行政院國家科學委員會專題研究計畫 成果報告
鼻咽癌之抗藥性及其逆轉:著重於 EB 病毒、一般抗藥機制、
及 HER 訊號傳遞徑路之研究(3/3)
計畫類別: 個別型計畫 計畫編號: NSC91-2314-B-002-134- 執行期間: 91 年 08 月 01 日至 92 年 07 月 31 日 執行單位: 國立臺灣大學醫學院內科 計畫主持人: 鄭安理 計畫參與人員: 鄭安理、徐志宏、高明 報告類型: 完整報告 處理方式: 本計畫可公開查詢中 華 民 國 92 年 10 月 30 日
行政院國家科學委員會補助專題研究計畫成果報告
※※※※※※※※※※※※※※※※※※※※※※※※※
※ ※
※
鼻咽癌之抗藥性及其逆轉—著重於 EB 病毒、
※
※
一般抗藥機制、及 HER 訊號傳遞徑路之研究(3/3) ※
※
※
※ ※
※※※※※※※※※※※※※※※※※※※※※※※※※
計畫類別:5個別型計畫 □整合型計畫
計畫編號:NSC
91-2314-B-002-134-執行期間:
91 年 8 月 1 日至 92 年 7 月 31 日(三年計劃)
計畫主持人: 鄭安理 教授 ([email protected])
共同主持人: 徐志宏 主治醫師([email protected])
陳志榮 副教授 ([email protected])
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
執行單位:國立台灣大學醫學院內科
中 華 民 國 92 年 10 月 25 日
行政院國家科學委員會專題研究計畫成果報告
計畫名稱:鼻咽癌之抗藥性及其逆轉—著重於 EB 病毒、一般抗
藥機制、及 HER 訊號傳遞徑路之研究(3/3)
Drug Resistance and Its Reversal in Nasopharyngeal Carcinoma--
A systemic study on the role of EB virus, Classical drug resistance
mechanisms, and signal transduction pathway of human
epidermal growth factor receptors (HER)
計畫編號:NSC
91-2314-B-002-134-執行期限:
91 年 8 月 1 日至 92 年 7 月 31 日
主持人:鄭安理 台大醫學院內科及台大醫院腫瘤醫學部
共同主持人:徐志宏 台大醫院腫瘤醫學部
共同主持人:陳志榮 中國醫藥學院及台大醫院病理部
一、中英文摘要 中文摘要 鼻咽癌是國人最重要的惡性腫瘤之 一。由於治療學上的進步,現今 50-90% 的局部鼻咽癌患者已可被治癒﹔然而大 多數復發或轉移的鼻咽癌患者,預後仍十 分不好。對此類病患而言,化學治療雖然 在開始治療時極為有效,但卻經常因為癌 細 胞 對 化 學 治 療 藥 物 產 生 抗 藥 性 而 失 敗。過去有關鼻咽癌的抗藥性機轉的研究 並不完整,我們希望藉由本研究能針對此 一問題做一系統性的探討。 在此一三年計劃中,我們嘗試以三個 研究面向來探索這個問題﹕(1). 傳統抗 藥機轉在鼻咽癌細胞化學治療抗藥性所 扮演的角色﹔(2). HER family 在鼻咽癌細 胞 化 學治療抗藥性所扮演的角色﹔(3). EB 病毒在鼻咽癌細胞化學治療抗藥性所 扮演的角色。研究方法包括有體外細胞株 研究,及臨床病理相關性研究。 首先,我們以臨床病理相關性研究方 法來探討傳統的抗藥機轉。我們從 202 位 鼻咽癌患者中挑選了 44 位,這 44 位患者 均因為復發或轉移之鼻咽癌而接受化學 治療為唯一治療策略,而且他們治療前之 組織均也完整地保留。MDR1、GSTπ及 p53 以免疫組織染色測定,進一步與病患 化學治療的成績(包括對化學治療的反應 率及病人的存活期)做相關性研究。我們 的結果顯示:MDR1 是預測病患存活的不 好因子,與化學治療之反應率並無相關。 P53 之高表現卻與較高的化學治療敏感度 呈正相關;P53 高表現病患的存活也有較 好之趨勢。 至於 HER family 之調控與鼻咽癌細 胞株的化療藥物敏感度的研究方面: 首 先我們確定 NPC-TW01, NPC-TW04 及 HONE1 三株鼻咽癌細胞株均表現 HER1 (EGFR) 的 mRNA 及蛋白質;然而,三株 鼻 咽 癌 細 胞 株 HER1 的表現量均少於 A431 (A431 是一株 HER1 表現量十分高 的上皮細胞癌)。使用不同的抑制 HER1 的藥劑,如 PD153035 或 ZD1839 等 HER1 的 tyrosine kinase 抑 制 劑 、 單 株 抗 體 mAb225 等,均可造成鼻咽癌細胞株生長 的抑制;惟其抑制細胞生長的 IC50 均比 A431 的 IC50 來得高。我們進一步針對 NPC-TW04 細胞進行合併 HER1 抑制劑 及 各 種 抗 癌 藥 物 的 實 驗 。 再 同 時 投 予 HER1 抑制劑及各種抗癌藥物時,藥物的 合併效果僅僅呈相互拮抗~相加之效果; 但若在「經 PD153035 或 ZD1839 處理 24小 時 後 再 加 抗 癌 藥 物 」 則 有 較 好 的 synergistic 效果。此外,我們也進一步發 現使用 PI-3K 抑制劑(LY294002,可抑制 PI-3K/Akt 之訊息傳遞徑路)與各種抗癌 藥 物 同 時 使 用 , 可 以 達 到 十 分 明 顯 的 synergistic 效果。 有關 EB 病毒與鼻咽癌細胞化學治療 抗藥性的研究方面,我們先確認了三株鼻 咽癌細胞株均不表現 EB 病毒的各種基因 後,再以基因轉殖方式將 EB 病毒的 Zta 蛋 白轉殖入 NPC-TW04 細胞株,經篩選並確 認有四株轉殖細胞株,這四株轉殖細胞株 均表現 Zta,而且這些轉殖細胞株對不同的 化療藥物的毒殺作用均較其原始細胞更不 敏感。這些資料顯示:在鼻咽癌細胞株大 量表現 Zta 會導致癌細胞抗藥性的產生, 其可能的分子機轉正進一步深入探討中。 關鍵詞:鼻咽癌,化學治療抗藥性,EB 病 毒,EB 病毒之 Zta 蛋白,Human epidermoid growth factor receptor (HER)
Abstract
Nasopharyngeal carcinoma (NPC) is one of the major endemic cancers in Taiwan. Although 50 to 90% of loco-regional NPC patients can be cured by definitive local treatments, the outcome of patients with recurrent or metastatic NPC remains poor. The successful use of systemic chemotherapy, despite high tumor response rate initially, is limited by the emergence of drug resistance in cancer cells. The mechanisms of drug resistance to chemotherapy in NPC have been largely unknown. We thus proposed this 3-year project to study this important issue systemically. Three possible drug resistance mechanisms have been covered, including classical drug resistance mechanisms, the human epidermal growth factor receptor (HER) family, and EBV-viral proteins.
