國立臺灣大學公共衛生學院職業醫學與工業衛生研究所 碩士論文
Graduate Institute of Occupational Medicine and Industrial Hygiene College of Public Health
National Taiwan University Master Thesis
職業性肌肉骨骼疾病與就業場所相關暴露因子之探討:
腕道症候群及腰部椎間盤疾患
The Relationship Between Work-related Musculoskeletal Disorders and Workplace Exposure Factors - CTS and HIVD
楊善圍
Shan-Wei Yang
指導教授:郭育良 博士 黃耀輝 博士 Advisor:Yue-liang Leon Guo, Ph.D.
Yaw-Huei Hwang Ph.D.
中華民國 102 年 07 月 July 2013
致謝
人生晃眼兩年,在職衛所,學到的太多,要繼續學習的還有更多。
感謝我的指導教授:郭育良老師,願意指導我,並且給我機會讓我接觸不同 的計劃,從中使我成長,並且耐心地逐步實作讓我學習,除此之外,在待人接物 上也使我實際體會到所謂「身教重於言教」的本質!而在將屆畢業之時,更要謝 謝老師,引介我至另一個世界與舞台,讓我可以走出學校接受更嚴峻的挑戰。同 時也要感謝另一位指導教授:黃耀輝老師,總是很認真傾聽與閱讀我的報告,並 且給予相當多中肯且實用的建議;另外還有高雄第一科技大學的許昺奇老師,在 合作的計畫中給予我相當多的幫助,以及成為最堅強的後盾,支持著整個計畫的 順利進行;清華大學的游志雲老師,提供了相當專業的人因工程相關的技術,讓 我們的整個計畫具畫龍點睛之妙;感謝職業傷病管理服務中心職業傷病診察網所 提供的資料;感謝勞工安全衛生研究所的多項支持,包括工作衛生安全認知調查 團隊提供的資訊,還有潘儀聰副研究員的辛勤付出。
感謝郭家研究室的支持:謝謝博後秉鈺學姊總是聽我報告,幫忙我修改不完 善的地方,並且教導我相當相當多的統計方式;謝謝博士班的唯珊學姊,聽我發
牢騷給我鼓勵,並且耐心教導我完成第一篇的Poster,真正帶我進入研究的領域;
謝謝座位旁邊的曉鈴學姊,因為地緣的關係,常常可以跟您聊天,也從您那邊學 習到了許多為人處世的方法;謝謝博士班的瑜嬬學姊,跟我分享好多經驗,給我 心靈上的滋潤,讓我開花;謝謝博士班的冠含學姊,總是溫柔和善地鼓勵我、和 我聊天,給我心理上的支持;謝謝博士班的銘杰學長,努力地幫忙我一起思考、
分析問題解決的辦法;謝謝同屆的姿瑋,在修課以及研究上面給了我相當多的幫 助以及建議;還有念偉學長、亦潔學姊、仕哲學長、雅慧姊、均和、冠霆、育禎 等等,郭家要感謝的人實在太多,謝謝你們陪我度過兩年的時光。感謝計畫進行 中,清華大學建偉學長的幫忙與聯繫,以及高科大雅婷的行政作業幫助。
謝謝同屆的儷瑾、欣華、佳嫻以及嘉曜,很開心你們始終沒有忘記在三樓的 我,總是拉上我一起聚會吃飯,一起歡笑、抱怨、流淚,兩年有你們,給我相當 多的溫暖與力量。
感謝我的家人,永遠是最穩固的避風港。最感謝我的學長柏宇,在各個層面 都給我最大的支持,學業上:在公司加班之後回家還要加班,逐字逐句幫我修改 論文;學業外:陪我一起完成了五場全馬,七場半馬,無數次河濱與寶山清交的 路線;生活上:容忍我任性、龜毛又孤僻的那一面,陪伴著我,我想要什麼,都 會想辦法帶我去達成。希望我們可以一起,一步一步地完成我們小小的溫馨的世 界。謝謝橘橘跟粉圓,給我很多溫度。
謝謝Facebook 上的鍵盤好友們,給我拍拍、抱抱、關心我的近態,鼓勵我度
過每個人生的重大難關。
這本論文能夠完成,要感謝的人太多,謝謝每個你,伴我度過這段時光。
祝福大家都順利平安、身體健康。
最後,期許自己進入社會染缸後,不要忘記初衷:「為生民立命,為天地立心,
為往聖繼絕學,為萬世開太平。」--張載。
摘要
職業性肌肉骨骼疾病 (Work-related musculoskeletal disorders, WMSDs) 在國 際間已成為最常見的職業疾病,因職業性肌肉骨骼疾病連帶而來財務花費也高居 所有職業性疾病之冠。在台灣,職業性肌肉骨骼疾病幾乎佔了所有職業性疾病的 一半,而且也耗費了相當多的勞保補償。
本研究希望能找到罹患職業性肌肉骨骼疾病的高風險行業,以及釐清人因相 關因子與勞工自覺肌肉骨骼症狀與罹患職業性肌肉骨骼疾病之關係;另外,亦期 望能以工作場所人因暴露以及勞工自覺痠痛症狀調查,發展偵測罹患職業性肌肉 骨骼疾病風險之方法。職業性肌肉骨骼疾病種類繁多,本研究選取腕道症候群 (Carpal tunnel syndrome, CTS)為上肢部位代表、腰部椎間盤疾患 (Herniation of intervertebral disc, HIVD)為頸椎、腰椎部位代表,進行深入的探討。
利用生態研究架構,將兩個互相獨立的資料庫依 89 個行業別作為連結:(1)
臺灣職業傷病通報系統,取得 2008-2011 四年間腕道症候群及腰部椎間盤疾患的
通報資料,並分性別算出調整年齡之標準化發生率為依變項;(2) 勞研所 2010 年
之工作環境安全衛生狀況認知調查,取得勞工自填之工作環境人因暴露因子及勞 工自覺痠痛且影響工作表現在各行業之暴露比例為自變項。
以各行業總就業人口數為比重,線性迴歸分析結果顯示:「重複性手部動作」
(β: 0.027, 95% CI: 0.008, 0.046) 是男性罹患腕道症候群主要的危險因子、「使用震
動的手部工具」 (β: 0.124, 95% CI: 0.063, 0.185)則是女性罹患腕道症候群主要的危 險因子;在腰部椎間盤疾患部分,男性以「全身震動」 (β: 0.106, 95% CI: 0.082, 0.133) 及「搬運重物」 (β: 0.008, 95% CI: 0.001, 0.015)、女性以「全身震動」 (β: 0.086, 95%
CI: 0.016, 0.157)及「不自然的姿勢」 (β: 0.030, 95% CI: 0.008, 0.052)為主要危險因 子,此外,更發現男性與女性與各別的二種因子都有顯著的加成作用,同時暴露 於二種因子而罹患腰部椎間盤疾患的危險性,高於僅暴露於單一種危險因子。
本研究亦針對一光電廠進行上肢肌肉骨骼問題的調查,結果顯示:在填答問
卷之359 位員工之中,76 位有自覺肌肉骨骼不適症狀,而其中有 19 位被超音波診
斷出確實有肌肉骨骼的問題。最常見的上肢肌肉骨骼問題為旋轉肌袖症候群 (N=17) 以及肩峰鎖骨關節腫脹 (N=7)。
工作場所人因暴露因子以及勞工自覺痠痛症狀,與職業性肌肉骨骼疾病確實 有其相關性,更深入探討相關貢獻量以及機轉有其必要性。且此方法可以使用相 當簡單的問卷取得相關資料,未來應可以用來發展篩檢各種工作場所,以評估或 預測各職業場所引起職業性肌肉骨骼疾病之相關風險。
關鍵字:職業性肌肉骨骼疾病、腕道症候群、腰部椎間盤疾患、人因工程、自覺 症狀、通報系統、共同作用
Abstract
Work-related musculoskeletal disorders (WMSDs) have become the most common occupational diseases internationally. Expenses due to WMSDs are most important among all occupational diseases. In Taiwan, WMSDs accounted for almost 50% of the total occupational diseases, and caused a significant portion of labor insurance payments.
The aim of this study is to find the high risk industries which have higher WMSDs incidence. Therefore, we wish to develop a method which use workplace factors to detect the risk of workers suffering from WMSDs. Because carpal tunnel syndrome (CTS) and herniation of intervertebral disc (HIVD) was the most two common WMSDs, this study chose these two WMSDs as outcome variables.
We designed an ecological study using two separate databases: (1) Taiwan's occupational disease and injury notification system (ODIS). (2) Survey of Perceptions of Safety and Health in the Work Environment in 2010. We used the CTS and HIVD as cases reported on ODIS from 2008 to 2011 to calculate the age-adjusted standardized incidence rates (SIR) as dependent variable. The independent variables included the self-reported ergonomic factors and self-reported musculoskeletal discomforts. The two databases were connecting by 89 job divisions.
In this study, linear regression was used to find the relationship between workplace factors and CTS and HIVD, and we used the number of employed workers in each job category as weighting. From this study, we found out that “repetitive hand movements”
(β: 0.027, 95% CI: 0.008, 0.046) was a major risk factor for male with CTS and
“vibration from hand tools” (β: 0.124, 95% CI: 0.063, 0.185) for female with CTS. As for HIVD, the risk factors were “whole body vibration” (β: 0.106, 95% CI: 0.082, 0.133) and “heavy lifting” (β: 0.008, 95% CI: 0.001, 0.015) for male, and “whole body vibration” (β: 0.086, 95% CI: 0.016, 0.157) and “awkward posture” (β: 0.030, 95% CI:
0.008, 0.052) for female respectively. Moreover, “whole body vibration” and “heavy lifting” showed significant additive effect for the male and “whole body vibration”;
“awkward posture” showed significant additive effect for the female.
