i
國立臺灣大學生物資源暨農學院農業經濟學系 碩士論文
Department of Agriculture Economics College of Bio-Resources and Agriculture
National Taiwan University Master Thesis
運動強度與老人心理健康之探討 Exercise Intensity and Mental Health
of the Elderly in Taiwan
楊豐安 Feng-An Yang
指導教授:張宏浩 博士 Advisor: Hung-Hao Chang, Ph.D.
中華民國 99 年 7 月
July, 2010
i
謝辭
兩年的碩士生活很快地過去了,在這段期間很幸運地能接受張宏浩老師的指 導,使我成長很多。感謝老師,我真的學到很多東西,除了學術研究能力的培養 之外,在做人與做事的態度上,老師也給我很多啟發,讓我知道做人要有責任感,
做事要有責任心。
碩士班兩年的日子,有歡笑也有淚水,首先感謝同門的純嫣,妳是最好的夥 伴,有妳的幫忙事情總是能快速的解決,還有大師兄大川及學妹彥慈、婉婷,很 開心能與你們共事、互相幫忙。當然還有林儂、子凡、致豪及 R97 的好朋友們,
還記得一起熬夜唸書、出遊、聚餐及唱歌的日子,有太多的回憶,謝謝你們。也 要感謝系辦公室最親切的美華姊及系電腦室的秀姬姊,謝謝妳們這兩年來的幫忙 及照顧。
感謝我的家人一直以來對我的付出與支持,雖然碩士班的日子相當忙碌,但 一回到家總是能感受到家庭的溫暖。謝謝老爸、老媽對我的栽培,謝謝老弟的支 持,也謝謝伴我長大的親人們,謝謝你們的鼓勵。
最後要特別謝謝宥苡這六年來的陪伴,謝謝妳陪我渡過大學與碩士生涯的時 光,不管我遇到任何的困難,妳都會仔細聽我訴說及伴我左右。也謝謝妳在我撰 寫論文時,給我最大的包容與體諒,謝謝妳。
楊豐安 謹誌於 國立臺灣大學農業經濟學研究所 中華民國九十九年七月
ii
摘要
過去幾十年來,長期低出生率及死亡率使得台灣人口結構快速老化,此一現 象也帶來許多社會及公共衛生問題,其中老年憂鬱症已備受關注,它除了會降低 生活品質之外,還會造成老人自殺的問題。在影響老年憂鬱的因素當中,運動已 被提及為有效促進老人心理健康的方法,甚而運動強度也被認為是影響老人心理 健康的關鍵因素,但是過去研究運動強度的文獻多以小樣本實驗或橫斷面資料來 分析,對老人最適運動強度的決定也尚未有明確定論。因此本研究探討台灣老人 運動強度與心理健康的關係來做為老人運動處方的參考。
本研究的資料來源為 1996、1999 及 2003 年的中老年身心社會生活狀況長期 追蹤調查,並以運動後喘氣的程度做為衡量運動強度的指標。不同於以往文獻,
本文先建立三期均衡式追蹤資料,並利用固定效果模型來進行實證分析,藉此方 法可以控制潛在無法觀察到的異質性(unobserved heterogeneity)對老人心理健康 之影響。實證結果顯示,運動對老人心理健康有顯著的助益,其中低強度運動較 中強度運動為優;平常規律做低強度運動的老人得到憂鬱症的機率較沒運動的老 人低 12%,然而中強度運動卻對老年憂鬱症沒有顯著的影響。研究結果亦有其政 策意涵:儘管低強度與中強度運動皆可以改善老人心理健康,本研究建議未來推 廣老人運動與心理健康時,需特別注意運動強度,對台灣老人而言,低強度運動 為最適運動強度。
關鍵字:心理健康、憂鬱、運動強度、老人、追蹤資料
iii
Abstract
Due to the high prevalence of depression among the elderly in Taiwan, the objective of this study is to investigate the relationship between exercise intensity and mental health. Although it has been documented that regular exercise is a significant factor associated with older people’s psychological well-being, the optimal pattern of exercise intensity is at best inconclusive.
In contrast to previous studies, this study utilizes a longitudinal survey of the elderly in Taiwan. The nonlinear panel data models are estimated using the fixed-effect method to control for potential unobserved heterogeneity and accommodate the censored and binary outcome variables.
Using personal perceived breathing level as the measurement of exercise intensity, the estimation results revealed that regular exercise contribute to better mental health, but low intensity was much better than moderate intensity. The results also suggested that moderate intensity exercise is not significant of depression, while low intensity exercise had led to twelve percent lower in probability of depression.
Some policy implications can be inferred from our findings. Although the results support that both light and moderate exercise are aggressive tools for improving mental health of the elderly, however, light intensity exercise can be seen as an optimal pattern of exercise for the Taiwanese elderly.
Key words: mental health, depression, exercise intensity, elderly, panel data
iv
Contents
謝辭... i
摘要... ii
Abstract ... iii
Chapter 1 Introduction ... 1
1.1 Motivation ... 1
1.2 Objective ... 3
1.3 Organization ... 4
Chapter 2 Literature Review... 5
2.1 Depression in late life ... 5
2.2 An overview of exercise and mental health among elderly ... 7
2.3 Intensity of exercise ... 9
2.4 Summary ... 13
Chapter 3 Data ... 15
3.1 Source ... 15
3.2 Measures of dependent variables ... 16
3.3 Measures of independent variables ... 18
3.3 Sample Description ... 21
Chapter 4 Methodology ... 26
4.1 Econometric specifications ... 26
4.2 Fixed-effect Tobit model ... 28
4.3 Fixed-effect probit model ... 30
Chapter 5 Results ... 32
5.1 The determinants on mental health... 32
5.2 The determinants on depression ... 35
Chapter 6 Conclusion ... 37
Reference ... 40
v
List of Tables
Table 1 Summary table of studies examining the relationship between exercise
intensity and depression ... 14
Table 2 Mean score of mental illness by exercise type ... 22
Table 3 Distribution of depression by exercise type ... 23
Table 4 Sample statistics ... 25
Table 5 Estimation of continuous CESD score... 34
Table 6 Estimation of the depression equation ... 35
List of Figures Figure 1 The annual proportion of Taiwanese elderly aged 65 or over ... 2
Figure 2 The relationship between exercise intensity and affective benefits ... 11
1
Chapter 1 Introduction
1.1 Motivation
In the past few decades, one of the most significant demographic changes in
Taiwan is the increase in the proportion of the old population. Similar to other
developed and developing countries, Taiwan has experienced a decline in fertility and
mortality rates, which result in a faster process of demographic transition and higher
proportion of older population. To understand the increase in old population in recent
decades, we present the annual proportion of Taiwanese elderly aged 65 or over based
on a statistical report by Directorate-General of Budget, Accounting and Statistics in
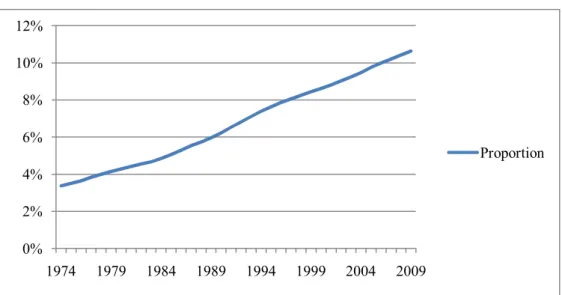
Taiwan (Figure 1). It shows that the proportion of the elderly has increasingly risen and
tripled from 3.4% in 1974 to 10.6% in 2009. Due to the considerable proportion of the
old population, Taiwan is now facing an immense challenge on both social and health
care service.