Regarding the classical drug resistance mechanisms of NPC, we performed a clinico-pathological correlation study. From 202 archive NPC patients, 44 who received systemic chemotherapy for
recurrent or metastatic diseases were included because of complete medical records and adequate pre-treatment tissue specimens. Immunohistochemical staining of the expression of MDR1, GSTπ, and p53 were correlated with the treatment outcomes of the patients. The results indicate that MDR1, although correlated with a poor overall survival, did not appear to predict chemoresistance of NPC. Over-expression of p53 by immunohistochemical staining, was associated with a better response rate to systemic chemotherapy and a trend towards better survival.
As for the study of modulation of human epidermoid growth factor receptors in relation to chemoresistance in NPC, 3 NPC cell lines, including NPC-TW01, NPC-TW04, and HONE-1, were employed for in vitro studies. All 3 NPC cell lines expressed mRNA and protein of EGFR, although with expression levels lower than that of A431, an EGFR-overexpressing cell line. Two EGFR-specific tyrosine kinase inhibitors (PD153035 or ZD1839) and a monoclonal antibody to EGFR (mAb 225) inhibited the growth of NPC cells with IC50s
higher than those for A431 cells. The combination effect of EGFR inhibitors and cytotoxic agents were further explored in NPC-TW04 cells. Concomitant treatment of EGFR-inhibitors and cytotoxic chemotherapeutic agents did not improve the growth inhibitory effect. With the pretreatment of PD153035 or ZD1839 for 24 hours followed by cytotoxic agents, the cytotoxicity of several anticancer drugs, including doxorubicin, paclitaxel, cisplatin, and 5-fluororuacil, was improved with the combination index well below 0.5 at fraction inhibition >70%. Further, when cytotoxic chemotherapeutic agents were combined with LY294002, an inhibitor of PI-3K/Akt pathway which was downstream to EGFR, a significantly better synergism was demonstrated. The data suggest that combination of EGFR inhibition with cytotoxic drugs may be further developed as a treatment modality for NPC.
Finally, we also tried to evaluate the possible role of Epstein-Barr virus (EBV) in the development of drug resistance in NPC cells. We first characterized that there was no expression of several EBV viral genes, including BamH1W, BZLF1, and EBNA1, in all 3 NPC cell lines. Zta (ZEBRA, Z, encoded by BZLF1 of EBV), a transcriptional factor responsible for the switch of viral latency into lytic cycles, was selected because several previous studies have shown a close interaction between this viral proteins and several host proteins, including p53, NF-κB, and cyclin kinase inhibitors, which have all bee linked to drug resistance in human cancer cells. At least 4 stable transfectants of a Zta-expressing vector, pRCMV-Zta, were selected from NPC-TW04. Overexpression of Zta message was confirmed by real-time RT-PCR. The IC50s to different kinds of
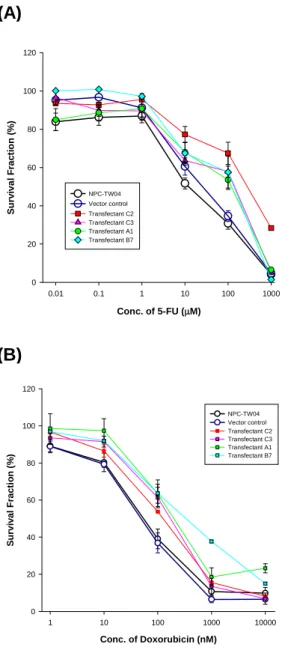
cytotoxic agents in these transfectants were much higher than those of parental lines and vector-control lines, especially to paclitaxel and doxorubicin. These data suggest that over-expression of Zta in NPC cells confers a phenotype of resistance to multiple cytotoxic drugs in vitro. The possible mechanisms underlying this phenotype are now under investigation.
Keywords : Nasopharyngeal carcinoma (NPC), Chemoresistance, Epstein-Barr virus (EBV), Zta protein of EBV, Human epidermoid growth factor receptor (HER)
二、 計畫緣由與目的 (Background) Nasopharyngeal carcinoma (NPC), well known for its distinctive epidemiologic features and association with Epstein-Barr virus (EBV), 1,2,3 is an important endemic malignancy of Taiwan. In 1998, NPC was responsible for more than 800 deaths in Taiwan. 4
Radiotherapy is the standard treatment for loco-regional NPC. Recent progress on incorporating systemic chemotherapy into standard radiotherapy has improved the 5-year survival rates for patient with
loco-regional NPC from 52 to 97%, depending on the clinical stages. 5-7 On the other hand, although combination chemotherapy may result in a high response rate in patients with recurrent or metastatic NPC initially, only less than 10% of these patients can survive more than 2 years. 1,3,8
Inherent or acquired resistance to anticancer drugs is a major obstacle to the success of chemotherapy.9 However, the mechanism of drug resistance of NPC have seldom been studied before.
Traditionally, the drug resistance mechanisms included those specific to drug exporters (such as MDR1 and MRP), detoxification mechanisms (such as GSTπ), and the altered drug targets. Recently, mechanisms related to cell death control and cellular stress response have also been linked to the resistance to chemotherapy. The roles of these markers in the prediction of chemosensitivity in NPC are largely unknown.
The expression of human epidermal growth factor receptor (HER) family, including EGFR (HER1), HER2, has been demonstrated in NPC tissues.10-12 The expression of these markers correlates with advanced stage of disease, predicting a poor clinical outcome. 10 Recently, enhancing chemosensitivity by anti-HER1 or anti-HER2 strategies have been shown in both pre-clinical and clinical studies of a variety of human cancers. 13-15 Whether modulation of HER family can be employed as a treatment modality for NPC has not yet been addressed.