A field study was conducted in a factory, in order to understand the gap between self-reported symptoms and diagnosed musculoskeletal disorders in upper extremities.
A total of 359 questionnaires were completed. There were 76 workers having self-reported musculoskeletal symptoms and a total of 19 workers were diagnosed as having musculoskeletal disorders by ultrasound. The most frequently diagnosed conditions were rotator cuff syndrome (N=17) and acromioclavicular joint distention (N=7).
In conclusion, the workplace factors had relationship with the incidence of WMSDs.
Such factors can be identified by sample screening tools as questionnaire. By using this approach, it is possible to screen various kinds of workplaces and assess or predict the risk of WMSDs. Also, this will promote future efforts to improve the effectiveness in ergonomic intervention in workplaces and also establish the model for prevention against WMSDs.
Key words: WMSDs; Carpal tunnel syndrome (CTS); Herniation of intervertebral disc
(HIVD); Ergonomic; Self-reported discomforts; Surveillance; combination of risk factors
Contents
口試委員會審定書 ... I 致謝 ... II 摘要 ... IV Abstract ... VI Contents ... IX List of Tables ... XI List of Figures ... XIII
Chapter 1 Introduction ... 1
Chapter 2 Literature review ... 3
2.1 The significance of WMSDs ... 3
2.2 The risk factors of WMSDs, CTS and HIVD ... 5
2.2.1 Risk factors of CTS ... 6
2.2.2 Risk factors of HIVD ... 7
2.3 WMSDs in different industries and occupations ... 7
Chapter 3 Material and Method ... 10
3.1 Research Design ... 10
3.2 Subjects/Materials ... 10
3.2.1 Standard Industrial Classification System ... 11
3.2.2 Collected and classified the WMSDs cases nearly four years (2008-2011) ... 12
3.2.3 Selected and recognized the disease types of WMSDs ... 14
3.2.4 Survey of Perceptions of Safety and Health in the Work Environment 15 3.3 Data analysis ... 15
3.3.1 Standardized incidence rates (SIR) ... 16
3.3.2 Linear regression ... 16
3.3.3 Geometric mean of SIR ... 17
Chapter 4 Results ... 19
4.1 The collected and classified WMSDs cases for nearly four years (2008-2011) ... 19
4.2 Selected and recognized the disease types of WMSDs ... 20
4.3 Standardized incidence rates in different job categories of WMSDs ... 21
4.3.1 Different job categories with CTS: case numbers and SIR ... 21
4.3.2 Different job categories with HIVD: case numbers and SIR ... 22
4.4 Survey of Perceptions of Safety and Health in the Work Environment ... 23
4.4.1 Workplace exposure factors - ergonomic factors ... 23
4.4.2 Workplace exposure factors - self-reported musculoskeletal discomforts ... 25
4.5 The relationship between Work-related musculoskeletal disorders and workplace ergonomic factors ... 26
4.5.1 Log-transformed SIR (case/year/million workers) and workplace ergonomic factors (% reported +) - CTS ... 27
4.5.2 Log-transformed SIR (case/year/million workers) and workplace ergonomic factors (% reported +) -HIVD ... 27
4.6 The relationship between the geometric mean of SIR and different levels of workplace exposure factors ... 28
4.6.1 Geometric Mean SIR of CTS and ergonomic factors ... 29
4.6.2 Geometric Mean SIR of HIVD and ergonomic factors ... 30
4.6.3 Combination of risk factors - HIVD ... 33
4.7 The relationship between the geometric mean of SIR and different levels of self-reported musculoskeletal discomforts ... 35
4.7.1 Geometric Mean SIR of CTS and hands or wrists musculoskeletal discomfort ... 35
4.7.2 Geometric Mean SIR of HIVD and low back or waist musculoskeletal discomfort ... 36
Chapter 5 Field study ... 37
5.1 The objective of the field study ... 37
5.2 Material and method of the field study ... 37
5.3 Results of the field study ... 38
5.4 Conclusion and future works ... 39
Chapter 6 Discussion ... 40
6.1 WMSDs accounted for the largest part of occupational diseases ... 40
6.2 The high risk industrial categories suffering from WMSDs ... 41
6.3 The risk factors of WMSDs ... 42
6.4 Secondary self-reported questionnaire ... 44
6.5 Limitation ... 45
Chapter 7 Conclusion ... 47
Reference ... 48
Appendix ... 147
1. Questionnaire of field study ... 147
2. Scandinavian criteria of physical examination ... 152
List of Tables
Table 1. Standard Industrial Classification System of the republic of china ... 53
Table 2. Incidence rate of occupational diseases ... 56
Table 3. Demographic data of 2008-2011 ODIS cases ... 57
Table 4. Classification and selection for WMSDs ... 58
Table 5. The CTS cases by age and industry sector distribution ... 58
Table 6. SIR of CTS in 89 job divisions (Cases per 106 population per year) ... 59
Table 7. The HIVD cases by age and industry sector distribution ... 64
Table 8. SIR of HIVD in 89 job divisions (Cases per 106 population per year) ... 65
Table 9. Workplace ergonomic factors in difference job divisions, Male ... 70
Table 10. Workplace ergonomic factors in difference job categories, Female ... 76
Table 11. Self-reported musculoskeletal discomforts in different job divisions ... 82
Table 12. Simple linear regression of log transformed SIR of CTS (case/yr/million workers) and workplace ergonomic factors (% reported +) ... 87
Table 13. Multiple linear regression of SIR in CTS and ergonomic risk factors ... 87
Table 14. Simple linear regression of log transformed SIR of HIVD (case/yr/million workers) and workplace ergonomic factors (% reported +) ... 87
Table 15. Multiple linear regression of SIR in HIVD and ergonomic risk factors ... 87
Table 16. Level of groups and its included job divisions covering the percentage range and the groups in “vibration from hand tools” ... 88
Table 17. Level of groups and its included job divisions covering the percentage range and the groups in “repetitive hand movements” ... 93
Table 18. Level of groups and its included job divisions covering the percentage range and the groups in “heavy tools used” ... 97
Table 19. Level of groups and its included job divisions covering the percentage range and the groups in “whole body vibration” ... 102
Table 20. Level of groups and its included job divisions covering the percentage range and the groups in “heavy lifting” ... 106
Table 21. Level of groups and its included job divisions covering the percentage range and the groups in “awkward posture” ... 110
Table 22. Relationship between SIR of HIVD and combination of ergonomic factors, Male ... 114
Table 23. Relationship between SIR of HIVD and combination of ergonomic factors, Female ... 114
Table 24. Level of groups and its included job divisions covering the percentage range and the groups in “hands or wrists musculoskeletal discomfort” ... 115 Table 25. Level of groups and its included job divisions covering the percentage range
and the groups in “low back or waist musculoskeletal discomfort ... 120 Table 26. Results of physical examination and ultrasound examination ... 125 Table 27. Distribution of demographics and working conditions of workers ... 131
List of Figures
Figure 1. A conceptual model of the possible roles and influences that various factors may
play in the development of musculoskeletal disorders [25]. ... 133
Figure 2. The network for Occupational Disease and Injury Services in Taiwan ... 134
Figure 3. Calculated process of SIR ... 135
Figure 4. Flow chart of statistical methods ... 135
Figure 5. Results of selected and recognized the WMSDs ... 136
Figure 6. The SIR of CTS with the self-reported percentage of workers exposure to “vibration from hand tools” levels, Male ... 137
Figure 7. The SIR of CTS with the self-reported percentage of workers exposure to “vibration from hand tools” levels, Female ... 137
Figure 8. The SIR of CTS with the self-reported percentage of workers exposure to “repetitive hand movements” levels, Male ... 138
Figure 9. The SIR of CTS with the self-reported percentage of workers exposure to “heavy tools used” levels, male ... 138
Figure 10. The SIR of HIVD with the self-reported percentage of workers exposure to “whole body vibration” levels, Male ... 139
Figure 11. The SIR of HIVD with the self-reported percentage of workers exposure to “whole body vibration” levels, Female ... 139
Figure 12. The SIR of HIVD with the self-reported percentage of workers exposure to “heavy lifting” levels, Male ... 140
Figure 13. The SIR of HIVD with the self-reported percentage of workers exposure to “heavy lifting” levels, Female ... 140
Figure 14. The SIR of HIVD with the self-reported percentage of workers exposure to “heavy tools used” levels, Male ... 141
Figure 15. The SIR of HIVD with the self-reported percentage of workers exposure to “heavy tools used” levels, Female ... 141
Figure 16. The SIR of HIVD with the self-reported percentage of workers exposure to “awkward posture” levels, Male ... 142
Figure 17. The SIR of HIVD with the self-reported percentage of workers exposure to “awkward posture” levels, Female ... 142
Figure 18. The SIR of CTS with the self-reported percentage of “hands or wrists musculoskeletal discomfort” levels, Male ... 143 Figure 19. The SIR of CTS with the self-reported percentage of “hands or wrists
musculoskeletal discomfort” levels, Female ... 143
Figure 20. The SIR of HIVD with the self-reported percentage of “low back or waist musculoskeletal discomfort” levels, Male and Female ... 144
Figure 21. Case including criteria in the field study ... 144
Figure 22. Flow chart of field study ... 145
Figure 23. Flow chart of workers inclusion in field study ... 146
Chapter 1 Introduction
Work-related musculoskeletal disorders (WMSDs) are common health problem in the working population. WMSDs include many conditions that affect the muscles, tendons, ligaments, and joint cartilage, and spinal discs, as well as the anatomically associated peripheral motor and sensory nerves [1-4]. As well, these include such ailments as low back pain, shoulder disorders, and distal upper extremity disorders, including tendonitis, epicondolytis, and carpal tunnel syndrome. WMSDs are the leading nature of injury among non-fatal occupational injuries and illnesses [5].
