國立臺灣大學醫學院臨床醫學研究所 碩士論文
Graduate Institute of Clinical Medicine College of Medicine
National Taiwan University Master Thesis
第二型糖尿病女性患者的嚴重排尿障礙發生率較高:
根據全國人口所進行的世代研究
Women with type 2 diabetes are associated with higher incidence of significant voiding dysfunction:
A nationwide population-based cohort study 賴明志
Ming-Chih Lai
指導教授: 余宏政 台大醫院泌尿部教授
陳祈玲 台大臨床醫學研究所副教授 Advisor: Hong-Jeng Yu, Professor
Chi-Ling Chen, Associate professor
中華民國 108 年 07 月
國立臺灣大學碩士學位論文 口試委員會審定書
第二型糖尿病女性患者的嚴重排尿障礙發生率較高:
根據全國人口所進行的世代研究
目 錄
口試委員會審定書 ... 1
誌謝 ... 4
中文摘要 ... 5
英文摘要 ... 7
碩士論文內容 1. Introduction ... 9
1.1 Background ... 9
1.2 Objectives ... 9
2. Materials and methods ... 10
2.1 Data source ... 10
2.2 Study design ... 11
2.3 Study participants ... 11
2.4 Statistical analysis ... 12
3. Results ... 12
3.1 Participants and descriptive data ... 12
3.2 Main results ... 13
3.3 The analysis of subgroups ... 14
3.4 The analysis of new users of bethanechol, tamsulosin or combination therapy... 14
4. Discussion ... 15
4.1 The interpretation of our database ... 15
4.2 Summarize main results ... 15
4.3 The interpretation of results of subgroup analysis ... 17
4.4 Summarize the trend of new users of bethanechol, tamsulosin or combination therapy .. 18
4.5 Limitations ... 19
5. Conclusion ... 20
6. Future perspectives ... 20
7. References ... 22
8. Figures and tables ... 27
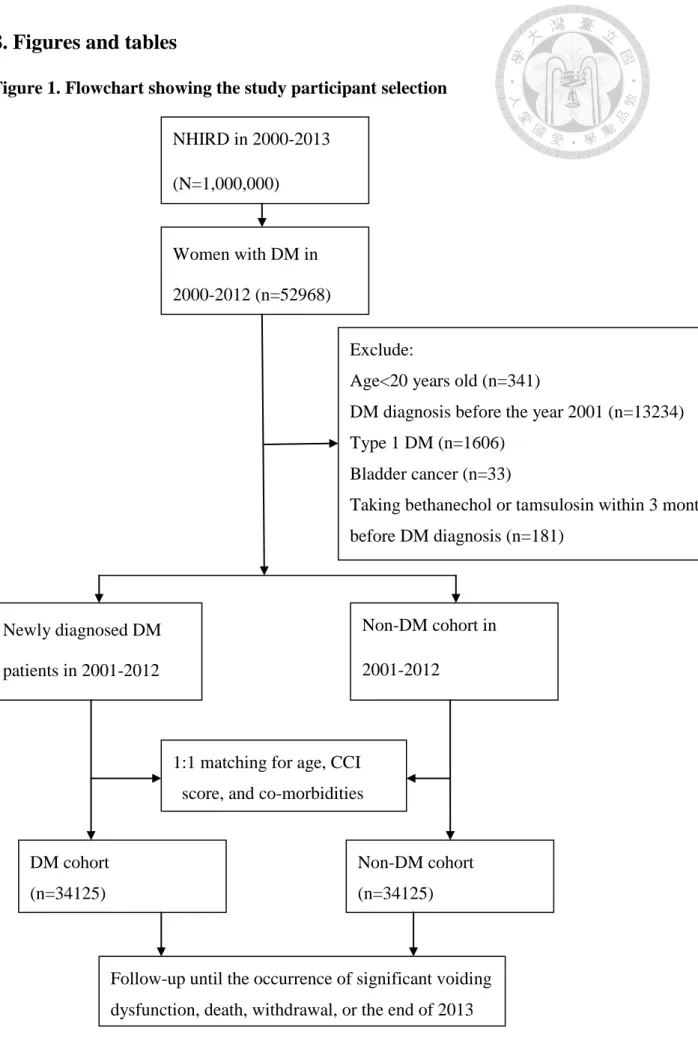
Figure 1. Flowchart showing the study participant selection ... 27
Table 1. Characteristics between patients with and without DM ... 28
Table 2. Incidence rates and hazard ratios (HR) of significant VD for DM and potential risk factors in multivariate cox regression model analysis ... 30
Table 3. Subgroup analysis for incidence and hazard ratio (HR) of significant VD between patients with and without DM, stratified by age and CCI ... 32
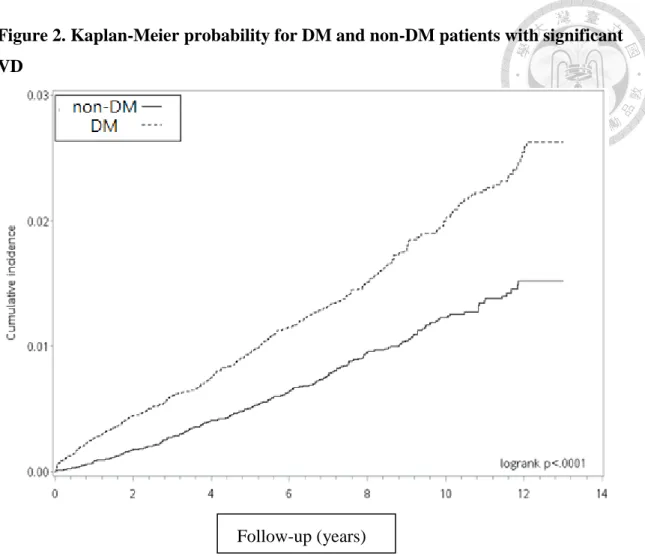
Figure 2. Kaplan-Meier probability for DM and non-DM patients with significant VD ... 34
Figure 3. The number of new users of bethanechol, tamsulosin, or combination therapy by year ... 35
Appendix ... 36
誌謝
特別謝謝余宏政教授和陳祈玲副教授不辭辛勞、不厭其煩的指導。
謝謝戴槐青醫師一起討論與寶貴的建議。
感謝台北市立醫院教學研究部公衛中心提供研究資料與協助。
賴明志 中華民國一零八年七月二十四日
中文摘要
目標
本研究是在13年的期間內,評估第二型糖尿病女性患者的嚴重排尿障礙(VD)的 發生率和風險。
研究材料和方法
這 份 世 代 群 組 研 究 使 用 了 台 灣 全 民 健 保 研 究 資 料 庫 (National Health Insurance Research Database, NHIRD)的資料,從2001年到2013年中,找出新診 斷的第二型糖尿病患者(DM世代群組),以及符合年齡、共病現象和Charlson共 病指標(CCI)分數的患者(非DM世代群組)。嚴重VD的定義為膀胱排尿有困難,需 要bethanechol或tamsulosin的治療。對於嚴重VD的發生率,我們調查到2013年底 為止。據此計算出嚴重VD的發生率(每年每一萬人),並使用Cox比例風險迴歸模 型 (Cox proportional hazards regression model) 估 算 風 險 比 例 。 使 用 Kaplan-Meier法(Kaplan-Meier),在兩個世代群組中,繪製出嚴重VD的累積發生 率圖形。
結果
在13年期間,第二型糖尿病女性患者的嚴重VD發生率為1.42%。DM世代群組和非
DM世代群組共納入34,125位病患。嚴重VD發生率在DM世代群組和非DM世代群組中,
分別約為有20.0位和11.4位(每年每一萬人)。針對混擾因子進行修正後,可以 推算出,第二型糖尿病女性患者的嚴重VD發生率風險增加1.79倍。在10年的後續 追 蹤 期 間 ,DM 世 代 群 組 的嚴 重 VD 累 積 發 生 率 顯 著 較 高(2.01% vs. 1.07%, p<0.0001)。
結論
對於女性,第二型糖尿病和嚴重 VD 的風險上升有關聯性。因此,臨床醫師應該教 育女性病患,使其了解第二型糖尿病和嚴重 VD 之間的關聯性。
