A Lower Limb Fracture Postoperative-guided Interactive Rehabilitation Training
System and Its Effectiveness Analysis
Shih-Ching Yeh1, Shun-Min Chang2, Shu-Ya Chen3, Wu-Yuin Hwang4, Tzu-Chuan Huang1, Te-Lu Tsai5 1 Department of Computer Science & Information Engineering, National Central University, Taiwan
2 Department of Orthkijopedics, Landseed Hospital, Taiwan 3 Department of Physical Therapy, China Medical University, Taiwan 4 Institute of Network Learning Technology, National Central University, Taiwan
5 Institute for Information Industry
Abstract—Prior studies show that active-motion early after a fracture surgery can effectively reduce the tissue viscosity. However, due to the postoperative pain and unawareness of the postoperative limitations, a patient prefers to take medication to alleviate pain while complicated rehabilitation exercises can only be implemented under the limited intervention of a therapist, resulting in the patient's lack of interactive feedback on a daily basis and a failure of self-motions to miss the timing of rehabilitation. This study is intended to develop a lower limb fracture postoperative-guided interactive rehabilitation training system for the hip, knee and ankle joints, and establish a method of motion analysis and a method of motion performance assessment in conjunction with the wireless sensor technology and animation techniques, providing an objective assessment from the caregiver and learning the patient's rehabilitation status with a simple and easy recording means. Additionally, with the design of interactive feedback, the improved postoperative rehabilitations are tried to increase the participant’s interest in self-management of health and facilitate to keep tracking the rehabilitation information. The medical evidences show that a guided rehabilitation system can enhance the patient's motive and willingness to be committed to a rehabilitation training as well as increase Quality and Amount of the exercise activity during the training process.
Keywords-rehabilitation; wireless sensor; virtual reality I.INTRODUCTION
A century ago, surgical masters H. Owen, Thomas, Robert Jones and Watson, Jones [1] believed that a fracture healing would absolutely need continuously uninterruptedly rest and immobilization. However, in Europe, the philosophy of MD Lucas-Championniere [2] was “Life is Motion”, and even by means of surgery, the motion function of muscles and joints must be restored early.
With development of pathological physiology, biomechanics, mechanics of materials, adequate fracture reduction and stable fixation can restore the original structure and stability of the bone, so that the limbs can move earlier. Many studies have found that earlier motions provide better functional recovery than immobilization and have a better effect on the functional recovery of acute limb trauma. A treatment of forced rest and motion restriction is
likely to cause complications. Due to lack of motive and knowledge, most patients can not reach the amount of motion as they are required, which lead to their abandonment of rehabilitation, and the medical staff thus can not objectively assess the patient's physical exercise and can not determine whethera the patient observes the doctor's instructions.
The major joints of the lower extremity include ankle, knee, and hip. The ankle joint has the following ranges of movement: dorsiflexion, plantar flexion, varus and valgus. The knee joint has the following ranges of movement: flexion and extenstion. The hip joint has the following ranges of movement: flexion, extension, abductio, adduction, internal rotation, and external rotation. To remember all these movements is too difficult to a patient without medical background. The complicated and puzzled rehabilitation exercises are coupled with too many procedures that are hard to remember, resulting in improper motions that adversely affect the patient who in turn is reluctant to continue the rehabilitation exercises. On the other hand, in addition to the physical injury caused by a fracture, a patient of previously independent individual may become someone who relies on caring, being unable to move freely and go to work, the usual interpersonal relations and social interactions being affected, and the anxiety and feeling of helplessness also reduce the patient’s willingness for rehabilitation.
With the ever-changing sensor technology, wireless communication technology, three-dimensional display technology, robot technology, 3D animation technology and network technology, not only there is an improvement at technical level but popularity at economical level. Many scholars in studies relating to medical rehabilitation in the world and frontline medical physicians or therapists constantly try to utilize and integrate the above technologies. On theoretical basis of Virtual Reality, Augmented Reality, Mixed Reality, introducing the concept of User Centered design (patient), taking into account of the user’s perception, usability and immersion, and using the interactive mode and strategy provided by a man-machine interface, they developed a wide variety of innovative rehabilitation therapies and rehabilitation techniques.