2
Figure 1 The annual proportion of Taiwanese elderly aged 65 or over
The health care for the elderly has become an important issue in public health
policies, because elderly are more vulnerable to functional transitions than their younger
cohort, which result in a higher hospital use and medical cost (Mor et al. 1994). In
addition to functional disability, mental disorders such as depression among old age
population have also gained increasing prominence. It has been widely recognized that
depression is one of the most common mental disorders among the elderly.
Epidemiological studies have also shown a high rate of prevalence in older adults
among many countries. For example, the estimated prevalence of depression was 33.5%
for Japanese community-dwelling elderly (Wada et al. 2004). Another study raised the
same alarm in Taiwan, Chong et al. (2001) studied 1,500 elderly aged 65 or over in
three communities and found the prevalence of mental illness was 37.7%. This causes
growing concern because depression can substantially reduce quality of life
0%
2%
4%
6%
8%
10%
12%
1974 1979 1984 1989 1994 1999 2004 2009
Proportion
3
(Doraiswamy et al. 2002) and cause serious suicide problem (Conwell, Duberstein and
Caine 2002; Wærn et al. 2002). Furthermore, previous researches have documented that
individuals with depression have higher medical care utilization and cost, which yield a
heavy social and economic burden to society (Chan et al. 2006; Sobocki et al. 2007).
An increasing number of studies have identified the potential determinants of
mental health. Among all of the other factors, regular exercise has been shown to have
positive influence on individual's mental well-being. However, the optimal patterns (e.g.
intensity, frequency and duration) of exercise for elderly are still at best inconclusive.
Furthermore, it is crucial to distinguish the intensity of exercise for older adults. Unlike
the general population, elderly health is sensitive to the exercise intensity because too
much exercise will cause adverse health impacts and lower degree of exercise makes
little effect on their health. Since little evidence has been provided regarding the
relationship between exercise intensity and mental health of the elderly, this paper aims
to fulfill the knowledge gap by investigating the optimal intensity of exercise for elderly
health.
1.2 Objective
4
The objective of this study is to examine association between the intensity of
exercise and mental health among the elderly in Taiwan. In addition to exercise, we also
control for family, socioeconomic, health status, lifestyle and social support
characteristics. Several special features may set our study apart from previous studies.
First, in contrast to the small-scale random survey among specific groups, a large-scale
national representative sample of elderly in Taiwan was used. Second, a panel data is
constructed and used for controlling for the individual fixed effect to explore the
relationship between exercise and mental health of the elderly. Additionally, unlike the
epidemic or public studies which usually relied on the qualitative or descriptive analysis,
this study aims to quantify the associations between exercise and mental health.
1.3 Organization
This paper is structured as follows: in Chapter 2 we introduce old age depression
and review previous literatures that have examined the impact of exercise on mental
health. Details of data, definitions of the variables and corresponding sample statistics
are provided in Chapter 3. In Chapter 4 we outline the statistical approach and
econometric models. Chapter 5 presents our estimation results that compare
performance of exercise intensity with related determinants, and finally conclusions are
drawn in Chapter 6.
5
Chapter 2 Literature Review
In this chapter, we first review the main theme of depression in late life and then
review the literatures that have attempted to examine the association between exercise
and mental health. The intensity of exercise is expatiated in section 2.3. As indicated,
considerable evidence had been shown exercise can improve individual mental health
and reduce depressive symptoms.
2.1 Depression in late life
Depression is a variety of psychiatric symptom that reflects individual mental
health conditions such as sadness, loneliness and negative self-concept (see Beck and
Alford 2009). In late life, the prevalence of clinical relevant depressive symptoms has
been reported to a wide range from 7.2% to 49% across countries (Djernes 2006). For
example, epidemiological studies on elderly aged 65 or above have reported different
prevalence rates. Prince et al. (1997) conducted a survey of all residents of an electoral
district in London and found that 17% elderly reported pervasive depression. On the
other hand, a higher prevalence of depression can be found in Wada et al. (2004) who
estimated the prevalence of depression was 33.5% for Japanese community-dwelling
6
elderly.
Depression can lead to both physiological and psychological disorders. For
example, Jaffe, Froom and Galambos (1994) compared depressed and non-depressed
elderly patients and found that patients of depressive symptoms had more functional
impairment. The reduction in quality of life can also be attributed to depression.
Doraiswamy et al. (2002) examined 100 elderly with depression and found that
depressed elderly showed a significant reduction in quality of life. In addition, previous
researches have documented that the economic costs of depression had become a heavy
social burden to society. Chan et al. (2006) found that the economic burden of
Taiwanese adult depression rose from US$ 93 million in 2000 to US $140 million in
2002. In Sweden, the cost of depression has doubled from 1997 (€ 1.7 billion) to 2005
(€ 3.5 billion) due to sick live and early retirement (Sobocki et al. 2007).
With the increasing prevalence of depression among old population, researchers
have examined the association between potential determinants and depression. For
example, researchers have consistently indicated that volunteer work is beneficial to
mental health for elderly (Musick and Wilson 2003). Socioeconomic status (SES) is also
important for depression, especially among lower SES elderly. Using cross-sectional
data from Dutch elderly, Koster et al. (2006) found lower SES is a strong predictor of
depression. In addition, regular exercise has been shown to improve individual mental
7
well-being. We will review the related literatures shortly.
2.2 An overview of exercise and mental health among elderly
Over the recent decades, the association between exercise and mental health has
caught increasingly attention. It is of great concern whether exercise is beneficial to
individual psychological well-being. Researchers addressing this issue have
continuously conducted experimental controlled trials as well as observational analysis
that attempted to test its validity (e.g. Mather et al. 2002; Ruuskanen and Ruoppila 1995;
Kritz-Silverstein, Barrett-Connor, and Corbeau 2001).
Most of researchers have consistently agreed the advantage of exercise in terms of
mental health and depression. For example, Mather et al. (2002) used a randomized
controlled trial to study the effects of exercise on older adults. They randomized the 86
patients aged 53 and over to attend either exercise classes or health classes for 10 weeks,
and found that participants in exercise group have a significant reduction in depression
than those in health classes group. Similar evidence can be found in observational
studies. Using a community-based sample in southern California, Kritz-Silverstein,
Barrett-Connor and Corbeau (2001) examined cross-sectional and prospective
8
association between exercise and depression mood of older people. They found that
exercise was significantly negative associated with depression.