關鍵字:糖尿病;排尿障礙;發生率;女性;台灣
英文摘要
Objective:
To evaluate the incidence and risk of significant voiding dysfunction (VD) in women with type 2 diabetes during a 13-year study period.
Materials and methods:
This cohort study utilized data from the National Health Insurance Research Database (NHIRD) of Taiwan to identify patients with type 2 diabetes (DM cohort) and age-, comorbidity-, and Charlson comorbidity index (CCI) score-matched cohort (non-DM cohort) from 2001 to 2013. Significant VD was defined as difficulty in bladder emptying requiring bethanechol or tamsulosin treatment. Significant VD occurrence was monitored until the end of 2013. Incidence rate of significant VD (per 10,000 person-years) was calculated, and hazards ratios were estimated using Cox proportional hazards regression models. Cumulative incidence of significant VD in both cohorts were plotted using the Kaplan-Meier method.
Results
Incidence of significant VD in women with type 2 diabetes is 1.42% during a 13-year period. A total of 34,125 patients were selected for the DM and non-DM cohorts, respectively. Incidence rates of significant VD were approximately 20.0 and 11.4 per 10,000 person-years for the DM and non-DM cohorts, respectively. After adjusting for potential confounders, a 1.79-fold increased risk of significant VD was observed in
women with type 2 diabetes. Cumulative incidence of significant VD was significantly higher in the DM cohort at the 10-year follow-up (2.01% vs. 1.07%, p<0.0001).
Conclusion
Type 2 diabetes is independently associated with increased significant VD risk in women. Therefore, clinicians should be aware of and educate female patients about the association between type 2 diabetes and significant VD.
Key words: diabetes mellitus; voiding dysfunction; incidence; women; Taiwan
1. Introduction
1.1 Background
The prevalence of diabetes mellitus has been increasing worldwide over the past few decades. In Taiwan, the prevalence of diabetes mellitus was 9.2 % in 1996 ( Chang et al, 2000). Besides, more than 99% of people with diabetes had type 2 diabetes, with a higher incidence in patients aged 20-59 years (Jiang et al, 2012).
People with diabetes mellitus are at an increased risk for developing macrovascular and microvascular complications (Gross et al, 2005 ; Barr et al, 2007).. In the present study, the widely recognized microvascular and macrovascular complications from diabetes mellitus predispose patients to develop lower urinary tract dysfunction, including bladder dysfunction or urethropathy (Yu et al, 2004; Yang et al, 2007;
Robinson et al, 2012). Studies showed that more than 50% of men and women with diabetes had bladder dysfunction (Goldman, 1999; Hill et al, 2008; Daneshgari et al, 2009). Diabetic bladder dysfunction or urethropathy can involve different degrees and combinations of voiding and storage symptoms. Voiding dysfunction (VD) is defined by ICS/IUGA as abnormally slow and/or incomplete micturition (Abrams et al, 2002).