For this reason, this study is primarily intended to develop a lower limb fracture postoperative-guided
interactive rehabilitation training system for the hip, knee and ankle joints with the wireless sensor technology and 3D animation techniques and examine an interactive feedback mechanism’s [3] impact on the patient’s motive to be committed to rehabilitation training and whether the patient will further stick to rehabilitation; and use the motion data acquired by wireless sensors through clinical experiments to establish the method of motion analysis to assess patient’s lower limb exercise capacity and achievement through a rehabilitation training program, and provide caregivers with an assessing-objective and recording-easy means for accurately tracking the patient's rehabilitation status; and further analyze whether the guided interactive rehabilitation system by using technology can increase a exercise training’s amount within the fixed timeframe of rehabilitation training arrangement and increase the exercise training’s quality during each single training activity while using a network to provide links from medical staff to medical staff, from medical staff to patient, and even from patient to patient without compromising any security of patient information.
II.LITERATUREREVIEW
Mirelman et al. [4] also published the results of using virtual reality to assist rehabilitation in 2009 and the study divided 18 patients into 2 groups, where one group received Robot Virtual Reality System assisted lower limb walking training and another group took Robot Alone for walking training. After four weeks, the walking distances before and after the training were compared by 6-minute walk test (6MWT) and it was found that in terms of the patient's walking speed or walking distances, every patient in the group of Robot Virtual Reality System assisted lower limb walking training performed better than the group of Robot Alone walking training, and the training effect could last up to 3 months after end of the training.
The scholars Kenyon & Afenya et al. [5] suggested an exercise training in 1995, where 24 subjects (age 21 to 45 years old) repeated pickup and drop task in a virtual reality or moved the jars in position of certain color in front row to the position of same color in rear row. As a result, these trained subjects virtually made more progress when they did the same thing in the real world, which proved that the training effect in a virtual reality can virtually be transferred to the real environment. Further, The scholars Rose et al. [6] suggested a grouping training for 210 subjects (average age 35.5 years old) in 2000, where it was found that the group using steadiness tester for sensorimotor task training in a virtual reality made a significant progress after the therapy, that is, these subjects would make a significant progress when they were back in a real environment to do the same thing after the therapy, which also proved that the training effect in a virtual reality can virtually be transferred to the real environment.
The scholars Merians et al. [7] in 2002 suggested a 1.5 hours non-immersive hand function training in a virtual
reality based on the case reports for three chronic stroke patients, where the content of training includes finger joint ROM, movement speed, muscle strength and movement ability of one single finger, and a 3.5 hours constraint induced movement treatment. After nine number of therapies, it was found that the finger joint ROM, movement speed, muscle strength and movement ability of one single finger had all been improved. The scholars Broeren et al. [8] in 2004 suggested a ball knockdown bricks game training in a non-immersive virtual reality based on the case report for a stroke patient of 3 months history, where one therapy took 90 minutes in a total of 12 times for four weeks, and it was found that on the impaired side, the finger’s delicate movement, grasp strength and movement control had all been improved, and the therapeutic effect could be maintained for 20 weeks. The scholars Jeffe [9] et al. in 2004 suggested a hurdling training in an immersive virtual reality for 10 chronic stroke patients, where one therapy took 60 minutes in a total of six times for two weeks. In contrast with the control group, it was found that their walking speed, step length, walking endurance and hurdling ability had all been improved significantly.
