-69, 70-74, 75-80 and >80), systolic pressure, diastolic pressure, smoking and alcohol drinking status (never, previous and everyday) by multiple logistical regression.
As shown in Table 4, our data indicate that in elderly men and women, insufficiency in vitamin B12 is the one most strongly associated with hyperhomocysteinemia in those who have adequate levels of the three other B vitamins (AOR =6.3, 95% CI 3.54-11.95 for males, AOR =6.5, 95% CI 3.18-23.28 for females). In addition, the presence of vitamin B2 or B6 insufficiency did not increase the odds of hyperhomocysteinemia in elderly males and females who had poor vitamin B12 status. As the association be-tween vitamin B12 insufficiency and hyperhomocys-teinemia does not seem to be greatly influenced by vita-min B2 or B6 status, greater attention should be paid to maintaining adequate vitamin B12 status in the elderly. Our results also showed that vitamin B6 insufficiency alone (AOR = 2.1, 95% CI 1.05 -3.87 for males, AOR = 2.4, 95% CI 1.06-5.25 for females), or folate in-sufficiency alone (AOR = 3.1, 95% CI 1.17-6.59 for males, AOR = 3.9, 95% CI 1.49-9.56 for females) were also associated with hyperhomocysteinemia. Moreover, the odds ratio of hyperhomocysteinemia in elderly males and females with both poor folate and vitamin B6 status (AOR = 12.5, 95% CI 4.56-34.63 for males; AOR = 12.4, 95% CI 3.71-41.50 for females) increased 3~4-fold com-pared to subjects with either poor folate alone or poor vitamin B6 status alone. In addition, the odds ratio of hyperhomocysteinemia in elderly males with both poor folate and vitamin B12 status (AOR = 16.4, 95% CI 3.76-71.78) increased 3~5-fold as compared with that in subjects with either poor vitamin B12 alone (AOR = 6.3, 95% CI 3.54-11.95) or poor folate status alone (AOR = 3.1, 95% CI 1.17-6.59). These data suggest that poor vitamin B6 status and poor vitamin B12 status each have a synergistic effect on the risk of hyperhomocysteinemia in elderly people with folate insufficiency.
Discussion
The average plasma Hcy concentration in Taiwanese el-derly persons aged 65 and over was 13.3 µmol/L for males and 10.6 µmol/L for females. Our study showed that the plasma Hcy level was higher in males than in fe-males and significantly increased with age, which is con-sistent with other studies.24,25 To compare our Hcy levels with other studies, we stratified age according to the age groups used in these studies and then reanalyzed our data. The mean Hcy level in Taiwanese elderly females was lower than figures from the USA (10.4 vs 10.7 µmol/L, aged 67-74yrs; 11.3 vs 11.9 µmol/L, aged 75-79yrs; 12.7 vs 13.2 µmol/L, aged >80yrs, Framingham study),24 Nor-way (9.4 vs 11.0 µmol/L, aged 65-67 yrs),25 Finland (10.1 vs 11.2 µmol/L, aged 65-74 yrs),26 England (10.6 vs 13.9 µmol/L, aged >65 yrs),27 Spain (10.6 vs 12.2 µmol/L, aged >65yrs),28 and New Zealand (11.0 vs 11.6 µmol/L, aged 70-80 yrs).29 However, Taiwanese elderly females had a higher mean value than Mexicans in the USA (9.7 vs 9.3 µmol/L, aged 60-69yrs; 11.0 vs 9.5 µmol/L, aged 70-79yrs; 12.8 vs 11.0 µmol/L, aged >80yrs, NHANES III).30 In other words, Taiwanese elderly women had lower Hcy levels than the elderly in countries with meat-dominated diets as the major dietary pattern, but did not have a lower value than Mexican Americans. This sug-gests that a vegetable-rich diet is beneficial, although ra-cial or ethnic differences may not be excluded.30 In addi-tion, higher folate intake by Taiwanese elderly women may contribute to their lower Hcy levels.31
The mean Hcy level in Taiwanese elderly males was lower than that in a British study (13.3 vs 16.0 µmol/L, aged >65),27 and similar to levels in Norway (12.3 µmol/L, aged 65-67 yrs) and Finland (12.8 vs 13.0 µmol/L, aged 65-74yrs).25,26 However, Taiwanese elderly males had a higher mean value than those reported in the Table 4. Adjusted Odds ratio (AOR) of hyperhomocysteinemia and insufficiency in one or two B vitamins in elderly persons with a serum creatinine below 1.5 mg/dL1,2