In particular, to prevent the elderly from mental illness, researchers have further
compared the efficiency between exercise and standard anti-depression medication
(Babyak et al. 2000; Blumenthal et al. 2007). Babyak et al. (2000) studied how regular
exercise affects the 156 elder patients aged 50 and over with major depression. They
distributed the patients into three groups: exercise group, medication group and
combined therapies group. After 16 weeks of exercise treatments, participants in
exercise group exhibit a significant reduction in depression as those with medication
only and those with combined therapies. The remission rates of depression were 60%,
66% and 69% respectively. The authors also recommended regular exercise as an
alternative treatment instead of antidepressant. On the contrary, some studies showed
opposite results. For instance, Emery and Gatz (1990) showed little change in
psychological well-being for older adults after a 12-week aerobic exercise program.
Researchers are also interested in the mechanisms of antidepressant effect of
exercise. This important issue is also open to more debate. Several hypotheses have
been proposed to explain the anti-depression effect (see Craft and Perna 2004). For example, the endorphin hypothesis assumes that β-endorphins are increasingly released
after exercise which yields an overall enhancement of well-being.
9
Although the mechanisms of antidepressant effect are not transparent, the
relationship between exercise and mental health has been well established, and
researchers have generally drawn a similar conclusion that exercise can lead to better
mental health.
2.3 Intensity of exercise
With growing evidence that exercise is positive associated with mental health, it is
now important to focus further on the relationship between exercise and mental health.
For example, factors such as intensity, frequency and duration play significant roles in
determining individual mental health (see Teychenne, Ball, and Salmon 2008). Among
the factors, the intensity of exercise has come under spotlight in recent years. In addition
to the benefits of exercise, exercise can also result an insignificant change or even
impaired mental health. Therefore, it is important to study the relationship between
exercise intensity and mental health.
There are several ways to measure exercise intensity. For randomized controlled
experiments, the common measurements include heart rates, percentage of maximum
oxygen consumption (Hiilloskorpi et al. 2003) and energy expenditure (Dunn et al.
10
2005). However, supervised exercise training and such intensity measurements are
generally not feasible in observational studies. An alternatively method is to use
metabolic equivalent (MET) values to measure exercise intensity (Ainsworth et al.
2000). The MET values are defined by the levels of breathing efforts across a variety of
physical activity. For example, the MET value is assigned to 2.5 or 3.3 if respondents do
slow walking with “no change in breathing pattern” or “breath somewhat harder than
normal”. To identify the optimal level of intensity, researchers have stimulated a number
of papers to examine how exercise intensity affects mood states.
Since the 1990s, the shape of relationship between exercise intensity and affective
benefits has been found as approximated an inverted-U as displayed in figure 2
(Acevedo and Ekkekakis 2006; Ekkekakis, Hall and Petruzzello 2005). The traditional
inverted-U hypothesis has sketched the idea that moderate exercise is the optimal
intensity level for overall affective benefits; low intensity exercise may insufficiently
cause significant affective changes while high intensity exercise may cause insignificant
or aversive changes (Kirkcaldy and Shephard 1990; Ojanen 1994). Some researchers
have found similar results in normal population. One of the first studies was Moses et al.
(1989), who compared how different intensities of aerobic training affected mood and
mental well-being. After the training program, they found mood improvements were
significantly associated with the moderate exercise rather than high intensity. Similar
11
evidence can be found in Dunn et al. (2005). The authors showed that the degree of
reduction in depression was varied with different exercise intensities; the moderated
exercise was more effective than light exercise.
Figure 2 The relationship between exercise intensity and affective benefits
Despite the popularity of the hypotheses, considerable different findings are
revealed in extent literatures. For example, Wise et al. (2006) found that vigorous
intensity exercise was more strongly association with reduction in depression than light
intensity exercise. Moreover, Landuyt et al. (2000) examined short-term moderate
exercise effects among 82 university students and found that some participants reported
improvement in mood state but some reported a decline.
While the link between exercise intensity and mental health has been examined for
general population, there are only few papers focusing on older population (Lampinen,
12
Heikkinen, and Ruoppila 2000). Furthermore, these studies have report inconsistent
results. Some reports have argued that both moderated and high intensity exercise could
improve individual mental health. For example, using a randomized controlled trial for
357 elderly aged 50-65, King, Taylor and Haskell (1993) found that both moderate and
high intensity exercise reduced depression. The same conclusion can be found in
Ruuskanen and Ruoppila (1995) who studied the association between physical activity
and psychological well-being among the 1844 elderly in Finland. Based on a
cross-sectional study, they found that both moderated and intense exercise could reduce
depressive symptoms. On the other hand, Singh et al. (2005) studied the clinically
depressed elder patients and showed that high intensity progressive resistance training
(PRT) was more effective for depressive symptoms and quality of life than low intensity
PRT. Conversely, Lindwall et al. (2007) studied 860 Swedish suburb-dwelling elderly
and found that reduction in depression was associated with light exercise for women
only and strenuous exercise for men only.
There was another study which used longitudinal data to examine the long-term
relationship between changes in intensity of exercise and depressive symptoms
(Lampinen, Heikkinen, and Ruoppila 2000). Participants aged 65 or above were first
interviewed in 1988 and resurveyed 8 years later. The authors compared current and
past intensity of exercise and categorized changes in intensity of exercise as a predictor
13
of depressive symptoms. In general, participants who reduced their exercise intensity
had more depressive symptoms than their counterparts.
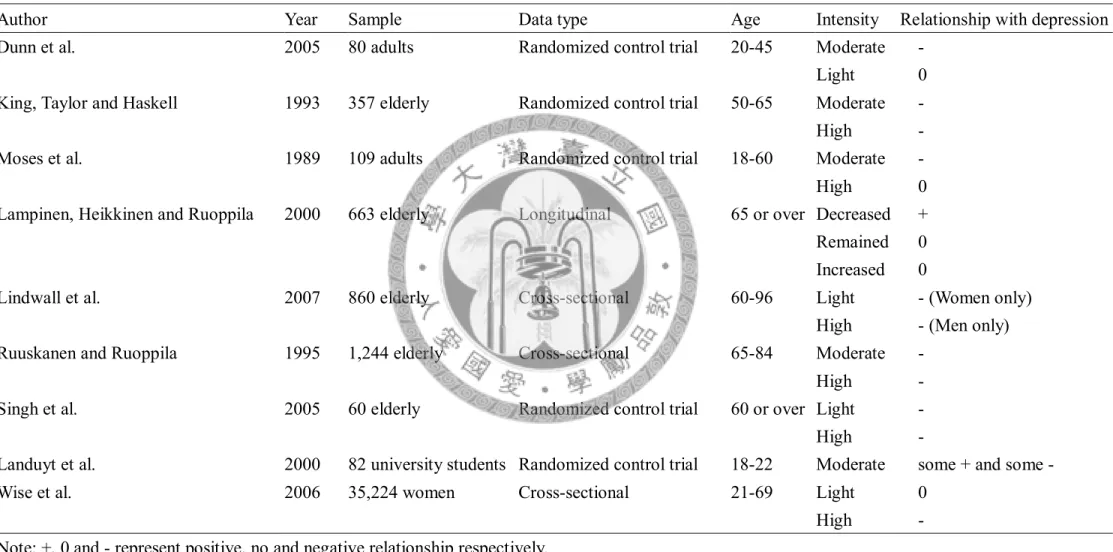
In summary, we provide studies examining the relationship between exercise
intensity and depression in Table 1.