III.RESEARCHMETHODS
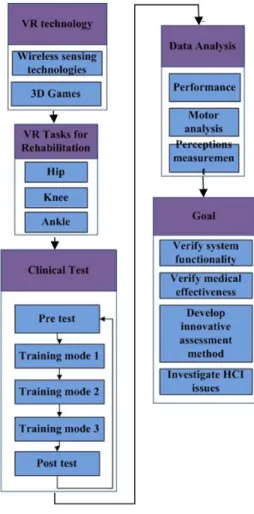
The aim of this study is to develop a lower limb fracture postoperative-guided interactive rehabilitation training system for the hip, knee and no ankle motion this time with the wireless sensor technology and 3D animation techniques and examine Interactive Feedback mechanism’s impact on the patient’s motive to be committed to rehabilitation training; use the motion data acquired by clinical experiments to develop new assessment methods to assess the patient's rehabilitation status; and further analyze the impact on quality and amount of the rehabilitation exercise training. The architecture of this study is shown in Figure 1.
This study hypothesizes:
1. Compared to a traditional rehabilitation method, the patients who use a guided interactive rehabilitation training system have a higher motive to be committed to the rehabilitation training.
2. Compared to a traditional rehabilitation method, the patients who use a guided interactive rehabilitation training system have a higher quality during the rehabilitation exercise training.
3. Compared to a traditional rehabilitation method, the patients who use a guided interactive rehabilitation training system have a higher amount during the rehabilitation exercise training.
A. SYSTEM ARCHITECTURE
This system substantially comprises a motion sensor unit and an immersive interaction unit (as shown in figure 2). The motion sensor unit includes the developed wireless sensors, where the IMU sensor measures an object’s posture values (pitch, yaw and row) and transmits the measured data by
wireless transmission module. The lower limb sensor converts the received angle degrees to 0 - 255 digital signals which are sent to a PC via Zigbee with a plurality of wireless sensors attached to the lower limb to form a wireless sensor network and acquire the posture values of the overall lower limb (including hip, knee and no ankle motion this time). Immersive interaction unit will reconstruct a plurality of received overall posture values of lower limb sensors and display them in animation on screen for viewing by the medical staff and patients, enabling the patients to know their lower limb’s posture; the multi-representations including texts, images and sounds are designated to advise the patient about the current status and desirable task in order to guide and motivate the patient to achieve or surpass the desirable task set by the physician or therapist. Also, when the rehabilitation is finished each time, the related data will be saved to the database to allow the physician or therapist to review the patient’s rehabilitation.
Figure 1. Research framework
(1)Wireless IMU sensor
Advances in technology can bring a brand new solution to existing problems. With development of MEMS process in recent years, IMU (Inertial measurement unit) is already acceptable in the consumer market in terms of its size, weight and cost, which can sensitively detect a moving limb’s trajectory only if it is put on that limb, and using a
low-power wireless transmission can avoid haltering cables and all the patient’s motions can be recorded to a computer only by analyzing the sensed postures to provide the medical staff with detailed and objective records and to allow learning the participant’s exercise quality. 9DOF Razor IMU is integrated with three sensors of gyro, accelerometer and magnetometer to provide measurement of nine degrees of freedom. All the sensor signals will be processed before transmission through a serial interface. XBee is a wireless transmission device based on ZigBee, providing up to 250kps rate, where the transmission range and power consumption vary from its types. XBee explorer switches Xbee to USB interface and UART signals are analoged by FTDI to USB Arduino FIO, and XBee 20pin connector and FTDI interface are provided to connect Xbee to 9DOF Razor IMU and the posture data is obtained by the IMU that can connect with an external power (LIPO battery) and power recharging, and output by UART and switched by FIO to Xbee and then transmitted to Xbee that is connected to a computer’s receiving port through XBee explorer, at this point, the data is send to the interface of serial port before being read and converted by the program. The power required by the separately transmitting port is provided by a FIO connected lithium-ion battery.