Currently, the two categories of drugs, cholinergic agents and alpha blockers, are being used for the treatment of VD in women (Chang et al, 2008; Gaitonde S, 2018).
Although it is not life-threatening, diabetic VD substantially affects a patient's quality of life and may be associated with recurrent urinary tract infections and upper urinary tract damage.
1.2 Objectives
Data on lower urinary tract symptoms in women with diabetes mellitus have been widely reported (Brown et al, 1999; Hill et al, 2008; Dereli et al, 2016). However,
studies on VD in women with diabetes mellitus are limited. In a hospital-based questionnaire study conducted in UK, 56 (38%) had VD in women with diabetes mellitus (Fayyad et al. 2009). Changxiao et al. estimated that the prevalence rate of VD by urodynamic diagnosis was 55.9% in Chinese women with DM (Changxiao H et al, 2014). The two reasons of this high prevalence of VD in women with DM may be as follows: the hospital-based study may involve patients with more comorbidities, and the questionnaire survey tends to identify patients with mild VD. In addition, these studies may be associated with very mild VD, which does not require treatment. Little is known about the impact of type 2 diabetes on seeking treatment for significant VD in women in a community. The aim of this study was to analyze the incidence and risk of seeking treatment for significant VD in women with type 2 diabetes during a 13-year period in Taiwan using data from a nationwide population-based healthcare database.
2. Materials and methods
2.1 Data source
The Longitudinal Health Insurance Database (LHID) contains 1 million randomly sampled beneficiaries (Bøje et al, 2014). The source population consisted of nearly the entire population of Taiwan (23 million inhabitants), and the LHID was derived from the National Health Insurance Research database (NHIRD) between 1999 and 2013.
Clinical diagnoses of patients in the LHID were made by the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). This study involved a secondary analysis of health-related databases and was approved by the Ethics Review Board of National Taiwan University Hospital (201903099W).
2.2 Study design
A population-based retrospective cohort study was conducted using the LHID derived from the NHIRD in Taiwan from 1999 to 2013. This study was designed to evaluate the incidence and risk of significant VD in women with type 2 diabetes.
Significant VD was defined as a feeling of difficulty in emptying the bladder which required bethanechol or tamsulosin treatment of more than 3 months in one year. The occurrence of significant VD was monitored until the end of 2013. The cohort group was matched with healthy volunteers stratified by age, Charlson comorbidity index (CCI) score, and comorbidities using the propensity score method at a 1:1 ratio (Alam et al, 2019).
2.3 Study participants
Patients older than 20 years old diagnosed with diabetes mellitus (ICD-9-CM code 250) between 2001 and 2012 were classified as the DM cohort. We excluded patients diagnosed with diabetes mellitus before 2001, with type 1 diabetes (ICD-9-CM code 250.X1), and with bladder cancer (ICD-9-CM code 188). The date of type 2 diabetes diagnosis was defined as the index date. Patients taking bethanechol or tamsulosin for 3 months before the index date were excluded (Fig. 1). The matched cohort without diabetes mellitus was also selected from the LHID.
The DM and non-DM groups were matched by stratifying age, CCI score, and comorbidities, including cerebrovascular diseases (CVA) (ICD-9-CM code 430-438), Parkinson’s disease (PD) (ICD-9-CM code 332), spinal cord injury (SCI) (ICD-9-CM codes 952, 1, 806), and history of hysterectomy (the procedure codes of 65.5, 65.6, 68.3–5, 68.9). All patients included in the study were followed up between the index
date and either the occurrence of significant VD, death, withdrawal from the National Health Insurance Program, or the end of the study period in 2013.
2.4 Statistical analysis
Basic demographic characteristics, CCI score, and comorbidities were compared between the two cohorts using t-test for age and chi-squared test for CCI score and comorbidities. The incidence rate of VD (per 10,000 person-years) was calculated for both cohorts. The number of new users of bethanechol or tamsulosin were calculated and reported annually from 2001 to 2013. The risk of developing significant VD was estimated for patients with and without type 2 diabetes, as well as those with associated risk factors. Hazards ratios (HRs) and 95% confidence intervals (CIs) were calculated by applying the univariate and multivariate Cox regression models. The cumulative incidence of significant VD in DM and non-DM cohorts were plotted using the Kaplan-Meier method, and their differences were examined using the log-rank test.
Furthermore, the risk of developing significant VD was evaluated and stratified by age, CCI score, and comorbidities in each cohort. All data analyses were performed using SAS statistical software (Version 9.4, SAS Institute, Cary, NC, United States), and the two-sided significance level was set at p < 0.05.
3. Results
3.1 Participants and descriptive data
During the follow-up period, there were 37,573 women with type 2 diabetes, including 536 patients (1.42%) with significant VD, but 3448 patients with type 2 diabetes (9.1%), including 96 patients with significant VD, could not be matched. After propensity score matching, there were 34,125 patients for each DM and non-DM cohorts. Moreover, the incidence of significant VD in the DM and non-DM cohorts was
1.28% and 0.75%, respectively. The distributions of age, CCI score, and comorbidities were similar between the two cohorts (Table 1). The mean (± standard deviation; SD) ages of DM and non-DM cohorts were 57.8 (±13.7) and 57.9 (±13.6) years, respectively.
The comorbidities in the DM and non-DM cohorts were CVA (7.24% vs. 7.24%), PD (0.97% vs. 0.97%), SCI (0.02% vs. 0.02%), and history of hysterectomy (0.47% vs.
0.47%). The mean follow-up periods were 6.4 and 6.6 years for the DM and non-DM cohorts, respectively. The mean interval between the diagnosis of type 2 diabetes and significant VD occurrence was approximately 4.3 years.