B vitamins status3,4 Male (N = 656) Female (N = 694)
Vitamin B2 Vitamin B12 Vitamin B6 Folate Case/normal (N) AOR 5
95 % CI Case/ normal (N) AOR 5 95 % CI + + + + 24/194 1.0 19/316 1.0 - + + + 12/53 1.9 (0.89-4.14) 7/87 1.3 (0.54-3.34) - + - + 20/47 3.5 (1.75-6.90) 8/46 2.7 (0.92-5.62) - + + - 5/11 4.5 (1.41-14.60) 1/4 4.2 (0.46-39.2) - - + + 6/8 6.4 (1.50-16.62) - - + - + + 14/18 6.3 (3.54-11.95) 6/15 6.5 (3.18-23.28) + - - + 8/10 6.5 (1.20-10.43) 4/10 6.4 (1.79-22.66) + + - + 20/78 2.1 (1.05-3.87) 11/79 2.4 (1.06-5.25) + + + - 10/29 3.1 (1.17-6.59) 7/28 3.9 (1.49-9.56) + + - - 12/8 12.5 (4.56-34.63) 6/8 12.4 (3.71-41.50) + - + - 6/3 16.4 (3.76-71.78) 1/5 4.2 (0.46-39.2)
1All data excludes subjects with a serum creatinine ≥1.5 mg/dL. 2Hyperhomocysteinemia: plasma homocysteine levels > 15 µmol/L. 3The
criteria for various B vitamins status was defined as following: insufficient vitamin B2 status was defined as EGRAC value ≥1.2,insufficient
folate was defined as plasma folate ≤14 nmol/L (6 ng/ml), insufficient vitamin B6 status was defined as plasma pyridoxal phosphate <30
nmol/L, and insufficient vitamin B12 status was defined as serum cobalamin ≤ 258 pmol/L. 4 '+' indicates B vitamin adequacy; '-' indicates B
vitamin insufficiency. 5Adjusted for age (65-69, 70-74, 75-80 and >80), systolic pressure, diastolic pressure, smoking and alcohol drinking
USA (13.0 vs 11.8µmol/L, aged 67-74yrs; 14.1 vs 11.9 µmol/L, aged 75-79yrs; 15.6 vs 14.1 µmol/L, aged >80yrs, Framingham study),24 Australia (14.6 vs 13.5µmol/L, aged 75yrs, Perth),32 and Spain (13.3 vs 12.6µmol/L, aged >65yrs).28 It is of note that Taiwanese elderly men had comparatively higher Hcy levels than men from the other countries, which is in contrast to the comparatively lower Hcy levels in Taiwanese elderly women.
The prevalence of hyperhomocysteinemia in the elder-ly has varied substantialelder-ly due to different cut-offs used by different studies. In our study, 23.4% of elderly men and 11.2% of elderly women had elevated Hcy levels (>15µmol/L). The overall prevalence was lower than that in the Framingham Study, USA (25.7 vs 29.3% >14µmol/ L, aged 70~80yrs).24 The prevalence of high Hcy levels in Taiwanese elderly females was lower than that in elderly women in New Zealand (18.0% >15µmol/L) and in NHANES III (44.0 vs 46.7% >10.4µmol/L, aged >60y),29,33 and similar to that in Australia (24.0% >13 µmol/L, aged >70y).32 In contrast, the prevalence of high Hcy levels in Taiwanese elderly men was higher (~1.4 fold) than that in Australia (33.8 vs 24.0% >15µmol/L, aged >75y),32 and in NHANES III (60.0 vs 43.2%>11.4 µmol/L, aged >60y).33 This indicates that the higher pre-valence of hyperhomocysteinemia in Taiwanese elderly males still needs to be monitored and improved upon. The average age of subjects with hyperhomocys-teinemia was significantly higher than that of subjects with normal Hcy levels, which agreed with the trend of an increased plasma Hcy level with age.24,25 Our study showed that females with hyperhomocysteinemia had higher systolic pressures than those with normal Hcy levels. This result supports the findings of the Hordaland Study and the paper by Brattstrom et al,25,34 although other studies have reported no association between sys-tolic pressure and Hcy.8
The four B vitamins – vitamin B2, B6, B12 and folate – which are involved in Hcy metabolism have been re-ported to be important determinants of plasma Hcy.6-11 Our data indicates that folate, vitamin B6 and B12 are in-dependent nutritional factors associated with hyper-homocysteinemia. In addition, elderly persons who have poor folate and vitamin B6 status, or poor folate and vita-min B12 status had a 3-5 fold increased risk of hyper-homocysteinemia compared to those with only one B vitamin insufficiency. These results agreed with the report that elevated Hcy concentration was associated with a combination of low plasma levels of vitamin B6, B12 and folate.24