2.4 Summary
Although evidence is growing on the effectiveness of exercise on depression, there
are several limitations in existing literatures as we reviewed in previous sections. First,
small selected random sample was commonly used in intervention studies. Second,
findings based on cross-sectional studies are not suitable to explore the causal
inferences between exercise and mental health. Third, diverse definition or classification
of exercise intensity may provide different implications for policy recommendation.
Fourth, results from young adults cannot be directly applied without any modification to
the older population. At these points, little is known about how different intensity of
exercise affects the elderly mental health.
14
Table 1 Summary table of studies examining the relationship between exercise intensity and depression
Author Year Sample Data type Age Intensity Relationship with depression
Dunn et al. 2005 80 adults Randomized control trial 20-45 Moderate -
Light 0
King, Taylor and Haskell 1993 357 elderly Randomized control trial 50-65 Moderate -
High -
Moses et al. 1989 109 adults Randomized control trial 18-60 Moderate -
High 0
Lampinen, Heikkinen and Ruoppila 2000 663 elderly Longitudinal 65 or over Decreased + Remained 0 Increased 0
Lindwall et al. 2007 860 elderly Cross-sectional 60-96 Light - (Women only)
High - (Men only)
Ruuskanen and Ruoppila 1995 1,244 elderly Cross-sectional 65-84 Moderate -
High -
Singh et al. 2005 60 elderly Randomized control trial 60 or over Light -
High -
Landuyt et al. 2000 82 university students Randomized control trial 18-22 Moderate some + and some -
Wise et al. 2006 35,224 women Cross-sectional 21-69 Light 0
High -
Note: +, 0 and - represent positive, no and negative relationship respectively.
15
Chapter 3 Data
3.1 Source
To examine the impact of exercise intensity on mental health for Taiwanese elderly,
we use data from Survey of Health and Living Status of the Elderly (SHLSE). The
SHLSE is a longitudinal survey conducted by the Department of Health in Taiwan. The
main objective is to explore the role of elderly in the context of family structure,
economic status, health status, social support and related issues for rapidly aging
population. Therefore, detailed information on socio-demographic characteristics, health
status, employment and other topics are collected.
The baseline survey began in 1989 covered 4,412 elderly aged 60 or over drawn
from 56 communities. A total of 4,049 elderly were successfully interviewed and
achieved a response rate of 92%. Since then, the respondents were traced and
resurveyed in 1993, 1996, 1999 and 2003. However, over one quarter of respondents
had passed away in 1996 and only 2,669 elderly were re-interviewed. In order to
maintain a representative sample of Taiwanese elderly, a younger cohort aged 50-66 was
included in 1996. The survey also added a new sample of elderly aged 50-56 in 2003.
With the appropriate sampling design, the sample is nationally representative for the
middle and elderly population in Taiwan. Further details of the SHLSE can be found in
16
the survey documentations (see Taiwan Department of Health 2008).
Although the survey offers rich information for Taiwanese elderly, the survey
design differs slightly across years. For example, there were 10 items in the
questionnaire for measuring individual mental health in 1996, 1999 and 2003, while
another 17 items and 5 items were included in the questionnaire in 1989 and 1993
respectively; information about exercise behavior was not included in 1989 and 1993,
while it was included in 1996, 1999 and 2003. In order to maintain the consistency of
the data, we only used the last three waves of the survey without the newly added
sample in 2003 in our empirical analysis.
After deleting observations with missing values on key variables in each survey
period, there are 3,564, 3,430 and 3,312 observations in 1996, 1999 and 2003
respectively. Individuals who were not surveyed in entire three periods are also
excluded. The final balanced panel data comprises 1,825 elderly individuals in each
year.
3.2 Measures of dependent variables
The dependent variable in this study is the mental illness of the elderly. Consistent
with the empirical specifications in the previous studies and to show the robustness of
17
our findings, three differential types of the dependent variables are specified. The first
dependent variable, a continuous measure of mental illness, is measured using a 10-item
short version of the Center for Epidemiologic Studies Depression Scale (CES-D), which
is one of the most valuable tools for helping identify an individual at-risk for depression
(Beekman et al. 1997). The measurement has been used to examine elderly mental
illness (e.g., O’Hara, Kohout, and Wallace 1985) and found adequate validity in Chinese
elderly population (Boey 1999). In SHLSE, 10 questions about mood swings were
included to reflect individual’s mental health condition. Each respondent was asked to
rate each question with a 0-3 scale point whether they had experienced a variety of
symptoms during the past week (e.g. “feel sad,” “feel lonely,” “feel happy”). We then
reversed codes of the positive items, and summed them up with the other 8 items as the
CES-D score. As result, the total points of CES-D scores range from 0 to 30, with
higher scores indicating worse mental health.
Although the CES-D score is widely used for many of the studies, it is commonly
seen that a certain proportions of respondents report zero scores of all of the questions,.
That is, they report no related depressive symptoms for all of the requested questions. In
this case, treating these groups of respondents the same as others may be not appropriate.
Econometrically, this problem is consistent with the censoring problems of the observed
data. To accommodate this issue, we define a censored CES-D score by treating those
18
who have zero scores of the overall CES-D score differently. In what follow, a tobit
model is used to estimate this type of the dependent variable.1
The third dependent variable is a binary variable measuring whether the individual
has depression or depressive symptoms. Because the survey didn’t include depression in
individual’s history of disease, we introduce a suggested cut-off point at CES-D ≥ 10 to
identify the elderly with clinically relevant levels of depression. This optimal cut-off
point was first established and analyzed by Andresen et al. (1994), and has been widely
used by many studies in examining elderly depression (e.g., Schulz et al. 2000).
3.3 Measures of independent variables
Exercise intensity measurement
All respondents were firstly divided into non-exercisers (no exercise) and
regular-exercisers (exercise at least once per week). Because further information of
exercise intensity was also obtained for regular-exercisers including duration, sweat rate
and breathing effort. Among the indicators, breathing effort has been used to measure
the intensity of exercise in another context (Wai et al. 2008).2 Because detailed
1 In Seplaki et al.(2006), they argued that a special treatment has to be made to disentangle those who report zero overall CES-D scores and those who don't. We follow their approach to make a distinction between those two types of respondents.
2 See Wai et al. (2008) for detailed information of using MET to measure exercise intensity.
19
information on types of exercise (e.g. walking, jogging and swimming) was not
collected in the survey, to calculate the metabolic equivalent (MET) values as used for
clinical or medical studies is not available. Instead, we used personal perceived
breathing level as an approximate indicator of exercise intensity. Three possible answers
of breathing effort were “no change in breathing”, “slight increase in breathing” and
“significant increase in breathing”. Considering elderly are prone to change in breathing
pattern after exercise and less likely to have vigorous exercise due to functional
transition, we classified those who report “no change in breathing” as having light
exercise, and the remaining respondents were classified as doing moderate exercise
among those report regular exercise at least once per week.3 To sum, three differential
types of exercise intensity are specified: for those who don't exercise at least once per
week, those who usually work out with light intensity; and those who usually work out
with moderate or even stronger intensities.