3.2 Main results
Table 2 shows the multivariate Cox hazard analysis with adjustment for age, CCI score, and comorbidities. The incidence rates of significant VD were approximately 20.0 and 11.4 per 10,000 person-years for the DM and non-DM cohorts, respectively, with a 1.79-fold (95% CI= 1.54-2.09, P<0.001) increased risk of significant VD after adjusting for age, CCI score, and comorbidities. The multivariate analysis showed that patients aged 70 years or older had an 8.48-fold (95% CI = 5.41-13.30, P<0.001) increased risk of significant VD than those aged 20-40 years. The multivariate risk of significant VD also increased with increasing CCI score, and patients with CCI score of
≥4 had a 2.68-fold (95% CI=1.68-4.30, P<0.001) increased risk of significant VD than those with CCI score of 0. After adjusting for age and CCI score, the risk of significant VD was higher in patients with CVA (HR =1.33, 95% CI = 1.06-1.66, P<0.05) and PD (HR = 1.71, 95% CI = 1.11-2.65, P<0.05) as comorbidities (Table 2). The cumulative incidence of significant VD estimated using the Kaplan-Meier analysis was significantly higher in the DM cohort than in the non-DM cohort by the end of the 13-year follow-up (log-rank test, p < 0.0001; Fig 2). Our population-based cohort study
revealed that the cumulative incidence of significant VD was 0.94% and 2.01% at the 5th and 10th year after type 2 diabetes diagnosis.
3.3 The analysis of subgroups
To examine whether type 2 diabetes is an age-dependent risk factor for significant VD, we divided the patients into five groups by age. The DM cohort had significantly greater risk for the development of significant VD than the non-DM cohort in the subgroup with inverse association, whereas the 20-40-year subgroup had a 4.42-fold (95% CI= 1.49-13.15, P<0.01) increased risk of significant VD. We also divided the patients into five groups according to their CCI score. The DM cohort still had a significantly greater risks for the development of significant VD than the non-DM cohort in the subgroup with inverse association, whereas those with CCI score of 0 had a 2.52-fold (95% CI= 1.93-3.29, P<0.001) increased risk of significant VD (Table 3).
3.4 The analysis of new users of bethanechol, tamsulosin or combination therapy
Fig. 3 shows that the number of new users of bethanechol or tamsulosin calculated annually from 2001 to 2013. There were 356 and 180 new users of bethanechol and tamsulosin, respectively, between 2001 and 2013. The number of new users of bethanechol increased by 2.04 times during the13-year period, from 23 in 2005 to 47 in 2013. The number of new users of tamsulosin increased by 8.25 times during the 13-year period, from 4 in 2005 to 33 in 2013. A steady increase was found in the new users of bethanechol, but the rapid increase in the new users of tamsulosin flattened after 6 years. Especially, the combination therapy of bethanechol and tamsulosin has been used since 2007. The number of new users of the combined therapy increased by 3.0 times during the 7-year period, from 3 in 2009 to 9 in 2013 (Fig. 3).
4. Discussion
4.1 The interpretation of our database
The NHIRD is nationwide anonymous eligibility, enrollment information, and claims for visits, procedures, and prescription medications of 99% of the entire estimated 23 million population of Taiwan (Hsiao et al, 2007). Our study used the LHID that contained all outpatient and inpatient medical claims of 1 million beneficiaries randomly sampled from the NHIRD during the period of January 1, 1999 to December 31, 2013. We identify a cohort based on health services, diagnoses, surgical procedures, and drug utilization from this database. As a result, we believe that our data are reliable, and the patients’ characteristics are similar to those of the whole population.
4.2 Summarize main results
To the best of our knowledge, this is the first study to report the incidence of significant VD (1.42%) in women with type 2 diabetes over a 13-year period. Our study involving only women with type 2 diabetes decreases the confounding effect of concurrent benign prostate enlargement, which shares the same VD. However, information regarding the incidence of VD in women with DM is extremely limited. In hospital-based studies, only the prevalence of VD in women with DM reported in UK and China are 38 % and 55.9%, individually (Fayyad et al, 2009; Changxiao H et al, 2014).. In our community-based study, the incidence of significant VD in women with type 2 diabetes is 1.42%. Although the higher prevalence of VD in women with DM was reported in previous studies, our results showed the lower incidence of significant VD in women with type 2 diabetes. This difference may be present because our patients may only have visited the hospitals when their conditions were already serious. In this
study, we found that increased risks of significant VD in women were associated with age of more than 50 years, CCI score of more than 0, and comorbidities of CVA and PD, but comorbidities of SCI and history of hysterectomy were not associated with increased risk of significant VD. No event of significant VD in SCI patients may be a reflection of more serious VD with intermittent catheterization program or Foley catheter insertion. Only three events of significant VD were observed in patients with history of hysterectomy, which may reflect advances in surgical techniques and management options (Kietpeerakool et al, 2019) After adjusting the effects of age, CCI score, CVA, and PD, the risk of significant VD remained higher in the DM cohort than in the non-DM cohort. Our finding showed a 1.79-fold increased risk of significant VD in women with type 2 diabetes after adjusting for these confounding factors. The incidence rates of significant VD in women was 20.0 and 10.5 per 10,000 person-years in the DM and non-DM cohorts, respectively. Although after matching, the incidence of significant VD in women with type 2 diabetes was underestimated and decreased to 1.28%, the relationship between type 2 diabetes and significant VD in women is still established suggesting that it is highly probable that type 2 diabetes is an independent medical condition that causes significant VD in women.