Figure 2. System Architecture
(2)Interactive guided system (Visual, Auditory)
The system uses Unity 3D to make a demonstration of the lower body’s movements to provide the participant with exercise guidance, and a real-time instruction of health knowledge can bring more impressions and memories to the participant than an only oral instruction, which can not only increase the early motives for exercise but self-care knowledge, and if the design of interactive feedback game is added, it can further deflect attention from pain and remove worries, additionally, it can easily keep contact with the participant and follow up using a network. The integration of technology with medicals brings progress to the rehabilitation program, which both enables the participant to have a strong motive to persist in rehabilitation and provides caregivers with an objectively assessing and recording means for accurately tracking the patient's condition. The user interface provides options for time-motions and measurement methods which include selecting rehabilitation exercise for legs (e.g. thighs or calves) and selecting 30, 60, and 90 seconds or no time limit for measurement time, and the experimental process includes a control group and an experimental group and thus the interface is also divided into
two areas for physiatrist and computer respectively to facilitate selection during the experiment. The subject watches the screen that provides real-time rehabilitation information and makes various movements for rehabilitation according to the operator’s instruction and display which provides a virtual animation of leg movements as exercise instructions or as a means to allow the subject know his/her performance, and if the rehabilitation requirement is not met, the leg’s angle information will also be displayed. The system also provides the subject with a real movie regarding this rehabilitation exercise for reference. After finishing all experiments, the statistical data will be listed for the subject to review.
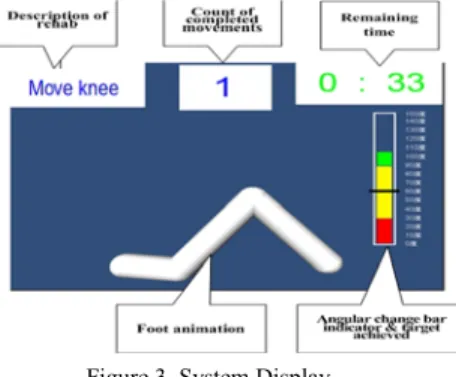
During the experiment, the Gyro sensor transfers the coordinate information in strings to the computer in which the software connects and receives it through Socket Client, and once the received strings are split, the coordinate of the sensor will be identified. Through thigh and calf sensors, the thigh and knee’s bending angle can be identified, by means of which, the subject can freely control the leg animation in the system to achieve the required movement for rehabilitation. The received angle information is also displayed in real-time to allow the subject to know at any time the thigh and knee’s bending degree. Additionally, the information of angles and movements in the experiment will be recorded and then downloaded in txt file for data analysis (as shown in figure 3).
Figure 3. System Display
B. EXPERIMENTAL DESIGN
This study lasts for two days, each about 30 minutes. At the beginning, the investigator put on a movement analyzer for the subject and the experimental group is equipped with a notebook computer. The interaction feedback program is run after verifying proper connection between the movement analyzer and the computer and all the instruments including the analyzer, wearing gears and notebook computer are recovered after finishing each time. The control group wears the analyzer and is instructed by the investigator about traditional rehabilitation according to the same rehabilitation program, the analyzer and wearing gears are also recovered after finishing each time.
(1) This study’s case acceptance criteria: 1. Age: 20 – 65 years old.
2. Acute ankle fracture (<72 hours from injury). 3. AO-Weber fracture classification system: type A
or B.
4. Open reduction and internal fixation according to AO/ASIF surgical principles.
5. The precise indications for surgery: a. single, double or three ankle injury and/or fibula shift > 2 mm found in any plane X-ray. (b) No attempt to repair ligaments or other potential soft tissue injuries.
6. Spinal anesthesia or general anesthesia.
7. The attending physician professionally identifies the postoperative rehabilitation will not involve any concern about nail fixing or joints.
8.
The patient who is in stable condition after surgery and needs not to be moved into ICU for further treatment.9. The patient who can observe the postoperative agreement and doctor’s prescriptions.
(2) Exclude criteria: 1. Open fractures. 2. Pilon tibial fractures. 3. Compartment syndrome.
4. Screws fixed tibiofibular syndesmosis.
5. Multiple fractures or accompanying other serious system injuries.
6. Serious complications during hospitalization: myocardial infarction, stroke, neurovascular injury, deep infection, or back surgery room.
7. The patient who can not complete the
rehabilitation program during hospitalization due to personal or medical factors.
8. can not be discharged within seven days after surgery due to medical conditions.