Other Independent Variables
In addition to exercise intensity, we also controlled for other potential determinants
that are related to mental health. Drawing on previous studies on mental health among
elderly, the potential determinants included family characteristics, socioeconomic
characteristics, health status, lifestyle and social support (see Djernes (2006) for a
3 There are less than 2% respondents reporting breathing much harder than normal.
20
review).
Family characteristics include marital status and whether an individual lived alone.
The socioeconomic variables include employment and family income (combined with
income of the respondent and his or hers spouse if present). In SHLSE, two questions
were asked related to family income. The first question asks each respondent to report
their family income per month if they can accurately indicate the absolute value, while
the second question asks each individual to check the approximate categories of their
family income if they don't have precise answer of their family income. In what follow,
the family income variable was created for those who reported the absolute values and
used the midpoint for each of income category for those who only check their income
status.
Similar to the definition of Seplaki et al. (2006), health status is assessed by an
index of mobility impairments. Respondents were asked to use a 0-to-3 scale to rate the
hardship for each activity. Selected activities included standing continuously for 15
minutes, squatting, raising hands overhead, grasping or turning objects with fingers,
lifting a 12kg object, running a short distance (20-30m) and climbing 2-3 flight of stairs.
The resulting mobility impairment scale ranges from 0 to 21 with higher scores
indicating more mobility limitation.
Two lifestyle indicators, drinking and smoking, of each individual are also
21
specified. Both drinker and smoker are coded as a binary variable reflecting
respondent’s self-reported current smoking or drinking behaviors. Since empirical
evidence has shown that social networking is also crucial to determine the mental health
of the elderly (Blazer 1983; Musick and Wilson 2003), we define two variables related
to social activities or social support. The first variable indicates the social score, which
is defined based on the number of community each respondent participates (e.g.
political party and religious community). The second variable reflects the volunteer
works which each individual involved. A binary variable of volunteer work is defined to
indicate whether the respondent offers to perform a social service voluntarily.
3.3 Sample Description
To highlight the differences in mental health by different intensities of exercise
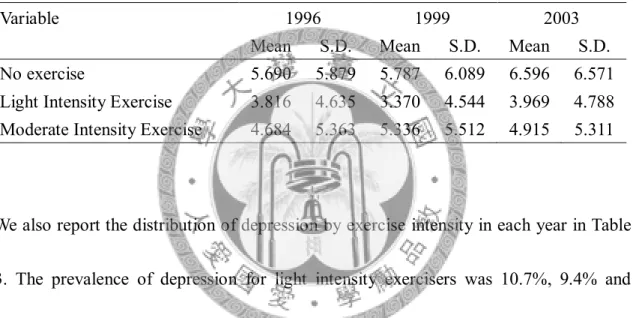
degree, we report the mean CES-D scores by exercise intensity in each year in Table 2.
As exhibited, among three exercise groups, non-exercisers have the highest CES-D
scores in each year. Moreover, their mental health has worsened during the 3 survey
periods. The average CES-D score was 5.69 in 1996 and 5.79 in 1999 and increased to
6.60 in 2003. On the other hand, regular-exercisers had a better mental health condition.
Moreover, substantial differences in CES-D scores are evident among different types of
22
exercise intensities: light intensity exercisers had lower CES-D scores by 1-2 points
than moderate exercisers. The CES-D scores were 3.82 (4.68), 3.37 (5.34) and 3.97
(4.92) in 1996, 1999 and 2003 respectively for light intensity exercisers (moderate
exercisers).
Table 2 Mean score of mental illness by exercise type
Variable 1996 1999 2003
Mean S.D. Mean S.D. Mean S.D.
No exercise 5.690 5.879 5.787 6.089 6.596 6.571
Light Intensity Exercise 3.816 4.635 3.370 4.544 3.969 4.788 Moderate Intensity Exercise 4.684 5.363 5.336 5.512 4.915 5.311
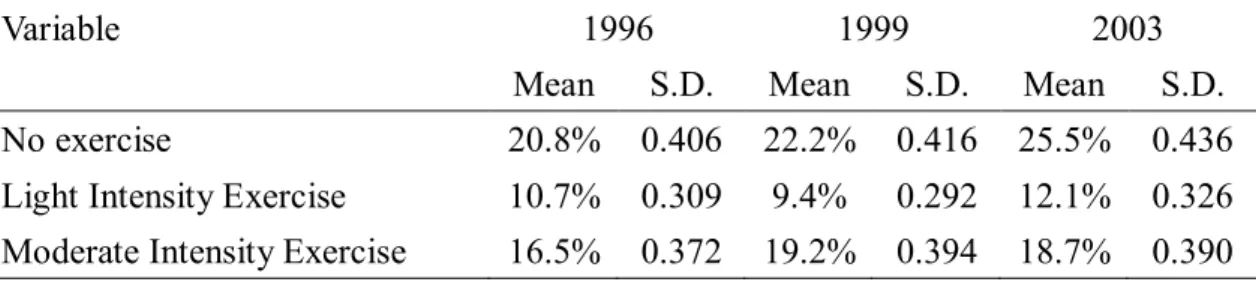
We also report the distribution of depression by exercise intensity in each year in Table
3. The prevalence of depression for light intensity exercisers was 10.7%, 9.4% and
12.1% in each year. Moderate intensity exercisers have a higher proportion of
depression, 16.5%, 19.2% and 18.7% of the elderly have depression in 1996, 1999 and
2003 respectively. Non-exercisers have the highest proportion of depression; the
corresponding proportions are 20.8%, 22.2% and 25.5%.
23
Table 3 Distribution of depression by exercise type
Variable 1996 1999 2003
Mean S.D. Mean S.D. Mean S.D.
No exercise 20.8% 0.406 22.2% 0.416 25.5% 0.436
Light Intensity Exercise 10.7% 0.309 9.4% 0.292 12.1% 0.326 Moderate Intensity Exercise 16.5% 0.372 19.2% 0.394 18.7% 0.390
Detailed definitions and sample statistics of each variable are presented in Table 4.
In our sample, the mean age of the elderly was about 64 in 1996. The mean CES-D
scores of the elderly were 4.86, 4.74 and 5.09 in 1996, 1999 and 2003 respectively; the
corresponding prevalence of depression were 17%, 16% 18%. The popularity of
exercise has increased, in 1996 only 54% elderly did exercise regularly, while in 2003,
almost 70% elderly did exercise regularly. Comparing the percentage of exercise for
various intensities, we find that both light and moderate exercise has increased 6% from
1996 to 2003, and the moderate exercise rate is roughly 10-15% which is lower than the
proportion of the light exercise.