Initial studies suggested that long standing diabetes mellitus causes paralysis of the detrusor muscle leading to VD (Hill et al, 2008). Our cohort study first indicated that the cumulative incidence of significant VD, which could be considered as long-term probability, was 0.93% and 2.01% at the 5th and 10th year, respectively, after the diagnosis of diabetes mellitus. These patients with type 2 diabetes in our cohort were newly diagnosed, and the mean interval between the diagnosis of type 2 diabetes and significant VD occurrence was 4.3 years. However, in a urodynamic study, time to
diabetic cystopathy with VD in women was reported in at least 8-9 years after the diagnosis of diabetes mellitus (Kebapci et al, 2007).. This difference may be due to detrusor underactivity, diabetic urethropathy, or poor health-habit counseling among women in Taiwan, as the time to occurrence of significant VD in women with type 2 diabetes is lower in our study than in the urodynamic study (Yang et al, 2007; Lee et al,2009).
4.3 The interpretation of results of subgroup analysis
Studies have shown that elderly women with CVA, PD, SCI, or history of hysterectomy complained of voiding difficulty, such as small caliber or urinary retention (Sveinbjornsdottir S, 2016 ; Quadri et al, 2018; Akkoç et al, 2019;
Kietpeerakool et al, 2019).In the earlier study, detrusor-impaired contractility with VD is common in elderly women older than 70 years old (Abarbanel et al, 2007). Our subgroup analyses showed that women with type 2 diabetes have an age-dependent increasing incidence rate of significant VD, but the risk of significant VD was higher in the patients aged 20-40 years, which may reflect the influence of childbirth, detrusor underactivity, or diabetic urethropathy (Yang et al, 2007; Lee et al,2009; Beaumont T, 2019).. In addition, a possible misclassification bias cannot be avoided because patients with type 1 diabetes cannot totally be excluded by ICD-9-CM codes 250.X1, especially patients aged 20-40 years. The small sample size of women with type 2 diabetes aged 20-40 years with significant VD is another bias with the effects of inflated false discovery rate. Therefore, it is more believable that the occurrence of significant VD in women with type 2 diabetes aged 41-50 years was 2.66-fold higher. The CCI-dependent increasing incidence rate of significant VD in women with type 2 diabetes was also found, but lower CCI score had a greater magnitude of the risk of significant VD and
the occurrence of significant VD in women with type 2 diabetes with a CCI score of 0 was 2.52-fold higher. This suggests that the urological and medical care of women with type 2 diabetes in Taiwan should be more aggressive. It is highly probable that type 2 diabetes is an independent medical condition that causes significant VD in women, which could impact the comprehensive care of urinary symptoms of patients with type 2 diabetes through effective diabetes mellitus therapy (Tai et al, 2016). However, because the severity of type 2 diabetes cannot be determined through our national databases, this hypothesis could not be validated. We recommend that additional prospective studies are conducted to verify the age- and CCI-related elevated risk of significant VD in women with type 2 diabetes. Owing to the effect of type 2 diabetes, the risk of significant VD in patients with CVA was 1.80-fold higher, which was similar to that in patients without CVA. On the contrary, the risk of significant VD in women with type 2 diabetes who have PD was not significantly different. In short, women with PD are highly associated with significant VD compared to those with CVA.
4.4 Summarize the trend of new users of
bethanechol, tamsulosin or combination therapyCurrent drugs, such as bethanechol or tamsulosin, have been used for the treatment of VD in women since 2000. Bethanechol, a cholinergic agent produces the effects of the parasympathetic nervous system stimulation. Bethanechol is usually prescribed in elderly women for detrusor atony, urinary retention, or incomplete bladder emptying (Gaitonde S, 2018). Tamsulosin, an alpha-1-adrenergic receptor (a1-AR) blocker is effectively used to improve voiding symptoms in those with benign prostatic hyperplasia (BPH) (Roehrborn et al, 2004).Tamsulosin is also used for the treatment of VD in women (Chang et al, 2008).. In Taiwan, bethanechol has been prescribed to treat
VD in women for a long time, and tamsulosin for treating VD in women has been the most commonly used alpha blocker. Other alpha blockers such as doxazosin or terazosin may be used for treating VD in women or hypertension. To eliminate the confounding effects, we only used the prescription of bethanechol or tamsulosin as the occurrence of significant VD. Owing to the occurrence of significant VD with seeking treatment, we believe that the incidence of significant VD among women with type 2 diabetes in our study is more reliable than those reported in a previous study by questionnaire or urodynamic studies (Fayyad et al, 2009; Changxiao H et al, 2014).
Given that doctors may use bethanechol to treat constipation (Poetter et al, 2013) or tamsulosin to shorten the passage time of smaller ureteral stones (Abdel-Meguid et al, 2010), we exclude patients receiving bethanechol or tamsulosin therapy within 3 months before the index date. In this study, we found that the number of new users of bethanechol and tamsulosin increased by 2.04 and 8.25 times, respectively, between 2005 and 2013. The number of new users of combination therapy of bethanechol and tamsulosin increased by 3.0 times between 2009 and 2013. We believe that many doctors know that tamsulosin can be used to treat women VD. We also find a gradually increasing trend of the use of combination therapy of bethanechol and tamsulosin since 2007.
4.5 Limitations
This study had limitations inherited from the NHIRD. First, ICD-9-CM codes were used to identify cohorts in the NHIRD. All insurance claims in the NHIRD were made by medical doctors according to the standard criteria, but this study may not have the same quality as that of a prospective well-designed study. Second, the NHIRD did not contain personal information regarding laboratory data, record of alcohol and cigarette
use, and exercise that may be confounding variables influencing voiding function.