WMSDs have caused serious social problems such as wage compensation, medical expenses and reduced productivity, as well as worker’s physical and psychological pain [6, 7]. WMSDs are a worldwide concern and distributed among both industrialized countries and industrially developing countries [8].In Taiwan, WMSDs accounted for almost 50% of the total occupational diseases, and caused a significant portion of labor insurance payments.
For most WMSDs, both onset and duration are more often chronic or sub-chronic than acute. Typically, they tend to develop after months or years of overuse of the soft tissues. It has been observed that within a population occupationally exposed to particular ergonomic stressors, several different types of clinical disorders may arise in
different individuals. Thus, it has often been statistically efficient to study WMSDs as a group [9]. However, each type of WMSD (e.g., low back WMSDs, carpal tunnel syndrome, tendinitis, epycondilitis, etc.) has different risk factors. It is difficult for a single study to satisfy all criteria to determine a causal relationship between risk factors and WMSDs [4]. Thus, it is important to integrate information derived from a comprehensive database to identify factors contributing to different types of WMSD.
This way, risk factors and the level of evidence of their relationship with each WMSD can be evaluated. WMSDs of the back and upper extremity appear to be more common than those affecting the lower extremity [9].
In 2011, Thomas compared 2002 and 2006 General Social Survey about WMSDs, concluded that new strategies for preventing both low back and upper extremity MSDs should focus on work stress, heavy lifting, and hand movement [10]. Therefore, in this study, we emphasized on carpal tunnel syndrome (CTS) and herniation of intervertebral disc (HIVD) as the targets. The aim of this study was to find the high risk industries which have higher WMSDs (CTS and HIVD) incidence rate. Furthermore, we anticipate to develope the research methods which use the workplace factors to detect the risk of WMSDs and identifying the relationship between Work-related musculoskeletal disorders and workplace exposure factors.
Chapter 2 Literature review
2.1 The significance of WMSDs
Musculoskeletal disorders (MSDs) are injuries or dysfunctions affecting muscles, bones, nerves, tendons, ligaments, joints, cartilages, and spinal discs. MSDs include sprains, strains, tears, soreness, pain, carpal tunnel syndrome, hernias, and connective tissue injuries of the structures previously mentioned [4].
WMSDs are a major cause of health problems, disability and health care utilization in industrialized countries [11], and are widespread in many countries, with substantial costs and impact on quality of life. Although not uniquely caused by work, they constitute a major proportion of all registered and/or compensable Work-related diseases in many countries. Accurate data on the incidence and prevalence of musculoskeletal disorders are difficult to obtain, and official statistics are difficult to compare across countries. Nevertheless, WMSDs are the single largest category of Work-related illness, representing a third or more of all registered occupational diseases in the United States, the Nordic countries, and Japan [12, 13]. WMSDs are not directly related to high mortality but still giving a major contribution to the burden of disease and perceived health [14]. WMSDs also cause great demands on health care services, constituting about one-third of all visits to primary care [15]. WMSDs are a major cause of sickness absence from work. Moreover, WMSDs are the most expensive form of
work disability [16, 17].
In Sweden, they have been the most common cause for sick leave and disability pension since the 1960s [18]. It was estimated that the cost of WMSD was approximately 215 billion dollars in 1995 in the US; 26 billion Canadian dollars in 1998 in Canada, and 38 billion Euros in 2002 in Germany [16, 19, 20]. The United Kingdom Health and Safety Executive estimated, on the basis of a Labor Force Survey, in 2009-2010 musculoskeletal disorders were the most commonly reported illness types and 37% of working days lost were due to musculoskeletal disorders [21]. In the state of Washington between 1997 and 2005, 27% of all state fund-accepted claims were due to Work-related musculoskeletal disorders (WMSDs) of the neck, back and upper extremities [22].
Also, musculoskeletal conditions are both common and have a major impact on pain, function, activity, participation in society and self-reported health.
Musculoskeletal conditions have been reported to be responsible for 40% of all chronic conditions, 54% of all long-term disability and 24% of all restricted activity days [11].
In the UK, approximately 20 million working days are lost each year because of low back pain (LBP), and the latter accounts for 40% of the time lost due to industrial injury [23]. In Korea, the number of compensated workers for WMSDs including LBP was 1,954 in 2007, which amounted to about 34.3% of total occupational diseases [24].
Regardless of the actual costs, the problem is large both in health and economic terms [5].
2.2 The risk factors of WMSDs, CTS and HIVD
Figure 1 shows a conceptual model of the possible roles and influences that various factors may play in the development of MSDs. The dotted box outline on the right indicates the possible pathways and processes that could occur within the person, including the biomechanical load-tolerance relationship and the factors that may mediate the load-tolerance relationship, such as individual factors and adaptation.
Outcomes may be a result of this relationship and may be influenced by individual factors, such as conditioning or psychological state. The dotted box on the left indicates the possible influences of the workplace on the sequence of events that can lead to musculoskeletal disorders in the person. Arrows between “the workplace” factors and
“the person” box indicate the various research disciplines (epidemiology, biomechanics, physiology, etc.) that have attempted to explain the relationship [25].
The physical job features that are frequently cited as risk factors for WMSDs, based on both experimental science and epidemiologic investigations, include rapid work pace and repetitive motion patterns; insufficient recovery time; heavy lifting and forceful manual exertions; non-neutral body postures (either dynamic or static); mechanical
pressure concentrations; segmental or whole body vibration; local or whole-body exposure to cold; and any of these in combination with each other or with undesirable features of the psychosocial [13].
The enormous scope of the problem is confirmed by statistics from the Annual Survey of Occupational Injuries and Illnesses, conducted by the Bureau of Labor Statistics (BLS). For those cases involving days away from work, BLS reports that in 2001 there were 522,528 WMSDs cases, 75% of those were due to overexertion and another 11.5% were due to repetitive motion disorders. The report indicated that 219,665 of these injuries involved lifting and another 69,247 were associated with bending, climbing, reaching, and twisting. Also, 60,099 injuries or illnesses occurred as a result of repetitive motion, including typing or key entry, repetitive use of tools, and repetitive placing, grasping, or moving of objects other than tools [26].
2.2.1 Risk factors of CTS
Carpal tunnel syndrome (CTS) is one of the most common upper limb compression neuropathies [27]. CTS derives from entrapment of the median nerve within the carpal canal of the wrist. Biomechanical risk factors: repetitive work, manual force, vibration transmitted to the hand, combination of risk factors (e.g., force and repetition, force and wrist bending) [28].
2.2.2 Risk factors of HIVD
Low-Back Disorders include low back syndrome which is soft tissue injury characterized by back pain with localized symptoms and no neurological deficits, and lumbosacral disc herniation disease which is lumbosacral disk degeneration or herniation, typically with nerve root compromise and associated neurological deficits [28]. The traditional view of intervertebral disc degeneration has been that it was a process related to normal ageing as well as changes related to physical loading over the lifetime [29]. Low back pain, have been associated with heavy workload, repetitive and static work, bending and twisting, whole body vibration, job dissatisfaction, imbalance between demand and control, and lack of psychological and social support at work [30-32].
2.3 WMSDs in different industries and occupations
Many industries and occupations have rates that are as much as three to four times higher than the overall frequencies. High risk industries are as varied as nursing facilities, air transportation, mining, food processing, leather tanning, heavy manufacturing of vehicles, furniture, appliances and electrical equipment, and light manufacturing, including electronic products, textiles, shoes, apparel, and upholstery [28].
The Annual Survey of Occupational Injuries and Illnesses, conducted by the Bureau of Labor Statistics (BLS) noted 41% of all reported MSDs were accounted for by one occupation—operators, fabricators, and laborers. Industries with the largest numbers of MSDs were services, manufacturing, and retail trade, with 25.8, 22.9, and 16.0%, respectively [26].
Upper extremity musculoskeletal disorders have been found to be highly prevalent in manual-intensive occupations such as clerical work, postal service work, janitorial work, industrial inspection, and packaging. Back and lower limb disorders often occur in occupations that require heavy work such as manual material handling, non-neutral trunk postures, or exposure to whole-body vibration, especially while seated. The occupations at highest risk were truck drivers, operators of cranes and other large vehicles, warehouse workers, airplane baggage handlers, various construction trades, nurses, nursing aides, and other patient-care workers [2, 33].
Saftic et al. [34] investigated that risk factors for lumbar disc herniation were severe enough to require surgery in a cohort of 1,001 Croatians. Their occupational analysis included those occupations involving sitting or standing and occupations involving hard physical activity, such as agricultural work, construction work, and mechanics, fishing and soldiering. These study suggested that the heritable risk of intervertebral disc surgery was independent of the risk conferred by heavy physical
occupations.
In a small occupational study, Luoma et al. [35] examined 164 men aged 40–45 years, including 53 machine drivers, 51 construction carpenters and 60 office workers, who underwent MRI imaging and assessment for back pain. An increased risk of back pain was found in relation to signs of disc degeneration, and LBP was strongly associated with occupational factors. For example, the adjusted OR of LBP for machine drivers was 8.1 (add 95% CI). LBP was more common among machine drivers and carpenters than officer workers.
Chapter 3 Material and Method
3.1 Research Design
An ecological study was designed to identify the high risk industries (groups) and the relationship between working place related factors and WMSDs. This ecological study using two separate databases as sources which using 89 job divisions to connect :
(1) Taiwan's occupational disease and injury notification system (ODIS), reported occupational WMSDs from 2008 to 2011, calculating the age-adjusted standardized incidence rates (SIR) as dependent variable.
(2) Survey of Perceptions of Safety and Health in the Work Environment in 2010, as independent variables including self-reported of the proportion of ergonomic factors, and self-reported musculoskeletal discomforts in workplace by each job category.