About 77% of the elderly were married in 1996 and 8% reported that they were
living alone. In 2003, the percentage of married elderly has decreased to 68%, and 11%
report they were living alone. Employment rate in our sample has declined
tremendously during the survey periods. While nearly 40% of the elderly were currently
employed in 1996, only 18% reported being employed in 2003. The average family
24
income per month was about NT$ 30,000, 35,000 and 26,000 in 1996, 1999 and 2003
respectively.
The mobility limitations were low for elderly across year. The mean scores of
mobility impairments were less than 4 in three survey periods. Drinking and smoking
were highly prevalent among older adults. 24% (28%), 29% (25%) and 26% (21%) of
the elderly were drinker (smoker) in 1996, 1999 and 2003 respectively. Social
participation rate was quietly low in entire survey periods. The average number of social
groups of participation was less than 1. In addition, the rate of participation in volunteer
work was less than 10%.
25
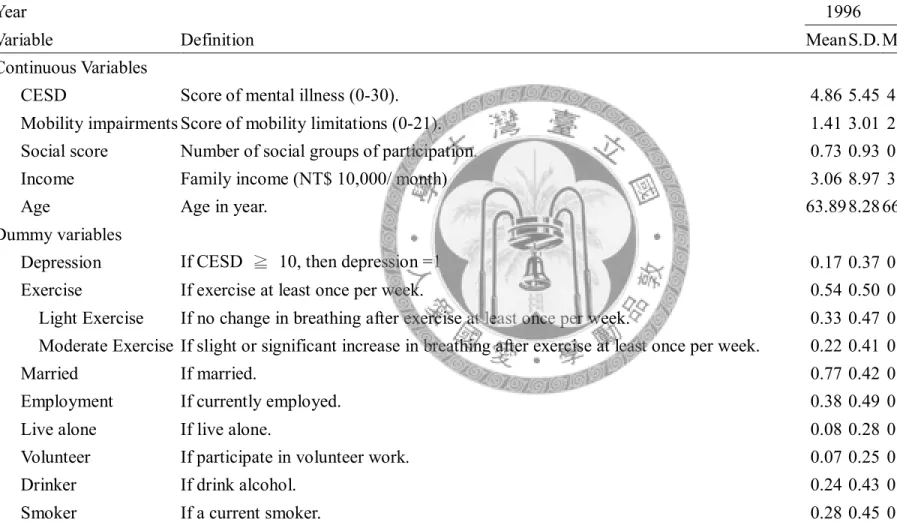
Table 4 Sample statistics
Year 1996 1999 2003
Variable Definition Mean S.D. Mean S.D. Mean S.D.
Continuous Variables
CESD Score of mental illness (0-30). 4.86 5.45 4.74 5.50 5.09 5.68
Mobility impairments Score of mobility limitations (0-21). 1.41 3.01 2.04 3.42 3.48 4.69 Social score Number of social groups of participation. 0.73 0.93 0.79 0.94 0.66 0.95
Income Family income (NT$ 10,000/ month) 3.06 8.97 3.48 4.49 2.57 3.40
Age Age in year. 63.89 8.28 66.89 8.28 70.89 8.28
Dummy variables
Depression If CESD ≧ 10, then depression =1 0.17 0.37 0.16 0.37 0.18 0.39
Exercise If exercise at least once per week. 0.54 0.50 0.63 0.48 0.67 0.47
Light Exercise If no change in breathing after exercise at least once per week. 0.33 0.47 0.39 0.49 0.39 0.49 Moderate Exercise If slight or significant increase in breathing after exercise at least once per week. 0.22 0.41 0.24 0.43 0.28 0.45
Married If married. 0.77 0.42 0.74 0.44 0.68 0.47
Employment If currently employed. 0.38 0.49 0.29 0.46 0.18 0.38
Live alone If live alone. 0.08 0.28 0.09 0.29 0.11 0.31
Volunteer If participate in volunteer work. 0.07 0.25 0.09 0.29 0.07 0.26
Drinker If drink alcohol. 0.24 0.43 0.29 0.45 0.26 0.44
Smoker If a current smoker. 0.28 0.45 0.25 0.44 0.21 0.41
* The balanced panel data include 1,825 respondents in each year.
26
Chapter 4 Methodology
The main objective of this research is to study the relationship between intensity of
exercise and mental health. Utilizing a panel data from SHLSE, the fixed-effect model
is estimated. We will begin the discussion of this section by introducing the formal
specification of each econometric model, and then we pay special attention on
fixed-effect Tobit and fixed-effect probit models in section 4.2 and 4.3.
4.1 Econometric specifications
To reach our goal, several econometric issues need to be tackled. First, it is
necessary to control for unobserved heterogeneity problem to address the effects of
exercise on mental health. Because there are likely to be some unobservable
components which jointly determine both exercise behavior and mental health, without
controlling for such effects will lead to be biased estimations. For instance,
unobservable personal characteristics, such as personality and motivation, may be
related to mental health. This would be true if those who are more introverted or less
motivated had less chance to work out and a higher depression tendency.4 Due to the
4 If such variables are unobserved, they will be captured by random error term, which results in a
27
lack of valid and convincing instruments of these variables, we use the
individual-specific fixed effects model to control for the effects of unobserved
heterogeneity on mental health of the elderly. Second, it is a need to correct the
censoring problem which violates the basic assumption of the least-squared estimation.
If a specific individual was not depressed at all, the estimations of the CES-D equations
will be zero. Therefore, treating those groups of people as the same as other groups of
respondents are not appropriate. Third, since our third dependent variable is classified
into two classes, it is reasonable to use a binary regression model rather than ordinary
least squares estimation.
In a panel data model, a popular estimation method is to use fixed-effect model.
Unlike the general linear panel data model, the random error term uit is decomposed to
individual-specific effects and an idiosyncratic error in fixed-effect model.5 Using a
fixed-effect estimation, we are able to control for all unobserved time-invarying
individual-specific factors that are related to mental health.6
Assuming that the individual's continuous CES-D score of mental health (yit) is
determined by a linear combination of exercise behavior and other time-varying
independent variables, the effect of exercise intensity on mental health can be estimated
correlation between exercise variables and random error term.
5 The general linear panel data model is specified as: yit=α+xitβ+uit, where yit and xit are dependent variable and independent variables respectively; uit is a random error term for individual i at time t.
6 In contrast to fixed-effect model, the random-effect model assumes that vi are random variables.
28
using the following fixed-effect OLS model:
_ β _ β β ,
it it M it L it i it
y M exercise L exercise x v
(1)where the subscript i and t refer to individual and time period respectively; M_exerciseit
and L_exerciseit represent the indicators of moderate and light exercise intensities
respectively. The reference group is those who don't work out regularly at least once per
week. Thus, the parameters βM and βL represent the effects on mental health score of
each corresponding group compared to the reference group; xit is a vector of other
independent variables with corresponding vector of the parameters β; vi is
individual-specific time-constant effect and εit is assumed to be a mean-zero,
constant-variance random error term that is uncorrelated with the independent variables.
4.2 Fixed-effect Tobit model
About 28% people reported zero CES-D scores in each year. Due to the censoring
nature of the second defined dependent variable, a fixed effect Tobit model is specified
with the following equation. In our sample,
* _ β _ β β ,
it it M it L it i it
y M exercise L exercise x v
(2) where y*it is a unobservable latent variable of the censored CES-D score of eachindividual's mental health; M_exerciseit, L_exerciseit, xit, vi and εit are defined as above.