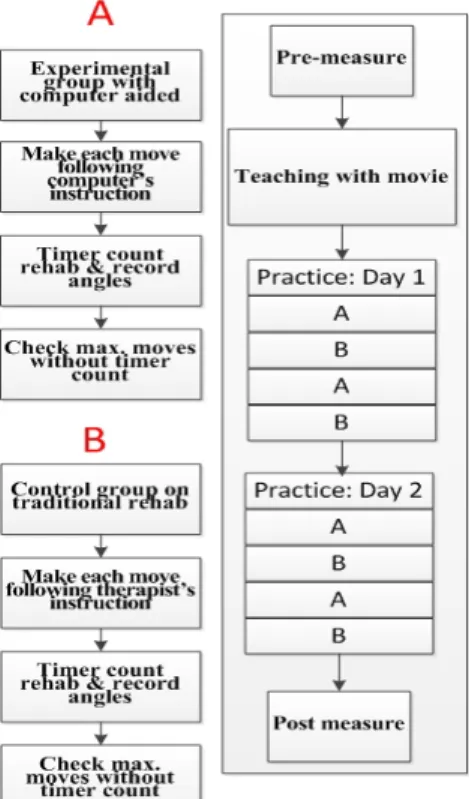
In event of feeling pain or unwell in any rehabilitation exercise, stop the exercise immediately and the trainer will ask the subject about the next exercise. The experiment takes two days and the experiment is carried out and completed in sequence of group A (experimental group), group B (control group), group A (experimental group) and group B (control group), and the experimental group sequentially makes every movement in a specific rehabilitation exercise, for which the patient is required to see a computer demonstration or listen to a rehabilitator’s instruction in advance; count the movements within a limited time and without any time limit respectively and see in which case the patient’s interest in rehabilitation exercise may be stimulate (as shown in figure 4).
For the experimental group, during the experiment, the subjects can real-time rehabilitating status of their legs through the system and learn the next movement mode. Through an animation presentation, a subject can properly determine his/her current deviation from the correct posture so as to achieve the correct guiding effect that enable the subject to focus on the entire process of rehabilitation and have a feeling of complete involvement while constantly knowing the rehabilitation progress information such as the completed movements for a rehabilitation, remaining time, angle of knee and thigh.
For the control group, the rehabilitator substantially dominates a rehabilitation process in which the subject can not learn any information that may be available to the experimental group or a subject must fully follow the rehabilitator’s instructions to complete such an experiment. The rehabilitation exercise includes bending knee and raising thigh, where a complete knee movement is to expect that the
knee’s bending angle exceeds 90 degrees and a complete thigh movement means it raises 40 degrees.
Figure 4. Experiment Architecture
(3)EXPERIMENTAL PROCEDURE
The experimental procedure comprises 4 stages, where the experimental group proceeds ahead of the control group for each stage.
a) Stage I: Alternative movements, firstly the knee’s bending exercise, then the thigh’s raising exercise. Record the completed number of exercises, durations and course angles of thigh and calf.
b) Stage II: 90 seconds each for the knee’s bending movement and the thigh’s raising movement and complete as many movements as possible within 90 seconds and record the completed exercise number.
c) Stage III: complete 15 times each for the knee’s bending movement and the thigh’s raising movement, and record durations and course angles of knee and thigh.
d) Stage IV: complete a number of knee bending movements and the thigh raising movements respectively according to the subject’s willingness without limiting time and number, and record durations, numbers and course angles of knee and thigh.
IV.MEASUREMENT AND ANALYSIS
A. Exercise performance assessment
The training items of this study include 90 second exercises (thigh/knee), knee rehabilitation exercises without time limit and fixed number of exercises (thigh/knee). After the training, record the exercise number, duration and course
angular change, and use a program of data analysis to obtain an average duration for both each bending knee and each raising thigh, finally use the data in SPSS for paired samples T-test.