By comparing the SIR, we can find out that the high risk industries (groups) in different WMSDs. Furthermore, linear regression was used to delineate the relationship between workplace exposure and WMSDs.
3.2 Subjects/Materials
The subjects for this study were employees belonging to the 89 job categories of
Standard Industrial Classification System. Data were collected using two separate databases as sources which connecting by 89 job categories: (1) Taiwan's occupational disease and injury notification system (ODIS) and (2) Survey of Perceptions of Safety and Health in the Work Environment.
3.2.1 Standard Industrial Classification System
The Standard Industrial Classification (SIC) is a system for classifying industries by a four-digit code, which was established in the United States in 1937. It is used by government agencies to classify industry areas. The SIC system is also used by agencies in other countries. In this study, we used the Standard Industrial Classification System of the Republic of China (Rev.9, 2011).
The SIC codes can be grouped into progressively broader industry classifications:
industry group, section (major group) and division. The first three digits of the SIC code indicate the industry group, and the first two digits indicate the major group. Each division encompasses a range of SIC codes. From 0100 till 0999, it stand for the division Agriculture, Forestry and Fishing; from 1000 till 1999, it stand for the division Mining; from 2000 till 3999, it stand for the division Manufacturing; from 4000 till 4999, it stand for the division Transportation, Communications, Electric, Gas and Sanitary service; from 5000 till 5199, it stand for the division Wholesale Trade; from
5200 till 5999, it stand for the division Retail Trade; from 6000 till 6799, it stand for the division Finance, Insurance and Real Estate; from 7000 till 8999, it stand for the division Services and from 9100 till 9729, it stand for the division Public Administration. The codes that start with 99 are No classifiable [36].
The 19 major groups and 89 divisions were listed in Table 1.
3.2.2 Collected and classified the WMSDs cases nearly four years (2008-2011)
In 2003, the system of occupational disease and injury services was launched, and the first center for Center of Occupational Disease and Injury Service (CODIS) was established. In 2007, a coordination center, Center of occupational Disease and Injury Management and Service (CODIMS), was also established [37]. In 2009, there were nine CODISs to provide the services, including three centers in northern, three in central, two in southern, and one in eastern Taiwan. Furthermore, each CODIS collaborates with surrounding hospitals to develop a network for occupational disease and injury services.
By the end of 2012, 56 network hospitals were established (Figure 2). The CODISs and network hospitals provide occupational health services, including diagnosing and preventing occupational diseases or injuries, occupational rehabilitation or return-to-work, and insurance compensation assistant.
The main tasks of CODIMS are:
(1) To provide the professional consultation on the management of occupational disease and injury.
(2) To establish the standard operation procedures for CODISs’ services, to ensure the quality of CODISs’ services.
(3) To investigate the clusters of occupational diseases, to develop the strategy for the prevention of occupational diseases or injuries.
(4) To maintain the reporting system of occupational diseases and injuries.
The reporting system of occupational diseases and injuries was formally launched in September 2007, which was based on the principle of previous reporting system at Department of Health [38].
The workers with injury or disease went the CODISs or network hospitals for help, and assessing, diagnosing and comparing with epidemiology studies that the occupational exposure factors were related more than 50% from the disease. Then, the doctor will report the case to Taiwan's occupational disease and injury notification
system (ODIS).
In this study, we collected the reported-cases from ODIS from 2008 to 2011 and exported data as excel form for data analysis. The reported cases used the “date of visit”
to collect cases, and its quality was examined by the reviewer who classified the cases to “probable”, “possible”, “not related” and “cannot be determined”. In our study, we
only choose the “probable” and “possible” cases for analysis.
We classified all the reported cases to occupational pulmonary disease, occupational liver disease, occupational skin disease, occupational cardiovascular disease, occupational neurological disease, occupational hematological disease, occupational renal diseases, occupational musculoskeletal diseases, occupational hearing loss, occupational eye disease, occupational physical disease, biological hazard and others. Base on the total number of employed population, the incidence of cases per 106 populations per year could be calculated.
3.2.3 Selected and recognized the disease types of WMSDs
The WMSDs reported cases from 2008 to 2011 were 2,239 cases in total, accounting for 46.8% of all the occupational disease notification. We used International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) to classify WMSDs. It was divided into upper extremities (including hand / wrist, elbow, shoulder), cervical and lumbar region and lower extremities (knee, foot / ankle) three categories according to the diseased parts and two or more diseased parts of the case will be classified in others.
In the upper extremities, we selected carpal tunnel syndrome (CTS) (ICD 354.0 Carpal tunnel syndrome), and in the cervical and lumbar region 722.93 Other and
unspecified disc disorder of lumbar region and 722.73 Lumbar region of intervertebral disc disorder with myelopathy were classified in herniated intervertebral disc (HIVD).
Furthermore, the joint region and lower extremities did not include in this study.
3.2.4 Survey of Perceptions of Safety and Health in the Work Environment
In order to provide workers with an equitable, humane, secure, and dignified environment it has always been the objective and responsibility of the Government. The Institute of Occupational Safety and Health (IOSH) has conducted surveys every three years since 1994 to characterize demand and perception of employees, employers and self-employed people for safety and health in the workplace [39].
Our study used the Survey of Perceptions of Safety and Health in the Work Environment in 2010 to get the self-reported information about working conditions such as workplace environmental ergonomic factors and musculoskeletal discomfort in the workers. We took the proportion of ergonomic factors, and the proportion of musculoskeletal discomforts in each job category.
3.3 Data analysis
Flow chart of the statistical methods was shown in Figure 4.
First, sex and age adjusted standardized Incidence Rate (SIR) for CTS and HIVD in every job category (89 divisions) were calculated. Then, the Survey of Perceptions of
Safety and Health in the Work Environment 2010 were used to count the situation of workplace in self-reported ergonomics, and musculoskeletal discomforts in each job category. Finally, simple and multiple linear regressions were to identify the relationship between WMSDs SIR and the risk factors.
3.3.1 Standardized incidence rates (SIR)
Because musculoskeletal disorders are, more common in women and will increase with age [40]. And the population component in every industry was not equivalent, it was necessary to standardize the incidence rate. In this study, SIR calculated by direct standardization using sex and age group, and use national total workforce as standard.
Incidence was calculated by 2008-2011 reported WMSDs from Taiwan's occupational disease and injury notification system (ODIS) by estimated numbers of employees in each job category. The denominator was the averaged manpower in each job category in 2008-2010 from Yearbook of manpower survey statistics. The calculation process of SIR was shown in Figure 3.
3.3.2 Linear regression
Simple and multiple linear regressions were to identify the relationship between SIR of WMSDs and the risk factors. Since the incidences of every industry were not normal distribution, we did a log-transformed to the SIR in every job category before
simple linear regression. Considering the different working population, we used the manpower survey statistical working population as weight in the statistical analysis. In the statistical model, dependent variables were log-transformed SIR of WMSDs and independent variables were the workplace environmental ergonomic factors, and musculoskeletal discomfort from Survey of Perceptions of Safety and Health in the Work Environment.
Then chose those p-values less than 0.05 from the results of simple linear regression as variables of multiple linear regression. The backward stepwise multiple linear regression was adopted here. The remained risk factors had greater contribution to WMSDs. Finally, the remained variables from multiple linear regression were chosen.
By using the median as the cut point and setting the dummy variables for the multiple linear regression, it can be checked whether there was any combination of risk factors for WMSDs.
3.3.3 Geometric mean of SIR
In order to show the relationship between the SIR of WMSDs and the risk factors clearly when finding the high correlation in WMSDs and risk factors, transforming the log-SIR back to the original SIR was needed. Furthermore, divided the exposure factors into four groups (Q1-Q3 as the cut point), and showed the relationship between the SIR
od WMSDs and the percentage level of exposure. By comparing the four groups to its SIR, we got the trend of exposure factors in every industries and the risk level of suffering from WMSDs.
Chapter 4 Results
4.1 The collected and classified WMSDs cases for nearly four years (2008-2011)
The ODIS from 2008/01/01 to 2011/12/31 had 4,781 probable or possible cases.
The incidence was 114.1 cases per (106) million working population per year.
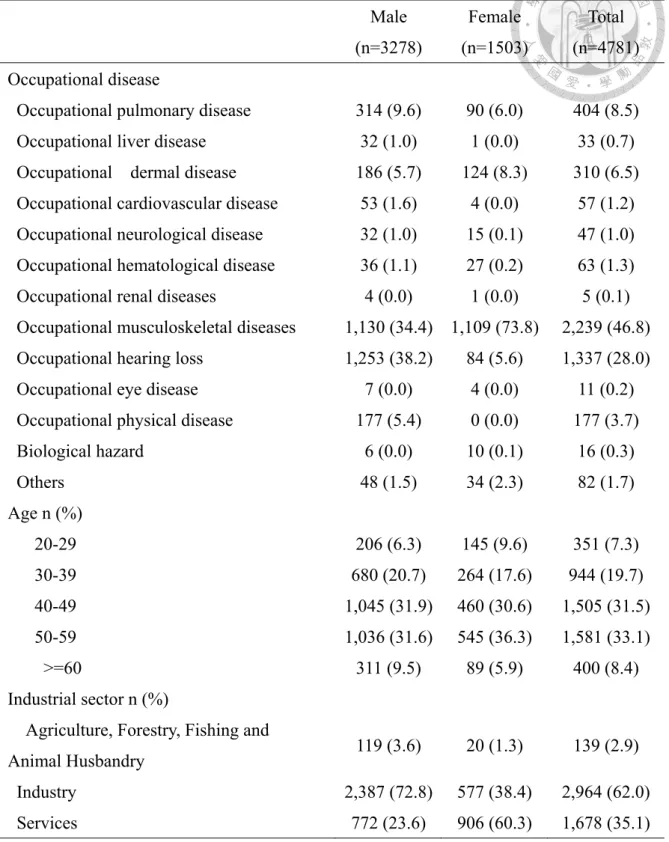
According to the diseases category, the calculated incidence rate cases per 106 working population per year was shown in Table 2. The highest incidence of occupational disease was the occupational musculoskeletal disease (53.5 cases per 106 working population per year), and the second highest one was occupational hearing loss (31.9 cases per 106 working population per year). The following ones were the occupational pulmonary disease (9.6 cases per 106 working population per year), occupational dermal disease (7.4 cases per 106 working population per year), occupational neurological disease (1.1 cases per 106 working population per year) and occupational physical disease (0.4 cases per 106 working population per year). The cases of ODIS, classified by age, sex, disease and industrial sectors from 2008 to 2011, were shown in Table 3.