Vitamin B2 insufficiency was only significantly asso-ciated with hyperhomocysteinemia in males. However, vitamin B2 insufficiency was not significantly associated with hyperhomocysteinemia in elderly persons who had adequate folate, vitamin B6 and B12 status. The combina-tion of vitamin B2 insufficiency with either vitamin B6 insufficiency or folate insufficiency increased drama-tically the adjusted odds ratio of hyperhomocysteinemia in elderly males as compared to deficiency in only one B vitamin. This suggests that the association between vita-min B2 insufficiency and hyperhomocysteinemia is influ-enced by folate and vitamin B6 status, and insufficiency of two B vitamins has a synergistic effect on the risk of
elevated Hcy. Therefore, adequate levels of vitamin B2, B6 , B12 and folate may be important for an optimal Hcy concentration in the elderly population.
Although the importance of vitamin B2 in Hcy meta-bolism is recognized,9,35 little attention has been paid to the relationship between Hcy and vitamin B2 levels in human studies, and the interactions among vitamin B2 and folate, or vitamin B6.36,37 The reason why this association has not been found in other studies might be due to good vitamin B2 status in the subjects investigated.38 The inadequate intake of milk and its products, which are a good food source of vitamin B2, has been reported in several surveys in Taiwan.39,40 Therefore, our results re-vealing the association between vitamin B2 and plasma Hcy levels may provide the rationale for a trial of the effect of Hcy lowering vitamin therapy for hyperhomo-cysteinemia in elderly persons in Taiwan.
In summary, this study provides information on plas-ma Hcy levels and the relationship between levels of Hcy and B vitamins in the Taiwanese elderly population. It is of note that the prevalence of plasma Hcy above 15 µmol/L was particularly high in elderly males at 23.4% but was lower at 11.2% in females. Vitamin B6, B12 and folate were independent nutritional factors associated with elevated Hcy levels in the Taiwanese elderly. A combination of insufficiency in two B vitamins had an additive effect on the risk of hyperhomocysteinemia. Although cause and effect was unable to be clarified in this cross-sectional study, good B vitamin status, par-ticularly that of folate and B12, should be emphasized as important for reducing Hcy concentrations of Taiwanese elderly persons, especially that of males .31
Acknowledgement
This study was supported by the Department of Health in Taiwan (DOH 94-TD-F-113-002). Data analyzed in this paper were collected by the research project "Elderly Nutrition and Health Survey in Taiwan (1999-2000) (Elderly NAHSIT)" carried out by the Institute of Biomedical Sciences of Academia Sinica. The Office of Nutrition Survey, The Center for Survey Research of Academia Sinica was responsible for data distribution. The assistance provided by the institutes and aforementioned individuals is greatly appreciated.
References
1. Finkelstein JD. Methionine metabolism in mammals. J Nutr Biochem 1990; 1: 228-237.
2. Guenther BD, Sheppard CA, Tran P, Rozen R, Matthews RG, Ludwig ML. The structure and properties of methylenetetrahydrofolate reductase from Escherichia coli suggest how folate ameliorates human hyperhomo-cysteinemia. Nat Struct Biol 1999; 6: 359-365.
3. Mckinley MC. Nutritional aspects and possible patho-logical mechanisms of hyperhomocysteinaemia: an independent risk factor for vascular disease. Pro Nutr Soc 2000; 59: 221-237.
4. Mccully KS. Vascular pathology of homocysteinemia: implications for the pathogenesis of arteriosclerosis. Am J Pathol 1969; 56: 111-228.