The data obtained from the training items: in a fixed number training, the efficiency is determined from a less time spent by either of the experimental group and the control group; and in a training of 90 second timer count up, the efficiency is also be determined from a significantly more exercise numbers carried out by either of the experimental group and the control group. Subsequently, in a training of knee rehabilitation exercise without time limit, the number and duration can be obtained for this training, and from these data, it can be learnt whether the computer-aided or traditional rehabilitation can stimulate a subject’s interest more and increase their willingness to be involved. Again, this study use a course angle information for data analysis and obtain the area for each angular change, from which it can be learnt whether the subject achieved a targeting angle quickly or moved slowly hesitantly.
C. Motion analysis assessment
This study use a course angle information for data analysis and calculate the area value for all the angel changes to time, from which it can be learnt whether the subject can achieve a targeting angle quickly or move slowly hesitantly.
The summed area per unit of time is the bending knee/raising thigh angular change sweep area. Accordingly, by comparing the area for the experimental group and control group, which group has exercised more efficiently can be determined.
V.DISCUSSION
This study recruited two healthy young people over 20 years old as the subjects for a pilot test, both subjects used the rehabilitation system described herein and the aforementioned experimental procedure for two-day experiment, and based on the data collected in the experiment, the assessments for exercise performance, motion analysis and susceptibility were carried out separately.
A. Motion analysis assessment
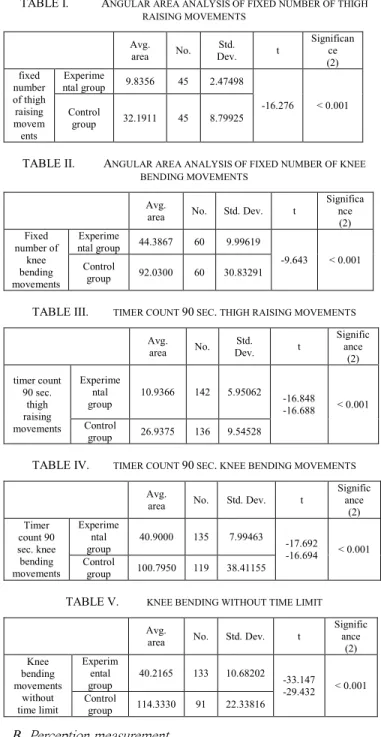
The indicator for motion analysis assessment is the area value of course angle data, where smaller area represents higher motion efficiency. The analysis result shows that for the training mode of fixed number (15) of exercises, both thigh raising exercise and knee bending exercise have significant deviation (p<0.001), as shown in table I & II, and the subject of a guided rehabilitation system has better motion efficiency; for the training mode for a fixed time (90 seconds), leg movement or knee bending motion subjects were significant differences (P <0.001), as shown in table III & IV, and the subject of a guided rehabilitation system has better motion efficiency; for the training mode without time limit, the knee bending exercise has a significant deviation (p<0.001), as shown in table V, and the subject of a guided rehabilitation system has better motion efficiency, thus indicating that assumption two is true.
TABLE I. ANGULAR AREA ANALYSIS OF FIXED NUMBER OF THIGH RAISING MOVEMENTS
Avg.
area No. Dev. Std. t
Significan ce (2) fixed number of thigh raising movem ents Experime ntal group 9.8356 45 2.47498 -16.276 < 0.001 Control group 32.1911 45 8.79925
TABLE II. ANGULAR AREA ANALYSIS OF FIXED NUMBER OF KNEE BENDING MOVEMENTS
Avg.
area No. Std. Dev. t
Significa nce (2) Fixed number of knee bending movements Experime ntal group 44.3867 60 9.99619 -9.643 < 0.001 Control group 92.0300 60 30.83291
TABLE III. TIMER COUNT 90 SEC. THIGH RAISING MOVEMENTS
Avg.
area No. Dev. Std. t
Signific ance (2) timer count 90 sec. thigh raising movements Experime ntal group 10.9366 142 5.95062 -16.848 -16.688 < 0.001 Control group 26.9375 136 9.54528
TABLE IV. TIMER COUNT 90 SEC. KNEE BENDING MOVEMENTS
Avg.
area No. Std. Dev. t
Signific ance (2) Timer count 90 sec. knee bending movements Experime ntal group 40.9000 135 7.99463 -17.692 -16.694 < 0.001 Control group 100.7950 119 38.41155
TABLE V. KNEE BENDING WITHOUT TIME LIMIT
Avg.