There were 2,239 WMSDs cases in 2008-2011 accounts for 46.8% of the ODIS reported cases. In Taiwan, WMSDs contributed most in occupational disease. The group of 40-59 years-old was the main age group with 3086 cases (64.5%). From
industrial sector perspective, industry, which accounted for the highest proportion with 2964 cases (62%).
4.2 Selected and recognized the disease types of WMSDs
There were 2,239 reported WMSDs cases from 2008 to 2011, which accounted for 46.8% of all the occupational disease notification. It was divided into four categories according to the diseased parts. The first category was the upper extremities (including hand / wrist, elbow, shoulder). The second one included the cervical and lumbar region.
The third one was the lower extremities (knee, foot / ankle). Two or more diseased parts of the case would be classified in others.
There were 1,467 cases (65.5%) from the upper extremities disease while 637 cases (28.5%) were from cervical and lumbar region disease. Furthermore, there were 56 (2.5%) and 79 (3.6%) cases from the lower extremities disease and other disease, respectively.
There were 1,269 cases from four selected four main diseases from upper extremities and cervical and lumbar region disease, which included 724 cases from carpal tunnel syndrome (CTS), and 545 cases from herniated intervertebral disc (HIVD), respectively. Classification and selection for CTS and HIVD cases were shown in Table 4 and the flow chart of the selected WMSDs cases was shown in Figure 5.
4.3 Standardized incidence rates in different job categories of WMSDs
4.3.1 Different job categories with CTS: case numbers and SIR
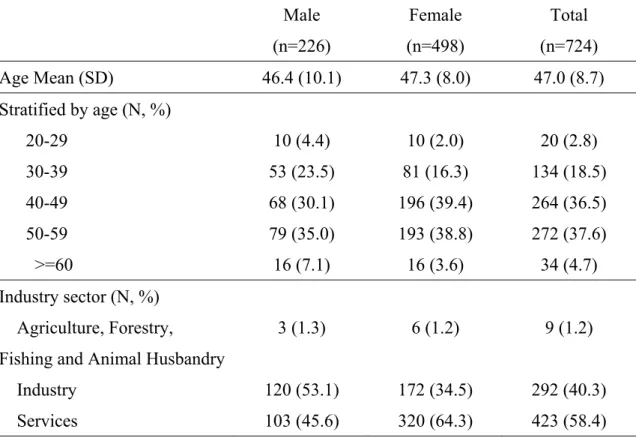
The reported cases of CTS from 2008 to 2011 were 724 cases in total.
In 226 CTS cases for male, the mean age was 46.4 (SD=10.1) years old. The highest two contributors were the sector Industrial (120 cases) and Service (103 cases), respectively. Top three major groups with reported cases were the group Manufacturing (71 cases), Construction (45 cases) and Accommodation and Food Services (39 cases).
In 498 CTS cases for female, the mean age was 47.3 (SD=8.0) years old. The highest two contributors were the sector Service (320 cases) and Industrial (172 cases), respectively. Top three major groups with reported cases were the group Manufacturing (136 cases), Accommodation and Food Services (107 cases) and Other Service (52 cases). The CTS cases with age and industry sector distribution were shown in Table 5.
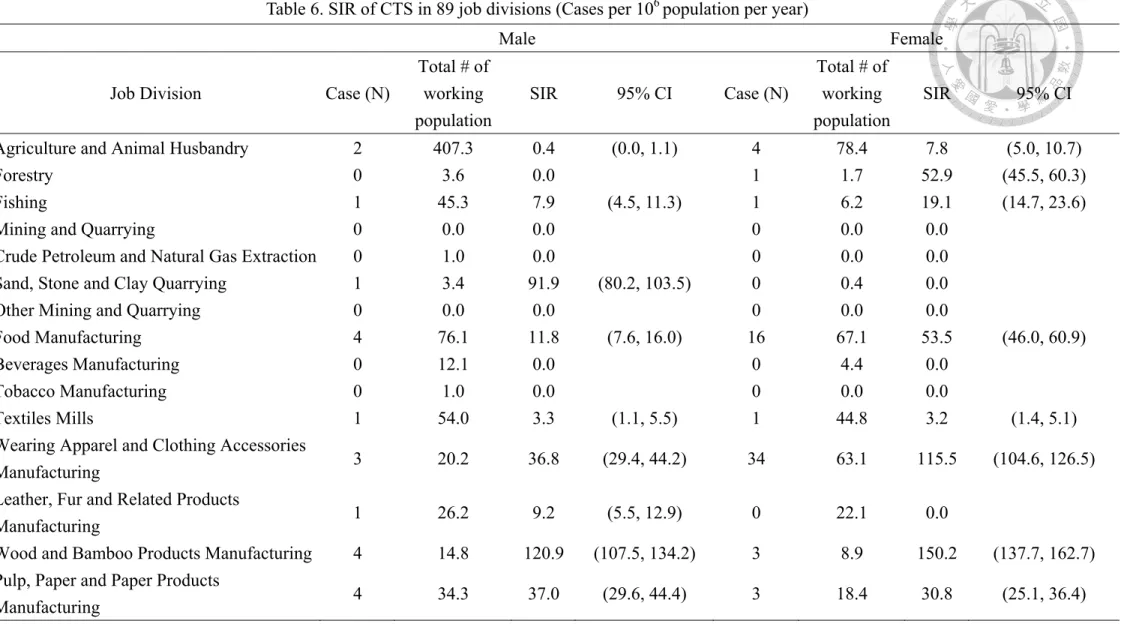
The three major industrial divisions with the highest SIR for male workers with CTS were the division Wood and Bamboo Products Manufacturing (120.9 cases per 106 working population per year), Sand, Stone and Clay Quarrying (91.9 cases per 106 working population per year) and Postal and Courier Services (58.5 cases per 106 working population per year), respectively As for female workers, it became the division Non-metallic Mineral Products Manufacturing (171.4 cases per 106 working
population per year), Buildings Construction (157.0 cases per 106 working population per year) and Residential Care Services (156.1 cases per 106 working population per year), respectively. All the SIR of CTS in job divisions were shown in Table 6.
4.3.2 Different job categories with HIVD: case numbers and SIR
There were 545 cases in total for the HIVD reported from 2008 to 2011.
The mean age was 45.3 (SD=8.9) years old for male in 418 cases with HIVD.
Among these cases, the highest two sectors were from the sector Industrial and Service, which included 250 and 163 cases, respectively. The major group was mainly distributed in the group Manufacturing (126 cases), Transportation and Storage (122 cases) and Construction (106 cases).
The mean age was 49.1 (SD=9.1) years old for female in 127 cases with HIVD.
Among these cases, the highest two sectors were from the sector Industrial and Service, which included 70 and 57 cases, respectively. The major group was mainly distributed in the group Construction (37 cases), Manufacturing (33 cases) and Human Health and Social Work Services (20 cases). The HIVD cases with different age and industry sector distribution were shown in Table 7.
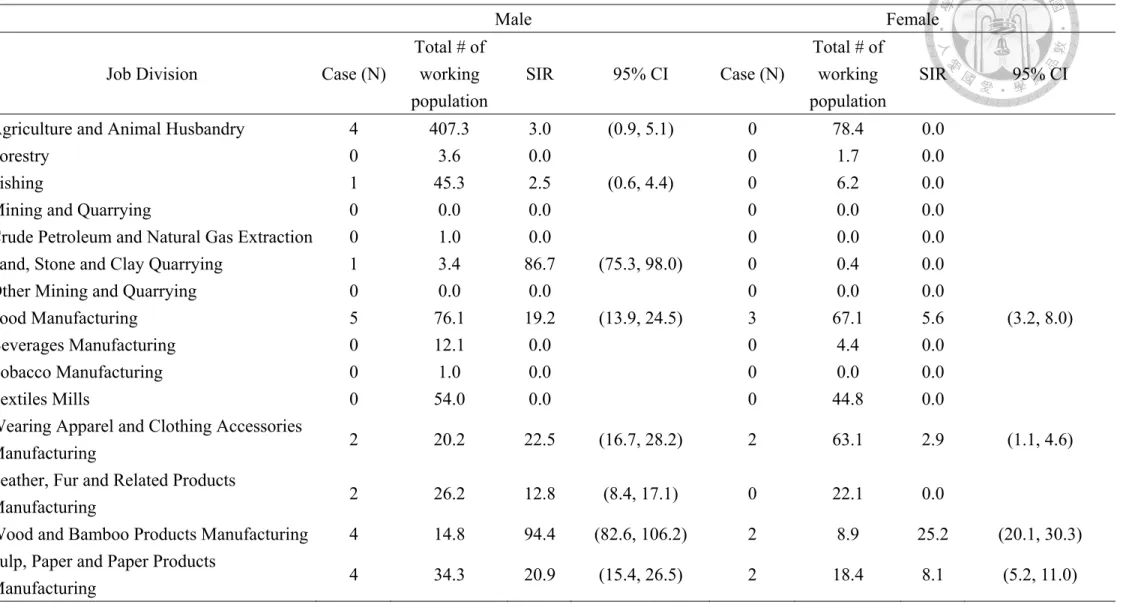
The three job divisions with the highest SIR for male workers with HIVD were the division Warehousing and Storage (213.4 cases per 106 working population per year),
Land Transportation (114.9 cases per 106 working population per year) and Electricity and Gas Supply (114.2 cases per 106 working population per year), respectively. As for female workers, it became the division Residential Care Services (114.5 cases per 106 working population per year), Warehousing and Storage (36.2 cases per 106 working population per year) and Accommodation Services (26.3 cases per 106 working population per year), respectively. All the SIR of HIVD in job divisions were shown in Table 8.