Therefore, we used a propensity score to match age, CCI score, and comorbidities to minimize this potential influence. Third, the diagnoses of diabetes mellitus and comorbidities were completely dependent on the ICD-9-CM codes, especially diabetes mellitus. We adopted the diabetes mellitus diagnosis as at least two outpatient visits or one hospitalization that was already validated (Lin et al,2017 ). Fourth, type 1 diabetes was present in less than 1% of the diabetic population in Taiwan (Jiang et al, 2012). We excluded the patients diagnosed with type 1 diabetes (ICD-9-CM codes 250.X1), but a possible misclassification bias cannot totally be avoided. Fifth, we only analyzed tamsulosin use for significant VD in women with type 2 diabetes, rather than including all alpha blockers. Therefore, the incidence of significant VD in women with T2DM might be mildly underestimated.
5. Conclusion
To our knowledge, this is the first study to report that the incidence of significant VD in women with type 2 diabetes was 1.42% during a 13-year period. Type 2 diabetes is independently associated with an increased risk of significant VD in women, especially women type 2 diabetes aged 41-50 years or with a lower CCI score. Therefore, clinicians should be aware of and educate patients about the association between type 2 diabetes and significant VD in women. Further large-scale prospective clinical studies are needed before definite conclusions can be drawn.
6. Future perspectives
This is the first study to report that the incidence and risk of significant VD in women with type 2 diabetes in a community. The data will be used to educate patients about the
association between type 2 diabetes and significant VD in women despite some inherited limitations from our database. Because the due date of our database is March 2019, we cannot modify our data. To solve this problem, we plan to perform further large-scale retrospective studies from the National Health Insurance Research database of the entire population in Taiwan.
7. References
1. Abarbanel J, Marcus EL. Impaired detrusor contractility in community-dwelling elderly presenting with lower urinary tract symptoms. Urology. 2007 Mar;69(3):436-40. Abdel-Meguid TA, Tayib A, Al-Sayyad A. Tamsulosin to treat uncomplicated distal ureteral calculi: a double blind randomized placebo-controlled trial. Can J Urol. 2010 Jun;17(3):5178-83.
2. Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, van Kerrebroeck P, Victor A, Wein A; Standardisation Sub-committee of the International Continence Society. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society.
Neurourol Urodyn. 2002;21(2):167-78.
3. Akkoç Y, Bardak AN, Ersöz M, Yılmaz B, Yıldız N, Erhan B, Tunç H, Koklu K, Alemdaroğlu E, Dogan A, Ozisler Z, Koyuncu E, Şimşir Atalay N, Gündüz B, Işık R, Güler A, Sekizkardeş M, Demir Y, Yaşar E, Sasmaz E, Şatır Ö . Post-stroke lower urinary system dysfunction and its relation with functional and mental status: a multicenter cross-sectional study. Top Stroke Rehabil. 2019 Mar;26(2):136-141.
4. Alam S, Moodie EEM, Stephens DA. Should a propensity score model be super?
The utility of ensemble procedures for causal adjustment. Stat Med. 2019 Apr 30;38(9):1690-1702.
5. Barr EL, Zimmet PZ, Welborn TA, Jolley D, Magliano DJ, Dunstan DW, Cameron AJ, Dwyer T, Taylor HR, Tonkin AM, Wong TY, McNeil J, Shaw JE. Risk of cardiovascular and all-cause mortality in individuals with diabetes mellitus, impaired fasting glucose, and impaired glucose tolerance: the Australian Diabetes, Obesity, and Lifestyle Study (AusDiab). Circulation. 2007 Jul 10;116(2):151-7
6. Beaumont T. Prevalence and outcome of postpartum urinary retention at an Australian hospital. Midwifery. 2019 Mar;70:92-99.
7. Bøje CR, Dalton SO, Primdahl H, et al. Evaluation of comorbidity in 9388 head and neck cancer patients: a national cohort study from the DAHANCA database.
Radiother Oncol 2014;110:91–7.
8. Brown JS, Grady D, Ouslander JG, et al. Prevalence of urinary incontinence and associated risk factors in postmenopausal women. Heart & Estrogen/ Progestin Replacement Study (HERS) Research Group. Obstet Gynecol 1999; 94:66–70.
9. Chang C, Lu F, Yang YC, Wu JS, Wu TJ, Chen MS, Chuang LM, Tai TY.
Epidemiologic study of type 2 diabetes in Taiwan. Diabetes Res Clin Pract. 2000 Oct;50 Suppl 2:S49-59
10. Chang SJ, Chiang IN, Yu HJ. The effectiveness of tamsulosin in treating women with voiding difficulty. Int J Urol. 2008 Oct;15(11):981-5.
11. Changxiao H, Zhengyong Y, Shibing Y, Caiwen W, Yingchuan H, Wei H, Hanhui W, Dong L, Peng H, Jing L, Rui Z, Jia L, Hong S. Clinical and urodynamic evaluation of women referred with diabetes mellitus. Int Urogynecol J. 2014 Jul;25(7):979-83
12. Daneshgari, F., Liu, G., Birder, L., Hanna-Mitchell, A. T., & Chacko, S. (2009).
Diabetic bladder dysfunction: Current translational knowledge. The Journal of Urology, 182, S18–S26.
13. Dereli Yilmaz S, Demirgoz Bal M, Celik S, Rathfisch G, Kizilkaya Beji N,
Dinccag N, Yalcin O. Lower Urinary Tract Symptoms in Women With Type 2 Diabetes Mellitus. J Wound Ostomy Continence Nurs. 2016 Sep-Oct;43(5):523-8.