Further, we have been working on drug resistance mechanisms in several virus-associated malignancies for years. We have shown before that a large portion of EBV-associated T-cell lymphoma and Hepatitis B virus (HBV) related hepatocellular carcinoma (HCC), and HTLV-1 associated adult T-cell lymphoma and leukemia (ATLL) express drug resistance markers. 16-20 We also demonstrated that both tax protein of HTLV-1 and pX protein of HBV
transactivated mdr-1 gene expression in T-cell lymphoma and hepatoma cell-lines, respectively.21,22 Whether Epstein-Barr virus (EBV), which is closely associated with NPC and encodes several biologically active viral proteins 23,24 may also contribute to drug resistance of NPC is a testable hypothesis.
In order to understand the possible drug resistance mechanisms of NPC, we planned to investigate the 3 above-mentioned research categories, using different approaches.
Approaches (Materials and Methods):
Two approaches were adopted: (1) in vitro cell-line study; (2). clinico-pathological correlation study.
(1). In vitro cell-line study: Three NPC cell lines, including NPC-TW01, NPC-TW04, and HONE1, were maintained in our laboratory. First, these cells were characterized for the expression of EBV-encoded genes (EBNA1, BamH1W, BZLF1), classical drug resistance markers (MDR1, MRP, GSTπ, TS, TP), and HER family (HER1, HER2, HER3, HER4) by Western blotting and reverse transcriptase polymerase chain reaction (RT-PCR). The sensitivity of these cells to different anticancer drugs, such as cisplatin, 5-FU, doxorubicin, paclitaxel, were determined by MTT assay. Further, we used both negative modulation and positive modulation approaches to try to modify the drug sensitivity profiles of these cells. Specific inhibitors of known signaling pathways, blocking antibodies, and anti-sense approaches were part of negative modulation strategies; gene transfer by transfection or infection was used in positive modulation experiments.
(2). Clinico-pathological correlation study: NPC patients with advanced NPC received systemic chemotherapy as the sole mode of therapy for the recurrent or metastatic disease were included for the clinicopathologic correlation study provided their pre-treatment tissues were adequate for analysis. The tissues were sectioned and
stained with proper antibodies by routine procedures. The clinical endpoints for the analysis were the response to chemotherapy and patients’ survival.
三、 結果與討論
Results
Base-line Characters of NPC Cell-lines The IC50s to 4 different anticancer drugs
for NPC-TW01, NPC-TW04, and HONE1 cells was tabulated in Table1. The classical drug resistance markers, including multi-drug resistance 1 (MDR1) and multidrug resistance- related protein (MRP) for doxorubicin and paclitaxel, glutathione-s- transferase π (GSTπ) for cisplatin, evaluated by RT-PCR; glutathione level measured by colorimetric assay for glutathione; and 4 members of HER family detected by RT-PCR and Western blotting were summarized in Table 2. The IC50 profiles in
3 cells did not differ very much, nor did the expression of the checked drug resistance markers. HER1 (EGFR) was universally expressed in 3 NPC cells, with the levels lower than that of A431, a well-characterized HER1-over-expressing cell line.
As for the expression of several EBV-related genes, we found no amplification of Bam H1W region of EBV genome and EBNA1 form 3 NPC cells by PCR. RT-PCR of BZLF1 and BHRF1 found no amplicon, either.
Correlation of the Expression of Classical Drug Resistance Markers in NPC tissues and Treatment Results of Recurrent or Metastatic NPC :
In a cohort of 202 consecutive patients diagnosed at the Department of Pathology of National Taiwan University Hospital, 44 patients were selected for this analysis. The correlation study was performed on the expression of MDR1, GSTπ, and p53 with tumor response to chemotherapy and survival of the patients.
Thirty-four patients received cisplatin- based regimens, and 28 of them were enrolled in a prospective trial using a
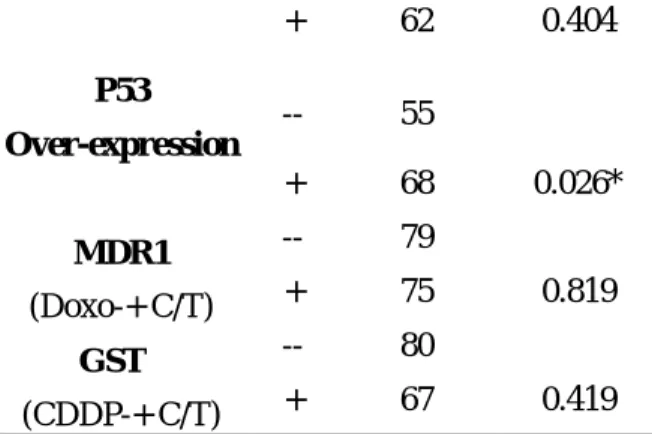
doxorubicin-containing regimen. The overall response rate was 70%. Expression of MDR1 was seen in only 5 cases (11%) and was associated with a significantly worse overall survival (P= 0.028), yet did not appear to predict chemoresistance to the doxorubicin-containing regimen. Over- expression of p53 was seen in 22 patients (50%), and surprisingly, was correlated with chemoresponse (P= 0.026) and a trend towards better survival. GSTπ expression was demonstrated in 13 cases (30%) and was not correlated with chemoresistance to cisplatin-containing regimens and overall survival (Table 3 and Fig.1).
Modulation of HER1 in NPC Cells
Since the 3 NPC cells express HER1, we tested several HER1-inhibitory strategies in NPC cells, focusing on the effects of growth inhibition of single agents or combination with cytotoxic drugs.
Anti-HER1 was achieved by specific monoclonal antibody (mAb225) or by two specific tyrosine kinase inhibitors (PD153035 and ZD1839). A HER1-overexpression cell line, A431, and a HER1-low-expression cell line, MCF7, were included for all of the studies. The IC50s of 3 NPC cells to PD153035 and ZD1839 were 10~20 µM and 20~30 µM, respectively. The IC50 to mAb225 of NPC-TW04 cells was about 3µg/ml. The inhibitory potency of these HER1 inhibitors in NPC cells, reflected by the lower IC50s, was inferior to that in A431 cells, but much higher that that of MCF7 (Fig.