5. Mattson MP, Kruman II, Duan W. Folic acid and homocysteine in age-related disease. Ageing Res Rev 2002; 1: 95-111.
6. Ubbink JB, Vermaak WJ, van der Merwe A, Backer PJ. Vitamin B-12, Vitamin B-6, and folate nutritional status in men with hyperhomocysteinemia. Am J Clin Nutr 1993; 57: 47-53.
7. Selhub J, Jacques PF, Wilson PW, Rush D, Rosenberg IH. Vitamin status and intake as primary determinants of homocysteinemia in an elderly population. JAMA 1993; 270: 2693-2698.
8. Jacques PF, Bostom AG, Wilson PW, Rich S, Rosenberg IH, Selhub J. Determinants of plasma total homocysteine concentration in the Framingham Offspring cohort. Am J Clin Nutr 2001; 73: 613-621.
9. Jacques PF, Kalmbach R, Bagley PJ, Russo GT, Rogers G, Wilson PW, Rosenberg IH, Selhub J. The relationship be-tween riboflavin and plasma total homocysteine in the Framingham offspring cohort is influenced by folate status and the C677T transition in the methylenetetrahydrofolate reductase gene. J Nutr 2002; 132: 283-288.
10. Kang SS, Wong PW, Norusis M. Homocysteinemia due to folate deficiency. Metabolism 1987; 36: 458-462.
11. Homocysteine Lowering Trialist’s Collaboration. Lowering blood homocysteine with folic acid-base supplements: meta-analysis of randomized trials. BMJ 1998; 316: 894-898.
12. Selhub J. Folate, vitamin B12 and vitamin B6 and one carbon metabolism. J Nutr Health Aging 2002; 6: 39-42. 13. Lin BF, Lin RF, Yeh WT, Pan WH. The folate status in
Taiwan population from the NAHSIT 1993-1996. Nutr Sci J 1999; 24: 99-117.
14. Pan WH,Hung YT, Shaw NS, Lin W, Lee SD, Chiu CF, Lin MC, Chen SY, Hong CM, Huang TY, Chang HY, Tu SH, Chang YH, Yeh WT, Su SC. Elderly Nutrition and Health Survey in Taiwan (1999–2000): research design, methodology and content. Asia Pac J Clin Nutr 2005; 14 (3): 203-210.
15. Kang SS, Wong PW, Malinow MR. Hyperhomo-cyst(e)inemia as a risk factor for occlusive vascular disease. Ann Rev Nutr 1992; 12: 279-298.
16. Jacobsen DW. Homocysteine and vitamins in cardio-vascular disease. Clin Chem 1998; 44: 1833-1843.
17. Sauberlich HE, Dowdy RP, Skala JH. Laboratory tests for the assessment of nutritional status. 2nded. Boca Raton, FL: CRC press, 1973:55-69.
18. Raiten DJ, Fisher KD. Assessment of folate methodology used in the third National health and Nutrition Examination Survey (NHANES III, 1988-1994). J Nutr 1995; 125: 1371S -1398S.
19. Waters AH, Mollin DL. Studies on the folic acid activity of human serum. J Clin Pathol 1961; 14: 335-351.
20. Leklem JE. Vitamin B-6: A status report. J N 1990; 120 (suppl 11): 1503-1507.
21. Lindenbaum J, Rosenberg IH, Wilson PW, Stabler SP, Allen RH. Prevalence of cobalamin deficiency in the Fra-mingham elderly population.Am J Clin Nutr 1994; 60:2-11. 22. Chauveau P, Chadefaux B, Coude M, Aupetit J,
Hannedouche T, Kamoun P, Jungers P. Increased plasma homocysteine concentration in patients with chronic renal failure. Miner Electrolyte Metab 1992; 18: 196-198. 23. Bostom AG, Lathrop L. Hyperhomocysteinemia in
end-stage renal disease: prevalence, etiology, and potential relationship to arteriosclerotic outcomes. Kidney Int 1997; 52: 10-20.
24. Selhub J, Jacques PF, Bostom AG, D’Agostino RB, Wilson PW, Belanger AJ, O’Leary DH, Wolf PA, Rush D, Schaefer EJ, Rosenberg IH. Relationship between plasma homocysteine, vitamin status and extracranial carotid-artery stenosis in the Framingham Study population. J Nutr 1996; 126(4 Suppl): 1258S-1265S.