4.4 Survey of Perceptions of Safety and Health in the Work Environment
Survey of Perceptions of Safety and Health in the Work Environment in 2010, including self-reported of the proportion of ergonomic factors and self-reported musculoskeletal discomforts in workplace. The proportion of self-reported ergonomic factors and self-reported musculoskeletal discomfort in workplace were calculated for each job division.
4.4.1 Workplace exposure factors - ergonomic factors
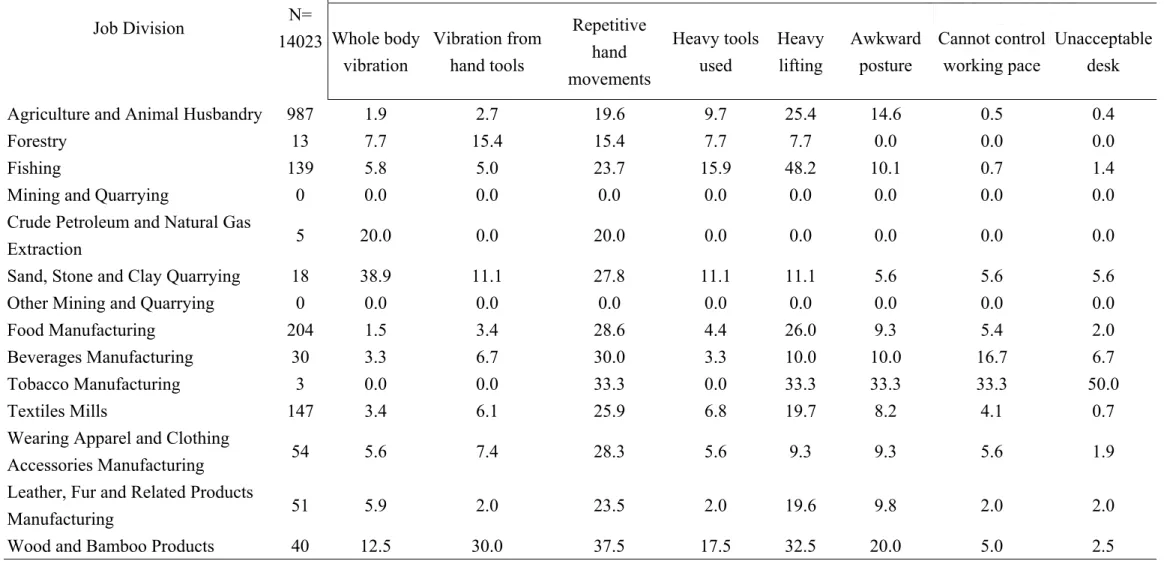
The workplace ergonomic factors for male and female in each job category were from the Survey of Perceptions of Safety and Health in the Work Environment in 2010.
The workplace ergonomic factors for male and female were shown in Table 9-10. From this table, the information about workplace ergonomic factors in 89 job divisions were
given.
For the male, the division Sand, Stone and Clay Quarrying had the largest self-reported proportion that workplace exposure to “whole body vibration” (38.9%);
the division Wood and Bamboo Products Manufacturing had the largest self-reported proportion that workplace exposure to “vibration from hand tools” (30.0%); the division Data Processing and Information Supply Services had the largest self-reported proportion that workplace exposure to “repetitive hand movements” (50.0%); the division Buildings Construction had the largest self-reported proportion that workplace exposure to “heavy tool used” (27.4%); the division Wholesale Trade had the largest self-report proportion that workplace exposure to “heavy lifting” (50%); the division Tobacco Manufacturing had the largest self-reported proportion that workplace exposure to” awkward posture” (33.3%); the division Tobacco Manufacturing had the largest self-reported proportion that workplace exposure to “cannot control working pace ” (33.3%); and division the Tobacco Manufacturing had the largest self-reported proportion that workplace exposure to “unacceptable desk” (50%).
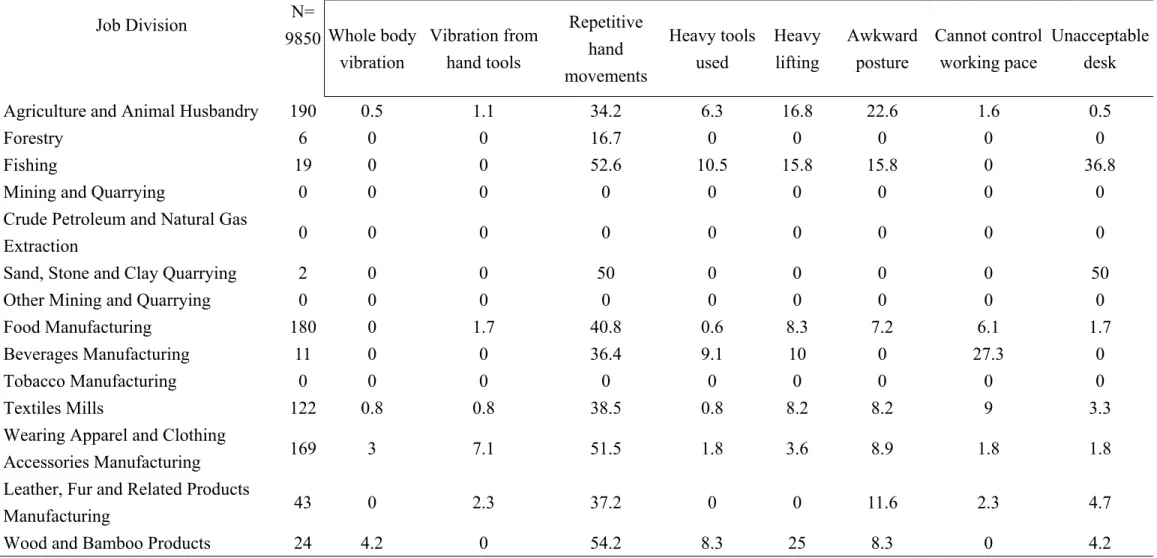
For the female, the division Furniture Manufacturing had the largest self-reported proportion that workplace exposure to “whole body vibration” (9.1%); the division Wearing Apparel and Clothing Accessories Manufacturing had the largest self-reported proportion that workplace exposure to “vibration from hand tools” (7.1%); the division
Electrical Equipment Manufacturing had the largest self-reported proportion that workplace exposure to “repetitive hand movements” (60.0%); the division Buildings Construction had the largest self-reported proportion that workplace exposure to “heavy tool used” (12.1%); the division Wood and Bamboo Products Manufacturing had the largest self-report proportion that workplace exposure to “heavy lifting” (25%); the division Agriculture and Animal Husbandry had the largest self-reported proportion that workplace exposure to” awkward posture” (22.6%); the division Beverages Manufacturing had the largest self-reported proportion that workplace exposure to
“cannot control working pace ” (27.3%); and the division Sand, Stone and Clay Quarrying had the largest self-reported proportion that workplace exposure to
“unacceptable desk” (50%).
4.4.2 Workplace exposure factors - self-reported musculoskeletal discomforts
The self-reported musculoskeletal discomforts for male and female in each job category were from Survey of Perceptions of Safety and Health in the Work Environment 2010. The workplace self-reported musculoskeletal discomforts for male and female were shown in Table 11. From this table we could get the information about workplace self-reported musculoskeletal discomforts in 89 job divisions.
For the male, the division Data Processing and Information Supply Services had
the largest self-reported proportion that subjectively experienced to “hand or wrists discomfort” (25.0%); the division Water Transportation had the largest self-reported proportion that subjectively experienced to “low back and waist discomforts” (31.6%).
As for the female, the division Fishing had the largest self-reported proportion that subjectively experienced to “hand or wrists discomfort” (36.8%); the division Fishing also had the largest self-reported proportion that subjectively experienced to “low back and waist discomforts” (47.4%).
4.5 The relationship between Work-related musculoskeletal disorders and
workplace ergonomic factors
From the literature [4, 12, 28, 29, 34, 41, 42], we chose occupational risk factors that were reported frequently for CTS and HIVD. The factors for CTS were “vibration from hand tools”, “repetitive hand movement”, “heavy tools used” and “cold temperatures”, and factors for HIVD were “whole body vibration”, “heavy tools used”,
“heavy lifting” , “awkward posture” and “unacceptable desk” respectively.
Because the SIR of 89 job divisions were not in normal distribution, we did logarithmic transformation to the SIR of 89 job divisions. Then, simple linear regression was to identify the relationship between SIR of WMSDs (case/year/million workers)
and the workplace ergonomic factors (% reported +).
4.5.1 Log-transformed SIR (case/year/million workers) and workplace ergonomic
factors (% reported +) - CTS
For the male, the increase of the proportion of vibration from hand tools (β: 0.035, 95% CI: 0.016, 0.055), repetitive hand movements (β: 0.036, 95% CI: 0.020, 0.052), and heavy tools used (β: 0.027, 95% CI: 0.006, 0.048) were associated with the in increase in log-transformed SIR of CTS. As for the female, the increase of vibration from hand tools (β: 0.124, 95% CI: 0.063, 0.185) were associated with the increased in log-transformed SIR of CTS. The simple linear regressions in log transformed SIR of CTS and workplace ergonomic factors for the male and female were shown in Table 12.