14. Fayyad AM, Hill SR, Jones G. Prevalence and risk factors for bothersome lower urinary tract symptoms in women with diabetes mellitus from hospital-based diabetes clinic. Int Urogynecol J Pelvic Floor Dysfunct. 2009 Nov;20(11):1339-44.
15. Gaitonde S, Malik RD, Christie AL, Zimmern PE. Bethanechol: Is it still being prescribed for bladder dysfunction in women? Int J Clin Pract. 2018 Aug 15:e13248.
16. Goldman HB, Appell RA. Voiding dysfunction in women with diabetes mellitus. Int Urogynecol J Pelvic Floor Dysfunct. 1999;10(2):130-3..
17. Gross JL, de Azevedo MJ, Silveiro SP, Canani LH, Caramori ML, Zelmanovitz T.
Diabetic nephropathy: diagnosis, prevention, and treatment. Diabetes Care. 2005 Jan;28(1):164-76.
18. Hill SR , Fayyad AM , Jones GR . Diabetes mellitus and female lower urinary tract symptoms: a review . Neurourol Urodyn . 2008 ; 27 : 362-367 .
19. Hsiao F, Yang C, Huang Y, et al. Using Taiwan’s national health insurance research databases for pharmacoepidemiology research. J Food Drug Anal. 2007;15(2):99.
20. Jiang YD, Chang CH, Tai TY, Chen JF, Chuang LM. Incidence and prevalence rates of diabetes mellitus in Taiwan: analysis of the 2000-2009 Nationwide Health Insurance database. J Formos Med Assoc. 2012 Nov;111(11):599-604.
21. Kebapci N, Yenilmez A, Efe B, Entok E, Demirustu C. Bladder dysfunction in type 2 diabetic patients. Neurourol Urodyn. 2007;26(6):814-9.
22. Kietpeerakool C, Aue-Aungkul A, Galaal K, Ngamjarus C, Lumbiganon P.
Nerve-sparing radical hysterectomy compared to standard radical hysterectomy for women with early stage cervical cancer (stage Ia2 to IIa). Cochrane Database Syst Rev. 2019 Feb 12;2:CD012828.
23. Lee WC, Wu HP, Tai TY, Yu HJ, Chiang PH. Investigation of urodynamic characteristics and bladder sensory function in the early stages of diabetic bladder dysfunction in women with type 2 diabetes. J Urol. 2009
Jan;181(1):198-203.
24. Lin YH, Hou CP, Chen TH, Juang HH, Chang PL, Yang PS, Lin YS, Chen CL, Tsui KH. Is diabetes mellitus associated with clinical outcomes in aging males treated with transurethral resection of prostate for bladder outlet obstruction:implications from Taiwan Nationwide Population-Based Cohort Study. Clin Interv Aging. 2017 Mar 16;12:535-541.
25. Poetter CE, Stewart JT. Treatment of clozapine-induced constipation with bethanechol. J Clin Psychopharmacol. 2013 Oct;33(5):713-4
26. Quadri SA, Farooqui M, Ikram A, Zafar A, Khan MA, Suriya SS, Claus CF, Fiani B, Rahman M, Ramachandran A, Armstrong IIT, Taqi MA, Mortazavi MM. Recent update on basic mechanisms of spinal cord injury. Neurosurg Rev. 2018 Jul 11. doi:
10.1007/s10143-018-1008-3.
27. Roehrborn CG, Schwinn DA. Alpha1-adrenergic receptors and their inhibitors in lower urinary tract symptoms and benign prostatic hyperplasia. J Urol. 2004 Mar;171(3):1029-35.
28. Robinson D, Staskin D, Laterza RM, Koelbl H. Defining female voiding dysfunction: ICI-RS 2011. Neurourol Urodyn. 2012 Mar;31(3):313-6.
29. Sveinbjornsdottir S. The clinical symptoms of Parkinson's disease. J Neurochem.
2016 Oct;139 Suppl 1:318-324.
30. Tai HC, Tai TY, Yang WS, Wang SW, Yu HJ. Associations between lower urinary tract dysfunction and glycemic control in women with type 2 diabetes: A
cross-sectional study. J Diabetes Complications. 2016 Apr;30(3):415-9.
31. Yang Z, Dolber PC, Fraser MO. Diabetic urethropathy compounds the effects of diabetic cystopathy. J Urol. 2007 Nov;178(5):2213-9.
32. Yu HJ, Lee WC, Liu SP, Tai TY, Wu HP, Chen J. Unrecognized voiding difficulty in female type 2 diabetic patients in the diabetes clinic: a prospective case-control study. Diabetes Care. 2004 Apr;27(4):988-9.