29
Instead of observingy*it, we observe yit:
* *
if 0 0 otherwise.
it it
it
y y
y
(3)
The estimators can be obtained by using maximum likelihood method with the
following likelihood function:
1
1 1
α α
1 1 ,
it it
d d
N T
it it i it i
i t
y z v z v
L
(4)where dit is an indicator that equals 1 (0) if yit > 0 (≤0); Φ(.) and (.) are cumulative
density function (CDF) and probability density function of standard normal distribution
respectively; note that we use z itα here to represent whole independent variables for
convenience.
As indicated in Greene (2003), the quantitative effects of the exogenous variables
are better presented by the marginal effects: which measure the changes in exogenous
variables on the conditional expected means of the mental health scores. Note that the
calculation of marginal effects is not trivial in nonlinear models, because taking direct
partial derivatives are not applicable for exogenous dummy variables (Greene 2003).
The appropriate formulates of the marginal effects for continuous and binary
independent variables are presented below. Here we distribute the independent variables
into a specific dummy variable (dit) and all the other variables (cit) for convenience.
Given the conditional mean function:
30
β β
[ , ] [ ] [ β β ]
( β β ),
it c it d i
it it it it c it d i
it c it d i
c d v
E y c d c d v
c d v
(5)
the marginal effects are
[ , , ] β β
β [ ]
it it it i it c it d i
TC c
it
E y c d v c d v
ME c
(6)
for continuous variables and
1 0 1 0 1[ , 1] [ , 0]
β β
TD it it it it it it
it c i it it it it d it
ME E y c d E y c d
c v
(7)
for each dummy variable, where 1it and
are evaluated at
it1 (citβcβd vi) /
;0
it and
are evaluated at
it0 (citβcvi) /
(Greene 2004). The corresponding standard errors are computed by delta method (Greene 2003).4.3 Fixed-effect probit model
Our third dependent variable is a binary indicator of depression which is defined
using the appropriate cut-off point (i.e. CES-D score ≥ 10 for depression; and 0
otherwise). If the unobserved latent variable is indicated by the continuous variable Iit
*,
we incorporate the same independent variables discussed above and use the following
fixed-effect probit model:
* _ β _ β β .
it it M it L it i it
I M exercise L exercise x v
(8)31
Given the observed rule if a binary indicator Iit = 1 for Iit* > 0:
1 if * 0 0 otherwise.
it it
I
I
(9)
The estimators can be obtained by using maximum likelihood method with the
following likelihood function:
11 1
α 1 α ,
it it
d d
N T
it i it i
i t
L z v z v
(10)where dit is an indicator that equals 1 (0) if Iit =1 (=0); Φ(.) is CDF of standard normal
distribution.
The mean function for fixed-effect probit model is
[ it it, it] ( itβc itβd i).
E I c d
c
d
v
(11)The corresponding marginal effects for fixed-effect probit model are
[ , , ]
β ( β β )
it it it i
PC c it c it d i
it
E y c d v
ME c d v
c
(12)
for continuous variables and
[ , 1] [ , 0]
( β β ) ( β )
PD it it it it it it
it c d i it c i
ME E y c d E y c d
c v c v
(13)
for each dummy variable (Greene 2004).
32
Chapter 5 Results
In this chapter, we examine the effect of exercise intensity and related variables on
mental health and depression. We begin our discussions of our results by presenting for
the case of the continuous and censored specifications of the mental health dependent
variables. The estimation results for our third binary dependent variable, whether each
individual is defined as depression or not, are exhibited in section 5.2.
5.1 The determinants on mental health
The estimation results of the fixed-effect OLS and fixed-effect Tobit model are
presented in Table 5. We report two sets of regression models: the first part is the results
of the fixed-effect OLS model, and the second part is the marginal effect of the
fixed-effect Tobit model. The estimated coefficients of the Tobit model are not reported
because they show no meanings of the magnitudes or quantitative effects of the
exogenous variables on mental health. In general, the estimated coefficients and implied
marginal effects are consistent for the two models, though quantitative differences do
observed.
The results, most noticeably, indicated that regular exercise dose significantly
improve elderly mental health. However, the intensity of exercise plays an important
33
role in determining mental health. In particular, evidence shows that the effect of light
exercise is more substantial than the effect of moderate exercise. The estimates indicate
that comparing to non-exercisers, light intensity exercisers lead to a lower CES-D score
by 0.62 point in the OLS model, and by 0.67 point in the Tobit model. On the other
hand, the effects are subtle for moderate intensity exercisers; they have a lower CES-D
score by about 0.3-0.4 point in these two models. This improvement is roughly half as
long as light intensity exercisers. One possible interpretation is that moderate intensity
exercise may be too much for maintaining the necessary health condition of the elderly.
Therefore, moderate intensity exercise is not as effective as light intensity exercise on
elderly health.
Among the other factors, family characteristics are also significantly associated
with mental health among the elderly. First, evidence points to a positive relationship
between marital status and mental health. Elderly with a spouse or partner have better
mental health by about 0.8 point in these two models. Second, living alone is negatively
associated with mental health. The estimated marginal effect is 0.66 in the Tobit model,
and a slightly higher effect is found in the OLS model (0.73). Health status also plays an
important role on mental health. Both OLS and Tobit results indicate that an additional
score of mobility impairment increases the CES-D score by 0.27 point.
Regarding to the two lifestyle indicators, current drinkers are more likely to have
34
better mental health, though the effect is only significant in the Tobit model. The
marginal effect of drinker implies that the CES-D scores of drinkers are 0.38 compared
to non-drinkers. As to the roles of social support, interestingly, we find a strong and
significant relationship between volunteer work and mental health. The estimated
coefficient in the OLS model shows that the CES-D scores of volunteers are reduced by
approximately 0.9 point. The quantitative size of this effect (1.2) is much larger in the
Tobit model. This likely reflects that volunteer involvement is beneficial to improve the
individual mental health.
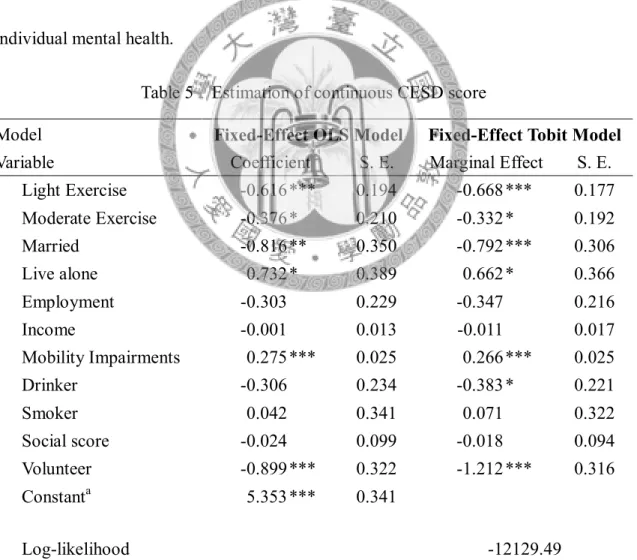
Table 5 Estimation of continuous CESD score
Model
Fixed-Effect OLS Model Fixed-Effect Tobit Model
Variable Coefficient S. E. Marginal Effect S. E.