2 & Fig. 3).
The combination effect of EGFR inhibitors and cytotoxic agents were further explored in NPC-TW04. When EGFR inhibitors and cytotoxic agents were used concomitantly for 72 hours, the interaction between drugs were mainly antagonistic by median effect analysis, indicating no chemosensitization effect by EGFR inhibitors
(Fig.4 A~D). However, with pretreatment
of HER1 inhibitors for 24 hours followed by cytotoxic agents, a synergistic interaction of either PD1530305 or ZD1839 with several anticancer drugs, including doxorubicin, paclitaxel, cisplatin, and 5-fluororuacil, can
be demonstrated with combination index well below 0.5 at fraction inhibition >70% (Fig.4 E-H).
Since PI-3K/Akt pathway, one of the important signaling pathways downstream to EGFR, have been shown to involve in resistance to chemotherapeutic agents in cancer cells. We further tested the effect of combining inhibiting PI-3K by LY294002 and cytotoxic chemotherapeutic agents in NPC-TW04 cells. Despite concomitant use of LY294002 and cytotoxic agents, a strong synergistic interaction was clearly demonstrated (Fig. 5).
EBV-encoded Zta Protein and Drug resistance of NPC Cells
The expression of BZLF1 transcript and its coded ZEBRA (Zta, Z, EB1) protein, the pivotal protein responsible for the switch of latent viral infection and lytic infection of EBV, has been demonstrated in NPC tumor cells. 25-27 Zta is a transcriptional factor and acts to activate immediate early and early genes of EBV lytic cycle. It has been reported before that Zta overexpression in human cells can transactivate several human genes. 28-31
A Zta-constitutively expression vector (pRCMV-Zta) driven by CMV-promoter, was constructed, and was introduced to NPC-TW04 cells. At least 4 stable transfectants of Zta were selected from single cell cloning. Overexpression of Zta message was confirmed by real-time RT-PCR.
Cytotoxicity to various kinds of cytotoxic agents was compared in these 4 transfectants, vector-transfected cell line, and parental NPC-TW04 cells. The IC50s to different kinds of cytotoxic agents in these transfectants were much higher than those of parental lines and vector-control lines. (Fig
4).
In order to exclude the possibility of effects conferred through the process of selection, we also checked the growth-inhibition in NPC-TW04 cells in non-selected Zta-overexpressing batches. The data was consistent with what we have observed in stably selected clones.
Discussion
The purpose of this study is to systemically explore the possible drug resistance mechanisms of NPC. Three major categories were covered, including classical drug resistance markers, such as MDR1, GSTπ, and p53, members of HER family, and EBV-encoded Zta protein.
In the clinico-pathologic study, we demonstrated that the expression of MDR1 is uncommon in NPC tissues, does not predict chemoresistance, and appears to be correlated with poor survival. Overexpression of p53 is found in half of the NPC patients and is correlated with a better treatment outcome.
While the significance of MDR1 has been shown to predict poor chemosensitivity and prognosis in many cancers,32-38 the role of MDR1 in NPC has never been reported. On the contrary, there are some other tumors for which MDR1 expression is not correlated with chemoresistance.39-42 Previous studies also pointed out that MDR1 is a marker of aggressive tumor behavior and a poor prognostic factor for patients’ survival.43 Our findings on NPC supported this notion.
Most previous reports indicated that altered p53 function is associated with poor prognosis of patients in a variety of human cancers.44,45 Mutated p53 protein has longer half life and thus results in p53 overexpression in immunohistochemical examination. P53 over- expression has been identified as a poor prognostic factor in a variety of human cancers, including breast cancer, ovarian cancer, stomach cancer, lung cancer, and sarcomas. In some of these cancers, over-expressed p53 was further correlated with chemoresistance. 46 These data are in general consistent with the notion that p53 mutation results in a defective cellular apoptotic response to cytotoxic insults, and leads to chemoresistance of the tumors and a poor outcome. However, p53 over- expression, as detected by immunohistochemical examination, may not
always indicate an underlying p53 gene mutation. For example, while p53 overexpression is detected in the vast majority of testicular cancers, p53 mutation is an extremely rare event.47,48 It appears that a similar situation may exist in NPC, since p53 mutation is also a rare event in NPC, with a prevalence rate ranging from 0 to 20%.49-53 In other words, the overexpression of p53 in NPC or testicular cancers may actually indicate more abundant functional wild-type or mutant p53 molecules, which contribute to a more effective p53-mediated repairing or apoptotic mechanisms following DNA damage. This may help explain the association between chemo-responsiveness and p53 over- expression in our NPC patients.
GSTπ is the prototype of molecules responsible for cellular resistance to cisplatin. Our data did not support its role in the clinical drug resistance of NPC. However, because of limited number of patients in this analysis, further larger-series studies are needed.
Regarding the modulation of HER1 (EGFR) in NPC, our findings showed that several anti-HER1 strategies inhibited the growth of NPC cells, and possibly have some impact on enhancing chemotherapeutic effect of multiple cytotoxic drugs in NPC cells. The results are basically compatible with previous reports on heed and neck squamous cell carcinoma (HNSCC). 10-12,54-56 Interestingly, our in vitro data did not support concomitant use of EGFR-inhibitor and chemotherapeutic agents, which showed basically antagonistic interaction in NPC cells. In stead, we demonstrate two possible ways to achieve chemosensitization effect by manipulating EGFR pathways. One is using the EGFR-inhibitor pretreatment sequence; the other possibility is to modulate molecules downstream to EGFR57-59, which might be more relevant to be resistant to chemotherapy in cancer cells. Our preliminary result did support the PI-3K/Akt pathway is indeed worth of exploring in this angle.
Previous studies of anti-Zta antibody titer on NPC patients and immunohistochemistry of Zta on NPC tissues
supported the expression of Zta in the progressive and metastatic stages of NPC.
60
Overexpression of Zta in various types of cells resulted in alteration of cell cycle propagation, increased metastatic potential, and etc.. P53, cyclin-dependent kinase inhibitors, NF-κB, and tyrosine kinases have been found as targets of Zta overexpression.
28-31, 61-63
Our data did show Zta protein confer a drug resistant phenotype in NPC-TW04 cells. We currently are focusing on p53 and NF-κB, both of which have been linked to chemoresistance in a variety of cancer cells and have also been shown to have protein-protein interaction with Zta.