8. Figures and tables
Figure 1. Flowchart showing the study participant selection
Women with DM in 2000-2012 (n=52968) (N=1,000,000)
Newly diagnosed DM patients in 2001-2012 (n=37573)
Non-DM cohort in 2001-2012
Exclude:
Age<20 years old (n=341)
DM diagnosis before the year 2001 (n=13234) Type 1 DM (n=1606)
Bladder cancer (n=33)
Taking bethanechol or tamsulosin within 3 months before DM diagnosis (n=181)
Follow-up until the occurrence of significant voiding dysfunction, death, withdrawal, or the end of 2013 DM cohort
(n=34125)
Non-DM cohort (n=34125) 1:1 matching for age, CCI
score, and co-morbidities NHIRD in 2000-2013 (N=1,000,000)
Table 1. Characteristics between patients with and without DM
DM non-DM P-value
Female, no, (%) 34125 (100.00) 34125 (100.00)
age, year, no, (%) 0.99
20-40 3600 (10.55) 3600 (10.55)
41-50 6106 (17.89) 6106 (17.89)
51-60 10341 (30.30) 10341 (30.30)
61-70 7796 (22.85) 7796 (22.85)
≧71 6282 (18.41) 6282 (18.41)
CCI, no. (%) 0.99
0 18838 (55.20) 18838 (55.20)
1 10097 (29.59) 10097 (29.59)
2 3806 (11.15) 3806 (11.15)
3 1032 (3.02) 1032 (3.02)
≧4 352 (1.03) 352 (1.03)
comorbidity, no. (%)
CVA 1.00
No 31654 (92.76) 31654 (92.76)
Yes 2471 (7.24) 2471 (7.24)
PD 1.00
No 33794 (99.03) 33794 (99.03)
Yes 331 (0.97) 331 (0.97)
SCI 1.00
No 34119 (99.98) 34119 (99.98)
Yes 6 (0.02) 6 (0.02)
Hysterectomy 1.00
No 33966 (99.53) 33966 (99.53)
Yes 159 (0.47) 159 (0.47)
Abbreviations: DM, diabetes mellitus; CCI, Charlson comorbidity index; CVA, cerebrovascular diseases; PD, Parkinson’s disease; SCI, spinal cord injury
Table 2. Incidence rates and hazard ratios (HR) of significant VD for DM and potential risk factors in multivariate cox regression model analysis
variables Event Person-years Rate
HR (95% CI)
Univariate Multivariate
DM
No 258 226195 11.4 1.00 1.00
Yes 440 219063 20.0 1.76 (1.51, 2.06)*** 1.79 (1.54, 2.09)***
age, year
20-40 21 51401 4.0 1.00 1.00
41-50 54 87521 6.1 1.51 (0.91, 2.50) 1.44 (0.87, 2.38)
51-60 130 135764 9.5 2.38 (1.50, 3.77)*** 2.15 (1.35, 3.41)**
61-70 187 101752 18.3 4.56 (2.91, 7.16)*** 3.85 (2.45, 6.07)***
≧71 306 68819 44.4 11.23 (7.22, 17.49)*** 8.48 (5.41, 13.30)***
CCI
0 256 252464 10.1 1.00 1.00
1 258 131636 19.6 1.94 (1.63, 2.30)*** 1.49 (1.24, 1.78)***
2 125 46436 26.9 2.67 (2.15, 3.30)*** 1.55 (1.23, 1.95)***
3 38 11645 32.6 3.24 (2.30, 4.55)*** 1.52 (1.06, 2.17)*
≧4 21 3076 68.2 6.82 (4.37, 10.65)*** 2.68 (1.68, 4.30)***
comorbidity꒳
CVA
No 580 417150 13.9 1.00 1.00
Yes 118 28107 41.9 3.04 (2.50, 3.71)*** 1.33 (1.06, 1.66)*
PD
No 676 442117 15.2 1.00 1.00
Yes 22 3141 70.0 4.68 (3.06, 7.16)*** 1.71 (1.11, 2.65)*
SCI
No 698 445209 15.6 1.00 1.00
Yes 0 49 0 - -
Hysterectomy
No 695 442991 15.6 1.00 1.00
Yes 3 2267 13.2 0.83 (0.27, 2.59) -
CI: confidence interval.
Rate: incidence rate, per 10,000 person-years.
*p<0.05.
**p<0.01.
***p<0.001.
Table 3. Subgroup analysis for incidence and hazard ratio (HR) of significant VD between patients with and without DM, stratified by age and CCI
DM non-DM HR (95%CI)
Event Person-years Rate Event Person-years Rate Multivariate
age, year
20-40 17 25605 6.6 4 25795 1.5 4.42 (1.49, 13.15)**
41-50 39 43350 9.0 15 44170 3.4 2.66 (1.46, 4.82)**
51-60 90 66858 13.4 40 68905 5.8 2.34 (1.61, 3.39)***
61-70 119 50218 23.7 68 51533 13.2 1.78 (1.32, 2.40)***
≧71 175 33029 52.9 131 35790 36.6 1.45 (1.16, 1.82)**
CCI
0 180 124142 14.5 76 128321 5.9 2.52 (1.93, 3.29)***
1 155 64832 23.9 103 66803 15.4 1.57 (1.22, 2.01)***
2 69 22799 30.2 56 23636 23.6 1.28 (0.90, 1.83)
3 22 5767 38.1 16 5877 27.2 1.50 (0.78, 2.85)
≧4 14 1520 92.0 7 1555 44.9 2.28 (0.92, 5.65)
comorbidity
CVA
No 367 205592 17.8 213 211558 10.0 1.79 (1.52, 2.12)***
Yes 73 13470 54.1 45 14637 30.7 1.80 (1.24, 2.60)***
PD
No 428 217573 19.6 248 224543 11.0 1.82 (1.55, 2.12)***
Yes 12 1490 80.5 10 1651 60.5 1.28 (0.55, 2.96)
꒳: comorbidities of SCI and hysterectomy not listed due to small sample sizes about
both of significant VD events
Figure 2. Kaplan-Meier probability for DM and non-DM patients with significant VD
Follow-up (years)
Figure 3. The number of new users of bethanechol, tamsulosin, or combination therapy by year
0 10 20 30 40 50 60
bethanechol tamsulosin combination
Appendix
Lai MC, Kuo YC, Kuo HC. Intravesical hyaluronic acid for interstitial cystitis/painful bladder syndrome: a comparative randomized assessment of different regimens. Int J Urol. 2013 Feb;20(2):203-7.