Light Exercise -0.616 *** 0.194 -0.668 *** 0.177 Moderate Exercise -0.376 * 0.210 -0.332 * 0.192
Married -0.816 ** 0.350 -0.792 *** 0.306
Live alone 0.732 * 0.389 0.662 * 0.366
Employment -0.303 0.229 -0.347 0.216
Income -0.001 0.013 -0.011 0.017
Mobility Impairments 0.275 *** 0.025 0.266 *** 0.025
Drinker -0.306 0.234 -0.383 * 0.221
Smoker 0.042 0.341 0.071 0.322
Social score -0.024 0.099 -0.018 0.094
Volunteer -0.899 *** 0.322 -1.212 *** 0.316
Constanta 5.353 *** 0.341
Log-likelihood -12129.49
Note: S.E. = standard error. ***, ** and * indicated the significance at the 1%, 5%, and 10% levels.
a STATA reports the constant term as average value of the fixed effects.
35
5.2 The determinants on depression
Our third dependent variable, whether the individual has depressive symptoms or
not, is coded as a binary response. The estimates from the fixed-effect probit model are
shown in Table 6. In addition to the estimated coefficients, we also report the marginal
effects to quantify the effects of the exogenous variables on the probability of being
depressed.
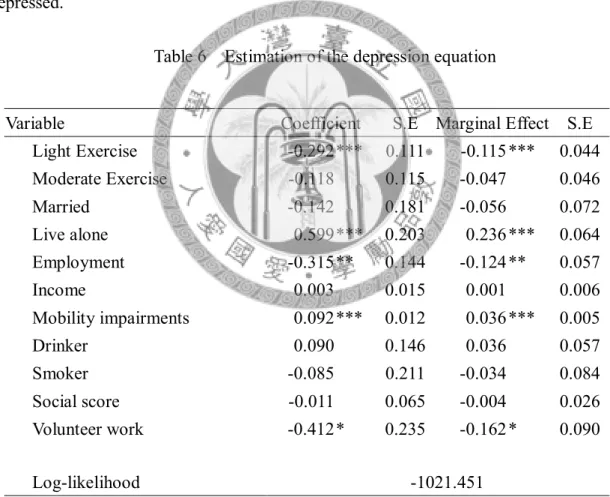
Table 6 Estimation of the depression equation
Variable Coefficient S.E Marginal Effect S.E
Light Exercise -0.292 *** 0.111 -0.115 *** 0.044 Moderate Exercise -0.118 0.115 -0.047 0.046
Married -0.142 0.181 -0.056 0.072
Live alone 0.599 *** 0.203 0.236 *** 0.064 Employment -0.315 ** 0.144 -0.124 ** 0.057
Income 0.003 0.015 0.001 0.006
Mobility impairments 0.092 *** 0.012 0.036 *** 0.005
Drinker 0.090 0.146 0.036 0.057
Smoker -0.085 0.211 -0.034 0.084
Social score -0.011 0.065 -0.004 0.026
Volunteer work -0.412 * 0.235 -0.162 * 0.090
Log-likelihood -1021.451
Note: S.E. = standard error. ***, ** and * indicated the significance at the 1%, 5%, and 10% levels.
The results present a notable difference between light and moderate intensity
exercise on the likelihood of being depressed, which is different from the exercise
intensity effects on mental health. In the fixed-effect probit model, moderate intensity
36
exercise is not significant to determine the likelihood of depression, while light intensity
exercise leads to a lower probability of being depressed: 11.5% at the 1% level of
significance. This is a reasonable result, as those moderate intensity exercisers might
receive less benefits from exercise, which results in insufficient efforts to fighting
against depression. The empirical literature is inconclusive on the relationship between
exercise intensity and depression of the elderly. Our result is similar to Lindwall et al.
(2007), who found that light intensity exercise had a strong effect on elderly women, but
differs to Singh et al. (2005), who found high intensity PRT was more effective than low
intensity PRT.
Living alone appears to exert an influence on depression. The estimated marginal
effect indicates that elderly who live alone have a higher probability of being depressed
(23.6%). In addition, working status is associated with depression. Elderly who have a
current job are less likely to suffer from depression. On average, they have 12.4% lower
in probability of being depressed, holding other things constant.
As in mental health equation, health status is also significant in determining
psychological disorders. An additional score of mobility impairment increases the
likelihood of depression by 3.6%. Volunteer work can reduce depression as well. The
estimated marginal effect suggests that volunteers for social activities have a 16.2%
lower in probability of being depressed.
37
Chapter 6 Conclusion
Old age depression has been one of the widely studied topics in public health.
Researchers have examined the association between potential determinants and
depression among the elderly, and have demonstrated that exercise is an effective
treatment for mental illness. Although little attention had been paid to examine the
intensity of exercise on mental health, the findings are still inconclusive. In addition,
few studies are conducted specifically on the elderly population. In this study, we
provide new evidence on the effects of exercise intensities on mental health by using a
longitudinal survey of Taiwanese elderly. A more sophisticated econometric model is
then applied to control for potential unobserved heterogeneity. We also take the issues
of limited dependent variables into account, and use panel version of nonlinear models.
The estimation results indicate that exercise behavior, family characteristics,
socioeconomic status, health status, lifestyle and social support play important roles on
elderly mental health and depression. Most importantly, our estimation results suggest
that exercise be good for mental health of the elderly, but significant difference does
exist in different degree of intensities. In contrast to traditional inverted-U hypothesis
which assumes that moderate intensity exercise is the optimal pattern for positive
affective change, our results indicate that light intensity exercise is much better than
moderate intensity exercise for elderly mental health. In addition, our results also
38
suggest that light intensity exercise decreases the likelihood of depression, while
moderate intensity exercise doesn’t. Some policy implications can be inferred from our
findings for Taiwan’s public health policy. In order to promote mental health and reduce
symptoms of depression among the elderly, it is important to encourage them to exercise
regularly. Furthermore, our results suggest that interventions on psychological outcomes
should focus on exercise intensity. For Taiwanese elderly, light intensity exercise (i.e. no
change in breathing after exercise) is better to enhance elderly mental health.
Although we have investigated the relationship between exercise intensity and
mental health among the elderly, several limitations are revealed. First, because our
exercise intensity measurement is constrained by the data, it may be difficult to
distinguish the effects of exercise intensity on mental health in this study from previous
literatures that used a variety of intensity measurements. Second, both non-response in
sequent survey waves and missing values on key variables contribute to sample attrition
in our panel data, which reduces the sample size and thus reduces precision of estimates.
Third, some interviews were conducted with proxies who were not asked for any of
subjective questions (e.g. self-report health). This may lead to potential sample selection
bias, because it is reasonable to believe those individuals are more likely to be in poor
health and depressed.