四、 計畫成果自評(Self Assessment) In this 3-year study, we have made some progress on the planned 3 angles of drug resistance mechanism research of NPC cells. Part of our findings has been published64; others have been presented to annual meetings of ASCO 2002, USA, and annual meeting of AACR 2003. 65,66
Our data have both clinical implication and basic research interest. For the former, our results not only reveal possible predictors for chemotherapy in NPC patients (MDR and p53), but also direct possible approaches to improve efficacy of cancer chemotherapy by modulating EGFR pathway on NPC cells. This information will be very useful in designing clinical protocols in the treatment of advanced NPC patients in the future. On the other hand, how the modulation of signaling pathways leads to chemosensitization effect remains to be clarified. Although our preliminary data indicate the importance of PI-3K/Akt, this surely needs further confirmatory studies. Finally, over-expression of a viral transcriptional factor, Zta, of EBV confers a multi-drug resistance phenotype in NPC cells. Further in-depth mechanistic studies may reveal interesting aspects in terms of the evolution of virus-host cell interaction and possible new approaches to reverse drug resistance in virus-associated malignancies.
五、參考文獻(References)
1. Fandi A, Altun M, Azli N, Armand JP, Cvitkovic E.: Nasopharyngeal cancer: Epidemiology, staging, and treatment.
Semin Oncol 1994;21:382-97.
2. Leibowitz D.: Nasopharyngeal carcinoma: The Epstein-Barr virus association. Semin Oncol 1994;21:376-81.
3. Altun M, Fandi A, Dupuis O, Cvitkovic E, Krajina Z, Eschwege F.: Undifferentiated nasopharyngeal cancer (UCNT): Current diagnostic and therapeutic aspects. Int J
Radiat Oncol Biol Phys 1995;32:859-77.
4. Health Bio-statistics of Taiwan in 1998. Department of Health, Executive Yuan, R.O.C..
5. Al-Sarraf M, LeBlanc M, Giri PG, Fu KK, Cooper J, Vuong T, Forastiere AA, Adams G, Sakr WA, Schuller DE, Ensley JF.: Chemoradiotherapy versus radiotherapy in patients with advanced nasopharyngeal cancer: phase III randomized Intergroup study 0099. J
Clin Oncol 1998; 16(4):1310-7.
6. Cooper JS, Lee H, Torrey M, Hochster H.: Improved outcome secondary to concurrent chemoradiotherapy for advanced carcinoma of the nasopharynx: preliminary corroboration of the intergroup experience. Inter J Radiation
Oncol Biol Physics 2000;47(4):861-6.
7. Cheng SH, Jian JJ, Tsai SY, Yen KL, Chu NM, Chan KY, Tan TD, Cheng JC, Leu SY, Hsieh CY, Huang AT.: Long-term survival of nasopharyngeal carcinoma following Inter J
Radiation Oncol Biol Physics 2000 ;48(5):1323-30.
8. Chan AT, Teo PM, Leung TW, Johnson PJ.: The role of chemotherapy in the management of nasopharyngeal carcinoma. Cancer 1998; 82(6 ):1003-12.
9. Lehnert M.: Clinical multidrug resistance in cancer: a multifactorial problem. Eur J
Cancer 1996;32A:912-20.
10. Roychowdhury DF, Tseng A Jr., Fu KK, Weinburg V, Weidner N.: New prognostic factors in nasopharyngeal carcinoma. Tumor angiogenesis and C-erbB2 expression. Cancer 1996;77(8):1419-26.
11. Jin O, Chen S, Li G, Yao K.: Expression of CerbB-2 and EGFR mRNA in human nasopharyngeal carcinomas and pericarcinomatous tissues. [Chinese] Bulletin
of Hunan Med Univer 1997; 22(6):487-90.
12. Zheng X, Hu L, Chen F.: Christensson B. Expression of Ki67 antigen, epidermal growth factor receptor and Epstein-Barr virus-encoded latent membrane protein (LMP1) in nasopharyngeal carcinoma. Eur J Cancer.
Part B, Oral Oncology 1994;30B(5):290-5.
13. Alaouli MA, Paterson J, Al Moustafa AE, Yen L.: The role of ErbB-2 tyrosine kinase receptor
in cellular intrinsic chemoresistance: mechanisms and implications. Biochem Cell
Biol 1997;75:315-25.
14. Lango MN, Shin DM, Grandis JR.: Targeting growth factor receptors: integration of novel therapeutics in the management of head and neck cancer. Curr Opinion Oncol 2001;13:168-75.
15. Mendelsohn J.: Epidermoidal growth factor receptor inhibition by a monoclonal antibody as anticancer therapy. Clin Cancer Res 1997;3:2703-7.
16. Su IJ, Chang IC, Cheng AL.: Expression of growth-related genes and drug-resistance genes in HTLV-1-positive and HTLV-1-negative post-thymic T-cell malignancies. Annals
Oncol 1991; 2(suppl 2): 151-5.
17. Huang C, Wu M, Xu G, Li D, Cheng H, Tu Z, Jiang H, and Gu J.: Overexpression of the MDR1 gene and P-glycoprotein in human hepatocellular carcinoma. J Natl Cancer Inst 1992; 84: 262-4.
18. Chou YY, Cheng AL, Hsu HC.: Expression of P-glycoprotein and p53 in advanced hepatocellular carcinoma treated by single agent chemotherapy: clinical correlation. J
Gastroenterol Hepatol 1997; 12: 569-75.
19. Cheng AL, Su IJ , Chen YC, Uen WC, Wang CH.: Characteristic clinicopathologic features of Epstein-Barr virus-associated peripheral T-cell lymphoma Cancer 1993; 72: 909-16.
20. Cheng AL, Su IJ, Chen YC, Lee TC, Wang CH.: Expression of p-glycoprotein and glutathione-s-transferase in recurrent lymphoma: The possible role of Epstein-Barr virus, immunophenotypes, and other predisposing factors. J Clin Oncol 1993; 11: 109-15.
21. Chuang SE, Doong SL, Lin MT, Cheng AL: Tax of the human T-lymphotropic virus type I transactivates promoter of the MDR-1 gene.
Biochem Biophysical Res Commun 1997; 238:
482-6.