area No. Std. Dev. t
Signific ance (2) Knee bending movements without time limit Experim ental group 40.2165 133 10.68202 -33.147 -29.432 < 0.001 Control group 114.3330 91 22.33816 B. Perception measurement
The result of questionnaires is shown in table VI and by analyzing the data, it is found that the scores are higher with respect to Presence, Ease of use and Flow theory, indicating that the subject’s immersion for the guided rehabilitation system is high and thus assumption one is true, and it is felt that a guided rehabilitation system can be used more easily.
TABLE VI. PERCEPTION MEASUREMENT
Presence Usefulness Playfulness Ease of use Intention to use theory Flow Control group 4.3 4.0 3.6 4.2 4.4 4.1 Experim ental group 4.5 4.0 3.2 4.0 4.4 4.6 VI.CONCLUSION
This study has successfully integrated the wireless sensor technology with animation techniques to develop a lower limb fracture postoperative-guided interactive rehabilitation training system for the hip, knee and no ankle motion this time joints; has successfully developed a motion analysis method to assess the motion efficiency using the motion data acquired by clinical experiments; and the medical evidences have showed that a guided rehabilitation system can enhance the patient's motive and willingness to be committed to rehabilitation training as well as increase quality and amount of the exercise activity during the training process. Accordingly, this study believe that using a guided rehabilitation system can help the patient alleviate feel of the injury pain and make the patient more focused and pay more attention in order to achieve the best rehabilitation result. Additionally, the patient’s lower limb rehabilitation data can be saved to a database to provide the rehabilitation physician for analysis and comparison and enable the rehabilitation physician to review the patient’s rehabilitation condition, and it can also be used as an indicator for improvement.
ACKNOWLEDGEMENT
We are grateful for the support of the National Science Council, Taiwan, under NSC 100-2221-E-008-043- & NSC 100-2631-S-008-001, and Microsoft in Taiwan. Also, this study is conducted under the ”Smart terminal software and networked television platform development ”of the Institute for Information Industry which is subsidized by the Ministry of Economy Affairs of the Republic of China.
REFERENCES
[1] Thomas, G., H. Whalley, and C. Modi. "Early mobilization of operatively fixed ankle fractures: a systematic review." Foot Ankle Int. 30.7 (2009): 666-74.
[2] Lucas-Championniere, J. "The treatment of fractures by mobilization and massage. 1908." Hand Clin. 12.1 (1996): 167-71.
[3] Reusch, A., et al. "Effectiveness of small-group interactive education vs. lecture-based information-only programs on motivation to change and lifestyle behaviours. A prospective controlled trial of rehabilitation inpatients." Patient.Educ.Couns. (2010).
[4] Mirelman A, Bonato P, Deutsch JE. Effects of training with a robot-virtual reality system compared with a robot alone on the gait of individuals after stroke.Stroke 2009;40:169-74.
[5] Kenyon RV, Afenya MB. Training in virtual and real environments. Ann Biomed Eng 1995; 23:445-.
[6] Rose FD, Attree EA, Brooks BM, Parslow DM, Penn PR, Ambihaipahan N et al. Training in virtual environments: transfer to real world tasks and equivalence to real task training. Ergonomics 2000; 43:494-511.
[7] Merians AS, Jack D, Boian R, Tremaine M, Burdea GC, Adamovich SV et al. Virtual reality-augmented rehabilitation for patients following stroke. Phys Ther 2002;82:898-915.
[8] Broeren J, Rydmark M, Sunnerhagen KS. Virtual reality and haptics as a training device for movement rehabilitation after stroke: a single-case study. Arch Phys Med Rehabil 2004;85:1247-50.
[9] Jaffe DL, Brown DA, Pierson-Carey CD, Buckley EL, Lew HL. Stepping over obstacles to improve walking in individuals with poststroke hemiplegia. J Rehabil Res Dev 2004;41:283-92.