Then, the multiple linear regression was done for male, and the only chosen risk factors was repetitive hand movements (P=0.0171, aR2=0.19). Multiple linear regression of SIR in CTS and ergonomic risk factors was shown in Table 13.
4.5.2 Log-transformed SIR (case/year/million workers) and workplace ergonomic
factors (% reported +) -HIVD
For the male, the increase of the proportion of whole body vibration (β: 0.120, 95%
CI: 0.095, 0.144), vibration from hand tools (β: 0.049, 95% CI: 0.032, 0.066), heavy
tools used (β: 0.058, 95% CI: 0.041, 0.075), heavy lifting (β: 0.020, 95% CI: 0.011, 0.029) and awkward posture (β: 0.053, 95% CI: 0.033, 0.072) were associated with the increase in log transformed SIR of HIVD. As for the female, whole body vibration (β:
0.114, 95% CI: 0.043, 0.184), heavy tools used (β: 0.085, 95% CI: 0.039, 0.131), heavy lifting (β: 0.023, 95% CI: 0.008, 0.038) and awkward posture (β: 0.038, 95% CI: 0.016, 0.060) were associated with the increased in log transformed SIR of HIVD. The simple linear regressions in log transformed SIR of HIVD and workplace ergonomic factors in male and female were shown in Table 14.
Then, the multiple linear regression was done for both male and female. For the male, the remained variables were whole body vibration and heavy lifting (P<0.0001, aR2=0.55). As for the female, the remained variables were whole body vibration and awkward posture (P=0.0002, aR2=0.17). Multiple linear regression of SIR in HIVD and ergonomic risk factors was shown in Table 15.
4.6 The relationship between the geometric mean of SIR and different levels of
workplace exposure factors
Chose those p-values less than 0.05 from the results of simple linear regression as factors and showed the relationship between the SIR and the percentage of exposure factors.
4.6.1 Geometric Mean SIR of CTS and ergonomic factors
The SIR of CTS was associated with the self-reported percentage of workers exposure to “vibration from hand tools” levels, shown in Figure 6-7. For the male, 1.0 case per 106 working population per year for the lowest quartile of SIR of CTS (range 0%), 2.9 cases per 106 working population per year for the second lowest quartile (0–3%), 3.6 cases per 106 working population per year for the third lowest quartile (3-6.5%), and 5.5 cases per 106 working population per year for the highest quartile (>6.5%). As for the female, 6.4 cases per 106 working population per year for two lowest quartile of SIR of CTS (range 0%), 22.6 cases per 106 working population per year for the third lowest quartile (0-2%), and 32.3 cases per 106 working population per year for the highest quartile (>2%). Each level of groups which included job divisions while covering the percentage range and the groups with their job divisions in
“vibration from hand tools” were shown in Table 16.
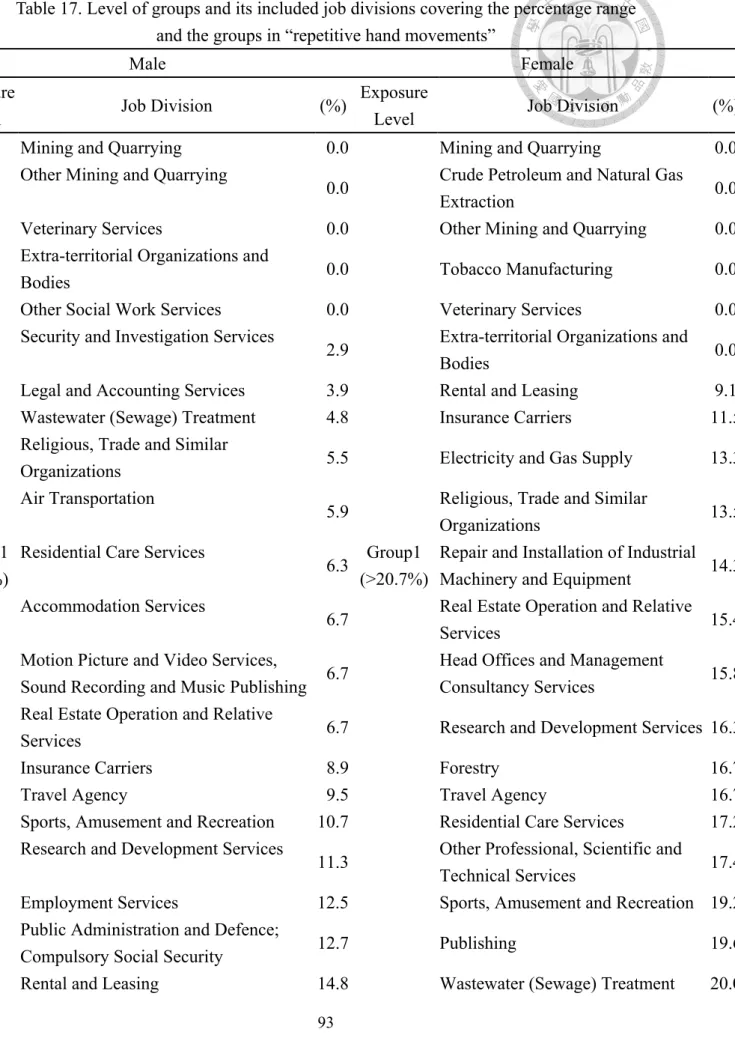
The SIR of CTS was associated with the self-reported percentage of workers exposure to “repetitive hand movements” levels, shown in Figure 8. For the male, 0.4 cases per 106 working population per year for lowest quartile of SIR of CTS (range
<15%), 1.7 cases per 106 working population per year for the second lowest quartile (15%-23%), 5.3 cases per 106 working population per year for the third lowest quartile
(23-30%), and 6.9 cases per 106 working population per year for the highest quartile (>30%). Each level of groups included job divisions which covering the percentage range and the groups with their job divisions in “repetitive hand movements” were shown in Table 17.
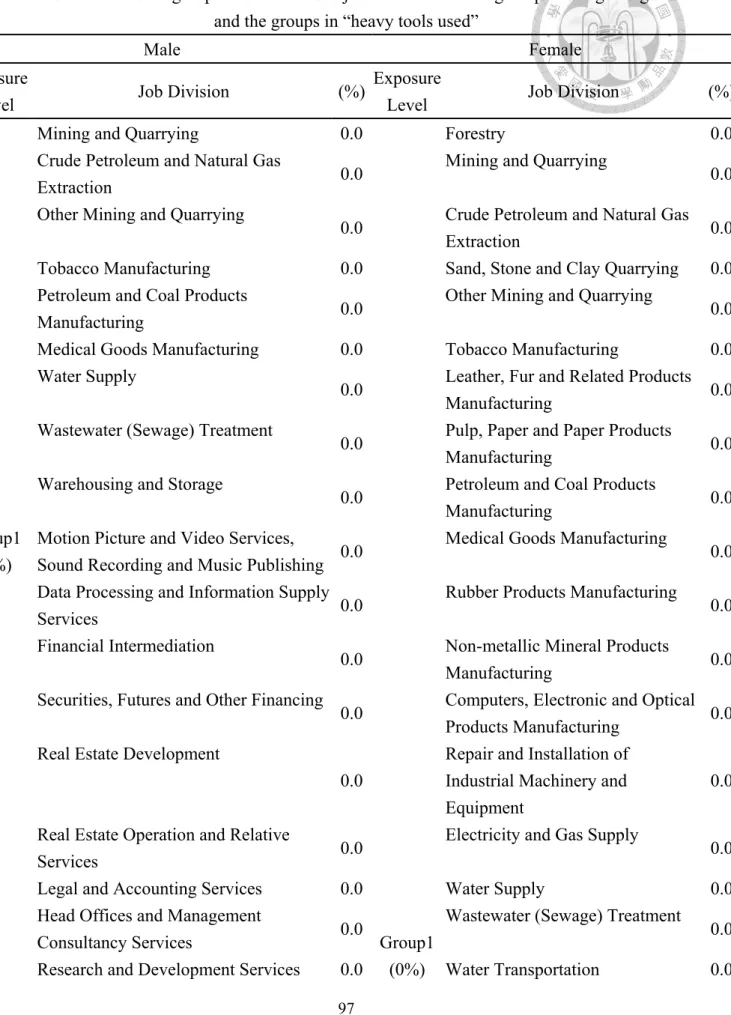
The SIR of CTS was associated with the self-reported percentage of workers exposure to “heavy tools used” levels, shown in Figure 9. For the male, 0.9 cases per 106 working population per year for lowest quartile of SIR of CTS (range 0%), 2.9 cases per 106 working population per year for the second lowest quartile (0%-2.9%), 5.0 cases per 106 working population per year for the third lowest quartile (2.9-8.6%), and 4.1 cases per 106 working population per year for the highest quartile (>8.6%). Each level of groups included job divisions which covering the percentage range and the groups with their job divisions in “heavy tools used” were shown in Table 18.
4.6.2 Geometric Mean SIR of HIVD and ergonomic factors
The SIR of HIVD was associated with the self-reported percentage of workers exposure to “whole body vibration” levels, shown in Figure 10-11. For the male, 1.4 cases per 106 working population per year for lowest quartile of SIR of HIVD (range 0%), 1.8 cases per 106 working population per year for the second lowest quartile
(0–2%), 5.1 cases per 106 working population per year for the third lowest quartile (2-6%), and 27.0 per 106 working population per year for the highest quartile (>6). As for the female, 0.7 cases per 106 working population per year for two lowest quartile of SIR of HIVD (range 0%), 1.5 cases per 106 working population per year for the third lowest quartile (0-1.5%), and 2.2 cases per 106 working population per year for the highest quartile (>1.5%). Each level of groups included job divisions which covering the percentage range and the groups with their job divisions in “whole body vibration”
were shown in Table 19.