22. Doong SL, Lin MH, Tsai MM, Li TR, Chuang SE, Cheng AL.: Transactivation of the human MDR1 gene by hepatitis B virus X gene product.
J Hepatol 1998; 29(6):872-8.
23. Rabb-Traub N.: Pathogenesis of Epstein-Barr virus and its associated malignancies. Semin
Virol 1996;7:315-23.
24. Niedobitek G.: Epstein-Barr infection in the pathogenesis of nasopharyngeal carcinoma.
Mol Pathol 2000;53(5):248-54.
25. Cochet C, Martel-Renoir D, Grunewald V, Bosq J, Cochet G, Schwaab G, Bernaudin JF, Joab I..:Expression of the Epstein-Barr virus immediate early gene, BZLF1, in nasopharyngeal carcinoma tumor cells. Virol 1993;197(1):358-65.
26. Martel-Renoir D, Grunewald V, Touitou R, Schwaab G, Joab I.:. Qualitative analysis of the
expression of Epstein-Barr virus lytic genes in nasopharyngeal carcinoma biopsies. J Gen Virol 1995;76:1401-8.
27. Chen CL, Hsu MM, Hsu HC.: Differential expression of EBER1 in nontumor nasopharyngeal biopsies and nontumor component of nasopharyngeal carcinoma.
Intervirol 1996;39:230-5.
28. Lu J, Chen SY, Chua HH, Liu YS, Huang YT, Chang Y, Chen JY, Sheen TS, Tsai CH:. Upregulation of tyrosine kinase TKT by the Epstein-Barr virus transactivator Zta. Journal of
Virology. 2000;74(16):7391-9,
29. Dreyfus DH, Nagasawa M, Kelleher CA, Gelfand EW.: Stable expression of Epstein-Barr virus BZLF-1-encoded ZEBRA protein activates p53-dependent transcription in human Jurkat T-lymphoblastoid cells. Blood. 2000;96(2):625-34.
30. Yoshizaki T, Sato H, Murono S,. Pagano JS, Furukawa M.: Matrix metalloproteinase 9 is induced by the Epstein-Barr virus BZLF1 transactivator. Clinical & Experimental Metastasis.1999;17(5):431-6.
31. Cayrol C. Flemington EK. The Epstein-Barr virus bZIP transcription factor Zta causes G0/G1 cell cycle arrest through induction of cyclin-dependent kinase inhibitors. EMBO
Journal. 1996;15(11):2748-59.
32. Leighton JC, Goldstein LJ: P-glycoprotein in adult solid tumors: expression and prognostic significance. Hematol Oncol Clin North Am 1995;9:251-274.
33. Marie JP: P-glycoprotein in adult hematologic malignancies. Hematol Oncol Clin North Am 1995;9:239-250.
34. Arceci RJ: Clinical significancer of P-glycoprotein in multidrug resistance malignancies. Blood 1993;82:2215-2222.
35. Chan HSL, Thorner PS, Haddad G, Ling V: Immunohistochemical detection of P-glycoprotein: prognostic correlation in soft tissue sarcoma of childhood. J Clin Oncol 1990;8:689-704.
36. Chan HS, Haddad G, Thorner PS, DeBoer G, Lin YP, Ondrusek N, Yeger H, Ling V:P-glycoprotein expression as a predictor of the outcome of therapy for neurobalstoma. N
Eng J Med 1991;325:1608-1614.
37. Verrelle P, Meissonnier F, Fonck Y, Feillel V, Dionet C, Kwiatkowski F, Plagne R, Chassagne J: Clinical relevance of immunohistochemical detection of multidrug resistance p-glycoprotein in breast carcinoma. J Natl Cancer Inst 1991;83:111-116.
38. Baldini N, Scotlandi K, Barbanti-Brodano G, Manara MC, Maurici D, Bacci G, Bertoni F, Picci P, Sottili S, Campanacci M, Serra M: Expression of p-glycoprotein in high-grade osteosarcomas in relation to clinical outcome.
N Eng J Med 1995;333:1380-1385.
39. Pu YS, Tsai TC, Cheng AL, Tsai CY, Tseng NF, Su IJ, Hsieh CY, Lai MK: Expression of MDR-1 gene in transitional cell carcinoma and its correlation with chemotherapy response. J
Urol 1996;156:271-275.
40. Kawasaki M, Nakanishi Y, Kuwano K, Takayama K, Kiyohara C, Hara N: Immunohistochemically detected p53 and P-glycoprotein predicts the response of chemotherapy in lung cancer. Eur J Cancer 1998;34:1352-1357.
41. Linn SC, Pinedo HM, van Ark-Otte J, van der Valk P, Hoekman K, Honkoop AH, Vermorken JB, Giaccone G: Expression of drug resistance proteins in breast cancer, in relation to chemotherapy. Int J Cancer 1997;71:787-795.
42. Yeh KH, Chen CL, Shun CT, Lin JT, Lee WJ, Lee PH, Chen YC, Cheng AL: Relatively low expression of multidrug resistance-1 (MDR-1) and its possible clinical implication in gastric cancers. J Clin Gastroeneterol
1998;26:274-278.
43. Pinedo HM, Giaccone G: P-glycoprotein—a marker of cancer cell behavior. N Eng J Med 1995;333:459-462.
44. Chang F, Syrjanen S, Syrjanen K: Implications of the p53 tumor-suppressor gene in clinical oncology. J Clin Oncol 1995;13:1009-1022.
45. Ruley HE: p53 and response to chemotherapy and radiotherapy. Important Advances in
Oncology 1996:37-56.
46. Ferreira CG, Tolis C, Giaccone G: P53 and chemosensitivity .Ann Oncol 1999; 10:1011-21.
47. Eid H, Geczi L, Magori A, Bodrogi I, Institoris E, Bak M: Drug resistance and sensitivity of germ cell testicular tumors: evaluation of clinical relevance of MDR1/Pgp, p53, and metallothionein (MT) proteins. Anticancer Res 1998; 18:3059-3064.
48. Schenkman NS, Sesterhenn IA, Washington L, Tong Y, Weghorst CM, Buzard GS, Srivastava S, Moul JW: Increased p53 protein does not correlate to p53 gene mutations in microdissected human testicular germ cell tumors. J Urol 1995; 154(2 Pt 1):617-621.