25. Nygard O, Vollset SE, Refsum H, Stensvold I, Tverdal A, Nordrehaug JE, Ueland M, Kvale G. Total plasma homo-cysteine and cardiovascular risk profile: The Hordaland Homocysteine Study. JAMA 1995; 274: 1526-1533. 26. Alfthan G, Laurinen MS, Valsta LM, Pastinen T, Aro A.
Folate intake, plasma folate and homocysteine status in a random Finish population. Euro J Clin Nutr 2003; 57:81-88. 27. Bates CJ, Schneede J, Mishra G, Prentice A, Mansoor MA.
Relationship between methylmalonic acid, homocysteine, vitamin B12 intake and status and socio-economic indices, in a subset of participants in the British National Diet and Nutrition Survey of people aged 65 y and over. J Clin Nutr 2003; 57: 349-357.
28. Ortega RM, Jimenez A, Andres P, Faci M, Lolo JM, Lozano MC, Bermejo LM, Lopez- Sobaler AM, Requejo AM. Homocysteine levels in elderly Spanish people: influence of pyridoxine, vitamin B12 and folic acid intakes. J Nutr Health Aging 2002; 6: 69-71.
29. de Jong N, Green TJ, Gibson RS, Mckenzie JE, Ferguson EL, Horwath CC, Thomson CD. Vitamin B12 and folate status of older New Zealand women. Asia Pac J Clin Nutr 003; 12 (1): 85-91.
30. Jacques PF, Rosenberg IH, Rogers G, Selhub J, Bowman BA, Gunter EW, Wright JD, Johnson CL. Serum total homocysteine concentrations in adolescent and adult Ame-ricans: results from the third National Health and Nutrition Examination Survey. Am J Clin Nutr 1999; 69: 482-489. 31. Chen KJ, Pan WH, Shaw NS, Huang RFS, Lin BF.
Association between dietary folate-rich food intake and folate status of elderly Taiwanese. Asia Pac J Clin Nutr 2005; 14: 244-249.
32. Flicker LA, Vasikaran SD, Thomas J, Acres JG, Norman PE, Jamrozik K, Lautenschlager NT, Leedman PJ, Almeida OP. Homocysteine and vitamin status in older people in Perth. Med J Aust 2004; 180 (10): 539-40.
33. Selhub J, Jacques PF, Rosenberg IH, Rogers G, Bowman BA, Gunter EW, Wright JD,Johnson CL: Serum total homocysteine concentrations in the third National Health and Nutrition Examination Survey (1991-1994): population reference ranges and contribution of vitamin status to high serum concentrations. Ann Intern Med 1999; 131: 331-339. 34. Brattstrom L, Lindgren A, Israelsson B, Anderson A,
Hultberg B. Homocysteine and cysteine: determinants of plasma levels in middle-aged and elderly subjects. J Intern Med 1994; 236: 633-41.
35. Hustad S, Ueland PM, Vollset SE, Zhang Y, Bjorke-Monsen AL, Schneede J. Riboflavin as a determinant of plasma total homocysteine: effect modification by the methylenetetrahydrofolate reductase C677T polymorphism. Clin Chem 2000; 46: 1065-1071.
36. Moat SJ, Ashfield-Watt PA, Powers HJ, Newcombe RG, McDowell IF. Effect of riboflavin status on the homo-cysteine-lowering effect of folate in relation to the MTHFR (C677T) genotype. Clin Chem 2003; 49: 295-302.
37. Lowik MR, van den Berg H, Kistemaker C, Brants HA, Brussaard JH. Interrelationships between riboflavin and vitamin B-6 among elderly people (Dutch Nutrition Sur-veillance System). Int J Vitam Nutr Res 1994; 64: 198-203. 38. Wolters M, Hermann S, Hahn A.B vitamins status and con-centrations of homocysteine and methylmalonic acid in el-derly German Women. Am J Clin Nutr 2003; 78: 765-772. 39. Wu SJ, Chang YH, Fang CW, Pan WH. Food sources of
weight, calories, and three macro-nutrients-NAHSIT 1993-1996. Nutr Sci J 1999; 24: 41-58.
40. Wu SJ, Chang YH, Wei IL, Kao MD, Lin YC, Pan WH. Intake levels and major food sources of energy and nutrients in the Taiwanese elderly. Asia Pac J Clin Nutr 2005; 14: 211-220.