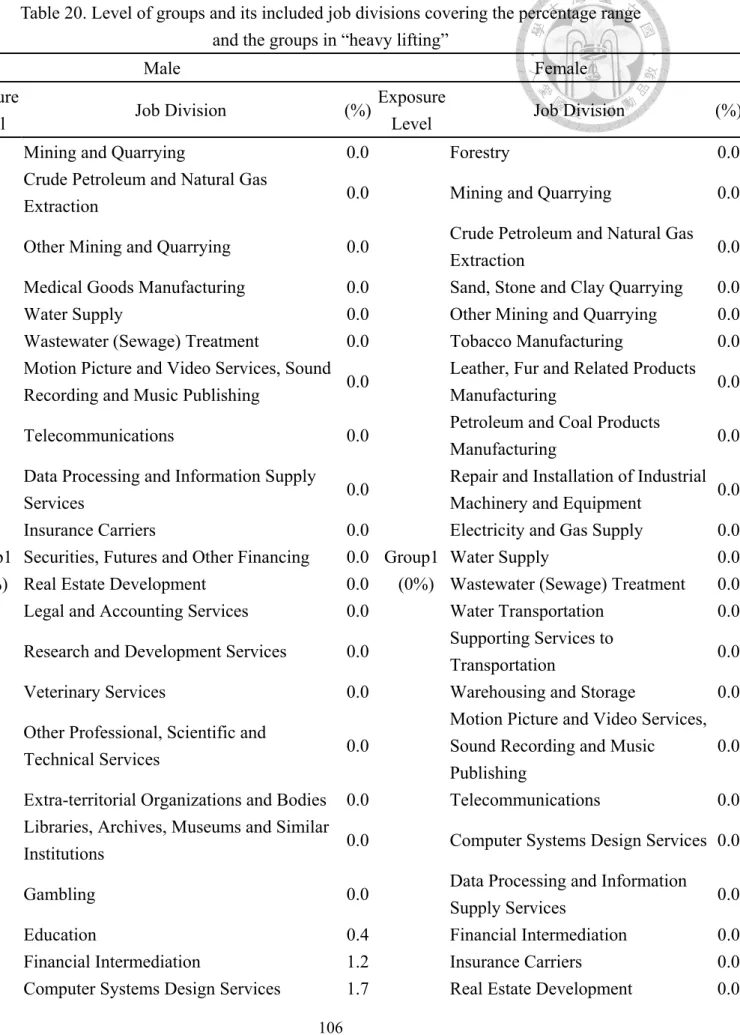
The SIR of HIVD associated with the self-reported percentage of workers exposure to “heavy lifting” levels, shown in Figure 12-13. For the male, 0.7 cases per 106 working population per year for lowest quartile of SIR of HIVD (range <2%), 1.9cases per 106 working population per year for the second lowest quartile (2-10%), 9.6 cases per 106 working population per year for the third lowest quartile (10-25%), and 8.6 cases per 106 working population per year for the highest quartile (>25%). As for the female, 0.4 cases per 106 working population per year for lowest quartile of SIR of HIVD (range 0%), 0.8 cases per 106 working population per year for the second lowest quartile (0-3%), 1.8 cases per 106 working population per year for the third lowest quartile (3-9%), and 1.8 cases per 106 working population per year for the highest quartile (>9%). Each level of groups included job divisions which covering the
percentage range and the groups with their job divisions in “heavy lifting” were shown in Table 20.
The SIR of HIVD associated with the self-reported percentage of workers exposure to “heavy tools used” levels, shown in Figure 14-15. For the male, 1.0 cases per 106 working population per year for lowest quartile of SIR of HIVD (range 0%), 1.4 cases per 106 working population per year for the second lowest quartile (0-2.9%), 6.3 cases per 106 working population per year for the third lowest quartile (2.9-8.6%), and 11.9 cases per 106 working population per year for the highest quartile (>8.6%). As for the female, 0.6 cases per 106 working population per year for two lowest quartile of SIR of HIVD (range 0%), 1.3 cases per 106 working population per year for the second lowest quartile (0-2.8%), and 1.8 cases per 106 working population per year for the third lowest quartile (>2.8%). Each level of groups included job divisions which covering the percentage range and the groups with their job divisions in “heavy tools used” were shown in Table 18.
The SIR of HIVD associated with the self-reported percentage of workers exposure to “awkward posture” levels, shown in Figure 16-17. For the male, 1.7 cases per 106 working population per year for lowest quartile of SIR of HIVD (range <2.1%), 1.1 cases per 106 working population per year for the second lowest quartile (2.1-7.4%), 7.5 cases per 106 working population per year for the third lowest quartile (7.4-10.3%),
and 9.6 cases per 106 working population per year for the highest quartile (>10.3%). As for the female, 0.4 cases per 106 working population per year for lowest quartile of SIR of HIVD (range 0%), 0.8 cases per 106 working population per year for the second lowest quartile (0-4.3%), 1.2 cases per 106 working population per year for the third lowest quartile (4.3-8.7%), and 2.3 cases per 106 working population per year for the highest quartile (>8.7%). Each level of groups included job divisions which covering the percentage range and the groups with their job divisions in “awkward posture” were shown in Table 21.
4.6.3 Combination of risk factors - HIVD
For the male, in the multiple linear regression, workplace without whole body vibration and heavy lifting were used as reference group. When the workers exposed to the workplace with whole body vibration and no exposure to heavy lifting, there was no significant positive relationship between SIR of HIVD and vibration from hand tools.
However, while the workers were exposed to heavy lifting and no exposure to whole body vibration, there had positive relationship between SIR of HIVD and heavy lifting (β: 0.174, 95% CI: 0.011, 0.337). Moreover, when the workers exposed to both whole body vibration and heavy lifting, there were also positive relationship between SIR of HIVD and whole body vibration and heavy lifting (β: 0.532, 95% CI: 0.403, 0.661). For
the male with HIVD, we could find out that there had combinational effect in whole body vibration and heavy lifting. And whole body vibration and heavy lifting factors had an additive effect to HIVD.
As for the female, in the multiple linear regression, workplace without whole body vibration and awkward posture were used as reference group. When the workers exposed to the workplace with whole body vibration and no exposure to awkward posture, there was positive relationship between SIR of HIVD and vibration from hand tools (β: 0.171, 95% CI: 0.002, 0.341). Then, while the workers were exposed to awkward posture and no exposure to whole body vibration, there had positive relationship between SIR of HIVD and repetitive hand movements (β: 0.191, 95% CI:
0.043, 0.339). Moreover, when the workers exposed to both whole body vibration and awkward posture, there were also positive relationship between SIR of HIVD and whole body vibration and awkward posture (β: 0.334, 95% CI: 0.204, 0.465). For the female with HIVD, we could find out that there had combinational effect in whole body vibration and awkward posture. And the whole body vibration and awkward posture factors had an additive effect to HIVD.
The relationship between SIR of HIVD and ergonomic factors within and without combination of risk factors was shown in Table 22-23.
4.7 The relationship between the geometric mean of SIR and different levels of
self-reported musculoskeletal discomforts
4.7.1 Geometric Mean SIR of CTS and hands or wrists musculoskeletal discomfort
The SIR of CTS associated with the self-reported percentage of workers having
“hands or wrists musculoskeletal discomfort” levels, shown in Figure 18-19. For the male, 0.6 cases per 106 working population per year for lowest quartile of SIR of CTS (range 0-3.5%), 3.3 cases per 106 working population per year for the second lowest quartile (3.5-7.5%), 5.5 cases per 106 working population per year for the third lowest quartile (7.5-11.5%), and 3.8 cases per 106 working population per year for the highest quartile (>11.5%). As for the female, 4.2 cases per 106 working population per year for lowest quartile of SIR of CTS (range 0-4.5%), 17.3 cases per 106 working population per year for the second lowest quartile (4.5-11%), 27.6 cases per 106 working population per year for the third lowest quartile (11-16%), and 15.0 cases per 106 working population per year for the highest quartile (>16%). Each level of groups included job divisions which covering the percentage range and the groups with their job divisions in “hands or wrists musculoskeletal discomfort” were shown in Table 24.
4.7.2 Geometric Mean SIR of HIVD and low back or waist musculoskeletal
discomfort
The SIR of CTS associated with the self-reported percentage of workers having
“low back or waist musculoskeletal discomfort” levels, shown in Figure 20. For the male and female, 1.0/0.4 cases per 106 working population per year for lowest quartile of SIR of CTS (range <6%), 2.1/0.7 cases per 106 working population per year for the second lowest quartile (6-10%), 8.1/1.7 cases per 106 working population per year for the third lowest quartile (10-14%), and 10.5/1.5 cases per 106 working population per year for the highest quartile (>14%). Each level of groups included job divisions which covering the percentage range and the groups with their job divisions in “low back or waist musculoskeletal discomfort” were shown in Table 25.
Chapter 5 Field study
5.1 The objective of the field study
Violante et al. [43] defined a “disorder” as a condition that includes both symptoms (subjective evidence perceived by patient) and signs (objective evidence from physical examination) as well as any positive result arising from a diagnostic procedure to identify musculoskeletal pathology. On the other hand, “symptoms”
(including discomfort, complaint and pain) represent subjective feelings [44] and are often self-reported. In order to understand the gap between self-reported symptoms and diagnosed musculoskeletal disorders in upper extremities, a field study was conducted in a factory (division Computers, Electronic and Optical Products Manufacturing).
5.2 Material and method of the field study
First, classified the similar exposure groups by the departments, and chose the departments to conduct the questionnaire. Then, analyzed the questionnaire and screened out the workers who reported to have upper extremity musculoskeletal symptoms (neck, shoulder, elbow, hand or wrist). Case including criteria was shown in Figure 21. Third, doctors with professional training would arrange to do the physical examination to those who reported to have upper extremity musculoskeletal symptoms