49. Chakrani F, Aramnd JP, Lenoir G, Ju LY, Liang JP, May E, May P: Mutations clustered in exon 5 of the p53 gene in primary nasopharyngeal carcinomas from southeastern Asia. Int J
Cancer 1995;61:316-320.
50. Lo KW, Mok CH, Huang DP, Liu YX, Choi PH, Lee JC, Tsao SW: P53 mutation in human nasopharyngeal carcinomas. Anticancer Res 1992;12:1957-1963.
51. Lung ML, Hu Y, Cheng Y, Li MF, Tang CM, O SK, Iggo RD: P53 inactivation mutations in Chinese nasopharyngeal carcinomas. Cancer
Letters 1998;111:89-94.
52. Sheu LF, Chen A, Tseng HH, Leu FJ, Lin JK,
Ho KC, Meng CL: Assessment of p53 expression in nasopharyngeal carcinoma.
Human Pathol 1995;26:380-386.
53. Murono S, Yoshizaki T, Park CS, Furukawa M: Association of Epstein-Barr virus infection with p53 protein accumulation but not bcl-2 protein in nasopharyngeal carcinoma. Histopathol 1999;34(5):432-438.
54. Hoffmann T, Hafner D, Ballo H, Haas I, Bier H.: Antitumor activity of anti-epidermal growth receptor monoclonal antibodies and cisplatin in ten human head and neck squamous cell carcinoma lines. Anticancer Res 1997;17:4410-26.
55. Sirotnak FM, Zakowski MF, Miller VA, Scher HI, Kris MG: Efficacy of cytotoxic agents against human tumor xenografts in markedly enhanced by coadministration of ZD1839 (Iressa), an inhibitor of EGFR tyrosine kinase. Clin Cancer Res 2000;6:4885-92.
56. Ciardiello F, Caputo R, Biano R, Damiano V, Pomatico G, Placido SD, Bianco AR, Tortora G: Antitumor effect and potentiation of cytotoxic drugs activity in human cancer cells by ZD1839 (Iressa), an epidermal growth factor receptor-selective tyrosine kinase inhibitor. Clin Cancer Res 2000;6:2053-63.
57. Gill GN, Bertics PJ, Santon JB: Epidermal growth factor and its receptor. Mol Cell
Endocrinol 51: 169-186, 1987.
58. Wells A: EGF receptor. Int J Biochem Cell
Biol 31: 637-643, 1999.
59. Prenzel N, Fischer OM, Streit S, Hart S, Ullrich: The epidermal growth factor receptor family as a central element for cellular signal transduction and diversification. Endocrine-related Cancer 8: 11-31, 2001.
60. Yip TTC, Ngan RKC, Lau WH, Poon YF, Joab I, Cochet C, Cheng AKP.: A possible prognostic role of immunoglobulin-G antibody against recombinant Epstein-Barr virus BZLF-1 transactivator protein ZEBRA in patients with nasopharyngeal carcinoma. Cancer 1994; 74: 2414-24.
61. Dreyfus DH, Nagasawa M, Kelleher CA, Gelfand EW. Stable expression of Epstein-Barr virus BZLF-1-encoded ZEBRA protein activates p53-dependent transcription in human Jurkat T-lymphoblastoid cells. Blood. 2000;96(2):625-34.
62. Zhang Q, Gutsch D, Kenney S. Functional and physical interaction between p53 and BZLF1: implications for Epstein-Barr virus latency. Mol
Cell Biol 1994; 14(3):1929-38.
63. Gutsch DE, Holley-Guthrie EA, Zhang Q, Stein B, Blanar MA, Baldwin AS, Kenney SC. The bZIP transactivator of Epstein-Barr virus, BZLF1, functionally and physically interacts with the p65 subunit of NF-kappa B. Mol Cell
64. Hsu CH, Chen CL, Hong RL, Chen KL, Lin JF, Cheng AL: Prognostic value of multidrug resistance 1 (MDR1), glutathione-S-transferase
π (GSTπ), and p53 in advanced nasopharyngeal carcinoma (NPC) treated with systemic chemotherapy. Oncology 2002; 62: 305-12.
65. Hsu CH, Chen CL, Chou CH, Gao M, Yeh PY, Cheng AL.: Inhibition of Epidermoid growth factor receptor (EGFR) signaling pathway enhances the chemosensitivity of nasopharyngeal cancer (NPC) cells In Vitro. Proc Am Soc Clin
Oncol 2002; 21(Abstract).
66. Hsu CH, Gao M, Chuang SE, Yeh PY, Hsiech HY, Cheng AL.: Overexpression of Zta protein of EBV confers a multidrug resistance in NPC cells in vitro. Proc Am Asso Cancer Res 2003;22 (Abstract).
Table 1. IC50s to Anticancer Drugs NPC Cell Lines NPC- TW01 NPC- TW04 HONE1 CDDP (µM) 5.3 ± 2.5 3.0 ± 0.1 1.8 ± 0.2 5-FU (µM) 11.4 ± 5.2 8.4 ± 3.9 17.3 ± 3.2 DOXO (nM) 0.27 ± 0.02 0.44 ± 0.06 0.27 ± 0.05 Taxol (nM) 3.0 ± 4.7 59.3 ± 102 6.4 ± 5.4
Table 2. Drug-resistance Markers in NPC cells NPC- TW01 NPC- TW04 HONE1 MDR11 -- -- -- MRP1 + + + GSTπ1 + + + G-SH 3 21.85 17.76 16.95 HER12 + + + HER22 +* +* +* HER31 -- -- -- HER41 -- -- --
1. Checked by RT-PCR; 2. Checked both by RT-PCR and Western blotting; 3. Checked by colorimetirc glutathione detection kit (expressed as µM/µg of cellular protein) * The expression of HER2 in under verification.
Table 3. Correlation of MDR1, GSTπ, p53
with Treatment Response for 44 NPC patients Response rate P-Value MDR1 -- 72 + 60 0.589 GSTπ -- 74 + 62 0.404 P53 Over-expression -- 55 + 68 0.026* MDR1 -- 79 (Doxo-+ C/T) + 75 0.819 GSTπ -- 80 (CDDP-+ C/T) + 67 0.419
Fig.1 Survival curves for patients with metastatic or recurrent NPC treated with systemic chemotherapy. Analysis was mode
according to the expression of different markers: (A), MDR1; (B)
GSTπ; (C)p53.
Cytotoxicity Effect of PD13035 on A431, MCF7, and NPC Cells
Conc. of PD153035 (µM) 0.001 0.01 0.1 1 10 100 S u rv iv a l P roba bi li ty ( % ) 0 20 40 60 80 100 120 A431 NPC-TW01 NPC-TW04 HONE1 MCF7 Cytotoxicity Effect of ZD1839 on A431, MCF7, and NPC Cells
Conc. of ZD1839 (µM) 0.001 0.01 0.1 1 10 100 S u rv iv a l P roba bi lit y ( % ) 0 20 40 60 80 100 120 A431 NPC-TW01 NPC-TW04 HONE1 MCF7
Effect on A431 Cells
Conc. of Antibody (µg/ml) 0.1 1 10 S u rv iv al P ro b ab ilit y ( % ) 0 20 40 60 80 100 120 mouse IgG mAb 225 Effect on NPC-TW04 Cells Conc. of Antibody (µg/ml) 0.1 1 10 S u rv ival P ro b ab ilit y ( % ) 0 20 40 60 80 100 120 mouse IgG mAb 225 (A) MDR1(--) MDR1(+) p=0.028 (B) GST-low expression GST-high expression p=0.896 (C) P53-over-expression P53- not overepression p=0.171
Fig 2. Growth Inhibitory Effect of HER1-specific tyrosine kinase inhibitors (PD153035, left; ZD1839, right) in NPC cells, A431 cells, and MCF7 cells.
Fig 3. Growth Inhibitory Effect of mAb225 (a murine monoclonal antibody against EGFR) in A431 and NPC-TW04 cells. cells, and MCF7 cells.
(E): Effect of Combining Cisplatin
Fraction Affected (Fa)
0.0 0.2 0.4 0.6 0.8 1.0 C o m b in at io n In d ex ( C I) ( in L o g10 scale) 0.001 0.01 0.1 1 10 100 1000 ZD1839 PD153035
(F): Effect of Combining 5-Fluorouracil
Fraction Affected (Fa)
0.0 0.2 0.4 0.6 0.8 1.0 C o m b in atio n In d ex ( C I) (in L o g10 scale) 0.001 0.01 0.1 1 10 100 1000 ZD1839 PD153035
(G): Effect of Combining Doxorubicin
Fraction Affected (Fa)
0.0 0.2 0.4 0.6 0.8 1.0 Co m b in at io n In d ex ( C I) ( in L o g10 scale ) 0.001 0.01 0.1 1 10 100 1000 ZD1839 PD153035
(H): Effect of Combining Paclitaxel
Fraction Affected (Fa)
0.0 0.2 0.4 0.6 0.8 1.0 C o m b in atio n In d ex (C I) ( in L o g10 scale) 0.001 0.01 0.1 1 10 100 1000 ZD1839 PD153035
(A): Effect of Combining Cisplatin
Fraction Affected (Fa)
0.0 0.2 0.4 0.6 0.8 1.0 Co m b in at io n In d ex ( C I) ( in L o g10 scale) 0.001 0.01 0.1 1 10 100 1000 ZD1839 PD153035
(B): Effect of Combining 5-Fluorouracil
Fraction Affected (Fa)
0.0 0.2 0.4 0.6 0.8 1.0 C o m b in at io n In d e x (C I) ( in L o g10 scale) 0.001 0.01 0.1 1 10 100 1000 ZD1839 PD153035
(C): Effect of Combining Doxorubicin
Fraction Affected (Fa)
0.0 0.2 0.4 0.6 0.8 1.0 Co m b in at io n In d ex ( C I) ( in L o g10 scale) 0.001 0.01 0.1 1 10 100 1000 ZD1839 PD153035
(D): Effect of Combining Paclitaxel
Fraction Affected (Fa)
0.0 0.2 0.4 0.6 0.8 1.0 C o m b in at io n In d ex ( C I) (in L o g10 scale) 0.001 0.01 0.1 1 10 100 1000 ZD1839 PD153035
Concomitant Exposure Pretreatment 24 hours
Fig 4. Combination effect of EGFR-TK inhibitors (PD98059 or ZD1839) and different cytotoxic chemotherapeutic agents in growth-inhibitory effect of NPC-TW04 cells, evlauted by median effect analsyis.
Fraction Affected (Fa) 0.0 0.2 0.4 0.6 0.8 1.0 C o m b in ation Ind ex ( C I) 0.001 0.01 0.1 1 10 100 1000 (A) Doxorubicin
Fraction Affected (Fa)
0.0 0.2 0.4 0.6 0.8 1.0 C o m b in atio n Ind e x ( C I) 0.001 0.01 0.1 1 10 100 1000
Fraction Affected (Fa)
0.0 0.2 0.4 0.6 0.8 1.0 C o m b in atio n Ind e x ( C I) 0.001 0.01 0.1 1 10 100 1000 (C) Cisplatin (B) Paclitaxel
Fraction Affected (Fa)
0.0 0.2 0.4 0.6 0.8 1.0 C o m b in atio n Ind ex ( C I) 0.001 0.01 0.1 1 10 100 1000 (D) 5-Fluorouracil
Fig 5. Combination effect of PI-3K/Akt inhibitor
(LY294002) and different cytotoxic
chemotherapeutic agents in growth-inhibitory effect of NPC-TW04 cells: Cells were treated with both drugs concomitantly for 72 hours.
Fig 6 Cytotoxicity Effect of 5-FU (panel A) and Doxorubicin (panel B) in NPC-TW04 cells, vector control cells, and pRCMV-Zta- over- expressing transfectants (C2,C3, B7, A1). (Data regarding cisplatin and paclitaxel, which showed similar tendency was not included in this figure.) Conc. of 5-FU (µM) 0.01 0.1 1 10 100 1000 S u rv iv al F rac ti on ( % ) 0 20 40 60 80 100 120 NPC-TW04 Vector control Transfectant C2 Transfectant C3 Transfectant A1 Transfectant B7 Conc. of Doxorubicin (nM) 1 10 100 1000 10000 S u rv iv al Fr act io n ( % ) 0 20 40 60 80 100 120 NPC-TW04 Vector control Transfectant C2 Transfectant C3 Transfectant A1 Transfectant B7 (A) (B)